Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
|
|
|
- Roderick Lamb
- 5 years ago
- Views:
Transcription
1 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard Medical School Boston, MA
2 Barrett s Esophagus: Metaplasia and Dysplasia Metaplasia - Def n/types - Pathogenesis - Differential Diagnosis Dysplasia - Incidence/risk factors - Pathologic features - Adjunctive Diagnostic tests - Natural History - Treatment
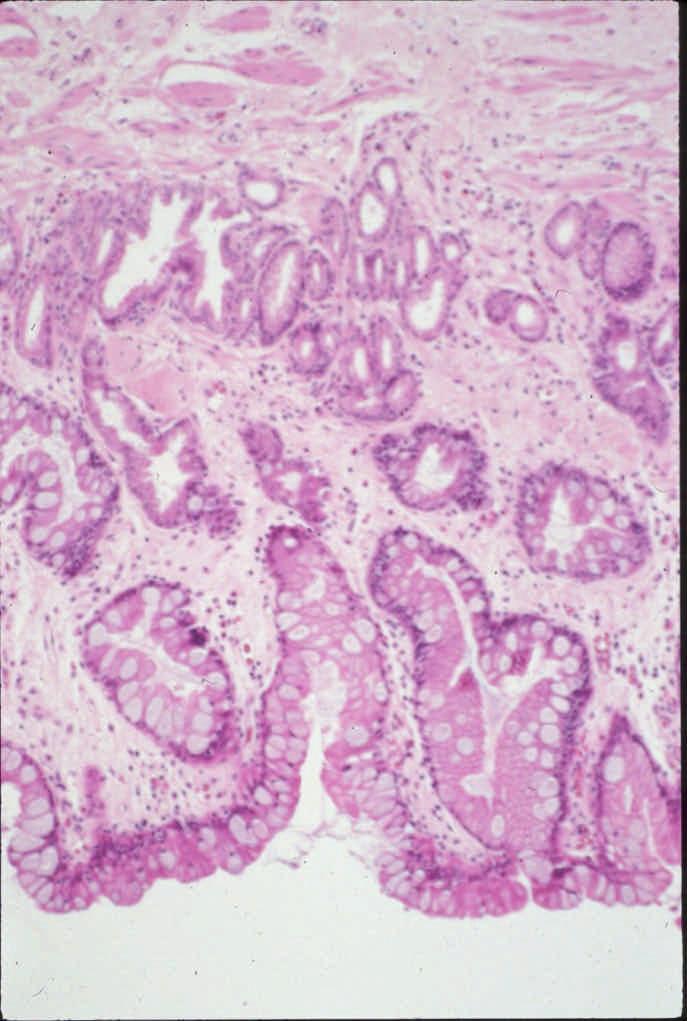
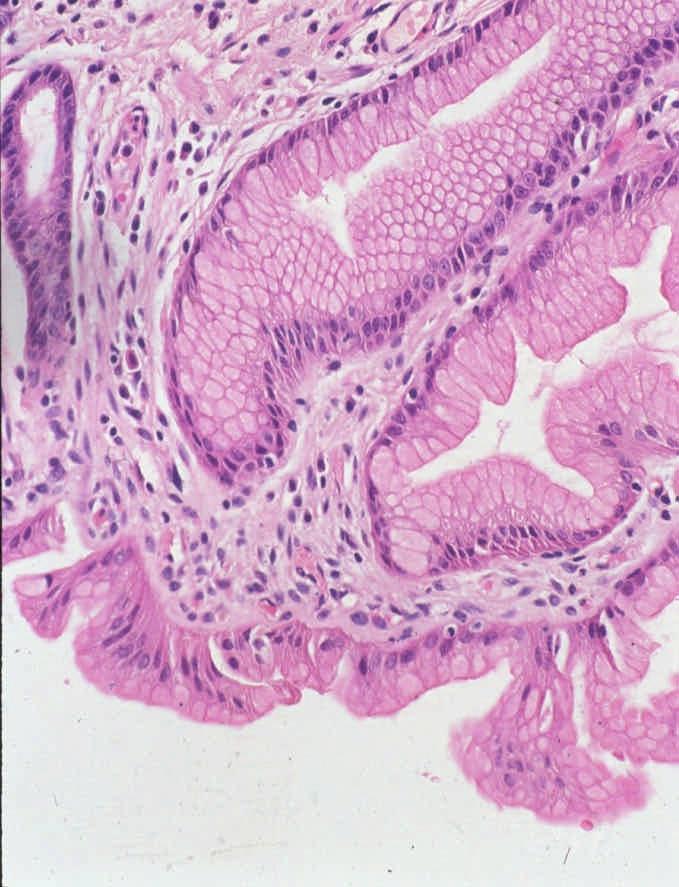
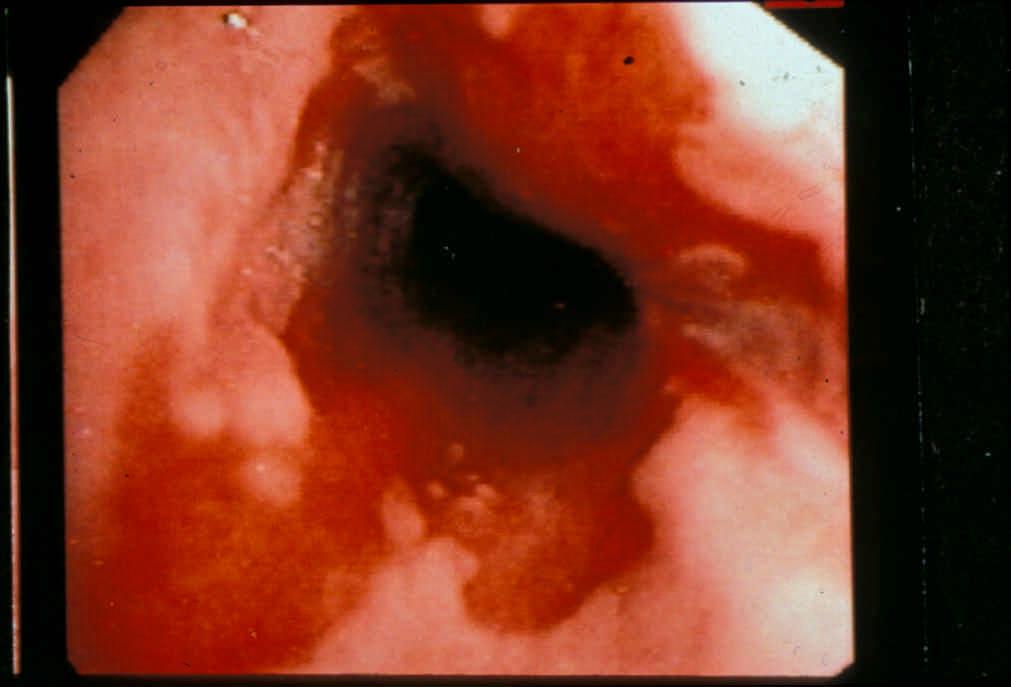
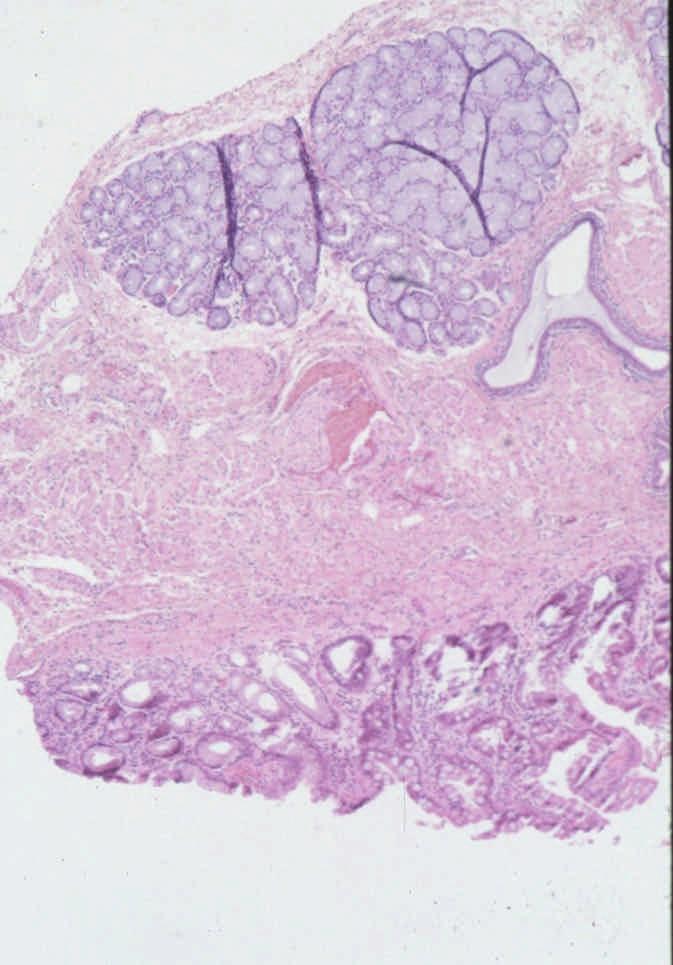
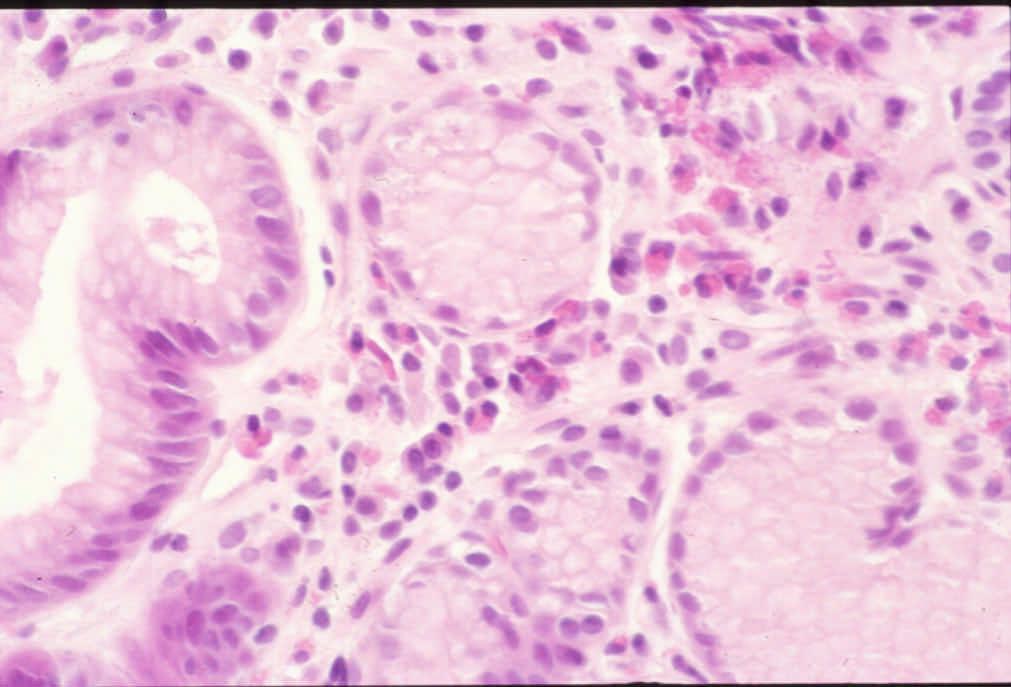
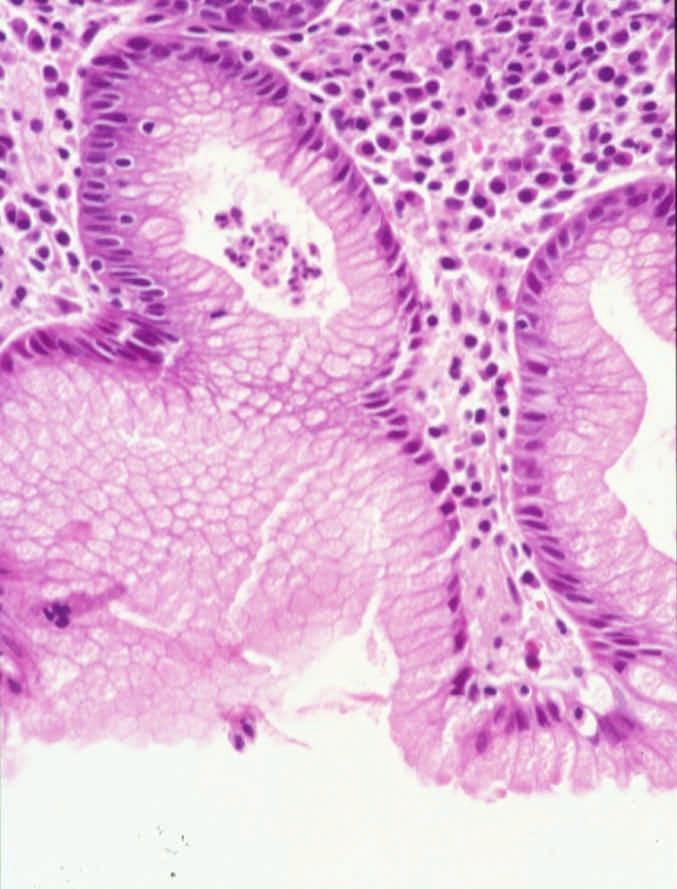
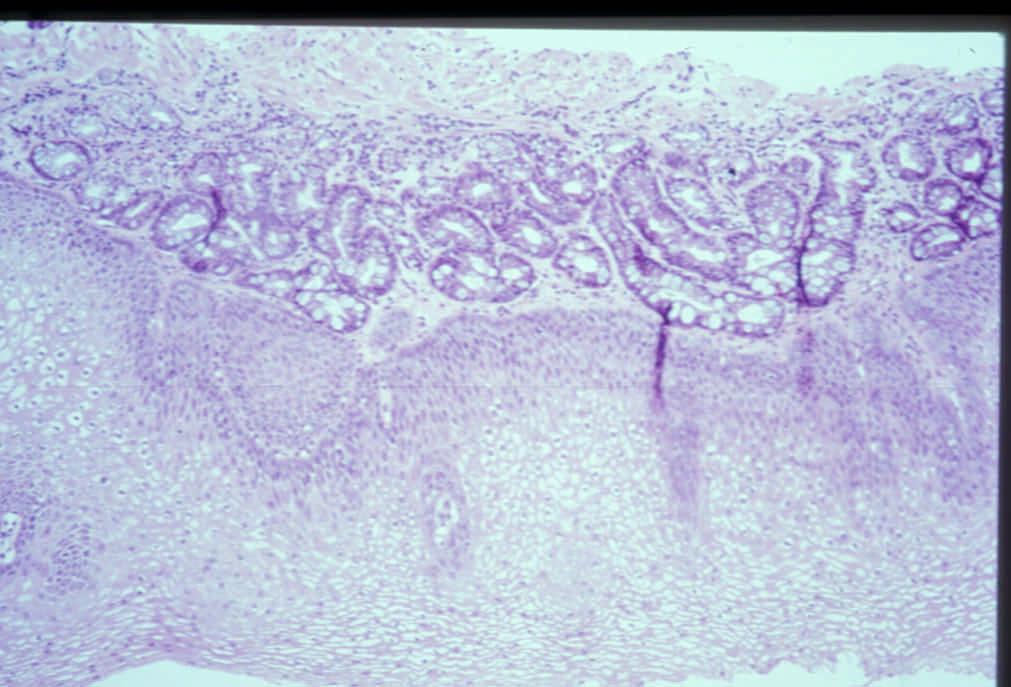
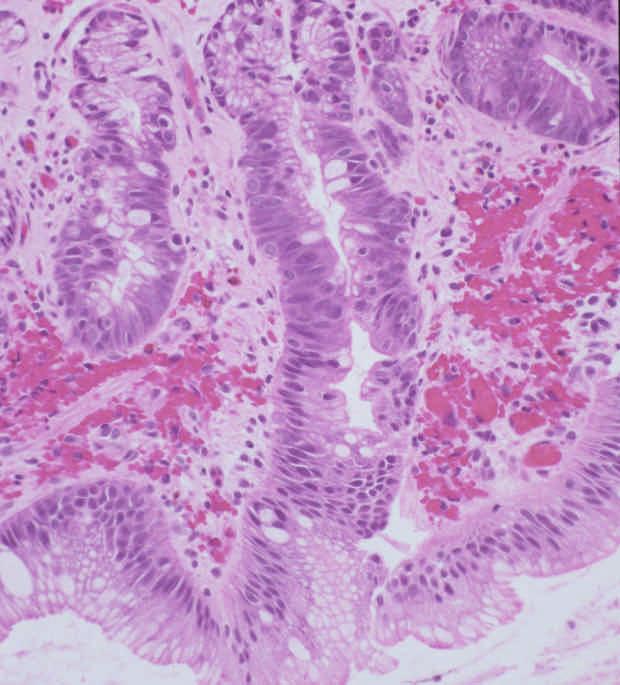
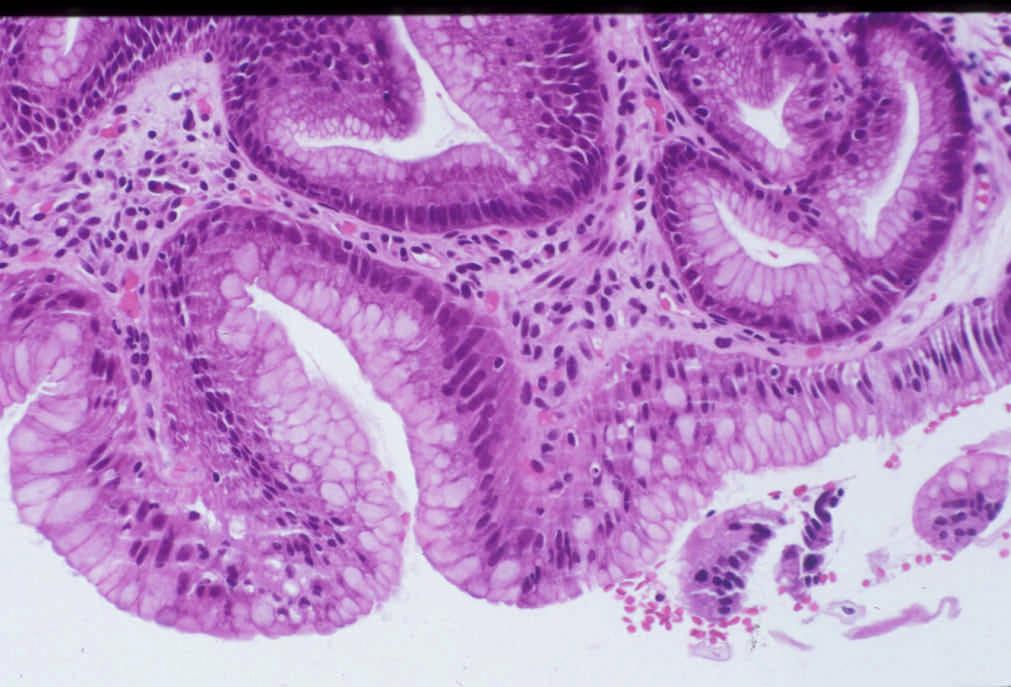
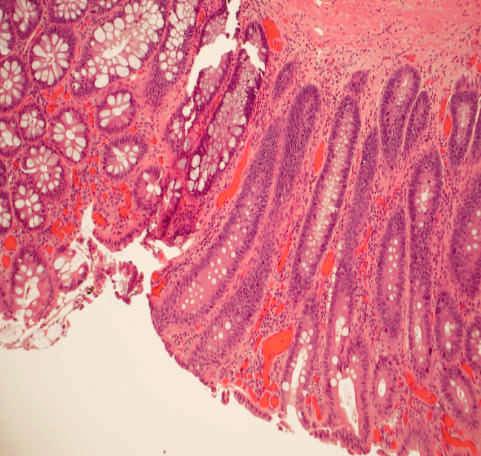
3 Barrett s Esophagus Definition Columnar metaplasia of esophageal squamous epithelium (any length) Recognized at endoscopy Goblet cell metaplasia
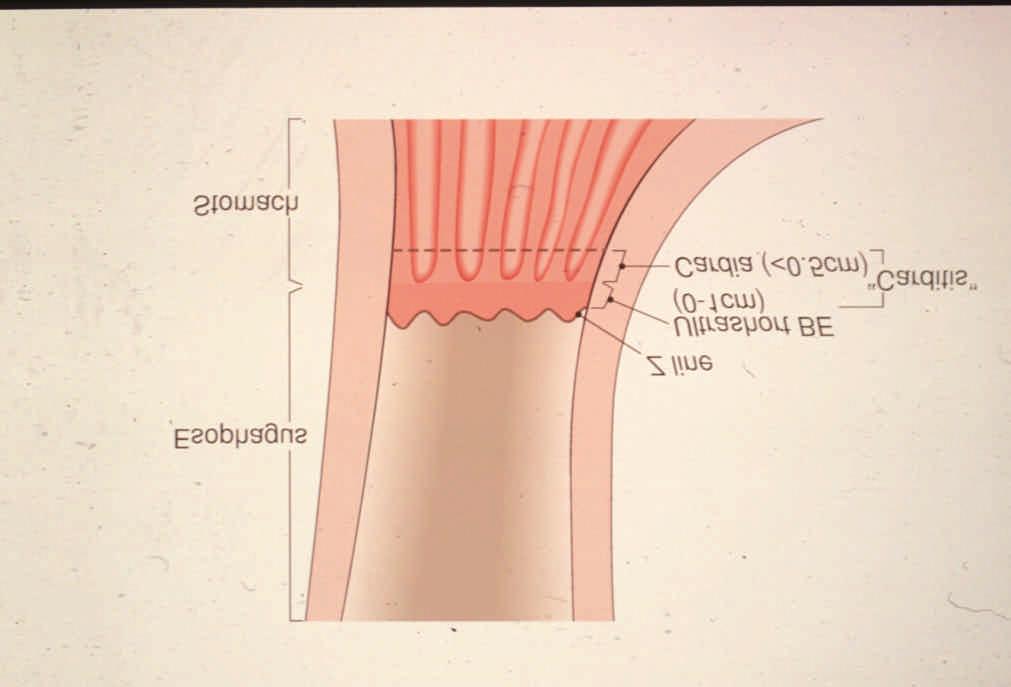
4 Barrett s Esophagus Gross Types Long segment (>3cm) Short segment (1-3cm) Ultrashort segment (0-1cm)
5 Barrett s Esophagus Epithelial Types Intestinal ( specialized ) type (99%>2cm) Cardia type ( junctional ) Fundic type
6
7
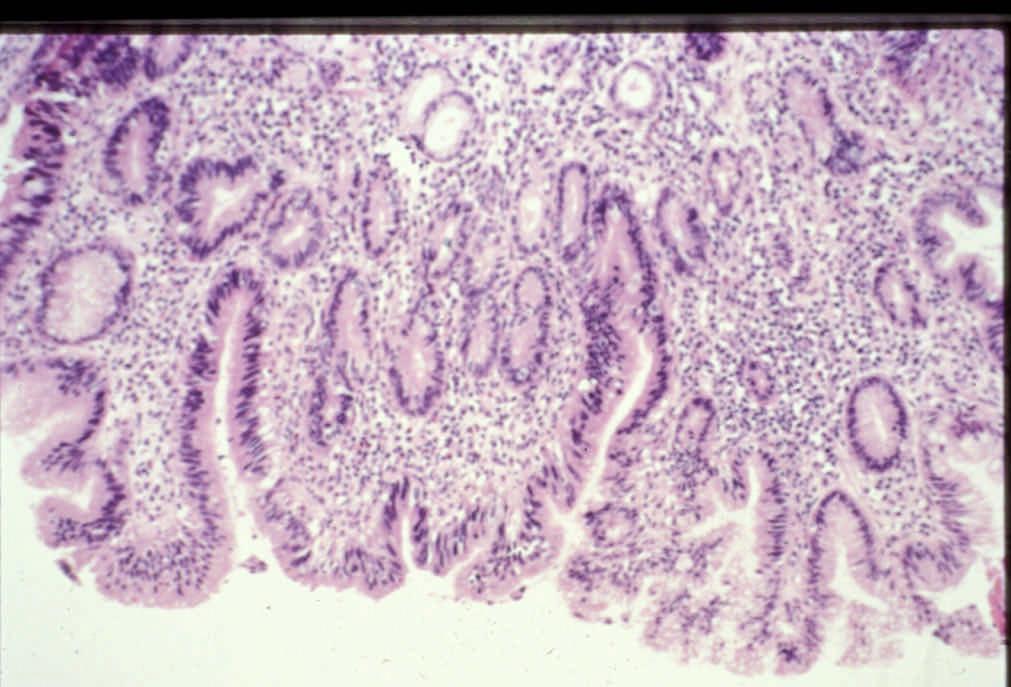
8 Short (Ultrashort ) BE vs. Chronic Carditis Distinction important Different clinical, etiologic, pathologic, outcome, risk of malignancy
