Endocrine Emergencies: Recognition and Management
|
|
|
- Jonah Ford
- 5 years ago
- Views:
Transcription




1 Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address is 21 Prescot Street London, E1 8BB - Monday 11th September 2017
2 HYPONATRAEMIA 1-6% hospital admissions Na < 130 mmol/l 15-22% Na < 135 mmol/l
3 Hyponatraemia Dilutional Salt deficiency excess intake of water increased water re-absorption e.g, cirrhosis, CCF, nephrotic reduced renal excretion e.g., SIADH, steroid deficiency renal loss Pseudohyponatremia lipids non renal loss, e.g, GI tract protein
4 Features of hyponatreamia Dependant on rate of development and cause Develops if Na < 115 mmol/l or more rapidly if fall is rapid Na < 100 mmol/l is life threatening Features neurological confused headache seizures
5 Investigations Urinary sodium (greater or less than 20 mmol/l) Volume status needs assessing Others osmolality cortisol thyroid function liver biochemistry electrophoresis
6 SIADH More common in the elderly Diagnosis Na plasma osmolality (<270) Inappropriate urine osmolality (>100) Excessive renal loss > 30mmol/L Normal adrenal, thyroid function Investigate chest head Ellison & Ben (2007) NEJM 356: 2064
7 Challenges in the treatment of Cushing s disease Diagnosis - Do they have it? Where is it? Mortality/morbidity - infection - psychiatric - clotting tendency - diabetes - hypertension - obesity - osteoporosis

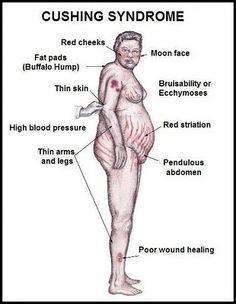
8 Cushing s disease
9 Causes of Cushing s syndrome Pseudo-Cushing s syndrome: Alcoholism <1% Severe depression 1% ACTH dependent: Pituitary adenoma 68% (Cushing s disease) Ectopic ACTH syndrome 12% (where is it?) Ectopic CRH syndrome <1% ACTH-independent: Adrenal adenoma 10% Adrenal carcinoma 8% Nodular (macro-or micro-) hyperplasia 1% Carney complex (skin pigmentation, myxomas endocrine tumours, e.g., nodular

10 Diagnosis of Cushing s

11 Differential Diagnosis of Cushing s
12 Phaeochromocytoma - who screened? Family history MEN II von Hippel Lindau neurofibromatosis Paroxysmal symptoms Hypertension Hypertension during anaesthetic induction Unexplained heart failure Adrenal incidentaloma 10% normotensive
13 Phaeochromocytoma blockade then β blockade blockade phenoxybenzamine or doxazosin 10mg twice daily to 20mg x 4 daily Β blockade - propranolol 20-80mg 8 hourly Aim BP 130/80 or less Lenders et al (2005) Lancet 366: 665 Jafri and Maher 2012 ESE 166: 151
14 Contraindicated drugs in Phaeochromocytoma β blockers D2 receptor antagonists Tricyclic antidepressants MAOI s Opioids
15 Background Addison s Disease Any form of stress in patients with adrenal insufficiency is a significant risk of adrenal crisis or even death Recommendation:- 100mg at induction 200mg per 24 hours by continuous infusion until end of peri-operative period then resume replacement in normal doses
16 Case History C.C. Aged 23 Weight loss 65 to 45kg Holiday in Borneo pigmented Vomiting Na 126 x 2 Not investigated
17 Case History C.C. Aged 23 Weight loss 65 to 45kg Holiday in Borneo pigmented Vomiting Na 126 x 2 Not investigated Died undiagnosed Addison's
18 Addison s disease Primary Prevalence /million Incidence /million in Caucasians Secondary Hypothalamo-pituitary disease Exogenous steroids > 5mg prednisolone > 1 month: - oral - inhaler - joint - steroid creams for eczema Congenital adrenal hyperplasia Post treatment of Cushing s Charmandari et al Lancet
19 Features of Addison s Anorexia & weight loss 100% Tiredness, weakness 100% Skin pigmentation 94% Postural hypotension 88-94% Abdominal pain Arthralgia Headache PUO 13% Salt craving 16%
20 Secondary vs. Primary No mineralocorticoid deficiency No pigmentation
21 Investigation Na (90%) (normocytic) K (65%) Cortisol ACTH Synacthen Anaemia Eosinophilia Mild-hypercalcaemia Adrenal suppression - Depot synacthen
22 Diagnosis of adrenal insufficiency Synacthen test 250mcg i.m/i.v. Measure cortisol at 30 peak > 600 nmol/l Any time of day
23 Prevalence of adrenal insufficiency 9 per 100,000 Adrenal crisis occurs 6-8 times per 100 years These can be fatal Patients on steroids 7 in 1,000
24 Features of impending Addisonian crisis Volume resistant hypotension Early - malaise somnolence cognitive dysfunction - postural hypotension - hponatraemia - pyrexia If in doubt give hydrocortisone In the short term - side effects are minimal
