SPECIALISED ACCESSORY CELLS OF LYMPHOID TISSUES. Interdigitating dendritic cell (IDC) of lymph node T-zone
|
|
|
- Joy Lane
- 5 years ago
- Views:
Transcription

 Interdigitating dendritic cell (IDC) of")
 Follicular dendritic cells (FDC) of lymph node B-cell follicles Fibroblastic reticular")
1 KRISTIN HENRY IMPERIAL COLLEGE LONDON at CHARING CROSS HOSPITAL 23 rd ADIAP INTERNATIONAL CONGRESS Beirut November 29 - December 3, 2011 Dendritic Cell Associated Diseases: neoplastic and non-neoplastic SPECIALISED ACCESSORY CELLS OF LYMPHOID TISSUES Macrophages amd histiocytes Veiled cells Langerhans cells (LC) Interdigitating dendritic cell (IDC) of lymph node T-zone Interstitial DC of parenchymal organs Plasmacytoid dendritic cells (PDCs ) Follicular dendritic cells (FDC) of lymph node B-cell follicles Fibroblastic reticular cells (FRCs) 1
, CD1a+, S100+ Langerhans cell: langerin +, CD1a+, S100+ IDC: langerin-, CD1a-, S100+, fascin+ PDC:")
 & processing Morphology: LM: mononucleated cells, folded nuclei dendritic")
2 TABLE I IMMUNOPHENOTYPE OF ACCESSORY CELLS OF THE IMMUNE RESPONSE BM CD34+ DERIVED Macrophages: CD14+, CD11c+, CD68+, CD163+ Interstitial DC: CD1a-, FXIIIa+, CD68+, DCSIGN+ MESENCHYME DERIVED FDC: CD21+, CD23+, CD35+,desmoplakin+, fascin+ FRC: Muscle actin+, keratins-/+ Veiled cell: langerin +(V), CD1a+, S100+ Langerhans cell: langerin +, CD1a+, S100+ IDC: langerin-, CD1a-, S100+, fascin+ PDC: IL3, CD4, CD68+, CD123+, CD303, TCL1, MxA THE LANGERHANS CELL Specialised accessory dendritic cells involved in T-cell immunity Origin: Bone Marrow Site: Skin & other squamous epithelia eg. cervix, vagina oesophagus, respiratory tract, thymus Function : dendritic cells involved in antigen capture (endocytosis) & processing Morphology: LM: mononucleated cells, folded nuclei dendritic processes EM: Birbeck granules. No cell junctions CD1a Phenotype: MHC Class II S100+, CD1a+, Langerin* + Immature: CD40+, CD83-, CD86-, DC- LAMP, CD68+, lyzozyme+ Mature: CD40+, CD83+. CD86+, CD208** +, CD68-, lysozyme- Adhesion molecules differ between LCH and normal LCs * CD lectin involved in BG ** DC LAMP- lysosome associated membrane protein CD1a 2




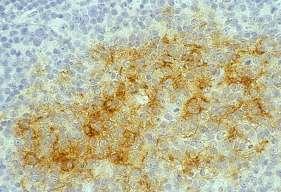
3 INTERDIGITATING DENDRITIC CELL (IDC) Specialised accessory Ag presenting dendritic cells Origin: Bone Marrow Site: paracortex of lymph nodes; T-zones of extra-nodal tissues, BM, thymus Function : dendritic cells involved in T-cell immunity antigen presentation T cells Morphology: LM: mononucleated cells with rounded to irregular folded nuclei, indistinct cytoplasm; EM: Complex interdigitating dendritic processes. No Birbeck granules. No cell junctions Phenotype: MHC Class II++ S100+, CD1a-, CD68+/-, fascin+ Prominent in dermatopathic lymphadenpathy and in lymph nodes in Sezary syvdrome IDC s Lymph node Thymus 3
?")



4 IDCs in dermatopathic lymphadenopathy CD1a FOLLICULAR DENDRITIC CELLS (FDC) Specialised non-phagocytic Ag. presenting dendritic cells involved in B-cell immunity Origin: mesenchymal precursor cell -? Fibroblast precursor (3C8)? endotheleal cells Function: Involved in migration, proliferation, cell selection and differentiation into memory B-cells and plasma cells. Direct B- cells undergo isotype switching and affinity maturation and differentiation by trapping and presenting Ag/immune complexes to B-cells Only high affinity B- cells survive and escape apoptosis. Site: GCs of lymph nodes. Most numerous in relation of non-proliferating B- lymphocytes in the light zone Overall, FDC comprise 1-2% of all GC cells Also found in non-lymphoid sites a with germinal centre (GC) reaction: eg. synovium in rheumatoid arthritis, gastric mucosa in H. pylori infection, thyroid in Hashimoto s disease, soft tissues in Kimura s disease Morphology LM: Elongate ovoid nuclei, angulated, often in pairs. Cytoplasm ill defined Central small to medium sized nucleus. Form polykaryocytes. EM: Long slender interdigitating dendritic processes connected by desmosomes. Processes coated with electron dense protein ( IC) Phenotype: CD21+, CD23+, CD35+, desmoplakin+, fascin+, S100-/+, CD68-, lysozyme- Specific markers: mab to long splice isoform of CD21 (CD21L). 3 other markers also recognise CD 21L; DRC-1, KiM4, 7Dk6 4






5 Germinal centres (GCs) MGP Ki67 FDCs in GCs CD21 5



6 F C F C F C F C F C POLYKARYOCYTES CD21 6

7 PLASMACYTOID DENDRITIC CELL (PDCs) Specialised monocytes ( plasmacytoid monocytes) type 1 interferon α secreting cells Origin: Bone marrow Previously designated as plasmacytoid T-cells Site: recruited to lymphoid tissues and various non-lymphoid sites from circulating monocytes Morphology: LM: mononucleated cells with slightly irregular nuclei and scanty well delineated cytoplasm lacking dendritic processes Phenotype: CD45+, CD4+, CD68+, CD123+ (interleukin-3 α chain receptor), BDCA-2/CD303, TCL1, CLA, Mx A (interferon α dependent molecule) CD56-, lysozyme-, MPO-, CD3- Prominent in reactive lymphadenopathies, viral infections- eg. HIV, toxoplasmosis, Castleman s disease and Kikuchi s disease* May also rarely be found in association with myeloid neoplasia and CD1a some lymphomas, eg. HL and AML * may possibly be the target cells involved in the necrotic process 7