9 Summary of Factors That Impede the Ability to Separate the True Gastric Cardia from the Distal Esophagus at Endoscopy Hiatal Hernia (which causes obliteration of the proximal gastric folds) Irregular Z line Erosions in Distal Esophagus (which mimicks BE) Respiratory Movements Sampling Error Similar Histology
10
11
12
13
14
15
16 Table 1. Frequency of significant morphologic parameters in biopsies from patients with BE or CIM Disease Squamous Crypt Crypt Incomplete Diffuse IM HG MEP EG/ED Category over IM Disarray Atrophy IM (>50%) BE 8/14 17/20 12/20 20/20 12/20 8/20 14/20 6/20 (%) CIM 0/7 10/20 5/20 10/20 2/20 0/20 3/20 0/20 (%) P value < BE: Barrett s esophagus; CIM: carditis with intestinal metaplasia; IM: intestinal metaplasia; MEP: Multilayered epithelium; HG: Hybrid glands; EG/ED: esophageal glands/ducts
17 Mucin Histochemistry Stain Esoph Cardia Goblet Non-Goblet Goblet Non-Goblet Alcian blue (acid mucin High Iron diamine (sulphomucin)
18
19
20
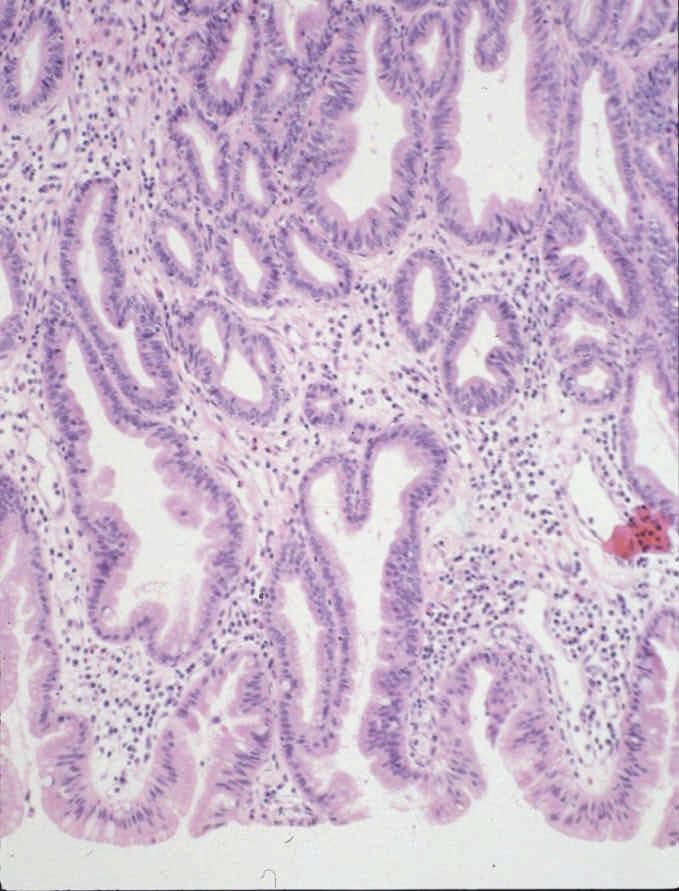
21 Multilayered Epithelium 1. Hybrid epithelium (squam/colum) - EM, cytokeratins 2. Biologically active 3. Phenotypically similar to Barrett s Esophagus 4. Highly associated with Barrett s esophagus and GERD
22
23
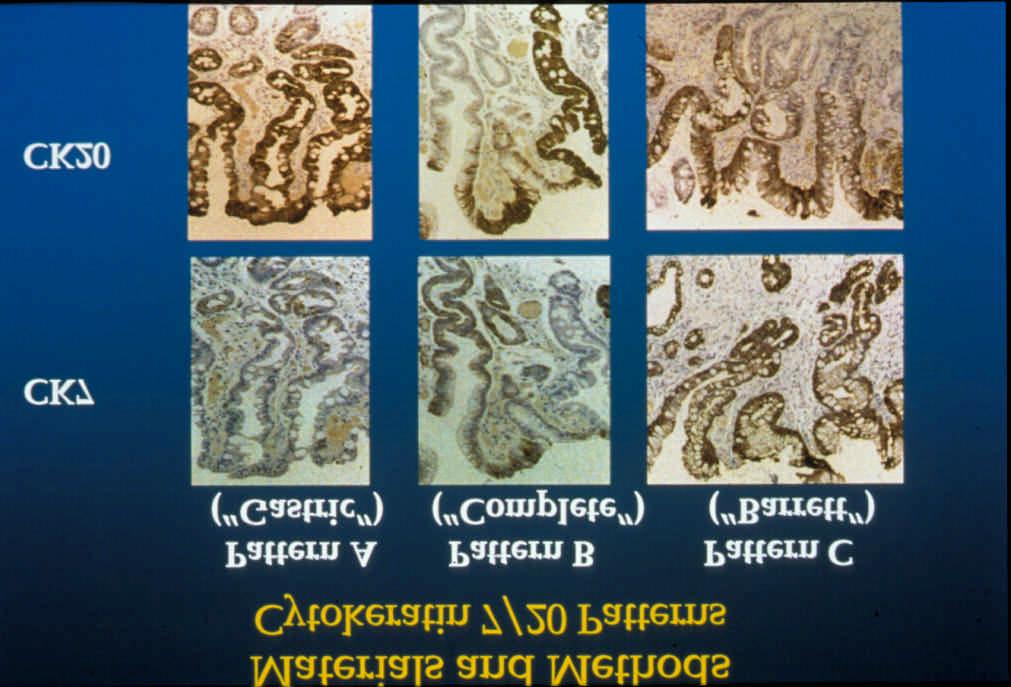
24 Esophageal versus Cardia Intestinal Metaplasia Feature Esophagus IM Cardia IM (BE) 1. GERD clinical profile Irregular Z line Esophagitis (histologic) Gastritis (histologic) H. Pylori Eosinophils Neut, Plasma, Lymphocytes Multilayered epithelium HID stain positive MUC 1, 6 positive BE CK 7/20 pattern + +/- 12. Complete > incomplete IM - +
