PDA LIGATION Management. Physiology Meets Clinical Care?? Patrick J McNamara Associate Professor of Pediatrics Hospital for Sick Children, Toronto
|
|
|
- Stella King
- 5 years ago
- Views:
Transcription





1 PDA LIGATION Management. Physiology Meets Clinical Care?? Patrick J McNamara Associate Professor of Pediatrics Hospital for Sick Children, Toronto






2 Mistaken Beliefs FLAT DISK COSMOGRAPHY and EARTH CENTRALITY- Ancient philosophers and writers (Aristotle, Homer)
3 on the subject of resuscitation, knowledge and experience have now reached a very satisfactory level of completion Henderson 1928 JAMA
4 Evidence from Human Studies Neonate Child Adult Oxygen Yes No No Ventilation Limited No Yes Chest compressions No No Yes Epinephrine i No Yes Yes Sodium Bicarbonate No No Yes
5 Is intravenous Vasopressin superior to Epinephrine in a neonatal model of asphyxial cardiac arrest?
6 Methods: Study Design Model: Neonatal Porcine model of Ashyxial Cardiac arrest Standardized Resuscitation: Single resuscitator performing chest compressions Compression to ventilation rate of 5:1 Intervention: Placebo controlled randomized control trial of single dose Vasopressin vs Epinephrine Block randomization Resuscitation medications prepared in standardized solution to ensure a consistent dose of 0.1 mls/kg administered
7 Interventions Placebo (0.9% saline) Low-dose epinephrine p (LDE) mg/kg High-dose epinephrine (HDE) mg/kg Low-dose vasopressin (LDV) U/kg
8 Evaluation time-points A-I (Baseline) A-II (Serial Assessments) A-III (Final) 1. Vital signs 2. 2D echo 3. ABG / Lac 4. Plasma catecholamine, vasopressin & troponin levels 1. Vital signs: T2, 10, 30, 60 & 90 mins 2. 2D echo: T2, 10, 30, 60 & 90 mins 3. ABG / Lac: T10, 30 & 120 mins 1. Vital signs 2. 2D echo 3. ABG / Lac 4. Plasma catecholamine, vasopressin & troponin levels 5. Histology 6. Wet dry ratio T0 T2 T10 T30 T60 T90 T120 4 mins Arrest CPR Asphyxial insult started tloaf (mins) trosc (mins)
9 Survival rate (%) Improved survival with vasopressin vs control, p=0.01 ANOVA # # 90% 80 73% % 60 64% 40 40% 35.7% 20 0 Control LDE HDE LDV HDV
10 Plasma Troponin - Survivors #, mmol/l # # # # # Control Epi-Lo Epi-Hi VP-Lo Vp-Hi Group Elevated troponin levels in all groups but no intergroup difference




11 Patent Ductus Arteriosus (PDA) Incidence: 60% in infants born < 28 wks GA 80% in infants born < 26 wks GA 1 st line treatment: t t NSAID but failure rate 35-40% needing surgical closure Need for surgery is most common in extreme preterm infants
12 Teixeira 2006 Acta Paed
13 Merrit J Pediatr 1978



14 Role of the Ductus Arteriosus Transitional Physiology PPHN, RV dysfunction Duct dependant cardiac lesions Systemic-pulmonary shunting
15 Trends in Ductal Care Era of prophylactic p NSAIDs Alternative agents End of the era Era of the Permissive Ductus
16 PDA Ligation & Outcome Kabra 2007 J Pediatrics Chorne 2007 Pediatrics
17 PRETERM INFANT Hemodynamically significant Ductus Arteriosus (HSDA) THERAPEUTIC INTERVENTION NEONATAL MORBIDITY e.g. NEC, PVL ADVERSE OUTCOME
18 Issues.. Variable role of the Ductus arteriosus Challenges of making the diagnosis Clinical confounders Echocardiography confounders Failure to streamline those patients where the ductus arteriosus is an innocent bystander from a hemodynamically y significant ductus arteriosus (HSDA) Oversimplification of study designs and remoteness of long term outcomes
19 Scenario I 31 day old (27/40 weeks) referred for emergency PDA ligation Issues: Oxygenation failure (HFOV) and hypotension (Dobutamine 20) fecho: 3.2 mm HSDA with L-R flow, dilated LA LV, LVO 420 mls/kg/min Refractory hypotension dobutamine, dopamine, epinephrine, hydrocortisone Respiratory Failure Respiratory Failure Died day 2 postop
20 Therapeutic window of opportunity D RDS Extubated Desaturations Referral (CIII) Ligation (CI) Surf ncpap Cardiomegaly Pulmonary edema Reintubated Full enteral feeds
21 Lessons learned Hazards of an expectant approach and All or none approach to care Disconnect between clinical scenario and findings on 2D echo Intervention may have saved this life
22 Pre-Ligation Post-Ligation FiO2 30% 50% MAP 7 11
23 Perioperative Management of Hypotension Early Group Late Group p (n=32) (n=33) Fluid bolus 7 (24.1) 8 (22.2) 1.0 Post op inotropes 8 (27.6) 2 (5.6) 0.019* Teixeira et al. J Perinat 2008
24 Post-Ligation Cardiac Syndrome (PLCS) Clinical deterioration with predictable onset at 8-12 hours characterized by: Oxygenation Failure 20% < 1000g (p<0.01) Systolic Hypotension X 8 fold increase < 1000g Need for cardiotropes Teixeira et al. J Perinat 2008
25 Teixeira et al. J Perinat 2008


