Endocrinology A Primer for Primary Care
|
|
|
- Penelope Harrington
- 6 years ago
- Views:
Transcription

1 Endocrinology A Primer for Primary Care KM Pantalone Staff Endocrinologist Director of Clinical Research Department of Endocrinology Cleveland Clinic
2 Objectives Review common endocrinology cases encountered by primary care Discuss appropriate treatment decisions To become comfortable managing primary care-related endocrine conditions
3 Common Endocrinology Cases in Primary Care Type 2 Diabetes Hypothyroidism Hypercalcemia Osteoporosis Male Hypogonadism
4 DM-2 Case 48-year-old Caucasian male with uncontrolled DM-2 BMI 36 Kidney function is normal Currently receiving metformin 1000 mg BID, and glipizide 10 mg once daily A1C 9.1% What is the most appropriate plan of care?
5 Options A) Increase glipizide to 10 mg BID B) Add a new therapy
6 DM-2 Case 1 Unlikely that increasing SFU will get A1C to goal, <7% It is even unlikely that adding an additional therapy, alone, will get the patient to goal A1C lowering of 0.7% at most, on average, can be expected when adding a 3 rd or 4 th agent to improve glycemia Choice of new therapy also matters
7 CCF Data (Submitted for Publication) Baseline/Initial A1C 9%
8 DM-2 Case #2 56-year-old African American female Weight 80 kg Kidney function good On Januvia 100 mg daily, metformin 1000 mg BID, and 50 units of insulin glargine A1C 7.8% What is the most appropriate next step?
9 DM-2 Case 2 A) Increase Lantus to 60 units B) Add an SGLT2 inhibitor C) Add glipizide D) A&C
10 Correct Answer: B Why? Basal insulin dose already > 0.5 units/kg Need to look at her BG log to see if increasing basal is really a good/safe idea Adding SFU would only lower fasting BG further, which is not what is driving the residual A1C elevation
11 BG Log (mg/dl) Day pre-breakfast pre-lunch pre-dinner bedtime The problem is post-prandial hyperglycemia, particularly after larger meals (dinner) Adding an agent that will help with post-prandial control -SGLT-2 inhibitor -Consider switching the DPP-4 inhibitor to a GLP-1 receptor agonist -A more potent incretin therapy Lower the dose of insulin glargine when start new medication Fasting BG is already at goal, and BG is dropping too much while sleeping. What happens if she doesn t eat much dinner and her BG is 130 mg/dl at bedtime?
12 Basal Insulin Generally, once a patient s dose of basal insulin exceeds 0.5 units/kg, you need to reassess the plan-of-care If BG is dropping more than mg/dl from HS to am, patient is at a high risk of hypoglycemia Studies evaluating higher basal insulin doses failed to show better glycemic control (A1C): 0.5 units/kg vs. 0.7 units/kg vs. 1 units/kg More weight gain and hypoglycemia

13

14 It is interesting that in many patients who fail metformin, who have an A1C < 8.5%, a SFU is added, despite the fact that it does NOT address the postprandial hyperglycemia, which is largely responsible for the residual A1C elevation!

15 Shifting down the plasma glucose, but wide glycemic excursions continue

16
17 Hypothyroidism Case: A 38-year-old Caucasian female BMI 32 Otherwise healthy Diagnosed with hypothyroidism a year ago Takes 112 mcg of LT4 TSH ( ) Free T4 1.2 ( ) Free T3 2.9 ( ) Energy is not good, + fatigue; wants to try Armour thyroid..
18 Primary Hypothyroidism-Common Causes Hashimoto s Disease Autoimmune Post-surgical Hypothyroidism Post-RAI treatment Graves Toxic MNG
19 Primary Hypothyroidism Diagnosis Elevated serum TSH in routine clinical practice Very few other disorders than can cause an elevated TSH Lab interference (HAMA) TSH secreting pituitary adenoma (rare) Recovery from Euthyroid Sick Syndrome Adrenal Insufficiency
20 Diagnosis, per the experts In most patients with symptoms or signs suggestive of hypothyroidism the serum TSH should be the initial test TSH, repeat the TSH with a serum free T4 to make the dx Repeat TSH and FT4 Consistent with primary hypothyroidism, replacement therapy with T4 should be initiated Repeat TSH but normal range FT4 May indicate subclinical hypothyroidism The decision about T4 replacement is made on a case by case basis and depends partly upon the degree of TSH elevation and symptoms reported by the patient
21 Diagnosis If TSH is within the normal reference range, but the patient has convincing symptoms of hypothyroidism Repeat serum TSH and obtain free T4 to assess for central hypothyroidism (hypothalamic/pituitary disorder) Do not always assume that because the TSH is normal they do not have a thyroid problem Rarely, central hypothyroidism can present with TSH values within the normal reference range, or even slightly elevated Key is that the TSH level is clearly inadequate for the level of free T4 Example: Free T4 0.4 ng/dl ( ), but TSH is 5.4 μiu/ml ( ) Almost always accompanied by other anterior pituitary abnormalities and symptoms
22 Some Patients have Persistent Symptoms Despite Adequate T4 Therapy Some patients have symptoms consistent with hypothyroidism despite adequate TSH and T4 levels Saravanan P. Clin Endocrinol 2002; 57: Walsh JP. Curr Opin Pharmacol 2002; 2: Wekking EM. Eur J Endocrinol 2005; 153:
23 Some Patients have Persistent Symptoms Despite Adequate T4 Therapy Some of these patients ask for addition of T3 to the treatment regimen Many of them have found claims of need for T3 on the internet Some have friends whose doctors claim that only combination therapy works
24 It Is Not Your Thyroid (usually)!!!
25 A significant number of these patients will have other conditions responsible for these residual symptoms Sleep disorders (Untreated OSA) Depression Medications causing fatigue Obesity Anemia Vitamin D deficiency Lack of EXERCISE!!!! Adrenal Insufficiency (rare) Note, I did not mention Adrenal Fatigue! Treatment of these may lead to clinical improvement
26 But, is there more to this story?
27 Abnormal Survey score How many with persistent symptoms? 50% Community based health questionnaire: 397 patients with normal TSH and T4 397 age and sex matched controls P=0.014 P< % 34% 36% Controls 25% 26% Patients 0% General Health Questionnaire Thyroid Health Questionnaire Saravanan P. Clin Endo. 2002:57:


