Parathyroid Imaging in Twyla B Bartel, DO, MBA, FACNM
|
|
|
- Theodore Cole
- 6 years ago
- Views:
Transcription

1 Parathyroid Imaging in 2015 Twyla B Bartel, DO, MBA, FACNM
2 I do not have any relevant financial and nonfinancial disclosures to make.

3 Incidence ~1 per 1,000 in general population in USA Incidence increases with age & especially in postmenopausal women (female-to-male ratio 3:1; up to ~21 per 1,000 in post-menopausal women) MC in Blacks Incidence of Primary Hyperparathyroidism Lower in countries where serum calcium is not yet routinely measured Deshmukh RG et al. Primary hyperparathyroidism presenting with pathological fracture. J Royal Coll of Surg. 1998;43: Bolland MJ et al. Association between primary hyperparathyroidism and increased body weight: a metanalysis. 2004;90:1525. Yeh MW et al. Incidence and primary hyperparathyroidism in a racially mixed population. J Clin Endocrinol Metab. 2013; 98:
: - 3 rd pharyngeal pouch - Anywhere along where thymus travels during development, but usually posterolateral to lower thyroid")
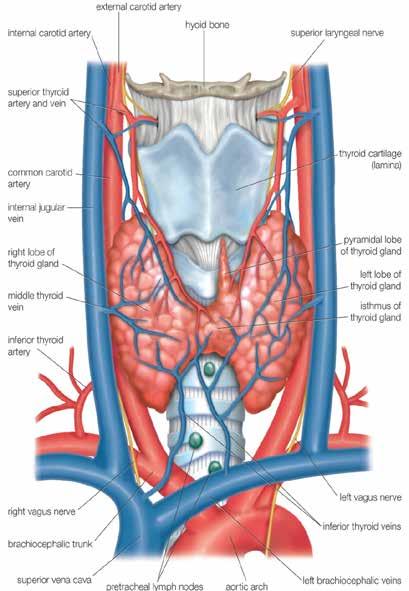
4 Most have 2 upper & 2 lower Anatomy Thyroid Parathyroid Upper (superior): - 4 th pharyngeal pouch - Posterolateral to upper thyroid lobes - Usually 1-2 cm superior to recurrent laryngeal nerve Lower (inferior): - 3 rd pharyngeal pouch - Anywhere along where thymus travels during development, but usually posterolateral to lower thyroid lobes

5 16% incidence of ectopic glands MC ectopic sites mirror routes of descent Intra-Thymic & Intra-Thyroidal 33-38% Retroesophageal 31% Phitayakorn R et al. Incidence and location of ectopic abnormal parathyroid glands. Am J Surg. 2006;191: Gomes EMS et al. Ectopic and extranumerary parathyroid glands location in patients with hyperparathyroidism secondary to end-stage renal disease
, bone (resorption) to raise serum calcium levels PTH biog1105-1106.org Rapidly metabolized by liver (70%)/kidneys (20%), disappearing from circulation with biologic T1/2 of 2-3 min")
6 Function PTH Regulates free ionized calcium Negative feedback system Synthesized in parathyroid chief cells & secreted in response to low calcium levels Acts on kidneys (absorption), intestines (resorption), bone (resorption) to raise serum calcium levels PTH biog org Rapidly metabolized by liver (70%)/kidneys (20%), disappearing from circulation with biologic T1/2 of 2-3 min
7 Hyperparathyroidism Signs/SXs stones, bones, abdominal groans, and psychic moans GI GU MS Dry mouth, thirst, polydipsia, anorexia, nausea, vomiting, constipation Polyuria/nocturia,renal stones, nephrocalcinosis, uremia Fatigue, muscle weakness, arthralgia, bone pain, osteoporosis Neuro Drowsiness, lethargy, stupor, confusion Most (~50%) are asymptomatic at presentation Brown tumors, osteitis fibrosa cystica, pathologic fractures, etc.
8 Lab Investigation Blood tests - Calcium - PTH - Bone markers (alkaline phosphatase, osteocalcin marker for bone formation) - Others (phosphorous, vitamin D) Urine - 24-hr urinary calcium
9 Forms of Hyperparathyroidism PRIMARY MC form Intrinsic parathyroid abnormality Characterized by PTH, Ca, phosphate
10 Forms of Hyperparathyroidism PRIMARY Single adenoma in 80-90% Multiple in 10-19% - Hyperplasia - Multiple Endocrine Neoplasia - Multiple Adenomas (2-3%) Malignancy < 1%
11 Forms of Hyperparathyroidism SECONDARY Hypertrophy of glands as compensation for another dysfunctional organ (i.e. chronic renal failure, Paget s disease, multiple myeloma) Elevated PTH in response to chronic hypocalcemia
12 Forms of Hyperparathyroidism TERTIARY Usually state of excessive secretion of PTH after a long period of secondary hyperparathyroidism and resulting hypercalcemia Irrepressible PTH
13 Imaging Ultrasound MRI Conventional CT 4DCT Interventional Scintigraphy
14 Imaging Many surgeons advocate for 2 concurrent imaging studies for localizing a parathyroid adenoma US and scintigraphy level II evidence as first-line imaging (US first, then scintigraphy confirmatory) Phillips CD, Shatzkes DR. Imaging of the parathyroid glands. Semin US CT MR. 2012; 33:123-9.
 Sensitivity 88% Specificity 82% MIBI (SPECT) 100% 85% MRI 94% 95% Denham et al.")
15 Imaging Performance N = 56 Mohammadi A et al. Preoperative localization of parathyroid lesion: diagnostic usefulness of color doppler ultrasonography. Int J Clin Exp Med. 2012;5:80-6. MIBI (planar) Sensitivity 88% Specificity 82% MIBI (SPECT) 100% 85% MRI 94% 95% Denham et al. J Am Coll Surg 1998;186: Meta-analysis of 50 studies 4DCT - 92% sensitivity, 93% specificity Chazen JL et al. AJNR. 2012;33: N = 35 CEUS - Did not improve from US or MIBI Karakas E et al. J Clin Imaging Sci. 2012;2:64 N = 25
16 Ultrasound Considered a first line modality Noninvasive localization Supine & neck hyperextended Longitudinal and transverse images from carotid bifurcations to sternal notch Measurements in 3 dimensions Evaluate relationship to thyroid gland; may be intrathyroidal May not see PA unless > 1 cm Sensitivity 53-88%; Specificity 40-98% 2013 AIUM/ACR Guidelines
")

17 Homogeneously hypoechoic to thyroid gland, ovoid Doppler may show feeding vessel with arc or rim of hypervascularity & entering at one pole of the gland (Polar Vessel Sign) Increases sensitivity Lane MJ, Desser TS, Weigel RJ et al. Use of power and color Doppler sonography to identify feeding arteries associated with parathyroid adenomas. AJR; 1998; 171:
18 MRI Not typically first line Surface neck and chest coils for mediastinum Hyoid bone to lung apices; 3 mm thickness T1 hypointense, T2/STIR hyperintense, avid enhancement (but 30% without this typical pattern) Sensitivity 64 78%; Specificity 88 95% Useful for detecting ectopic mediastinal glands (sensitivity > 80%) Medscape Dijkstra B, Healy C, Kelly LM et al. Parathyroid localization current practice. J R Coll Edinb. 2002; 47:
19 MRI FP: lymph nodes, thyroid nodules (adenomas, exophytic colloid cysts), enlarged cervical ganglia, other neck masses (sarcoid nodules, neurofibromas) FN: small parathyroid glands, concomitant thyroid disease, anatomic distortion from prior surgery, atypical signal

