FLOOVIDEOFLUOROSCOPIC SWALLOW STUDIES: LOOKING BEYOND ASPIRATION. Brenda Sitzmann, MA, CCC-SLP (816)
|
|
|
- Roderick Perkins
- 5 years ago
- Views:
Transcription
1 FLOOVIDEOFLUOROSCOPIC SWALLOW STUDIES: LOOKING BEYOND ASPIRATION Brenda Sitzmann, MA, CCC-SLP (816)
2 DISCLOSURES Ms. Sitzmann is speech-language pathologist at Children s Mercy for which she receives a salary. Ms. Sitzmann is receiving an honorarium for presenting this workshop. Ms. Sitzmann has no non-financial relationships to disclose.
3 VIDEOFLUOROSCOPIC SWALLOW STUDIES VFS or VFSS for short Previously known as an OPM (Oral Pharyngeal Motility Study) at Children s Mercy (CMH) Modified Barium Swallow Study It is video x-ray of the patient s swallow
4 REFERRALS Clinical signs of aspiration coughing choking frequent respiratory infections Pneumonia, Bronchiolitis vs. RSV wet breath or vocal sounds with feedings Poor weight gain Limited interest in oral feedings
5 A WORD OF CAUTION RE: CLINICAL SIGNS OF ASPIRATION Clinical signs and symptoms of oropharyngeal aspiration and dysphagia in children (Weir et al. 2009) 150 children median age = 16 months; range 2 weeks weeks (nearly 3 years) 106 (71%) had a neurological impairment Findings Cough, wet voice and wet breathing were most significantly associated with aspiration on thin liquids These markers were NOT associated with aspiration on purees No markers were associated with isolated laryngeal penetration or postswallow residue on purees Post swallow residue on thin liquids was associated with coughing
6 A WORD OF CAUTION RE: CLINICAL SIGNS OF ASPIRATION Clinical signs and symptoms of oropharyngeal aspiration and dysphagia in children (Weir et al. 2009) Findings (continued) Infants were more likely to have wet voice on thin liquids Older children who aspirated were more likely to demonstrate wet breathing with thin liquids and purees Isolated laryngeal penetration or post-swallow residue = no clinical markers regardless of consistency or age group Neurological impairment = strong correlation between wet voice and breathing and aspiration on thin liquids Non-neurological group = wet voice was associated with aspiration
7 REFERRALS A VFSS is not the best assessment for: Limited oral intake Ideally patient is accepting at least 1 oz. orally Chewing concerns Multidimensional process but VFSS typically only offers a lateral view Best assessed clinically Barium allergy Rare
8 PREPARATION FOR THE STUDY Requires a physician order Patient preparation: Nothing to eat or drink for 2-3 hours prior to the study goal = hungry and willing to accept barium patient should be hungry but not hangry No metal on clothing from the waist up No siblings in the radiology suite Bring familiar bottles, cups, utensils, preferred food Items for a typical feeding after the study Ideally caregiver will be present for the study
9 SET UP FOR THE PROCEDURE Goal is to replicate a typical feeding as much as possible Positioning Upright Reclined Side-lying Bottle/cup Utensils Feeder techniques Most patients benefit from a clinical feeding evaluation prior to a VFS

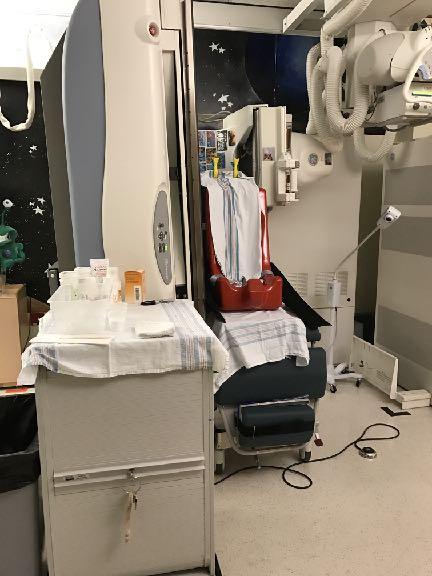
10 SET UP FOR THE PROCEDURE
11 PROCEDURE Typically start with thin liquids prefer to use patient s current bottle or cup may evaluate swallow after a fatigue period (i.e. the patient continues to drink the barium but there is no fluoroscopy for a period of time (typically seconds) Implement compensatory strategies before increasing viscosity of the liquid Typically progress from thin to nectar to honey to honey plus this pattern varies depending on observations
12 COMPENSATORY STRATEGIES Ideally, we want to try all other options before thickening liquids. Positioning Elevated side-lying More upright Slightly reclined Flow rate Slower flowing nipple Sippy cup vs. open cup Straw Use with caution
13 COMPENSATORY STRATEGIES Techniques Pacing Chin tuck Multiple swallows Chin/jaw support Consistency of liquids Thin Nectar Honey Spoon Thick typically requires supplemental non-oral feedings due to dehydration concerns
14 COMPENSATORY STRATEGIES Information from the feeding therapist is very helpful Helpful strategies Positioning Pacing Bolus presentation Challenging liquids/foods Current treatment plan Clinical feeding plan prior to the VFSS
15 BARIUM Basic Element On the periodic table White when it goes in and white when it comes out Can be mildly constipating but typically intake during a VFSS is limited Slightly chalking Can flavor it Kool-Aid packets Avoid products that would alter the consistency
16 BARIUM We use Varibar Barium at CMH Thin Nectar Thin Honey this corresponds to the standard honey recipe for most thickening agents Honey Pudding
17 LIQUID CONSISTENCIES At Children s Mercy, we use the following consistencies clinically: Thin Water, milk, breastmilk Nectar 3 teaspoons of Thick & Easy per 4 oz. of liquid Syrup (this is typically called honey consistency) 4 1/2 teaspoons of Thick & Easy per 4 oz. of liquid Honey (this is typically called spoon thick) 5 1/2 teaspoons of Thick & Easy per 4 oz. of liquid
18 LIQUID CONSISTENCIES Currently working on standardizing recipes and identifying the best thickening agents Would like our recipes to match the viscosity of the Varibar Barium products we use during swallow studies Visualization is a very inaccurate way to assess viscosity Improve education and compliance with thickening recommendations
19 OPTIMAL SAMPLING RATE ASHA recommends a national standard of 30 frames per second We currently use 15 fps at Children s Mercy SLPs are working with radiology to change this practice Bonilha, et. al scores from MBSImp and Penetration-Aspiration Scale varied between pulse rates Cohen 2009 The full depth of laryngeal penetration was visible on only 1 frame for 70% of the studies
20 THREE PHASES OF SWALLOWING Oral phase Pharyngeal phase Esophageal phase At CMH, a swallow study is used to evaluate the first 2 phases
21 ORAL PHASE During a swallow study, we are evaluating the following areas: Lip seal Bottling Cup drinking Spoon feeding Oral containment of the bolus Tongue movement Tongue base retraction Tongue pumping, fasciculations
22 ORAL PHASE Bolus control Is the bolus split, pocketed Chewing A swallow study is not typically the best evaluation of chewing concerns (recommend a clinical feeding evaluation) Lingual-palatal seal Prevents the bolus from entering the pharynx too soon Piecemeal deglutition Bolus is divided into smaller parts before swallowing
23 ORAL PHASE Residue after the swallow Bolus size Too big Too small Inefficient extraction Pacing Difficulty coordinating suck-swallow-breathe pattern Consecutive swallows Controlled pattern
24 PHARYNGEAL PHASE Trigger of the swallow response Lots of opinions on this topic Pooling/filling in the valleculae and pyriforms Associated with poor oral containment and a delayed swallow Acceptable pooling varies by age Epiglottic inversion Simplified version of airway protection: Epiglottis inverts ( caps the larynx ) Aryepiglottic folds tighten (purse-like strings) Vocal folds adduct (close)
25 PHARYNGEAL PHASE Hyo-laryngeal elevation The larynx moves up and forward during the swallow to initiate airway protection Decreased elevation may contribute to reduced epiglottic inversion, laryngeal penetration, aspiration, cricopharyngeal dysfunction, and residue after the swallow Cricopharyngeal dysfunction may cause reduced hyo-laryngeal elevation Nasopharyngeal reflux Part of the bolus enters the nasal cavity Somewhat acceptable in neonates Common in infants with unrepaired cleft palate
26 PHARYNGEAL PHASE Pharyngeal peristalsis Pharyngeal weakness will result in residue Increases risk for aspiration Uncoordinated May divide the bolus May contribute to nasopharyngeal reflux Laryngeal penetration Aspiration Residue after the swallow Location of residue can provide cues about swallowing difficulties