8 PCDs Reactive lymphadenopathy Ki67 CD4 CD3 CD68 Ki67 8
9 SPECIALISED ACCESSORY CELLS OF LYMPHOID TISSUES Macrophages amd histiocytes Langerhans cells (LC) Interdigitating dendritic cell (IDC) of lymph node T-zone Interstitial DC of parenchymal organs Veiled cells Follicular dendritic Cells (FDC) of lymph node B-cell follicles Plasmacytoid dendritic cells (PDCs ) CLASSIFICATION OF HISTIOCYTIC AND DENDRITIC CELL NEOPLASMS WHO 2008 Histiocytic sarcoma Tumours derived from Langerhans cells Langerhans cell histiocytosis Langerhans cell sarcoma Interditating cell sarcoma Folicular dendritic cell sarcoma Other rare dendritic cell tumours Fibroblastic reticular cell tumour Indeterminate reticular cell tumour Disseminated juvenile xanthogranuloma Blastic plasmacytoid dendritic neoplasm + 9
10 LCH Clonal granulomatous disease characterized by accumulation of LCs at various sites*: eg. bone, skin, lung**, BM, lymph nodes, CNS Rare disease; about 5/million. Lesions solitary or multiple; involve one or more systems Any age: mainly children (peak incidence 1-3 years) but adults also Familial cases occur but no consistent cytogenetic defect Aetiology unknown*: malignant clonal disorder V inflammatory/reactive cytokine expression eg response to virus v aberrant T cell function increased survival of LCs* Course: spontaneous regression, frequent recurrences, progression * increased survival of LCs due to **Isolated pulmonary LCH- associated with smoking altered T-cell function (Senechal B et al.2006) TUMOURS OF HISTIOCYTES AND ACCESSORY DENDRITIC CELLS I International Lymphoma Study Group (ILSG). Histopathology 41: Study based on 61 cases using IHC In order of frequency LCH- n= 26: typical (LC tumour) = 17 atypical (LC sarcoma) = 9 Histiocytic Sarcoma - n=18 FDC tumours - n= 13 IDC tumours- n=4 Unclassified n=4 10

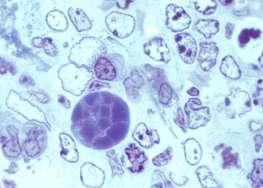
11 LANGERHANS CELL HISTIOCYTOSIS (LCH) Clinical syndrome Letterer- Siwe disease (L-S D) Hand- Schuller- Christian disease (H-S-C D) Eosinophilic granuloma (EG) Classification Scheme Unifocal unisystem disease: eg. - bone (skull, femur, rib, pelvis) lymph node, skin, lung Multifocal unisystem disease : H-S-C D; multiple bone sites; skull bones diabetes insipidus Multifocal multisystem disease: L-S D - multiple organs (bones, skin liver, spleen, lungs*, lymph nodes, BM) * Associated with smoking Morphology LANGERHANS CELL HISTIOCYTOSIS LM: LC cells medium to large with distinctive folded nuclei and linear grooves resembling coffee beans. Atypia minimal. Mitoses variable-usually few Cytoplasm moderately abundant; lack dendritic processes. LCs mixed with variable numbers of eosinophils, lymphocytes, macrophages. In lymph nodes, eosinophilic abscesses +/- central necrisis Lymphocytic component comprise many T- cells Lesions may contain multinucleated cells and giant cell similar to osteoclasts. Chronic lesions - foamy macrophages, plasma cells; fibrosis EM: Birbeck granules 11
 Sub-domain of")
 LCH, Skin LCH, LN LCH: IMMUNOPHENOTYPE CDIa +ve, S100 +, CD40+, CD4 +,")
 - usually < 10%; may be 25% Chronic lesions - immature phenotype Isolated skin lesions -")

12 Birbeck Granules (BGs) Organelles seen only at EM level Pentalaminar rods nm long, 33 nm wide; derive from cell membrane Terminal flask-like expansions (tennis racket-like) Sub-domain of the endoplasmic reticulum compartment (ERC) Identified in LCs and LCH. Express langerin (CD207) LCH, Skin LCH, LN LCH: IMMUNOPHENOTYPE CDIa +ve, S100 +, CD40+, CD4 +, HLA DR +, vimentin +, CD207+ (langerin) PLAP+*, CD68-/+, lysozyme -/+, CD208+/- SEMAG6A+** S100 PI (Ki67) - usually < 10%; may be 25% Chronic lesions - immature phenotype Isolated skin lesions - more mature phenotype Lesions rich in cytokines; eg. IFN γ, CD10 osteolysis, fibrosis CDIa * cf. normal LCs - PLAP ve. Also adhesion molecule expression differs between LCH and normal LC ** glycoprotein involved in T- cell immunity* 12







13 LCH middle ear/temporal bone S100 CD1a LCH - lymph node (eosinophilic granuloma) Sinus involvement paracortex Eosinophils +++; eosinophilic abscesses +/- central necrosis 13