20 Pre and post-contrast T1 MRI From Terris Parathyroid Book Chapter right inferior parathyroid adenoma (enhances)
21 Conventional CT Not typically first-line More difficult to localize PA s above shoulders and in neck region Sensitivity 46 80%; Specificity 88 90% Medscape Dijkstra B, Healy C, Kelly LM et al. Parathyroid localization current practice. J R Coll Edinb. 2002; 47:
22 4DCT 4 th Phase = contrast enhancement with time NECT followed by 3-phase CECT (75 cc iohexol 300 IV; Imaging at 30, 60, and 90 sec (Philips Brilliance 64-slice scanner (120 kvp, mas, 2.0 mm)) Mandible to carina NECT can help distinguish PA from intrinsically dense iodine-rich thyroid gland (esp if intrathyroidal); PA demonstrates attenuation similar to muscle CECT demonstrates hypervascular PA (early enhancement) with characteristic early washout May see an extrathyroidal feeding artery entering one pole of the parathyroid adenoma (Polar Vessel Sign)
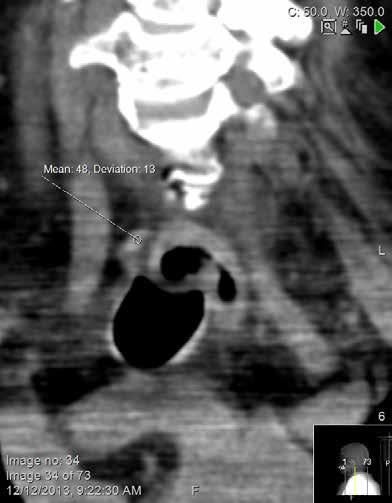
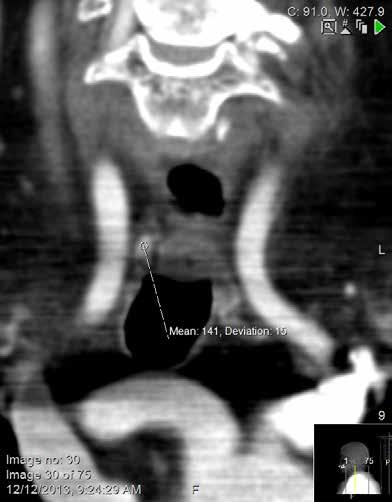

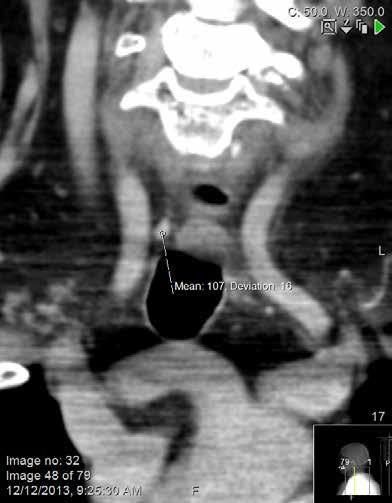
23

24 Axial CT images in noncontrast (A) early post-contrast (B) and delayed post-contrast (C) phases demonstrate an intrathyroidal lesion with subtle hypodensity on precontrast imaging and delayed enhancement. This enhancement pattern is seen less commonly than early enhancement and washout.

25 Polar Vessel Sign Bahl M et al. Prevalence of polar vessel sign in parathyroid adenomas on the arterial phase of 4DCT. AJNR. 2014;35:
26 Parathyroid Venous Sampling Introduced in 1970 as outpatient procedure Typically performed after other image localization studies have failed Proceed to surgery if 2 noninvasive studies (US, CT, MRI, MIBI) identify abnormal parathyroid gland If equivocal, perform digital arteriography or venous sampling with rapid PTH Savader SJ et al. Venous interventional radiology with clinical perspectives. 2 nd Ed Thieme. Sensitivity 80-90% in experienced hands Combined with rapid PTH assay 100% cure rate when venous gradient demonstrated More significant contrast load and radiation exposure Invasive
 when > 50% gradient (2:1) between PTH concentration at specific sites compared to peripheral blood")
27 Access femoral vein with Seldinger technique, then fluoroscopically- guided to veins with contrast injected to document catheter position with permanently-recorded image at each site; small amount venous blood collected at each site from multiple veins (+) when > 50% gradient (2:1) between PTH concentration at specific sites compared to peripheral blood samples


28 L

29 Adenoma appears as rounded, densely staining blush Bakal CW, Silberzweig JE et al. Vascular and Interventional Radiology Principles and Practice Thieme.
30 Scintigraphy C-11 methionine (MET-PET) Meta-analysis: 9 studies with 258 patients Sensitivity - 81% Detection Rate - 70% Not recommended as first line Caldarella et al. Diagnostic performance of positron emission tomography using C-11-methionine in patients with suspected parathyroid adenoma: a meta-analysis.
31 Scintigraphy FDG-PET vs DPMIBI SPECT FDG-PET (N=21): Sensitivity - 86% Specificity - 78% Able to detect smaller adenomas More FPs Higher cost Neumann et al. J Nucl Med 1996;37(11):

32 Scintigraphy Parathyroid Surgery Fundamental and Advanced Concepts. Plural Publishing
33 Scintigraphy Noninvasive localization of PA (& minimally invasive surgery) - Reduces operating time - Limited neck dissection - Shorter hospital stay - Reduce reoperation incidence
34 Some Radiotracers/Methods Used: -Can be combined for Dual-Isotope Subtraction Scan -Or single radiotracer for Single-Isotope Dual-Phase Scan Tc-99m-sestamibi (MIBI) gold standard today; thyroid & parathyroid uptake; look at washout pattern; 140 kev, T1/2 = 6 hours Tc-99m-tetrofosmin thyroid & parathyroid; slower washout from thyroid than MIBI; 140 kev, T½ = 6 hrs Thallium-201 thyroid & parathyroid uptake; kev, T½ = 73 hrs In-111-pentetrotide (Octreoscan) - some parathyroid glands have somatostatin receptors; 173 & 247 kev, T½ = 67 hrs I-123 thyroid uptake only; 159 kev, T1/2 = 13 hrs Tc-99m pertechnetate thyroid uptake only; 140 kev, T1/2 = 6 hrs


35 Example of Dual-Isotope Subtraction Scan: 99m Tc-sestamibi/ 123 I - MIBI uptake by thyroid & parathyroid I uptake by thyroid only - Administer MIBI, then I Final image = (I-123 MIBI)
36 Tc-99m sestamibi Coakley incidentally discovered uptake & retention in abnormal parathyroids while doing myocardial perfusion studies Coakley et al. Nucl Med Commun 1989;10:791-4 O'Doherty published 1st results of using a MIBI scan for preop localization of PA O Doherty et al. J Nucl Med 1992;33:313-8 Preferred parathyroid imaging agent worldwide T1/2 = 6 hours, 140 kev
37 Tc-99m sestamibi Uptake depends on: - **Number of MITOCHONDRIA** Hetrakul et al. Surgery 2001;130: Number of oxyphil cells (mitochondria-rich) - Active growth of gland - Elevated PTH - Blood flow - Gland size
38 Tc-99m sestamibi False Positives: - Thyroid adenomas - Cervical lymph nodes - Malignancy False Negatives: - Small adenomas - Displaced/obscured by goiter - Ectopic adenoma - Low mitochondrial activity
39 Tc-99m sestamibi Advantages over other radiotracers: - Higher sensitivity (70-100%)/specificity - Superior image quality - Single radiotracer