27 PHARYNGEAL PHASE Cricopharyngeal/upper esophageal sphincter function Does the bolus easily pass into the esophagus? May be caused by reduced hyo-laryngeal elevation but may also be limiting hyo-laryngeal elevation (tethering effect) Signs of a tracheoesophageal fistula Barium in the airway without aspiration
28 LARYNGEAL PENETRATION Food or liquid enters the laryngeal vestibule but does not go below the vocal folds Severity: Amount of barium Trace, slight, moderate, entire bolus Level of penetration Upper 1/3 of the laryngeal vestibule Upper 2/3 Deep = touches or nearly touches the vocal folds Not a safe feeding plan Will often stop testing that consistency during a VFS to minimize radiation exposure Residue in laryngeal vestibule
29 LARYNGEAL PENETRATION Gurberg, J., et al pediatric patients with a wide range of diagnoses 58 had neither laryngeal penetration or aspiration 59 had laryngeal penetration 48 had tracheobronchial aspiration Children with laryngeal penetration on videofluoroscopic swallowing study had significantly more pneumonia than patients with neither penetration nor aspiration. 2 pneumonias compared to 0 Increased risk for pneumonia and aspiration for patients with glottic abnormalities (ex. laryngeal cleft) Associated syndromes did not appear to impact risk for pneumonia or aspiration
30 LARYNGEAL PENETRATION Friedman, B., et al % of the 125 children in the study demonstrated laryngeal penetration 31% = deep laryngeal penetration 85% of these children eventually aspirated during the study Why are these studies important? Laryngeal penetration is not benign Minimize radiation exposure deep laryngeal penetration is not a safe plan so we can move to the next strategy or consistency faster vs. waiting to witness aspiration
31 ASPIRATION Food or liquid passes through the vocal folds and into the subglottic space Types Silent (no cough) very common in the pediatric population Can be very hard to detect silent aspiration clinically VFSS is the gold standard Aspiration with a cough Aspiration with a delayed cough
32 ASPIRATION Timing of the aspiration event Before the swallow suggests a delayed or absent swallow During suggests incomplete vocal fold closure, reduced hyo-laryngeal elevation, laryngeal cleft After often due to residue
33 ASPIRATION Amount of barium aspirated Trace, minimal Was the patient able to clear the barium from the airway? Effective cough Cue to cough or spontaneous Other signs of aspiration Watery eyes Stopped the feeding Wet breath or vocal sounds
34 PENETRATION-ASPIRATION SCALE Rosenbeck, J.C., et al = Material does not enter the airway 2 = Material enters the airway, remains above the vocal folds, and is not ejected from the airway 3 = Material enters the airway, remains above the vocal folds, and is not ejected from the airway 4 = Material enters the airway, contacts the vocal folds, and is ejected from the airway 5 = Material enters with airway, passes below the vocal folds, and is not ejected from the airway 6 = Material enters the airway, passes below the vocal folds, and is ejected into the larynx or out of the airway 7 = Material enters the airway, passes below the vocal folds, and is not ejected from the trachea despite effort 8 = Material enters the airway, passes below the vocal folds, and no effort is made to eject
35 MBSIMP Martin-Harris, B. et al Modified Barium Swallow Impairment Profile (MBSImP) A standardized approach to instruction, assessment, and reporting of physiologic swallowing impairment Evidence based Assesses 17 components of swallowing SLPs become a Registered MBSImP Clinician upon successful completion of the MBSImP Online Training and Reliability Testing Pediatric protocol is being developed
36 DOCUMENTATION Findings Safe swallow for Aspiration/penetration note consistencies Possible reason for dysphagia concerns Diagnosis Oral dysphagia Pharyngeal dysphagia Oral-pharyngeal dysphagia Support for diagnosis
37 DOCUMENTATION Recommendations Feeding plan liquid consistency recommended recipe recommended thickening agent solids will require physician approval for thickening Therapy ideally will include recommendations for therapy goals/ activities
38 DOCUMENTATION Recommendations (continued) Referrals ENT GI Repeat swallow study recommend limiting studies as much as possible Approximately every 6-12 months Change in swallow Change in medical status Clinical feeding evaluation prior to a repeat study
39 FEES VS. VFSS
40 FEES Flexible Endoscopic Evaluation of Swallowing (FEES) A flexible endoscope is used to evaluate the pharyngeal phase of the swallow At Children s Mercy, ENT typically places the scope Use green dye for contrast Multiple positioning options including: Caregiver's lap Exam chair Wheelchair
41 FEES Candidates for FEES include: Suspect structural issues are impacting swallow safety Assessing secretion management typically done with children who are not oral eaters Only instrumental assessment to further evaluate breastfeeding Special positioning needs Unable to tolerate a VFSS
42 FEES Pros: No radiation exposure Study time is limited only by patient s tolerance/ willingness to participate Able to use the patient s preferred foods Breastfeeding No need to alter taste or texture with barium Green dye is optional Able to view saliva swallows More flexible seating/positioning
43 FEES Pros (continued): Excellent view of pharyngeal anatomy Base of tongue Epiglottis Vocal folds Arytenoid cartilage Able to view asymmetry Unilateral pooling
44 FEES Cons: White out during the swallow Challenging to identify aspiration looking for signs of the aspirated bolus between or below the vocal folds Blocks the nasal airway May impact bottle and breastfeeding Nasogastric tubes May be uncomfortable Pharyngeal phase only unable to assess tongue movement or other elements of the oral phase
45 VFSS Pros: Gold standard for identification of laryngeal penetration and aspiration Able to track the bolus through the oral and pharyngeal phases as well as esophageal phase May be able to see possible signs of a TE fistula and/or laryngeal cleft further work-up may be necessary to fully evaluate these concerns
46 VFSS Cons: Radiation exposure Must use barium Unable to clearly evaluate structures vocal folds More challenging to identify asymmetries At CMH, we typically only complete a lateral view to minimize radiation exposure Anterior posture view
47 CASE STUDIES & VIDEOS
48 REFERENCES Bonilha, H.S., Blair, J., Carnes, B., Huda, W., Humphries, K., McGrattan, K., Michel, Y., Martin-Harris, B., Preliminary investigation of the effect of pulse rate on judgments of swallowing impairment and treatment recommendations. Dysphagia. 28(4): Cohen, M.D Can we use pulsed fluoroscopy to decrease the radiation does during video fluoroscopic feeding studies in children? Clinical Radiology. 64(1): Delaney, A.L., Barkmeier-Kraemer, J Instrumental Swallowing Assessment: Considerations for standardized protocols and on-line decision making. Feeding Matters. Phoenix, AZ. Friedman, B., Frazier, J.B Dysphagia. 15:
49 REFERENCES Gurberg, J., Birnbaum, R., Daniel, S.J Laryngeal penetration on videofluoroscopic swallowing study is associated with increased pneumonia in children. International Journal of Pediatric Otorhinolaryngology. 79: Ro Rosenbek, J.C., Robbins, J., Roecker, E.B., Coyle, J.I., Wood, J.L A Penetration-Aspiration Scale. Dysphagia. 11: Martin-Harris, B., Brodsky, M., Michel. Y., Castell, D., Schleicher, M., Sandige, J., Maxwell, R., Blair, J MBS measurement tool of swallow impairment - MBSImp: Establishing a standard. Dysphagia. (4): Weir, K., McMahon, S., Barry, L., Masters, I.B., & Chang, A.B Clinical signs and symptoms of oropharyngeal aspiration and dysphagia in children. European Respiratory Journal. 33:
