Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
|
|
|
- Jemima Cross
- 5 years ago
- Views:
Transcription

1 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma 57,000. Colonic Adenocarcinoma (Overview of lecture) - Precursor lesions (Adenoma- Carcinoma sequence) - Pathologic staging of colorectal tumors - Chronic inflammation (IBD, including UC and Crohns) - Genetics (genetic predisposition) FAP (germline mutation of APC gene) HNPCC (germline mutation of mismatch repair gene) - Molecular pathways of colorectal carcinogenesis Suppressor pathway (APC/beta catenin) Mutator pathway (DNA mismatch repair genes) Colonic Polyps : Hyperplastic vs. Adenomatous 1



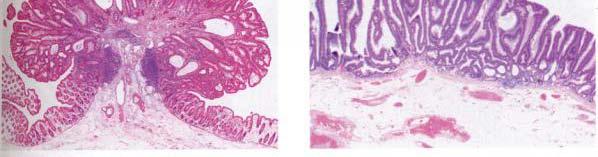
2 Colonic Polyps : Hyperplastic Saw tooth shape of surface epithelium No dysplasia. 2


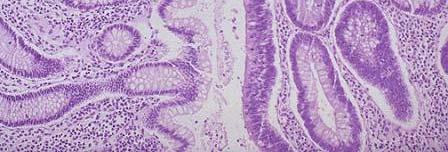
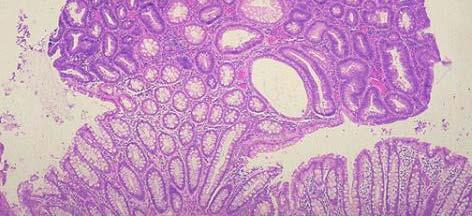
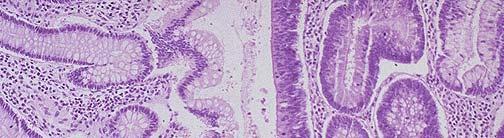

3 Colonic Polyps : Adenoma Adenomas by definition have dysplasia. Lack of surface maturation 3
 nuclear")


4 Colonic Polyps : Hyperplastic vs. Adenomatous MIB-1 (immuno) nuclear staining Adenoma- lacks surface maturation; Hyperplastic Polyp Adenoma Abnormal proliferation is a hallmark of neoplasia Lack of surface maturation Proliferation extends to the surface 4
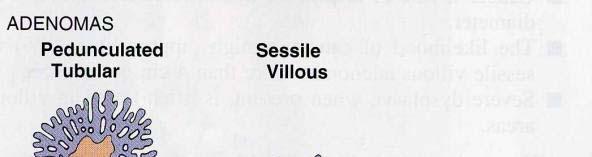
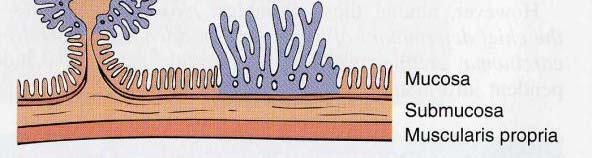





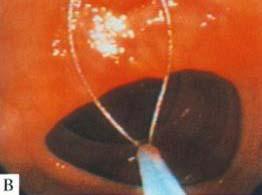
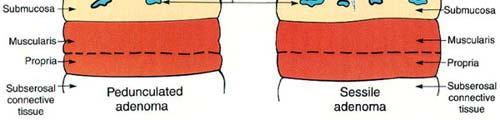
5 Adenomas pedunculated vs sessile Endoscopic polypectomy 5




6 Adenoma on endoscopy 6



7 Sessile adenoma Sessile villous adenoma 7

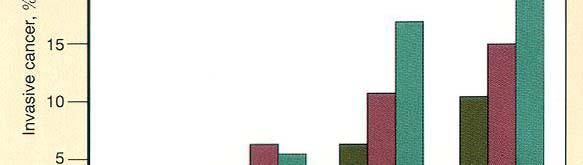
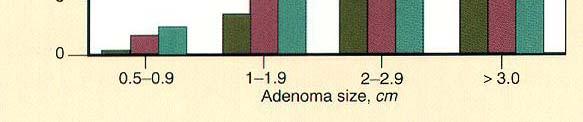
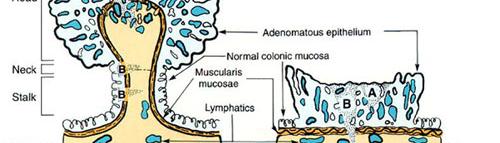
8 Percent of adenomas containing invasive cancer Carcinoma within a polyp 8