25 Treatment of Acute Adrenal Suppression BMJ 2012: 345 e6333
26 Emergency Management - Life threatening! Fluids several litres first 24 hours Hydrocortisone or + 100mg i.v. 100mg i.m then 6 hourly 200mg i.v. by continuous infusion/24 hours Not mineralocorticoid because xs glucocorticoid steroids Patients will die if inadequately treated
27 Patients on Steroids Prednisolone more than 5mg/day more than 1 month NB. Inhaled steroids dermatological steroids joint injected steroids All suppress the synacthen test
28 Steroid equivalent doses Hydrocortisone 10mg Prednisolone 2.5 mg Dexamethasone 0.4mg
29 Physiology 20mg of hydrocortisone released from adrenals daily Bound to cortisol binding proteins 95%- free 5%
30 Pathophysiology Primary (Addison s disease) - deficient in cortisol & aldosterone Secondary Congenital adrenal Hyperplasia: causing deficiency of cortisol** - deficient only in cortisol - enzyme deficiency - children and adults - need steroid cover
31 Hydrocortisone Minor - endoscopy 100mg i.m. before Moderate - hernia repair - 100mg i.m. 6 hourly/24 hours Major - open heart surgery - 100mg i.m 6 hourly/72 hours Then resume normal medication Major illness Hydrocortisone 100mg i.m. 6 hourly until illness resolved
32 Hypothyroidism Epidemiology 7.5% of females 2.5% of men > 65 years 1.7% overt hypothyroidism 13.7% subclinical hypothyroidism Oxford Handbook of Endocrinology 2014 Ed. Wass & Owen
33 Causes of Hypothyroidism Hashimoto s thyroiditis Post operative 131 Iodine Drugs e.g., amiodarone Pituitary/Hypothalamic disease Post partum De Quervain s
34 Subclinical Hypothyroidism Diagnosis TSH Normal T4 Repeat TSH twice Treat if + a/b past radioiodine TSH > 10 MU/L or less if symptoms
35 Treatment of Hypothyroidism mcg/kg/day Give am on fasting stomach Start mcg/day except elderly elderly mcg Increments 25 mcg at 4 weekly intervals TSH above normal and <2.5 mu/l Check annually T4 in hypopituitary patients
36 Myxodema Madness
Hormone replacement therapy in endocrinology 2014
 Hormone replacement therapy in endocrinology 2014 John Wass Department of Endocrinology, Oxford University, UK Academic Vice President, Royal College of Physicians, London ESA Clinical Weekend, Torquay,
Hormone replacement therapy in endocrinology 2014 John Wass Department of Endocrinology, Oxford University, UK Academic Vice President, Royal College of Physicians, London ESA Clinical Weekend, Torquay,
Clinical Guideline. SPEG MCN Protocols Sub Group SPEG Steering Group
 Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Hyponatraemia- Principles, Investigation and Management. Sirazum Choudhury Biochemistry
 Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
Hyponatraemia- Principles, Investigation and Management Sirazum Choudhury Biochemistry Contents Background Investigation Classification Normal Osmolality General management and SIADH Cases Background Relatively
Managing Addison s Disease
 Managing Addison s Disease Dr Charles R Buchanan Consultant Paediatric Endocrinologist Kings College Hospital, London Thomas Addison 1793-1860 Guy s Hospial Described Symptoms 1855 My experience 25 years
Managing Addison s Disease Dr Charles R Buchanan Consultant Paediatric Endocrinologist Kings College Hospital, London Thomas Addison 1793-1860 Guy s Hospial Described Symptoms 1855 My experience 25 years
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Audit of Adrenal Function Tests. Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK
 Audit of Adrenal Function Tests Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK Introduction Audit Overview of adrenal function tests Education Audit why? Explore
Audit of Adrenal Function Tests Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK Introduction Audit Overview of adrenal function tests Education Audit why? Explore
NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST: Clinical Chemistry Guidelines
 Adrenocortical Insufficiency Guideline Document Information Policy Reference: Adrenocortical Insufficiency Issue: 1: Version 3 Author Job Title: Peter Prinsloo Consultant in Chemical Pathology STATUS:
Adrenocortical Insufficiency Guideline Document Information Policy Reference: Adrenocortical Insufficiency Issue: 1: Version 3 Author Job Title: Peter Prinsloo Consultant in Chemical Pathology STATUS:
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT.
 HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
HYPONATRAEMIA: NUH GUIDELINE FOR INITIAL ASSESSMENT AND MANAGEMENT. HYPONATRAEMIA: SODIUM < 130 MMOL/L SIGNIFICANT. Symptoms/signs usually only occur when sodium < 125 mmol/l. Acute hyponatraemia is less
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Overview. Fluid & Electrolyte Disorders. Water distribution. Introduction 5/10/2014
 Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
Overview Fluid & Electrolyte Disorders Dr Nicola Barlow Clinical Biochemistry Department, City Hospital Introduction Fluid and electrolyte homeostasis Electrolyte disturbances Analytical parameters Methods
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management
 C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines
 Management of Hyponatraemia in Intensive Care Guidelines") Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
The analysis of Glucocorticoid Steroids in Plasma, Urine and Saliva by UPLC/MS/MS
 The analysis of Glucocorticoid Steroids in Plasma, Urine and Saliva by UPLC/MS/MS Brett McWhinney, Supervising Scientist, HPLC Section, Pathology Central, Pathology Queensland Overview 1. Overview of Pathology
The analysis of Glucocorticoid Steroids in Plasma, Urine and Saliva by UPLC/MS/MS Brett McWhinney, Supervising Scientist, HPLC Section, Pathology Central, Pathology Queensland Overview 1. Overview of Pathology
Assessing Adrenal Function in Ill, Hospitalized Patients. Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism
 Assessing Adrenal Function in Ill, Hospitalized Patients Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism Disclosures Very surprised when I received an email two weeks ago disclosing
Assessing Adrenal Function in Ill, Hospitalized Patients Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism Disclosures Very surprised when I received an email two weeks ago disclosing
Southern Derbyshire Shared Care Pathology Guidelines. Hyponatraemia in Adults
 Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Southern Derbyshire Shared Care Pathology Guidelines Hyponatraemia in Adults Purpose of Guideline The investigation and management of adult patients with newly diagnosed hyponatraemia. Hyponatraemia can
Adrenal Gland Disorders
 1 Adrenal Gland Disorders Adrenal cortex steroid hormones (corticosteroids) 1. Glucocorticoids Regulate metabolism and blood glucose Critical to physiologic stress response 2. Mineralocorticoids Regulate
1 Adrenal Gland Disorders Adrenal cortex steroid hormones (corticosteroids) 1. Glucocorticoids Regulate metabolism and blood glucose Critical to physiologic stress response 2. Mineralocorticoids Regulate
WARD INSTRUCTIONS WEBSITE
 DEPARTMENT OF CLINICAL CHEMISTRY NEW CROSS HOSPITAL WOLVERHAMPTON WARD INSTRUCTIONS WEBSITE Edition 1.1 SOP E1.120P.CHE Date issued: June 2016 Review interval: Authorised copy: Printed copies Author Location
DEPARTMENT OF CLINICAL CHEMISTRY NEW CROSS HOSPITAL WOLVERHAMPTON WARD INSTRUCTIONS WEBSITE Edition 1.1 SOP E1.120P.CHE Date issued: June 2016 Review interval: Authorised copy: Printed copies Author Location
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Southern Derbyshire Shared Care Pathology Guidelines. Secondary Hypertension
 Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Corticosteroids. Abdulmoein Al-Agha, FRCPCH Professor of Pediatric Endocrinology, King Abdulaziz University Hospital,
 Corticosteroids Abdulmoein Al-Agha, FRCPCH Professor of Pediatric Endocrinology, King Abdulaziz University Hospital, http://aagha.kau.edu.sa History 1855 Addison's disease 1856 Adrenal glands essential
Corticosteroids Abdulmoein Al-Agha, FRCPCH Professor of Pediatric Endocrinology, King Abdulaziz University Hospital, http://aagha.kau.edu.sa History 1855 Addison's disease 1856 Adrenal glands essential
Protocol for Hypoadrenalism / Addison s Disease
 Protocol for Hypoadrenalism / Addison s Disease Relevance This protocol is relevant to all diagnosing clinicians, ie GPs and Nurses. HCAs and other staff should be aware of the possible presenting symptoms
Protocol for Hypoadrenalism / Addison s Disease Relevance This protocol is relevant to all diagnosing clinicians, ie GPs and Nurses. HCAs and other staff should be aware of the possible presenting symptoms
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Hormones. Introduction to Endocrine Disorders. Hormone actions. Modulation of hormone levels. Modulation of hormone levels
 Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis
Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis
CPY 605 ADVANCED ENDOCRINOLOGY
 CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters. Dr James Ahlquist Endocrinologist Southend Hospital
 Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
Hyponatraemia: confident diagnosis, effective treatment and avoiding disasters Dr James Ahlquist Endocrinologist Southend Hospital Hyponatraemia: a common electrolyte disorder Electrolyte disorder Prevalence
W. Heath Giles, M.D. University of Tennessee College of Medicine Chattanooga Assistant Professor of Surgery Associate Residency Program Director
 W. Heath Giles, M.D. University of Tennessee College of Medicine Chattanooga Assistant Professor of Surgery Associate Residency Program Director It is our duty to each learner to honor your right to expect
W. Heath Giles, M.D. University of Tennessee College of Medicine Chattanooga Assistant Professor of Surgery Associate Residency Program Director It is our duty to each learner to honor your right to expect
ULTIMATE BEAUTY OF BIOCHEMISTRY. Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017
 ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
Adrenal gland consist of: Outer Cortex and Inner Medulla Hormones secreted by Adrenal Cortex are: Glucocorticoid, Mineralocorticoid and Sex Steroids
 1 UNIVERSITY OF PAPUA NEW GUINEA SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY PBL MBBS Year III; BMLS & BDS Year 3 ADRENAL
1 UNIVERSITY OF PAPUA NEW GUINEA SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY PBL MBBS Year III; BMLS & BDS Year 3 ADRENAL
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
ENDOCRINOLOGY 3. R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice
 Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
Subclinical Problems in the ICU:
 Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
Adrenal Incidentaloma Management
 Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal insufficiency 25/09/57
 Adrenal insufficiency นายแพทย อ ดมศ กด เล ศส ทธ พร โรงพยาบาลมหาราชนครราชส มา 25/09/57 Adrenal insufficiency Cause Primary VS secondary Acute VS Chronic Diagnosis Critically ill VS non-critically ill Treatment
Adrenal insufficiency นายแพทย อ ดมศ กด เล ศส ทธ พร โรงพยาบาลมหาราชนครราชส มา 25/09/57 Adrenal insufficiency Cause Primary VS secondary Acute VS Chronic Diagnosis Critically ill VS non-critically ill Treatment
Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia
 Precocious Puberty Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia Faculty Disclosure Faculty: Laura Stewart No relationships with
Precocious Puberty Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia Faculty Disclosure Faculty: Laura Stewart No relationships with
Adrenal insufficiency Recogni2on & Management. Prof. Simon Pearce
 Adrenal insufficiency Recogni2on & Management Prof. Simon Pearce Declara2on Received speaker fees from: Merck- Serono Shire Objec2ves Recognise Addison s disease Understand and treat adrenal crisis Raise
Adrenal insufficiency Recogni2on & Management Prof. Simon Pearce Declara2on Received speaker fees from: Merck- Serono Shire Objec2ves Recognise Addison s disease Understand and treat adrenal crisis Raise
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
What is the best thing to do or say in the Emergency Room to make sure the ER staff knows how to treat me if I am in a crisis??
 What is the best thing to do or say in the Emergency Room to make sure the ER staff knows how to treat me if I am in a crisis?? APRIL 6, 2014 Susan S. Braithwaite, MD Visiting Clinical Professor Division
What is the best thing to do or say in the Emergency Room to make sure the ER staff knows how to treat me if I am in a crisis?? APRIL 6, 2014 Susan S. Braithwaite, MD Visiting Clinical Professor Division
Adrenal Pharmacology
 Adrenal Pharmacology Pharmacology Team Naim Kittana, Suhaib Hattab, Ansam Sawalha, Adham Abu Taha, Waleed Sweileh, Ramzi Shawahneh Faculty of Medicine & Health Sciences An-Najah National University 1 Steroidal
Adrenal Pharmacology Pharmacology Team Naim Kittana, Suhaib Hattab, Ansam Sawalha, Adham Abu Taha, Waleed Sweileh, Ramzi Shawahneh Faculty of Medicine & Health Sciences An-Najah National University 1 Steroidal
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Endocrine part two. Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy
 Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Sajeev Menon MD ADRENAL INSUFFICIENCY? FATIGUE? OUTLINE OBJECTIVES PATIENT 1 PATIENT 1 : CLINICAL COURSE
 ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
In memory of Thomas Addison M.D. Son of Joseph and Sarah Addison. Died June 29th 1860 aged 66 years. For 36 years physician to Guy s Hospital London.