![[Normal]](/docs-images/92/108919123/images/26-2.jpg "8 HOURS")

![function]](/docs-images/92/108919123/images/26-5.jpg)




26 Systemic blood flow PRE-OP [Normal] 8 HOURS [Impaired LV function]
27 Study II Is this an effect of LV exposed afterload on myocardial performance? Hypothesis: Increased LVE-VR (Left ventricle exposed vascular resistance), after PDA ligation, was associated with impaired myocardial performance
28 Left Ventricle Exposed Vascular Resistance (LVER) PVR ++ PDA Ao SVR Ao Left Ventricle
 NEONATE CHILD Rowland 1995")
29 Stress-Velocity Relationship (Afterload) NEONATE CHILD Rowland 1995 Am J Card
30 LV dysfunction after PDA ligation in preterm baboon Taylor 1990 J Surg Res SF SVR
31 Myocardial Performance LV Exposed Vascular Resistance mvcfc p < p < Dy ynes *# #* #* cir c/min * 1.4 * * # # # Time Time # p < 0.05 vs baseline McNamara, 2010 J Thorac Cardiovasc Surg
32 LVO < 170 mls/kg < 1000 g n= 23 > 1000 g n= 23 p 0 1(43) (4.3) 0(0) (13) 4 (17.4) (30.4) 2(87) (8.7) (4.3) 3 (13) 0.61 FS < 25% 0 0 (0) 0 (0) (8.7) 3 (13) (30.4) 1 (4.3) (4.3) 3 (13) 0.61 Data presented as number (%)
33 Stress-Velocity < 1000g Stress-Velocity > 1000g c) mvcfc (circ/se mvcfc (circ/se ec) ESWS (g/cm 2 ) Baseline 8 hours ESWS (g/cm 2 ) Baseline 8 hours Time (h) y x r Time (h) y X r *
34




35 Speckle Tracking and Strain Analysis






36 Strain Analysis and PDA Ligation Post Sept Lat Inf Ant Four Chamber Two Chamber AntSept Three Chamber
37 Global Strain (n=15) Global Longitudinal Strain (%)


38 Segmental Strain
39 . Tissue Doppler Imaging g
40 Transmitral Flow A wave E wave IVCT IVRT Transmitral flow Aortic flow Transmitral flow
41 Tissue Doppler measurements during the three time points Preoperative 1 hour post op 18 hours post op MV Annulus S 53(11)* 5.3 (1.1) 34(09)* 3.4 (0.9) 41(09) 4.1 (0.9) < E 8.8 (4.3)* 4.1 (1.7)* 4.5 (1.6) <0.001 A 9.5 (3.3)* 6.3 (2.6)* 5.4 (1.6) IVS TV Annulus S 5.0 (0.7)* 3.3 (0.9)* 4.0 (0.5)* <0.001 E 6.4 (1.9)* 4.1 (2.1)* 4.9 (2.0) A 7.0 (1.3) * 5.3 (1.4)* 5.7 (1.3) <0.001 S 7.8 (2.0)* 6.7 (2.2) 6.3 (1.2)* E 9.2 (3.4)* 7.4 (3.2)* 8.3 (3.4) 0.17 A 10.4 (2.6) 14.1 (21.1) 9.1 (2.6) 0.41 p
42 S ` Isovolemic relaxation E A` ` Isovolemic contraction
43 Isovolemic Phases: Mitral valve Pre Op 1 hour post op 24 hour post op IVCT (ms) 36.2 [ ]* 54.8 [ ]* 47.9 [ ]* < IVC velocity 5.1 [ ]* 7.2 [ ]* 5.2 [ ] (cm/s) IVRT (ms) 43.0 [ ]* 70.2 [ [ ] ]* IVR velocity 5.0 [ ] * 3.0 [ ] * 3.0 [ ] <0.001 (cm/s) MPI 0.47 [ ]* 0.82 [ ]* 0.73 [ ]* <0.001


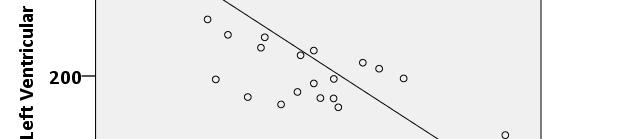

44 Isovolumic Contractile Time Pearson: r=0.799, p<0.001 Pearson: r=-0.739, p<0.001
45 Afterload DIASTOLIC PERFORMANCE Duration of Ventricular Relaxation IVRT, IVCT, Tau index E wave Passive filling with increased residual atrial blood Abnormal cardiac output Ishida 1986 Circulation
46 Scenario II 7 day old (24/40 weeks) referred for PDA ligation Issues Anuric, creatinine 260 mmol/l Refractory shock (Dobutamine 20 & Dopamine10 μg/kg/min) Metabolic acidosis ( ) with lactate 6-10 mmol/l 2d ECHO 3.8 mm HSDA with unrestrictive L-R flow Dilated LA and LV, cardiac output 380 mls/kgmin Reversed end-diastolic flow in SMA, MCA & renal artery
47 BENEFIT HARM Optimize perfusion Lung compliance LV dysfunction
48 Study III Can high h risk patients t be identified d earlier?
49 Phase I Understand the Physiology! PDA Ligation Systemic bld flow (LV afterload) pulmonary bld flow (LV preload) Impaired LV relaxation (diastolic dysfunction) Impaired LV contraction (systolic dysfunction) Low Cardiac Output State + Clinical decompensation Noori 2007 J Pediatrics, McNamara et al J Thorac Cardiovasc Surg