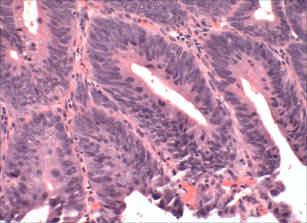
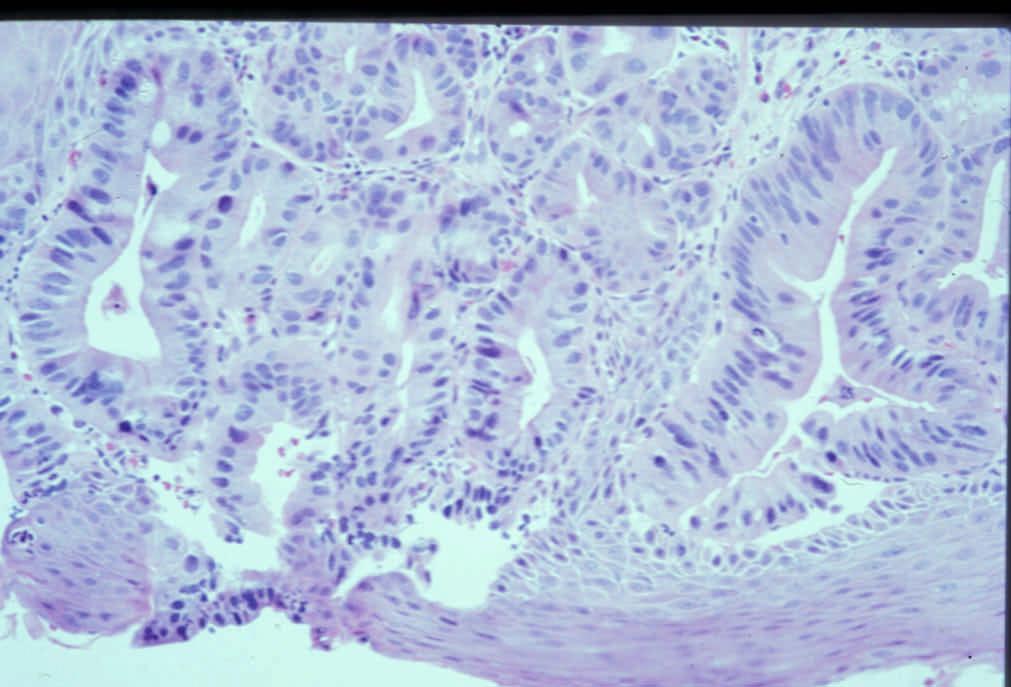
25 Barrett s Esophagus Dysplasia: Definition Neoplastic epithelium that remains confined within the basement membrane not reactive not synonymous with atypical unlikely to spontaneously regress Both a marker and a precursor of adenocarcinoma
26 Barrett s Dysplasia/Carcinoma Risk Prevalence : 6-8% Incidence : 0.2 3% (1/52 1/208 patient years) Relative Risk: x
27 Incidence Rate of Adenocarcinoma in Barrett s Esophagus Incidence Follow-up Series Patients Cases (Patient Incidence (No.) (No) Years) Rate Haammeeteman et al /52 Bonelli et al /55 Roberston et al /56 Miros et al /96 Iftikhar et al /115 Drewitz et al /208 O Connor et al /285 Sepchler et al /259 Sharma et al /212
28 Barrett s Dysplasia/Carcinoma Risk Factors Length of BE Severity of Reflux Hiatus Hernia size Gender Ethnicity Age Smoking? Alcohol?
29 Patient Characteristics Variable GERD Barrett s HGD/CA (N=2170) (N=1189) (N=131) Male sex 98% 99% 99% Age (yr*) White ethnicity 76% 83% 89% Ethanol Consumption 40% 37% 42% Smoking 34% 25% 27% Hiatal hernia 24% 65% 84% Hiatal hernia size (cm*) Barrett s length (cm*) Avidan et al. Am J Gastroenterol2002;97(8)
30 Dysplasia Pathologic Features 1. Gross - Flat - Elevated (plaque, nodule, polyp) 2. Microscopic - Adenoma-like - Non-adenoma like
31 Dysplasia in the GI Tract Negative Indefinite Positive (low, high) Intramucosal AdenoCa Submucosal (Invasive) AdenoCa