50 QUESTIONS?
51 THANK YOU! Brenda Sitzmann, MA, CCC-SLP (816)
Guideline of Videofluoroscopic Swallowing Study (VFSS) in Speech Therapy
 in Speech Therapy") Page 1 of 9 Guideline of Videofluoroscopic Swallowing Study (VFSS) in Speech Therapy Version 1.0 Effective Date Document Number HKIST-C-VFG-v1 Author HKAST AR Sub-committee Custodian Chairperson of HKIST
Page 1 of 9 Guideline of Videofluoroscopic Swallowing Study (VFSS) in Speech Therapy Version 1.0 Effective Date Document Number HKIST-C-VFG-v1 Author HKAST AR Sub-committee Custodian Chairperson of HKIST
SWALLOWING DIFFICULTIES IN HD
 Nutrition, eating and swallowing needs, challenges and solutions Workshop SWALLOWING DIFFICULTIES IN HD Angela Nuzzi Speech and Language Pathologist (SLP) EHDN Language Coordinator - Italy The role of
Nutrition, eating and swallowing needs, challenges and solutions Workshop SWALLOWING DIFFICULTIES IN HD Angela Nuzzi Speech and Language Pathologist (SLP) EHDN Language Coordinator - Italy The role of
Pediatric Modified Barium Swallow Studies. Presented by Jody Bousquet, MA, CCC- SLP Susan Shonbrun, MS, CCC- SLP November 7, 2015
 Pediatric Modified Barium Swallow Studies Presented by Jody Bousquet, MA, CCC- SLP Susan Shonbrun, MS, CCC- SLP November 7, 2015 Definition * Modified Barium Swallow Study * Assesses swallow functions
Pediatric Modified Barium Swallow Studies Presented by Jody Bousquet, MA, CCC- SLP Susan Shonbrun, MS, CCC- SLP November 7, 2015 Definition * Modified Barium Swallow Study * Assesses swallow functions
Understanding your child s videofluoroscopic swallow study report
 Understanding your child s videofluoroscopic swallow study report This leaflet is given to you during your child s appointment in order to explain some of the words used by the speech and language therapist
Understanding your child s videofluoroscopic swallow study report This leaflet is given to you during your child s appointment in order to explain some of the words used by the speech and language therapist
VIDEOFLUOROSCOPIC SWALLOWING EXAM
 VIDEOFLUOROSCOPIC SWALLOWING EXAM INDENTIFYING INFORMATION May include the following: Name, ID/medical record number, date of birth, date of exam, referred by, reason for referral HISTORY/SUBJECTIVE INFORMATION
VIDEOFLUOROSCOPIC SWALLOWING EXAM INDENTIFYING INFORMATION May include the following: Name, ID/medical record number, date of birth, date of exam, referred by, reason for referral HISTORY/SUBJECTIVE INFORMATION
Swallowing Screen Why? How? and So What? พญ.พวงแก ว ธ ต สก ลช ย ภาคว ชาเวชศาสตร ฟ นฟ คณะแพทยศาสตร ศ ร ราชพยาบาล
 Swallowing Screen Why? How? and So What? พญ.พวงแก ว ธ ต สก ลช ย ภาคว ชาเวชศาสตร ฟ นฟ คณะแพทยศาสตร ศ ร ราชพยาบาล Dysphagia in Stroke The incidence of dysphagia after stroke ranging from 23-50% 1 Location
Swallowing Screen Why? How? and So What? พญ.พวงแก ว ธ ต สก ลช ย ภาคว ชาเวชศาสตร ฟ นฟ คณะแพทยศาสตร ศ ร ราชพยาบาล Dysphagia in Stroke The incidence of dysphagia after stroke ranging from 23-50% 1 Location
Analyzing Swallow Studies in Pediatrics
 Analyzing Swallow Studies in Pediatrics About the Speaker Robert Beecher, M.S., CCC-SLP was formerly senior speech-language pahologist at the Children's Hospital of Wisconsin in Milwaukee. He is specialized
Analyzing Swallow Studies in Pediatrics About the Speaker Robert Beecher, M.S., CCC-SLP was formerly senior speech-language pahologist at the Children's Hospital of Wisconsin in Milwaukee. He is specialized
Video Fluoroscopic Swallowing Exam (VFSE)
") Scan for mobile link. Video Fluoroscopic Swallowing Exam (VFSE) A video fluoroscopic swallowing exam (VFSE) uses a form of real-time x-ray called fluoroscopy to evaluate a patient s ability to swallow
Scan for mobile link. Video Fluoroscopic Swallowing Exam (VFSE) A video fluoroscopic swallowing exam (VFSE) uses a form of real-time x-ray called fluoroscopy to evaluate a patient s ability to swallow
The Role of the Speech Language Pathologist & Spinal Cord Injury
 The Role of the Speech Language Pathologist & Spinal Cord Injury Facts According to the National Spinal Cord Injury Statistical Center (NSCISC) there are approxiamtely 12,000 new spinal cord injuries (SCI)
The Role of the Speech Language Pathologist & Spinal Cord Injury Facts According to the National Spinal Cord Injury Statistical Center (NSCISC) there are approxiamtely 12,000 new spinal cord injuries (SCI)
Clinical Swallowing Exam
 Clinical Evaluation Template 1 Clinical Exam Name: ID/Medical record number: Date of exam: Referred by: Reason for referral: Medical diagnosis: Date of onset of diagnosis: Other relevant medical history/diagnoses/surgery
Clinical Evaluation Template 1 Clinical Exam Name: ID/Medical record number: Date of exam: Referred by: Reason for referral: Medical diagnosis: Date of onset of diagnosis: Other relevant medical history/diagnoses/surgery
State of Art & Science for Evaluation of Infants & Children with Signs/Symptoms of Dysphagia. Introduction. Instrumental Swallow Evaluations
 Problem Solving with Instrumental Swallow Evaluations & Management 49 th Annual Mid-South Conference, Feb. 21, 2019 Joan C. Arvedson, PhD, CCC-SLP, BCS-S, ASHA Honors & Fellow jcarved@aol.com & jarvedson@chw.org
Problem Solving with Instrumental Swallow Evaluations & Management 49 th Annual Mid-South Conference, Feb. 21, 2019 Joan C. Arvedson, PhD, CCC-SLP, BCS-S, ASHA Honors & Fellow jcarved@aol.com & jarvedson@chw.org
SWALLOWING: HOW CAN WE HELP
 SWALLOWING: HOW CAN WE HELP Carol Romero-Clark, M.S., CCC-SLP University of New Mexico Hospital Speech Pathology Department November 10, 2017 What happens when you swallow? Mouth (Oral Phase) Your tongue
SWALLOWING: HOW CAN WE HELP Carol Romero-Clark, M.S., CCC-SLP University of New Mexico Hospital Speech Pathology Department November 10, 2017 What happens when you swallow? Mouth (Oral Phase) Your tongue
Feeding and Oral Hygiene: How to Address the Challenges
 Feeding and Oral Hygiene: How to Address the Challenges Paige W. Roberts, OTR/L Occupational Therapist Pediatric Feeding Disorders Program Marcus Autism Center Disclaimer: This content is for personal
Feeding and Oral Hygiene: How to Address the Challenges Paige W. Roberts, OTR/L Occupational Therapist Pediatric Feeding Disorders Program Marcus Autism Center Disclaimer: This content is for personal
MS Learn Online Feature Presentation Swallowing Difficulties in Multiple Sclerosis Featuring Patricia Bednarik, MS, CCC-SLP, MSCS
 Page 1 MS Learn Online Feature Presentation Swallowing Difficulties in Multiple Sclerosis Featuring, MS, CCC-SLP, MSCS >>Kate Milliken: Welcome to MS Learn Online. I am Kate Milliken. Swallowing is something
Page 1 MS Learn Online Feature Presentation Swallowing Difficulties in Multiple Sclerosis Featuring, MS, CCC-SLP, MSCS >>Kate Milliken: Welcome to MS Learn Online. I am Kate Milliken. Swallowing is something
Swallowing disorder, aspiration: now what?
 Swallowing disorder, aspiration: now what? Poster No.: C-0691 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Kavka, M. Kysilko, M. Rocek; Prague/CZ Keywords: Swallowing disorders, Dynamic swallowing
Swallowing disorder, aspiration: now what? Poster No.: C-0691 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Kavka, M. Kysilko, M. Rocek; Prague/CZ Keywords: Swallowing disorders, Dynamic swallowing
15/11/2011. Swallowing
 Swallowing Swallowing starts from placement of the food in the mouth and continues until food enters the stomach. Dysphagia: any difficulty in moving food from mouth to stomach. Pharynx is shared for both
Swallowing Swallowing starts from placement of the food in the mouth and continues until food enters the stomach. Dysphagia: any difficulty in moving food from mouth to stomach. Pharynx is shared for both
When Eating Becomes A Challenge Dysphagia
 When Eating Becomes A Challenge Dysphagia 1. DYSPHAGIA, WHAT IS IT? 2. IMPLICATIONS 3. ASSESSMENT 4. COMPENSATORY SWALLOWING AND EXERCISES 5. DIET TEXTURE ADJUSTMENTS Swallowing Dysfunction = Dysphagia
When Eating Becomes A Challenge Dysphagia 1. DYSPHAGIA, WHAT IS IT? 2. IMPLICATIONS 3. ASSESSMENT 4. COMPENSATORY SWALLOWING AND EXERCISES 5. DIET TEXTURE ADJUSTMENTS Swallowing Dysfunction = Dysphagia
Swallowing Disorders and Their Management in Patients with Multiple Sclerosis
 National Multiple Sclerosis Society 733 Third Avenue New York, NY 10017-3288 Clinical Bulletin Information for Health Professionals Swallowing Disorders and Their Management in Patients with Multiple Sclerosis
National Multiple Sclerosis Society 733 Third Avenue New York, NY 10017-3288 Clinical Bulletin Information for Health Professionals Swallowing Disorders and Their Management in Patients with Multiple Sclerosis
Daniels SK & Huckabee ML (2008). Dysphagia Following Stroke. Muscles of Deglutition. Lateral & Mesial Premotor Area 6. Primary Sensory
. Dysphagia Following Stroke. Muscles of Deglutition. Lateral & Mesial Premotor Area 6. Primary Sensory") An Overview of Dysphagia in the Stroke Population Stephanie K. Daniels, PhD Michael E. DeBakey VA Medical Center PM & R, Baylor College of Medicine Communication Sciences and Disorders, University of Houston
An Overview of Dysphagia in the Stroke Population Stephanie K. Daniels, PhD Michael E. DeBakey VA Medical Center PM & R, Baylor College of Medicine Communication Sciences and Disorders, University of Houston
Feeding and Swallowing Problems in the Child with Special Needs
 Feeding and Swallowing Problems in the Child with Special Needs Joan Surfus, OTR/L, SWC Amy Lynch, MS, OTR/L Misericordia University This presentation is made possible, in part, by the support of the American
Feeding and Swallowing Problems in the Child with Special Needs Joan Surfus, OTR/L, SWC Amy Lynch, MS, OTR/L Misericordia University This presentation is made possible, in part, by the support of the American
Standardisation of Videofluoroscopy: Where is it taking us?