")


50 Post-Ligation Cardiac Syndrome Clinical instability Increased morbidity PDA ligation High risk pts prophylaxis hypotension (30%) ventilation (45%) oxygen (60% ) Teixeira et al. J Perinat 2008 Natarajan et al. Am J Perinatol 2010 Harting et al. J Invest Surg 2008 Schmidt et al. Pediatrics 2007
51 Left Ventricular Output t8 [mls/kg/ /min] LVI r = 0.63, p< LVI - t1 [mls/kg/min] Sahni 2008 PAS








52 Outcomes for infants with LVO< 200 mls/min/kg on first postoperative ECHO 75% Critically low LVO Sensitivity 1.0 Specificity.86 42% 38% Systolic hypotension Need for inotropes Sensitivity.83 Sensitivity 1.0 Specificity.72 Specificity.71 Jain 2011 J Pediatr (in press)
53 Targeted neonatal ECHO directed therapy program introduced d in January TnECHO at 1 hour post surgery LVO < 200 mls/min/kg MILRINONE infusion at 0.33 mics/kg/min LVO > 200 ml/min/kg continue observation 2. Comparative evaluation of postoperative course before and after introduction of new program 3. Matched for gestation and LVO Jain 2011 J Pediatr
54 Study V To compare the rate and components of PLCS in infants who have undergone PDA ligation before and after the introduction of targeted neonatal echocardiography (TnECHO) directed therapy program
55 Comparison of clinical stability
56 Primary outcome Outcome PLCS n (%) Epoch I (N=25) Epoch II (N=27) p ARR NTT 11 (44%) 3 (11%) *PLCS: composite outcome of need of inotropes and either oxygenation or ventilation failure in the absence of any other etiology Jain 2011 J Pediatr (in press)
57 Secondary Outcomes Outcome Epoch I (N=25) Epoch II (N=27) p ARR NTT Need for inotropes n (%) Oxygenation failure n (%) Ventilation failure n (%) Corticosteroids use n (%) 14 (56%) 5 (19%) (52%) 7 (26%) (48%) 4 (15%) (16%) 0.03 na na
58 Conclusion Targeted prophylactic milrinone i therapy after PDA ligation for babies with LVO <200 ml/min/kg / at 1 hour appears safe and associated with improved hemodynamic and respiratory stability and reduced the need for inotropes and steroids

59 Evolution of post operative care TnECHO, dobutamine Use of vasodilators, PLCS ECHO Research/analysis TnECHO Directed Therapy ACTH
60 BENEFIT HARM Optimize perfusion Lung compliance LV dysfunction
61 Focused ICU care Prophylactic milrinone (afterload reduction) Serial functional echocardiography Intermediary outcome Off cardiotropes within 72 hours Creatinine 125 within 12 hours of surgical intervention, normal by day 5 Extubated 10 days after surgical intervention Uneventful neonatal course
62 Preterm infant ADVERSE OUTCOME PDA ligation Hemodynamically significant DA Neonatal morbidities
63 Preterm infant Developmental / maturational factors Co-treatments ADVERSE OUTCOME Neonatal morbidities HSDA cerebral blood flow cerebral oxygen saturation Altered EEG IVH White matter injury PDA ligation ADVERSE OUTCOME cardiac output cerebral oxygen saturation ADVERSE OUTCOME
64 PDA ligation and aeeg - 4 hours PDA LIGATION 4 hours 8 hours 24 hours aeeg ECHO Clinical





65





66 Normal trace Moderately abnormal trace Severely abnormal trace
67
68 Pre op 4h 8h 24h p 2D ECHO LVO (ml/min/kg) 390 ( ) 203 ( ) * 233 ( ) * 280 ( ) * <0.001 LVFS 41± ±8.9 34±6.9 38±8.3 NS aeeg Lower border (μv) 4.2 (3.2-5) 3 ( ) * 3 ( ) * 3.5 ( ) 0.01 Upper border (μv) 24.1 ( ) 9.4 ( ) 7.2 (5.5-12) 9.4 (7.1-14) 0.02 Median % change in lower band voltage was 26% Altered lower bandwidth was associated with gestation and PDA diameter on univariate analysis
69 Conclusions PDA ligation was associated with altered cerebral electrical activity independent of any change in LVO.
70 Implications for clinical practice PDA ligation may be followed by postoperative cardiorespiratory instability Risk related to postnatal age, weight < 1000 grams, preoperative need for inotropes Need for early identification of infants at increased risk of PLCS Early fecho (1 hour) Targeted prophylaxis (LVO<200 mls/min/kg) / appears promising Rationalization of candidates for PDA ligation Rationalization of candidates for PDA ligation needed
71 Ductal Staging McNamara 2007 Arch Dis Child
72 Benefits of this approach Streamline Innocent bystanders from Pathological l cases - ligation rates [82/year (2005) to 30 /year (2019)] - Prevent transfers or cancellations PDA Ligation [Toronto] Categorization & Prioritization - determine urgency and level of intervention Ra ate Facilitates a more physiologic approach Evaluate response to therapy and better define responders Year El-Khuffash 2011 J Pediatr
73
74 Jhaveri 2010 J Pediatr
75 Future Directions Predictive value of troponin in the setting of PDA ligation Evaluation of neonates undergoing g PDA ligation using MRI
76
77 Special Thanks Neonatal Research Fellows Arvind Sehgal Lilian Teixeira Sandesh Shivananda Emer Finan Research Assistants t Wendy Mak Derek Stephens (Statistical support) Derek Stephens (Statistical support) Glen Van Arsdell & CVS team
78 aeeg and PDA ligation Lemmers 2010 ADC
79