9 Polypectomy is only Treatment IF: 1) Stalk margin is negative 2) No lymphatic/vascular invasion 3) Tumor is not poorly differentiated. Adenoma Carcinoma Sequence Populations that have a high prevalence of adenomas have a high prevalence of colorectal carcinoma. The distribution of adenomas within the colorectum is similar to that of colorectal carcinoma. Peak incidence of adenomas antedates the peak for colorectal carcinoma. Adenomatous epithelium is often co-existent with adenocarcinoma. Screening programs that carefully follow patients for the development of adenomas and remove all that are identified, reduce the incidence of colorectal cancer. 9

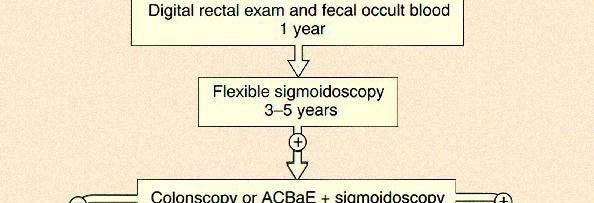




10 Algorithm for colon cancer surveillance Adenocarcinomas and carcinomas affecting colon 10

11 Colon cancer -endoscopy Adenocarcinoma 11



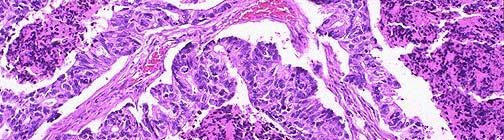
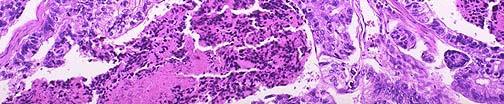
12 Invasive adenocarcinoma Irregular infiltrative glands within submucosa Desmoplastic loose fibrotic tissue response Survival probabilities according to stage of disease (b) Astler-Coller 12
13 TNM classification of colorectal adenocarcinoma T- Primary tumor Tx T0 Tis T1 T2 T3 T4 Primary tumor cannot be assessed No evidence of primary tumor Carcinoma in situ (intraepithelial or intramucosal invasion of lamina propria)*** Tumor invades submucosa Tumor invades muscularis propria Tumor invades through muscularis propria into subserosa or into pericolic/perirectal fat. Tumor directly invades other organs or structures and/or perforates visceral peritoneum. *** In the colon, unless a tumor invades into the submucosa, it is not considered an invasive adenocarcinoma. TNM classification of colorectal adenocarcinoma N-Regional Lymph Nodes Nx Regional lymph nodes cannot be assessed N0 No regional lymph node metastasis N1 Metastasis in 1 to 3 regional lymph nodes N2 Metastasis in 4 or more regional lymph nodes M- Distant Metastases Mx Distant metastasis cannot be assessed M0 No distant metastasis M1 Distant metastasis 13


14 Major classes of proteins encoded by cancer-associated genes: Tumor suppressor genes, DNA repair genes, Protooncogenes, Proteins regulating apoptosis. Familial Adenomatous Polyposis 14
 APC- tumor")






15 Familial adenomatous polyposis (FAP) APC- tumor suppressor gene Germline mutation of APC gene Patients develop thousands of polyps by their 2 nd decade. The second APC gene must be lost for adenoma formation. Virtually 100% risk for developing Colorectal adenocarcinoma; also high risk of ampullary carcinoma. Earliest precursor lesion aberrant crypt Familial Adenomatous Polyposis (FAP) 15


16 WNT signaling pathway involves APC/beta-catenin and Tcf-4. In malignant cells with loss of APC, beta catenin degradation is prevented, tdso WNT signaling response is continually activated. WNT-soluble factor that induces cellular proliferation by binding to its cytoplasmic receptor Preventing degradation of beta-catenin allowing it to translocate to the nucleus where it acts as a transcriptional activator in conjunction with Tcf-4. APC protein- antiproliferative effect; integral part of complex that destoys beta-catenin. HNPCC Hereditary Non-Polyposis Colon Cancer 16


