Pediatric TB Intensive Houston, Texas
|
|
|
- Curtis Patrick
- 6 years ago
- Views:
Transcription
1 Pediatric TB Intensive Houston, Texas November 13, 2009 Treatment of Pediatric TB Jeffrey R. Starke, M.D. November 13, 2009 MANAGEMENT OF CHILDHOOD TUBERCULOSIS Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine 1
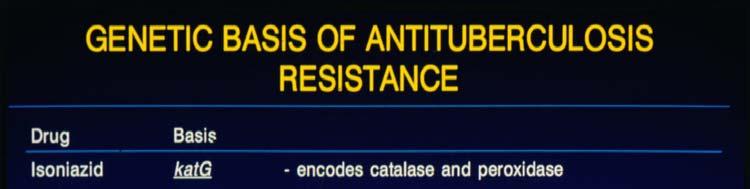
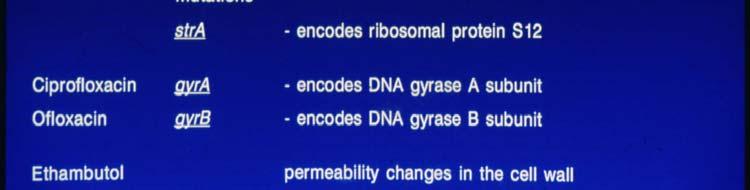
2 DRUG RESISTANCE IN TUBERCULOSIS The development of drug resistance in M. tuberculosis is the result of a conspiracy among the organism, the patient, t the doctor and the healthcare system! DRUG RESISTANCE IN MYCOBACTERIUM TUBERCULOSIS genetic loci for resistance on chromosome, unlinked resistance of drugs independent frequency of mutations at loci is known more likely to have mutations when mycobacterial population is larger : infection vs. disease 2

3 3



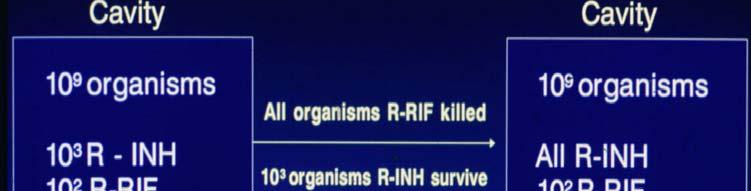
4 TREATMENT OF TUBERCULOSIS More bugs, more drugs! Question: When does tuberculosis infection turn into tuberculosis disease? When do we cross the threshold or using more than one drug? 4
5 TB DRUGS IN CHILDREN Isoniazid: [10 15 mg/kg/day] Well tolerated with few AEs Both hepatitis and neuritis are rare Better tolerated with food in stomach Poor tolerance of suspension > 5 kg Rifampin: [10 15 mg/kg/day] Well tolerated; only rare AEs Watch for contact lenses Can t use OCPs for birth control TB DRUGS IN CHILDREN Pyrazinamide: [30 40 mg/kg/day] Large pill, no standard d suspension itching > joint pain > hepatitis Ethambutol: [20 mg/kg/day] Ocular toxicity very, very rare Watch for renal disease [elimination] Now standard 4 th drug for children 5
6 TB DRUGS IN CHILDREN Aminoglycosides: Mostly CNS, drug-resistant resistant TB Amikacin preferred for CNS [more resistance to streptomycin] Oto- and renal toxicity possible Ethionamide: [15 mg/kg/day] Excellent drug for CNS TB Difficult-to-use dosage form GI intolerance, but less than in adults TB DRUGS IN CHILDREN Fluoroquinolones: Used for drug-resistant resistant TB or intolerance to standard drugs Few studies, mostly ciprofloxacin Dosages unknown for moxafloxacin and gatifloxacin Levofloxacin: twice daily dosing for children < 5 years of age 6
7 DIRECTLY OBSERVED THERAPY FOR TUBERCULOSIS means a dispassionate 3rd party is actually present when medications are taken with every dose standard of care in U.S. for treating tuberculosis disease desirable for high risk infections - newborns and infants, household contacts, HIV - infected or immune compromised TUBERCULOSIS IN CHILDREN TREATING EXPOSED CHILDREN Very high rate of infection Takes up to 3 months for the skin test to turn positive U.S. studies 10% to 20% of childhood TB cases can be prevented if children exposed in a household receive isoniazid Assume young children are infected until proven they are not 7
8 TREATING TB EXPOSED CHILDREN Usually treat for 8 to 10 weeks after exposure has been broken by loss of contact or treatment Must follow both the patient and the source case [sputum conversion, drug susceptibility pattern, contact] Infants:? TST or IGRA reliable if child < 6 months of age [little data] 8
9 TREATMENT OF LTBI IN CHILDREN 9 months of isoniazid (daily or twice weekly under DOT) is only accepted regimen INH-resistance/intolerance rifampin for 4-6 months Multidrug-resistance lid resistance consult an expert Use isoniazid unless there is documented exposure to a specific case of drug-resistant resistant TB ALTERNATIVE REGIMENS FOR LTBI INH for 6 months Rifampin for 4-6 months INH + RIF for 3-4 months 9