 Standardisation of Videofluoroscopy: Where is it taking us? Jodi Allen, Senior Speech and Language Therapist, The National Hospital for Neurology and Neurosurgery If somebody asked you. What do you start
Standardisation of Videofluoroscopy: Where is it taking us? Jodi Allen, Senior Speech and Language Therapist, The National Hospital for Neurology and Neurosurgery If somebody asked you. What do you start
2013 Charleston Swallowing Conference
 Providing Quality Affordable Continuing Education and Treatment Materials for over 30 years. 2013 Charleston Swallowing Conference Session 9 Bedside Assessment: What Does It Tell You? 10:00 11:30 am Saturday,
Providing Quality Affordable Continuing Education and Treatment Materials for over 30 years. 2013 Charleston Swallowing Conference Session 9 Bedside Assessment: What Does It Tell You? 10:00 11:30 am Saturday,
RECOMMENDATIONS & UPDATES IN THE MANAGEMENT OF POST- STROKE DYSPHAGIA
 RECOMMENDATIONS & UPDATES IN THE MANAGEMENT OF POST- STROKE DYSPHAGIA Feeding in the Acute Stroke Period: - Early initiation of feeding is beneficial w/c decreases the risk of infections, improve survival
RECOMMENDATIONS & UPDATES IN THE MANAGEMENT OF POST- STROKE DYSPHAGIA Feeding in the Acute Stroke Period: - Early initiation of feeding is beneficial w/c decreases the risk of infections, improve survival
Review of dysphagia in poststroke
 Review of dysphagia in poststroke patients Danielle Thompson, Speech and Language Therapist Northwick Park Hospital With acknowledgement to Mary McFarlane, Principal Speech and Language Therapist, Acute
Review of dysphagia in poststroke patients Danielle Thompson, Speech and Language Therapist Northwick Park Hospital With acknowledgement to Mary McFarlane, Principal Speech and Language Therapist, Acute
Reluctance or refusal to feed or eat. Understanding Feeding Aversion in a City Full of Foodies. Presentation Outline. Learning Objectives
 Understanding Feeding Aversion in a City Full of Foodies Amy Houtrow, MD, MPH Pediatric Physical Medicine & Rehabilitation UCSF Department of Pediatrics June 2, 2007 Learning Objectives Learners will be
Understanding Feeding Aversion in a City Full of Foodies Amy Houtrow, MD, MPH Pediatric Physical Medicine & Rehabilitation UCSF Department of Pediatrics June 2, 2007 Learning Objectives Learners will be
EATING SAFELY AND TALKING ABOUT IT KIERA N BERGGREN, MA/CCC-SLP, MS 2018 FSHD CONNECT CONFERENCE
 EATING SAFELY AND TALKING ABOUT IT KIERA N BERGGREN, MA/CCC-SLP, MS 2018 FSHD CONNECT CONFERENCE DISCLOSURES I have no personal financial relationships with commercial interests relevant to this presentation
EATING SAFELY AND TALKING ABOUT IT KIERA N BERGGREN, MA/CCC-SLP, MS 2018 FSHD CONNECT CONFERENCE DISCLOSURES I have no personal financial relationships with commercial interests relevant to this presentation
Dysphagia and Swallowing. Jan Adams, DNP, MPA, RN and Karen Kern
 Dysphagia and Swallowing Jan Adams, DNP, MPA, RN and Karen Kern Scope of the Problem and Incidence 15 million people in the US have some form of Dysphagia. Every year, 1 million people are diagnosed with
Dysphagia and Swallowing Jan Adams, DNP, MPA, RN and Karen Kern Scope of the Problem and Incidence 15 million people in the US have some form of Dysphagia. Every year, 1 million people are diagnosed with
Speech and Language Therapy. Kerrie McCarthy Senior Speech and Language Therapist
 Speech and Language Therapy Kerrie McCarthy Senior Speech and Language Therapist Contents 1. Voice disorders 2. Swallow disorders 3. Videofluroscopy 4. Adult Acquired Communication Disorders 5. How to
Speech and Language Therapy Kerrie McCarthy Senior Speech and Language Therapist Contents 1. Voice disorders 2. Swallow disorders 3. Videofluroscopy 4. Adult Acquired Communication Disorders 5. How to
Applied physiology. 7- Apr- 15 Swallowing Course/ Anatomy and Physiology
 Applied physiology Temporal measures: Oral Transit Time (OTT) Pharyngeal Delay Time (PDT) Pharyngeal Transit Time (PTT) Oropharyngeal Swallowing Efficiency Score (OPSE score) 7- Apr- 15 Swallowing Course/
Applied physiology Temporal measures: Oral Transit Time (OTT) Pharyngeal Delay Time (PDT) Pharyngeal Transit Time (PTT) Oropharyngeal Swallowing Efficiency Score (OPSE score) 7- Apr- 15 Swallowing Course/
Dysphagia Identification and Management
 Dysphagia Identification and Management Presented By Speech-Language Pathologist Developmental Disabilities Administration DC Department on Disability Services Training Objectives After this training session
Dysphagia Identification and Management Presented By Speech-Language Pathologist Developmental Disabilities Administration DC Department on Disability Services Training Objectives After this training session
Dysphagia Management in TCP. Susan Smith and Vanessa Barkla Speech Pathologists, Ballarat Health Services May 2012
 Dysphagia Management in TCP Susan Smith and Vanessa Barkla Speech Pathologists, Ballarat Health Services May 2012 The role of the Speech Pathologist To assess swallowing status To provide management and
Dysphagia Management in TCP Susan Smith and Vanessa Barkla Speech Pathologists, Ballarat Health Services May 2012 The role of the Speech Pathologist To assess swallowing status To provide management and
DYSPHAGIA SCREENING and CLINICAL SWALLOW EVALUATIONS. Debra M. Suiter, Ph.D., CCC-SLP, BRS-S VA Medical Center-Memphis
 DYSPHAGIA SCREENING and CLINICAL SWALLOW EVALUATIONS Debra M. Suiter, Ph.D., CCC-SLP, BRS-S VA Medical Center-Memphis Suiter, ASHA, 2012 Diagnostic Tests vs. Screening Diagnostic tests are used when a
DYSPHAGIA SCREENING and CLINICAL SWALLOW EVALUATIONS Debra M. Suiter, Ph.D., CCC-SLP, BRS-S VA Medical Center-Memphis Suiter, ASHA, 2012 Diagnostic Tests vs. Screening Diagnostic tests are used when a
ESSD. EUGMS-ESSD Working Group on Oropharyngeal Dysphagia. 9 th Congress of the European Union Geriatric Medicine Society (EUGMS)
") ESSD EUGMS-ESSD Working Group on Oropharyngeal Dysphagia 9 th Congress of the European Union Geriatric Medicine Society (EUGMS) ESSD European Society for Swallowing Disorders (ESSD). ESSD Mission. The
ESSD EUGMS-ESSD Working Group on Oropharyngeal Dysphagia 9 th Congress of the European Union Geriatric Medicine Society (EUGMS) ESSD European Society for Swallowing Disorders (ESSD). ESSD Mission. The
Management of oropharyngeal dysphagia
 Management of oropharyngeal dysphagia Course Objectives Know the normal anatomy of swallowing Know the normal physiology of swallowing Enumerate different etiologies of oropharyngeal dysphagia Be able
Management of oropharyngeal dysphagia Course Objectives Know the normal anatomy of swallowing Know the normal physiology of swallowing Enumerate different etiologies of oropharyngeal dysphagia Be able
Communication and Swallowing with PSP/CBD. Megan DePuy, MBA, MS, CCC-SLP Private Speech Pathologist
 Communication and Swallowing with PSP/CBD Megan DePuy, MBA, MS, CCC-SLP Private Speech Pathologist A Speech Therapist? Why? Swallowing (Dysphagia) Speech (Dysarthria, Dysphonia) Language (Aphasia) An Experienced
Communication and Swallowing with PSP/CBD Megan DePuy, MBA, MS, CCC-SLP Private Speech Pathologist A Speech Therapist? Why? Swallowing (Dysphagia) Speech (Dysarthria, Dysphonia) Language (Aphasia) An Experienced
Assessing the Eating Needs of Personal Care Services (PCS) Beneficiaries Effective 12/1/2016
 Beneficiaries Effective 12/1/2016") Assessing the Eating Needs of Personal Care Services (PCS) Beneficiaries Effective 12/1/2016 The Freedom to Succeed November 22,2016 Content Introduction Signs and Symptoms Caring for Individuals with
Assessing the Eating Needs of Personal Care Services (PCS) Beneficiaries Effective 12/1/2016 The Freedom to Succeed November 22,2016 Content Introduction Signs and Symptoms Caring for Individuals with
Normal and Abnormal Oral and Pharyngeal Swallow. Complications.