17 Inheritance in family with cancer family syndrome HNPCC Clinical Criteria for HNPCC Amsterdam criteria: At least 3 relatives with colon cancer and all of the following: -One affected person is a first degree relative of the other two affected persons -Two successive generations affected. -At least one case of colon cancer diagnosed before age 50 y -FAP excluded d Modified Amsterdam criteria: same as Amsterdam criteria except cancer can involve (colon, endometrium, small bowel, ureter or renal pelvis) instead of only colon cancer. 17


; Most microsatellites are in")




18 Microsatellite Instability- the result of mismatch repair gene mutations Normal Tumor Microsatellites are simple repetitive DNA sequences (mono or dinucleotide repeats); Most microsatellites are in non-coding regions but a few are in coding regions of critical genes TGF-beta RII, IGFIIR, Tcf-4, BAX. Immunohistochemical Staining for mismatch repair enzymes MLH1 MSH2 Tubular adenoma in an HNPCC patient. Neoplastic epithelium shows of loss of MSH2 expression, which correlates with mutation of the MSH2 mismatch repair gene. 18
19 Summary of clinical, pathological and genetic features of HNPCC - Familial clustering of colorectal and/or endometrial cancer - Excess risk of cancer of the ovary, ureter/renal pelvis, small bowel, stomach, brain, hepatobiliary tract, and skin (sebaceous tumors) - Development of multiple cancers at an early age - Features of colorectal adenoma include: i. variable ibl numbers (one to a few) ii. high degree of dysplasia iii. rapid progression from adenoma to carcinoma (additional mutations rapidly accumulate ACCELERATED TUMORIGENESIS) iv. high frequency of MSI - Features of colorectal cancer include: i. predilection to proximal colon ii. improved survival iii. iv. multiple colorectal tumors increased proportion of mucinous tumors, poorly differentiated tumors, and tumors with marked host lymphocytic infiltrate at tumor margin. HNPCC clinical characteristics HNPCC CLINICAL CHARACTERISTICS HNPCC Mean age at diagnosis, i y Sporadic Multiple colon cancers, % Synchronous Metachronous Proximal location, % Excess malignancies at other sites Yes No Mucinous and poorly differentiated cancers Common Infrequent ent RER + %
, and DNA repair genes (hmsh2, hmlh1).")
20 Molecular genetic events in evolution of colon cancer The progression to colorectal cancer is associated with an accumulation of genetic alterations, including alterations in oncogenes (K-ras), tumor suppressor genes (APC, DCC, p53), and DNA repair genes (hmsh2, hmlh1). The exact sequence of events is approximate and may vary in sporadic cancers compared with those arising in hereditary syndromes or inflammatory bowel disease. Genes altered in colon cancer GENES ALTERED IN COLON CANCER Gene Sporadic tumors with Chromosome alterations, % Class Function K - ras Protooncogene Signal transduction?cell adhesion APC 5 60 Tumor supressor Anti-proliferative function DCC Tumor supressor?cell adhesion p Tumor supressor hmsh2 2 hmlh1 3 DNA Mismatch repair DNA Mismatch repair Cell cycle control (G1/S arrest) Maintains fidelity of DNA replication Maintains fidelity of DNA replication 20

 -negligible risk.")
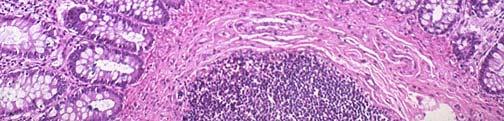
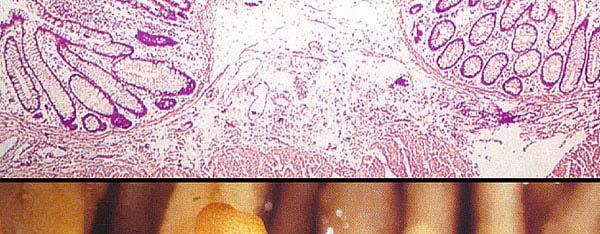
21 Dysplasia and Carcinoma in Inflammatory Bowel disease Dysplasia-associated lesion/mass (DALM) in Ulcerative Colitis High grade Dsplasia Dysplasia Risk of dysplasia in UC correlate with EXTENT and DURATION of disease. UC patients with pancolitis are at highest risk. Ulcerative proctitis (disease limited to rectum) -negligible risk. DALM (dysplasia associated lesions) greater than 50% chance of coexistent invasive adenocarcinoma. 21