28 T3 Therapy Needed Theory: Pilo A, Am J Physiol 1990; 258:E

29 No T3 Therapy Needed Theory: Pilo A, Am J Physiol 1990; 258:E
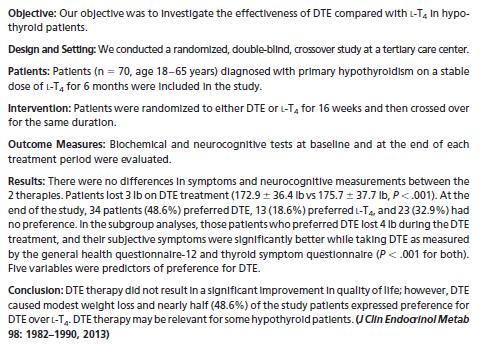
30 Early Randomized Controlled Trials of T4/T3 Combination Therapies Objective Subjectove T4/T3 Study Benefit Benefit Preference Bunevicious 1999 Yes Yes Yes Walsh 2003 No No No Sawka 2003 No No NA Clyde 2003 No No NA Siegmund 2004 No No NA Saravanan 2005 No No NA Escobar-Morreale 2005 No No Yes Apelhof 2005 No No Yes Rodriguez 2005 No No NA Levitt 2005 No No NA Regalbuto 2007 No No No Slawik 2007 (Central) No No NA Escobar-Morreale 2005 Review: Grozinsky-Glasberg 2006 Meta-Analysis: No benefit of T4/T3 No benefit of T4/T3

31
32 Follow-up Testing TSH is all that is required unless there is something that does not make sense In most circumstances, there is very little information gained from checking FT4 or FT3 once the patients have started thyroid hormone therapy Patients (and Dr. Google) will very frequently disagree Do NOT let them convince you to order a reverse T3!
33 Hypercalcemia 44-year-old Caucasian female, DM-1, well controlled, otherwise healthy
34 Typical Course We will continue to monitor your calcium It is not magically going to get better Need to be more aggressive, evaluate/manage Check PTH, her PTH was 85 pg/ml (15-65) while calcium was 10.8 mg/dl (8.6-10) Watch out for PTH values that remain in reference range in setting of hypercalcemia Inappropriately normal PTH levels when the calcium is elevated PTH normal range is only normal if calcium is normal Should be suppressed if calcium is elevated She has primary hyperparathyroidism
35 Primary Hyperparathyroidism Primary hyperparathyroidism can occur at any age, but the great majority of cases occur in patients over the age of 50 to 65 years Women are affected twice as often as men In one study, the incidence of hyperparathyroidism was highest among blacks, followed by whites, Asians, Hispanics, and others Griebeler ML et al. Bone 2015; 73:1. Yeh MW et al. JCEM 2013; 98:1122. Abood A, Vestergaard P. Dan Med J 2013; 60:A4567.

36 Who to refer for surgery?
37 Approach to Hypercalcemia
38 Osteoporosis: 68-year-old female Referred to you for a recent fracture She fell down trying to sit in a chair, fractured her T8 vertebrae Only medical condition is HTN treated with a beta blocker Started menstruation at the age of 13 Menopause occurred naturally at the age of 51 No family history of bone disorders
39 BMD Her DXA scan reported a T-score of -1.1 She was told she had osteopenia and did not require therapy at this time Placed on vitamin D and calcium supplements She comes to see you for a 2 nd opinion What should you tell her?
40 Does She Have Osteoporosis? A) YES B) NO
41 Osteoporosis Can be diagnosed irrespective of BMD and T-score The presence of a low trauma or fragility fracture is enough to make the diagnosis A fracture resulting from the force of a fall from a standing height or less Bone that breaks under conditions that would not cause a normal bone to break

42 Bone Loss Wrist Vertebral Hip ISCD Bone Densitometry Course Syllabus
43 Diagnosis & Treatment Osteoporosis Calcium and Vitamin D supplementation Bisphosphonate, or perhaps denosumab (Prolia) Physical therapy Addressing fall risks (banisters, rugs, etc.) BMD is only one component of bone strength Bone quality is not as easy to assess Presence of fracture, irrespective of BMD, reflects poor bone quality
44 Diagnosis Make sure any low trauma or fragility fracture is really not a pathological fracture Tumor, infection, inherited bone disorder Obtain X-ray and further labs if unsure! Careful history and physical Review of films
45 Osteoporosis Review A skeletal disorder characterized by compromised bone strength predisposing to an increased risk of fracture Bone strength reflects the integration of two main features Bone Density and Bone Quality

46 Bone Quality Healthy Unhealthy Bone Strength=Bone Quality +Bone Density Age Architecture Turnover Damage accumulation Mineralization Collagen quality g/cm2 hydroxyapatite
47 T-Score Number of SD the patient s BMD is above or below average BMD of young adult reference populations Caucasian Can ONLY diagnosis osteoporosis via T-score alone in Postmenopausal women -Menopausal transition Men 50
48 T-Score Lumbar spine, total hip, or femoral neck In certain circumstances, the 33% radius (AKA 1/3 radius) may be utilized -1.0 is normal Between -1.0 and -2.5 Low bone mass Previously referred to as osteopenia -2.5 is osteoporosis
49 Z-Score Number of standard deviations the patient s BMD is above or below age-sex-matched mean reference value Adjusted for self reported ethnicity Premenopausal women Males <50 Children/Adolescents
50 Z-Score -2.0 is below the expected range for age >-2.0 is within the expected range for age
51 Diagnosis Lowest T-score or Z-score is used to make the diagnosis Use appropriate score in appropriate setting T-score reporting for a 44-year-old male or premenopausal female is incorrect Often times the BMD reports incorrectly list two diagnoses: osteopenia at the lumbar spine and osteoporosis of the hip
52 Low BMD Does not necessarily mean Bone Loss Determining bone loss requires prior BMD measurement Low BMD can evolve in different ways: Low peak bone mass Low BMD followed by normal rate of loss Normal peak BMD with accelerated loss A single BMD can not distinguish these