 Prognosis; aggressive tumour.")
14 LCH of thymus Langerhans Cell Sarcoma: ILSG 2002 Patients older than LCH Multi organ involvement 9/26 cases of LC tumours Histology: LC cells show pronounced atypia; prominent nucleoli; fewer grooved cells; higher mitotic count-usually>50/10 hpf Fewer eosinophils Immunophenotype: similar to LCH but CD1a + cells focal PI (Ki %) Prognosis; aggressive tumour. overall survival 50% 14
15 LCH ASSOCIATIONS HIV lymphadenitis Lymphomas, especially HL Leukaemias, myelomonocytic LCH LC sarcoma LCH: PROGNOSTIC FACTORS Clinical outcome depends on number of organs affected Overall survival is 95% if disease unifocal (75% if 2 organs involved) Progression from unifocal lesions to multi-focal disease occurs in 10% of patients No correlation of cytological atypia & increased mitotic rate with prognosis (except in LCS) 15
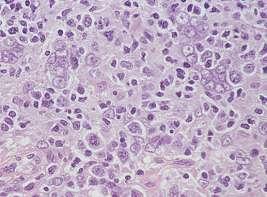
16 INTERDIGITATING DENDRITIC CELL (IDC) SARCOMA Extremely rare neoplasm; single case reports or very small series - 4 cases Adults predominantly affected (only one paediatric series of 4 cases reported) Slight male predominance Sites of involvement variable; LN involvement most common but extranodal sites eg. skin, soft tissues also recorded Presentation usually with asymptomatic mass; B-symptoms have also been reported and rarely, generalised lympgadenopathy, splenomegaly or hepatomegaly Prognosis: aggressive clinical course; 50% die from disease and visceral organ involvement - most commonly liver, spleen, kidney, lung TUMOURS OF HISTIOCYTES AND ACCESSORY DENDRITIC CELLS I International Lymphoma Study Group (ILSG). Histopathology 41: Study based on 61 cases using IHC In order of frequency LCH- n= 26: typical (LC tumour) = 17 atypical (LC sarcoma) = 9 Histiocytic Sarcoma - n=18 FDC tumours - n= 13 IDC tumours- n=4 Unclassified n=4 16


 10-20% Genetics: no specific abnormalities currently known Ig heavy chain gene and T-cell receptor genes all in germline")
17 IDC SARCOMA Morphology: Paracortical involvement of lymph nodes with residual follicles Spindle to rounded cells fascicles, whorls and storiform patterns Occasionally sheets of round cells Nuclei; spindled to ovoid, dispersed chromatin and small to large nucleoli. Occasionally, multinucleated Cytoplasm; usually abundant, eosinophilic and borders indistinct Cytologic atypia variable. Necrosis not a feature Admixed lymphocytes numerous Morphologic features may be indistinguishable from FDC sarcoma Immunophenotype: S100+, fascin+, CD68 & lyzozyme variable + Langerin -, CD1a-, CD21-, CD23-, CD35- MPO-, CD34-, CD30-, EMA- Admixed small lymphocytes* CD3+ T-cells PI (Ki67) 10-20% Genetics: no specific abnormalities currently known Ig heavy chain gene and T-cell receptor genes all in germline configuration * B-cells virtually absent IDC SARCOMA 17







18 IDC Tumour CD68 S100 IDC tumour S100 S100 18
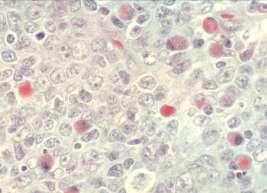
19 BLASTIC PLASMACYTOID DENDRITIC CELL NEOPLASM Aggressive tumour derived from precursor of plasmacytoid dendritic cells (plasmacytoid monocytes professional type 1 interferon producing cells ) with high frequency of skin and bone marrow involvement and leukaemic dissemination Synonyms: Blastic NK-cell lymphoma; agranular CD4+ natural killer cell leukaemia; CD4+CD56+ haematodermic tumour Rare haematologic tumour: M/F ratio 3.3:1 Majority of patients elderly (61-67yrs) but can occur at any age Presentation: Usually asymptomatic solitary or multiple skin lesions Regional lymph node involvement common (20%) PB and BM involvement minimal;invariable with progressive disease. Associated with AML or myelomonocytic leukamia (10-20%) Prognosis: Aggressive course. Survival months despite initial response to multi-agent chemotherapy Long lasting remissions reported in sporadic cases. Usually young patients in first remission treated with AML induction therapy followed by ASC transplantation BLASTIC PLASMACYTOID DENDRITIC CELL NEOPLASM Morphology: Diffuse infiltrate of medium sized blast cells with slightly irregular nuclei, fine chromatin and one to several small nucleoli. Cytoplasm scant and agranular Mitoses variable in number Angioinvasion and necrosis absent Skin involvement: sparing of epidermis; extension into subcutis. Lymph nodes; leukaemic patter of involvement of inter-follicular areas and medulla. BM; varies from mild interstitial infiltrate to massive infiltration. Residual marrow shows dysplasia- especially MgK lineage. Immunophenotype: CD4+, CD43+, CD45+, CD56+, CD68+(50%), TdT+ (33%) CD123+, BDCA-2/CD303+, TCL1 CLA+, MxA+ Other lymphoid and myeloid ass. Ags may be +ve eg. CD7, CD33 Lysozyme-, MPI-. Granzyme B- & TIA 1 ve in tissue sections Genotype: 2/3 of patients abnormal karyotype Specific chromosomal aberrations lacking but 6 complex karyotypes common Gene expression profiling and array- based comparative genomic hybridisation have shown certain consistent aberrations 19