32 Vienna System and Dysplasia Morphology Study Group Classification of Dysplasia in IBD Vienna DMSG 1. Negative for neoplasia/dysplasia Negative for dysplasia 2. Indefinite for neoplasia/dysplasia Indefinite for dysplasia 3. Non-invasive low-grade neoplasia Low-grade dysplasia (low-grade adenoma/dysplasia) 4. Non-invasive high-grade neoplasia High-grade dysplasia 4.1 High-grade adenoma/dysplasia 4.2 Non-invasive carcinoma (carcinoma in situ) 4.3 Suspicious of invasive carcinoma 5. Invasive Neoplasia Adenocarcinoma* 5.1 Intramucosal Adenocarcinoma Intramucosal 5.2 Submucosal carcinoma or beyond Invasive *not described by DMSG
33 Non-Recommended Terms Atypia Adenomatous Changes Carcinoma in Situ
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54 Crypt Dysplasia with surface maturation. A clinical, pathologic and molecular study of a Barrett s Cohort L. Lomo, P. Blount, R. Sanchez, P. Galipeau, D. Cowan, D. Ayub, P. Rabinovitch, B. Reid, R. Odze Am J Surg Pathol (In Press)
55 Pathologic Features of the Study Cohort (N=206) Feature BCDA Controls (N=15) (N=191) p value Maximum diagnosis Associated neoplasia (total) 13/15 (87%) 112/191 (59%) Low-grade dysplasia 2/15 (13%) 70/191 (37%) 0.09 High-grade dysplasia 8/15 (53%) 35/191 (18%) Adenocarcinoma 3/15 (20%) 7/191 (4%) 0.03
56 Summary of Molecular Biomarkers of the Study Cohort Feature BCDA Controls (N=15) (N=191) p value > 1 Molecular abnormality 12/15 (80%) 100/191 (52%) p LOH 8/9 (89%) 67/116 (58%) p LOH 4/9 (44%) 12/116 (10%) 0.016?4N 2/15 (13%) 11/191 (5.8%) 0.24 Aneuploidy 5/15 (33%) 12/191 (6.3%) Any flow abnormality 6/15 (40%) 15/191 (7.9%) 0.001
