Ductus Arteriosus: Dilemmas of Treatment vs. No Treatment in the Premature Neonate
|
|
|
- Hortense Phillips
- 6 years ago
- Views:
Transcription



, FACC, FASE, FAHA.")
 U.C. San Francisco, NHS.")
1 Ductus Arteriosus: Dilemmas of Treatment vs. No Treatment in the Premature Neonate Time allotted: 30 Minutes. No Disclosures. Norman H Silverman MD. D Sc (Med), FACC, FASE, FAHA. Professor of Pediatrics ( Cardiology) U.C. San Francisco, NHS. Professor Emeritus, Stanford University


2 Where is the Ductus

3 Rat Patent Ductus Momma





4 The Course & Histology of Ductus Closure The ductus arteriosus in the preterrn infant: Histologic and clinical observations Adriana C. Gittenberger-de Groot, M.D.,* Ingrid van Ertbruggen, M.D., Andr~ J.M.G. Moulaert, M.D., and Eric Harinck, M.D., January The Journal of P E D I A T R I C S Vol. 96, No. 1, pp
5 The Problem in Perspective In reality prematurity is a multisystem disorder of every organ and the consequences of immaturity in one organ may have consequences for many other organs. The premature infant with a patent ductus arteriosus has problems due to immaturity of most physiological processes respiration, absorption and nutrition, central nervous system, circulation, renal function, electrolyte balance, and metabolism all of which occur even in the absence of a patent ductus arteriosus. As a result, it is difficult to know what contribution the patent ductus arteriosus is making to the infant s problems, and therefore difficult to decide if the ductus should be closed and if closure has made a difference to the child s course. Early experience after closure of the ductus in premature infants has shown that expectations of normality after closure of the patent ductus arteriosus are unrealistic. PDA may remain asymptomatic in the face of respiratory disease. Is the big ductus shunt affecting the infant? This is the hardest question to answer, because none of the findings listed above can tell us how well the left ventricle is compensating. Failure to distinguish between a large but well compensated shunt and a shunt that is causing problems is at least part of the reason why closing the ductus may not appear to be useful therapy.

6 The Problem in Perspective In a nutshell we can say that there has been a general shift in the management of PDA in preterm neonates from the aggressive approach to a more conservative approach. On the basis of available evidences, rationalization and individual emphasis on precise identification of a hemodynamically significant duct seem to be the way forward.
7 Incidence of PDA in Preemies 1/100- Live births In Preemies 8/1000 In healthy preterm neonates >30 weeks gestation, PDA closes by day 4 in 90% and by day 7 in 98% <24 weeks gestation babies stand at a dismal 8% and 13% by day 4 and day 7, respectively In 50 70% of preterm infants with birth weight <1,500 g. the ductus remains patent Among infants less than 1500 g who still have a PDA at the time of hospital discharge, it will spontaneously close by the end of the first year in 86% of the infants Among infants <27 weeks of gestation, with a PDA at the time of hospital discharge, 75% of the infants spontaneously close the duct by the end of the first year.
 31, S42-S48 Five decades after the recognition of delayed closure of the ductus in preterm")
8 William E Benitz of Stanford. Learning to live with patency of the ductus arteriosus in preterm infants Journal of Perinatology (2011) 31, S42-S48 Five decades after the recognition of delayed closure of the ductus in preterm infants, management remains heterogeneous and controversial. Routine early treatment to close the ductus does not appear to be beneficial, but selective later treatment may still prove valuable. The timing, criteria, objectives and methods for such treatments remain to be established. Potential strategies for minimizing the adverse effects of PDA while awaiting spontaneous closure or achievement of treatment criteria need careful evaluation in clinical trials. Elimination of ductal shunting and its consequences by surgical ligation or by induction of ductal constriction with cyclo-oxygenase (C0X) inhibition promised to ameliorate the adverse outcomes associated with ductal patency. However, neither individual randomized controlled trials nor meta-analyses of those trials? have confirmed this hypothesis.



9 What did Charlie Say? PP Treatment of the PDA in infants >1000 g BW is rarely warranted, as nearly all (94%) will spontaneously close and the rate of complications in this population are low. However, among infants <1000 g BW, the PDA is far less likely to close spontaneously.


10 The Issue of a PDA
11 . In 50 70% of preterm infants with birth weight <1,500 g, the ductus remains patent An open ductus may contribute to the development of BPD by shunting blood into the lungs, resulting in pulmonary edema and the persistent need for ventilatory support. This population of preterm infants with a PDA would benefit from strategies to reduce complications and optimize outcomes. 615 preterm infants with birth weight <1,500 g admitted to the Neonatal IntensiveCare Unit, of whom 209 (34%) were found to have a PDA by ECHO. Twenty-two patients were excluded and 187 remaining subjects had their PDA either treated (75%) or conservatively managed. The mean gestational age of the 187 subjects was 27.6 ± 2 wk and the mean age at PDA treatment was 4 ± 4 d among those treated. Mean ductal diameter at the time of treatment was 1.7 ± 0.6 mm. Only lower gestational age and not PDA treatment or ECHO score was associated with the adverse outcome of death or BPD. Further investigation of PDA management strategies and effects on adverse outcomes of prematurity is needed.