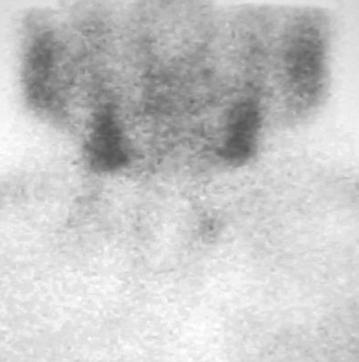
40 Tc-99m Sestamibi Dual-Phase Imaging Planar Imaging Early Delayed Uptake by thyroid & parathyroid Delayed imaging w/ greater washout from thyroid compared to parathyroid adenoma (persistent focal uptake on delayed images)
41 Single Isotope Dual-Phase SPECT Imaging Can do immediately after planar imaging Increases sensitivity (91 96%) Adds depth info and topographic correlation w/ anatomic structures Improves contrast Aids in evaluation of mediastinum for ectopic adenomas Helps guide surgeon


42 Tc-99m Sestamibi Dual-Phase SPECT Imaging Early Images Delayed Images

43 SPECT/CT From Terris Parathyroid Book Chapter SPECT/CT localized to left inferior-posterior parathyroid gland

44 SPECT/CT From Terris Parathyroid Book Chapter ectopic parathyroid adenoma

45 SPECT/CT From Terris Parathyroid Book Chapter right inferior parathyroid adenoma & lung cancer
46 Operative Procedures Bilateral Exploration Unilateral Exploration Radioguided Parathyroidectomy Minimally-Invasive Radioguided Parathyroidectomy (MIRP) Autologous Transplantation



47 Radioguided Parathyroidectomy Intraoperative gamma probe localization Courtesy, Brendan Stack, MD
48 Our Protocol Hyperparathyroidism Sestamibi Scan positive negative MIRP ultrasound positive negative unilateral exploration with turbo PTH bilateral exploration with turbo PTH Courtesy, Brendan Stack, MD
49 MIRP Advantages: Local anesthesia (not general) Dissection minimal Outpatient procedure Less post-op pain Frozen section pathology Perioperative calcium supplementation Eliminates post-op blood tests Costello D, Norman J. Surg Oncol Clin No Amer. 1999; 3:555-64
 Venous blood (usually anterior jugular) sample before gland removal & 10 min after excision > 50% decline in PTH @ 10")
 Immulite Elecsys 1010 Adenoma ex-vivo counting rate of at least > 20% higher than thyroid background Richards ML, Thompson GB, Farley DR")
50 Intraoperative PTH Eliminates need for intraoperative frozen-section analysis Measure PTH drop during safety window (time between adenoma excision & when other glands start producing PTH) Venous blood (usually anterior jugular) sample before gland removal & 10 min after excision > 50% decline in 10 minutes from baseline indicates successful removal of adenoma (relying on drop only has 22.4% failure rate) Immulite Elecsys 1010 Adenoma ex-vivo counting rate of at least > 20% higher than thyroid background Richards ML, Thompson GB, Farley DR et al. Arch Surg. 2011; 146: Murphy et al. Surgery 1999;126:1023-9



51
52 MIRP Case Example African American female with an incidental finding of hypercalcemia Co-morbidities of hypertension and diabetes No history of stones, neuromusc. SXs, or GI complaints Post-menopausal Courtesy, Brendan Stack, MD


53 MIRP Gamma probe guided external marking


54 MIRP Minimal access incision

55 MIRP Pre-op Post-op
56 Cost/Benefit Analysis Use of any localization technique: - Reduces the risk of RLN injury by 37% to 52% - Produces a cost-benefit when compared w/ nondirected BNE Preop MIBI scanning afforded a > $3000 reduction in charges when compared w/ nondirected BNE Approximately equivalent savings were found if preop MIBI scanning was combined with ipth Fahey et al. Arch Surg 2002;137:917-23
57 Costs based on 2011 Medicare reimbursement schedules: US + 4DCT least expensive strategy ($5,901) US alone ($6,028) or 4DCT alone ($6,110) - 2 nd least expensive US + MIBI ($6,329) 4-gland, bilateral neck exploration (BNE) most expensive strategy ($6,824) Lubitz CC et al. Preoperative localization strategies for primary hyperparathyroidism: an economic analysis. 2012;19:4202-9
58 Radiation Radiation Dose Comparison of Parathyroid Planar Scintigraphy, Combined SPECT/CT, and Multiphase 4DCT Bartel TB 1, Stack, Jr, BC 2, Yarbrough TL 3, Medarametla S 1, Samant R 1, Fitzgerald RT 1 Objective: Compare radiation doses for planar scintigraphy, SPECT/CT, & 4DCT in cases of difficult-to-detect parathyroid adenomas in pts with primary hyperparathyroidism Methods: 4DCT performed in 5 pts where no lesion was detected by P or S/CT. Dual-phase planar and SPECT/CT (15 min,2 hr) also performed prior to but no PA detected. Radiation doses were calculated using Stanford s RADAR (P, S/CT) and BCM s effective dose calculator (4DCT) which utilizes DLP (dose-length product) info.
59 Results: Planar or SPECT/CT gives lowest radiation dose. Optimized 4DCT alone similar if utilized as initial study. Combined radiation dose is nearly doubled or tripled for P+S/CT+4DCT, and multiple localization studies in difficult cases even further increases total dose. Prior to 4DCT, Pt 1 had 3 nonlocalizing scintigraphic studies giving a total radiation dose of 35.7 msv. Pt 5 had 3 nonlocalizing scintigraphic studies and 1 CT-neck prior to 4DCT with a total dose of 52.4 msv. All pts were successfully localized and treated surgically. We are further optimizing our 4DCT protocol. Conclusions: For PA localization, P alone provides the lowest dose. Nonlocalized lesions may require S/CT and/or 4DCT. Given the implications of localization for surgical morbidity, the benefit of additional exams likely outweighs the added radiation dose. Acknowledgement: Martin A. Lodge, PhD, Johns Hopkins Medicine, Dept of Radiology.
60 Hyperparathyroidism Sestamibi Scan positive negative MIRP ultrasound positive unilateral exploration with turbo PTH negative 4DCT??? bilateral exploration with turbo PTH Courtesy, Brendan Stack, MD
61 SUMMARY Pre-op PA image localization is beneficial to the patient MIBI Scintigraphy considered standard for this SPECT/CT esp. useful for difficult cases 4DCT may prove useful for last resort, costeffective, & if optimized to similar radiation dose This is a team effort!