10 PEARLS OF WISDOM FOR TREATING LTBI Use INH suspension only in children 5 kg Use DOPT for: recent contacts, infants, immune compromised When children aren t tolerating INH, the problem is more often with the parent than the child Routine LFTs only for: other liver toxic drugs, liver disease, signs or symptoms of hepatitis Pyridoxine needed only for breast- feeding infants, pregnancy, poor diets TREATMENT OF TUBERCULOSIS DISEASE IN CHILDREN Pulmonary INH, RIF for 6 months + PZA for first 2 months Add EMB initially if risk of INH resistance Can be q.day or twice weekly INH-resistant: RIF+PZA+EMB for 9 months MDR - depends on susceptibility - at least 18 months CNS, Disseminated usually start with 4 drugs (INH, RIF, PZA + EMB) usual length: 9-12 months q.day initially, may use twice weekly later 10
11 TREATMENT RULE OF THUMB FOR CNS TUBERCULOSIS Treatment for tuberculous meningitis should be started, while the work-up is being undertaken, for any child with meningitis, no obvious cause [such as a positive Gram stain] and any of: basilar enhancement, hydrocephalus, cranial nerve abnormality, infarction, possible tuberculoma TREATMENT OF TUBERCULOUS MENINGITIS Medications Always start at least 4 anti-tb drugs 1. Isoniazid 2. Rifampin 3. Pyrazinamide 4. Ethionamide or an aminoglycoside Always start corticosteroids [4-6 weeks] 11
12 TREATMENT OF TUBERCULOUS MENINGITIS Other Measures Fluid/electrolyte management Airway management Seizure control Ventriculostomy or VP shunt Physical therapy TREATMENT OF LYMPHATIC TUBERCULOSIS Biggest problem is differentiating TB from NTM adenitis and Bartonella Surgical Approach 1. Fine needle aspirate 2. Incision and drainage [Not!] 3. Excisional biopsy 12



13 TREATMENT OF LYMPHATIC TUBERCULOSIS Can use standard anti-tb regimens Relapse/recrudescence rates are fairly high Empiric regimen for mycobacterial lymphadenitis: INH+RIF+EMB+Clarithromycin [covers TB, M. bovis, many NTM] 13



14 TUBERCULOSIS IN CHILDREN IMPACT OF DRUG-RESISTANCE RESISTANCE Usually must link the child with an adult case to identify it Adults with drug-resistant resistant TB are as contagious as those with susceptible disease Disease expression ess in children the same as with susceptible strains Children tolerate and respond well to second- line drugs 14
15 PRINCIPLES OF TREATING MDR TUBERCULOSIS IN CHILDREN Exposure: often don t treat Infection: two best available drugs Disease: usually 4 to 6 drugs, best available PRINCIPLES OF TREATING DRUG- RESISTANT TB IN CHILDREN 1. Get susceptibility pattern 2. LTBI: RIF if susceptible; if resistant to both INH and RIF, use two best drugs PZA+EMB or PZA+quinolone; 9-12 mos. 3. Disease: Need 2 cidal drugs, if possible, plus at least 2 other drugs daily therapy only INH-R: 9 months of therapy MDR: at least 12 months of therapy XDR:??? 15
16 25 YEAR EXPERIENCE WITH DRUG RESISTANT TB IN CHILDREN Jeffrey Starke, MD Lydia Ong, PA-C and Andrea Cruz, MD 158 patients: 65 exposure, 55 infection, 38 disease 79 MDR-TB: 41 exposure, 28 infection, 10 disease Resistance: INH 150, RIF 103, PZA 33, EMB-27 No child with exposure or infection progressed to disease All children with disease had resolution For 76% of patients, drug resistance known at onset of treatment [contact investigation] Adverse reactions very infrequent CORTICOSTEROIDS IN PEDIATRIC TUBERCULOSIS Useful when host inflammatory response is contributing to tissue damage or dysfunction meningitis endobronchial miliary with alveolar block pericardial with constriction vertebral with spinal root irritation Can use prednisone or dexamethasone 16