53 ISCD Bone Densitometry Course Syllabus

54 Estimated incidence of fracture as a function of age and bone mass in 521 white women Followed for an average of 6.5 years Hui SL et al. J Clin Inve st 1988; 81:
55 What to order? Basic Testing CMP Total protein, albumin, alk phos, LFTs, Cr Phosphorus CBC 25-OH Vitamin D 24 hour urine calcium/creatinine/sodium
56 What to order? Further testing, if appropriate: Testosterone in males PTH TFTs Celiac disease Ab 4 hour urine free cortisol (and creatinine) or 1 mg DST SPEP/UPEP ESR, urine ph, serum bicarbonate Urine N-methylhistamine Bone turnover markers
57 Secondary causes, when to look beyond the basics? Men with osteoporosis Unexplained fracture Fragility fracture with normal BMD Non-responder to therapy BMD loss that exceeds expected loss (LSC) High index of clinical suspicion
58 Least Significant Change? Did patient have repeat BMD completed on same machine? Without a process called cross-calibration, you can NOT compare DXA results from different machines/manufacturers! This is the biggest mistake made by health care providers! You also can NOT compare T-scores and infer bone loss or gain
59 Least Significant Change If done at same facility/machine, is this difference greater than the least significant change (LSC)? Lease Significant Change There will be some difference from just error, differences in technician, etc. LSC is based on precision error and reproducibility, which is largely determined by technician
60 Serial BMD Useful to determine whether treatment should be started on untreated patients Significant loss may be an indication for treatment (or further evaluation) Can also be used to monitor response to therapy or identify lack of response to therapy
61 When to repeat BMD? Interval varies, based on if expected change equals or exceeds the LSC Typically one year after initiation or change of therapy Longer intervals once therapeutic effect is established
62 Treatment Mainstays: Oral bisphosphonates IV yearly bisphosphonates (Reclast) SC denosumab (Prolia), every 6 months
63 Male Hypogonadism Case 54-year-old man is referred for evaluation of low testosterone. He had seen his primary care physician for complaints of diminished libido and erectile dysfunction for the past year and worsening fatigue over the past few years. He has not been formally diagnosed with any medical condition. His serum testosterone level is 180 ng/dl (reference range ng/dl). On physical examination, he is obese (body mass index 31 kg/m2) with a normal-appearing male body habitus, no gynecomastia, and normal testicles and prostate gland. How should this patient be evaluated?


64 Signs & Symptoms of Low Testosterone Chances are, Clinical if you Findings are overweight, of Male Hypogonadism physically inactive, have chronic medical problems, or married (with children) you will fail this test.. Symptoms of low T are vague and non-specific
:717-25.")
65 Hypothalamic-Pituitary-Gonadal Axis Pantalone KM, Faiman C. Cleve Clin J Med Oct;79(10):
66 Low Testosterone Confronted with the finding of a low serum testosterone level, physicians should not jump to the diagnosis of hypogonadism and treat with testosterone supplementation Confirmation and thorough evaluation are warranted prior to making a diagnosis and/or starting therapy
67 Approach to Low Serum Testosterone Verify low testosterone near 8 am 1,2 Check LH/FSH 3 Low or normal range LH/FSH (Hypogonadotropic) Elevated LH/FSH (Hypergonadotropic) Secondary Hypogonadism Primary Hypogonadism Evaluate for Gonadotroph Suppression or Deficiency (Hypothalamic/Pituitary Process) Evaluate for Testicular Disorder 1-Repeat confirmatory level should always be performed at a reliable reference laboratory 2-On occasion, total testosterone levels may be low but bioavailable and/or free testosterone levels may be normal 3-Initial evaluation should also include serum prolactin, TSH, free T4, and ferritin
68 Primary Hypogonadism LH/FSH in the setting of testosterone Age of the patient at presentation, and careful questioning regarding pubertal development and fertility must be undertaken
69 Primary Hypogonadism Toxin exposure (chemotherapy) Congenital defects Anorchia, cryptorchidism Karyotype abnormalities Klinefelter Syndrome (47 XXY) Orchitis (mumps, autoimmune) Testicular trauma or infarction Hemochromatosis Increase in temperature of testicular environment Varicocele, large panniculus Medications which inhibit androgen synthesis Ketoconazole Farrer JH et al. Fertil Steril Jul;44(1): McDermott JH et al. J Clin Endocrinol Metab Apr;90(4): Sikka SC et al. Endocrinology May;116(5):
70 Secondary Hypogonadism or normal LH/FSH in the setting of testosterone Congenital Disorders Inherited/Genetic defect Acquired Damage to gonadotrophs Suppression of gonadotrophs
71 Congenital Disorders Kallmann syndrome Anosmia and GnRH deficiency Additional findings: cleft lip and/or palate, syndactyly, unilateral renal agenesis, and cryptorchidism KAL1 X-linked inheritance FGFR1, PROKR2, and PROK2 autosomal dominant Mutation/Deficiency of the GnRH receptors Genetic mutations associated with pituitary hormone deficiencies (PROP-1 mutation) Pallais JC et al. GeneReviews [Internet]. Seattle (WA): University of Washington, Seattle, [updated 2011 Aug 18]. Romero CJ et al. J Mol Endocrinol Jun 9;46(3):R93-R102. Print Chevrier L et al. Mol Cell Endocrinol Oct 22;346(1-2):21-8. Epub 2011 Apr 30.
72 Acquired Damage to Gonadotrophs Sellar mass/cysts pituitary adenomas, craniopharyngioma, Rathke cleft cyst, meningioma Infiltrative lesions lymphocytic hypophysitis, Langerhans cell hystiocytosis, sarcoidosis, hemochromatosis, infection Metastatic lesions (breast, renal cell, lung) Trauma (head injury) Radiation exposure/surgery to sellar region Pituitary apoplexy Stalk severance
:717-25.")
73 Acquired Suppression of Gonadotrophs Pantalone KM, Faiman C. Cleve Clin J Med Oct;79(10):
 used in the treatment of")
:38-43 Morrison D et al. Respir Med.")
74 Medications Chronic therapy with common medications such opioids and/or corticosteroids can result in secondary hypogonadism GnRH analogues (leuprolide) used in the treatment of prostate cancer Colameco S et al. Postgrad Med Jul;121(4):61-6. Fraser LA et al. Exp Clin Endocrinol Diabetes Jan;117(1):38-43 Morrison D et al. Respir Med Oct;88(9):