22 Probability of developing colorectal carcinoma in ulcerative colitis Cumulative risk of developing adenocarcinoma correlates with duration of UC: 5% in 5 years 15% in 25 years 30-50% in 40 years 1% per year cumulative incidence of carcinoma after 10 years duration of disease. Bresalier RS, Kim YS, In Gastrointestinal Disease: Pathophysiology/Diagnosis/Management, edn 5. Edited by Sleisenger MH, Fordtran JS. Philadelphia: WB Saunders; Estimates of the predisposing causes of Colorectal Carcinoma 22
23 Current screening (average risk) FOBT FOBT annual Positive tests Flex sig Flex sig - 5yr Colonoscopy Colonoscopy every 10 yr Barium Enema every 5 yr Current screening (increased risk) 1 adenoma <1cm 3-6 yr after initial polypectomy Adenoma>1cm, 3 yrs after Multiple adenomas initial polypectomy Curative resection of colon cancer Colonoscopy Within 1 yr If normal, repeat in 3yr. 23
24 Current screening (high risk) FAP (family hx) puberty Genetic testing HNPCC (family hx) IBD age 21 Risk greater with Pancolitis, >10yr duration Genetic testing, 1-2 yr until age 40, then annually Every 1-2 yr. Colonic Neoplasia Colonic Adenocarcinoma (Summary) - Precursor lesions (Adenoma- Carcinoma sequence) - Pathologic staging of colorectal tumors - Chronic inflammation (IBD, including UC and Crohns) - Genetics (genetic predisposition) FAP (germline mutation of APC gene) HNPCC (germline mutation of mismatch repair gene) - Molecular pathways of colorectal carcinogenesis Suppressor pathway (APC/beta catenin) Mutator pathway (DNA mismatch repair genes) 24
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Hereditary Non Polyposis Colorectal Cancer(HNPCC) From clinic to genetics
 From clinic to genetics") From clinic to genetics Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Autosomal dominant Question 2) Incidence of
From clinic to genetics Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Autosomal dominant Question 2) Incidence of
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Colon Cancer Screening & Surveillance. Amit Patel, MD PGY-4 GI Fellow
 Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Content. Diagnostic approach and clinical management of Lynch Syndrome: guidelines. Terminology. Identification of Lynch Syndrome
 of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
EARLY DETECTION OF COLORECTAL CANCER. Epidemiology of CRC
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Neoplasia 18 lecture 6. Dr Heyam Awad MD, FRCPath
 Neoplasia 18 lecture 6 Dr Heyam Awad MD, FRCPath ILOS 1. understand the role of TGF beta, contact inhibition and APC in tumorigenesis. 2. implement the above knowledge in understanding histopathology reports.
Neoplasia 18 lecture 6 Dr Heyam Awad MD, FRCPath ILOS 1. understand the role of TGF beta, contact inhibition and APC in tumorigenesis. 2. implement the above knowledge in understanding histopathology reports.
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Serrated Polyps and a Classification of Colorectal Cancer
 Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Lynch Syndrome. Angie Strang, PGY2
 Lynch Syndrome Angie Strang, PGY2 Background Previously hereditary nonpolyposis colorectal cancer Autosomal dominant inherited cancer susceptibility syndrome Caused by defects in the mismatch repair system
Lynch Syndrome Angie Strang, PGY2 Background Previously hereditary nonpolyposis colorectal cancer Autosomal dominant inherited cancer susceptibility syndrome Caused by defects in the mismatch repair system
Development of Carcinoma Pathways
 The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
Multistep nature of cancer development. Cancer genes
 Multistep nature of cancer development Phenotypic progression loss of control over cell growth/death (neoplasm) invasiveness (carcinoma) distal spread (metastatic tumor) Genetic progression multiple genetic
Multistep nature of cancer development Phenotypic progression loss of control over cell growth/death (neoplasm) invasiveness (carcinoma) distal spread (metastatic tumor) Genetic progression multiple genetic
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
General Surgery Grand Grounds
 General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
Risk of Colorectal Cancer (CRC) Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE
 Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE") Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
B Base excision repair, in MUTYH-associated polyposis and colorectal cancer, BRAF testing, for hereditary colorectal cancer, 696
 Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma
 Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population
 Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Pr
 Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Professor Yong Loo Lin School of Medicine, National University
Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Professor Yong Loo Lin School of Medicine, National University
removal of adenomatous polyps detects important effectively as follow-up colonoscopy after both constitute a low-risk Patients with 1 or 2
 Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist
 ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist limhweeyong@live.com CRC: Epidemiology in 2012 Third most common cancer diagnosis in US [1] Estimated 143,460 new cases
ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist limhweeyong@live.com CRC: Epidemiology in 2012 Third most common cancer diagnosis in US [1] Estimated 143,460 new cases
Yes when meets criteria below. Dean Health Plan covers when Medicare also covers the benefit.
 Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post test genetic counseling is
Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post test genetic counseling is
Colon Cancer and Hereditary Cancer Syndromes
 Colon Cancer and Hereditary Cancer Syndromes Gisela Keller Institute of Pathology Technische Universität München gisela.keller@lrz.tum.de Colon Cancer and Hereditary Cancer Syndromes epidemiology models
Colon Cancer and Hereditary Cancer Syndromes Gisela Keller Institute of Pathology Technische Universität München gisela.keller@lrz.tum.de Colon Cancer and Hereditary Cancer Syndromes epidemiology models
BIOLOGY OF CANCER. Definition: Cancer. Why is it Important to Understand the Biology of Cancer? Regulation of the Cell Cycle 2/13/2015
 BIOLOGY OF CANCER Why is it Important to Understand the Biology of Cancer? Cynthia Smith, RN, BA, MSN, AOCN Oncology Clinical Nurse Specialist Harrison Medical Center Definition: Cancer Regulation of the
BIOLOGY OF CANCER Why is it Important to Understand the Biology of Cancer? Cynthia Smith, RN, BA, MSN, AOCN Oncology Clinical Nurse Specialist Harrison Medical Center Definition: Cancer Regulation of the
Test Bank for Robbins and Cotran Pathologic Basis of Disease 9th Edition by Kumar
 Link full download:https://getbooksolutions.com/download/test-bank-for-robbinsand-cotran-pathologic-basis-of-disease-9th-edition-by-kumar Test Bank for Robbins and Cotran Pathologic Basis of Disease 9th
Link full download:https://getbooksolutions.com/download/test-bank-for-robbinsand-cotran-pathologic-basis-of-disease-9th-edition-by-kumar Test Bank for Robbins and Cotran Pathologic Basis of Disease 9th
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING
 CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
Test Bank for Robbins and Cotran Pathologic Basis of Disease 9th Edition by Kumar
 Link full download: http://testbankair.com/download/test-bank-for-robbins-cotran-pathologic-basis-of-disease-9th-edition-bykumar-abbas-and-aster Test Bank for Robbins and Cotran Pathologic Basis of Disease
Link full download: http://testbankair.com/download/test-bank-for-robbins-cotran-pathologic-basis-of-disease-9th-edition-bykumar-abbas-and-aster Test Bank for Robbins and Cotran Pathologic Basis of Disease
David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH
 Colon Cancer 2015 David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH Colon Cancer Case presentation 72yo woman presented 1/03 abd discomfort and nausea Found to have
Colon Cancer 2015 David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH Colon Cancer Case presentation 72yo woman presented 1/03 abd discomfort and nausea Found to have
What All of Us Should Know About Cancer and Genetics
 What All of Us Should Know About Cancer and Genetics Beth A. Pletcher, MD, FAAP, FACMG Associate Professor of Pediatrics UMDNJ- New Jersey Medical School Disclosures I have no relevant financial relationships
What All of Us Should Know About Cancer and Genetics Beth A. Pletcher, MD, FAAP, FACMG Associate Professor of Pediatrics UMDNJ- New Jersey Medical School Disclosures I have no relevant financial relationships
Sessile Serrated Polyps
 Årsmøtet i Den norske Patologforening 2014 Sessile Serrated Polyps Tor J. Eide Oslo Universitetssykehus The term serrated include a group of lesions with a sawtoothlike appearance of the crypts and the