12 Arvind Sehgal Patrick J McNamara

13 Jet Physics Vena contracta: Smallest area of flow in or downstream from a restrictive orifice.




14 Proximal Flow Convergence in PDA Duct Flow AO PISA LA D Ao LPA Jet physics is important and the value of Doppler color flow signals in determining the size of the duct. As with a garden hose stream, the size of the jet diminishes to a point called the vena contracta. This narrowest point in a jet is a little smaller than the actual size of the tube (the duct) through which it is traveling, but provides a reasonable estimate of its true size. The PISA stands for Proximal Isovelocity Surface Acceleration.

15 The Other PISA
16 Quantitation of Patent Ductus Size. Documentation of size of duc >1 indicated a large PDA, <1 but >0.5 moderate and <0.5 a small. duct LA/Ao Ratio (>1.3:1) and Left Ventricular hyperdynamic contractions Retrograde abdominal aortic flow If Prograde Flow--> Mild; If Retrograde flow---> large (VTI of Reverse vs. Forward F:ow) Ductus Doppler --> Restrictive if velocity is >2 msec and contiuous Non-resrictive, if goes to baseline PISA Small-- small shunt Pisa Moderate- moderate sized shunt No Pisa Large Shunt Apgar-like score
17 Echocardiographic Scoring System for Patent Ductus Arteriosus Start with 10 points Parameter LA:Ao ratio < >1.3 Retrograde aortic flow (reverse:forward flow) None >0.4 PISA No ductus Some None when ductus present Ductus:LPA ratio < >0.5 Doppler of PDA Continuous flow Left-right and stops at baseline Hemodynamically significant ductus if score <5 Bidirection al



18 THE LA:AO RATIO Strength: This is simple measurement made by the technologist usually fairly accurate. Can be made of Twodimensional Echo as well. Weakness: This technique was a surrogate for measuring left atrial size. Now Z scores are available Confounding associations on the cardiac basis, Premature infants have a PFO



19 The LA:AO Ratio ( > 1.3:1)
20



21 Flow Dynamics in the Juxtaductus Aorta. Ao Prox to Duct Ao Disatal to Duct Text Ductus Flow


")



22 Horizontal Ductus (Transposition) Ductus Size Strength: This is a measurement that is linear and easy to make. It certainly parallels whether the duct is large, moderate or small Vertical Ductus ( Pulmonary Undercirculation ) Weakness: Minor differences of the type that relate to pixels differences can make large differences in the amount of flow. The question of where the narrowest portion of the ductus might be makes it be difficult sometimes to see the exact point of narrowing




23 Large Patent Ductus Arteriosus The Ducuts Cut PA D LA DAO NHS.



24 Ductus Cut and Flow Dynamics MPA Arch LPA Duct D Ao Isthmus


25 Large PDA Subcostal Sagittal Image Suprasternal Sagittal Image




26 Ductus Size



27 Ductus Size Pulm Htn
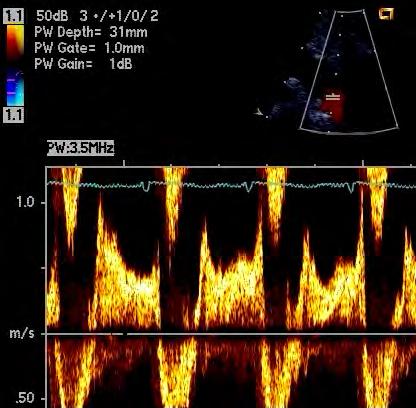
28 Ductus Size: Doppler Velocities. Tiny Small Moderate Large
29 Ductus Size: Doppler Velocities. Tiny Strength: This is a simple measurement. A pressure difference> 1 m/s means the duct must be constricted. When there is a large ducts and /or when there is PHT Small Moderate Large Weakness: Angle of insonation has to be low Gradation of the degree of ductus constriction related to variations in low systemic pressures

 2.")


30 Patent Ductus SizeAssessment by Color Q= 2πr 2.NL = 2.22/7 (0.04cm) (= NL) = 6.29x x. 55 = ml/sec...x60 secs/min = ml/min... BSA 0.18 = 185 ml/min/m 2 BSA = l/min/m 2 BSA


31 Large PDA: PISA The Ductus Cut


32 Small Ducts : Pisa & Vena Contracta Parasternal Ducuts Cut Subcostal The Ducuts Cut


33 Smaller PISA

34 Closing Ductus
35 Color Techniques Strength: Doppler color flow is often more sensitive than imaging in defining flow, defining blood flow better than imaging, particularly with smaller ducts also more 3- dimensional in is character as the slice thickness is as limited in the regular image. Weakness: With all Color Doppler modalities the techniques is sensitive to machine type, gain, filtering, and changes in the Nyquist limit. So we can have a variety of possibilities, which make assessment s somewhat artifactual. (i) The PISA Method. Strength: This technique has been validated in laboratory situations permitting fairly accurate assessment for flow on the proximal side of a jet. This is the only Doppler technique which allows for the assessment of flow within a jet system Weakness: Unfortunately, it requires two circumstances to be accurate. The first is the orifice through which the flow occurs has to be round and the second is that the jet should not be interfered with by the lateral confines of the duct. Not being a free just and some of it may be confined and altered by the shape of the duct. There are many confounding problems in assessing flow across the duct by this means because there is no free jet in this situation. What we have observed is that when there is a large ductus with large amount of flow, there is no PISA because there is no constriction, when there is a moderate sized ductus with a moderate amount of flow, there is a large PISA and when there is when there is a small ductus with small amount of flow, there is a small PISA.
36 Color Techniques (ii) Vena Contracta and Color Doppler Jet Width Measurement. Strength: The same as for the previous sections on Doppler color flow. Weakness: The same as for the previous sections on Doppler color flow






