University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D
|
|
|
- Cecilia Willis
- 5 years ago
- Views:
Transcription
1 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Cardiovascular Pharmacology 1. Antihypertensives 2. Antianginal 3. Drugs for HF 4. Antiarrythemics 5. Drugs for Hyperlipoproteniemia Hypertension Hypertension is currently defined as usual BP of 140/80 mmhg. Hypertension may defined as an abnormal elevation of either SBP or DBP Hypertension is a condition that afflicts almost 1 billion people worldwide and is a leading cause of morbidity and mortality. More than 20% of Americans are hypertensive, and one-third of these Americans are not even aware they are hypertensive. Therefore, this disease is sometimes called the "silent killer" Hypertension - Etiology The are two basic types of hypertension: Primary (essential or idiopathic) hypertension Secondary hypertension Hypertension Aetiology Primary hypertension: The majority of patients (90-95%) have essential hypertension, which is a form with no identifiable underlying cause. This form of hypertension is commonly treated with drugs in addition to lifestyle changes Secondary hypertension: A smaller number of patients (5-10%) have secondary hypertension that is caused by an identifiable underlying condition. These patients are best treated by controlling or removing the underlying disease or pathology, although they may still require antihypertensive drugs Causes of 2 nd Hypertension Renal or renovascular disease Endocrine disease Phaeochomocytoma Cusings syndrome Conn s syndrome Acromegaly and hypo or hyperthyroidism Coarctation of the aorta Pre-eclampsia Stress (equivocal!!) Iatrogenic (steroid, oral contraceptive, NSAIDs) Normal <120 and <80 Prehypertensive or Stage 1 Hypertension or Stage 2 Hypertension > 160 or >100
2 Target Organs 1. Stroke 2. LVH, IHD HF 3. Nephropathy 4. Retinopathy A Significant CV and Renal Disease Risk Factor 1- Stroke 2- CAD 3- CHF LVH 4- Renal disease 5- Peripheral vascular disease 6- Morbidity 7- Disability Goal of Treatment 1- To control blood pressure. 2- To prevent complications. 3- Because the majority of patients (with mild-moderate) HT are entirely asymptomatic our primarily goal is to decrease CV risk. 4- The objective of anti-ht therapy is to decrease BP (<140/80 mmhg) or even less in high risk patient like DM. 5- The benefit of treatment is greatest in those with high risk. Non-Pharmacological Measures 1. Weight reduction (obese patients) 2. Aerobic exercise 3. Diet control low calories, low fat, moderate Na intake High in fruits and vegetables fresh rather than proceed 4. Moderation of al cohol intake (red wine) 5. Cessation of Smoking Independent risk factor Malignant HT via renal artery damage. What Determines Arterial Pressure? Arterial Pressure = Cardiac Output * Peripheral Resistance Cardiac Output affected by (Heart Rate, Filling Pressure, Contractility) Peripheral Resistance affected by (Arteriolar Radius)
3 Anti-hypertensive drugs 1. Diuretics 2. Beta Blockers 3. a 1 -adrenoceptor antagonists (a 1 -blockers) 4. a 2 -adrenoceptor agonists 5. Angiotensin Converting Enzyme Inhibitors (ACE inhibitors) 6. Angiotensin Receptor blockers (ARBs) 7. Renin Inhibitors 8. Calcium Channel Blockers (CCBs) 9. Potassium Channel openers 10. Peripheral Vasodilators Diuretics Diuretics are basically acting as antihypertensive drugs by increasing Na and H2O renal excretion thereby decreasing the blood volume and CO. This is initial effects, later on diuretics decrease PVR. As a class agents diuretics are effective in treating: 1. Patients with volume dependant form of HT (black, elderly, obese, renal). 2. HT complicated with HF. 3. Resistant HT 4. Renal impairment Thiazides Diuretics Thiazide and thiazide related agents are widely used as monotherapy or in combination with other antihypertensives (B-Blockers, ACEIs or ARBs). Low dose thiazide diuretics are effective and safe AntiHT agents in mild-moderate HT (12.5 mg of hydrochlorthiazide, chorthalidone and bendrofluzide). Low dose TD are preferred initial therapy for HT especially in elderly, obese and black patients. They are more effective in elderly and less effective in younger white. 1. TD are not effective when GFR severely reduced 2. Advantages of low dose TD: To minimize the adverse metabolic effects To decrease the risk of impotence To avoid E disturbances To avoid risk of RCCa especially in women. Loop Diuretics Loop diuretics are not usually used as AntiHT agent (short acting, required multiple daily dosing). However they are indicated in HT emergency, renal insufficiency and when multiple drugs with salt retaining properties are used.