62 Thank You!! Iws.collin.edu/mweis
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE
 HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
Parathyroid Imaging: Current Concepts. Maria Gule-Monroe, M.D. Nancy Perrier, M.D.
 Parathyroid Imaging: Current Concepts Maria Gule-Monroe, M.D. Nancy Perrier, M.D. Disclosures None Objectives Ultrasound characteristics of parathyroid adenomas vs. lymph nodes 4D-CT evaluation of hyperparathyroidism
Parathyroid Imaging: Current Concepts Maria Gule-Monroe, M.D. Nancy Perrier, M.D. Disclosures None Objectives Ultrasound characteristics of parathyroid adenomas vs. lymph nodes 4D-CT evaluation of hyperparathyroidism
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones
 Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Parathyroid Imaging. A Guide to Parathyroid Surgery
 Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
PARATHYROID NUCLEAR MEDICINE IMAGING REVIEW DISCLOSURES
 PARATHYROID NUCLEAR MEDICINE IMAGING REVIEW Miguel Hernandez Pampaloni, M.D., Ph.D. Chief, Nuclear Medicine Assistant Professor of Radiology UCSF Department of Radiology and Biomedical Imaging DISCLOSURES
PARATHYROID NUCLEAR MEDICINE IMAGING REVIEW Miguel Hernandez Pampaloni, M.D., Ph.D. Chief, Nuclear Medicine Assistant Professor of Radiology UCSF Department of Radiology and Biomedical Imaging DISCLOSURES
PARATHYROID IMAGING. James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center
 PARATHYROID IMAGING James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center NO DISCLOSURES Overview The hallmarks of the ideal test Benefits
PARATHYROID IMAGING James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center NO DISCLOSURES Overview The hallmarks of the ideal test Benefits
Outline. Parathyroid Localization Studies. Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center
 Parathyroid Localization Studies Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center Outline Clinical Context of Primary Hyperparathyroidism Ultrasound, Sestamibi, and Other
Parathyroid Localization Studies Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center Outline Clinical Context of Primary Hyperparathyroidism Ultrasound, Sestamibi, and Other
Outline. Primary Hyperparathyriodism. SPECT/CT in Parathyroid Localisation. Ann-Marie Quigley Nuclear Medicine Royal Free Hospital London
 SPECT/CT in Parathyroid Localisation Ann-Marie Quigley Nuclear Medicine Royal Free Hospital London Outline Pathophysiology Current guidelines SPECT/CT the evidence SPECT/CT in clinical scenarios MGD, Nodular
SPECT/CT in Parathyroid Localisation Ann-Marie Quigley Nuclear Medicine Royal Free Hospital London Outline Pathophysiology Current guidelines SPECT/CT the evidence SPECT/CT in clinical scenarios MGD, Nodular
Outline. SPECT/CT in Parathyroid Disease. Pathophysiology. Current guidelines. SPECT/CT the evidence. SPECT/CT in clinical scenarios
 SPECT/CT in Parathyroid Disease Ann-Marie Quigley Nuclear Medicine Royal Free Hospital London Outline Pathophysiology Current guidelines SPECT/CT the evidence SPECT/CT in clinical scenarios MGD, Nodular
SPECT/CT in Parathyroid Disease Ann-Marie Quigley Nuclear Medicine Royal Free Hospital London Outline Pathophysiology Current guidelines SPECT/CT the evidence SPECT/CT in clinical scenarios MGD, Nodular
Case 4: 27 yr-old woman with history of kidney stones and hyperparathyroidism.
 Case 4: 27 yr-old woman with history of kidney stones and hyperparathyroidism. Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Hyperparathyroidism
Case 4: 27 yr-old woman with history of kidney stones and hyperparathyroidism. Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Hyperparathyroidism
Minimally invasive parathyroidectomy
 Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
THE PARATHYROID GLAND THEORY AND NUCLEAR MEDICINE PRACTICE
 THE PARATHYROID GLAND THEORY AND NUCLEAR MEDICINE PRACTICE George N. Sfakianakis MD Professor of Radiology and Pediatrics Director, Division of Nuclear Medicine UM/JMMC Miami FL October 2009 ENDONCRINE
THE PARATHYROID GLAND THEORY AND NUCLEAR MEDICINE PRACTICE George N. Sfakianakis MD Professor of Radiology and Pediatrics Director, Division of Nuclear Medicine UM/JMMC Miami FL October 2009 ENDONCRINE
HPI joint pain/arthritis serum calcium 11.5 PTH 147pg/ml
 HPI 45 yo female Increased calcium level during evaluation for joint pain/arthritis W/U showed serum calcium 11.5 and PTH 147pg/ml (Normal 11-67pg/ml) Otherwise asymptomatic PMH/PSH Arthritis Tonsillectomy
HPI 45 yo female Increased calcium level during evaluation for joint pain/arthritis W/U showed serum calcium 11.5 and PTH 147pg/ml (Normal 11-67pg/ml) Otherwise asymptomatic PMH/PSH Arthritis Tonsillectomy
Parathyroid Imaging What is best
 Parathyroid Imaging What is best Mike Avison Bradford Why me? I m honoured to be asked to present this. There is no killer paper or text which clearly proves the best methodology. Bradford has performed
Parathyroid Imaging What is best Mike Avison Bradford Why me? I m honoured to be asked to present this. There is no killer paper or text which clearly proves the best methodology. Bradford has performed
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
Parathyroid Glands: location, condition and value of imaging tests.
 Parathyroid Glands: location, condition and value of imaging tests. Poster No.: C-2283 Congress: ECR 2015 Type: Educational Exhibit Authors: E. Elías Cabot, P. Segui, G. D. Tobar Murgueitio; Cordoba/ES
Parathyroid Glands: location, condition and value of imaging tests. Poster No.: C-2283 Congress: ECR 2015 Type: Educational Exhibit Authors: E. Elías Cabot, P. Segui, G. D. Tobar Murgueitio; Cordoba/ES
Marcin Barczynski, 1 Aleksander Konturek, 2 Alicja Hubalewska-Dydejczyk, 2. Filip Gołkowski, 1 Stanislaw Cichon, 1 Piotr Richter, 1 Wojciech Nowak
 3 rd Chair and Department of General Surgery 1 and Chair and Department of Endocrinology 2 Jagiellonian University, Medical College Head: Prof. Wojciech Nowak, MD, PhD INTRAOPERATIVE BILATERAL INTERNAL
3 rd Chair and Department of General Surgery 1 and Chair and Department of Endocrinology 2 Jagiellonian University, Medical College Head: Prof. Wojciech Nowak, MD, PhD INTRAOPERATIVE BILATERAL INTERNAL
Nuclear Medicine Head and Neck Region. Bán Zsuzsanna, MD University of Pécs, Department of Nuclear Medicine
 Nuclear Medicine Head and Neck Region Bán Zsuzsanna, MD University of Pécs, Department of Nuclear Medicine Thyroid scintigraphy Parathyroid scintigraphy F18-FDG PET examinations in head and neck cancer
Nuclear Medicine Head and Neck Region Bán Zsuzsanna, MD University of Pécs, Department of Nuclear Medicine Thyroid scintigraphy Parathyroid scintigraphy F18-FDG PET examinations in head and neck cancer
The parathyroid glands participate in the regulation