Årsmøtet i Den norske Patologforening 2014 Sessile Serrated Polyps Tor J. Eide Oslo Universitetssykehus The term serrated include a group of lesions with a sawtoothlike appearance of the crypts and the
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colorectal cancer Chapelle, J Clin Oncol, 2010
 Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer
 General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
FACT SHEET 49. What is meant by a family history of bowel cancer? What is bowel cancer? What causes bowel cancer?
 Important points The most important factors that can influence an individual s chance of developing bowel cancer are getting older and having a family history of bowel cancer A family history of bowel
Important points The most important factors that can influence an individual s chance of developing bowel cancer are getting older and having a family history of bowel cancer A family history of bowel
FAMILIAL COLORECTAL CANCER. Lyn Schofield Manager Familial Cancer Registry
 FAMILIAL COLORECTAL CANCER Lyn Schofield Manager Familial Cancer Registry Cancer in WA 2004 4000 3500 ASPR, rate per 100,000 3000 2500 2000 1500 1000 Male incidence Female incidence Male mortality Female
FAMILIAL COLORECTAL CANCER Lyn Schofield Manager Familial Cancer Registry Cancer in WA 2004 4000 3500 ASPR, rate per 100,000 3000 2500 2000 1500 1000 Male incidence Female incidence Male mortality Female
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE
 COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
A class of genes that normally suppress cell proliferation. p53 and Rb..ect. suppressor gene products can release cells. hyperproliferation.
 Tumor Suppressor Genes A class of genes that normally suppress cell proliferation. p53 and Rb..ect Mutations that inactivate the tumor suppressor gene products can release cells from growth suppression
Tumor Suppressor Genes A class of genes that normally suppress cell proliferation. p53 and Rb..ect Mutations that inactivate the tumor suppressor gene products can release cells from growth suppression
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Policy Specific Section: Medical Necessity and Investigational / Experimental. October 14, 1998 March 28, 2014
 Medical Policy Genetic Testing for Colorectal Cancer Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date: Effective Date: October
Medical Policy Genetic Testing for Colorectal Cancer Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date: Effective Date: October
Colonic polyps and colon cancer. Andrew Macpherson Director of Gastroentology University of Bern
 Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
Colorectal carcinoma: Pathologic aspects
 Review Article Colorectal carcinoma: Pathologic aspects Matthew Fleming*, Sreelakshmi Ravula*, Sergei F. Tatishchev*, Hanlin L. Wang Department of Pathology and Laboratory Medicine, David Geffen School
Review Article Colorectal carcinoma: Pathologic aspects Matthew Fleming*, Sreelakshmi Ravula*, Sergei F. Tatishchev*, Hanlin L. Wang Department of Pathology and Laboratory Medicine, David Geffen School
LIST OF ABBREVIATIONS
 Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By. Magnitude of the Problem. Magnitude of the Problem. Cardinal Features of Lynch Syndrome
 GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By HENRY T. LYNCH, M.D. 1 Could this be hereditary Colon Cancer 4 Creighton University School of Medicine Omaha, Nebraska Magnitude of the Problem Annual
GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By HENRY T. LYNCH, M.D. 1 Could this be hereditary Colon Cancer 4 Creighton University School of Medicine Omaha, Nebraska Magnitude of the Problem Annual
Colorectal Cancer Prevention Quantity and Quality Count
 Colorectal Cancer Prevention Quantity and Quality Count Ernesto Drelichman, MD Gastrointestinal Surgery & Endoscopy Providence Hospital Key Messages Colorectal cancer can be prevented Screening reduces
Colorectal Cancer Prevention Quantity and Quality Count Ernesto Drelichman, MD Gastrointestinal Surgery & Endoscopy Providence Hospital Key Messages Colorectal cancer can be prevented Screening reduces
The Whys OAP Annual Meeting CCO Symposium September 20. Immunohistochemical Assessment Dr. Terence Colgan Mount Sinai Hospital, Toronto
 Immunohistochemical Assessment of Mismatch Repair Proteins in Endometrial Cancer: The Whys and How Terence J. Colgan, MD Head of Gynaecological Pathology, Mount Sinai Hospital, University of Toronto, Toronto.