4 B-blockers 1. Propranolol 2. Atenolol 3. Metoprolol. 4. Timolol 5. Nadolol Primarily by decreasing HR, stroke volume and so COP followed by reduction in PVR. Inhibit renin release from the kidney and so decreasing the formation of Ang II and aldosterone secretion. Release of vasodilator PGs. Blockage of prejunctional B-receptors. Ideal Profile of Anti-HT B-blockers Cardioselective Long acting (to prevent BP fluctuation) Simple Pks profile (good patient compliance) Effective in standard dose Has added vasolilating effect Has neutral effect on lipids B-blocker B-blockers are commonly used as first line therapy for HT especially for young (rather than elderly), white (rather than black) patients or as alternative for diuretics. B-blockers are suitable antiht drugs for patients with increase adrenergic drive and those with renin value. Conditions that discourage use of B-blockers Severe COLD Chronic sever congestive HF Severe occlusive PVDs These are commonly found in elderly and diabetic patients
5 ά blockers: Prazocin Terazocin Doxazocin Selective ά -blockers are competitive blockers of ά 1-adrenoceptors and they have direct vasodilating effect (due to PDE inhibition). They decrease PVR and so Bp by dilating both arterioles and venules so they reduce preload and after load (balanced vasodilators). They are free from metabolic side effects. They have no or lesser place in initial monotherapy for HT. These drugs are usually combined with B-blocker (to prevent reflex tachycardia) and diuretics (to counter salt and water retention). Mild-moderate HT especially those patients with metabolic syndrome and those with BPH PVDs Refractory HF. Side Effects Reflex tachycardia First-dose phenomena: brisk sever hypotension after the first or second dose of the drug usually 2 hours after administration. To avoid this phenomenon, we give the dose at bed time or start with small dose and increase it gradually. Orthostatic hypotension Nasal and conjunctival congestion Failure of (or retrograde) ejaculation Mixed ά and β-blockers Labetalol: Hypertensive emergency and first line therapy for HT in black patients Carvidolol: Mild-Moderate HF and first line therapy for HT in black patients Drugs acting on RAAS 1. Angiotensin Converting Enzyme Inhibitors (ACEIs) 2. Angiotensin Receptor Blockers (ARBs) 3. Renin Inhibitors

6 ACE Inhibitors ARBs Renin Inhibitor Captopril Losartan Aliskiren Enanlapril Irbesartan Lisinopril Candesartan Ramipril Valsartan Perindopril Telmisartan Quinapril Olmesartan Angiotensin Converting Enzyme Inhibitor, ACEIs Captopril Lisinopril Enlapril Fosinopril Zofinopril

7 ACEIs: Mechanism of Action
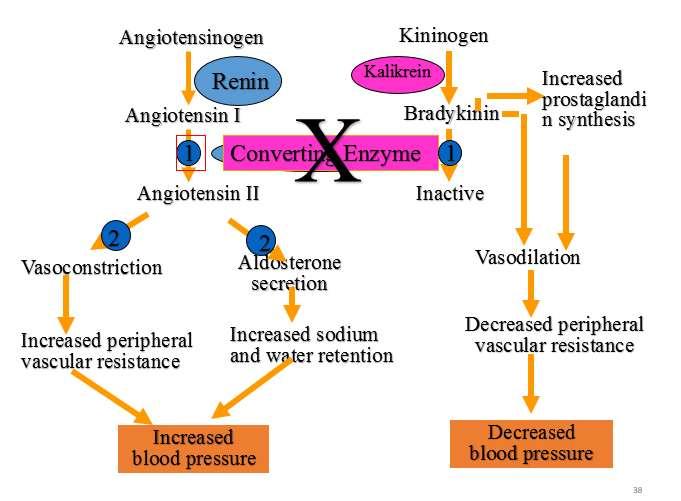
8 ACEIs: Mechanism of Action Renin is produced by the kidney in response to renal ischemia, hypoxemia and B2-adrenergic stimulation. Renin converts angiotensinogen (circulating protein) into Angiotensin-I (Ang I) which is inert substance. Later, Ang-I is converted into Ang-II by the action of ACI (and by Chymases). Ang-II is a potent vasoconsitrictor cuasing increase in PVR and stimulate aldosteron release (Na and H2O retention). Further Ang-II caues progressive vascular growth and end-organ damage. Action of Ang-II is mediated through specific receptors called Ang receptors (AT1 and AT2). AT1 (vasoconstriction, aldosterone release and vascular growth) AT2 (antigrowth so has favorable effects) ACEIs block the conversion of Ang-I to Ang-II. Further they lead to accumulation of Bradykinin (vasodilator) which is also substrate for ACE. Decreased formation of Ang-II (vasodilatation and decrease aldosterone release) and accumulation of Bradykinin (vasodilatation) results in reduction in BP Angiotensin II is one of the most potent vasoconstrictors known to man Angiotensin II releases aldosterone from the adrenal cortex Aldosterone enhances sodium and water retention and potassium loss from the kidney Blood volume and BP increase as a result Renin release from the juxtaglomerular cell Sympathetic nerve stimulation beta-1 receptor Low blood sodium Low renal artery pressure Renin acts upon angiotensinogen to