57
58
59
60
61
62
63
64 Barrett s Esophagus Feature Regeneration Dysplasia Inflammation ++ +/- Ulceration ++ +/- Surface Maturation + - Pleomorphism - +/- Loss of Polarity - +/- Atypical Mitoses - +/- Surface Proliferation +/- ++ Villiform Change +- +/- Mucin Depletion +/- ++
65 Barrett s-related Dysplasia Interobserver Agreement Category % agreement HGD + IMC vs. others 85-87% Negative vs. others 71-72% Negative + Ind vs. others 75-77% Neg vs. Ind/LGD vs. HGD/IMC 58-61% Reid BJ et al. Hum Pathol 1988
66 Barrett s-related Dysplasia Interobserver Variation Category Set 1 Set 2 No dysplasia 0.44 (mod) 0.58 Indefinite 0.13 (slight) 0.15 Low grade 0/23 (fair) 0.31 High grade/cancer 0.63 (substantial) 0.64 Montgomery EA et al. Hum Pathol 2001
67 Adjunctive Techniques Proliferation Markers DNA content (aneuploidy) Telomerase Genetic mutations (p53, p16, Kras, APC, B catenin) Growth Factors Apoptosis Inhibitors Cyclooxygenase 2

68 p53 in Negative/ Indefinite Mucosa
69 AMACR Immunostaining is Useful in Detecting Dysplastic Epithelium in BE, UC and CD R Dorer, J Glickman, RD Odze Am J Surg Pathol (In Press)
70 Dorer et al Results AMACR Positive Dysplasia BE UC/CD Negative 0% 0% Indefinite 21% 14% Low Grade 38% 96% High Grade 81% 80% AdenoCa 72% 71%



, with")
, and")
71 A B C Figure 2. AMACR expression in colitis without dysplasia (A), with high-grade dysplasia (B), and invasive adenocarcinoma (C).