75 Obesity Obesity and the related conditions are independently associated with decreased plasma testosterone Obstructive sleep apnea Insulin resistance and/or type 2 diabetes mellitus Mah PM et al. Mol Cell Endocrinol Mar 25;316(2):180-6
 Testosterone replacement")
76 Obstructive Sleep Apnea Disturbances in the sleep cycle, regardless of the underlying cause, can result in decreased serum testosterone Often, correction of the underlying sleep disturbance can result in normalization of serum testosterone levels Caution must be used, and a thorough evaluation for sleep apnea should take place in high-risk individuals (obese) Testosterone replacement therapy can adversely affect ventilatory drive and induce or worsen obstructive sleep apnea! Santamaria JD et al. Clin Endocrinol (Oxf) May;28(5): Grunstein RR et al. J Clin Endocrinol Metab Feb;68(2): Matsumoto AM et al. Clin Endocrinol (Oxf) Jun;22(6):
77 Aging (? Andropause) There is an age-related decline in testosterone levels Testosterone peaks during adolescence and early adulthood With aging, levels gradually decline Typically about 1 percent per year after age 30 The circadian rhythm is often lost in older men Matsumoto AM. Rev Urol. 2003;5(Suppl 1):S3-S10. Feldman HA et al. J Clin Endocrinol Metab Feb;87(2): Bremner WJ et al. J Clin Endocrinol Metab Jun;56(6): Diver MJ et al. Clin Endocrinol (Oxf) Jun;58(6):710-7.
78 Aging (? Andropause) Factors such as functional status and overall health may play a more important role in the pathophysiology of hypogonadism in males of advanced age rather than age itself Matsumoto AM. Rev Urol. 2003;5(Suppl 1):S3-S10. Feldman HA et al. J Clin Endocrinol Metab Feb;87(2): Bremner WJ et al. J Clin Endocrinol Metab Jun;56(6): Diver MJ et al. Clin Endocrinol (Oxf) Jun;58(6):710-7.
79 Key Points Testosterone measurements should occur near 8 am A low serum testosterone value should always be confirmed by a reliable reference laboratory The definition of a low testosterone level varies from lab-to-lab In general, values < ng/dl are clearly low in most laboratories, and values between ng/dl may be considered borderline low Determine if the etiology is primary (testicular) or secondary (hypothalamic/pituitary) Acute illness and treatment with opioids, anabolic steroids, or corticosteroids can cause hypogonadism
80 Bhasin S et al. J Clin Endocrinol Metab, May 2018, 103(5):1 30. MRI &Secondary Hypogonadism The yield of pituitary-hypothalamic imaging in older men is fairly low in the absence of other pituitary hormone abnormalities/deficiencies There are limited data regarding appropriate criteria for performing pituitary imaging studies Cost-effectiveness to exclude pituitary and/or hypothalamic disease is unknown Guidelines/experts recommend imaging in patients with secondary hypogonadism when: The total testosterone level is very low (<150 ng/dl) There are abnormalities of multiple hypothalamic-pituitary axes panhypopituitarism Persistent hyperprolactinemia If clinical signs/symptoms warrant imaging Visual field deficits, cranial nerve palsy, etc.
81 Risks/Benefits/Alternatives of Treatment Discuss the R/B/A of treatment This conversation between the physician and patient should include dialogue regarding the uncertainty of the risks and benefits of testosterone supplementation in the older male population Treatment is only recommended in patients with clinically significant symptoms of androgen deficiency simply treating low T values is not recommended Recent guidelines suggest against routinely prescribing testosterone therapy to all men 65 years or older with low testosterone concentrations Treat the underlying cause, if one can be found Bhasin S et al. J Clin Endocrinol Metab, May 2018, 103(5):1 30.
82 Treatment Make decision on individual basis You prescribe the testosterone, you do the f/u testing and monitoring! HCT??? PSA and/or DRE Baseline, and at 3 to 12 months, and then annually Bhasin S et al. J Clin Endocrinol Metab, May 2018, 103(5):1 30.
83 Treatment Options Available modalities of testosterone replacement therapy (TRT) in the United States include: Depot-testosterone-IM cypionate or enanthate Topical solutions-axiron Gels-Testim, Androgel, or Fortesta, Natesto (nasal) Patches-Androderm Subcutaneous testosterone pellets-testopel Buccal-Striant SR
84 Treatment Goals Mid-normal Serum Testosterone Levels Transdermal preparations mid-normal range approximately ng/dl IM testosterone cypionate or enanthate approximately ng/dlmidway between injections some advocate trough of ng/dl Subcutaneous pellets within the normal range at the end of the dosing interval Bhasin S et al. J Clin Endocrinol Metab, May 2018, 103(5):1 30.
85 Low Testosterone and Cardiovascular Risk Low testosterone levels are associated with an increase in cardiovascular morbidity and mortality Independent of multiple risk factors and several preexisting medical conditions Mean/Median age >70 years This does not mean treating the low testosterone ameliorates this risk The low T may simply be a marker of overall poor health It remains uncertain if treating the low serum testosterone with supplementation reduces cardiovascular risk Health status and age at initiation of supplementation may be important Analogous to problems seen with HRT in women (WHI) Laughlin GA et al. J Clin Endocrinol Metab Jan;93(1): Tivesten A et al. J Clin Endocrinol Metab Jul;94(7):
86 Basaria S et al. N Engl J Med Jul 8;363(2):