Immunohistochemical Assessment of Mismatch Repair Proteins in Endometrial Cancer: The Whys and How Terence J. Colgan, MD Head of Gynaecological Pathology, Mount Sinai Hospital, University of Toronto, Toronto.
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
Aberrant cell Growth. Younas Masih New Life College of Nursing Karachi. 3/4/2016 Younas Masih ( NLCON)
") Aberrant cell Growth Younas Masih New Life College of Nursing Karachi 1 Objectives By the end of this session the learners will be able to, Define the characteristics of the normal cell Describe the characteristics
Aberrant cell Growth Younas Masih New Life College of Nursing Karachi 1 Objectives By the end of this session the learners will be able to, Define the characteristics of the normal cell Describe the characteristics
Molecular markers in colorectal cancer. Wolfram Jochum
 Molecular markers in colorectal cancer Wolfram Jochum Biomarkers in cancer Patient characteristics Tumor tissue Normal cells Serum Body fluids Predisposition Diagnostic marker Specific diagnosis Prognostic
Molecular markers in colorectal cancer Wolfram Jochum Biomarkers in cancer Patient characteristics Tumor tissue Normal cells Serum Body fluids Predisposition Diagnostic marker Specific diagnosis Prognostic
Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School
 Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Update on Colonic Serrated (and Conventional) Adenomatous Polyps
 Adenomatous Polyps") Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University
 Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University") COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
Mr Chris Wakeman. General Surgeon University of Otago, Christchurch. 12:15-12:40 Management of Colorectal Cancer
 Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Pathology Today American Society for Clinical Pathology Annual Meeting Workshop No: 1340 Gastrointestinal Pathology: New Approaches to Old Problems
 Pathology Today American Society for Clinical Pathology Annual Meeting Workshop No: 1340 Gastrointestinal Pathology: New Approaches to Old Problems ASCP Annual Meeting/WASPaLM XXVI World Congress Las Vegas,
Pathology Today American Society for Clinical Pathology Annual Meeting Workshop No: 1340 Gastrointestinal Pathology: New Approaches to Old Problems ASCP Annual Meeting/WASPaLM XXVI World Congress Las Vegas,
Hereditary Gastric Cancer
 Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
Genetic Testing for Lynch Syndrome
 Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post-test genetic counseling is
Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post-test genetic counseling is
Cancer and Oncogenes Bioscience in the 21 st Century. Linda Lowe-Krentz
 Cancer and Oncogenes Bioscience in the 21 st Century Linda Lowe-Krentz December 1, 2010 Just a Few Numbers Becoming Cancer Genetic Defects Drugs Our friends and family 25 More mutations as 20 you get older
Cancer and Oncogenes Bioscience in the 21 st Century Linda Lowe-Krentz December 1, 2010 Just a Few Numbers Becoming Cancer Genetic Defects Drugs Our friends and family 25 More mutations as 20 you get older
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
Prior Authorization. Additional Information:
 Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post test genetic counseling is
Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post test genetic counseling is
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
Quality Measures In Colonoscopy: Why Should I Care?
 Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
M. Azzam Kayasseh,Dubai,UAE
 Thanks A Lot Prof. Linda + Prof. Ernst #drkayasseh_crc_rsm #WEO_CRCSC #UEGW17 @dubaiendoscopyforum @drkayasseh.care.to.cure Twenty World Areas Age-Standardized CRC Incidence Rates by Sex GLOBOCAN 2008
Thanks A Lot Prof. Linda + Prof. Ernst #drkayasseh_crc_rsm #WEO_CRCSC #UEGW17 @dubaiendoscopyforum @drkayasseh.care.to.cure Twenty World Areas Age-Standardized CRC Incidence Rates by Sex GLOBOCAN 2008
TumorNext-Lynch. genetic testing for hereditary colorectal or uterine cancer
 TumorNet-Lynch genetic testing for hereditary colorectal or uterine cancer What Are the Causes of Hereditary Colorectal Cancer? sporadic 70% familial 20% hereditary 10% Lynch syndrome, up to 4% Familial
TumorNet-Lynch genetic testing for hereditary colorectal or uterine cancer What Are the Causes of Hereditary Colorectal Cancer? sporadic 70% familial 20% hereditary 10% Lynch syndrome, up to 4% Familial