form angiotensin I Angiotensin I is converted to Angiotensin II by a converting enzyme called ACE Angiotensin II constricts the renal efferent arteriole more than the afferent arteriole It therefore increases or maintains high glomerular filtration pressure As mentioned previously, AT-II causes high levels of aldosterone, and therefore leads to water and salt conservation Blocking the Renin-Angiotensin System BP decreases MAINLY by lowered TPVR Cardiac output is usually NOT significantly affected For some reason, reflex sympathetic stimulation DOES NOT OCCUR Absence of cardiostimulation makes these drugs safe in patients with ischemia ACEIs: Uses Hypertension: as monotherapy or in combination therapy. Heart failure MI: post MI phase, they prevent vascular and cardiac remodelling. Asymptomatic LV dysfunction, they prevent development of overt CHF. Nephroprotection: prevent protein urea in diabetic and non-diabetic nephropathy. Side Effects Hypertension: as monotherapy or in combination therapy. Heart failure MI: post MI phase, they prevent vascular and cardiac remodelling. Asymptomatic LV dysfunction, they prevent development of overt CHF. Nephroprotection: prevent protein urea in diabetic and non-diabetic nephropathy.
9 Calcium Channel Blockers (CCBs) 1. Dihydropyridines (DHP) 2. Non-DHP Dihydropyridines (DHP) Nifedipine Nimodipine Amlodipine Felodipine Isradipine Non-DHP Diliazem Verapamil CCBs: Mechanism of Action CCBs block the inward movement of the Ca by binding and blocking the L-type voltage gated Ca channels in the heart and smooth muscles (of peripheral arterioles and coronary arteries) causing dilatation and relaxation mainly of the arterioles. All CCBs are therefore vasodilators decreasing arteriolar tone and systemic PVR resulting arterial BP (decrease after load). In addition CCBs decrease myocardial contractility (-ve inotropic) and the conduction in cardiac muscles (- chronotropic) Diliazem and verapamil: primary action on heart Dihydropyridines: primary action on arterioles Peripheral Effects: Nefidipine >Diliazem > verapamil Cardiac Effect: verapamil >Diliazem > Nefidipine CCBs: PKs They are orally active agents;verapamil and nicardipine are also given by IV route Most of them have short half lives High plasma protein binding and extensive metabolism All CCBs are save in pregnancy and renal failure CCBs: Uses 1. Hypertension and HT emergencies: CCBs are alternative first line antihypertensive agents and can be used safely in pregnancy, asthma, DM or renal impairment. Nifidipine (SL) and nicardipine (IV) are used in HT emergencies 2. Angina pectoris (stable, unstable and it s the drug of choice in variant type) 3. As antiarrythmeic especially verapamil; it is the second choice in treatment or termination of SVT 4. PVDs 5. Subarrchinoid hemorrhage (nimodipine causes cerebral vasodilatation 6. Al though CCBs are contraindicated in HF, amlodipine can be used in the treatment of HF 7. Migraine prophylaxis especially verapamil 8. Tocolytics
10 CCBs: Side effects Headache, flushing of the face and dizziness Edema (nifedipine) Constipation (verapamil) Gingival hyperplasia AV block & heart failure (verapamil and diltiazem) Drug interactions: beta blockers (verapamil and diltiazem), cimetidine Centrally Acting Drugs Methyldopa Clonidine Direct Vasodilators Hydralazine Minixidil Diazoxid Hypertensive emergencies Sodium Nitroprusside GTN Diazoxide Hydralazine Enalaprilat Nicardipine Esmolol Nifedipine Sublingual Fenoldopam
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI
 DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
HYPERTENSION: Sustained elevation of arterial blood pressure above normal o Systolic 140 mm Hg and/or o Diastolic 90 mm Hg
 Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
sympatholytics sympatholytics sympatholytics
 sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
Beta 1 Beta blockers A - Propranolol,
 Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Introduction. Factors affecting blood pressure: 1-COP = HR X SV mainly affect SBP. 2-TPR = diameter of arterioles X viscosity of blood affect DBP
 Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
Antihypertensives. Diagnostic category
 Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Categories of HTN. Overview of Hypertension. Types of Hypertension
 Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
TREATMENT OF HYPERTENSION
 TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
ANTIHYPERTENSIVES. Assoc. Prof. Bilgen Başgut
 ANTIHYPERTENSIVES Assoc. Prof. Bilgen Başgut Hypertension Hypertension is a condition in which the blood pressure is persistently higher than normal Hypertension > 140 mmhg > 90 mmhg Systolic Blood Pressure
ANTIHYPERTENSIVES Assoc. Prof. Bilgen Başgut Hypertension Hypertension is a condition in which the blood pressure is persistently higher than normal Hypertension > 140 mmhg > 90 mmhg Systolic Blood Pressure
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Antihypertensive Agents
 Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Antihypertensive Drugs. Nafrialdi
 Antihypertensive Drugs Nafrialdi 1 Mechanisms of Blood Pressure Regulation Blood Presure Cardiac Output Peripheral Resistance Heart Rate Stroke volume Vascular tone Vessel elasticity Myocardial contractility
Antihypertensive Drugs Nafrialdi 1 Mechanisms of Blood Pressure Regulation Blood Presure Cardiac Output Peripheral Resistance Heart Rate Stroke volume Vascular tone Vessel elasticity Myocardial contractility
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias
 1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood:
 Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
ANTIHYPERTENSIVE AGENTS AND VASODILATORS. Lecture 5
 ANTIHYPERTENSIVE AGENTS AND VASODILATORS Lecture 5 Hypertension Blood pressure BP = CO x PVR n Interaction between autonomic nervous system, cardiovascular system and renal system Normal: 110/70 Prehypertension
ANTIHYPERTENSIVE AGENTS AND VASODILATORS Lecture 5 Hypertension Blood pressure BP = CO x PVR n Interaction between autonomic nervous system, cardiovascular system and renal system Normal: 110/70 Prehypertension
Hypertension. Penny Mosley MRPharmS
 Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Chapter (9) Calcium Antagonists
 Calcium Antagonists") Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS)
") DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
Cardiovascular drugs
 chapter 13 Cardiovascular drugs Cardiovascular drugs act on the heart or blood vessels to control the cardiovascular system. They are used to treat a variety of conditions from hypertension to chronic
chapter 13 Cardiovascular drugs Cardiovascular drugs act on the heart or blood vessels to control the cardiovascular system. They are used to treat a variety of conditions from hypertension to chronic
New classification of HT Systolic Diastolic Normal <120 <80 Prehypertension Stage1HT Stage 2 HT >160 or >100
 Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
Antihypertensive Agents
 Antihypertensive Agents Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 13.11.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Süzer Farmakoloji 3. Baskı 2005
Antihypertensive Agents Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 13.11.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Süzer Farmakoloji 3. Baskı 2005
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Treatment of Essential Hypertension
 2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
Hypertension Management - Summary
 Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Prof. Ramzy H. El Mawardy. Cairo Egypt 2009
 Prof. Ramzy H. El Mawardy Ain Shams University Cairo Egypt 2009 Burden of HRN is increasing worldwide = 7 billion individuals. BP control is still poor = 60.70%. Global risk assessment is essential in
Prof. Ramzy H. El Mawardy Ain Shams University Cairo Egypt 2009 Burden of HRN is increasing worldwide = 7 billion individuals. BP control is still poor = 60.70%. Global risk assessment is essential in
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Circulation. Blood Pressure and Antihypertensive Medications. Venous Return. Arterial flow. Regulation of Cardiac Output.
 Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Antihypertensive Drugs. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014
 Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Antihypertensive Drugs What is Hypertension: A common, incurable, persistent, but usually
Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Antihypertensive Drugs What is Hypertension: A common, incurable, persistent, but usually
Treatment of T Angina reatment of By Ali Alalawi
 Treatment of Angina By Ali Alalawi Determinants of Oxygen Demand Need to improve ratio of: Coronary blood flow / cardiac work Or Cardiac O2 Supply / Cardiac Requirement Coronary Circulation vs Other Circulation
Treatment of Angina By Ali Alalawi Determinants of Oxygen Demand Need to improve ratio of: Coronary blood flow / cardiac work Or Cardiac O2 Supply / Cardiac Requirement Coronary Circulation vs Other Circulation
COMPLEX HYPERTENSION. Anita Ralstin, FNP-BC Next Step Health Consultant, LLC
 COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
Low Efficacy Diuretics. Potassium sparing diuretics. Carbonic anhydrase inhibitors. Osmotic diuretics. Miscellaneous
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
What in the World is Functional Medicine?
 What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
Hypertension Management Focus on new RAAS blocker. Disclosure
 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Angina Pectoris. Edward JN Ishac, Ph.D. Smith Building, Room
 Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth University
Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth University
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Treatment of Essential Hypertension
 2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
ANTI- HYPERTENSIVE AGENTS
 CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Antihypertensive Drugs. Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan October, 2017
 Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan October, 2017 Antihypertensive Drugs What is Hypertension? A common, incurable, persistent, but usually
Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan October, 2017 Antihypertensive Drugs What is Hypertension? A common, incurable, persistent, but usually
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
HTN of pregnancy is serious and must be controlled, because without monitoring it can develop into pre-eclampsia and finally to eclampsia.
 Sheet Pharmacology #7 1 Antihypertensive drugs of pregnancy: ببسسممم الله االرححممننن االرححيممم Usage of normal drugs of chronic HTN is controversial in pregnancy, because after few weeks or second trimester,
Sheet Pharmacology #7 1 Antihypertensive drugs of pregnancy: ببسسممم الله االرححممننن االرححيممم Usage of normal drugs of chronic HTN is controversial in pregnancy, because after few weeks or second trimester,
Pharmacologic Management of Hypertension
 Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Chapter 10 Worksheet Blood Pressure and Antithrombotic Agents
 Complete the following. 1. A layer of cells lines each vessel in the vascular system. This layer is a passive barrier that keeps cells and proteins from going into tissues; it also contains substances
Complete the following. 1. A layer of cells lines each vessel in the vascular system. This layer is a passive barrier that keeps cells and proteins from going into tissues; it also contains substances
Pharmacotherapy of Angina Pectoris
 Pharmacotherapy of Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth
Pharmacotherapy of Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Pharmacotherapy of Angina Pectoris
 Pharmacotherapy of Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth
Pharmacotherapy of Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide
 Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
 Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION
 VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
Factors Involved in Poor Control of Risk Factors
 Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Objectives. Upon completion of the learning activity the participant will be able to: Hypertension: The Latest Treatment Options
 Objectives Hypertension: The Latest Treatment Options Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC President, Fitzgerald Health Education Associates, Inc. North Andover, MA Family Nurse
Objectives Hypertension: The Latest Treatment Options Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC President, Fitzgerald Health Education Associates, Inc. North Andover, MA Family Nurse
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to
 Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
INDIAN HYPERTENSION GUIDELINES-II
 HYPERTENSION IN SPECIAL SITUATIONS Hypertension with diabetes mellitus Co-existence of hypertension and diabetes is being increasingly recognised. 30-35% of hypertensives are detected to have diabetes.
HYPERTENSION IN SPECIAL SITUATIONS Hypertension with diabetes mellitus Co-existence of hypertension and diabetes is being increasingly recognised. 30-35% of hypertensives are detected to have diabetes.
Heart failure. Failure? blood supply insufficient for body needs. CHF = congestive heart failure. increased blood volume, interstitial fluid
 Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Hypertension is also an important risk factor in the development of chronic kidney disease and heart failure.