 ESPEN Congress Gothenburg 2011 Assessment and treatment of dysphagia What is the evidence? Normal and Abnormal Oral and Pharyngeal Swallow. Complications. Pere Clavé Educational Session. Assessment and
ESPEN Congress Gothenburg 2011 Assessment and treatment of dysphagia What is the evidence? Normal and Abnormal Oral and Pharyngeal Swallow. Complications. Pere Clavé Educational Session. Assessment and
The Clinical Swallow Evaluation: What it can and cannot tell us. Introduction
 The Clinical Swallow Evaluation: What it can and cannot tell us Debra M. Suiter, Ph.D., CCC-SLP, BCS-S Director, Voice & Swallow Clinic Associate Professor, Division of Communication Sciences & Disorders
The Clinical Swallow Evaluation: What it can and cannot tell us Debra M. Suiter, Ph.D., CCC-SLP, BCS-S Director, Voice & Swallow Clinic Associate Professor, Division of Communication Sciences & Disorders
11/10/11. Memorie M. Gosa, M.S. CCC-SLP, BRS-S Senior Speech-Language Pathologist/ PhD Candidate LeBonheur Children s Hospital/ University of Memphis
 Memorie M. Gosa, M.S. CCC-SLP, BRS-S Senior Speech-Language Pathologist/ PhD Candidate LeBonheur Children s Hospital/ University of Memphis Developed an 8 point interval scale to describe penetration &
Memorie M. Gosa, M.S. CCC-SLP, BRS-S Senior Speech-Language Pathologist/ PhD Candidate LeBonheur Children s Hospital/ University of Memphis Developed an 8 point interval scale to describe penetration &
Pediatric Fiberoptic Endoscopic Evaluation of Swallowing (FEES) When, Where, How, & Who?
 When, Where, How, & Who?") Pediatric Fiberoptic Endoscopic Evaluation of Swallowing (FEES) When, Where, How, & Who? Claire Kane Miller, PhD CCC/SLP, BRS-S J. Paul Willging, MD Professor, Pediatric Otolaryngology, Head and Neck Surgery
Pediatric Fiberoptic Endoscopic Evaluation of Swallowing (FEES) When, Where, How, & Who? Claire Kane Miller, PhD CCC/SLP, BRS-S J. Paul Willging, MD Professor, Pediatric Otolaryngology, Head and Neck Surgery
IVOR LEWIS Esophagogastrectomy
 IVOR LEWIS Esophagogastrectomy SPEECH-LANGUAGE PATHOLOGY S ROLE MAGGIE BOYD, MS, CCC/SLP Biography Maggie Boyd, MS, CCC-SLP is a dysphagia clinical specialist at UAB hospital. She has 14 years clinical
IVOR LEWIS Esophagogastrectomy SPEECH-LANGUAGE PATHOLOGY S ROLE MAGGIE BOYD, MS, CCC/SLP Biography Maggie Boyd, MS, CCC-SLP is a dysphagia clinical specialist at UAB hospital. She has 14 years clinical
Swallow Function: Passy-Muir Valve Use for Evaluation & Rehabilitation David A. Muir Course Outline Physiology of Swallow
 Swallow Function: Passy-Muir Valve Use for Evaluation & Rehabilitation Mary Spremulli, MA, CCC-SLP Passy-Muir Clinical Consultant spre713@hotmail.com (949) 833-8255 David A. Muir 23 year-old ventilator
Swallow Function: Passy-Muir Valve Use for Evaluation & Rehabilitation Mary Spremulli, MA, CCC-SLP Passy-Muir Clinical Consultant spre713@hotmail.com (949) 833-8255 David A. Muir 23 year-old ventilator
Speech and Language Therapy Guidelines for Practitioner Led Videofluoroscopy Service. Contents
 Speech and Language Therapy Guidelines for Practitioner Led Classification: Clinical Guidelines Lead Author: Laura O Shea AHP Lead for Adult SLT Additional author(s): Lisa Lyon Senior Radiographer Authors
Speech and Language Therapy Guidelines for Practitioner Led Classification: Clinical Guidelines Lead Author: Laura O Shea AHP Lead for Adult SLT Additional author(s): Lisa Lyon Senior Radiographer Authors
Safe swallowing strategies
 Learning Guide Safe swallowing strategies 27468 Apply safe swallowing strategies in a health or wellbeing setting Level 3 5 credits Name: Workplace: Issue 2.0 Copyright 2017 Careerforce All rights reserved.
Learning Guide Safe swallowing strategies 27468 Apply safe swallowing strategies in a health or wellbeing setting Level 3 5 credits Name: Workplace: Issue 2.0 Copyright 2017 Careerforce All rights reserved.
Anatomical and Physiological Changes Due to Growth. The ABCs of Pediatric Dysphagia: Evaluation & Treatment
 The ABCs of Pediatric Dysphagia: Evaluation & Treatment Rima I. Polikaitis, MA, CCC-SLP Michele Wesling, MA, CCC-SLP Marianjoy Rehabilitation Hospital Wheaton, IL Anatomical and Physiological Changes Due
The ABCs of Pediatric Dysphagia: Evaluation & Treatment Rima I. Polikaitis, MA, CCC-SLP Michele Wesling, MA, CCC-SLP Marianjoy Rehabilitation Hospital Wheaton, IL Anatomical and Physiological Changes Due
Dysphagia as a Geriatric Syndrome Assessment and Treatment. Ashton Galyen M.A., CCC-SLP St. Vincent Indianapolis Acute Rehabilitation Unit
 Dysphagia as a Geriatric Syndrome Assessment and Treatment Ashton Galyen M.A., CCC-SLP St. Vincent Indianapolis Acute Rehabilitation Unit March 16, 2018 Ashton Galyen, M.A., CCC-SLP Master s degree in
Dysphagia as a Geriatric Syndrome Assessment and Treatment Ashton Galyen M.A., CCC-SLP St. Vincent Indianapolis Acute Rehabilitation Unit March 16, 2018 Ashton Galyen, M.A., CCC-SLP Master s degree in
Oral care & swallowing
 Oral care & swallowing Oral care is important as it has a role to play in preventing healthcare associated infections. Dental plaque and the oropharynx can become colonized by bacteria and a biofilm can
Oral care & swallowing Oral care is important as it has a role to play in preventing healthcare associated infections. Dental plaque and the oropharynx can become colonized by bacteria and a biofilm can
Respiratory Swallow Coordination in Healthy Individuals
 Cloud Publications International Journal of Advanced Speech and Hearing Research 2012, Volume 1, Issue 1, pp. 1-9, Article ID Med-03 Research Article Open Access Respiratory Swallow Coordination in Healthy
Cloud Publications International Journal of Advanced Speech and Hearing Research 2012, Volume 1, Issue 1, pp. 1-9, Article ID Med-03 Research Article Open Access Respiratory Swallow Coordination in Healthy
DYSPHAGIA MANAGEMENT IN ACUTE CARE AMANDA HEREFORD, MA, CCC- SLP
 DYSPHAGIA MANAGEMENT IN ACUTE CARE AMANDA HEREFORD, MA, CCC- SLP OVERVIEW Decision making re: swallowing in the medically compromised patient Swallow evaluation vs. Nursing Swallow Screening Instrumental
DYSPHAGIA MANAGEMENT IN ACUTE CARE AMANDA HEREFORD, MA, CCC- SLP OVERVIEW Decision making re: swallowing in the medically compromised patient Swallow evaluation vs. Nursing Swallow Screening Instrumental
Swallowing after a Total Laryngectomy
 Swallowing after a Total Laryngectomy Diane Longnecker, M.S.,CCC-SLP, BCS-S Baylor Institute for Rehabilitation at Baylor University Medical Center Dallas, TX Disclosure Statement No relevant financial
Swallowing after a Total Laryngectomy Diane Longnecker, M.S.,CCC-SLP, BCS-S Baylor Institute for Rehabilitation at Baylor University Medical Center Dallas, TX Disclosure Statement No relevant financial
Respiratory Compromise and Swallowing
 Speech Pathology and Respiratory Care April 11, 2013 By Angela Parcaro-Tucker, MA, CCC-SLP, LSVT How can Speech Therapy help? 1 Respiratory Compromise and Swallowing Swallowing is a complex sequence of
Speech Pathology and Respiratory Care April 11, 2013 By Angela Parcaro-Tucker, MA, CCC-SLP, LSVT How can Speech Therapy help? 1 Respiratory Compromise and Swallowing Swallowing is a complex sequence of
Workbook. Apply safe swallowing strategies as a health assistant in an aged care, health or disability context. US Level 4 Credits 4. Name...