80






81 Biomarkers and Ductal significance B-Natriuretic Peptide Troponin T Reflective of left heart volume loading and systemic hypoperfusion respectively Beneficial if lack of access to serial echocardiography Useful as an adjunct to clinical care
82 NTpBNP and PDA El Khuffash A, et al. ArchDis Child Fetal Neonatal Ed 2007.
83 Troponin & HSDA Al Khuffash 2008 Arch Dis Child


![53 VTI [c cm] 3 2 1 0 1.](/docs-images/92/108919123/images/84-2.jpg "5 2.0 2.5 3.0 3.5 4.0 4.")


84 CORONARY ARTERY FLOW and HSDA Sehgal 2007 E-PAS CA p< , r=053 =0.53 VTI [c cm] Transductal diameter [mm] CA:LVO flow ratio Time [hrs] p = 0.001
85 Plasma ctnt and NTpBNP in first 48 hours of life El-Khuffash Arch Dis Child (In press)
86 Figure 2: ROC for ctnt, NTpBNP and PDA score in predicting outcome El-Khuffash Arch Dis Child (In press) Area p value 95% CI Cut off Sensitivity Specificity NTpBNP 0.84 < % 75% ctnt 0.92 < % 79% PDA Score % 79%
87 Baseline Hemodynamic and Respiratory Characteristics ti at the three time points Preoperativ 1 hour post 18 hours post p e op op Heart Rate 157 (13) 149 (13) 156 (20) 0.23 Systolic BP (mmhg) 56 (9) 57 (12) 57(17) 0.67 Diastolic BP (mmhg) 25 (4)* 37 (8)* 33 (10) <0.00 Mean BP (mmhg) 38 (6) 43 (9) 42 (12) 0.21 MAP (cmh2o) 9.5 (1.6) 9.5 (2.2) 9.6 (2.4) Oxygen requirement 36 (11) 36 (15) 40 (18) 0.67 (%)
88 Global and segmental strain Preoperative 1 hour 18 hours p Global l Strain (-4.4)* 44)* (-3.6)* 36)* (-3.5)* 35)* < Septal Wall (-3.6)* (-4.4)* (4.4)* <0.001 Lateral Wall (-2.5)* -9.9 (-5.1) * (-4.8) <0.001 Inferior Wall (-3 3.8) 8)* (-5 5.3) 3)* (-3 3.5) 5)* < Posterior Wall (-5.9)* (-4.3)* (-6.4) Anterior Wall (-3.6)* -9.5 (-4.5)* (-2.8) <0.001 Anteroseptal (-5.5) * (-2.9)* (-3.2) <0.001 wall


89 Pearson: r=-0.577, p=0.002
90 CA Flow & Post-ligation instability Cardiotropic Support 5 DCA VTI [cm] 4 * 3 2 Increased risk of myocardial dysfunction may relate to chronic myocardial ischemia 1 0 yes Cardiotropes no Sehgal In press J Card Thor Surg * p<0.05 vs no inotropes