 In memory of Thomas Addison M.D. Son of Joseph and Sarah Addison. Died June 29th 1860 aged 66 years. For 36 years physician to Guy s Hospital London. Adrenal insufficiency & Sick Day Rules Case history
In memory of Thomas Addison M.D. Son of Joseph and Sarah Addison. Died June 29th 1860 aged 66 years. For 36 years physician to Guy s Hospital London. Adrenal insufficiency & Sick Day Rules Case history
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES
 HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HYPONATRAEMIA GUIDELINES
 HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
HYPONATRAEMIA GUIDELINES Na + < 130 mmol/l For all patients: Acute = onset < 48 hours Chronic = onset > 48 hours or not known Follow acute hyponatraemia flow chart on page 2 Follow chronic hyponatraemia
B-Resistance to the action of hormones, Hormone resistance characterized by receptor mediated, postreceptor.
 Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Endocrine part one. Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy
 Endocrine part one Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy HORMONES Hormones are chemicals released by a cell or a gland
Endocrine part one Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy HORMONES Hormones are chemicals released by a cell or a gland
THE VALUE OF 24 HOUR PROFILES IN CONGENITAL ADRENAL HYPERPLASIA
 THE VALUE OF 24 HOUR PROFILES IN CONGENITAL ADRENAL HYPERPLASIA This leaflet is a joint production between Professor Peter Hindmarsh and Kathy Geertsma The series editor is Professor Peter Hindmarsh Professor
THE VALUE OF 24 HOUR PROFILES IN CONGENITAL ADRENAL HYPERPLASIA This leaflet is a joint production between Professor Peter Hindmarsh and Kathy Geertsma The series editor is Professor Peter Hindmarsh Professor
THE VALUE OF 24 HOUR PROFILES IN ASSESSING CORTISOL REPLACEMENT IN HYPOPITUITARISM
 THE VALUE OF 24 HOUR PROFILES IN ASSESSING CORTISOL REPLACEMENT IN HYPOPITUITARISM Professor Peter Hindmarsh and Kathy Geertsma Cortisol is produced in the body by the adrenal glands and the levels in
THE VALUE OF 24 HOUR PROFILES IN ASSESSING CORTISOL REPLACEMENT IN HYPOPITUITARISM Professor Peter Hindmarsh and Kathy Geertsma Cortisol is produced in the body by the adrenal glands and the levels in
Assistant Professor of Endocrinology
 Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Cortisol (serum, plasma)
") Cortisol (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Cortisol 1.2 Alternative names Hydrocortisone, 11β; 17, 21 trihydroxypregn 4 ene 3,20 dione 1.3 NMLC code 1.4 Description
Cortisol (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Cortisol 1.2 Alternative names Hydrocortisone, 11β; 17, 21 trihydroxypregn 4 ene 3,20 dione 1.3 NMLC code 1.4 Description
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pharmacology of Corticosteroids
 Pharmacology of Corticosteroids Dr. Aliah Alshanwani Dept. of Pharmacology College of Medicine, KSU Feb 2018 1 The Corticosteroids are steroid hormones produced by the adrenal cortex. They consist of two
Pharmacology of Corticosteroids Dr. Aliah Alshanwani Dept. of Pharmacology College of Medicine, KSU Feb 2018 1 The Corticosteroids are steroid hormones produced by the adrenal cortex. They consist of two
COPYRIGHTED MATERIAL. Adrenal Imaging. 1.1 Introduction. Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M.
 1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW
 CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
Adrenal Insufficiency
 Adrenal Insufficiency Normal adrenal physiology Clinical features, Laboratory findings Common causes of primary adrenal insufficiency Evaluation of suspected adrenal insufficiency Acute and chronic management
Adrenal Insufficiency Normal adrenal physiology Clinical features, Laboratory findings Common causes of primary adrenal insufficiency Evaluation of suspected adrenal insufficiency Acute and chronic management
REFERRAL GUIDELINES ENDOCRINOLOGY
 REFERRAL GUIDELINES ENDOCRINOLOGY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
REFERRAL GUIDELINES ENDOCRINOLOGY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
The Adrenal Glands. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement. II.