 Workbook Apply safe swallowing strategies as a health assistant in an aged care, health or disability context US 27468 Level 4 Credits 4 Name... US 27468 Level 4 Credits 4 All rights reserved. Careerforce
Workbook Apply safe swallowing strategies as a health assistant in an aged care, health or disability context US 27468 Level 4 Credits 4 Name... US 27468 Level 4 Credits 4 All rights reserved. Careerforce
Radiation Therapy to the Head and Neck: What You Need to Know About Swallowing
 PATIENT & CAREGIVER EDUCATION Radiation Therapy to the Head and Neck: What You Need to Know About Swallowing This information describes swallowing problems that can be caused by radiation therapy to the
PATIENT & CAREGIVER EDUCATION Radiation Therapy to the Head and Neck: What You Need to Know About Swallowing This information describes swallowing problems that can be caused by radiation therapy to the
HOMES AND SENIORS SERVICES. APPROVAL DATE: August 1985 REVISION DATE: January 2015 REVIEW DATE: May 2018
 POLICY: Page 1 of 10 Residents who experience signs and symptoms associated with dysphagia will have their nutrition and hydration needs met in a safe, coordinated manner as managed by the interdisciplinary
POLICY: Page 1 of 10 Residents who experience signs and symptoms associated with dysphagia will have their nutrition and hydration needs met in a safe, coordinated manner as managed by the interdisciplinary
Examination of Swallowing Varies Depending on Food Types
 Tohoku J. Exp. Med., 2010, 220, 41-46 The Risk of Penetration or Aspiration during VF 41 The Risk of Penetration or Aspiration during Videofluoroscopic Examination of Swallowing Varies Depending on Food
Tohoku J. Exp. Med., 2010, 220, 41-46 The Risk of Penetration or Aspiration during VF 41 The Risk of Penetration or Aspiration during Videofluoroscopic Examination of Swallowing Varies Depending on Food
Managing the Patient with Dysphagia
 Managing the Patient with Dysphagia Patricia K. Lerner, MA, CCC, ASHA Fellow Board Certified Specialist in Swallowing & Swallowing Disorders Clinical Assistant Professor New York University School of Medicine
Managing the Patient with Dysphagia Patricia K. Lerner, MA, CCC, ASHA Fellow Board Certified Specialist in Swallowing & Swallowing Disorders Clinical Assistant Professor New York University School of Medicine
New Evidence-Based Support of a 3 Ounce Water Swallow Challenge Protocol
 New Evidence-Based Support of a 3 Ounce Water Swallow Challenge Protocol Steven B. Leder, Ph.D. Yale University School of Medicine New Haven, Connecticut Debra M. Suiter, Ph.D. VA Medical Center-Memphis
New Evidence-Based Support of a 3 Ounce Water Swallow Challenge Protocol Steven B. Leder, Ph.D. Yale University School of Medicine New Haven, Connecticut Debra M. Suiter, Ph.D. VA Medical Center-Memphis
FEEDING THE MEDICAL COMPLEX PEDIATRIC PATIENT. Brenda Sitzmann, MA, CCC-SLP (816)
") FEEDING THE MEDICAL COMPLEX PEDIATRIC PATIENT Brenda Sitzmann, MA, CCC-SLP bksitzmann@cmh.edu (816) 302-8037 DISCLOSURES Ms. Sitzmann is speech-language pathologist at Children s Mercy for which she receives
FEEDING THE MEDICAL COMPLEX PEDIATRIC PATIENT Brenda Sitzmann, MA, CCC-SLP bksitzmann@cmh.edu (816) 302-8037 DISCLOSURES Ms. Sitzmann is speech-language pathologist at Children s Mercy for which she receives
Dysphagia Treatment: What are We Doing, and Why?
 Dysphagia Treatment: What are We Doing, and Why? ASHA Convention, 2014; Orlando James L. Coyle, Ph.D., CCC SLP, BCS S University of Pittsburgh jcoyle@pitt.edu 1 Treatment 2 Aims, targets and ingredients
Dysphagia Treatment: What are We Doing, and Why? ASHA Convention, 2014; Orlando James L. Coyle, Ph.D., CCC SLP, BCS S University of Pittsburgh jcoyle@pitt.edu 1 Treatment 2 Aims, targets and ingredients
Feeding Evaluation Case History Form
 Feeding Evaluation Case History Form Child s Name: Date of Birth: Current Age: Person Completing Form & Relationship to patient: Date: The following information will be read by the therapist who is performing
Feeding Evaluation Case History Form Child s Name: Date of Birth: Current Age: Person Completing Form & Relationship to patient: Date: The following information will be read by the therapist who is performing
Ancillary care team (nursing, therapists, etc):
:") 1 A. Preliminary Information Reason for referral: Chronological age (Adjusted age): Primary caregiver: Informant for evaluation: Primary language: Interpreter Family concerns Barriers to learning: B. Background
1 A. Preliminary Information Reason for referral: Chronological age (Adjusted age): Primary caregiver: Informant for evaluation: Primary language: Interpreter Family concerns Barriers to learning: B. Background
SILENT ASPIRATION AND SWALLOWING PHYSIOLOGY AFTER RADIOTHERAPY IN PATIENTS WITH NASOPHARYNGEAL CARCINOMA
 ORIGINAL ARTICLE SILENT ASPIRATION AND SWALLOWING PHYSIOLOGY AFTER RADIOTHERAPY IN PATIENTS WITH NASOPHARYNGEAL CARCINOMA Louisa K. Y. Ng, MSc, 1 Kathy Y. S. Lee, PhD, 1 Sung Nok Chiu, Dr.rer.nat., 2 Peter
ORIGINAL ARTICLE SILENT ASPIRATION AND SWALLOWING PHYSIOLOGY AFTER RADIOTHERAPY IN PATIENTS WITH NASOPHARYNGEAL CARCINOMA Louisa K. Y. Ng, MSc, 1 Kathy Y. S. Lee, PhD, 1 Sung Nok Chiu, Dr.rer.nat., 2 Peter
Non-Oral Feedings. Disclosures. Feeding the Medical Complex Pediatric Patient. Pediatric Feeding Disorder. Overview.
 Feeding the Medical Complex Pediatric Patient Brenda Sitzmann, MA, CCC-SLP bksitzmann@cmh.edu (816) 302-8037 Disclosures Ms. Sitzmann is speech-language pathologist at Children s Mercy for which she receives
Feeding the Medical Complex Pediatric Patient Brenda Sitzmann, MA, CCC-SLP bksitzmann@cmh.edu (816) 302-8037 Disclosures Ms. Sitzmann is speech-language pathologist at Children s Mercy for which she receives
Critical Review: Is a chin-down posture more effective than thickened liquids in eliminating aspiration for patients with Parkinson s disease?
 Critical Review: Is a chin-down posture more effective than thickened liquids in eliminating aspiration for patients with Parkinson s disease? Nadia Torrieri, M.Cl.Sc. (SLP) Candidate The Unversity of
Critical Review: Is a chin-down posture more effective than thickened liquids in eliminating aspiration for patients with Parkinson s disease? Nadia Torrieri, M.Cl.Sc. (SLP) Candidate The Unversity of
SUPER-SUPRAGLOTTIC SWALLOW IN IRRADIATED HEAD AND NECK CANCER PATIENTS
 SUPER-SUPRAGLOTTIC SWALLOW IN IRRADIATED HEAD AND NECK CANCER PATIENTS Jeri A. Logemann, PhD, 1 Barbara Roa Pauloski, PhD, 1 Alfred W. Rademaker, PhD, 2 Laura A. Colangelo, MS 2 1 Department of Communication
SUPER-SUPRAGLOTTIC SWALLOW IN IRRADIATED HEAD AND NECK CANCER PATIENTS Jeri A. Logemann, PhD, 1 Barbara Roa Pauloski, PhD, 1 Alfred W. Rademaker, PhD, 2 Laura A. Colangelo, MS 2 1 Department of Communication
What are the Challenges? Spreading the Word in NICU. Need for NICU Care: Impact. Baby Trachs: Use of the Passy Muir Valve in the NICU to
 What are the Challenges? Baby Trachs: Use of the Passy Muir Valve in the NICU to Optimize Swallowing and Feeding Catherine S Shaker, MS/CCC SLP, BRS S and Cari Mutnick, MS/CCC SLP Florida Hospital for
What are the Challenges? Baby Trachs: Use of the Passy Muir Valve in the NICU to Optimize Swallowing and Feeding Catherine S Shaker, MS/CCC SLP, BRS S and Cari Mutnick, MS/CCC SLP Florida Hospital for
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/32744 holds various files of this Leiden University dissertation Author: Heemskerk, Anne-Wil Title: Dysphagia in Huntington s disease Issue Date: 2015-04-15
Cover Page The handle http://hdl.handle.net/1887/32744 holds various files of this Leiden University dissertation Author: Heemskerk, Anne-Wil Title: Dysphagia in Huntington s disease Issue Date: 2015-04-15
Validation of the Yale Swallow Protocol: A Prospective Double-Blinded Videofluoroscopic Study
 Dysphagia (2014) 29:199 203 DOI 10.1007/s00455-013-9488-3 ORIGINAL ARTICLE Validation of the Yale Swallow Protocol: A Prospective Double-Blinded Videofluoroscopic Study Debra M. Suiter JoAnna Sloggy Steven
Dysphagia (2014) 29:199 203 DOI 10.1007/s00455-013-9488-3 ORIGINAL ARTICLE Validation of the Yale Swallow Protocol: A Prospective Double-Blinded Videofluoroscopic Study Debra M. Suiter JoAnna Sloggy Steven
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP. Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D.