91 Pearson: r=-0.515, p=0.005




92 Surfactant Hypocapnia Oxygen or Nitric oxide Hypocapnia / Alkalosis Pressors Oxygen Hypothermia PVR +++ PDA Ao SVR Ao Left Ventricle
93 Ductal Continuum INNOCENT BYSTANDER PATHOPHYSIOLOGY 3.0 mm DA, url-r flow 3.0 mm DA, url-r flow Full feeds HFOV [MAP 16, FiO2 0.8] Room air Pulmonary hemorrhage Systemic Hypotension Anuria, Creatinine 360 Abdominal distension
94 Relationship between global longitudinal strain and LV fractional shortening, LVEDD and LVO
95 Risk factors for Cardiotropic support Parameter (n=166) p value surgery Surgery < 28 days of life 0.04 Pre-operative shock requiring cardiotropic i support 0.02 PDA size, preoperative LV systolic performance not predictive of postoperative deterioration Finan et al
Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation?
 can help prevent Postoperative Cardiorespiratory instability following PDA ligation?") Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation? Amish Jain, Mohit Sahni, Afif El Khuffash, Arvind Sehgal, Patrick J
Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation? Amish Jain, Mohit Sahni, Afif El Khuffash, Arvind Sehgal, Patrick J
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC & SBH Child Health Standards Committee Pages: 1 of 6 Supercedes: N/A 1.0 PURPOSE and INTENT
NEONATAL CLINICAL PRACTICE GUIDELINE Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC & SBH Child Health Standards Committee Pages: 1 of 6 Supercedes: N/A 1.0 PURPOSE and INTENT
Physiologic Aspects of the Preterm Circulation
 Staff Neonatologist, Hospital for Sick Children, Toronto Physiologic Aspects of the Preterm Circulation Patrick McNamara Associate Professor of Pediatrics, University of Toronto The Vulnerable Neonate
Staff Neonatologist, Hospital for Sick Children, Toronto Physiologic Aspects of the Preterm Circulation Patrick McNamara Associate Professor of Pediatrics, University of Toronto The Vulnerable Neonate
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Physiologic Based Management of Circulatory Shock Kuwait 2018
 Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
State of Florida Systemic Supportive Care Guidelines. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
Enhancing Management of Circulatory Instability in Neonates
 Associate Scientist Enhancing Management of Circulatory Instability in Neonates Patrick McNamara Associate Professor of Pediatrics The Vulnerable Neonate How will you ensure cardiovascular stability? Myths
Associate Scientist Enhancing Management of Circulatory Instability in Neonates Patrick McNamara Associate Professor of Pediatrics The Vulnerable Neonate How will you ensure cardiovascular stability? Myths
Hypotension in the Neonate
 Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
MANAGEMENT OF CIRCULATORY FAILURE
 MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Perioperative Management of TAPVC
 Perioperative Management of TAPVC Professor Andrew Wolf Rush University Medical Center,Chicago USA Bristol Royal Children s Hospital UK I have no financial disclosures relevant to this presentation TAPVC
Perioperative Management of TAPVC Professor Andrew Wolf Rush University Medical Center,Chicago USA Bristol Royal Children s Hospital UK I have no financial disclosures relevant to this presentation TAPVC
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
NOT YET!! PDA - Pathological or innocent physiologic bystander? PDA From Physiology to Treatment 9/8/2014
 PDA - Pathological or innocent physiologic bystander? PDA From Physiology to Treatment Martin Kluckow MBBS FRACP PhD CCPU Associate Professor Royal North Shore Hospital & University of Sydney, Australia
PDA - Pathological or innocent physiologic bystander? PDA From Physiology to Treatment Martin Kluckow MBBS FRACP PhD CCPU Associate Professor Royal North Shore Hospital & University of Sydney, Australia
Functional Echocardiography in the Preterm infant. Adam James
 Functional Echocardiography in the Preterm infant Adam James A thesis submitted to Trinity College Dublin in fulfilment of the requirements for the degree Medical Doctorate (M.D.) September 2017 Rotunda
Functional Echocardiography in the Preterm infant Adam James A thesis submitted to Trinity College Dublin in fulfilment of the requirements for the degree Medical Doctorate (M.D.) September 2017 Rotunda
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations. Eric M. Graham, MD
 Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
I intend to discuss an unapproved/investigative use of a commercial product/device in my presentation
 Istvan Seri MD PhD Center for Fetal and Neonatal Medicine USC Division of Neonatal Medicine Children Hospital Los Angeles and LAC+USC Medical Center Keck School of Medicine University of Southern California
Istvan Seri MD PhD Center for Fetal and Neonatal Medicine USC Division of Neonatal Medicine Children Hospital Los Angeles and LAC+USC Medical Center Keck School of Medicine University of Southern California
PPHN (see also ECMO guideline)
") Children s Acute Transport Service Clinical Guidelines PPHN (see also ECMO guideline) Document Control Information Author P Brooke E.Randle Author Position Medical Student Consultant Document Owner E.
Children s Acute Transport Service Clinical Guidelines PPHN (see also ECMO guideline) Document Control Information Author P Brooke E.Randle Author Position Medical Student Consultant Document Owner E.
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
WHY ADMINISTER CARDIOTONIC AGENTS?
 Cardiac Pharmacology: Ideas For Advancing Your Clinical Practice The image cannot be displayed. Your computer may not have enough memory to open the image, or Roberta L. Hines, M.D. Nicholas M. Greene
Cardiac Pharmacology: Ideas For Advancing Your Clinical Practice The image cannot be displayed. Your computer may not have enough memory to open the image, or Roberta L. Hines, M.D. Nicholas M. Greene