 41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
This PDF is available for free download from a site hosted by Medknow Publications
 Original Article Role of radionuclide scintigraphy in the detection of parathyroid adenoma Singh N, Krishna BA Department of Nuclear Medicine, P. D. Hinduja National Hospital and MRC, Mumbai, India Correspondence
Original Article Role of radionuclide scintigraphy in the detection of parathyroid adenoma Singh N, Krishna BA Department of Nuclear Medicine, P. D. Hinduja National Hospital and MRC, Mumbai, India Correspondence
Potential conflicts of interest: None
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
RADIOGUIDED PARATHYROIDECTOMY IS SUCCESSFUL IN 98.7% OF SELECTED PATIENTS
 Original Article RADIOGUIDED PARATHYROIDECTOMY IS SUCCESSFUL IN 98.7% OF SELECTED PATIENTS Charles D. Livingston, MD, FACS ABSTRACT Objective: To examine an individualized approach to patients with primary
Original Article RADIOGUIDED PARATHYROIDECTOMY IS SUCCESSFUL IN 98.7% OF SELECTED PATIENTS Charles D. Livingston, MD, FACS ABSTRACT Objective: To examine an individualized approach to patients with primary
Complementary sestamibi scintigraphy and ultrasound for primary hyperparathyroidism
 Nuclear Medicine and Biomedical Imaging Research Article Complementary sestamibi scintigraphy and ultrasound for primary hyperparathyroidism Yang Z 1,3 *, Li AY 2, Alexander G 3 and Chadha M 3 1 Department
Nuclear Medicine and Biomedical Imaging Research Article Complementary sestamibi scintigraphy and ultrasound for primary hyperparathyroidism Yang Z 1,3 *, Li AY 2, Alexander G 3 and Chadha M 3 1 Department
Diagnosis and Treatment of Primary Hyperparathyroidism. Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic
 Diagnosis and Treatment of Primary Hyperparathyroidism Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Disclosure Nothing to Disclose Primary HPT Autonomous secretion of
Diagnosis and Treatment of Primary Hyperparathyroidism Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Disclosure Nothing to Disclose Primary HPT Autonomous secretion of
Primary hyperparathyroidism (HPT) has an incidence of
 has an incidence of") Dual-Phase Tc-Sestamibi Imaging: Its Utility in Parathyroid Hyperplasia and Use of Immediate/ Delayed Image Ratios to Improve Diagnosis of Hyperparathyroidism Leonie Gordon, MD; William Burkhalter, MD;
Dual-Phase Tc-Sestamibi Imaging: Its Utility in Parathyroid Hyperplasia and Use of Immediate/ Delayed Image Ratios to Improve Diagnosis of Hyperparathyroidism Leonie Gordon, MD; William Burkhalter, MD;
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
PTH > 60pg/ml PRIMARY HYPERPARATHYROIDISM. Introduction Biochemical Diagnosis. Normal Parathyroid. Parathyroid Glands
 next speaker: Declan Neeson Belfast/UK SPECT/CT scanning and parathyroid surgery in Southern Trust, N. Ireland D Neeson M Korda, G Gray, C Leonard, M Fawzy, R Lambon Parathyroid Glands PRIMARY HYPERPARATHYROIDISM
next speaker: Declan Neeson Belfast/UK SPECT/CT scanning and parathyroid surgery in Southern Trust, N. Ireland D Neeson M Korda, G Gray, C Leonard, M Fawzy, R Lambon Parathyroid Glands PRIMARY HYPERPARATHYROIDISM
SPECT/CT in Endocrine Diseases and Dosimetry
 SPECT/CT in Endocrine Diseases and Dosimetry Heather A. Jacene, MD Division of Nuclear Medicine Russell H. Morgan Dept. of Radiology and Radiological Science Johns Hopkins University Baltimore, MD Disclosures
SPECT/CT in Endocrine Diseases and Dosimetry Heather A. Jacene, MD Division of Nuclear Medicine Russell H. Morgan Dept. of Radiology and Radiological Science Johns Hopkins University Baltimore, MD Disclosures
Preoperative Tc-99m-sestamibi (MIBI) scintigraphy and
 scintigraphy and") Otolaryngology Head and Neck Surgery (2006) 134, 316-320 ORIGINAL RESEARCH In Vivo Characterisation of Parathyroid Lesions by Use of Gamma Probe: Comparison With Ex Vivo Count Method and Frozen Section
Otolaryngology Head and Neck Surgery (2006) 134, 316-320 ORIGINAL RESEARCH In Vivo Characterisation of Parathyroid Lesions by Use of Gamma Probe: Comparison With Ex Vivo Count Method and Frozen Section
Surgical anatomy of thyroid and parathyroid glands
 Head & Neck Surgery Course Surgical anatomy of thyroid and parathyroid glands Dr Pierfrancesco PELLICCIA Pr Benjamin LALLEMANT Service ORL et CMF CHU de Nîmes CH de Arles Thyroid glands Dr Pierfrancesco
Head & Neck Surgery Course Surgical anatomy of thyroid and parathyroid glands Dr Pierfrancesco PELLICCIA Pr Benjamin LALLEMANT Service ORL et CMF CHU de Nîmes CH de Arles Thyroid glands Dr Pierfrancesco
4/20/2015. The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy. Learning Objectives
 Testing During Surgical Parathyroidectomy. Learning Objectives") The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Use of PTH at Point of Surgery for Non-Localized Cases of Hyperparathyoidism
 Use of PTH at Point of Surgery for Non-Localized Cases of Hyperparathyoidism Keck Hospital of USC Private, non-profit 400 bed hospital Teaching and research, USC Keck School of Medicine Approx. 40 parathyroid
Use of PTH at Point of Surgery for Non-Localized Cases of Hyperparathyoidism Keck Hospital of USC Private, non-profit 400 bed hospital Teaching and research, USC Keck School of Medicine Approx. 40 parathyroid
Multimodality imaging of the parathyroid adenoma
 Multimodality imaging of the parathyroid adenoma Poster No.: C-0256 Congress: ECR 2015 Type: Educational Exhibit Authors: S. Liddy, J. Feeney; Dublin/IE Keywords: Head and neck, Nuclear medicine, Thyroid
Multimodality imaging of the parathyroid adenoma Poster No.: C-0256 Congress: ECR 2015 Type: Educational Exhibit Authors: S. Liddy, J. Feeney; Dublin/IE Keywords: Head and neck, Nuclear medicine, Thyroid
ORIGINAL ARTICLE. Appearance of Ectopic Undescended Inferior Parathyroid Adenomas on Technetium Tc 99m Sestamibi Scintigraphy
 ORIGINAL ARTICLE Appearance of Ectopic Undescended Inferior Parathyroid Adenomas on Technetium Tc 99m Sestamibi Scintigraphy A Lesson From Reoperative Parathyroidectomy David Axelrod, MD; James C. Sisson,
ORIGINAL ARTICLE Appearance of Ectopic Undescended Inferior Parathyroid Adenomas on Technetium Tc 99m Sestamibi Scintigraphy A Lesson From Reoperative Parathyroidectomy David Axelrod, MD; James C. Sisson,
Southern Derbyshire Shared Care Pathology Guidelines. Primary Hyperparathyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
O~iginalArtrc!~'" MINIMALLY INVASIVE RADIO-GUIDED PARATHYROIDECTOMY IN 152 CONSECUTIVE PATIENTS WITH PRIMARY HYPERPARATHYROIDISM
 O~iginalArtrc!~'",,_.~.~_.,_,,~_......_. ~.o:-'';:...:/-.~. ~'.:::.., MINIMALLY INVASIVE RADIO-GUIDED PARATHYROIDECTOMY IN 152 CONSECUTIVE PATIENTS WITH PRIMARY HYPERPARATHYROIDISM Douglas Politz, MD,