37 Ductus Size: Doppler Velocities in the Abdominal Aorta. No Duct Strength: Surrogate for blood pressure measurement, It really looks for runoff of a large shunt and for retrograde flow. Lesser degrees of flow are found to occur with lesser shunts. Small Moderate Weakness:: Technologists often don t get axial enough to evaluate Blow adequately and in that circumstance the low velocity of the retrograde Blow can be lost. Wall Filter issues: If the wall Bilter- if too high, obfuscates the low Blow velocity in diastole. Large



38 The Ductus and Pressure Assessment TR Duct pressure assessment CW Duct PFO
39 Ductus Assessment. There are many critical issues in measurement of ductus size. We need to get better at measurements What we need to concentrate on is which ductus is critical in terms of defining outcomes Perhaps we need to concentrate only on the large PDA in terms of outcomes Clearly prospective trials are necessary We have been examining too many ductuses by Echo in preemies!
40 What about Cox inhibitors? Based on current evidence, prophylactic indomethacin is not recommended for the treatment of PDA in preterm infants. There are well-established side effects of indomethacin, such as significant reduction in cerebral, mesenteric, and renal blood flow velocities as measured by Doppler ultrasonography, as well as possible adverse effects on platelet function, have raised serious questions on the prophylactic use of this drug With growing concerns over the side effects of indomethacin, a safer alternative was requested. Ibuprofen has been shown to be less nephrotoxic than indomethacin. It has been found that 85.2% of PDAs closed if the first dose of indomethacin was administered within 24 hours of birth. However, this rate decreased to 48.1% when treatment was started 72 hours or later after birth. It has been shown that although early indomethacin treatment improved PDA closure rates, it was associated with increased renal side effects and offered no respiratory advantage over late indomethacin administration in ventilated surfactant-treated infants.
41 What about Surgical Ligation? They found that even though infants were exposed to larger PDA shunts for longer durations in the conservative treatment period, the rates of BPD, sepsis, retinopathy of prematurity (ROP) neurological injury, and death did not change. However, their overall rate of was significantly lower. It has also been shown in experimental models that early surgical ligation of the duct impedes lung growth in preterm baboons. The lack of any respiratory or neurological benefit shown by these studies, recent research also indicates that surgical ligation of the duct may in fact cause more harm than good. It has been shown that secondary surgical closure was associated with increased odds for neurodevelopmental impairment and increased adjusted odds for BPD but decreased adjusted odds for death..