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Patent Ductus Arteriosus: Philosophy or Pathology?
 Patent Ductus Arteriosus: Philosophy or Pathology? Disclosure Ray Sato, MD is a speaker for Prolacta Biosciences, Inc. This presentation will discuss off-label uses of acetaminophen and ibuprofen. RAY
Patent Ductus Arteriosus: Philosophy or Pathology? Disclosure Ray Sato, MD is a speaker for Prolacta Biosciences, Inc. This presentation will discuss off-label uses of acetaminophen and ibuprofen. RAY
1
 1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
Disclosures. ICU Management of Advanced Lung Disease 5/9/2015. No Disclosures. All pictures from commercial sources
 Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Update on mangement of patent ductus arteriosus in preterm infants. Dr. Trinh Thi Thu Ha
 Update on mangement of patent ductus arteriosus in preterm infants Dr. Trinh Thi Thu Ha Outline 1. Overview of PDA 2. Timing of screening PDA? 3. When to treat PDA? Timing of ductal closure Prenatal
Update on mangement of patent ductus arteriosus in preterm infants Dr. Trinh Thi Thu Ha Outline 1. Overview of PDA 2. Timing of screening PDA? 3. When to treat PDA? Timing of ductal closure Prenatal
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
I have no relevant financial relationships with the manufacturers of any. commercial products and/or provider of commercial services discussed in
 I have no relevant financial relationships with the manufacturers of any commercial products and/or provider of commercial services discussed in this activity I do intend to discuss an unapproved/investigative
I have no relevant financial relationships with the manufacturers of any commercial products and/or provider of commercial services discussed in this activity I do intend to discuss an unapproved/investigative
Neonatal Shock. Imbalance between tissue oxygen delivery and oxygen consumption
 Neonatal Shock Moira Crowley, MD Assistant Professor, Pediatrics Co-director, Neonatal ECMO Program Rainbow Babies and Children s Hospital Case Western Resverve University School of Medicine 1 Objectives
Neonatal Shock Moira Crowley, MD Assistant Professor, Pediatrics Co-director, Neonatal ECMO Program Rainbow Babies and Children s Hospital Case Western Resverve University School of Medicine 1 Objectives
ino in neonates with cardiac disorders
 ino in neonates with cardiac disorders Duncan Macrae Paediatric Critical Care Terminology PAP Pulmonary artery pressure PVR Pulmonary vascular resistance PHT Pulmonary hypertension - PAP > 25, PVR >3,
ino in neonates with cardiac disorders Duncan Macrae Paediatric Critical Care Terminology PAP Pulmonary artery pressure PVR Pulmonary vascular resistance PHT Pulmonary hypertension - PAP > 25, PVR >3,
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Valutazione del neonato con sospetta ipertensione polmonare
 Valutazione del neonato con sospetta ipertensione polmonare Cardiologia Pediatrica Seconda Università degli Studi di Napoli A.O. R.N. dei Colli-Monaldi Napoli Hypoxiemic infant Full or near-term neonate
Valutazione del neonato con sospetta ipertensione polmonare Cardiologia Pediatrica Seconda Università degli Studi di Napoli A.O. R.N. dei Colli-Monaldi Napoli Hypoxiemic infant Full or near-term neonate
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Disclosure Information : No conflict of interest
 Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation.
 Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation. Evaluation of RVAD Function. Ioannis A Paraskevaidis Attikon University Hospital Historical Perspective
Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation. Evaluation of RVAD Function. Ioannis A Paraskevaidis Attikon University Hospital Historical Perspective
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal
 Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University
 Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
Diastology State of The Art Assessment
 Diastology State of The Art Assessment Dr. Mohammad AlGhamdi Assistant professor, KSAU-HS Consultant Cardiologist King AbdulAziz Cardiac Center Ministry of National Guard Health Affairs Diagnostic Clinical
Diastology State of The Art Assessment Dr. Mohammad AlGhamdi Assistant professor, KSAU-HS Consultant Cardiologist King AbdulAziz Cardiac Center Ministry of National Guard Health Affairs Diagnostic Clinical
9/16/2012. Progression of Shock. Blood pressure: Pathophysiology & Clinical Management
 Mean BP (mm Hg) 9/16/212 September 2, 14: 6 min Blood pressure: Pathophysiology & Clinical Management Shahab Noori, MD Associate Professor of Pediatrics Division of Neonatology Progression of Shock BP
Mean BP (mm Hg) 9/16/212 September 2, 14: 6 min Blood pressure: Pathophysiology & Clinical Management Shahab Noori, MD Associate Professor of Pediatrics Division of Neonatology Progression of Shock BP
Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling. What is the pathophysiology at presentation?
 Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling What is the pathophysiology at presentation? Ventricular-arterial coupling elastance Central arterial pressure
Mechanisms of heart failure with normal EF Arterial stiffness and ventricular-arterial coupling What is the pathophysiology at presentation? Ventricular-arterial coupling elastance Central arterial pressure
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Title: Integrated Evaluation of Neonatal Hemodynamics (IENH) and Targeted Echocardiogram Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC &
NEONATAL CLINICAL PRACTICE GUIDELINE Title: Integrated Evaluation of Neonatal Hemodynamics (IENH) and Targeted Echocardiogram Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC &
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY
 가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension
 ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
IABP to prevent pulmonary edema under VA-ECMO
 IABP to prevent pulmonary edema under VA-ECMO Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie,
IABP to prevent pulmonary edema under VA-ECMO Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie,
Deok Young Choi, Gil Hospital, Gachon University NEONATES WITH EBSTEIN S ANOMALY: PROBLEMS AND SOLUTION
 Deok Young Choi, Gil Hospital, Gachon University NEONATES WITH EBSTEIN S ANOMALY: PROBLEMS AND SOLUTION Carpentier classification Chauvaud S, Carpentier A. Multimedia Manual of Cardiothoracic Surgery 2007
Deok Young Choi, Gil Hospital, Gachon University NEONATES WITH EBSTEIN S ANOMALY: PROBLEMS AND SOLUTION Carpentier classification Chauvaud S, Carpentier A. Multimedia Manual of Cardiothoracic Surgery 2007
Weeks 1-3:Cardiovascular
 Weeks 1-3:Cardiovascular Cardiac Output The total volume of blood ejected from the ventricles in one minute is known as the cardiac output. Heart Rate (HR) X Stroke Volume (SV) = Cardiac Output Normal
Weeks 1-3:Cardiovascular Cardiac Output The total volume of blood ejected from the ventricles in one minute is known as the cardiac output. Heart Rate (HR) X Stroke Volume (SV) = Cardiac Output Normal
Failing right ventricle
 Failing right ventricle U. Herberg 1, U. Gembruch 2 1 Pediatric Cardiology, 2 Prenatal Diagnostics and Fetal Therapy, University of Bonn, Germany Prenatal Physiology Right ventricle dominant ventricle
Failing right ventricle U. Herberg 1, U. Gembruch 2 1 Pediatric Cardiology, 2 Prenatal Diagnostics and Fetal Therapy, University of Bonn, Germany Prenatal Physiology Right ventricle dominant ventricle
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Left atrial function. Aliakbar Arvandi MD
 In the clinic Left atrial function Abstract The left atrium (LA) is a left posterior cardiac chamber which is located adjacent to the esophagus. It is separated from the right atrium by the inter-atrial
In the clinic Left atrial function Abstract The left atrium (LA) is a left posterior cardiac chamber which is located adjacent to the esophagus. It is separated from the right atrium by the inter-atrial
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Neonatal/Pediatric Cardiopulmonary Care. Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN. Other. Other Diseases
 PPHN. Other. Other Diseases") Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
Stabilization and Transportation guidelines for Neonates and infants with Heart disease:
 Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Objectives. Diastology: What the Radiologist Needs to Know. LV Diastolic Function: Introduction. LV Diastolic Function: Introduction
 Objectives Diastology: What the Radiologist Needs to Know. Jacobo Kirsch, MD Cardiopulmonary Imaging, Section Head Division of Radiology Cleveland Clinic Florida Weston, FL To review the physiology and
Objectives Diastology: What the Radiologist Needs to Know. Jacobo Kirsch, MD Cardiopulmonary Imaging, Section Head Division of Radiology Cleveland Clinic Florida Weston, FL To review the physiology and
Conflicts of Interest
 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Ruminations about the Past, Present, and Future
 Ruminations about the Past, Present, and Future Raymond L. Fowler, MD, FACEP, DABEMS Professor and Chief Division of Emergency Medical Services Department of Emergency Medicine UT Southwestern Medical
Ruminations about the Past, Present, and Future Raymond L. Fowler, MD, FACEP, DABEMS Professor and Chief Division of Emergency Medical Services Department of Emergency Medicine UT Southwestern Medical
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION
 LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Short-Term Outcome Of Different Treatment Modalities Of Patent Ductus Arteriosus In Preterm Infants. Five Years Experiences In Qatar
 ISPUB.COM The Internet Journal of Cardiovascular Research Volume 7 Number 2 Short-Term Outcome Of Different Treatment Modalities Of Patent Ductus Arteriosus In Preterm Infants. Five Years Experiences In
ISPUB.COM The Internet Journal of Cardiovascular Research Volume 7 Number 2 Short-Term Outcome Of Different Treatment Modalities Of Patent Ductus Arteriosus In Preterm Infants. Five Years Experiences In
Maternal and Fetal Physiology
 Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Fetal cardiac function: what to use and does it make a difference?
 17 th International Conference on Prenatal Diagnosis and Therapy Lisbon, June 2013 Fetal cardiac function: what to use and does it make a difference? Fàtima Crispi Department of Maternal-Fetal Medicine,
17 th International Conference on Prenatal Diagnosis and Therapy Lisbon, June 2013 Fetal cardiac function: what to use and does it make a difference? Fàtima Crispi Department of Maternal-Fetal Medicine,
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)
of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)") Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Imaging to Measure Cardiac Contractility: Current and Future. Safety Pharmacology Society 2012 Jon Heyen on behalf of Bob Coatney
 Imaging to Measure Cardiac Contractility: Current and Future Safety Pharmacology Society 2012 Jon Heyen on behalf of Bob Coatney Background / Context / Scope How do we bridge? Contractility = Force generated
Imaging to Measure Cardiac Contractility: Current and Future Safety Pharmacology Society 2012 Jon Heyen on behalf of Bob Coatney Background / Context / Scope How do we bridge? Contractility = Force generated
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children?
 Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
Topics to be Covered. Cardiac Measurements. Distribution of Blood Volume. Distribution of Pulmonary Ventilation & Blood Flow
 Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH
 Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH Javier Jimenez MD PhD FACC Director, Advanced Heart Failure and Pulmonary Hypertension Miami Cardiac & Vascular Institute
Squeeze, Squeeze, Squeeze: The Importance of Right Ventricular Function and PH Javier Jimenez MD PhD FACC Director, Advanced Heart Failure and Pulmonary Hypertension Miami Cardiac & Vascular Institute
Hybrid Stage I Palliation / Bilateral PAB
 Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Ventriculo-arterial coupling and diastolic elastance. MasterclassIC Schiermonnikoog 2015
 Ventriculo-arterial coupling and diastolic elastance MasterclassIC Schiermonnikoog 2015 Ventriculo-arterial coupling Dynamic interaction between heart and systemic circulation (modulation of compliance
Ventriculo-arterial coupling and diastolic elastance MasterclassIC Schiermonnikoog 2015 Ventriculo-arterial coupling Dynamic interaction between heart and systemic circulation (modulation of compliance
First Trimester Fetal Echocardiography: Insight Into the Fetal Circulation
 First Trimester Fetal Echocardiography: Insight Into the Fetal Circulation Lisa K. Hornberger, MD Fetal & Neonatal Cardiology Program Department of Pediatrics, Division of Cardiology Department of Obstetrics
First Trimester Fetal Echocardiography: Insight Into the Fetal Circulation Lisa K. Hornberger, MD Fetal & Neonatal Cardiology Program Department of Pediatrics, Division of Cardiology Department of Obstetrics
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A2b. PDA Management--A Reflection on the Evidence: Does it Help with Management? Session Summary. Session Objectives. References.
 FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UTE AND REVIEW A2b Management--A Reflection on the Evidence: Does it Help with Management? Alfonso Vargas, MD Neonatologist Pediatrix Medical Group, Tampa, FL
FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UTE AND REVIEW A2b Management--A Reflection on the Evidence: Does it Help with Management? Alfonso Vargas, MD Neonatologist Pediatrix Medical Group, Tampa, FL
Is there an Optimal Mode of Ventilation Following Paediatric Cardiac Surgery? Dr Steve Ponde Busamed Modderfontein Hospital
 Is there an Optimal Mode of Ventilation Following Paediatric Cardiac Surgery? Dr Steve Ponde Busamed Modderfontein Hospital There have been many advances in the perioperative care of adults and children
Is there an Optimal Mode of Ventilation Following Paediatric Cardiac Surgery? Dr Steve Ponde Busamed Modderfontein Hospital There have been many advances in the perioperative care of adults and children
INTRAUTERINE GROWTH RESTRICTION AND ITS IMPACT ON CARDIAC FUNCTION AND ARTERIAL COMPLIANCE IN THE YOUNG CHILD
 INTRAUTERINE GROWTH RESTRICTION AND ITS IMPACT ON CARDIAC FUNCTION AND ARTERIAL COMPLIANCE IN THE YOUNG CHILD Edgar Jaeggi, MD, FRCPC Associate Scientist, RI Fetal Cardiac Program, The Hospital for Sick
INTRAUTERINE GROWTH RESTRICTION AND ITS IMPACT ON CARDIAC FUNCTION AND ARTERIAL COMPLIANCE IN THE YOUNG CHILD Edgar Jaeggi, MD, FRCPC Associate Scientist, RI Fetal Cardiac Program, The Hospital for Sick
Incorporating the New Echo Guidelines Into Everyday Practice
 Incorporating the New Echo Guidelines Into Everyday Practice Clinical Case RIGHT VENTRICULAR FAILURE Gustavo Restrepo MD President Elect Interamerican Society of Cardiology Director Fellowship Training
Incorporating the New Echo Guidelines Into Everyday Practice Clinical Case RIGHT VENTRICULAR FAILURE Gustavo Restrepo MD President Elect Interamerican Society of Cardiology Director Fellowship Training
Pediatric Neurointervention: Vein of Galen Malformations
 Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
ACUTE HEART FAILURE. Julie Gorchynski MD, MSc, FACEP, FAAEM. Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014
 ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
Objectives Part 1. Objectives Part 2. Fetal Circulation Transition to Postnatal Circulation Normal Cardiac Anatomy Ductal Dependence and use of PGE1
 Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Premature Infants with Patent Ductus Arteriosus and Res iratory Distress: Selection for mdap Ligation
 Premature Infants with Patent Ductus Arteriosus and Res iratory Distress: Selection for mdap Ligation George S. Hall, M.D., James A. Helmsworth, M.D., J. Tracy Schreiber, M.D., Jens G. Rosenkrantz, M.D.,
Premature Infants with Patent Ductus Arteriosus and Res iratory Distress: Selection for mdap Ligation George S. Hall, M.D., James A. Helmsworth, M.D., J. Tracy Schreiber, M.D., Jens G. Rosenkrantz, M.D.,
Ventricular Interactions in the Normal and Failing Heart
 Ventricular Interactions in the Normal and Failing Heart Congenital Cardiac Anesthesia Society 2015 Pressure-volume relations Matched Left ventricle to low hydraulic impedance Maximal stroke work limited
Ventricular Interactions in the Normal and Failing Heart Congenital Cardiac Anesthesia Society 2015 Pressure-volume relations Matched Left ventricle to low hydraulic impedance Maximal stroke work limited
Index. K Knobology, TTE artifact, image resolution, ultrasound, 14
 A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
Fluid Boluses in Preterm Babies with Poor Perfusion: A Hot Potato. Win Tin The James Cook University Hospital University of Durham
 Fluid Boluses in Preterm Babies with Poor Perfusion: A Hot Potato Win Tin The James Cook University Hospital University of Durham Introduction Fluid Bolus/es (Intravascular Volume Expansion) - One of the
Fluid Boluses in Preterm Babies with Poor Perfusion: A Hot Potato Win Tin The James Cook University Hospital University of Durham Introduction Fluid Bolus/es (Intravascular Volume Expansion) - One of the
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
British Society of Echocardiography
 British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education