72 Natural History Dysplasia (%) n Cancer (%) None (2) Low grade 72 5 (7) High grade (22) Sampliner. Am J Gastroenterol 2002:97(8);
73 Esophagectomy for High-Grade Dysplasia Series Unsuspected Carcinoma Edwards (1996) 8/11 (73%) Heimiller (1996) 13/30 (43%) Cameron (1997) 2/19 (10.5%) Ferguson (1997) 8/15 (53%) Falk (1997) 4/12 (33%) Total 35/87 (40%)
74 Natural History of High-Grade Dysplasia Prospective Studies Proportion with Cancer Seattle (Baseline HGD) N=76 Kansas VA, N=15 Seattle (Incident HGD) N=27 Hines VA, N=75 (Excluded 4 cancers in 1 st year) Years Schnell et al, Gastroenterol 2001; 120: Reid et al, Am J Gastroenterol 2000; 95: Weston et al, Am J Gastroenterol 2000; 95:
75 Low-Grade Dysplasia Prospective Studies Study No. LGD Progress to Cancer (%) Regression (%) Weston et al (2%) 31 (65%) Schnell et al (3%) ND Sharma et al. Conio et al (3%) 1 (6%) 103 (66%) 12 (75%) Weston et al, Am J. Gastroenterol 2001; 96: Schnell et al, Gastroenterology 2001; 120: Sharma et al, Gastroenterology 2002; 122:A20 Conio et al, Am J Gastroenterol 2003;
76 Management Controversial Varies between institutions Dependent on surveillance techniques
77 ACG guidelines for Surveillance in Barrett s esophagus: (Sampliner et al, Am J Gastroenterol 97:1888,2002) Chronic GERD Symptoms Screening Endoscopy with Biopsies Negative for dysplasia Low grade dysplasia High-grade dysplasia x2 endoscopies Repeat endoscopy with biopsy Expert pathologist opinion 3 year surveillance Repeat x 1 Focal Mucosal Multifocal Annual surveillance irregularity Until no dysplasia 3 months Intervention surveillance EMR (surgical)
78 The Case for Barrett s Surveillance 5-year Survival of Surveyed and Non-surveyed Cases 100% 90% 90.0% 80% 73.3% 70% 5-year Survival 60% 50% 40% 30% 20% 52.9% 20.0% 20.0% Surveyed cases Non-surveyed cases 10% 0% 0.0% Corley Streitz Peters Corley et al, Gastroenterology 2002; 122:633 Streitz et al, J Thorac Cardiovasc Surg 1993; 105:383 Peters et al, J Thorac Cardiovasc Surg 1994; 108:813
79 Ideal Biopsy Protocol Jumbo forceps 4 quadrant Q2 cm in BE 4 quadrant Q1 cm in dysplasia All nodules/polyps/masses Confirm with experienced GI pathologist
80 Management Considerations Surveillance vs. Esophagectomy Extent of HGD Extent of LGD Nodularity Patient age Comorbidities Length of BE
81 Extent of dysplasia in BE Buttar et al, Gastro 2001;120: # 1 year 3 year RR Patients survival survival Carcinoma Cancer Focal HGD 33 93% 86% 12% - Diffuse HGD* 67 62% 66% 42% 5.36 Nodularity % 3.98 Lack of acid suppression % 2.48 Focal <5 crypts, diffuse >5 crypts or >1 biopsy
82 Extent of Low Grade Dysplasia is a Significant Risk Factor for Cancer in Barrett s Esophagus Odze et al, Mod Pathol 2005;18(1):119
83 Table 3: Mean number of crypts/biopsy in each diagnostic category Maximum Diagnosis Non-Progressors Progressors Negative for dysplasia (range; SD) ( ; 9.51) ( ; 9.07) Indefinite for dysplasia (range; SD) ( ; ( ; 0.088) LGD (range; SD ( ; 4.98) ( ; 6.25) HGD (range; SD) ( ; 2.27) ( ; 2.4)
84 Flow Cytometry: Prospective Studies Patients without High-Grade Dysplasia Probability of Cancer Reid et al N=247 patients ½ biopsy every 2 cm Aneuploid and/or 4N 28% 0% p < Diploid, normal 4N Normal Cytometry (N=17) Teodori et al N=30 patients Abnormal Cytometry (N=13) 0% cancer 23% cancer p<0.01 for dysplasia or cancer (46% Reid et al, Am J Gastro 2000; 95:1669 Teodori et al, Cytometry 1998; 34:254
85 Ulcers in BE (Montgomery et al, Am J Gastro 2002;97(11):27-31) Ulcer-related Dysplasia # cases Ulcers CA on Grade (35/138) follow-up Neg 44 7% 0% Indef 22 9% 0% LGD 26 0% 0% HGD 33 33% 8/10 (80%)* CA 13 54% - *8/10 vs 12/23 p<.05
86 Barrett s Esophagus: New Surveillance Strategies Balloon cytology Fluorescence spectroscopy Chromoendoscopy Flow cytometry
87
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL
 THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
THE USE OF SPECIAL STAINS IN THE DIAGNOSIS OF BARRETT ESOPHAGUS AND BARRETT DYSPLASIA: RECOMMENDATIONS FROM THE RODGER C. HAGGITT GASTROINTESTINAL PATHOLOGY SOCIETY Amitabh Srivastava 1, Henry Appelman
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Relative risk of dysplasia for patients with intestinal metaplasia in the distal oesophagus and in the gastric cardia
 Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
The presence of intestinal-type goblet cells (ITGCs) in
 in") Goblet Cell Mimickers in Esophageal Biopsies Are Not Associated With an Increased Risk for Dysplasia Mamoun Younes, MD; Atilla Ertan, MD; Gulchin Ergun, MD; Ray Verm, MD; Margaret Bridges, MD; Karen Woods,
Goblet Cell Mimickers in Esophageal Biopsies Are Not Associated With an Increased Risk for Dysplasia Mamoun Younes, MD; Atilla Ertan, MD; Gulchin Ergun, MD; Ray Verm, MD; Margaret Bridges, MD; Karen Woods,
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Burning Issues in the Esophagus
 Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
Burning Issues in the Esophagus Elizabeth Montgomery, MD Johns Hopkins Medical Institutions Dr. Montgomery reports no relevant financial relationships with commercial interests. Squamous Epithelium Muscularis
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Diagnosis and grading of dysplasia in Barrett s oesophagus ... J Clin Pathol 2006;59: doi: /jcp
 1029 MY APPROACH Diagnosis and grading of dysplasia in Barrett s oesophagus R D Odze... This review focuses on the pathological features of dysplasia in Barrett s oesophagus. Two categorisation schemes