20 BLASTIC PLASMACYTOID DENDRITIC CELL NEOPLASM CD4 CD8 CD4 CD56 20
 Cervical lymph nodes most common site but")

 No sex predominance except")
21 Ki67 CD43 CD68 FOLLICULAR DENDRITIC CELL TUMOUR/SARCOMA Rare tumour Most commonly present in lymph nodes (2/3 of patients) Cervical lymph nodes most common site but axillary, mesenteric and retroperitoneallymph nodes also frequently involved Other sites: Extra nodal lymphoid tissues - tonsil, oral cavity, spleen Extra nodal non-lymphoid tissues skin, soft tissue, lung, thyroid liver, pancreas, GI tract, breast Adults predominate; mean age 47 (range 14-77) No sex predominance except liver (F > M) 21
22 TUMOURS OF HISTIOCYTES AND ACCESSORY DENDRITIC CELLS I International Lymphoma Study Group (ILSG). Histopathology 41: Study based on 61 cases using IHC In order of frequency LCH- n= 26: typical (LC tumour) = 17 atypical (LC sarcoma) = 9 Histiocytic Sarcoma - n=18 FDC tumours - n= 13 IDC tumours- n=4 Unclassified n=4 FDC Tumour Histology Tumours usually well circumscribed Spindle cells arranged in whorls, fascicles; sometimes storiform pattern Nuclei usually ovoid: may also be binucleate, multinucleate or assume bizarre forms; usually low mitotic rate Cytoplasm poorly visualised at LM level EM, long processes connected by desmosomes Small lymphocytes scattered throughout Liver and spleen FDC tumours resemble inflammatory pseudotumour Misdiagnoses without IHC frequent Mimic carcinoma, thymoma, meningioma, melanoma, inflammatory MFH, lymphomas and other spindle cell tumours- especially IDC sarcoma 22




23 FDC tumour/sarcoma FDC tumour FDC sarcoma : differential diagnoses Spindle cell carcinoma Malignant melanoma Thymoma Meningioma Inflammatory MFH IDC sarcoma 23







24 CD21 CD21 lyzozyme S100 S100 CD68 CD68 FDC tumour CD68 CD68 CD21 CD21 p53 24
25 FDC Tumour: Phenotype CD21+, CD23+, CD35+ FDC specific markers +ve: KiM4, K1-FDC1, R4/23 Fascin +ve (non-specific) Clusterin +ve (highly specific) Desmoplakin, EMA & HLA DR - +/-ve S100 & CD68 very variable CD1a-ve, lyzozyme -ve, MPO-ve, CD34-ve, cytokeratins-ve Ki % FDC Tumours Aetiology: Unknown Although expressing CD21( EBV receptor), no association with EBV except liver tumours (common in Asians) Prognosis variable: 40-50% local recurrences Aggressive behaviour: if large tumour > 6cm intra abdominal tumour high PI significant cytologic atypia Metastases: Lymph nodes, lung and liver most common sites 25
26 Diseases with FDC involvement IMMUNE MEDIATED DISEASES - Autoimmune diseases: eg. rheumatoid arthritis, Hashimoto s thyroiditis, H. pylori gastritis - Castleman s disease* - Kimura s disease* INFECTIONS: - Viral diseases eg. HIV* - Prion diseases eg. Spongiform encephalopathies LYMPHOMAS - Follicular lymphoma - Hodgkin lymphoma - AIL T cell lymphoma* - Mantle cell lymphoma *Associated with increased vascularity CASTLEMAN S DISEASE Hyaline vascular type (HVCD) Plasma cell type (PCCD) Multicentric (MCD) single node group of nodes generalised associated with HIV infection Kaposi s sarcoma POEMS syndrome 26

27 CASTLEMAN S DISEASE A poorly understood lymphoproliferative disorder related to immune dysregulation Lymphoid and vascular proliferation with dysfunctional follicles Prominance of PDCs around vessels Usually a polyclonal non-neoplastic disorder PCCD associated with generalised lymphadenopathy and systemic symptoms and immunological disorders. May rarely progress to a BCL (usually plasmacytic) FDC sarcoma seen in conjunction with CD (10-20% cases) or follows yrs later. Evidence that HVCD is a precursor of FDC sarcoma >95% of MCD cases occur in HIV+ patients MCD may: - be associated with HHV8 (KSHV) and KS. PEL may also co-exist. - HHV8 encodes a viral IL 6; Il 6 induces B-cell proliferation and angiogenesis. - vil 6 is expressed in cells around GCS which are monotypic for lambda light chains and may undergo monoclonal expansion to plasmablastic lymphoma. CASTLEMAN S DISEASE HYALINE VASCULAR (HV) TYPE Masson trichrome 27




28 HVCD CD21 28




29 HVCD vascularity CD34 Castleman s disease plasma cell (PCCD) 29




30 PCCD CD21 λ PCCD Plasmacytoid dendritic cells CD68 30
 Factor VIII, Ulex, laminin +ve in PC CD (Hall et al 1989) Associated with KS")
 Clonal cytogenic aberration of chr.")
31 FDCs in CASTLEMAN S DISEASE FDC are hyperplastic; express CD21 CD35 Dysplastic FDCs in HV CD express ICAM-1 VCAM-1 ELAM-1 (Ruco et al 1991) Factor VIII, Ulex, laminin +ve in PC CD (Hall et al 1989) Associated with KS and other vascular tumours Associated with HHV8+ve pl.blasts in MC CD (Du et al 2001) Clonal cytogenic aberration of chr.12 (Cokelaere et al 2002) EGFR +ve ( Sun et al. 2003) MCD HIV+ve Vascular proliferation CD34 31



32 HIV ASSOCIATED LYMPHADENITIS Follicular hyperplasia; follicular lysis and disrupted FDC network Hyperplasia of FDCs & formation of polykaryocytes Increased vascularity Prominance of Ig secreting plasma cells CD-like changes Trapping of HIV on FDC processes as highly infectious HIV IC; no budding of HIV indicative of active infection of FDC HIV infection of target T cells requires CD4 R and CXCR4- a chemokine receptor expressed only by T-cells in the GC FDCs increase CXCR4 expression of T- cells and susceptibility to HIV infection HIV lymphadenitis CD21 32