42 What About Interventional Catheterization?
43 Conclusion From Mitra There is no generally accepted understanding of the echocardiographic markers of hemodynamic significance and their importance for treatment or prognosis. Echocardiography could be looked upon as the best representation of the circulatory state, but a fundamental problem is the lack of gold standard for the physiologic effects of a ductal shunt related to the echocardiographic findings. The relative importance of pulmonary over circulation, vascular resistances, and systemic hypoperfusion also remain to be clarified.
44 ACP High Value Care Misuse and overuse of medical interventions that do not directly improve a patient s health contribute significantly to the unsustainable growth of healthcare spending. ACP s goal is to determine whether diagnostic tests and treatments for various diseases provide good value, i.e. medical benefits that are commensurate with their costs and outweigh any harm. We do this by analyzing their benefits, harms, and costs based on the best available evidence. Approximately 30% of healthcare costs (more than $750 billion annually) are spent on wasted care. ACP has developed clinical recommendations, physician resources, curriculum and public policy recommendations around this initiative.
45 Comparison of Data Points on Stanford Study Left arial size by M-mode normalized to the aorta as LA:Ao ratio Also Left atrial by 2 D area as a reflection of LA Size Ventricular Function. Fractional Sortening index as a surrogate for ejection fraction Mitral regurgitation and atrial left to right shunt which might comrpomise estimate of LA size Retrograde diastolic flow by Doppler ultrasound in the abd. aorta as a surrogate for systolic: diastolic and pulse pressure. Ductus size measurement by 2 D or and by Doppler color flow at the vena contracta, measured by Doppler or Doppler color flow Pulmonary artery size as a refection of the size fo the Ductus. A ration between the Duct: LPA > 1 suggests a large duct. Proximal Isovelocy Surface acceleration as a reflection ductus left to right shunt. Aortopulmonary pressure differences across the arterial duct measured by Doppler or Doppler color flow.
46 Impressions The data on the original study used patient data unrelated to the temporal time of the decision making process. It seemed that the neonatologists neither read the reports or consulted with cardiology about ductus closure. I reread the reports to see if I disagreed with anyone in the Echo lab who read a report and found near 100% concordance. Looking at the data it seemed that once the ductus was constricted there was very little chance that patient was going to reopen the duct. I have encountered only one patient in the series Following on this point it seems that there was a large number of patients who got unnecessary $4, /10 patients sampled for the surgically closed ductus cohort of 70 patients had no hemodynamic reason for having their ductus ligated! Compliance between the two observers was much better than in the original study..
47 Lessons Check and re-check your data. Remember garbage in + garbage out! If you want to do good research you have to do it your self! or at least have a close supervision of the plan, measurements and results..
48 Plan Will we be able to make inferences from our retrospective study? What can we do going forward? We must do a better job talking to each other and pay as a team for the benefit of our patients We need a prospective study. This is a neonatology study, involving cardiology.
Ductus Arteriosus: Dilemmas of Treatment vs. No Treatment in the Premature Neonate
 Ductus Arteriosus: Dilemmas of Treatment vs. No Treatment in the Premature Neonate Time allotted: 30 Minutes. No Disclosures. Norman H Silverman MD. D Sc (Med), FACC, FASE, FAHA. Professor of Pediatrics
Ductus Arteriosus: Dilemmas of Treatment vs. No Treatment in the Premature Neonate Time allotted: 30 Minutes. No Disclosures. Norman H Silverman MD. D Sc (Med), FACC, FASE, FAHA. Professor of Pediatrics
PATENT DUCTUS ARTERIOSUS IN THE PRETERM INFANT EVIDENCE FOR & AGAINST TREATMENT
 PATENT DUCTUS ARTERIOSUS IN THE PRETERM INFANT EVIDENCE FOR & AGAINST TREATMENT Dr. Youssef Abou Zanouna, FRCPI, FACC Consultant Pediatric Cardiologist King Fahd Military Medical Complex Dhahran Introduction
PATENT DUCTUS ARTERIOSUS IN THE PRETERM INFANT EVIDENCE FOR & AGAINST TREATMENT Dr. Youssef Abou Zanouna, FRCPI, FACC Consultant Pediatric Cardiologist King Fahd Military Medical Complex Dhahran Introduction
Standardising echocardiography and images. Version 2, 13/04/15
 Standardising echocardiography and images 1. Review of ECHO eligibility criteria - trial entry - rescue treatment 2. Assessments - personnel - timing 3. Technical aspects of ECHO examination 1. Trial entry
Standardising echocardiography and images 1. Review of ECHO eligibility criteria - trial entry - rescue treatment 2. Assessments - personnel - timing 3. Technical aspects of ECHO examination 1. Trial entry
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Update on mangement of patent ductus arteriosus in preterm infants. Dr. Trinh Thi Thu Ha
 Update on mangement of patent ductus arteriosus in preterm infants Dr. Trinh Thi Thu Ha Outline 1. Overview of PDA 2. Timing of screening PDA? 3. When to treat PDA? Timing of ductal closure Prenatal
Update on mangement of patent ductus arteriosus in preterm infants Dr. Trinh Thi Thu Ha Outline 1. Overview of PDA 2. Timing of screening PDA? 3. When to treat PDA? Timing of ductal closure Prenatal
Short-Term Outcome Of Different Treatment Modalities Of Patent Ductus Arteriosus In Preterm Infants. Five Years Experiences In Qatar
 ISPUB.COM The Internet Journal of Cardiovascular Research Volume 7 Number 2 Short-Term Outcome Of Different Treatment Modalities Of Patent Ductus Arteriosus In Preterm Infants. Five Years Experiences In
ISPUB.COM The Internet Journal of Cardiovascular Research Volume 7 Number 2 Short-Term Outcome Of Different Treatment Modalities Of Patent Ductus Arteriosus In Preterm Infants. Five Years Experiences In
Quantifying Aortic Regurgitation
 Quantifying Aortic Regurgitation Linda D. Gillam, MD, MPH Morristown Medical Center Dorothy and Lloyd Huck Chair Cardiovascular Medicine Atlantic Health System No Disclosures 1 Valve Dysfunction Functional
Quantifying Aortic Regurgitation Linda D. Gillam, MD, MPH Morristown Medical Center Dorothy and Lloyd Huck Chair Cardiovascular Medicine Atlantic Health System No Disclosures 1 Valve Dysfunction Functional
Patent Ductus Arteriosus: Philosophy or Pathology?
 Patent Ductus Arteriosus: Philosophy or Pathology? Disclosure Ray Sato, MD is a speaker for Prolacta Biosciences, Inc. This presentation will discuss off-label uses of acetaminophen and ibuprofen. RAY
Patent Ductus Arteriosus: Philosophy or Pathology? Disclosure Ray Sato, MD is a speaker for Prolacta Biosciences, Inc. This presentation will discuss off-label uses of acetaminophen and ibuprofen. RAY
A2b. PDA Management--A Reflection on the Evidence: Does it Help with Management? Session Summary. Session Objectives. References.
 FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UTE AND REVIEW A2b Management--A Reflection on the Evidence: Does it Help with Management? Alfonso Vargas, MD Neonatologist Pediatrix Medical Group, Tampa, FL
FANNP 23RD NATIONAL NNP SYMPOSIUM: CLINICAL UTE AND REVIEW A2b Management--A Reflection on the Evidence: Does it Help with Management? Alfonso Vargas, MD Neonatologist Pediatrix Medical Group, Tampa, FL
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency
 Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING
 PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
NOT YET!! PDA - Pathological or innocent physiologic bystander? PDA From Physiology to Treatment 9/8/2014
 PDA - Pathological or innocent physiologic bystander? PDA From Physiology to Treatment Martin Kluckow MBBS FRACP PhD CCPU Associate Professor Royal North Shore Hospital & University of Sydney, Australia
PDA - Pathological or innocent physiologic bystander? PDA From Physiology to Treatment Martin Kluckow MBBS FRACP PhD CCPU Associate Professor Royal North Shore Hospital & University of Sydney, Australia
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC & SBH Child Health Standards Committee Pages: 1 of 6 Supercedes: N/A 1.0 PURPOSE and INTENT
NEONATAL CLINICAL PRACTICE GUIDELINE Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC & SBH Child Health Standards Committee Pages: 1 of 6 Supercedes: N/A 1.0 PURPOSE and INTENT
A preliminary study of the application of the transductal velocity ratio for assessing persistent ductus arteriosus
 Arch Dis Child Fetal Neonatal Ed 2000;82:F195 F199 F195 Division of Neonatal Services, Royal Women s Hospital, Melbourne, Australia M W Davies F R Betheras M Swaminathan Correspondence to: Dr Davies, Perinatal
Arch Dis Child Fetal Neonatal Ed 2000;82:F195 F199 F195 Division of Neonatal Services, Royal Women s Hospital, Melbourne, Australia M W Davies F R Betheras M Swaminathan Correspondence to: Dr Davies, Perinatal
Natural history of innocent heart murmurs in newborn babies: controlled echocardiographic study
 F166 Arch Dis Child Fetal Neonatal Ed 1998;78:F166 F170 ORIGINAL ARTICLES Natural history of innocent heart murmurs in newborn babies: controlled echocardiographic study Romaine Arlettaz, Nicholas Archer,
F166 Arch Dis Child Fetal Neonatal Ed 1998;78:F166 F170 ORIGINAL ARTICLES Natural history of innocent heart murmurs in newborn babies: controlled echocardiographic study Romaine Arlettaz, Nicholas Archer,
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment
 Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
Predictors of bronchopulmonary dysplasia or death in premature infants with a patent ductus arteriosus
 Articles Clinical Investigation nature publishing group Predictors of bronchopulmonary dysplasia or death in premature infants with a patent ductus arteriosus Valerie Y. Chock 1, Rajesh Punn 2, Anushri
Articles Clinical Investigation nature publishing group Predictors of bronchopulmonary dysplasia or death in premature infants with a patent ductus arteriosus Valerie Y. Chock 1, Rajesh Punn 2, Anushri
The Patent Ductus Arteriosus (PDA) and the Preterm Baby. Tanya Hatfield, RNC-NIC, MSN Neonatal Outreach Educator
 and the Preterm Baby. Tanya Hatfield, RNC-NIC, MSN Neonatal Outreach Educator") The Patent Ductus Arteriosus (PDA) and the Preterm Baby Tanya Hatfield, RNC-NIC, MSN Neonatal Outreach Educator Objectives Describe normal cardiac physiology and development Understand the unique physiologic
The Patent Ductus Arteriosus (PDA) and the Preterm Baby Tanya Hatfield, RNC-NIC, MSN Neonatal Outreach Educator Objectives Describe normal cardiac physiology and development Understand the unique physiologic
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Project 1: Circulation
 Project 1: Circulation This project refers to the matlab files located at: http://www.math.nyu.edu/faculty/peskin/modsimprograms/ch1/. Model of the systemic arteries. The first thing to do is adjust the
Project 1: Circulation This project refers to the matlab files located at: http://www.math.nyu.edu/faculty/peskin/modsimprograms/ch1/. Model of the systemic arteries. The first thing to do is adjust the
New 3D Quantification of Mitral Regurgitation Severity. Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA
 New 3D Quantification of Mitral Regurgitation Severity Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA No Financial Disclosures No off label discussion of devices
New 3D Quantification of Mitral Regurgitation Severity Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA No Financial Disclosures No off label discussion of devices
Doppler Basic & Hemodynamic Calculations
 Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
PIAF study: Placental insufficiency and aortic isthmus flow Jean-Claude Fouron, MD
 Dear colleagues, I would like to thank you very sincerely for agreeing to participate in our multicentre study on the clinical significance of recording fetal aortic isthmus flow during placental circulatory
Dear colleagues, I would like to thank you very sincerely for agreeing to participate in our multicentre study on the clinical significance of recording fetal aortic isthmus flow during placental circulatory
PISA Evaluation of Mitral Regurgitation. Raymond Graber, MD Cardiac Anesthesia Group University Hospitals Case Medical Center 4/07/2011
 PISA Evaluation of Mitral Regurgitation Raymond Graber, MD Cardiac Anesthesia Group University Hospitals Case Medical Center 4/07/2011 Introduction Evaluation of MR. What is PISA? Physiologic basis Issues
PISA Evaluation of Mitral Regurgitation Raymond Graber, MD Cardiac Anesthesia Group University Hospitals Case Medical Center 4/07/2011 Introduction Evaluation of MR. What is PISA? Physiologic basis Issues
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies
 ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
SWISS SOCIETY OF NEONATOLOGY. Prenatal closure of the ductus arteriosus
 SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
SWISS SOCIETY OF NEONATOLOGY Prenatal closure of the ductus arteriosus March 2007 Leone A, Fasnacht M, Beinder E, Arlettaz R, Neonatal Intensive Care Unit (LA, AR), University Hospital Zurich, Cardiology
Is there any Benefit to Closing the Ductus Arteriosus?
 Controversies in the Management of a Patent Ductus Arteriosus Is there any Benefit to Closing the Ductus Arteriosus? Richard A. Polin M.D. Morgan Stanley Children s Hospital Columbia University Galen 130-200
Controversies in the Management of a Patent Ductus Arteriosus Is there any Benefit to Closing the Ductus Arteriosus? Richard A. Polin M.D. Morgan Stanley Children s Hospital Columbia University Galen 130-200
Hybrid Stage I Palliation / Bilateral PAB
 Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas
 Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Diagnostic approach to heart disease
 Diagnostic approach to heart disease Initial work up History Physical exam Chest radiographs ECG Special studies Echocardiography Cardiac catheterization Echocardiography principles Technique of producing
Diagnostic approach to heart disease Initial work up History Physical exam Chest radiographs ECG Special studies Echocardiography Cardiac catheterization Echocardiography principles Technique of producing
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD. UCL -Cliniques Saint Luc
 New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY
 가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
Transcatheter closure of the patent ductus arteriosus using the new Amplatzer duct occluder: Initial clinical applications in children
 Transcatheter closure of the patent ductus arteriosus using the new Amplatzer duct occluder: Initial clinical applications in children Basil Thanopoulos, MD, PhD, a Nikolaos Eleftherakis, MD, a Konstantinos
Transcatheter closure of the patent ductus arteriosus using the new Amplatzer duct occluder: Initial clinical applications in children Basil Thanopoulos, MD, PhD, a Nikolaos Eleftherakis, MD, a Konstantinos
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Patent ductus arteriosus: pathophysiology and management
 (2006) 26, S14 S18 r 2006 Nature Publishing Group All rights reserved. 0743-8346/06 $30 www.nature.com/jp ORIGINAL ARTICLE Patent ductus arteriosus: pathophysiology and management ER Hermes-DeSantis 1
(2006) 26, S14 S18 r 2006 Nature Publishing Group All rights reserved. 0743-8346/06 $30 www.nature.com/jp ORIGINAL ARTICLE Patent ductus arteriosus: pathophysiology and management ER Hermes-DeSantis 1
Echocardiography: Guidelines for Valve Quantification
 Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Echocardiography. Guidelines for Valve and Chamber Quantification. In partnership with
 Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
An understanding of the many factors involved in the
 Atrioventricular Valve Dysfunction: Evaluation by Doppler and Cross-Sectional Ultrasound Norman H. Silverman, MD, and Doff B. McElhinney, MD Division of Pediatric Cardiology, Department of Pediatrics,
Atrioventricular Valve Dysfunction: Evaluation by Doppler and Cross-Sectional Ultrasound Norman H. Silverman, MD, and Doff B. McElhinney, MD Division of Pediatric Cardiology, Department of Pediatrics,
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
British Society of Echocardiography
 British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
PDA: As the Pendulum Swings. Cathy Hammerman Shaare Zedek Medical Center & Hebrew University Faculty of Medicine, Jerusalem, Israel
 PDA: As the Pendulum Swings Cathy Hammerman Shaare Zedek Medical Center & Hebrew University Faculty of Medicine, Jerusalem, Israel Six Blind Neonatologists Approach PDA It s not physiologic - all must
PDA: As the Pendulum Swings Cathy Hammerman Shaare Zedek Medical Center & Hebrew University Faculty of Medicine, Jerusalem, Israel Six Blind Neonatologists Approach PDA It s not physiologic - all must
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
The Physiology of the Fetal Cardiovascular System
 The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Premature Infants with Patent Ductus Arteriosus and Res iratory Distress: Selection for mdap Ligation
 Premature Infants with Patent Ductus Arteriosus and Res iratory Distress: Selection for mdap Ligation George S. Hall, M.D., James A. Helmsworth, M.D., J. Tracy Schreiber, M.D., Jens G. Rosenkrantz, M.D.,
Premature Infants with Patent Ductus Arteriosus and Res iratory Distress: Selection for mdap Ligation George S. Hall, M.D., James A. Helmsworth, M.D., J. Tracy Schreiber, M.D., Jens G. Rosenkrantz, M.D.,
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Aortic arch anomalies Coarctation of the Aorta Interrupted Aortic Arch Echocardiography
 Aortic arch anomalies Coarctation of the Aorta Interrupted Aortic Arch Echocardiography V.Tomek, J. Marek, J. Škovránek, J. Gilík No disclosures Kardiocentrum, University Hospital Motol, Prague, Czech
Aortic arch anomalies Coarctation of the Aorta Interrupted Aortic Arch Echocardiography V.Tomek, J. Marek, J. Škovránek, J. Gilík No disclosures Kardiocentrum, University Hospital Motol, Prague, Czech
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Aortic Arch Abnormalities
 Aortic Arch Abnormalities IPOK Norman H Silverman MD, D Sc (Med.). FACC, FAHA. Stanford University & Lucile Packard Children s Hospital E mail: norm.silverman@stanford.edu. NHS. www.md1world.com Abnormalities
Aortic Arch Abnormalities IPOK Norman H Silverman MD, D Sc (Med.). FACC, FAHA. Stanford University & Lucile Packard Children s Hospital E mail: norm.silverman@stanford.edu. NHS. www.md1world.com Abnormalities
Journal of American Science 2014;10(9) Congenital Heart Disease in Pediatric with Down's Syndrome
 Congenital Heart Disease in Pediatric with Down's Syndrome") Journal of American Science 2014;10(9) http://www.jofamericanscience.org Congenital Heart Disease in Pediatric with Down's Syndrome Jawaher Khalid Almaimani; Maryam Faisal Zafir; Hanan Yousif Abbas and
Journal of American Science 2014;10(9) http://www.jofamericanscience.org Congenital Heart Disease in Pediatric with Down's Syndrome Jawaher Khalid Almaimani; Maryam Faisal Zafir; Hanan Yousif Abbas and
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging
 Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction
 Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
Paediatrica Indonesiana. Echocardiographic patterns in asphyxiated neonates. Maswin Masyhur, Idham Amir, Sukman Tulus Putra, Alan Roland Tumbelaka
 Paediatrica Indonesiana VOLUME 49 July NUMBER 4 Original Article Echocardiographic patterns in asphyxiated neonates Maswin Masyhur, Idham Amir, Sukman Tulus Putra, Alan Roland Tumbelaka Abstract Background
Paediatrica Indonesiana VOLUME 49 July NUMBER 4 Original Article Echocardiographic patterns in asphyxiated neonates Maswin Masyhur, Idham Amir, Sukman Tulus Putra, Alan Roland Tumbelaka Abstract Background
ASCeXAM / ReASCE. Practice Board Exam Questions Monday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona
, FASE Mayo Clinic, Arizona") Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
Hazards and Benefits of Postnatal Steroids. David J. Burchfield, MD Professor and Chief, Neonatology University of Florida
 Hazards and Benefits of Postnatal Steroids David J. Burchfield, MD Professor and Chief, Neonatology University of Florida Disclosures I have no financial affiliations or relationships to disclose. I will
Hazards and Benefits of Postnatal Steroids David J. Burchfield, MD Professor and Chief, Neonatology University of Florida Disclosures I have no financial affiliations or relationships to disclose. I will
Debate in Management of native COA; Balloon Versus Surgery
 Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
ViosWorks: A Paradigm Shift in Cardiac MR Imaging
 Figure 1. ViosWorks image of a patient with shunted pulmonary venous return. Image courtesy of Dr. Shreyas Vasanawala, Stanford University. ViosWorks: A Paradigm Shift in Cardiac MR Imaging The value of
Figure 1. ViosWorks image of a patient with shunted pulmonary venous return. Image courtesy of Dr. Shreyas Vasanawala, Stanford University. ViosWorks: A Paradigm Shift in Cardiac MR Imaging The value of
Index. K Knobology, TTE artifact, image resolution, ultrasound, 14
 A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
Cases in Adult Congenital Heart Disease
 Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
PDA: Closure Using Coils and Devices: Indications, Technique & Outcome
 PDA: Closure Using Coils and Devices: Indications, Technique & Outcome Daniel Levi, MD, FSCAI Associate Professor of Pediatrics UCLA Biomedical Engineering Mattel Children s Hospital at UCLA, Division
PDA: Closure Using Coils and Devices: Indications, Technique & Outcome Daniel Levi, MD, FSCAI Associate Professor of Pediatrics UCLA Biomedical Engineering Mattel Children s Hospital at UCLA, Division
Certificate in Allied Health Performed Ultrasound (CAHPU)
") Certificate in Allied Health Performed Ultrasound (CAHPU) Syllabus Advanced Allied Health Performed Neonatal Ultrasound Advanced Allied Health Performed Neonatal Ultrasound Purpose: Prerequisites: Training:
Certificate in Allied Health Performed Ultrasound (CAHPU) Syllabus Advanced Allied Health Performed Neonatal Ultrasound Advanced Allied Health Performed Neonatal Ultrasound Purpose: Prerequisites: Training:
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation?
 can help prevent Postoperative Cardiorespiratory instability following PDA ligation?") Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation? Amish Jain, Mohit Sahni, Afif El Khuffash, Arvind Sehgal, Patrick J
Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation? Amish Jain, Mohit Sahni, Afif El Khuffash, Arvind Sehgal, Patrick J
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
The background of the Cardiac Sonographer Network News masthead is a diagnostic image:
 Number 5 Welcome Number 5 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Number 5 Welcome Number 5 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Normal TTE/TEE Examinations
 Normal TTE/TEE Examinations Geoffrey A. Rose, MD FACC FASE Sanger Heart & Vascular Institute Before you begin imaging... Obtain the patient s Height Weight BP PLAX View PLAX View Is apex @ 9-10 o clock?
Normal TTE/TEE Examinations Geoffrey A. Rose, MD FACC FASE Sanger Heart & Vascular Institute Before you begin imaging... Obtain the patient s Height Weight BP PLAX View PLAX View Is apex @ 9-10 o clock?
Correlation of B-type natriuretic peptide levels and echocardiographic parameters in preterm infants with patent ductus arteriosus
 Original article Korean J Pediatr 2016;59(4):183-189 pissn 1738-1061 eissn 2092-7258 Korean J Pediatr 2016;59(4):183-189 Korean J Pediatr Correlation of B-type natriuretic peptide levels and echocardiographic
Original article Korean J Pediatr 2016;59(4):183-189 pissn 1738-1061 eissn 2092-7258 Korean J Pediatr 2016;59(4):183-189 Korean J Pediatr Correlation of B-type natriuretic peptide levels and echocardiographic
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation
 Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
The incidence and follow-up of isolated ventricular septal defect in newborns by echocardiographic screening
 The Turkish Journal of Pediatrics 2008; 50: 223-227 Original The incidence and follow-up of isolated ventricular septal defect in newborns by echocardiographic screening Filiz Ekici, Ercan Tutar, Semra
The Turkish Journal of Pediatrics 2008; 50: 223-227 Original The incidence and follow-up of isolated ventricular septal defect in newborns by echocardiographic screening Filiz Ekici, Ercan Tutar, Semra
Use of rectal ibuprofen for PDA closure in preterm neonates
 Use of rectal ibuprofen for PDA closure in preterm neonates D. Surkov, A. Obolonskiy, O. Kapustina, D. Volkov NICU, Regional Children s Hospital, Dnepropetrovsk, Ukraine Corresponding author: D. Surkov,
Use of rectal ibuprofen for PDA closure in preterm neonates D. Surkov, A. Obolonskiy, O. Kapustina, D. Volkov NICU, Regional Children s Hospital, Dnepropetrovsk, Ukraine Corresponding author: D. Surkov,
Introduction to Fetal Medicine. Lloyd R. Feit M.D. Associate Professor of Pediatrics Warren Alpert Medical School Brown University
 Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Objectives. Apnea Definition and Pitfalls. Pathophysiology of Apnea. Apnea of Prematurity and hypoxemia episodes 5/18/2015
 Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Incidental Discovery of a Patent Ductus Arteriosus in Adults
 BRIEF REPORT Incidental Discovery of a Patent Ductus Arteriosus in Adults Harvey D. Cassidy, MD, Lynsey A. Cassidy, MD, and Joseph L. Blackshear, MD Patent ductus arteriosus (PDA) is an uncommon clinical
BRIEF REPORT Incidental Discovery of a Patent Ductus Arteriosus in Adults Harvey D. Cassidy, MD, Lynsey A. Cassidy, MD, and Joseph L. Blackshear, MD Patent ductus arteriosus (PDA) is an uncommon clinical
Patent Ductus Arteriosus Ligation in Extremely Preterm Infants and Death or Neurodevelopmental Impairment. Dany Weisz
 Patent Ductus Arteriosus Ligation in Extremely Preterm Infants and Death or Neurodevelopmental Impairment by Dany Weisz A thesis submitted in conformity with the requirements for the degree of Masters
Patent Ductus Arteriosus Ligation in Extremely Preterm Infants and Death or Neurodevelopmental Impairment by Dany Weisz A thesis submitted in conformity with the requirements for the degree of Masters
Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care. Dr. Mark Tutschka Dr. Rob ArnAield
 Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care Dr. Mark Tutschka Dr. Rob ArnAield OBJECTIVES Provide an overview of common advanced echocardiographic techniques suitable for use
Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care Dr. Mark Tutschka Dr. Rob ArnAield OBJECTIVES Provide an overview of common advanced echocardiographic techniques suitable for use
Concepts of Imaging and Knobology
 Concepts of Imaging and Knobology Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz School of Medicine at Temple University Disclosures
Concepts of Imaging and Knobology Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz School of Medicine at Temple University Disclosures
Pattern of Congenital Heart Disease A Hospital-Based Study *Sadiq Mohammed Al-Hamash MBChB, FICMS
 Pattern of Congenital Heart Disease A Hospital-Based Study *Sadiq Mohammed Al-Hamash MBChB, FICMS ABSTRACT Background: The congenital heart disease occurs in 0,8% of live births and they have a wide spectrum
Pattern of Congenital Heart Disease A Hospital-Based Study *Sadiq Mohammed Al-Hamash MBChB, FICMS ABSTRACT Background: The congenital heart disease occurs in 0,8% of live births and they have a wide spectrum
Case Report DOUGLAS H. KING, MD, JAMES C. HUHTA, MD, HOWARD P. GUTGESELL, MD, FACC, DAVID A. OTT, MD*
 lacc Vol. 4, No.2 August 198'
lacc Vol. 4, No.2 August 198'
Transposition of the Great Arteries Preoperative Diagnostic Considerations. John Simpson Evelina Children s Hospital London, UK
 Transposition of the Great Arteries Preoperative Diagnostic Considerations John Simpson Evelina Children s Hospital London, UK Areas to be covered Definitions Scope of occurrence of transposition of the
Transposition of the Great Arteries Preoperative Diagnostic Considerations John Simpson Evelina Children s Hospital London, UK Areas to be covered Definitions Scope of occurrence of transposition of the
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Pediatric Cardiology. Spontaneous Closure of Atrial Septal Defects in Premature vs Full-Term Neonates
 Pediatr Cardiol 21:129 134, 2000 DOI: 10.1007/s002469910020 Pediatric Cardiology Springer-Verlag New York Inc. 2000 Spontaneous Closure of Atrial Septal Defects in Premature vs Full-Term Neonates T. Riggs,
Pediatr Cardiol 21:129 134, 2000 DOI: 10.1007/s002469910020 Pediatric Cardiology Springer-Verlag New York Inc. 2000 Spontaneous Closure of Atrial Septal Defects in Premature vs Full-Term Neonates T. Riggs,
AORTIC COARCTATION. Synonyms: - Coarctation of the aorta
 AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
Color Doppler Differentiation of Physiological from Pathological Mitral Regurgitation(MR): Avoiding The Fabrication of MR
: Avoiding The Fabrication of MR") Color Doppler Differentiation of Physiological from Pathological Mitral Regurgitation(MR): Avoiding The Fabrication of MR Ghassan Dalati MD, Glen P Kelly M.D, Fakhri Dalati M.D, Frederick Helmcke MD, D.
Color Doppler Differentiation of Physiological from Pathological Mitral Regurgitation(MR): Avoiding The Fabrication of MR Ghassan Dalati MD, Glen P Kelly M.D, Fakhri Dalati M.D, Frederick Helmcke MD, D.
PRACTICAL GUIDE TO FETAL ECHOCARDIOGRAPHY IC Huggon and LD Allan
 PRACTICAL GUIDE TO FETAL ECHOCARDIOGRAPHY IC Huggon and LD Allan Fetal Cardiology Unit, Harris Birthright Research Centre for Fetal Medicine, King's College Hospital, London, UK IMPORTANCE OF PRENATAL
PRACTICAL GUIDE TO FETAL ECHOCARDIOGRAPHY IC Huggon and LD Allan Fetal Cardiology Unit, Harris Birthright Research Centre for Fetal Medicine, King's College Hospital, London, UK IMPORTANCE OF PRENATAL