17 TREATMENT OF TB IN HIV- INFECTED CHILDREN Respond well to standard regimens Use 4 drugs initially for TB disease Length of therapy 9-12 months Rifampin drug interactions a problem *can give rifampin for 1-2 months, then change to other TB drugs *can use rifabutin [though few data for children, esp. infants] TREATING TB IN IATROGENICALLY IMMUNE SUPPRESSED CHILDREN Corticosteroids, anti-tnf antibodies, cancer chemotherapy, anti-rejection drugs Need to stop the immunosuppression as much as possible for at least 4-6 weeks, longer for anti-tnf antibodies Case-by-case basis 17
18 MOST COMMON REPORTED ADVERSE REACTIONS TO ANTI-TB TB DRUGS IN CHILDREN Upset stomach [all] Loose stools [INH suspension] Decreased appetite [? all] Change in behavior [? not related] Headaches [esp. INH;? Not related] Itching [PZA] Sore joints and muscles [PZA] Signs of peripheral neuritis [INH] DEALING WITH LIVER TOXICITY IN CHILDREN More common with severe TB disease, especially early on More common with underlying liver abnormality or co-administration of hepatotoxic drugs [anticonvulsants] Most common in first two months, but can occur at any time *Warn parents: Stop drugs first, call me second [child on INH alone] 18
19 DEALING WITH LIVER TOXICITY IN CHILDREN Check liver enzymes for vomiting, abdominal pain and/or jaundice Liver sparing regimen: ethambutol, aminoglycoside, fluoroquinolone Restart drugs one at a time; check liver enzymes after 3-5 days for each PZA is most expendable drug FOLLOW-UP EVALUATIONS FOR CHILDREN WITH TUBERCULOSIS skin test stays positive forever frequent chest x-rays unnecessary: at diagnosis, 1-2 months, end of therapy follow growth & development closely adequate nutrition routine liver enzyme monitoring not necessary routine vitamin B 6 not necessary except breast-feeding, pregnant adolescents, poor diet 19
20 IMMUNE RECONSTITUTION INFLAMMATORY SYNDROME [IRIS] happens in a variety of situations when severely immunocompromised patients have rapid restoration of immune function e.g.: neutropenic cancer patients with Candidemia in HIV, a/w a variety of organisms, including mycobacteria, CMV, hepatitis B and C viruses, HSV, JC virus (progressive multifocal leucoencephalopathy), Pneumocystis, Cryptococcus, leishmaniasis, cerebral toxoplasmosis Mycobacteria account for 40% of the cases IRIS AND MYCOBACTERIA So-called paradoxical reactions occur in 2% to 23% of HIV-negative adult patients receiving treatment for tuberculosis Most common features are fever and lymph node enlargement, though respiratory failure and neurologic deterioration also occur Median time is days after TB treatment is started Abnormality is at the original site of infection in 75% of cases, at a new location in 25% Mechanism: increased tumor necrosis factor 20
21 IRIS AND MYCOBACTERIA In HIV-uninfected children treated for tuberculosis, paradoxical reactions are common Enlarged hilar/mediastinal lymph nodes, tuberculomas are most common Changes may be only radiographic or clinical - stridor, respiratory distress, seizures (tuberculoma) Natural history vs. immune reconstitution IRIS AND MYCOBACTERIA Definition: presentation or clinical deterioration of an opportunistic infection in HIV-infected patients as a direct result of the enhancement of immune responses to those pathogens during HAART Strongest clue is usually a temporal association (30-90 days) No specific laboratory test available Clinical judgment is important (but may be nonspecific) Can also be a worsening of the opportunistic infection due to poor compliance, poor absorption or drug resistance Can also be a new infection or condition 21