87
88 New Data + Sexual Function, Mood & Depression + BMD + Anemia Cognitive Function No effect Coronary Artery Plaque Volume Increase in coronary artery non-calcified plaque volume Snyder PJ et al. N Engl J Med Feb 18;374(7): Snyder PJ et al. JAMA Intern Med. 2017;177(4): Roy CN et al. JAMA Intern Med. 2017;177(4): Resnick SM et al. JAMA. 2017;317(7): Budoff MJ et al. JAMA. 2017;317(7):
89 What to do? Despite the uncertainties, a 3-6 month trial in patients in whom the risks and benefits are unclear is reasonable May improve quality of life In the majority of patients, a positive response is usually delayed physicians should be suspect when dramatic improvements are reported very soon after the initiation of supplementation
90 Back to the case.. The patient s low serum testosterone was confirmed on subsequent measurements at 8 am, with levels of 128 and 182 ng/dl (reference range ). Other laboratory values: LH 1.4 miu/ml (reference range ) FSH 2.7 miu/ml ( miu/ml) Both of these values are inappropriately normal in the setting of the low testosterone TSH 248 μiu/ml ( ) Prolactin 24.6 ng/ml ( ). The patient was started on levothyroxine replacement therapy and after 3 months was noted to be euthyroid (TSH 1.8 μiu/ml) and to have a normal serum prolactin level. Testosterone levels (8 am) at this time were 350 ng/dl and 420 ng/dl. Therefore, the cause of this patient s hypogonadism was severe hypothyroidism and associated mild hyperprolactinemia. This case demonstrates that a thorough evaluation is warranted before initiating testosterone therapy.
91 Thank You! Questions????????
Endocrinology A Primer for Primary Care
 Endocrinology A Primer for Primary Care KM Pantalone Staff Endocrinologist Director of Clinical Research Department of Endocrinology Cleveland Clinic Objectives Review common endocrinology cases encountered
Endocrinology A Primer for Primary Care KM Pantalone Staff Endocrinologist Director of Clinical Research Department of Endocrinology Cleveland Clinic Objectives Review common endocrinology cases encountered
Hypogonadism 4/27/2018. Male Hypogonadism -- Definition. Epidemiology. Objectives HYPOGONADISM. Men with Hypogonadism. 95% untreated.
 Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
Male Hypogonadism. More than just a low testosterone? KM Pantalone Endocrinology
 Male Hypogonadism More than just a low testosterone? KM Pantalone Endocrinology Conflicts of Interest None to declare Case 1 A 54 year old man is referred for evaluation of low testosterone The patient
Male Hypogonadism More than just a low testosterone? KM Pantalone Endocrinology Conflicts of Interest None to declare Case 1 A 54 year old man is referred for evaluation of low testosterone The patient
Testosterone Therapy in Men with Hypogonadism
 Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Testosterone Treatment: Myths Vs Reality. Fadi Al-Khayer, M.D, F.A.C.E
 Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
GUIDELINES ON. Introduction. G.R. Dohle, S. Arver, C. Bettocchi, S. Kliesch, M. Punab, W. de Ronde
 GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
What Is the Low T Syndrome? Is Testosterone Supplementation Safe?
 What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or
What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or
Late onset Hypogonadism. Dr KhooSay Chuan Department of Urology Penang General Hospital
 Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients
 Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
6/14/2010. GnRH=Gonadotropin-Releasing Hormone.
 Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
GUIDELINES ON MALE HYPOGONADISM
 GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency
 Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
Disorders of Thyroid Function
 Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN
 International Society for Sexual Medicine - www.issm.info ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN Version: September 2015 What is testosterone deficiency? Testosterone deficiency
International Society for Sexual Medicine - www.issm.info ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN Version: September 2015 What is testosterone deficiency? Testosterone deficiency
Recognizing and Managing Testosterone Deficiency
 Recognizing and Managing Testosterone Deficiency J. Bruce Redmon, M.D. Professor Division of Endocrinology Departments of Medicine and Urologic Surgery Disclosure Information I have no financial relationships
Recognizing and Managing Testosterone Deficiency J. Bruce Redmon, M.D. Professor Division of Endocrinology Departments of Medicine and Urologic Surgery Disclosure Information I have no financial relationships
Androderm patch, AndroGel packets and pump, Axiron solution, First- Testosterone, First-Testosterone MC, Fortesta gel, Testim gel, Vogelxo
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.31 Subject: Testosterone Topical Page: 1 of 9 Last Review Date: September 23, 2016 Testosterone topical
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.31 Subject: Testosterone Topical Page: 1 of 9 Last Review Date: September 23, 2016 Testosterone topical
Disclosures. Learning Objectives. Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease. None
 Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
Testosterone Injection / Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Testosterone Injection / Implant Page: 1 of 9 Last Review Date: December 5, 2014 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Testosterone Injection / Implant Page: 1 of 9 Last Review Date: December 5, 2014 Testosterone
BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE
 Authoriser: Moya O Doherty Page 1 of 7 BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE The purpose of this protocol is to describe common tests used for the investigation
Authoriser: Moya O Doherty Page 1 of 7 BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE The purpose of this protocol is to describe common tests used for the investigation
in Primary Care (Part 2) Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University") Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
TESTOSTERONE DEFINITION
 DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone Oral Buccal Nasal Description