O~iginalArtrc!~'",,_.~.~_.,_,,~_......_. ~.o:-'';:...:/-.~. ~'.:::.., MINIMALLY INVASIVE RADIO-GUIDED PARATHYROIDECTOMY IN 152 CONSECUTIVE PATIENTS WITH PRIMARY HYPERPARATHYROIDISM Douglas Politz, MD,
The mystery of the hidden parathyroid adenoma. Case #1. Imaging. Case of missed adenoma. Ultrasound false nega9ves. Case of missed adenoma 5/16/16
 The mystery of the hidden parathyroid adenoma AACE Annual Mee+ng 2016 Orlando, FL Case #1 Moderator: Panel: Jennifer L Mar+ MD FACS Endocrine Surgery NYC Azeez Farooki MD Endocrinology MSKCC Peter Sadow
The mystery of the hidden parathyroid adenoma AACE Annual Mee+ng 2016 Orlando, FL Case #1 Moderator: Panel: Jennifer L Mar+ MD FACS Endocrine Surgery NYC Azeez Farooki MD Endocrinology MSKCC Peter Sadow
USEFULNESS OF INTRAOPERATIVE PARATHYROID HORMONE MONITORING DURING MINIMALLY INVASIVE VIDEO-ASSISTED PARATHYROIDECTOMY
 USEFULNESS OF INTRAOPERATIVE PARATHYROID HORMONE MONITORING DURING MINIMALLY INVASIVE VIDEO-ASSISTED PARATHYROIDECTOMY Elisabetta Stenner elisabetta.stenner@asuits.sanita.fvg.it Introduction: primary hyperparathyroidism
USEFULNESS OF INTRAOPERATIVE PARATHYROID HORMONE MONITORING DURING MINIMALLY INVASIVE VIDEO-ASSISTED PARATHYROIDECTOMY Elisabetta Stenner elisabetta.stenner@asuits.sanita.fvg.it Introduction: primary hyperparathyroidism
Hypercalcemia & Parathyroid Disorders. W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology
 Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand
 International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
DR. DARWISH H. BADRAN. Parathyroid glands
 Parathyroid glands History 1849 - Sir Richard owen provided 1st accurate description of normal parathyroid glands after examining Indian Rhinoceros 1879 - Anton Wölfer described tetany in a patient
Parathyroid glands History 1849 - Sir Richard owen provided 1st accurate description of normal parathyroid glands after examining Indian Rhinoceros 1879 - Anton Wölfer described tetany in a patient
PRIMARY HYPERPARATHYROIDISM PRIMARY HYPERPARATHYROIDISM. Hyperparathyroidism Etiology. Common Complex Insidious Chronic Global Only cure is surgery
 ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
Clinical Approach to Hypercalcemia For the Primary Care Provider
 Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Re-explorative Parathyroid Surgery for Persistent and Recurrent Primary Hyperparathyroidism
 10.5005/jp-journals-10002-1070 ORIGINAL ARTICLE WJOES Re-explorative Parathyroid Surgery for Persistent and Recurrent Primary Hyperparathyroidism Rachel L O Connell, Karolina Afors, Martin H Thomas Ashford
10.5005/jp-journals-10002-1070 ORIGINAL ARTICLE WJOES Re-explorative Parathyroid Surgery for Persistent and Recurrent Primary Hyperparathyroidism Rachel L O Connell, Karolina Afors, Martin H Thomas Ashford
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes
 Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes Allan Siperstein MD The Cleveland Clinic Audience Quiz Taken ultrasound course Perform
Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes Allan Siperstein MD The Cleveland Clinic Audience Quiz Taken ultrasound course Perform
Hyperparathyroidism. When to Suspect, How to Diagnose, When and How to Intervene. Johanna A. Pallotta, MD, FACP, FACE
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
The Concept of GOSTT
 IAEA Regional Training Course on Sentinel Lymph Node Mapping and Radioguided Surgery The Concept of GOSTT Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa,
IAEA Regional Training Course on Sentinel Lymph Node Mapping and Radioguided Surgery The Concept of GOSTT Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa,
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
INDEX. Note: Page numbers of issue and article titles are in boldface type. cell carcinoma. ENDOCRINE SURGERY
 ENDOCRINE SURGERY INDEX Note: Page numbers of issue and article titles are in boldface type. Adenylate cyclase, in signal transduction 425-426 Adrenal incidentalomas, 499-509 imaging of, 502-504 in patients
ENDOCRINE SURGERY INDEX Note: Page numbers of issue and article titles are in boldface type. Adenylate cyclase, in signal transduction 425-426 Adrenal incidentalomas, 499-509 imaging of, 502-504 in patients
Primary Hyperparathyroidism
 November 2002 Primary Hyperparathyroidism Lori Coburn, Harvard Medical School Year III Hyperparathyroidism An increase in parathyroid hormone (PTH) production Divided into Primary, Secondary and Tertiary
November 2002 Primary Hyperparathyroidism Lori Coburn, Harvard Medical School Year III Hyperparathyroidism An increase in parathyroid hormone (PTH) production Divided into Primary, Secondary and Tertiary
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
PRIMARY HYPERPARATHYROIDISM
 PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
SPECT/CT Fusion in the Diagnosis of Hyperparathyroidism
 SPECT/CT Fusion in the Diagnosis of Hyperparathyroidism Yoshio Monzen, Akihisa Tamura, Hajime Okazaki, Taichi Kurose, Masayuki Kobayashi, Masatsugu Kuraoka Department of Radiology, Hiroshima Prefectural
SPECT/CT Fusion in the Diagnosis of Hyperparathyroidism Yoshio Monzen, Akihisa Tamura, Hajime Okazaki, Taichi Kurose, Masayuki Kobayashi, Masatsugu Kuraoka Department of Radiology, Hiroshima Prefectural
Comparison Of Sestamibi Scintigraphy And Ultrasonography In Preoperative Localization Of Primary Hyperparathyroidism
 ISPUB.COM The Internet Journal of Surgery Volume 16 Number 1 Comparison Of Sestamibi Scintigraphy And Ultrasonography In Preoperative Localization Of Primary S Nasiri, A Sorush, A Hashemi, F Mehrkhani,
ISPUB.COM The Internet Journal of Surgery Volume 16 Number 1 Comparison Of Sestamibi Scintigraphy And Ultrasonography In Preoperative Localization Of Primary S Nasiri, A Sorush, A Hashemi, F Mehrkhani,
IMPACT OF CONCOMITANT THYROID PATHOLOGY ON PREOPERATIVE WORKUP FOR PRIMARY HYPERPARATHYROIDISM
 January 28, 2009 EUROPEAN JOURNAL OF MEDICAL RESEARCH 37 Eur J Med Res (2009) 14: 37-41 I. Holzapfel Publishers 2009 IMPACT OF CONCOMITANT THYROID PATHOLOGY ON PREOPERATIVE WORKUP FOR PRIMARY HYPERPARATHYROIDISM
January 28, 2009 EUROPEAN JOURNAL OF MEDICAL RESEARCH 37 Eur J Med Res (2009) 14: 37-41 I. Holzapfel Publishers 2009 IMPACT OF CONCOMITANT THYROID PATHOLOGY ON PREOPERATIVE WORKUP FOR PRIMARY HYPERPARATHYROIDISM
Hyperparathyroidism may present as an incidental finding. Parathyroid Imaging: How Good Is It and How Should It Be Done?
 Parathyroid Imaging: How Good Is It and How Should It Be Done? Andrew G. Kettle, BA, and Mike J. O Doherty, MBBS, MSc, MD, FRCP Hypersecretion of parathormone in primary hyperparathyroidism is common,
Parathyroid Imaging: How Good Is It and How Should It Be Done? Andrew G. Kettle, BA, and Mike J. O Doherty, MBBS, MSc, MD, FRCP Hypersecretion of parathormone in primary hyperparathyroidism is common,