33 HIV lymphadenitis FDC hyperplasia CD21 Masson trichrome HIV lymphadenitis plasma cell in GCs 33



34 HIV TYPE 1 LYMPHADENITIS CD21 CD21 CD21 HIV p24 34
35 FDC and HIV INFECTION Functional aspects: FDCs- trapped Ag (unprocessed) persists for many months and maintains long term memory IgG and IgE responses to soluble Ag. FDCs are reservoir for virus and play key role in CD4 infection Virus is trapped on FDC dendritic processes as highly infectious immune complexes (IC) FDCs AND LYMPHOMAS FDCs crucial to development and differentiation of B cells Specialised CXCL13+ve T-cells in GCs interact with FDCs FDCs contribute to lymphomagenesis by preventing apoptosis and proliferation of transformed B-cells Activated FDCs, T-cells, B cells may affect genetic instability and lymphoma FL, MCL & HL considered to derive from GCs Evidence now that T-cells in AIL T- cell lymphoma are GC derived 35
 Hodgkin lymphoma (HL) LN (FL) MC GC GC MZ")
36 LYMPHOMAS WITH FDC INVOLEMENT Follicular lymphoma (FL) Mantle cell lymphoma (MCL) Angioimmunoblastic T-cell lymphoma (AILT) Hodgkin lymphoma (HL) LN (FL) MC GC GC MZ 36






37 F L B CD20 Bcl2 CD21 CD3 Bcl 2 CD21 Ki67 37
 and ICAM-1 could result in detachment of B cells and progression to a diffuse growth pattern (Petrasch et al 1992, 1994) Absent or reduced FDC fascin")
38 FOLLICULAR LYMPHOMA (FL) Disturbance in FDC/B cell interactions in FL In FL, adhesion of B cells to FDC is via adhesion pathways LFA- 1/ICAM-1 VLA-4/VCAM- 1. B cells lacking VLA-4, LFA-1 α &β (CD11a, CD18) and ICAM-1 could result in detachment of B cells and progression to a diffuse growth pattern (Petrasch et al 1992, 1994) Absent or reduced FDC fascin expression in FL (Said et al 1998) Dense CD21 +ve FDC networks usually present in low grade FL and rare in high grade FL. Loss CD21+ve networks associated with progression to high grade FL (Shiozawa et al 2003). ANGIOIMMUNOBLASTIC T CELL LYMPHOMA 38



39 CD3 CD4 CD21 AILT and FDC FDCs - Key component of stromal-vascular change Diagnostic aid to diagnosis FDC proliferation pattern changes with progression of disease CD10 expressed by T- cells in % cases CD10/ CXCL13* co-expression by AILT T-cells and CG T- cell suggests origin of AILT from GC FDC associated T-cells Merchant et al. Am J Clin pathol 126:29-38, 2006 *also expressed by FDC 39





40 Mantle cell lymphoma MCL - diffuse Cyclin D1 CD5 Cyclin D1 CD21 40




41 MCL and FDC CD21 Study of 94 patients: FDC always present : in residual follicles in colonised follicles as residual networks Diffuse pattern worse prognosis than nodular pattern (regardless of whether blastoid variant) Schrader c et al. Virchows Arch 448: , 2006 CD20 CD20 Hodgkin lymphoma LP N CD21 41