 Hypertension Hypertension Hypertension is defined as either a sustained systolic blood pressure of greater than 140 mm Hg or a sustained diastolic blood pressure of greater than 90 mm Hg. Hypertension
Hypertension Hypertension Hypertension is defined as either a sustained systolic blood pressure of greater than 140 mm Hg or a sustained diastolic blood pressure of greater than 90 mm Hg. Hypertension
ASEBP and ARTA TARP Drugs and Reference Price by Categories
 ASEBP Pantoprazole Sodium 40 mg (generic) $0.2016 ASEBP Dexlansoprazole 30 mg Dexlansoprazole 60 mg Esomeprazole 10 mg Esomeprazole 20 mg Esomeprazole 40 mg Lansoprazole 15 mg Lansoprazole 30 mg Omeprazole
ASEBP Pantoprazole Sodium 40 mg (generic) $0.2016 ASEBP Dexlansoprazole 30 mg Dexlansoprazole 60 mg Esomeprazole 10 mg Esomeprazole 20 mg Esomeprazole 40 mg Lansoprazole 15 mg Lansoprazole 30 mg Omeprazole
SBP in range of 120 to 140 :no progression or regression of CAD. Sipahi et al., 2006
 Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Blood Pressure. Michelle Bertram- Nephrology- OBH
 Blood Pressure Michelle Bertram- Nephrology- OBH Hypertension- how common? 29-30% white adults 46-51% uncontrolled Diagnosis Two or more properly measured BP s after an initial screen NICE guidelines also
Blood Pressure Michelle Bertram- Nephrology- OBH Hypertension- how common? 29-30% white adults 46-51% uncontrolled Diagnosis Two or more properly measured BP s after an initial screen NICE guidelines also
THE RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM
 THE RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM The renin angiotensin system (RAS) or the renin angiotensin aldosterone system (RAAS) is a hormone system that is involved in the regulation of the plasma sodium
THE RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM The renin angiotensin system (RAS) or the renin angiotensin aldosterone system (RAAS) is a hormone system that is involved in the regulation of the plasma sodium
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Beta blockers in primary hypertension. Dr. Md. Billal Alam Associate Professor of Medicine DMC
 Beta blockers in primary hypertension Dr. Md. Billal Alam Associate Professor of Medicine DMC Development of antihypertensive drugs Beta blockers 1958 - The first beta-blocker, dichloroisoproterenol, was
Beta blockers in primary hypertension Dr. Md. Billal Alam Associate Professor of Medicine DMC Development of antihypertensive drugs Beta blockers 1958 - The first beta-blocker, dichloroisoproterenol, was
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
ANTI - ARRHYTHMIC DRUGS
 ANTI - ARRHYTHMIC DRUGS CARDIAC ACTION POTENTIAL K Out Balance Ca in/k out Na in K Out GENERATION OF ARRHYTHMIAS Four mechanisms of arrhythmia generation; Increased normal automaticity Abnormal automaticity
ANTI - ARRHYTHMIC DRUGS CARDIAC ACTION POTENTIAL K Out Balance Ca in/k out Na in K Out GENERATION OF ARRHYTHMIAS Four mechanisms of arrhythmia generation; Increased normal automaticity Abnormal automaticity
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Blood pressure (BP) control. Hypertension
 control. Hypertension") Blood pressure (BP) control Normal heart function Blood pressure (BP) control blood pressure (BP) cardiac output (CO) = total peripheral resistance (TPR) heart rate (HR) filling pressure arteriolar volume
Blood pressure (BP) control Normal heart function Blood pressure (BP) control blood pressure (BP) cardiac output (CO) = total peripheral resistance (TPR) heart rate (HR) filling pressure arteriolar volume
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Antihypertensive Agents
 1. Blood Pressure Regulation Antihypertensive Agents - 2007 Edward JN Ishac. Ph.D. Associate Professor, Dept. Pharmacology & Toxicology Office: Smith 742; Tel: 828 2127 eishac@hsc.vcu.edu Frank's formula,
1. Blood Pressure Regulation Antihypertensive Agents - 2007 Edward JN Ishac. Ph.D. Associate Professor, Dept. Pharmacology & Toxicology Office: Smith 742; Tel: 828 2127 eishac@hsc.vcu.edu Frank's formula,