 The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
MANAGEMENT OF PATIENTS WITH PITUITARY DISORDERS ON THE NEUROSUGERY WARDS RESPONSIBILITIES OF THE METABOLIC REGISTRAR
 MANAGEMENT OF PATIENTS WITH PITUITARY DISORDERS ON THE NEUROSUGERY WARDS RESPONSIBILITIES OF THE METABOLIC REGISTRAR We have clear links with DCN and a responsibility for the management of patients with
MANAGEMENT OF PATIENTS WITH PITUITARY DISORDERS ON THE NEUROSUGERY WARDS RESPONSIBILITIES OF THE METABOLIC REGISTRAR We have clear links with DCN and a responsibility for the management of patients with
PROBLEMS WITH REGULATION AND METABOLISM. Objectives A & P 8/11/2011
 PROBLEMS WITH REGULATION AND METABOLISM Lemone and Burke Chapters 18-20 Objectives Review A & P Recall age related changes Identify diagnostic tests Describe etiology, pathophysiology, clinical manifestation,
PROBLEMS WITH REGULATION AND METABOLISM Lemone and Burke Chapters 18-20 Objectives Review A & P Recall age related changes Identify diagnostic tests Describe etiology, pathophysiology, clinical manifestation,
Hypoadrenocorticism or Addison's Disease (Inadequate Production of Hormones by the Adrenal Glands) Basics
 Basics") Hypoadrenocorticism or Addison's Disease (Inadequate Production of Hormones by the Adrenal Glands) Basics OVERVIEW A hormonal disorder resulting from decreased production of hormones (glucocorticoids and/or
Hypoadrenocorticism or Addison's Disease (Inadequate Production of Hormones by the Adrenal Glands) Basics OVERVIEW A hormonal disorder resulting from decreased production of hormones (glucocorticoids and/or
Practical Management of Steroids in Non-Endocrine Practice
 Practical Management of Steroids in Non-Endocrine Practice Dr Miguel Debono MD MRCP PhD Consultant Physician in Endocrinology and Honorary Senior Lecturer February 2016 Outline Epidemiology of steroids
Practical Management of Steroids in Non-Endocrine Practice Dr Miguel Debono MD MRCP PhD Consultant Physician in Endocrinology and Honorary Senior Lecturer February 2016 Outline Epidemiology of steroids
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY
 JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
CHISCG1: Short Synacthen Test for the Investigation of Adrenal Insufficiency
 Pathology at the Royal Derby Hospital Short Synacthen Test Standard Clinical Guidelines Chemical Pathology Department Valid Until 31 st August 2011 Document Code: CHISCG1 Short Synacthen Test for the Investigation
Pathology at the Royal Derby Hospital Short Synacthen Test Standard Clinical Guidelines Chemical Pathology Department Valid Until 31 st August 2011 Document Code: CHISCG1 Short Synacthen Test for the Investigation
ADRENAL GLANDS. G M Kellerman. Hunter Area Pathology Service
 ADRENAL GLANDS G M Kellerman Hunter Area Pathology Service ADRENAL FUNCTIONS THE ADRENAL GLANDS ACTUALLY HAVE 4 QUITE SEPARATE FUNCTIONS 1. MINERALOCORTICOID SECRETION BY THE ZONA GLOMERULOSA OF THE CORTEX
ADRENAL GLANDS G M Kellerman Hunter Area Pathology Service ADRENAL FUNCTIONS THE ADRENAL GLANDS ACTUALLY HAVE 4 QUITE SEPARATE FUNCTIONS 1. MINERALOCORTICOID SECRETION BY THE ZONA GLOMERULOSA OF THE CORTEX
Adrenal Insufficiency in Children
 Adrenal Insufficiency in Children Stephanie Hsu, MD, PhD Assistant Professor Director of Quality Improvement and Patient Safety Pediatric Endocrinology Children s Hospital Colorado and the Barbara Davis
Adrenal Insufficiency in Children Stephanie Hsu, MD, PhD Assistant Professor Director of Quality Improvement and Patient Safety Pediatric Endocrinology Children s Hospital Colorado and the Barbara Davis
ADRENAL HYPOFUNCTION: GUIDELINES FOR INVESTIGATION
 ADRENAL HYPOFUNCTION: GUIDELINES FOR INVESTIGATION Version: 2.0 Ratified by: Clinical Biochemistry Senior Staff meeting Date ratified: 28-01-2014 Name of originator/author: Director responsible for implementation:
ADRENAL HYPOFUNCTION: GUIDELINES FOR INVESTIGATION Version: 2.0 Ratified by: Clinical Biochemistry Senior Staff meeting Date ratified: 28-01-2014 Name of originator/author: Director responsible for implementation:
Differential Diagnosis of Cushing s Syndrome
 Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
Lawrence S. Kirschner, MD, PhD Professor of Medicine
 Adrenal Insufficiency: Current Practice 2012 Lawrence S. Kirschner, MD, PhD Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism The Ohio State University s Wexner Medical Center Overview
Adrenal Insufficiency: Current Practice 2012 Lawrence S. Kirschner, MD, PhD Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism The Ohio State University s Wexner Medical Center Overview
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to
 Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to the Hypothalamus 3. Blood Supply of the Pituitary Gland
Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to the Hypothalamus 3. Blood Supply of the Pituitary Gland
Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC
 10 th Annual Canadian Endocrine Update 3 rd Canadian Endocrine Review Course Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC 10 th Annual Canadian Endocrine Update Dr.