 A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
10/26/2017. Diagnostic Tests vs. Screening. Dysphagia Screening: What it is and what it is not
 Dysphagia Screening: What it is and what it is not Debra M. Suiter, Ph.D., CCC-SLP, BCS-S Director University of Kentucky Voice & Swallow Clinic Lexington, Kentucky ASHA's Preferred Practice Pattern on
Dysphagia Screening: What it is and what it is not Debra M. Suiter, Ph.D., CCC-SLP, BCS-S Director University of Kentucky Voice & Swallow Clinic Lexington, Kentucky ASHA's Preferred Practice Pattern on
Dysphagia and the MBSS: Disclosures. Instrumental Assessment. The Disorder Guides the Treatment
 Dysphagia and the MBSS: The Disorder Guides the Treatment Jennifer Jones, PhD, CCC-SLP, BCS-S C/NDT Board Certified Specialist in Swallowing and Swallowing Disorders Certified in Neurodevelopmental Treatment
Dysphagia and the MBSS: The Disorder Guides the Treatment Jennifer Jones, PhD, CCC-SLP, BCS-S C/NDT Board Certified Specialist in Swallowing and Swallowing Disorders Certified in Neurodevelopmental Treatment
Videofluoroscopic swallowing exam: Technique, imaging findings and clinical implications.
 Videofluoroscopic swallowing exam: Technique, imaging findings and clinical implications. Poster No.: C-2088 Congress: ECR 2015 Type: Educational Exhibit Authors: L. Anton Mendez, A. M. Ibañez Zubiarrain,
Videofluoroscopic swallowing exam: Technique, imaging findings and clinical implications. Poster No.: C-2088 Congress: ECR 2015 Type: Educational Exhibit Authors: L. Anton Mendez, A. M. Ibañez Zubiarrain,
Dysphagia and Self Feeding in Acute Tetraplegia
 Dysphagia and Self Feeding in Acute Tetraplegia Danielle R. Karhut, OTR/L Robert Masterson, MS, CCC-SLP Spinal Cord Rehabilitation Unit UPMC Mercy Hospital/Centers for Rehab Services Pittsburgh, PA Tetraplegia
Dysphagia and Self Feeding in Acute Tetraplegia Danielle R. Karhut, OTR/L Robert Masterson, MS, CCC-SLP Spinal Cord Rehabilitation Unit UPMC Mercy Hospital/Centers for Rehab Services Pittsburgh, PA Tetraplegia
COMMUNICATION. Communication and Swallowing post Tracheostomy. Role of SLT. Impact of Tracheostomy. Normal Speech. Facilitating Communication
 Communication and Swallowing post Tracheostomy. Role of SLT 1. 2. 3. Management of communication needs. Management of swallowing issues. Working with the multidisciplinary team to facilitate weaning. Impact
Communication and Swallowing post Tracheostomy. Role of SLT 1. 2. 3. Management of communication needs. Management of swallowing issues. Working with the multidisciplinary team to facilitate weaning. Impact
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Swallowing problems. Patient information. Name: Date: Speech and Language Therapist: Reviewed: May 2016 Next review: June 2017 Version 1
 Patient information Swallowing problems Name: Date: Speech and Language Therapist: Golden Jubilee National Hospital Agamemnon Street Clydebank, G81 4DY (: 0141 951 5000 www.nhsgoldenjubilee.co.uk Reviewed:
Patient information Swallowing problems Name: Date: Speech and Language Therapist: Golden Jubilee National Hospital Agamemnon Street Clydebank, G81 4DY (: 0141 951 5000 www.nhsgoldenjubilee.co.uk Reviewed:
Dysphagia Diagnostic Procedures
 The Role of Lingual Pressures In Dysphagia Screening Andrew Kaufman, BS Jackie Hind, MS Georgia Malandraki, PhD JoAnne Robbins, PhD American Speech Language Hearing Association Annual Meeting New Orleans,
The Role of Lingual Pressures In Dysphagia Screening Andrew Kaufman, BS Jackie Hind, MS Georgia Malandraki, PhD JoAnne Robbins, PhD American Speech Language Hearing Association Annual Meeting New Orleans,
Tracheoesophageal Fistula and Esophageal Atresia
 Patient and Family Education Tracheoesophageal Fistula and Esophageal Atresia What is tracheoesophageal fistula? The word fistula means abnormal connection. Tracheoesophageal fistula (TEF) is a condition
Patient and Family Education Tracheoesophageal Fistula and Esophageal Atresia What is tracheoesophageal fistula? The word fistula means abnormal connection. Tracheoesophageal fistula (TEF) is a condition
Pharyngeal Effects of Bolus Volume, Viscosity, and Temperature in Patients With Dysphagia Resulting From Neurologic Impairment and in Normal Subjects
 Journal of Speech and Hearing Research, Volume 37, 1041-1049, October 1994 Pharyngeal Effects of Bolus Volume, Viscosity, and Temperature in Patients With Dysphagia Resulting From Neurologic Impairment
Journal of Speech and Hearing Research, Volume 37, 1041-1049, October 1994 Pharyngeal Effects of Bolus Volume, Viscosity, and Temperature in Patients With Dysphagia Resulting From Neurologic Impairment
Speech and Swallowing in KD: Soup to Nuts. Neil C. Porter, M.D. Assistant Professor of Neurology University of Maryland
 Speech and Swallowing in KD: Soup to Nuts Neil C. Porter, M.D. Assistant Professor of Neurology University of Maryland Disclosures I will not be speaking on off-label use of medications I have no relevant
Speech and Swallowing in KD: Soup to Nuts Neil C. Porter, M.D. Assistant Professor of Neurology University of Maryland Disclosures I will not be speaking on off-label use of medications I have no relevant
TREATMENT OF DYSPHAGIA IN PATIENTS AFTER STROKE IN ESTONIA
 TREATMENT OF DYSPHAGIA IN PATIENTS AFTER STROKE IN ESTONIA ANNE URIKO SPORTS MEDICINE AND REHABILITATION CLINIG OF TARTU UNIVERSITY HOSPITAL 17.09.2010 DYSPHAGIA DIFFICULTY MOVING FOOD FROM MOUTH TO STOMACH
TREATMENT OF DYSPHAGIA IN PATIENTS AFTER STROKE IN ESTONIA ANNE URIKO SPORTS MEDICINE AND REHABILITATION CLINIG OF TARTU UNIVERSITY HOSPITAL 17.09.2010 DYSPHAGIA DIFFICULTY MOVING FOOD FROM MOUTH TO STOMACH
Department of Pediatric Otolarygnology. ENT Specialty Programs
 Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Anterior Cervical Fusion: What is the Effect on Swallow Function?