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone Oral Buccal Nasal Description
Androgen deficiency. Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital
 Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
43 year old man with low libido. Katie Stanley, MD August 16, 2012
 43 year old man with low libido Katie Stanley, MD August 16, 2012 HPI 43 yo M with history of heroin addiction on methadone maintenance Reported low libido to PCP PCP checked testosterone and found to
43 year old man with low libido Katie Stanley, MD August 16, 2012 HPI 43 yo M with history of heroin addiction on methadone maintenance Reported low libido to PCP PCP checked testosterone and found to
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone Oral Buccal Nasal
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone Oral Buccal Nasal
Bone Densitometry Pathway
 Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
5/7/2013. Patrick Nolan, DO, FACE
 Patrick Nolan, DO, FACE Patient: T.W. 83 year old male 9/18/2012 AM sudden onset of Vertigo ER visit Had MRI, some labs Home on Zofran and medicines Complete resolution of sx after 2 days MRI chronic sinus
Patrick Nolan, DO, FACE Patient: T.W. 83 year old male 9/18/2012 AM sudden onset of Vertigo ER visit Had MRI, some labs Home on Zofran and medicines Complete resolution of sx after 2 days MRI chronic sinus
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel AXIRON transdermal solution FORTESTA transdermal gel NATESTO nasal gel STRIANT buccal mucoadhesive
TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel AXIRON transdermal solution FORTESTA transdermal gel NATESTO nasal gel STRIANT buccal mucoadhesive
Endocrine Update Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh
 Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: June 24, 2016 Testosterone Oral Buccal Nasal Description
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: June 24, 2016 Testosterone Oral Buccal Nasal Description
Male Hypogonadism. Types and causes of hypogonadism. What is male hypogonadism? Symptoms. Testosterone production. Patient Information.
 Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
Pituitary Tumors and Incidentalomas. Bijan Ahrari, MD, FACE, ECNU Palm Medical Group
 Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
Testosterone (cypionate, enanthate, and propionate) powder, Fluoxymesterone powder, Methyltestosterone powder
 powder, Fluoxymesterone powder, Methyltestosterone powder") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.08.37 Subject: Testosterone Powder Page: 1 of 11 Last Review Date: September 18, 2015 Testosterone powder
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.08.37 Subject: Testosterone Powder Page: 1 of 11 Last Review Date: September 18, 2015 Testosterone powder
Testosterone Therapy in Men An update
 Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
Testosterone (cypionate, enanthate, and propionate) powder, Fluoxymesterone powder, Methyltestosterone powder
 powder, Fluoxymesterone powder, Methyltestosterone powder") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.37 Subject: Testosterone Powder Page: 1 of 12 Last Review Date: November 30, 2018 Testosterone powder
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.37 Subject: Testosterone Powder Page: 1 of 12 Last Review Date: November 30, 2018 Testosterone powder
Androgens. Medication Strengths Quantity Limit Comments Androderm (testosterone patch) 1% pump 2 pump bottles per Non-Preferred
 1% pump 2 pump bottles per Non-Preferred") Market DC Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Androderm (testosterone patch) AndroGel (testosterone
Market DC Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Androderm (testosterone patch) AndroGel (testosterone
GA KS KY LA MD NJ NV NY TN TX WA Applicable X X N/A N/A X N/A X X X X X X N/A N/A NA *FHK- Florida Healthy Kids. Androgens
 Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Generic Androgel 1% (2.5 g) packet 2 packets per day (testosterone
Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Generic Androgel 1% (2.5 g) packet 2 packets per day (testosterone
ANDROGEN DEFICIENCY/MALE HYPOGONADISM
 ANDROGEN DEFICIENCY/MALE HYPOGONADISM 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (androgen deficiency)
ANDROGEN DEFICIENCY/MALE HYPOGONADISM 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (androgen deficiency)
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: December 8, 2017 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: December 8, 2017 Testosterone
Managing Testosterone Deficiency: A Practical Guide. John Grantmyre MD Professor of Urology Dalhousie University
 Managing Testosterone Deficiency: A Practical Guide John Grantmyre MD Professor of Urology Dalhousie University 1 2 Case Study #1 A 59-Year-Old Man with Erectile Dysfunction 3 Case History Robert is a
Managing Testosterone Deficiency: A Practical Guide John Grantmyre MD Professor of Urology Dalhousie University 1 2 Case Study #1 A 59-Year-Old Man with Erectile Dysfunction 3 Case History Robert is a
ANDROGEN DEFICIENCY Update on Evaluation and Management
 ANDROGEN DEFICIENCY Update on Evaluation and Management Kristen Gill Hairston, MD, MPH Associate Professor of Internal Medicine Section of Endocrinology and Metabolism Wake Forest University School of
ANDROGEN DEFICIENCY Update on Evaluation and Management Kristen Gill Hairston, MD, MPH Associate Professor of Internal Medicine Section of Endocrinology and Metabolism Wake Forest University School of
ANDROGEN DEFICIENCY/MALE HYPOGONADISM
 Medical Information to Support the Decisions of TUE Committees 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of
Medical Information to Support the Decisions of TUE Committees 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone
OSTEOPOROSIS IN MEN. Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone
Clinical Policy: Testosterone Pellet (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date:
![Clinical Policy: Testosterone Pellet (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date:](/thumbs/75/72057018.jpg "Clinical Policy: Testosterone Pellet (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date:") Clinical Policy: (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date: 07.25.17 Last Review Date: 11.17 Line of Business: Commercial Coding Implications Revision Log See Important Reminder