10 th Annual Canadian Endocrine Update 3 rd Canadian Endocrine Review Course Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC 10 th Annual Canadian Endocrine Update Dr.
Adrenal Insufficiency During Pregnancy
 Disclosures Adrenal Insufficiency During Pregnancy Research funding from Diurnal Limited via NIH CRADA mechanism Deborah P. Merke, M.D., M.S. Bethesda, MD Outline Primary Adrenal Insufficiency Physiological
Disclosures Adrenal Insufficiency During Pregnancy Research funding from Diurnal Limited via NIH CRADA mechanism Deborah P. Merke, M.D., M.S. Bethesda, MD Outline Primary Adrenal Insufficiency Physiological
Disclosures. The Endocrine System. Objectives. Diabetes. The Endocrine System 4/5/17. Common Medications in Pediatric Endocrinology
 Disclosures Common Medications in Pediatric Endocrinology I have nothing to disclose Carrie A. Tolman, CPNP Nationwide Children s Hospital Objectives The Endocrine System Review common endocrine disorders
Disclosures Common Medications in Pediatric Endocrinology I have nothing to disclose Carrie A. Tolman, CPNP Nationwide Children s Hospital Objectives The Endocrine System Review common endocrine disorders
Metopirone (metyrapone)
") 1 Metopirone (metyrapone) NAME OF THE DRUG Active ingredient: metyrapone Chemical names: 2-methyl-1,2-di-3-pyridyl-1-propanone CAS number: 54-36-4 Molecular weight: 226.27 Molecular formula C 14 H 14 N
1 Metopirone (metyrapone) NAME OF THE DRUG Active ingredient: metyrapone Chemical names: 2-methyl-1,2-di-3-pyridyl-1-propanone CAS number: 54-36-4 Molecular weight: 226.27 Molecular formula C 14 H 14 N
Adrenal Ganglioneuroma Presenting With Adrenal Insufficiency After Unilateral Adrenalectomy
 ISPUB.COM The Internet Journal of Urology Volume 9 Number 1 Adrenal Ganglioneuroma Presenting With Adrenal Insufficiency After Unilateral Adrenalectomy S Bontha, N Sanalkumar, M Istarabadi, G Lepsien,
ISPUB.COM The Internet Journal of Urology Volume 9 Number 1 Adrenal Ganglioneuroma Presenting With Adrenal Insufficiency After Unilateral Adrenalectomy S Bontha, N Sanalkumar, M Istarabadi, G Lepsien,
ADDISON S DISEASE THE FACTS YOU NEED TO KNOW
 ADDISON S DISEASE THE FACTS YOU NEED TO KNOW WHAT IS Addison's disease is a severe or total deficiency of the hormones made in the adrenal cortex, caused by its destruction. There are normally two adrenal
ADDISON S DISEASE THE FACTS YOU NEED TO KNOW WHAT IS Addison's disease is a severe or total deficiency of the hormones made in the adrenal cortex, caused by its destruction. There are normally two adrenal
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY
 THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
Anaesthesia and adrenocortical disease
 Anaesthesia and adrenocortical disease Melanie Davies FRCA Jonathan Hardman DM FRCA Key points Adrenocortical disease results in disturbances of body water volume and electrolyte concentrations; intra-cellular
Anaesthesia and adrenocortical disease Melanie Davies FRCA Jonathan Hardman DM FRCA Key points Adrenocortical disease results in disturbances of body water volume and electrolyte concentrations; intra-cellular
METOPIRONE Product Information
 METOPIRONE Product Information (metyrapone) NAME OF THE MEDICINE Active ingredient: metyrapone Chemical name: 2-methyl-1,2-di-3-pyridyl-1-propanone Molecular formula: C14H14N2 O CAS number: 54-36-4 Molecular
METOPIRONE Product Information (metyrapone) NAME OF THE MEDICINE Active ingredient: metyrapone Chemical name: 2-methyl-1,2-di-3-pyridyl-1-propanone Molecular formula: C14H14N2 O CAS number: 54-36-4 Molecular
Cushing s syndrome and adrenal insufficiency
 Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
Cushing's disease, Cushing's syndrome
 Greenville Veterinary Clinic LLC 409 E. Jamestown Rd. Greenville, PA 16125 (724) 588-5260 Canine hyperadrenocorticism Cushing's disease, Cushing's syndrome AffectedAnimals: Although dogs of almost every
Greenville Veterinary Clinic LLC 409 E. Jamestown Rd. Greenville, PA 16125 (724) 588-5260 Canine hyperadrenocorticism Cushing's disease, Cushing's syndrome AffectedAnimals: Although dogs of almost every
Brunel Health Core Ten Results for Sam Witter. Thank you for submitting a sample of your blood to be tested by Brunel Health.