AllinaHealthSystems 1
 Overview Biology and Introduction to the Genetics of Cancer Denise Jones, MS, CGC Certified Genetic Counselor Virginia Piper Cancer Service Line I. Our understanding of cancer the historical perspective
Overview Biology and Introduction to the Genetics of Cancer Denise Jones, MS, CGC Certified Genetic Counselor Virginia Piper Cancer Service Line I. Our understanding of cancer the historical perspective
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic. Scott Rieder Dr. Colquhoun
 Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
Genetics of Pancreatic Cancer. October 6, If you experience technical difficulty during the presentation:
 Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Microsatellite instability and other molecular markers: how useful are they?
 Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
Microsatellite instability and other molecular markers: how useful are they? Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship, Barcelona,
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions. South Island Cancer Nurses Network September 2013
 For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Serrated Lesions in the Bowel Cancer Screening Programme
 Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Colon Screening in 2014 Offering Patients a Choice. Clark A Harrison MD The Nevada Colon Cancer Partnership
 Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Hereditary Colorectal Cancer
 A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer testing is right for
A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer testing is right for
CRC and Endoscopy. Objectives. Background
 CRC and Endoscopy Darren Ballard, MD Assistant Professor Gastroenterology/Hepatology Medical College of Wisconsin Objectives Review background demographics and pathways for colon cancer Review colorectal
CRC and Endoscopy Darren Ballard, MD Assistant Professor Gastroenterology/Hepatology Medical College of Wisconsin Objectives Review background demographics and pathways for colon cancer Review colorectal
[A RESEARCH COORDINATOR S GUIDE]
![[A RESEARCH COORDINATOR S GUIDE]](/thumbs/88/117127924.jpg "[A RESEARCH COORDINATOR S GUIDE]") 2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Altorjay István dr. Occurance of gastrointestinal malignancies in world HO statistics (2002) incidency males females total place M.S.
 incidency males females total place M.S.") Altorjay István dr. Occurance of gastrointestinal malignancies in world HO statistics (2002) incidency males females total place M.S. CRC 550 465 472 687 1 023 152 3. 18-24 mo Stomach 603 419 330 518 933
Altorjay István dr. Occurance of gastrointestinal malignancies in world HO statistics (2002) incidency males females total place M.S. CRC 550 465 472 687 1 023 152 3. 18-24 mo Stomach 603 419 330 518 933
Pathology perspective of colonic polyposis syndromes
 Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
Colon Cancer Update Christie J. Hilton, DO
 POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Hyperplastic polyps in hereditary nonpolyposis colorectal cancer
 4 Hyperplastic polyps in hereditary nonpolyposis colorectal cancer F E M Rijcken 1, T van der Sluis 2, H Hollema 2, J H Kleibeuker 1 Department of Gastroenterology 1 and Pathology 2, University Medical
4 Hyperplastic polyps in hereditary nonpolyposis colorectal cancer F E M Rijcken 1, T van der Sluis 2, H Hollema 2, J H Kleibeuker 1 Department of Gastroenterology 1 and Pathology 2, University Medical
A Patient s Guide to risk assessment. Hereditary Colorectal Cancer
 A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? Overview of Syndromes This workbook is designed to help you decide if hereditary cancer
A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? Overview of Syndromes This workbook is designed to help you decide if hereditary cancer
Primary Care Approach to Genetic Cancer Syndromes
 Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
Early (and not so early) colorectal cancer: The pathologist s point of view
 colorectal cancer: The pathologist s point of view") Early (and not so early) colorectal cancer: The pathologist s point of view Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory board for
Early (and not so early) colorectal cancer: The pathologist s point of view Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory board for