42 HL NS CD21 CD30 CD3 HODGKIN LYMPHOMA PROGNOSIS AND FDC STATUS: Best prognosis - HL NLP Intermediate prognosis - HL NS and MC with FDC in neoplastic areas Absence of FDC in neoplastic areas - unfavourable prognosis Alavaikko et al 1994 DIAGNOSIS: Presence of FDC useful in separating HL NLP from T/HRBCL Boudova et al
43 FDCs AND LYMPHOMAS FDCs crucial to development and differentiation of B cells Specialised CXCL13+ve T-cells in GCs interact with FDCs FDCs contribute to lymphomagenesis by preventing apoptosis and proliferation of transformed B-cells Activated FDCs, T-cells, B cells may affect genetic instability and lymphoma FL, MCL & HL considered to derive from GCs Evidence now that T-cells in AIL T- cell lymphoma are GC derived DISEASE IS OF OLD AND NOTHING ABOUT IT HAS CHANGED IT IS WE WHO CHANGE WHEN WE LEARN TO RECOGNISE WHAT FORMERLY WAS IMPERCEPTIBLE Jean Marie Charcot Phycisian, Salpêtrière Hospital, Paris 43
3/24/2017 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS. Disclosure of Relevant Financial Relationships
 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
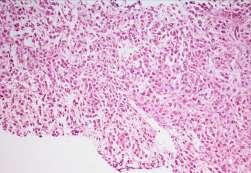
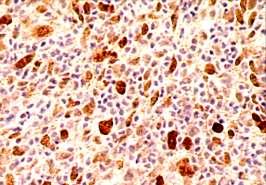
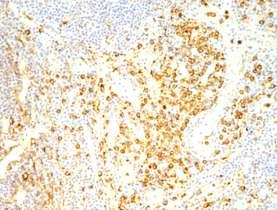
Case Presentation. Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD. Department of Pathology Jordan University Hospital Amman, Jordan
 Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Contents. vii. Preface... Acknowledgments... v xiii
 Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Spectrum of clinical presentations
 Spectrum of clinical presentations Case History A 7-day-old male patient born full-term via uncomplicated vaginal delivery was seen for multiple erythematous red-brown purpuric lesions that were present
Spectrum of clinical presentations Case History A 7-day-old male patient born full-term via uncomplicated vaginal delivery was seen for multiple erythematous red-brown purpuric lesions that were present
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
DETERMINATION OF A LYMPHOID PROCESS
 Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Combinations of morphology codes of haematological malignancies (HM) referring to the same tumour or to a potential transformation
 referring to the same tumour or to a potential transformation") Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Hematopathology Specialty Conference Case #1
 Hematopathology Specialty Conference Case #1 Robert (Bob) Ohgami, MD, PhD Assistant Professor Stanford University Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships
Hematopathology Specialty Conference Case #1 Robert (Bob) Ohgami, MD, PhD Assistant Professor Stanford University Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
2010 Hematopoietic and Lymphoid ICD-O Codes - Alphabetical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
2012 Hematopoietic and Lymphoid ICD-O Codes - Numerical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO
 HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
LYMPH GLAND. By : Group 1
 LYMPH GLAND By : Group 1 ANATOMY LYMPH NODE Lymphatic Organs Red bone marrow Thymus gland Lymph nodes Lymph nodules Spleen Primary organs Secondary organs Lymph Nodes Firm, smooth-surfaced, bean-shaped
LYMPH GLAND By : Group 1 ANATOMY LYMPH NODE Lymphatic Organs Red bone marrow Thymus gland Lymph nodes Lymph nodules Spleen Primary organs Secondary organs Lymph Nodes Firm, smooth-surfaced, bean-shaped
Classifications of lymphomas
 Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
SLIDE SEMINAR NON NEOPLASTIC LYMPH NODE DISORDERS DR SHEILA NAIR CMC, VELLORE
 SLIDE SEMINAR NON NEOPLASTIC LYMPH NODE DISORDERS DR SHEILA NAIR CMC, VELLORE Case 1 34 year old male, mass right cervical region, for 4 years. No other significant findings. Grossly, the mass was well
SLIDE SEMINAR NON NEOPLASTIC LYMPH NODE DISORDERS DR SHEILA NAIR CMC, VELLORE Case 1 34 year old male, mass right cervical region, for 4 years. No other significant findings. Grossly, the mass was well
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
MULTISYSTEMIC LANGERHANS CELL HISTIOCYTOSIS IN ADULT AN UNCOMMON INCIDENCE POSING A DIAGNOSTIC CHALLENGE. Monal Trisal
 Pathology Case Report International Journal of Clinical And Diagnostic Research ISSN 2395-3403 Volume 4, Issue 4, July-Aug 2016. Glorigin Lifesciences Private Limited. MULTISYSTEMIC LANGERHANS CELL HISTIOCYTOSIS
Pathology Case Report International Journal of Clinical And Diagnostic Research ISSN 2395-3403 Volume 4, Issue 4, July-Aug 2016. Glorigin Lifesciences Private Limited. MULTISYSTEMIC LANGERHANS CELL HISTIOCYTOSIS
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Osteosclerotic Myeloma (POEMS Syndrome)
") Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Small B-cell (Histologically Low Grade) Lymphoma
 Lymphoma") Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Anaplastic Large Cell Lymphoma (of T cell lineage)
") Anaplastic Large Cell Lymphoma (of T cell lineage) Definition T-cell lymphoma comprised of large cells with abundant cytoplasm and pleomorphic, often horseshoe-shaped nuclei CD30+ Most express cytotoxic
Anaplastic Large Cell Lymphoma (of T cell lineage) Definition T-cell lymphoma comprised of large cells with abundant cytoplasm and pleomorphic, often horseshoe-shaped nuclei CD30+ Most express cytotoxic
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Question 1. Kupffer cells, microglial cells and osteoclasts are all examples of what type of immune system cell?
 Abbas Chapter 2: Sarah Spriet February 8, 2015 Question 1. Kupffer cells, microglial cells and osteoclasts are all examples of what type of immune system cell? a. Dendritic cells b. Macrophages c. Monocytes
Abbas Chapter 2: Sarah Spriet February 8, 2015 Question 1. Kupffer cells, microglial cells and osteoclasts are all examples of what type of immune system cell? a. Dendritic cells b. Macrophages c. Monocytes
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
, , 2011 HODGKIN LYMPHOMA
 European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
Pathology of the indolent B-cell lymphomas Elias Campo
 Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Parts 2 and 3
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
The Adaptive Immune Response. T-cells
 The Adaptive Immune Response T-cells T Lymphocytes T lymphocytes develop from precursors in the thymus. Mature T cells are found in the blood, where they constitute 60% to 70% of lymphocytes, and in T-cell
The Adaptive Immune Response T-cells T Lymphocytes T lymphocytes develop from precursors in the thymus. Mature T cells are found in the blood, where they constitute 60% to 70% of lymphocytes, and in T-cell