 Brunel Health Core Ten Results for Sam Witter Dear Sam, Thank you for submitting a sample of your blood to be tested by Brunel Health. We are pleased to say that there was enough viable sample to test
Brunel Health Core Ten Results for Sam Witter Dear Sam, Thank you for submitting a sample of your blood to be tested by Brunel Health. We are pleased to say that there was enough viable sample to test
Summary of Treatment Benefits Page 72 of 111. Page 72
 1.8.2 Page 72 of 111 Page 72 need surgery to remove part or all of the thyroid gland. This procedure is known as a thyroidectomy (removal of thyroid gland), and is followed by life-long intake of levothyroxine.
1.8.2 Page 72 of 111 Page 72 need surgery to remove part or all of the thyroid gland. This procedure is known as a thyroidectomy (removal of thyroid gland), and is followed by life-long intake of levothyroxine.
Hypertension: Who and How (and Why) to Investigate. Jessica Triay Andy Levy
 to Investigate. Jessica Triay Andy Levy") Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
Great Ormond Street Hospital for Children NHS Foundation Trust
 Great Ormond Street Hospital for Children DEPARTMENT OF ENDOCRINOLOGY Great Ormond Street Tel: 2 745 9 Questions answered by Professor Peter Hindmarsh It is true that many centres work differently regarding
Great Ormond Street Hospital for Children DEPARTMENT OF ENDOCRINOLOGY Great Ormond Street Tel: 2 745 9 Questions answered by Professor Peter Hindmarsh It is true that many centres work differently regarding
Non Thyroid Surgery. In patients with Thyroid disorders
 Non Thyroid Surgery In patients with Thyroid disorders The Thyroid disease problem. Is Thyroid disease a problem with anaesthetic? Why worry? The Physiology The evidence. A pragmatic approach From: The
Non Thyroid Surgery In patients with Thyroid disorders The Thyroid disease problem. Is Thyroid disease a problem with anaesthetic? Why worry? The Physiology The evidence. A pragmatic approach From: The
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
The Pathological l Basis of Disease
 Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Hyperadrenocorticism or Cushing's Syndrome in Dogs
 Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Hyperadrenocorticism or Cushing's Syndrome in Dogs (Excessive Levels of Steroids
Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Hyperadrenocorticism or Cushing's Syndrome in Dogs (Excessive Levels of Steroids
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Running head: THE OPTIMAL TREATMENT FOR ADDISON S DISEASE
 Running head: THE OPTIMAL TREATMENT FOR ADDISON S DISEASE 1 Kelly Wetmore Merrimack College 2 Introduction Addison s disease is a rare autoimmune disorder caused by the body s destruction of its own adrenal
Running head: THE OPTIMAL TREATMENT FOR ADDISON S DISEASE 1 Kelly Wetmore Merrimack College 2 Introduction Addison s disease is a rare autoimmune disorder caused by the body s destruction of its own adrenal
Endocrinology Update. Dr Colin Johnston Hon Consultant West Herts Trust
 Endocrinology Update Dr Colin Johnston Hon Consultant West Herts Trust colin.johnston2@nhs.net Thyrotoxicosis Symptoms GI symptoms-diarrhoea Fatigue Anxiety Irreg Menstruation Do not be put off the diagnosis
Endocrinology Update Dr Colin Johnston Hon Consultant West Herts Trust colin.johnston2@nhs.net Thyrotoxicosis Symptoms GI symptoms-diarrhoea Fatigue Anxiety Irreg Menstruation Do not be put off the diagnosis
Kristen Dillard, M.D. Endorama December 6, 2012
 Kristen Dillard, M.D. Endorama December 6, 2012 12 7/12 yo girl with h/o Cushing s disease presented to OSH with concern for CVA Consumed ½plate of food the night before, had raisins and diet soda on the
Kristen Dillard, M.D. Endorama December 6, 2012 12 7/12 yo girl with h/o Cushing s disease presented to OSH with concern for CVA Consumed ½plate of food the night before, had raisins and diet soda on the