22 IRIS IN CHILDREN Puthanakit et al. Pediatr Infect Dis J 2006; 25:53 32/153 (21%) HIV-infected Thai children developed d IRIS after starting HAART 14/32 (44%) episodes associated with mycobacteria [3-TB, 2-BCG, 7-MAC Complex, 2-other] In 11 of 14 patients, the mycobacterial infections had not been diagnosed prior to starting HAART 7 varicella-zoster, 7HSV, 3 Cryptococcus, 1 Guillain- Barre Children who developed IRIS had significantly lower baseline CD4 lymphocyte counts PREVENTION AND TREATMENT OF IRIS Watch out! CD4 lymphocyte count < 100 cells viral load > 10 5 copies/ml? if HAART should be delayed in patients with TB Must balance risk of IRIS with risk of other opportunistic infection if CD4 count stays low and viral load stays high Adjunctive treatment - only anecdotal evidence at present Oral corticosteroids can help when severe manifestations occur ( same as TB in HIV- uninfected children!) 22
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric TB Intensive San Antonio, Texas October 14, 2013
 Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
LTBI Videos-Treatment
 LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
LTBI Videos-Treatment This program is presented by the Global Tuberculosis Institute and is based on recommendations from the Centers for Disease Control and Prevention. This is the third in a series of
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
LTBI in Special Populations John Nava, MD October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 LTBI in Special Populations John Nava, MD October 5, 2010 2 Treatment of Latent TB Infection in Special Populations John
Management of Immune Reconstitution Inflammatory Syndrome (IRIS)
") Management of Immune Reconstitution Inflammatory Syndrome (IRIS) Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the IRIS Guideline
Management of Immune Reconstitution Inflammatory Syndrome (IRIS) Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the IRIS Guideline
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]
![CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]](/thumbs/89/99628771.jpg "CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT]") CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
CHILDHOOD TUBERCULOSIS: NEW WRINKLES IN AN OLD DISEASE [FOR THE NON-TB EXPERT] QUESTION: : Which children in the United States should get a tuberculin skin test? Do questionnaires really work? Jeffrey
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Chapter 5 Treatment for Latent Tuberculosis Infection
 Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Chapter 5 Treatment for Latent Tuberculosis Infection Table of Contents Chapter Objectives.... 109 Introduction.... 111 Candidates for the Treatment of LTBI... 112 LTBI Treatment Regimens.... 118 LTBI
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Antimycobacterial drugs. Dr.Naza M.Ali lec Dec 2018
 Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Treatment of Tuberculosis
 TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents
 New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
New Approaches to the Diagnosis and Management of Tuberculosis Infection in Children and Adolescents Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea
Pre-Treatment Evaluation. Treatment of Latent TB Infection (LTBI) Initiating Treatment: Patient Education. Before initiating treatment for LTBI:
 Initiating Treatment: Patient Education. Before initiating treatment for LTBI:") Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Pre-Treatment Evaluation Before initiating treatment for LTBI: Treatment of Latent TB Infection (LTBI) Amee Patrawalla, MD Associate Professor, New Jersey Medical School Attending Physician, NJMS Global
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
Standard TB Treatment
 Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Standard TB Treatment Chris Keh, MD TB Controller, TB Prevention and Control Program, San Francisco Department of Public Health Assistant Clinical Professor, Division of Infectious Diseases, University