1029 MY APPROACH Diagnosis and grading of dysplasia in Barrett s oesophagus R D Odze... This review focuses on the pathological features of dysplasia in Barrett s oesophagus. Two categorisation schemes
Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful in characterizing esophageal location
 Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
Barrett s Esophagus Definition and Complications
 1 Barrett s Esophagus Definition and Complications Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Service Associate Professor of Pathology Brigham and Women s Hospital Harvard Medical School
1 Barrett s Esophagus Definition and Complications Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Service Associate Professor of Pathology Brigham and Women s Hospital Harvard Medical School
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018
 MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
The increasing incidence of esophageal adenocarcinoma
 GASTROENTEROLOGY 2004;127:310 330 A Critical Review of the Diagnosis and Management of Barrett s Esophagus: The AGA Chicago Workshop PRATEEK SHARMA,* KENNETH MCQUAID, JOHN DENT, M. BRIAN FENNERTY, RICHARD
GASTROENTEROLOGY 2004;127:310 330 A Critical Review of the Diagnosis and Management of Barrett s Esophagus: The AGA Chicago Workshop PRATEEK SHARMA,* KENNETH MCQUAID, JOHN DENT, M. BRIAN FENNERTY, RICHARD
Barrett s s Dysplasia
 Barrett s s Dysplasia Mary P. Bronner,, MD Director, GI Pathology Section Head, Molecular Pathology Cleveland Clinic Foundation Neoplastic Progression in Barrett s s Esophagus Chronic Reflux GERD Metaplasia
Barrett s s Dysplasia Mary P. Bronner,, MD Director, GI Pathology Section Head, Molecular Pathology Cleveland Clinic Foundation Neoplastic Progression in Barrett s s Esophagus Chronic Reflux GERD Metaplasia
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
One of the more common specimens encountered by
 Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
Controversies in the Diagnosis of Barrett Esophagus and Barrett-Related Dysplasia One Pathologist s Perspective John R. Goldblum, MD N Context. Pathologists frequently assess esophageal biopsy specimens
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, by Am. Coll. of Gastroenterology ISSN /02/$22.00
 THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 97, No. 1, 2002 2002 by Am. Coll. of Gastroenterology ISSN 0002-9270/02/$22.00 Published by Elsevier Science Inc. PII S0002-9270(01)03982-X ORIGINAL CONTRIBUTIONS
Barrett s Esophagus in Women: Demographic Features and Progression to High-Grade Dysplasia and Cancer
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1089 1094 Barrett s Esophagus in Women: Demographic Features and Progression to High-Grade Dysplasia and Cancer GARY W. FALK,* PRASHANTHI N. THOTA,* JOEL
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1089 1094 Barrett s Esophagus in Women: Demographic Features and Progression to High-Grade Dysplasia and Cancer GARY W. FALK,* PRASHANTHI N. THOTA,* JOEL
Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of the distal esophagus, gastroesophageal junction and gastric cardia?
 Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you)
") What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
Current issues in Barrett s oesophagus and the oesophago-gastric junction
 Current issues in Barrett s oesophagus and the oesophago-gastric junction Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The changing role of
Current issues in Barrett s oesophagus and the oesophago-gastric junction Professor Neil A Shepherd Gloucester & Cheltenham, UK Histopathology Regional Teaching Bristol May 11 2016 The changing role of
Vital staining and Barrett s esophagus
 Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Henry Moon was one of the giants in academic pathology during my early years.
 Henry Moon was one of the giants in academic pathology during my early years. Controversial stuff that occurs slightly above, within or slightly below the gastroesophageal junction, including Barrett s
Henry Moon was one of the giants in academic pathology during my early years. Controversial stuff that occurs slightly above, within or slightly below the gastroesophageal junction, including Barrett s
Barrett esophagus is a premalignant condition resulting
 Diagnostic Challenges in the Pathologic Evaluation of Barrett Esophagus Rhonda K. Yantiss, MD N Context. Barrett esophagus represents an unstable epithelium resulting from chronic gastroesophageal reflux
Diagnostic Challenges in the Pathologic Evaluation of Barrett Esophagus Rhonda K. Yantiss, MD N Context. Barrett esophagus represents an unstable epithelium resulting from chronic gastroesophageal reflux
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
ESMO Preceptorship Gastrointestinal Tumours Valencia October 2017
 www.esmo.org ESMO Preceptorship Valencia 06-07 October 2017 Gastrointestinal Tumours I have no conflicts of interest to declare Fátima Carneiro Gastrointestinal tumours Multidisciplinary management, standards
www.esmo.org ESMO Preceptorship Valencia 06-07 October 2017 Gastrointestinal Tumours I have no conflicts of interest to declare Fátima Carneiro Gastrointestinal tumours Multidisciplinary management, standards
In 1998, the American College of Gastroenterology issued ALIMENTARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT.
 PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
Barrett's Esophagus: Sorting Out the Controversy
 Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Current Management: Role of Radiofrequency Ablation
 Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease
 GASTROENTEROLOGY 2010;138:746 774 AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease AGA Podcast interview: www.gastro.org/gastropodcast. Learning
GASTROENTEROLOGY 2010;138:746 774 AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease AGA Podcast interview: www.gastro.org/gastropodcast. Learning
Gastrooesophageal reflux disease. Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia
 Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
What s New in the Management of Esophageal Disease
 What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
Update on Colonic Serrated (and Conventional) Adenomatous Polyps
 Adenomatous Polyps") Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment Barrett s esophagus
 E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
Barrett esophagus. Bible class Inselspital
 Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease
 Original Article Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease From Military Hospital, Rawalpindi Obaid Ullah Khan, Abdul Rasheed Correspondence: Dr. Abdul
Original Article Frequency of Barrett Esophagus in Patients with Symptoms of Gastroesophageal Reflux Disease From Military Hospital, Rawalpindi Obaid Ullah Khan, Abdul Rasheed Correspondence: Dr. Abdul
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastrointestinal pathology 2018 lecture 4. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis
 Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Part 1. A pragmatic approach to common problems in esophageal biopsy pathology
 Part 1 A pragmatic approach to common problems in esophageal biopsy pathology How I can help more patients than I hurt Barbara J McKenna University of Michigan barbmcke@med.umich.edu Case 1 The following
Part 1 A pragmatic approach to common problems in esophageal biopsy pathology How I can help more patients than I hurt Barbara J McKenna University of Michigan barbmcke@med.umich.edu Case 1 The following
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations
 Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
Gastroesophageal Junction Pathology: Diagnostic and Controversial Issues
 Gastroesophageal Junction Pathology: Diagnostic and Controversial Issues Robert D. Odze, MD, FRCPC BULLET POINTS The gastric cardia is the area of mucosa located distal to the GEJ (proximal aspect of gastric
Gastroesophageal Junction Pathology: Diagnostic and Controversial Issues Robert D. Odze, MD, FRCPC BULLET POINTS The gastric cardia is the area of mucosa located distal to the GEJ (proximal aspect of gastric
Changes to the diagnosis and management of Barrett s Oesophagus
 Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Primary mucinous adenocarcinoma developing in an ileostomy stoma
 Gut, 1988, 29, 1607-1612 Primary mucinous adenocarcinoma developing in an ileostomy stoma P J SMART, S SASTRY, AND S WELLS From the Departments of Histopathology and Surgery, Bolton General Hospital, Fan
Gut, 1988, 29, 1607-1612 Primary mucinous adenocarcinoma developing in an ileostomy stoma P J SMART, S SASTRY, AND S WELLS From the Departments of Histopathology and Surgery, Bolton General Hospital, Fan
Division of Anatomic Pathology & Molecular Oncology, University of Utah and ARUP Laboratories, Huntsman Cancer Institute, Salt Lake City, UT, USA
 REVIEW ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2014.14.3.131 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2014;14(3):131-162 Barrett s Esophagus Mary P. Bronner Division
REVIEW ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2014.14.3.131 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2014;14(3):131-162 Barrett s Esophagus Mary P. Bronner Division
American Journal of Gastroenterology. Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma
 Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
During the past 30 years, the incidence of esophageal ORIGINAL ARTICLES
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:38 43 ORIGINAL ARTICLES Optical Coherence Tomography to Identify Intramucosal Carcinoma and High-Grade Dysplasia in Barrett s Esophagus JOHN A. EVANS,* JOHN
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:38 43 ORIGINAL ARTICLES Optical Coherence Tomography to Identify Intramucosal Carcinoma and High-Grade Dysplasia in Barrett s Esophagus JOHN A. EVANS,* JOHN
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Barrett s Esophagus and Barrett s-associated Neoplasia: Etiology and Pathologic Features
 Barrett s Esophagus and Barrett s-associated Neoplasia: Etiology and Pathologic Features Domenico Coppola, MD, and Richard C. Karl, MD Enhancement of molecular markers and cytology may improve outcomes
Barrett s Esophagus and Barrett s-associated Neoplasia: Etiology and Pathologic Features Domenico Coppola, MD, and Richard C. Karl, MD Enhancement of molecular markers and cytology may improve outcomes
Pathology of the oesophagus and the stomach. Neil A Shepherd Gloucester, UK. Bristol Pathology 1 st Year Training School, The layers of the GI tract
 Pathology of the oesophagus and the stomach Neil A Shepherd Gloucester, UK Bristol Pathology 1 st Year Training School, The layers of the GI tract 1 Some facts about Histopathology and the upper GI tract
Pathology of the oesophagus and the stomach Neil A Shepherd Gloucester, UK Bristol Pathology 1 st Year Training School, The layers of the GI tract 1 Some facts about Histopathology and the upper GI tract
Adenocarcinoma of the distal esophagus is a recognized
 ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
Magnifying Endoscopy and Chromoendoscopy of the Upper Gastrointestinal Tract
 Magnifying Endoscopy and Chromoendoscopy of the Upper Gastrointestinal Tract Alina M.Boeriu 1, Daniela E.Dobru 1, Simona Mocan 2 1) Department of Gastroenterology, University of Medicine and Pharmacy;
Magnifying Endoscopy and Chromoendoscopy of the Upper Gastrointestinal Tract Alina M.Boeriu 1, Daniela E.Dobru 1, Simona Mocan 2 1) Department of Gastroenterology, University of Medicine and Pharmacy;
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Esophageal submucosal mass icd 10
 Esophageal submucosal mass icd 10 Search 6-6-2011 ICD-10; Risk Adjustment / HCC; Evaluation & Management (E/M). I'm hoping someone can help me with this DX, "soft tissue mass in. Upper gastrointestinal
Esophageal submucosal mass icd 10 Search 6-6-2011 ICD-10; Risk Adjustment / HCC; Evaluation & Management (E/M). I'm hoping someone can help me with this DX, "soft tissue mass in. Upper gastrointestinal
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
From reflux to esophageal cancer. Josh Boys, MD TCV 2 nd year indentured servant
 From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Avances en patología gástrica. Novedades de la clasificación WHO (2010)
") XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology Avances en patología gástrica. Novedades de la clasificación WHO (2010) Fátima Carneiro
XXV Congreso de la Sociedad Española de Anatomía Patológica y División Española de la International Academy of Pathology Avances en patología gástrica. Novedades de la clasificación WHO (2010) Fátima Carneiro
Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Recurrent intestinal metaplasia at the gastroesophageal junction following endoscopic eradication of dysplastic Barrett s esophagus may not be benign
 THIEME E849 Recurrent intestinal metaplasia at the gastroesophageal junction following endoscopic eradication of dysplastic Barrett s esophagus may not be benign Authors Georgina R. Cameron 1, 3, Paul
THIEME E849 Recurrent intestinal metaplasia at the gastroesophageal junction following endoscopic eradication of dysplastic Barrett s esophagus may not be benign Authors Georgina R. Cameron 1, 3, Paul
32 Adenocarcinoma of the oesophagogastric junction
 Adenocarcinoma of the oesophagogastric junction S.J. Spechler P. Hainaut M.F. Dixon R. Lambert R. Genta R. Siewert Definition Adenocarcinomas that straddle the junction of the oesophagus and stomach are
Adenocarcinoma of the oesophagogastric junction S.J. Spechler P. Hainaut M.F. Dixon R. Lambert R. Genta R. Siewert Definition Adenocarcinomas that straddle the junction of the oesophagus and stomach are
Sixteen-year follow-up of Barrett s esophagus, endoscopically treated with argon plasma coagulation
 Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
The normal esophagus is lined with squamous epithelium.
 .. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
.. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Barrett s Esophagus: State of the Art Management
 In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series
 E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
Archived at the Flinders Academic Commons:
 Archived at the Flinders Academic Commons: http://dspace.flinders.edu.au/dspace/ This is the authors version of an article published in Expert Review of Gastroenterology and Hepatology. The original publication
Archived at the Flinders Academic Commons: http://dspace.flinders.edu.au/dspace/ This is the authors version of an article published in Expert Review of Gastroenterology and Hepatology. The original publication
Speaker disclosure. Objectives. GERD: Who and When to Treat 7/21/2015
 GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia
 ...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
CDx Diagnostics THE NEW STANDARD FOR QUALITY GI CARE
 CDx Diagnostics THE NEW STANDARD FOR QUALITY GI CARE STUDYDESIGN 16 major academic GI centers participated in a double-blind, randomized, crossover study in which 160 high-risk patients undergoing BE surveillance
CDx Diagnostics THE NEW STANDARD FOR QUALITY GI CARE STUDYDESIGN 16 major academic GI centers participated in a double-blind, randomized, crossover study in which 160 high-risk patients undergoing BE surveillance
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
Kids Like to Break the Rules: Gastrointestinal Pathology in Children
 Kids Like to Break the Rules: Gastrointestinal Pathology in Children Jeffrey Goldsmith MD Director of Surgical Pathology, Beth Israel Deaconess Medical Center; Consultant in Gastrointestinal Pathology,
Kids Like to Break the Rules: Gastrointestinal Pathology in Children Jeffrey Goldsmith MD Director of Surgical Pathology, Beth Israel Deaconess Medical Center; Consultant in Gastrointestinal Pathology,