 Anterior Cervical Fusion: What is the Effect on Swallow Function? Rebecca L. Gould, MSC, CCC-SLP, BRS-S rebec26050@aol.com (561) 833-2090 www.med-speech.com STATE OF THE ART EVALUATION Anterior Cervical
Anterior Cervical Fusion: What is the Effect on Swallow Function? Rebecca L. Gould, MSC, CCC-SLP, BRS-S rebec26050@aol.com (561) 833-2090 www.med-speech.com STATE OF THE ART EVALUATION Anterior Cervical
When Swallowing Becomes Impossible
 University of Tennessee, Knoxville Trace: Tennessee Research and Creative Exchange University of Tennessee Honors Thesis Projects University of Tennessee Honors Program 5-2011 When Swallowing Becomes Impossible
University of Tennessee, Knoxville Trace: Tennessee Research and Creative Exchange University of Tennessee Honors Thesis Projects University of Tennessee Honors Program 5-2011 When Swallowing Becomes Impossible
COLLABORATION WITH OT IN TREATMENT OF DYSPHAGIA IN SEVERE DEMENTIA
 COLLABORATION WITH OT IN TREATMENT OF DYSPHAGIA IN SEVERE DEMENTIA Bob LeJeune; M.A., CCC SLP Progressive Step Rehab Sharon Kurfuerst; Ed.D.; OTR/L Christiana Health Services Dementia Defined The American
COLLABORATION WITH OT IN TREATMENT OF DYSPHAGIA IN SEVERE DEMENTIA Bob LeJeune; M.A., CCC SLP Progressive Step Rehab Sharon Kurfuerst; Ed.D.; OTR/L Christiana Health Services Dementia Defined The American
Chapter 19. Nutrition and Fluids. All items and derived items 2015, 2011 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved.
 Chapter 19 Nutrition and Fluids Nutrition Nutrition--processes involved in the ingestion, digestion, absorption & use of foods & fluids by the body. The person s diet affects physical & mental wellbeing
Chapter 19 Nutrition and Fluids Nutrition Nutrition--processes involved in the ingestion, digestion, absorption & use of foods & fluids by the body. The person s diet affects physical & mental wellbeing
B. Background Information B1. Summary Medical team (physicians, dentists, etc ): Ancillary care team (nursing, therapists, etc ):
: Ancillary care team (nursing, therapists, etc ):") 1 A. Preliminary Information Reason for referral: Chronological age (Adjusted age): Primary caregiver: Informant for evaluation: Primary language: Interpreter Family concerns Barriers to learning: B. Background
1 A. Preliminary Information Reason for referral: Chronological age (Adjusted age): Primary caregiver: Informant for evaluation: Primary language: Interpreter Family concerns Barriers to learning: B. Background
Swallow-respiratory coordination. Liza Bergström, Leg. logoped.
 Swallow-respiratory coordination Liza Bergström, Leg. logoped. Biological timeshare When we breathe, we don t swallow When we swallow, we don t breathe Body will always choose to breathe over anything
Swallow-respiratory coordination Liza Bergström, Leg. logoped. Biological timeshare When we breathe, we don t swallow When we swallow, we don t breathe Body will always choose to breathe over anything
Swallowing Strategies
 Department of Head and Neck Surgery Section of Speech Pathology & Audiology M.D. Anderson Cancer Center (713) 792-6525 Swallowing Strategies 1) POSTURAL CHANGES: a) Chin Tuck: (1) Delayed onset pharyngeal
Department of Head and Neck Surgery Section of Speech Pathology & Audiology M.D. Anderson Cancer Center (713) 792-6525 Swallowing Strategies 1) POSTURAL CHANGES: a) Chin Tuck: (1) Delayed onset pharyngeal
Stage Transition And Laryngeal Closure In Poststroke Patients With Dysphagia
 Archived version from NCDOCKS Institutional Repository http://libres.uncg.edu/ir/asu/ Stage Transition And Laryngeal Closure In Poststroke Patients With Dysphagia By: Elizabeth Rachel Oommen Youngsun Kim
Archived version from NCDOCKS Institutional Repository http://libres.uncg.edu/ir/asu/ Stage Transition And Laryngeal Closure In Poststroke Patients With Dysphagia By: Elizabeth Rachel Oommen Youngsun Kim
Dysphagia Questionnaire. Referring Doctor:
 Dysphagia Questionnaire Name: Date of Birth: Address: Referring Doctor: Diagnosis: Phone number: Email: What are your complaints regarding your swallowing: Date and onset of swallowing problems: Please
Dysphagia Questionnaire Name: Date of Birth: Address: Referring Doctor: Diagnosis: Phone number: Email: What are your complaints regarding your swallowing: Date and onset of swallowing problems: Please
Complex Decision Making in Pediatric Dysphagia
 Complex Decision Making in Pediatric Dysphagia Alana Lowry, MS, CCC-SLP Fletcher Allen Health Care Kara Fletcher Larson, MS, CCC-SLP Jennifer Miller, MS, CCC-SLP Children s s Hospital Boston ASHA November
Complex Decision Making in Pediatric Dysphagia Alana Lowry, MS, CCC-SLP Fletcher Allen Health Care Kara Fletcher Larson, MS, CCC-SLP Jennifer Miller, MS, CCC-SLP Children s s Hospital Boston ASHA November
Swallow Study and the Laryngectomy Patient Long Term Dysphagia after Treatment for Head and Neck Cancer
 Swallow Study and the Laryngectomy Patient Long Term Dysphagia after Treatment for Head and Neck Cancer Angela Campanelli, MS, CCC SLP Board Certified Specialist in Swallowing and Swallowing Disorders
Swallow Study and the Laryngectomy Patient Long Term Dysphagia after Treatment for Head and Neck Cancer Angela Campanelli, MS, CCC SLP Board Certified Specialist in Swallowing and Swallowing Disorders
Palliative Care Swallowing Management HEATHER STORIE M.S.,CCC-SLP, BCS-S SPEECH LANGUAGE PATHOLOGY, BOARD CERTIFIED SWALLOWING SPECIALIST
 Palliative Care Swallowing Management HEATHER STORIE M.S.,CCC-SLP, BCS-S SPEECH LANGUAGE PATHOLOGY, BOARD CERTIFIED SWALLOWING SPECIALIST Objectives Gain a general understanding of normal swallowing Gain
Palliative Care Swallowing Management HEATHER STORIE M.S.,CCC-SLP, BCS-S SPEECH LANGUAGE PATHOLOGY, BOARD CERTIFIED SWALLOWING SPECIALIST Objectives Gain a general understanding of normal swallowing Gain
Main Aspects of the Management of Neurogenic Dysphagia
 Main Aspects of the Management of Neurogenic Dysphagia Mario Prosiegel/München German Society of Neurology (DGN) prosiegel@t-online.de DYSPHAGIA October 8-10, 2015 Pavia, Italy Overview Diagnosis Causal
Main Aspects of the Management of Neurogenic Dysphagia Mario Prosiegel/München German Society of Neurology (DGN) prosiegel@t-online.de DYSPHAGIA October 8-10, 2015 Pavia, Italy Overview Diagnosis Causal
Videofluoroscopic Assessment of Patients with Dysphagia: Pharyngeal Retention Is a Predictive Factor for Aspiration
 Edith Eisenhuber 1 Wolfgang Schima Ewald Schober Peter Pokieser Alfred Stadler Martina Scharitzer Elisabeth Oschatz Received June 4, 2001; accepted after revision September 28, 2001. Presented at the annual
Edith Eisenhuber 1 Wolfgang Schima Ewald Schober Peter Pokieser Alfred Stadler Martina Scharitzer Elisabeth Oschatz Received June 4, 2001; accepted after revision September 28, 2001. Presented at the annual
TECHNICAL SKILLS COMPETENCY
 TECHNICAL SKILLS COMPETENCY Date Education Plan Knowledge Competencies 1. Demonstrates Understanding of rationale for performing FEES a) Identifies indications & contraindications for the procedure, MBS
TECHNICAL SKILLS COMPETENCY Date Education Plan Knowledge Competencies 1. Demonstrates Understanding of rationale for performing FEES a) Identifies indications & contraindications for the procedure, MBS
5 Things I Want You to Know About Dysphagia. Prof Maggie-Lee Huckabee The University of Canterbury Rose Centre for Stroke Recovery and Research
 5 Things I Want You to Know About Dysphagia Prof Maggie-Lee Huckabee The University of Canterbury Rose Centre for Stroke Recovery and Research 5 things 1) Why we can t diagnose dysphagia at bedside. 2)
5 Things I Want You to Know About Dysphagia Prof Maggie-Lee Huckabee The University of Canterbury Rose Centre for Stroke Recovery and Research 5 things 1) Why we can t diagnose dysphagia at bedside. 2)
2013 Charleston Swallowing Conference
 Providing Quality Affordable Continuing Education and Treatment Materials for over 30 years. 2013 Charleston Swallowing Conference Working Breakfast 7:30 8:00 am Saturday, Oct. 12, 2013 CE Seminars On-line
Providing Quality Affordable Continuing Education and Treatment Materials for over 30 years. 2013 Charleston Swallowing Conference Working Breakfast 7:30 8:00 am Saturday, Oct. 12, 2013 CE Seminars On-line
Disclosures. We have no relevant financial or conflicts of interest to disclose.
 Disclosures We have no relevant financial or conflicts of interest to disclose. We will discuss Current recommendations re: dysphagia screening. A brief review of dysphagia & aspiration including statistics,
Disclosures We have no relevant financial or conflicts of interest to disclose. We will discuss Current recommendations re: dysphagia screening. A brief review of dysphagia & aspiration including statistics,