Clinical Policy: (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date: 07.25.17 Last Review Date: 11.17 Line of Business: Commercial Coding Implications Revision Log See Important Reminder
DXA When to order? How to interpret? Dr Nikhil Tandon Department of Endocrinology and Metabolism All India Institute of Medical Sciences New Delhi
 DXA When to order? How to interpret? Dr Nikhil Tandon Department of Endocrinology and Metabolism All India Institute of Medical Sciences New Delhi Clinical Utility of Bone Densitometry Diagnosis (DXA)
DXA When to order? How to interpret? Dr Nikhil Tandon Department of Endocrinology and Metabolism All India Institute of Medical Sciences New Delhi Clinical Utility of Bone Densitometry Diagnosis (DXA)
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Men Getting Older Will Testosterone Keep Him Young?
 Men Getting Older Will Testosterone Keep Him Young? Alvin M. Matsumoto, M.D. Associate Director, GRECC V.A. Puget Sound Health Care System Professor, Department of Medicine Division of Gerontology and
Men Getting Older Will Testosterone Keep Him Young? Alvin M. Matsumoto, M.D. Associate Director, GRECC V.A. Puget Sound Health Care System Professor, Department of Medicine Division of Gerontology and
Diagnosis and Treatment of Osteoporosis. Department of Endocrinology and Metabolism Ajou University School of Medicine.
 Diagnosis and Treatment of Osteoporosis Department of Endocrinology and Metabolism Ajou University School of Medicine Yoon-Sok CHUNG WCIM, COEX, Seoul, 27Oct2014 Case 1 71-year old woman Back pain Emergency
Diagnosis and Treatment of Osteoporosis Department of Endocrinology and Metabolism Ajou University School of Medicine Yoon-Sok CHUNG WCIM, COEX, Seoul, 27Oct2014 Case 1 71-year old woman Back pain Emergency
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
Clinical Practice. Presented by: Internist, Endocrinologist
 Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY)
") HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
Implantable Hormone Pellets
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
BAD TO THE BONE. Peter Jones, Rheumatologist QE Health, Rotorua. GP CME Conference Rotorua, June 2008
 BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
Interpreting DEXA Scan and. the New Fracture Risk. Assessment. Algorithm
 Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
Breast Cancer and Bone Loss. One in seven women will develop breast cancer during a lifetime
 Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA
 Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
BREAST CANCER AND BONE HEALTH
 BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
Pharmacy Management Drug Policy
 Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Puberty and Pubertal Disorders Part 3: Delayed Puberty
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Puberty and Pubertal Disorders Part 3: Delayed Puberty These podcasts are designed to give medical students an overview
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Puberty and Pubertal Disorders Part 3: Delayed Puberty These podcasts are designed to give medical students an overview
Hormone Balance - Female Report SAMPLE. result graph based on Luteal Phase. result graph based on Luteal Phase
 Patient Name: Patient DOB: Gender: Physician: Test Hormone Balance - Female Report SAMPLE Grote, Mary Jane Batch Number: B6437 2/16/1954 Accession Number: N52281 F Date Received: 2/3/2015 Any Lab Test
Patient Name: Patient DOB: Gender: Physician: Test Hormone Balance - Female Report SAMPLE Grote, Mary Jane Batch Number: B6437 2/16/1954 Accession Number: N52281 F Date Received: 2/3/2015 Any Lab Test
TUE Physician Guidelines Medical Information to Support the Decisions of TUE Committees MALE HYPOGONADISM MALE HYPOGONADISM
 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (testosterone deficiency) and in some instances normal
1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (testosterone deficiency) and in some instances normal
66 M with erectile dysfunction and abnormal labs RAJESH JAIN ENDORAMA 10/29/2015
 66 M with erectile dysfunction and abnormal labs RAJESH JAIN ENDORAMA 10/29/2015 HPI 66 M presenting as a referral for erectile dysfunction and abnormal labs Has been seeing a facility specializing in
66 M with erectile dysfunction and abnormal labs RAJESH JAIN ENDORAMA 10/29/2015 HPI 66 M presenting as a referral for erectile dysfunction and abnormal labs Has been seeing a facility specializing in
Osteoporosis challenges
 Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
06-Mar-17. Premature menopause. Menopause. Premature menopause. Menstrual cycle oestradiol. Premature menopause. Prevalence ~1% Higher incidence:
 Menopause Dr Sonia Davison MBBS FRACP PhD Endocrinologist and Clinical Fellow, Jean Hailes for Women s Health Women s Health Research Program, Monash University = the last natural menstrual period depletion
Menopause Dr Sonia Davison MBBS FRACP PhD Endocrinologist and Clinical Fellow, Jean Hailes for Women s Health Women s Health Research Program, Monash University = the last natural menstrual period depletion
Endocrine Case Presentations
 Endocrine Case Presentations Matt Bouchonville Endocrinology Division Family Medicine Resident School March 19, 2014 Learning Objectives 1. Understand the evaluation and management of common thyroid disorders
Endocrine Case Presentations Matt Bouchonville Endocrinology Division Family Medicine Resident School March 19, 2014 Learning Objectives 1. Understand the evaluation and management of common thyroid disorders
Male hypogonadism: More than just a low testosterone
 REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will conduct an appropriate workup of low testosterone before considering prescribing testosterone replacement KEVIN M. PANTALONE, DO, ECNU, CCD Endocrinology
REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: Readers will conduct an appropriate workup of low testosterone before considering prescribing testosterone replacement KEVIN M. PANTALONE, DO, ECNU, CCD Endocrinology