Minimally invasive parathyroid surgery
 Review Article Minimally invasive parathyroid surgery Salem I. Noureldine, Zhen Gooi, Ralph P. Tufano Division of Head and Neck Endocrine Surgery, Department of Otolaryngology, Head and Neck Surgery, Johns
Review Article Minimally invasive parathyroid surgery Salem I. Noureldine, Zhen Gooi, Ralph P. Tufano Division of Head and Neck Endocrine Surgery, Department of Otolaryngology, Head and Neck Surgery, Johns
Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Medical Expert
 Medical Expert") Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Introduction Medical Expert This is a three month PGY 1-5 rotation in which residents gain exposure in the care and management of patients
Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Introduction Medical Expert This is a three month PGY 1-5 rotation in which residents gain exposure in the care and management of patients
Primary hyperparathyroidism is usually a clinical and
 Journal of Nuclear Medicine, published on November 7, 2008 as doi:10.2967/jnumed.108.054858 Preoperative 123 I/ 99m Tc-Sestamibi Subtraction SPECT and SPECT/CT in Primary Hyperparathyroidism Donald R.
Journal of Nuclear Medicine, published on November 7, 2008 as doi:10.2967/jnumed.108.054858 Preoperative 123 I/ 99m Tc-Sestamibi Subtraction SPECT and SPECT/CT in Primary Hyperparathyroidism Donald R.
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
Case study Group 2 presentation
 Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
Hybrid Imaging SPECT/CT PET/CT PET/MRI. SNMMI Southwest Chapter Aaron C. Jessop, MD
 Hybrid Imaging SPECT/CT PET/CT PET/MRI SNMMI Southwest Chapter 2014 Aaron C. Jessop, MD Assistant Professor, Department of Nuclear Medicine UT MD Anderson Cancer Center, Houston, Texas Complimentary role
Hybrid Imaging SPECT/CT PET/CT PET/MRI SNMMI Southwest Chapter 2014 Aaron C. Jessop, MD Assistant Professor, Department of Nuclear Medicine UT MD Anderson Cancer Center, Houston, Texas Complimentary role
Parathyroid surgery at Massachusetts General Hospital: Information for patients and families
 Parathyroid surgery at Massachusetts General Hospital: Information for patients and families We are pleased that you have chosen Massachusetts General Hospital to receive treatment for your parathyroid
Parathyroid surgery at Massachusetts General Hospital: Information for patients and families We are pleased that you have chosen Massachusetts General Hospital to receive treatment for your parathyroid
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS. Dr. Pamela Hanson DO PGY3
 PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
11/1/2014. Radiologic incidentalomas Ordering pitfalls Newer technology and applications
 Bilal Tahir, MD Gitasree Borthakur, MD Indiana University School of Medicine Department of Radiology & Imaging Sciences October 31, 2014 ACP 2014 Dr. V. Aaron Nuclear (vaaron@iupui.edu) Dr. S. Westphal
Bilal Tahir, MD Gitasree Borthakur, MD Indiana University School of Medicine Department of Radiology & Imaging Sciences October 31, 2014 ACP 2014 Dr. V. Aaron Nuclear (vaaron@iupui.edu) Dr. S. Westphal
Endocrine Surgery When to Refer and What We Do
 Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
PAPER. The Effectiveness of Radioguided Parathyroidectomy in Patients With Negative Technetium Tc 99m Sestamibi Scans
 PAPER The Effectiveness of Radioguided Parathyroidectomy in Patients With Negative Technetium Tc 99m Sestamibi Scans Herbert Chen, MD; Rebecca S. Sippel, MD; Sarah Schaefer, NP Background: Many surgeons
PAPER The Effectiveness of Radioguided Parathyroidectomy in Patients With Negative Technetium Tc 99m Sestamibi Scans Herbert Chen, MD; Rebecca S. Sippel, MD; Sarah Schaefer, NP Background: Many surgeons
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ENDOCRINE 5-May-2013 DEVELOPED BY: Jonathan Serpell
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ENDOCRINE 5-May-2013 DEVELOPED BY: Jonathan Serpell
Thyroid and Parathyroid Ultrasound Protocol
 Thyroid and Parathyroid Ultrasound Protocol Reviewed By: Anna Ellermeier, MD Last Reviewed: December 2017 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
Thyroid and Parathyroid Ultrasound Protocol Reviewed By: Anna Ellermeier, MD Last Reviewed: December 2017 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
Thallium 201 scanning can diagnose multiple recurrences in forearm implanted parathyroid tissue post total parathyroidectomy:
 CASE REPORT Thallium 201 scanning can diagnose multiple recurrences in forearm implanted parathyroid tissue post total parathyroidectomy: Salman AK., Wagieh S.,Munshy AT. and Al Ghamdy H.* King Abdulla
CASE REPORT Thallium 201 scanning can diagnose multiple recurrences in forearm implanted parathyroid tissue post total parathyroidectomy: Salman AK., Wagieh S.,Munshy AT. and Al Ghamdy H.* King Abdulla
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Preoperative Evaluation
 Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
General Nuclear Medicine
 General Nuclear Medicine What is General Nuclear Medicine? What are some common uses of the procedure? How should I prepare? What does the equipment look like? How does the procedure work? How is the procedure
General Nuclear Medicine What is General Nuclear Medicine? What are some common uses of the procedure? How should I prepare? What does the equipment look like? How does the procedure work? How is the procedure
Parathyroidectomy. Surgery for Parathyroid Problems
 Parathyroidectomy Surgery for Parathyroid Problems Why You Need Parathyroid Surgery Has your doctor just recommended that you have parathyroid surgery? If so, you likely have many questions. What are the
Parathyroidectomy Surgery for Parathyroid Problems Why You Need Parathyroid Surgery Has your doctor just recommended that you have parathyroid surgery? If so, you likely have many questions. What are the
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Head and Neck Endocrine Surgery
 Objectives Endocrine Physiology Risk factors for hypocalcemia Management strategies Passive vs. active Treatment of hypocalcemia Department of Head and Neck Management of Calcium in Thyroid and Parathyroid
Objectives Endocrine Physiology Risk factors for hypocalcemia Management strategies Passive vs. active Treatment of hypocalcemia Department of Head and Neck Management of Calcium in Thyroid and Parathyroid
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Ultrasound Evaluation of Hyperparathyroidism
 Ultrasound Evaluation of Hyperparathyroidism OBJECTIVES: 1. Why use US for localization? Advanced US course, Orlando, Florida September, 2018 2. Review the US findings and features of parathyroid adenomas