Stefano A. Pileri. Chair of Pathology Haematopathology Unit Department L. and A. Seràgnoli. Bologna University Anatomic Theatre
 Histiocytic and dendritic cell tumours Stefano A. Pileri Chair of Pathology Haematopathology Unit Department L. and A. Seràgnoli gnoli Bologna University Anatomic Theatre Ilya Ilyich Mechnikov CD163+ Macrophage
Histiocytic and dendritic cell tumours Stefano A. Pileri Chair of Pathology Haematopathology Unit Department L. and A. Seràgnoli gnoli Bologna University Anatomic Theatre Ilya Ilyich Mechnikov CD163+ Macrophage
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
PRECURSOR LYMHPOID NEOPLASMS. B lymphoblastic leukaemia/lymphoma T lymphoblastic leukaemia/lymphoma
 PRECURSOR LYMHPOID NEOPLASMS B lymphoblastic leukaemia/lymphoma T lymphoblastic leukaemia/lymphoma B lymphoblastic leukaemia/lymphoma Definition: B lymphoblastic leukaemia/lymphoma is a neoplasm of precursor
PRECURSOR LYMHPOID NEOPLASMS B lymphoblastic leukaemia/lymphoma T lymphoblastic leukaemia/lymphoma B lymphoblastic leukaemia/lymphoma Definition: B lymphoblastic leukaemia/lymphoma is a neoplasm of precursor
PHYSIOLOGY AND MANAGEMENT OF HISTIOCYTIC DISEASE. Brant Ward, MD, PhD Division of Rheumatology, Allergy, and Immunology
 PHYSIOLOGY AND MANAGEMENT OF HISTIOCYTIC DISEASE Brant Ward, MD, PhD Division of Rheumatology, Allergy, and Immunology What do histiocytes do? Apoptotic body removal Phagocytosis Antigen presentation Types
PHYSIOLOGY AND MANAGEMENT OF HISTIOCYTIC DISEASE Brant Ward, MD, PhD Division of Rheumatology, Allergy, and Immunology What do histiocytes do? Apoptotic body removal Phagocytosis Antigen presentation Types
Follicular dendritic cell sarcoma of inguinal lymph node A case report
 Malaysian J Pathol 2008; 30(2) : 115 119 CASE REPORT Follicular dendritic cell sarcoma of inguinal lymph node A case report Jayalakshmi PAILOOR, MPath, FRCPath, Krishnan R IYENGAR, MD, DNB, CHAN KS, MPath*
Malaysian J Pathol 2008; 30(2) : 115 119 CASE REPORT Follicular dendritic cell sarcoma of inguinal lymph node A case report Jayalakshmi PAILOOR, MPath, FRCPath, Krishnan R IYENGAR, MD, DNB, CHAN KS, MPath*
The development of clonality testing for lymphomas in the Bristol Genetics Laboratory. Dr Paula Waits Bristol Genetics Laboratory
 The development of clonality testing for lymphomas in the Bristol Genetics Laboratory Dr Paula Waits Bristol Genetics Laboratory Introduction The majority of lymphoid malignancies belong to the B cell
The development of clonality testing for lymphomas in the Bristol Genetics Laboratory Dr Paula Waits Bristol Genetics Laboratory Introduction The majority of lymphoid malignancies belong to the B cell
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH
 EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
Case year old male with abdominal lymphadenopathy Treated with 8 cycles of R-CHOP One year later B-symptoms and progressive disease
 Codirectors Tsieh Sun, M.D., FASCP Francisco Vega, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Houston Texas There is no conflict of interest involved in the content and presentation
Codirectors Tsieh Sun, M.D., FASCP Francisco Vega, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Houston Texas There is no conflict of interest involved in the content and presentation
Low grade High grade , immune suppression chronic persistent inflammation viruses B-symptoms
 We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
Mimics of Lymphoma in Routine Biopsies. Mixed follicular and paracortical hyperplasia. Types of Lymphoid Hyperplasia
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Mimics of Lymphoma in Routine Biopsies. I have nothing to disclose regarding the information to be reported in this talk.
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
MACROPHAGE "MONOCYTES" SURFACE RECEPTORS
 LECTURE: 13 Title: MACROPHAGE "MONOCYTES" SURFACE RECEPTORS LEARNING OBJECTIVES: The student should be able to: Describe the blood monocytes (size, and shape of nucleus). Enumerate some of the monocytes
LECTURE: 13 Title: MACROPHAGE "MONOCYTES" SURFACE RECEPTORS LEARNING OBJECTIVES: The student should be able to: Describe the blood monocytes (size, and shape of nucleus). Enumerate some of the monocytes
LYMPHOID ORGANS. Dr. Iram Tassaduq
 LYMPHOID ORGANS Dr. Iram Tassaduq COMPONENTS OF IMMUNE SYSTEM Lymphocytes Diffuse Lymphatic Tissue Lymphatic Nodules Lymph node Spleen Bone marrow Thymus Functions of Immune System Has the ability to distinguish
LYMPHOID ORGANS Dr. Iram Tassaduq COMPONENTS OF IMMUNE SYSTEM Lymphocytes Diffuse Lymphatic Tissue Lymphatic Nodules Lymph node Spleen Bone marrow Thymus Functions of Immune System Has the ability to distinguish
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
11/8/2018 DISCLOSURES. I have NO Conflicts of Interest to Disclose. UTILTY OF DETECTING PATTERNS
 Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
Immunohistochemical classification of haematolymphoid tumours. Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital
 Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Incidence. Bimodal age incidence 15-40, >55 years Childhood form (0-14) more common in developing countries M:F=1.5:1; in all subtypes except NS
 more common in developing countries M:F=1.5:1; in all subtypes except NS") Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Corrigenda. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run
: corrections made in second print run") Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
Andrea s SI Session PCB Practice Test Test 3
 Practice Test Test 3 READ BEFORE STARTING PRACTICE TEST: Remember to please use this practice test as a tool to measure your knowledge, and DO NOT use it as your only tool to study for the test, since
Practice Test Test 3 READ BEFORE STARTING PRACTICE TEST: Remember to please use this practice test as a tool to measure your knowledge, and DO NOT use it as your only tool to study for the test, since
Bone Marrow. Procedures Blood Film Aspirate, Cell Block Trephine Biopsy, Touch Imprint
 Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Pathology #07. Hussein Al-Sa di. Dr. Sohaib Al-Khatib. Mature B-Cell Neoplasm. 0 P a g e
 Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Lymphocytoma Cutis. Cynthia M. Magro MD. Director of Dermatopathology Weill Medical College of Cornell University New York, New York
 Lymphocytoma Cutis Cynthia M. Magro MD Professor of Pathology Director of Dermatopathology Weill Medical College of Cornell University New York, New York Lymphocytoma Cutis Falls under other designations
Lymphocytoma Cutis Cynthia M. Magro MD Professor of Pathology Director of Dermatopathology Weill Medical College of Cornell University New York, New York Lymphocytoma Cutis Falls under other designations