Pituitary Adenomas: Evaluation and Management. Fawn M. Wolf, MD 10/27/17
 Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
A dro r gen e R e R p e lac a e c m e e m n e t t T her e a r p a y Androgen Replacement Therapy in the Aging O j b ecti t ve v s Male
 Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
Overview of Reproductive Endocrinology
 Overview of Reproductive Endocrinology I have no conflicts of interest to report. Maria Yialamas, MD Female Hypothalamic--Gonadal Axis 15 4 Hormone Secretion in the Normal Menstrual Cycle LH FSH E2, Progesterone,
Overview of Reproductive Endocrinology I have no conflicts of interest to report. Maria Yialamas, MD Female Hypothalamic--Gonadal Axis 15 4 Hormone Secretion in the Normal Menstrual Cycle LH FSH E2, Progesterone,
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel ANDROID (methyltestosterone) oral capsule ANDROXY (fluoxymesterone) oral tablet AXIRON transdermal
TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel ANDROID (methyltestosterone) oral capsule ANDROXY (fluoxymesterone) oral tablet AXIRON transdermal
BMD: A Continuum of Risk WHO Bone Density Criteria
 Pathogenesis of Osteoporosis Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis AGING MENOPAUSE OTHER RISK FACTORS RESORPTION > FORMATION Bone Loss LOW PEAK BONE MASS Steven T Harris
Pathogenesis of Osteoporosis Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis AGING MENOPAUSE OTHER RISK FACTORS RESORPTION > FORMATION Bone Loss LOW PEAK BONE MASS Steven T Harris
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
More than meets the eye
 More than meets the eye Ana Paula Abreu, MD, PhD American Association of Clinical Endocrinologists New England Chapter Annual Meeting September 8, 2018 Disclosures No conflict of interest or significant
More than meets the eye Ana Paula Abreu, MD, PhD American Association of Clinical Endocrinologists New England Chapter Annual Meeting September 8, 2018 Disclosures No conflict of interest or significant
OVERVIEW OF PRESENTATION
 Thanh D. Hoang, DO, FACP, FACE Division of Endocrinology Department of Internal Medicine WRNMMC 13 Aug 2018 OVERVIEW OF PRESENTATION Take Home Points Definition of Hypogonadism Clinical Manifestations
Thanh D. Hoang, DO, FACP, FACE Division of Endocrinology Department of Internal Medicine WRNMMC 13 Aug 2018 OVERVIEW OF PRESENTATION Take Home Points Definition of Hypogonadism Clinical Manifestations
Study of secondary causes of male osteoporosis
 Study of secondary causes of male osteoporosis Suárez, S.M., Giunta J., Meneses G., Costanzo P.R., Knoblovits P. Department of Endocrinology, Metabolism and Nuclear Medicine of Hospital Italiano of Buenos
Study of secondary causes of male osteoporosis Suárez, S.M., Giunta J., Meneses G., Costanzo P.R., Knoblovits P. Department of Endocrinology, Metabolism and Nuclear Medicine of Hospital Italiano of Buenos
Skeletal Manifestations
 Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Men and Osteoporosis So you think that it can t happen to you
 Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Therapeutic Cohort Results
 Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
PRIMARY HYPERPARATHYROIDISM PRIMARY HYPERPARATHYROIDISM. Hyperparathyroidism Etiology. Common Complex Insidious Chronic Global Only cure is surgery
 ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
Hypogonadism in Men. CME Away India & Sri Lanka March 23 - April 7, 2018
 Hypogonadism in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
Hypogonadism in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
One Day Hormone Check
 One Day Hormone Check Patient: EMILY TEST DOB: January 18, 1948 Sex: F MRN: 0000000004 Order Number: J5070009 Completed: March 07, 2014 Received: March 07, 2014 Collected: March 07, 2014 Alec Smart, ND
One Day Hormone Check Patient: EMILY TEST DOB: January 18, 1948 Sex: F MRN: 0000000004 Order Number: J5070009 Completed: March 07, 2014 Received: March 07, 2014 Collected: March 07, 2014 Alec Smart, ND
Late onset hypogonadism
 Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
Drug Intervals (Holidays) with Oral Bisphosphonates
 with Oral Bisphosphonates") Drug Intervals (Holidays) with Oral Bisphosphonates Rizwan Rajak Consultant Rheumatologist & Lead for Osteoporosis GP Postgraduate Meeting April 2018 Contents Case presentation Pathway for Bisphosphonate
Drug Intervals (Holidays) with Oral Bisphosphonates Rizwan Rajak Consultant Rheumatologist & Lead for Osteoporosis GP Postgraduate Meeting April 2018 Contents Case presentation Pathway for Bisphosphonate
Adrenal Stress Profile (Saliva)
") Adrenal Stress Profile (Saliva) Ireland Cortisol Levels Sample 1 Post Awakening Sample 2 (+ 4-5 Hours) Sample 3 (+ 4-5 Hours) Sample 4 (Prior to Sleep) 11.42 2.10 1.60 0.47 Sum of Cortisol 15.590 DHEA
Adrenal Stress Profile (Saliva) Ireland Cortisol Levels Sample 1 Post Awakening Sample 2 (+ 4-5 Hours) Sample 3 (+ 4-5 Hours) Sample 4 (Prior to Sleep) 11.42 2.10 1.60 0.47 Sum of Cortisol 15.590 DHEA
Pituitary Apoplexy. Updated: April 22, 2018 CLINICAL RECOGNITION
 Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment. William D. Leslie, MD MSc FRCPC
 Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Guideline for the investigation and management of osteoporosis. for hospitals and General Practice
 Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Update on diagnosis and complications of adult and elderly male hypogonadism
 Hypoandrogenism in the elderly: to treat or not to treat? 12 th Italian AME Meeting; 6 th joint Meeting with AAC Bari november 10th Update on diagnosis and complications of adult and elderly male hypogonadism
Hypoandrogenism in the elderly: to treat or not to treat? 12 th Italian AME Meeting; 6 th joint Meeting with AAC Bari november 10th Update on diagnosis and complications of adult and elderly male hypogonadism
One Day Hormone Check
 One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
Hormones. Introduction to Endocrine Disorders. Hormone actions. Modulation of hormone levels. Modulation of hormone levels
 Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis
Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis