Single Pill Combinations Versus Generics: Prescribing Practices in a New Healthcare Era
|
|
|
- Ernest Townsend
- 6 years ago
- Views:
Transcription

1 Activity Code FM285
2 Single Pill Combinations Versus Generics: Prescribing Practices in a New Healthcare Era Monica Gandhi MD, MPH Clinic Director, Ward 86 HIV Clinic, SFGH/UCSF

3 Learning Objectives Upon completion of this presentation, learners should be better able to: Review the role of single pill combinations (SPCs) in HIV treatment and the advantages and disadvantages of available SPCs Assess how the availability of generics may change cost-benefit considerations for SPCs in HIV treatment
 Pros and cons Anticipated SPCs for HIV SPCs,")
4 Outline The problem of adherence Does co-formulating the pills help? Current single pill combinations (SPCs) Pros and cons Anticipated SPCs for HIV SPCs, healthcare reform and generics
5 Case 52 yo AA man with HIV CD4 257, viral load 17,000 copies/ml, marginally housed, depression, and polysubstance use. Presents to SFGH with PNA. Pt originally diagnosed w/ HIV in 05 and has had trouble adhering to ARVs in past. After treatment for PNA, ID Consult Service called for ARV recommendations. Virus W.T., HLA-B5701 negative, Cr 1.0, LFTs WNL; team concerned about adherence
6 Which ART regimen would you start given the pt s problems with adherence? A. TDF/FTC/EFV B. TDF/FTC + darunavir/ritonavir C. TDF/FTC + atazanavir/ritonavir D. TDF/FTC + raltegravir E. TDF/FTC/EVG/cobicistat F. ABC/3TC + dolutegravir 14% 14% 14% 14% 14% 14% 14% G. TDF/FTC + dolutegravir A. B. C. D. E. F. G. 8
7 Case (continued) The patient was prescribed multi-pill ART 2 months ago but hasn t taken regularly, because taking out lots of pills in the shelter just announces to the world that I have AIDS. Pt states he would take medications regularly if he could just take one pill once a day. Not on concomitant meds, but has h/o HTN and pt says he wants one pill so they will think this is for my blood pressure


8 Adherence Nonadherence has been labeled America s other drug problem National Council on Patient Information and Education: statistics on medicine use and compliance. utrx.org/
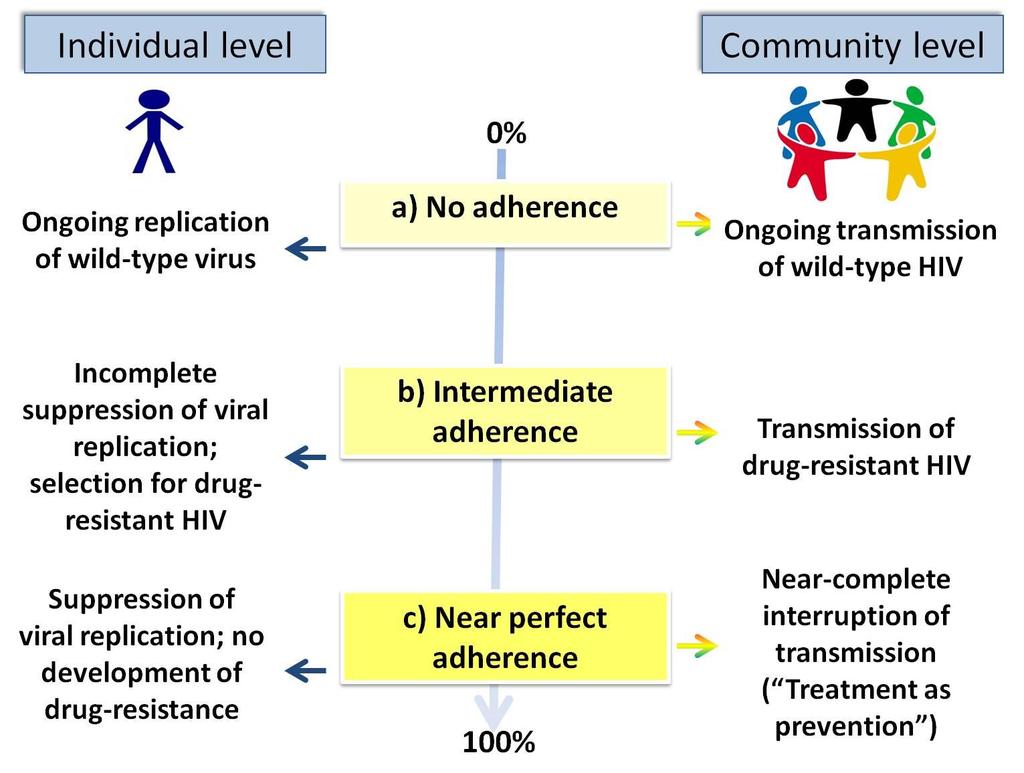
9 In era of universal ART in U.S., adherence is key HIV Infection ART is recommended for all HIVpositive individuals for individual and community-level benefits DHHS. Guidelines for the use of antiretroviral agents in HIV-1 infected adults and adolescents; Available at: March 27, 2012; last updated 5/1/14
10


 3")
11 CDC vital statistics Vital Signs: HIV Prevention Through Care and Treatment United States, MMWR December 2, 2011 / 60(47); Medical Monitoring Project (MMP) 3 surveillance datasets. Adherence

12 The Clinical Problem Multiple adherence barriers Combination ART- Major benefits for individual and community, but requires lifelong adherence to multicomponent therapy Depression Race/ethnicity Alcohol/substance use Younger age Pill fatigue Side effects Stigma
13 A new era
14 Which is your preferred SPC for HIV? A. TDF/FTC/efavirenz B. TDF/FTC/rilpivirine C. TDF/FTC/ elvitegravir/ cobicistat D. I am still waiting for my favorite SPC for HIV 25% 25% 25% 25% A. B. C. D. 8
15 Era of many options Nucleoside and nucleotide RTIs Zidovudine, AZT Abacavir, ABC Lamivudine, 3TC Didanosine, ddi Stavudine, d4t Tenofovir, TFV Emtricitabine, FTC AZT/3TC AZT/3TC/ABC 3TC/ABC TDF/FTC CCR5 receptor blocker Maraviroc Integrase inhibitor Raltegravir Elvitegravir Dolutegravir NNRTI s: Delavirdine (DLV) Nevirapine, NVP Efavirenz, EFV Etravirine Rilpivirine Fusion inhibitors: Enfuvirtide, ENF or T20 Combination (1 pill once daily) EFV/FTC/TDF RPV/FTC/TDF ELV/cobicistat/FTC/TDF Protease inhibitors: Indinavir, IDV Saquinavir, SQV Nelfinavir, NFV Amprenavir, APV Atazanavir, ATZ Fosamprenavir, FPV Lopinavir/ritonavir Tipranavir Darunavir red combination agents
16 HIV = SPC dream state? Need for multiple pills Can t be started sequentially; must be simultaneous Stigma, depression can make multiple pill-taking difficult Mistakes in taking one pill and not another can lead to resistance Near perfect adherence counseled
17 What s the evidence in HIV? Don t have much data comparing SPCs to free components Meta-analysis of 19 RCTs (n=6321) showed modestly better adherence with once daily versus BID (+2.55%, p <0.002); no difference in virologic outcomes Better adherence and virologic suppression rates with lower pill burden Parienti CID 2010; Nachega AB CID 2014 Favors twice daily Favors once daily
 compared to historical controls Higher rates of virologic suppression (69% v. 46%, p 0.")
18 Few studies in HIV REACH cohort Unannounced pill counts in marginally housed patients on TDF/FTC/EFV: mean adherence to SPC 86% versus 73% (p=0.001) compared to historical controls Higher rates of virologic suppression (69% v. 46%, p 0.02) mediated by adherence Treatment simplification trials Suppression maintained, happy patients Bangsberg AIDS 2010; Dejesus JAIDS 2009; Hodder AIDS Patient Care STDs 2010; Airoldi Patient Preference Adher 2010
19 3 retrospective observational studies,?confounding by indication Study design N Comparison Commercially insured database (Sax P, PLOS ONE 2012) Medicaid patients (Cohen CJ, BMJ Open, 2013) VA cohort (Rao, 53 rd ICAAC, 2013) 7,073 SPCs versus 3 pills per day 7,381 SPCS versus 2 pills per day 15,600 SPCS versus 2 pills per day h Adherence i Healthcare costs i Rate of hospitalization
20 Which SPCs are available? TFV/FTC/efavirenz, approved 2006 TFV/FTC/rilpivirine, approved 2011 TFV/FTC/elvitegravir/ cobicistat, approved 2012 Soon? ABC/3TC/dolutegravir (Filed to FDA 10/22/13)
21 Pros and cons of each PROS Long track record of safety and effectiveness TDF/FTC/EFV CONS Potentially teratogenic (don t worry about this) Neuropsychiatric effects Raises lipid levels Rash To ameliorate side effects, often dosed at bedtime; food increases absorption, which may increase adverse effects
22 PROS Lower rate of CNS and rash events than EFV More favorable lipid effects Pregnancy class B TDF/FTC/RPV CONS Higher failure with pre-therapy HIV-1 RNA levels >100,000 (also CD4 <200 adherence <95%) Needs solid meal (390 kcal + 12g fat studied, protein shake i absorption ~50%) Needs acid for absorption (no PPIs; space antacids, H2 blockers) Caution with drugs that prolong QT
23 PROS Lower rate of CNS and rash events than EFV More favorable lipid effects Pregnancy class B TDF/FTC/EVG/COBI CONS Cobi inhibits tubular secretion of creatinine, h serum Cr mg/dl (mean 0.14), early, reversible Approved only if GFR > 70 ml/min Cross resistance with RAL CYP3A4 inhibitor drug-drug interactions (statins, rifamycins, anticonvulsants, etc.) Take with food (studied w/ 373kcal, 20% fat) Separate from cation-containing antacids by 2 hours (Mg, Al, Ca)
 D. Increase transit time of medication in gut 25% 25% 25% 25% A. B.")
24 Why can t you co-administer elvitegravir with cationcontaining antacids? A. Reduces gastric absorption of medication B. Efflux transporter in gut ph-dependent C. Metal chelation of drug in gut (Integrase inhibitors bind to Mg 2+ at catalytic site of integrase) D. Increase transit time of medication in gut 25% 25% 25% 25% A. B. C. D. 8
 and Lancet ID (96 wks) SAILING: Cahn P. Lancet 2013 (48 wks) and IAS 2013 (96 wks) VIKING : Eron JJ.")
25 Next anticipated SPC Dolutegravir approved 8/12/13 for use in HIVinfected adults and children > 12 weighing 40kg Five major trials investigating its use in naïve and experienced patients SINGLE: Walmsley S. NEJM 2013 SPRING-2: Raffi F. et al. Lancet 2013 (48 wks) and Lancet ID (96 wks) SAILING: Cahn P. Lancet 2013 (48 wks) and IAS 2013 (96 wks) VIKING : Eron JJ. JID 2013, Nichols G CID 2014 FLAMINGO: Clotet B. Lancet 2014

26 Which were the 3 dolutegravir trials conducted in treatment naïve patients? A. VIKING, SPRING-2, SINGLE B. FLAMINGO, SPRING-2, SINGLE C. SAILING, SPRING-2, SINGLE D. I cannot keep these trial names straight, but I heard the drug works 25% 25% 25% 25% A. B. C. D. 8
27 Study Patient population Main outcome Dose SINGLE 1 Treatment naïve (ABC/3TC + DTG vs TDF/FTC/EFV) DTG regimen superior to EFV, driven mainly by more discontinuations with EFV 50mg once daily SPRING-2 2,3 Treatment-naïve (TDF/FTC or ABC/3TC with either DTG or RAL) DTG regimen non-inferior to RAL-based regimens 50mg once daily FLAMINGO 4 Treatment naïve (TDF/FTC or ABC/3TC with either DTG or DRV/r) DTG regimen superior to DRV/r, driven mainly by more discontinuations or f/u loss with DRV/r; more virologic response with DTG in viral loads >100,000 copies/ml group 50mg once daily SAILING 5,6 ART-experienced, INSTI-naïve patients with at least 2-class resistance: DTG vs RAL with OBR DTG regimen superior to RAL, driven by more discontinuations, virologic failures and treatment-emergent resistance with RAL 50mg once daily VIKING-3 7,8 LATTE (Phase IIB) 9 Patients with resistance to 2 or more ART classes, including INSTI. DTG vs optimized Treatment naïve GSK744 (dolutegravir analog with long half-life- 40 hours) + rilpivirine; Induction with 3 doses of NRTIs, switch to 744 +RPV vs 2 NRTIs + EFV. DTG regimen superior to optimized regimen with failures most prominent (76%) in patients with the Q148H/R +2 other mutations 82% of 744+RPV and 71% of EFV + NRTIs HIV-1 RNA <50 (ITT 93% 744+RPV and 94% EFV + NRTIs <50); Similar response rate across all 3 doses of 744; 1 subject with low 744 and RPV concentrations emerged INI and NNRTI mutations 50mg po twice daily 744 oral dose 10mg, 30mg, 60mg 1 Walmsley S. NEJM 2013; 2 Raffi F. Lancet 2013; 3 Raffi F. Lancet ID 2013; 4 Clotet B. Lancet 2014; 5 Cahn P. Lancet 2013; 6 Cahn P. IAS 2013; 7 Eron J.J. JID 2013; 8 Nichols G. CID 2014; 9 Margolis D. CROI 2014 (91LB)
28 What data does a company need to show to get a SPC approved? A. That the free drugs can actually be put into the same pill B. Phase I clinical trial data that the SPC is safe C. Phase III clinical trial data that the SPC is equivalent to the free components in patients D. Pharmacokinetic bioequivalence data that the SPC gives same general PK parameters as free components 25% 25% 25% 25% A. B. C. D. 8
 Weller S. JAIDS May 4, 2014")
29 Bioequivalence data for SPC 62 patients received DTG/ABC/3TC SPC vs DTG and ABC/3TC in single-dose open label randomized 2-period cross over study (also showed no significant effects of food) Weller S. JAIDS May 4, 2014
30 ABC/3TC + DOLUTEGRAVIR PROS Superior to efavirenz and DRV/r regimens in SINGLE, FLAMINGO (driven by d/c s in non-dol arm); non-inferior to raltegravirbased regimens in SPRING-2, superior in SAILING Well tolerated No food restrictions ABC/3TC backbone can be used in mild renal insufficiency (GFR >50 ml/min) Pregnancy class B Seems to have high genetic barrier to resistance Retains activity against some RAL, EVGresistance viruses October 22, 2013: SPC filed with FDA for approval CONS Inhibits creatinine secretion (mean rise Cr 0.11mg/dL) Abacavir needs HLA-B5701 testing Separate from Mg, Al, Ca-containing antacids by 2 hours Limited clinical experience (8/12/13) increase dose with concomitant rifampin, efavirenz; don't give with etravirine unless PIs present; no dose adjustments with rilpivirine
31 What is the next likely SPC to be developed? A. TAF/FTC/ELV/Cobi B. ATV/Cobi/TDF/FTC C. DRV/Cobi/TDF/FTC D. Dolutegravir/TDF/ FTC 25% 25% 25% 25% A. B. C. D. 8

32 TAF/FTC/ELV/Cobi Tenofovir alafenemide fumarate (TAF) Phase II study - Similar virologic efficacy, smaller decrease in egfr and smaller decrease in bone mineral density at 48 weeks with FTC/ELV/COBI Sax P. 53 rd ICAAC, Sept 2013, A1464d
33 Patients achieving a human immunodeficiency virus type 1 (HIV-1) RNA load of < 50 copies/ml through week 48 of the study, according to missing-equals-failure intention-totreat analysis. Week 48 results of atazanavir/ritonavir vs atazanavir/cobicistat Gallant J E et al. J Infect Dis. 2013;208:32-39
34 Darunavir/cobicistat
/COBI single pill combinations")
35 Kakuda T. IAS 2013 PIs co-formulated with cobicistat Data to date paves the way for eventual TDF/FTC/PI (ATV or DRV)/COBI single pill combinations Darunavir/cobicistat submitted to European Medicines Agency for approval 10/15/13 Atazanavir/cobicistat submitted to FDA April 2-14
36 Sign me up! or What did one cost-effectiveness study estimate as the cost-savings of switching TDF/FTC/EFV to 3 generic drugs? A. $5 million per year B. $10 million per year C. $100 million per year D. $1 billion per year 25% 25% 25% 25% A. B. C. D. 8
37 Cost considerations generic era and ACA Changing TDF/FTC/EFV SPC to a 3-pill regimen of generic EFV, generic 3TC and branded TDF would save almost a billion dollars per year, with a relatively small reduction in treatment efficacy Areas of uncertainty Walensky. Ann Intern Med 2013

38 Cost section, DHHS guidelines New cost section, DHHS guidelines ARVs $10,000/yr in resource-rich settings Branded combinations likely to cost patient more in co-pays, may be prohibitive Prior authorizations may help costs, but more likely to reduce prescribing Save money in reduced lab monitoring DHHS. Guidelines for the use of antiretroviral agents in HIV-1 infected adults and adolescents; Available at: 5/1/14
39 Follow-up on case You start an SPC in your marginally-housed patient and he is able to take it with him in the morning and adhere daily to the meds His Section 8 housing comes through and he moves into place with access to food, stabilized CD4 406 and viral load undetectable 6 months and thereafter You are patient s favorite provider!
40 Key clinical points HIV-1 is now a chronic controllable condition, requiring lifelong daily adherence to a combination of antiretroviral medications Inadequate adherence leads to HIV-1 resistance in individuals and ongoing transmission (including of drug-resistant virus) in communities Single pill combinations improve adherence in other chronic disease states Three SPCs currently marketed for HIV-1 infection, each with unique benefits/limitations, others in development Initial considerations are whether TDF/FTC is right for your patient, whether you want a PI, renal function Consider also drug resistance, HIV-1 RNA level and CD4 cell count, potency, durability of response, tolerability, food issues, drug-drug interactions, access and cost
41
42 Activity Code FM285
Starting and Switching ART: 2016
 Starting and Switching ART: 2016 Luke Jerram Rajesh T. Gandhi, M.D. Massachusetts General Hospital Harvard Medical School Disclosures: grant support from EBSCO, Gilead, Merck, Viiv Thanks to Henry Sunpath,
Starting and Switching ART: 2016 Luke Jerram Rajesh T. Gandhi, M.D. Massachusetts General Hospital Harvard Medical School Disclosures: grant support from EBSCO, Gilead, Merck, Viiv Thanks to Henry Sunpath,
HIV Treatment: State of the Art 2013
 HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches
 Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Pharmacological considerations on the use of ARVs in pregnancy
 Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
ARVs in Development: Where do they fit?
 The picture can't be displayed. ARVs in Development: Where do they fit? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker
The picture can't be displayed. ARVs in Development: Where do they fit? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker
ART and Prevention: What do we know?
 ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Antiretroviral Treatment 2014
 Activity Code FM285 Antiretroviral Treatment 2014 Rajesh Gandhi, MD Masssachusetts General Hospital Disclosures: Educational grants to my institution from Janssen, Viiv, Abbott Learning Objectives Upon
Activity Code FM285 Antiretroviral Treatment 2014 Rajesh Gandhi, MD Masssachusetts General Hospital Disclosures: Educational grants to my institution from Janssen, Viiv, Abbott Learning Objectives Upon
HIV Treatment: New and Veteran Drugs Classes
 HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
Antiretroviral Therapy: What to Start
 FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
The ART of Managing Drug-Drug Interactions in Patients with HIV
 The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
Third Agent Advantages Disadvantages. Component Tenofovir/emtricitabine (TDF/FTC) 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily
 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily") Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
Simplifying HIV Treatment Now and in the Future
 Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
SELECTING THE BEST ART FOR EACH PATIENT
 SELECTING THE BEST ART FOR EACH PATIENT Corklin R Steinhart, MD, PhD Head, Global Medical Directors ViiV Healthcare CNVX/HIVP/0025/16 5th Asian Conference on Hepatitis & AIDS 第五届亚洲肝炎与艾滋病学术会议 28-29 May
SELECTING THE BEST ART FOR EACH PATIENT Corklin R Steinhart, MD, PhD Head, Global Medical Directors ViiV Healthcare CNVX/HIVP/0025/16 5th Asian Conference on Hepatitis & AIDS 第五届亚洲肝炎与艾滋病学术会议 28-29 May
Disclosures. Update on HIV Drug Therapy: A Case based Discussion. Case # 1: Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv
 Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
STRIBILD (aka. The Quad Pill)
") NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
Continuing Education for Pharmacy Technicians
 Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
 Initial Therapy for Antiretroviral Naïve HIV Infected Patients Michelle Cespedes, MD, MS Associate Professor of Medicine Division of Infectious Disease Icahn School of Medicine at Mount Sinai Disclosures
Initial Therapy for Antiretroviral Naïve HIV Infected Patients Michelle Cespedes, MD, MS Associate Professor of Medicine Division of Infectious Disease Icahn School of Medicine at Mount Sinai Disclosures
HIV - Therapy Principles
 HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
Selecting an Initial Antiretroviral Therapy (ART) Regimen
 Regimen") Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
Criteria for Oral PrEP
 Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
L infettivologia del 3 millennio: AIDS ed altro
 L infettivologia del 3 millennio: AIDS ed altro VI Convegno Nazionale 15-16 -17 maggio 2014 Centro Congressi Hotel Ariston Paestum (SA) Nuove molecole ad azione anti-hiv Annalisa Saracino Clinica Malattie
L infettivologia del 3 millennio: AIDS ed altro VI Convegno Nazionale 15-16 -17 maggio 2014 Centro Congressi Hotel Ariston Paestum (SA) Nuove molecole ad azione anti-hiv Annalisa Saracino Clinica Malattie
HIV Update Allegra CPD Day Program Port Elizabeth Dr L E Nojoko
 HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
Case # 1. Case #1 (cont d)
") Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
Antiretroviral Dosing in Renal Impairment
 Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
The next generation of ART regimens
 The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
ACTHIV 2018: A State-of-the-Science Conference for Frontline Health Professionals
 Antiretroviral Medications: What you need to know Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Associate Professor, Department of Pharmacy Practice Jefferson College of Pharmacy, Thomas Jefferson University
Antiretroviral Medications: What you need to know Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Associate Professor, Department of Pharmacy Practice Jefferson College of Pharmacy, Thomas Jefferson University
HIV 101. Applications of Antiretroviral Therapy
 HIV 101. Applications of Antiretroviral Therapy Michael S. Saag, MD Professor of Medicine Associate Dean for Global Health Jim Straley Chair in AIDS Research University of Alabama at Birmingham Birmingham,
HIV 101. Applications of Antiretroviral Therapy Michael S. Saag, MD Professor of Medicine Associate Dean for Global Health Jim Straley Chair in AIDS Research University of Alabama at Birmingham Birmingham,
VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects
 VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects IL/DLG/0040/14 June 2014 GSK (Israel) Ltd. Basel 25, Petach Tikva. Tel-03-9297100 Medical information service: il.medinfo@gsk.com
VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects IL/DLG/0040/14 June 2014 GSK (Israel) Ltd. Basel 25, Petach Tikva. Tel-03-9297100 Medical information service: il.medinfo@gsk.com
Integrase Strand Transfer Inhibitors on the Horizon
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Integrase Strand Transfer Inhibitors on the Horizon David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Integrase Strand Transfer Inhibitors on the Horizon David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, University of Washington Presentation
ART: The New, The Old and The Ugly
 ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
Antiretroviral Drugs
 Antiretroviral Drugs Dr Paddy Mallon UCD HIV Molecular Research Group Associate Dean for Research and Innovation UCD School of Medicine and Medical Science paddy.mallon@ucd.ie UCD School of Medicine &
Antiretroviral Drugs Dr Paddy Mallon UCD HIV Molecular Research Group Associate Dean for Research and Innovation UCD School of Medicine and Medical Science paddy.mallon@ucd.ie UCD School of Medicine &
COMPREHENSIVE ANTIRETROVIRAL TABLE: ADULT DOSING, DOSAGE FORM MODIFICATIONS, ADVERSE REACTIONS and INTERACTION POTENTIAL
 Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
Dolutegravir: Pros and Cons (Are There Any Cons?)
") Mountain West AIDS Education and Training Center Dolutegravir: Pros and Cons (Are There Any Cons?) Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director, MW AETC
Mountain West AIDS Education and Training Center Dolutegravir: Pros and Cons (Are There Any Cons?) Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director, MW AETC
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop
 HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
Medication Errors Focus on the HIV-Infected Patient
 Medication Errors Focus on the HIV-Infected Patient Nimish Patel, Pharm.D., Ph.D., AAHIVP Associate Professor Albany College of Pharmacy & Health Sciences I do not have any conflict of interest in relation
Medication Errors Focus on the HIV-Infected Patient Nimish Patel, Pharm.D., Ph.D., AAHIVP Associate Professor Albany College of Pharmacy & Health Sciences I do not have any conflict of interest in relation
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD
 More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD More Options, Some Opinions: Initial Therapies for HIV Judith S. Currier, MD University of California Los Angeles Los Angeles,
More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD More Options, Some Opinions: Initial Therapies for HIV Judith S. Currier, MD University of California Los Angeles Los Angeles,
Approach to a Patient Newly Diagnosed with HIV, Including ART Basics Rajesh T. Gandhi, M.D.
 Approach to a Patient Newly Diagnosed with HIV, Including ART Basics Rajesh T. Gandhi, M.D. Disclosures: grant support from Gilead, Roche, EBSCO Objectives Apply current guidelines to initial evaluation
Approach to a Patient Newly Diagnosed with HIV, Including ART Basics Rajesh T. Gandhi, M.D. Disclosures: grant support from Gilead, Roche, EBSCO Objectives Apply current guidelines to initial evaluation
ANTIRETROVIRAL TREATMENTS (Part 1of
 CCR5 CO-RECEPTOR ANTAGONISTS maraviroc (MVC) Selzentry 25mg, 75mg, FUSION INHIBITORS 20mg/mL ANTIRETROVIRAL TREATMENTS (Part 1of 5) oral soln enfuvirtide (ENF, T-20) Fuzeon 90mg/mL pwd for SC inj after
CCR5 CO-RECEPTOR ANTAGONISTS maraviroc (MVC) Selzentry 25mg, 75mg, FUSION INHIBITORS 20mg/mL ANTIRETROVIRAL TREATMENTS (Part 1of 5) oral soln enfuvirtide (ENF, T-20) Fuzeon 90mg/mL pwd for SC inj after
Actualización y Futuro en VIH
 Actualización y Futuro en VIH Dr. Santiago Moreno Servicio de Enfermedades Infecciosas Hospital U. Ramón y Cajal. Universidad de Alcalá. IRYCIS. Madrid Agenda Control of the HIV-epidemic Coinfections Antiretroviral
Actualización y Futuro en VIH Dr. Santiago Moreno Servicio de Enfermedades Infecciosas Hospital U. Ramón y Cajal. Universidad de Alcalá. IRYCIS. Madrid Agenda Control of the HIV-epidemic Coinfections Antiretroviral
Principles of Antiretroviral Therapy
 Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
When to Start ART. Reduction in HIV transmission. ? Reduction in HIV-associated inflammation and associated complications» i.e. CV disease, neuro, etc
 When to Start ART Exact CD4 count at which to initiate therapy not known, but evidence points to starting at higher counts Current recommendation: ART for all patients with CD4 count of
When to Start ART Exact CD4 count at which to initiate therapy not known, but evidence points to starting at higher counts Current recommendation: ART for all patients with CD4 count of
First line ART Rilpirivine A New NNRTI. Chris Jack Physician, Durdoc Centre ethekwini
 First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
SINGLE. Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects
 in treatment-naïve subjects") SINGLE Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects SE/HIV/0023/14 January 2014 PHASE III DTG TRIALS IN TREATMENT-NAÏVE ADULT SUBJECTS WITH HIV SINGLE 1 N=833 Phase III non-inferiority,
SINGLE Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects SE/HIV/0023/14 January 2014 PHASE III DTG TRIALS IN TREATMENT-NAÏVE ADULT SUBJECTS WITH HIV SINGLE 1 N=833 Phase III non-inferiority,
Second-Line Therapy NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
2 nd Line Treatment and Resistance. Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012
 2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
Didactic Series. Switching Regimens in the Setting of Virologic Suppression
 Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
Didactic Series. CROI 2014 Update. March 27, 2014
 Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
Are the current doses of ARV correct. Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine
 Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
Cases from the Clinic(ians): Case-Based Panel Discussion
: Case-Based Panel Discussion") Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
Switching antiretroviral therapy to safer strategies based on integrase inhibitors
 Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
Update on Antiretroviral Treatment for HIV Infection 2008
 Update on Antiretroviral Treatment for HIV Infection 2008 Janet Gilmour MD FRCP(C) Clinical Associate Professor of Medicine University of Calgary November 2008 Disclosure and Acknowledgements Disclosure:
Update on Antiretroviral Treatment for HIV Infection 2008 Janet Gilmour MD FRCP(C) Clinical Associate Professor of Medicine University of Calgary November 2008 Disclosure and Acknowledgements Disclosure:
TDF containing ART: Efficacy and Safety. Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia
 TDF containing ART: Efficacy and Safety Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia 1 Indications Treatment of HIV-1 in combination with other antiretroviral
TDF containing ART: Efficacy and Safety Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia 1 Indications Treatment of HIV-1 in combination with other antiretroviral
Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi
 6 th INFECtivology TOday Paestum 15-16 -17 maggio 2014 Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi Istituto Nazionale per le Malattie
6 th INFECtivology TOday Paestum 15-16 -17 maggio 2014 Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi Istituto Nazionale per le Malattie
COMPREHENSIVE ANTIRETROVIRAL TABLE: ADULT DOSING**, DOSAGE FORM MODIFICATIONS, ADVERSE REACTIONS and INTERACTION POTENTIAL
 COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir) Stavudine
COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir) Stavudine
ARVs on an Empty Stomach: Food Interaction Studies in a resource Limited Setting
 ARVs on an Empty Stomach: Food Interaction Studies in a resource Limited Setting Dr. Andrew D Kambugu, FRCP (UK) Infectious Diseases Institute, Makerere University Outline of Discussion Key Definitions
ARVs on an Empty Stomach: Food Interaction Studies in a resource Limited Setting Dr. Andrew D Kambugu, FRCP (UK) Infectious Diseases Institute, Makerere University Outline of Discussion Key Definitions
HIV Drugs and the HIV Lifecycle
 HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
HIV Drugs and the HIV Lifecycle Together, we can change the course of the HIV epidemic one woman at a time. #onewomanatatime #thewellproject All HIV drugs work by interrupting different steps in HIV's
INTERGRASE INHIBITORS- WHAT S NEW?
 INTERGRASE INHIBITORS- WHAT S NEW? Professor Margaret Johnson Royal Free London Foundation Trust October 2018 Targeting the HIV life-cycle NEW HIV VIRON MATURATION CO-RECEPTOR BINDING FUSION BUDDING CD4
INTERGRASE INHIBITORS- WHAT S NEW? Professor Margaret Johnson Royal Free London Foundation Trust October 2018 Targeting the HIV life-cycle NEW HIV VIRON MATURATION CO-RECEPTOR BINDING FUSION BUDDING CD4
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care
 Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
Update on HIV Drug Resistance. Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School
 Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
Updates to the HHS Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents Living with HIV Updated October 17, 2017
 Mountain West AIDS Education and Training Center Updates to the HHS Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents Living with HIV Updated October 17, 2017 26 October 2017 Hillary
Mountain West AIDS Education and Training Center Updates to the HHS Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents Living with HIV Updated October 17, 2017 26 October 2017 Hillary
Outline Epidemiology: Global and U.S. How are we doing in terms of goals of treatment? Updates in the fast moving field of HIV medicine EPIDEMIOLOGY
 Updates in the fast moving field of HIV medicine 35 th Advances in Infectious Diseases April 25, 2014 Monica Gandhi MD, MPH Professor of Medicine and Clinic Director ( Ward 86 ), Division of HIV/AIDS San
Updates in the fast moving field of HIV medicine 35 th Advances in Infectious Diseases April 25, 2014 Monica Gandhi MD, MPH Professor of Medicine and Clinic Director ( Ward 86 ), Division of HIV/AIDS San
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 03/07/18 SECTION: DRUGS LAST REVIEW DATE: 02/19/19 LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
Approach for the Newly Diagnosed HIV Positive Patient
 Approach for the Newly Diagnosed HIV Positive Patient Jason E. Farley, PhD, MPH, ANP-BC, FAAN, AACRN Associate Professor & NP, Johns Hopkins University School of Nursing & Medicine Director, AETC Adult-Gerontology
Approach for the Newly Diagnosed HIV Positive Patient Jason E. Farley, PhD, MPH, ANP-BC, FAAN, AACRN Associate Professor & NP, Johns Hopkins University School of Nursing & Medicine Director, AETC Adult-Gerontology
1/13/16. Updated April 2015
 Bernadette Jakeman, PharmD, PhC, BCPS, AAHIVP Assistant Professor UNM College of Pharmacy bjakeman@salud.unm.edu Pharmacist objectives: 1. Summarize key updates to the DHHS treatment guidelines. 2. Identify
Bernadette Jakeman, PharmD, PhC, BCPS, AAHIVP Assistant Professor UNM College of Pharmacy bjakeman@salud.unm.edu Pharmacist objectives: 1. Summarize key updates to the DHHS treatment guidelines. 2. Identify
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
Genotypic Resistance Testing in Routine Care in South Africa:
 Genotypic Resistance Testing in Routine Care in South Africa: Is the Juice Worth the Squeeze? Mark Siedner Africa Health Research Institute Harvard Medical School Conflicts of Interest^* No financial conflicts
Genotypic Resistance Testing in Routine Care in South Africa: Is the Juice Worth the Squeeze? Mark Siedner Africa Health Research Institute Harvard Medical School Conflicts of Interest^* No financial conflicts
Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update
 Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
HIV Management Update 2015
 9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
9/30/15 HIV Management Update 2015 Larry Pineda, PharmD, PhC, BCPS Visiting Assistant Professor Pharmacy Practice and Administrative Science ljpineda@salud.unm.edu Pharmacist Learning Objectives Describe
HIV in in Women Women
 HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
HIV Treatment Update. Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London
 HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
Somnuek Sungkanuparph, M.D.
 HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
Second and third line paediatric ART strategies
 Second and third line paediatric ART strategies Dr. Marape Marape Assistant Professor Ohio University School of Health Professions Gaborone, Botswana Marape Marape MB, BCh, BAO, MPH, PhD Assistant Professor
Second and third line paediatric ART strategies Dr. Marape Marape Assistant Professor Ohio University School of Health Professions Gaborone, Botswana Marape Marape MB, BCh, BAO, MPH, PhD Assistant Professor
Case 1 continued. Case 1 (cont) 12/8/16. MMAH Debate Panel Thursday, December 8, Case 1
 12/8/16. MMAH Debate Panel Thursday, December 8, Case 1") MMAH Debate Panel Thursday, December 8, 2016 Case 1 HPI 55 yo man with newly diagnosed HIV initiates care in your clinic. His CD4+ cell count is 600, with HIV VL=90,000 copies/ml. He is asymptomatic at
MMAH Debate Panel Thursday, December 8, 2016 Case 1 HPI 55 yo man with newly diagnosed HIV initiates care in your clinic. His CD4+ cell count is 600, with HIV VL=90,000 copies/ml. He is asymptomatic at
SA HIV Clinicians Society Adult ART guidelines
 SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
DNA Genotyping in HIV Infection
 Frontier AIDS Education and Training Center DNA Genotyping in HIV Infection Steven C. Johnson M.D. Director, University of Colorado HIV/AIDS Clinical Program; Professor of Medicine, Division of Infectious
Frontier AIDS Education and Training Center DNA Genotyping in HIV Infection Steven C. Johnson M.D. Director, University of Colorado HIV/AIDS Clinical Program; Professor of Medicine, Division of Infectious
2/10/2015. Switching from old regimens. HIV treatment revision: As simple as old versus new? What is an old regimen? What is an old regimen?
 Switching from old regimens David Nolan Department of Immunology, Royal Perth Hospital, Western Australia Institute for Immunology and Infectious Diseases, Murdoch University, Western Australia What is
Switching from old regimens David Nolan Department of Immunology, Royal Perth Hospital, Western Australia Institute for Immunology and Infectious Diseases, Murdoch University, Western Australia What is
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications
 and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications") Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
Clinical Commissioning Policy: Use of cobicistat (Tybost ) as a booster in treatment of HIV positive adults and adolescents
 as a booster in treatment of HIV positive adults and adolescents") Clinical Commissioning Policy: Use of cobicistat (Tybost ) as a booster in treatment of HIV positive adults and adolescents 1 Clinical Commissioning Policy: Use of cobicistat (Tybost ) as a booster in
Clinical Commissioning Policy: Use of cobicistat (Tybost ) as a booster in treatment of HIV positive adults and adolescents 1 Clinical Commissioning Policy: Use of cobicistat (Tybost ) as a booster in
A Changing Landscape: New and Pipeline HIV Therapies
 A Changing Landscape: New and Pipeline HIV Therapies Sarah Turley, PharmD, BCPS PGY2 Internal Medicine Pharmacy Resident Virginia Commonwealth University Health System Financial Disclosure I have no relevant
A Changing Landscape: New and Pipeline HIV Therapies Sarah Turley, PharmD, BCPS PGY2 Internal Medicine Pharmacy Resident Virginia Commonwealth University Health System Financial Disclosure I have no relevant
Disclosures (last 12 months)
") HIV Research What s in the Pipeline? Samir K. Gupta, MD, MS Division of Infectious Diseases Indiana University School of Medicine Disclosures (last 12 months) Independent research grant funding by NIH/NHLBI,
HIV Research What s in the Pipeline? Samir K. Gupta, MD, MS Division of Infectious Diseases Indiana University School of Medicine Disclosures (last 12 months) Independent research grant funding by NIH/NHLBI,
Class Review: HIV Antiretroviral Agents
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
0% 0% 0% Parasite. 2. RNA-virus. RNA-virus
 HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
Bon Usage des Antirétroviraux dans l Infection par le VIH
 Bon Usage des Antirétroviraux dans l Infection par le VIH Pr. Jean-Michel Molina CHU St Louis, Assistance Publique Hôpitaux de Paris, INSERM U941 et Université Paris 7 Diderot, France 1 Liens d Intérêt
Bon Usage des Antirétroviraux dans l Infection par le VIH Pr. Jean-Michel Molina CHU St Louis, Assistance Publique Hôpitaux de Paris, INSERM U941 et Université Paris 7 Diderot, France 1 Liens d Intérêt
Introduction to HIV Drug Resistance. Kevin L. Ard, MD, MPH Massachusetts General Hospital Harvard Medical School
 Introduction to HIV Drug Resistance Kevin L. Ard, MD, MPH Massachusetts General Hospital Harvard Medical School Objectives 1. Describe the epidemiology of HIV drug resistance in sub-saharan Africa. 2.
Introduction to HIV Drug Resistance Kevin L. Ard, MD, MPH Massachusetts General Hospital Harvard Medical School Objectives 1. Describe the epidemiology of HIV drug resistance in sub-saharan Africa. 2.
Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary?
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
HIV Update Objectives. Epidemiology. Epidemiology, Transmission and Natural History. Transmission Risk by Exposure. Transmission 9/29/2014
 Objectives HIV Update 2014 Jay Sizemore, MD, MPH Medical Director Chattanooga CARES Assistant Professor UTCOM Chattanooga 2October 2014 Review HIV epidemiology and screening/testing guidelines Discuss
Objectives HIV Update 2014 Jay Sizemore, MD, MPH Medical Director Chattanooga CARES Assistant Professor UTCOM Chattanooga 2October 2014 Review HIV epidemiology and screening/testing guidelines Discuss
HIV basics. Katya Calvo Medical Director of Antimicrobial Stewardship
 HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies. Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine
 Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
Antiretroviral Treatment Strategies: Clinical Case Presentation
 Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Supplementary information
 Supplementary information Dose-response Curve Slope Sets Class-Specific Limits on Inhibitory Potential of Anti-HIV Drugs Lin Shen 1,2, Susan Peterson 1, Ahmad R. Sedaghat 1, Moira A. McMahon 1,2, Marc
Supplementary information Dose-response Curve Slope Sets Class-Specific Limits on Inhibitory Potential of Anti-HIV Drugs Lin Shen 1,2, Susan Peterson 1, Ahmad R. Sedaghat 1, Moira A. McMahon 1,2, Marc
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort
 Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,
Pharmacologic Characteristics and Delivery Options for Integrase Inhibitors
 Pharmacologic Characteristics and Delivery Options for Integrase Inhibitors Courtney V. Fletcher, Pharm.D. Dean, College of Pharmacy Professor, Department of Pharmacy Practice and Division of Infectious
Pharmacologic Characteristics and Delivery Options for Integrase Inhibitors Courtney V. Fletcher, Pharm.D. Dean, College of Pharmacy Professor, Department of Pharmacy Practice and Division of Infectious