Ultrasound Evaluation of Hyperparathyroidism OBJECTIVES: 1. Why use US for localization? Advanced US course, Orlando, Florida September, 2018 2. Review the US findings and features of parathyroid adenomas
Dilemma in diagnosing thyroid adenoma A case report
 BRIEF REPORT Dilemma in diagnosing thyroid adenoma A case report Faria Nasreen, Shamsun Nahar Bailey National Institute of Nuclear Medicine & Allied Sciences, BAEC, Dhaka, Bangladesh Correspondence: Faria
BRIEF REPORT Dilemma in diagnosing thyroid adenoma A case report Faria Nasreen, Shamsun Nahar Bailey National Institute of Nuclear Medicine & Allied Sciences, BAEC, Dhaka, Bangladesh Correspondence: Faria
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
Association of Histological Findings with Tc-99m Sestamibi Parathyroid Imaging in Hyperfunctional Parathyroid Gland
 http://www.banglajol.info/index.php/jninb Original Article Journal of National Institute of Neurosciences Bangladesh, January 2016, Vol. 2, No. 1 oissn 2518-6612 pissn 2410-8030 Association of Histological
http://www.banglajol.info/index.php/jninb Original Article Journal of National Institute of Neurosciences Bangladesh, January 2016, Vol. 2, No. 1 oissn 2518-6612 pissn 2410-8030 Association of Histological
Clinical Medicine Insights: Endocrinology and Diabetes 2013:6
 Open Access: Full open access to this and thousands of other papers at http://www.la-press.com. Clinical Medicine Insights: Endocrinology and Diabetes Surgery for Primary Hyperparathyroidism in Patients
Open Access: Full open access to this and thousands of other papers at http://www.la-press.com. Clinical Medicine Insights: Endocrinology and Diabetes Surgery for Primary Hyperparathyroidism in Patients
Chapter 16 Worksheet Code It
 Name: Class: Date: ID: A Chapter 16 Worksheet 3 2 1 Code It True/False Indicate whether the statement is true or false. 1. CT scans generate three-dimensional images. 2. An ultrasound produces images of
Name: Class: Date: ID: A Chapter 16 Worksheet 3 2 1 Code It True/False Indicate whether the statement is true or false. 1. CT scans generate three-dimensional images. 2. An ultrasound produces images of
PRIMARY HYPERPARATHYROIDISM WITH RICKETS. KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College
 PRIMARY HYPERPARATHYROIDISM WITH RICKETS KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College Presenting Complaints v 17 year old developmentally normal adolescent boy, first of a twin pregnancy,
PRIMARY HYPERPARATHYROIDISM WITH RICKETS KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College Presenting Complaints v 17 year old developmentally normal adolescent boy, first of a twin pregnancy,
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease
 Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease Mira Milas MD, FACS Professor of Surgery Director of Endocrine Surgery No conflicts of interest or financial
Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease Mira Milas MD, FACS Professor of Surgery Director of Endocrine Surgery No conflicts of interest or financial
CURRENTLY THERE is considerable discussion about
 0013-7227/02/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 87(3):1024 1029 Printed in U.S.A. Copyright 2002 by The Endocrine Society Parathyroid Surgery: Separating Promise from Reality NANCY
0013-7227/02/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 87(3):1024 1029 Printed in U.S.A. Copyright 2002 by The Endocrine Society Parathyroid Surgery: Separating Promise from Reality NANCY
SPECT- CT and PET- CT in Endocrine tumours. Prof John Buscombe
 SPECT- CT and PET- CT in Endocrine tumours Prof John Buscombe Introduc:on Parathyroid adenoma Hyperinsulinoma Adrenal imaging Pituitary imaging Parathyroid Tumours Can be seen in MEN1 Nuclear Medicine
SPECT- CT and PET- CT in Endocrine tumours Prof John Buscombe Introduc:on Parathyroid adenoma Hyperinsulinoma Adrenal imaging Pituitary imaging Parathyroid Tumours Can be seen in MEN1 Nuclear Medicine
Endoscopic Parathyroidectomy: Why and When?
 World J Surg (2008) 32:2509 2515 DOI 10.1007/s00268-008-9709-3 Endoscopic Parathyroidectomy: Why and When? Jean-François Henry Æ Frédéric Sebag Æ Mariya Cherenko Æ Giuseppe Ippolito Æ David Taieb Æ Josiane
World J Surg (2008) 32:2509 2515 DOI 10.1007/s00268-008-9709-3 Endoscopic Parathyroidectomy: Why and When? Jean-François Henry Æ Frédéric Sebag Æ Mariya Cherenko Æ Giuseppe Ippolito Æ David Taieb Æ Josiane
Thyroid and Parathyroid Disease. RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010
 Thyroid and Parathyroid Disease RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010 Case Presentation # 1 CC: Neck Mass HPI: 51f found to have a neck mass on routine PE.
Thyroid and Parathyroid Disease RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010 Case Presentation # 1 CC: Neck Mass HPI: 51f found to have a neck mass on routine PE.
ORIGINAL ARTICLE. Early, Postinjection MIBI-SPECT as the Only Preoperative Localizing Study for Minimally Invasive Parathyroidectomy
 ORIGINAL ARTICLE Early, Postinjection MIBI-SPECT as the Only Preoperative Localizing Study for Minimally Invasive Parathyroidectomy Pinhas P. Schachter, MD; Nidal Issa, MD; Mordechai Shimonov, MD; Abraham
ORIGINAL ARTICLE Early, Postinjection MIBI-SPECT as the Only Preoperative Localizing Study for Minimally Invasive Parathyroidectomy Pinhas P. Schachter, MD; Nidal Issa, MD; Mordechai Shimonov, MD; Abraham
Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP
 Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP Endocrine in 25 Minutes Joshua S. Coren, D.O., MBA, FACOFP Vice Chair and Associate Professor, Family Medicine Rowan University School
Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP Endocrine in 25 Minutes Joshua S. Coren, D.O., MBA, FACOFP Vice Chair and Associate Professor, Family Medicine Rowan University School
THYROID NODULES: THE ROLE OF ULTRASOUND
 THYROID NODULES: THE ROLE OF ULTRASOUND NOVEMBER 2017 DR. DEAN DURANT DEFINITION Thyroid nodule: Focal area within the thyroid gland with echogenicity different from surrounding parenchyma. THYROID NODULES
THYROID NODULES: THE ROLE OF ULTRASOUND NOVEMBER 2017 DR. DEAN DURANT DEFINITION Thyroid nodule: Focal area within the thyroid gland with echogenicity different from surrounding parenchyma. THYROID NODULES
Role of imaging in RCC. Ultrasonography. Solid lesion. Cystic RCC. Solid RCC 31/08/60. From Diagnosis to Treatment: the Radiologist Perspective
 Role of imaging in RCC From Diagnosis to Treatment: the Radiologist Perspective Diagnosis Staging Follow up Imaging modalities Limitations and pitfalls Duangkamon Prapruttam, MD Department of Therapeutic
Role of imaging in RCC From Diagnosis to Treatment: the Radiologist Perspective Diagnosis Staging Follow up Imaging modalities Limitations and pitfalls Duangkamon Prapruttam, MD Department of Therapeutic