Pediatric Tuberculosis: The Essentials October 8, 2014
 Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives
Pediatric Tuberculosis: The Essentials Ann M Loeffler, MD Randall Children s Hospital at Legacy Emanuel Portland, Oregon Curry International TB Center Disclosures Nothing to disclose Learning Objectives
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
5. HIV-positive individuals treated with INH should receive Pyridoxine (B6) 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH
 25 mg daily or 50 mg twice/thrice weekly on the same schedule as INH") V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
V. TB and HIV/AIDS A. Standards of Treatment and Management The majority of TB treatment principles apply to persons with HIV/AIDS who require treatment for TB disease. The following points are either
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
PEDIATRIC TUBERCULOSIS. Objectives. Children are not just small adults. Pediatric Tuberculosis 1
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
Treatment of Tuberculosis Disease. Treatment of Tuberculosis. Decision to Treat Initiation of Therapy 1
 Treatment of Tuberculosis Some Highlights of Most Recent Update Treatment of Tuberculosis Disease Germaine Jacquette, MD Physician Specialist NJMS Global Tuberculosis Institute September 15, 2010 The provider
Treatment of Tuberculosis Some Highlights of Most Recent Update Treatment of Tuberculosis Disease Germaine Jacquette, MD Physician Specialist NJMS Global Tuberculosis Institute September 15, 2010 The provider
PEDIATRIC TUBERCULOSIS
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
CNS Infections in the Pediatric Age Group
 CNS Infections in the Pediatric Age Group Introduction CNS infections are frequently life-threatening In the Philippines, bacterial meningitis is one of the top leading causes of mortality in children
CNS Infections in the Pediatric Age Group Introduction CNS infections are frequently life-threatening In the Philippines, bacterial meningitis is one of the top leading causes of mortality in children
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
TB Nurse Case Management
 TB Nurse Case Management San Antonio, Texas March 2-4, 2011 Pediatric TB Andrea T. Cruz, MD, MPH March 2, 2011 Andrea Cruz, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 2-4, 2011 Pediatric TB Andrea T. Cruz, MD, MPH March 2, 2011 Andrea Cruz, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis: update 2013
 Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
TB in the Correctional Setting Florence, Arizona October 7, 2014
 TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
TB in the Correctional Setting Florence, Arizona October 7, 2014 Diagnosis and Treatment of TB Disease Renuka Khurana, MBBS, MPH October 7, 2014 Renuka Khurana, MSSB, MPH has the following disclosures
Treatment of Tuberculosis
 TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
TB Intensive Tyler, Texas June 1-3, 2009 Treatment of Tuberculosis Barbara Seaworth, MD June 3, 2009 Treatment of Tuberculosis Barbara J Seaworth MD Medical Director Heartland National TB Center 1 Purpose
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Disclosures. Current Issues and Controversies in Child and Adolescent Tuberculosis 02/24/2016. NSTC 2016 Annual Meeting
 Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
TB Intensive San Antonio, Texas May 7-10, 2013
 TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas May 7-10, 2013 TB in the HIV Patient Lisa Armitige, MD, PhD May 09, 2013 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests No relevant
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!!
 Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Gary Reubenson 16 October 2012 PAEDIATRIC TUBERCULOSIS: AN OVERVIEW IN 40 MINUTES!! DECLARATION No relevant conflicts of interest to declare OVERVIEW Burden of disease & epidemiology Pathogenesis (not
Pediatric Tuberculosis
 Pediatric Tuberculosis Rafael E. Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Seattle Children s Hospital & University of Washington Disclosures No financial conflicts
Pediatric Tuberculosis Rafael E. Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Seattle Children s Hospital & University of Washington Disclosures No financial conflicts
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
Pediatric Tuberculosis
 Pediatric Tuberculosis Rafael E. Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Seattle Children s Hospital & University of Washington Disclosures No financial conflicts
Pediatric Tuberculosis Rafael E. Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Seattle Children s Hospital & University of Washington Disclosures No financial conflicts
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Pediatric Tuberculosis
 Pediatric Tuberculosis Rafael Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Disclosures No financial conflicts Off-label use: Drugs used in typical HZRE regimens are approved
Pediatric Tuberculosis Rafael Hernandez, MD PhD Attending Physician, Instructor Pediatric Infectious Diseases Disclosures No financial conflicts Off-label use: Drugs used in typical HZRE regimens are approved
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
Treatment of Tuberculosis
 Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society of America Please note: An erratum has been published for this article. To view the erratum, please click here.
Treatment of Tuberculosis American Thoracic Society, CDC, and Infectious Diseases Society of America Please note: An erratum has been published for this article. To view the erratum, please click here.
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
6/8/2018 TB TREATMENT. Bijan Ghassemieh, MD Seattle TB Clinical Intensive Disclosures. None
 TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
Jeffrey R. Starke, M.D. has the following disclosures to make:
 AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
AAP 2018 Red Book Tuberculosis: IGRAs and Treatment of TB Infection Jeffrey R. Starke, M.D. May 31, 2018 AAP 2018 Red Book Childhood Tuberculosis: IGRAs and Treatment of TB Infection May 31, 2018 WEBINAR
Immune Reconstitution Inflammatory Syndrome. Dr. Lesego Mawela
 Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB Disease Barbara J Seaworth MD Medical Director Heartland National TB Center Professor of Medicine University of Texas Health Center Tyler Barbara J Seaworth MD has
Research in Tuberculosis: Translation into Practice
 Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Pediatric Tuberculosis
 Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Tuberculosis (TB) Fundamentals for School Nurses
 Fundamentals for School Nurses") Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Tuberculosis (TB) Fundamentals for School Nurses June 9, 2015 Kristin Gall, RN, MSN/Pat Infield, RN-TB Program Manager Marsha Carlson, RN, BSN Two Rivers Public Health Department Nebraska Department of
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Disclosures. Outline. No disclosures or conflicts of interest to report. Special LTBI situations. H t it d id ff t
 Selected Topics in LTBI June 2, 2015 Bijan Ghassemieh, MD Senior Fellow UW Division of Pulmonary/Critical Care Disclosures No disclosures or conflicts of interest to report Outline Special LTBI situations
Selected Topics in LTBI June 2, 2015 Bijan Ghassemieh, MD Senior Fellow UW Division of Pulmonary/Critical Care Disclosures No disclosures or conflicts of interest to report Outline Special LTBI situations
10. TB and HIV Infection
 10. TB and HIV Infection The management of patients with TB and HIV infection is complex, requiring management by a multidisciplinary team which includes physicians with expertise in the treatment of both
10. TB and HIV Infection The management of patients with TB and HIV infection is complex, requiring management by a multidisciplinary team which includes physicians with expertise in the treatment of both
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Treatment and Monitoring
 Treatment and Monitoring Disclosures We have no actual or potential conflicts of interest in relation to this presentations. We have no financial relationships to disclose. Learning Objectives After this
Treatment and Monitoring Disclosures We have no actual or potential conflicts of interest in relation to this presentations. We have no financial relationships to disclose. Learning Objectives After this
Pediatric TB Theresa Barton, MD
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
Monica Manandhar. 2 ND YEAR RESEARCH ELECTIVE RESIDENT S JOURNAL Volume V, A. Study Purpose and Rationale
 Randomized Trial of lsoniazid as Secondary Prophylaxis for Prevention of Recurrent Pulmonary Tuberculosis in HIV-positive Patients After One Episode of Tuberculosis Monica Manandhar A. Study Purpose and
Randomized Trial of lsoniazid as Secondary Prophylaxis for Prevention of Recurrent Pulmonary Tuberculosis in HIV-positive Patients After One Episode of Tuberculosis Monica Manandhar A. Study Purpose and
Treatment of Latent TB Infection (LTBI)
") Treatment of Latent TB Infection (LTBI) Mahesh C. Patel, MD June 14, 2017 2014 MFMER slide-1 Mahesh C. Patel, MD Associate Professor Treatment of LTBI Department of Internal Medicine, Division of Infectious
Treatment of Latent TB Infection (LTBI) Mahesh C. Patel, MD June 14, 2017 2014 MFMER slide-1 Mahesh C. Patel, MD Associate Professor Treatment of LTBI Department of Internal Medicine, Division of Infectious
Dosage and Administration
 SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
SIRTURO product information for healthcare providers 2 WARNINGS: An increased risk of death was seen in the SIRTURO (bedaquiline) treatment group (9/79, 11.4%) compared to the placebo treatment group (2/81,
Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD
 Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD Consultant, Southern N.J. Regional Chest Clinic New Jersey State TB Physician Advisory Board Cooper Univ. Hospital EIP Program TB and HIV
Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD Consultant, Southern N.J. Regional Chest Clinic New Jersey State TB Physician Advisory Board Cooper Univ. Hospital EIP Program TB and HIV
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Management of Drug-resistant Tuberculosis (DR-TB)
") Management of Drug-resistant Tuberculosis (DR-TB) Nitipatana Chierakul Division of Respiratory Disease & Tuberculosis Department of Medicine Faculty of Medicine Siriraj Hospital October 14 th, 2008 Tropical
Management of Drug-resistant Tuberculosis (DR-TB) Nitipatana Chierakul Division of Respiratory Disease & Tuberculosis Department of Medicine Faculty of Medicine Siriraj Hospital October 14 th, 2008 Tropical
Treatment: First Line Drugs TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS TREATMENT: GENERAL PRINCIPLES MECHANISM OF ACTION MID 27
 TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
TUBERCULOSIS TREATMENT: MEDICATIONS & REGIMENS Treatment: First Line Drugs 1. ISONIAZID = INH Bacteriocidal against dividing organisms Dose = 300mg = one pill = well absorbed Good CNS penetration Can be
Pediatric TB Intensive Houston, Texas
 Pediatric TB Intensive Houston, Texas November 13, 2009 Extrapulmonary TB James B. McAuley MD MPH November 13, 2009 PEDIATRIC TB EXTRAPULMONARY DISEASE James B. McAuley MD MPH Rush University Medical Center
Pediatric TB Intensive Houston, Texas November 13, 2009 Extrapulmonary TB James B. McAuley MD MPH November 13, 2009 PEDIATRIC TB EXTRAPULMONARY DISEASE James B. McAuley MD MPH Rush University Medical Center
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, TB Nurse Case Management September 12 14, 2017
 Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Diagnosis and Medical Management of TB Infection Lisa Y. Armitige, MD, PhD September 12, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Extrapulmonary TB Linda Dooley, MD November 13, 2014 Linda Dooley, MD has the following disclosures to make: No conflict of interests No relevant financial
TB Intensive San Antonio, Texas November 11 14, 2014 Extrapulmonary TB Linda Dooley, MD November 13, 2014 Linda Dooley, MD has the following disclosures to make: No conflict of interests No relevant financial
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Pediatric TB Intensive Houston, Texas October 14, Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 TB in the HIV Patient Lisa Armitige, MD, PhD April 6, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 TB in the HIV Patient Lisa Armitige, MD, PhD April 6, 2012 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interests
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
Official American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America Clinical Practice Guidelines:
 Official American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis OBJECTIVES
Official American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis OBJECTIVES