Lymphoma and Pseudolymphoma
 Lymphoma and Pseudolymphoma Laura B. Pincus, MD Co-Director, Cutaneous Lymphoma Clinic Associate Professor Dermatology and Pathology University of California, San Francisco I HAVE NO RELEVANT RELATIONSHIPS
Lymphoma and Pseudolymphoma Laura B. Pincus, MD Co-Director, Cutaneous Lymphoma Clinic Associate Professor Dermatology and Pathology University of California, San Francisco I HAVE NO RELEVANT RELATIONSHIPS
The patient had a mild splenomegaly but no obvious lymph node enlargement. The consensus phenotype obtained from part one of the exercise was:
 Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
Hematolymphoid lesions of the skin Part II Myeloid neoplastic proliferations Houston Society of Clinical Pathologists Symposium April 14, 2018
 Hematolymphoid lesions of the skin Part II Myeloid neoplastic proliferations Houston Society of Clinical Pathologists Symposium April 14, 2018 Carlos A. Torres-Cabala, MD Associate Professor Chief, Dermatopathology
Hematolymphoid lesions of the skin Part II Myeloid neoplastic proliferations Houston Society of Clinical Pathologists Symposium April 14, 2018 Carlos A. Torres-Cabala, MD Associate Professor Chief, Dermatopathology
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Pathology of the Hematopoietic System. Case studies
 Pathology of the Hematopoietic System Case studies Shannon Martinson, September 2015 Signalment: 9 yr-old MC cat Case Study 1 History: Cat had been anorexic and developed bleeding in the eyes Physical
Pathology of the Hematopoietic System Case studies Shannon Martinson, September 2015 Signalment: 9 yr-old MC cat Case Study 1 History: Cat had been anorexic and developed bleeding in the eyes Physical
ACTIVATION OF T LYMPHOCYTES AND CELL MEDIATED IMMUNITY
 ACTIVATION OF T LYMPHOCYTES AND CELL MEDIATED IMMUNITY The recognition of specific antigen by naïve T cell induces its own activation and effector phases. T helper cells recognize peptide antigens through
ACTIVATION OF T LYMPHOCYTES AND CELL MEDIATED IMMUNITY The recognition of specific antigen by naïve T cell induces its own activation and effector phases. T helper cells recognize peptide antigens through
Follicular Lymphoma. ced3 APOPTOSIS. *In the nematode Caenorhabditis elegans 131 of the organism's 1031 cells die during development.
 Harvard-MIT Division of Health Sciences and Technology HST.176: Cellular and Molecular Immunology Course Director: Dr. Shiv Pillai Follicular Lymphoma 1. Characterized by t(14:18) translocation 2. Ig heavy
Harvard-MIT Division of Health Sciences and Technology HST.176: Cellular and Molecular Immunology Course Director: Dr. Shiv Pillai Follicular Lymphoma 1. Characterized by t(14:18) translocation 2. Ig heavy
The spectrum of flow cytometry of the bone marrow
 The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
Lymph node cytopathology : A practical approach to lymphoproliferative disorders
 Lymph node cytopathology : A practical approach to lymphoproliferative disorders Koray Ceyhan, M.D Department of Pathology Faculty of Medicine Ankara University Ankara, Turkey Diagnostic use of FNA in
Lymph node cytopathology : A practical approach to lymphoproliferative disorders Koray Ceyhan, M.D Department of Pathology Faculty of Medicine Ankara University Ankara, Turkey Diagnostic use of FNA in
SOPHOMORE DENTAL/OPTOMETRY MICROBIOLOGY SECTION: IMMUNOLOGY CELLS AND ORGANS OF THE IMMUNE SYSTEM
 SOPHOMORE DENTAL/OPTOMETRY MICROBIOLOGY SECTION: IMMUNOLOGY CELLS AND ORGANS OF THE IMMUNE SYSTEM Lecturer: Dr. John F Kearney 934-6557 jfk@uab.edu Objectives: To learn: 1) the basic cell types that make
SOPHOMORE DENTAL/OPTOMETRY MICROBIOLOGY SECTION: IMMUNOLOGY CELLS AND ORGANS OF THE IMMUNE SYSTEM Lecturer: Dr. John F Kearney 934-6557 jfk@uab.edu Objectives: To learn: 1) the basic cell types that make
HISTOPATHOLOGY. Shannon Martinson
 HISTOPATHOLOGY Shannon Martinson March 2013 Case #1 History: 8 year old beagle Neck pain for the past couple of weeks Paresis, followed by paralysis developed over the past few days Gross Description courtesy
HISTOPATHOLOGY Shannon Martinson March 2013 Case #1 History: 8 year old beagle Neck pain for the past couple of weeks Paresis, followed by paralysis developed over the past few days Gross Description courtesy
Figure 2: Lymph node Cortical follicular (F) and paracortical (PC) atrophy, with narrowing of the cortex relative to the medulla (M).
 and paracortical (PC) atrophy, with narrowing of the cortex relative to the medulla (M).") Figure 1: Lymph node Follicular hyperplasia, with expansion of the follicular germinal centres (F) by large blast cells. Paracortical hyperplasia, with expansion of the paracortex (PC) by small lymphocytes.
Figure 1: Lymph node Follicular hyperplasia, with expansion of the follicular germinal centres (F) by large blast cells. Paracortical hyperplasia, with expansion of the paracortex (PC) by small lymphocytes.
Aggressive B-Cell Lymphomas
 Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Pathology of the Lymphoid System
 Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Simon Haefliger. Pathologie. Fallvorstellung
 Simon Haefliger Pathologie Fallvorstellung Castleman s disease Historical perspective Classification Epidemiology and clinical aspects Microscopic caracteristics Pathogenesis Historical perspective First
Simon Haefliger Pathologie Fallvorstellung Castleman s disease Historical perspective Classification Epidemiology and clinical aspects Microscopic caracteristics Pathogenesis Historical perspective First
SMOOTH MUSCLE TUMOURS
 SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
Many of the hematolymphoid disorders are derived
 REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Canine Histiocytic Disorders DR. MEREDITH GAUTHIER, DVM DACVIM (ONCOLOGY) OCTOBER 29, 2015
 OCTOBER 29, 2015") Canine Histiocytic Disorders DR. MEREDITH GAUTHIER, DVM DACVIM (ONCOLOGY) OCTOBER 29, 2015 Canine Histiocytes! Cells derived from CD34+ stem cells and blood monocytes! Macrophages! Dendritic cells (DC)!
Canine Histiocytic Disorders DR. MEREDITH GAUTHIER, DVM DACVIM (ONCOLOGY) OCTOBER 29, 2015 Canine Histiocytes! Cells derived from CD34+ stem cells and blood monocytes! Macrophages! Dendritic cells (DC)!
HAEMATOLOGICAL MALIGNANCY
 HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
Case year female. Routine Pap smear
 Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Generation of post-germinal centre myeloma plasma B cell.
 Generation of post-germinal centre myeloma. DNA DAMAGE CXCR4 Homing to Lytic lesion activation CD38 CD138 CD56 Phenotypic markers Naive Secondary lymphoid organ Multiple myeloma is a malignancy of s caused
Generation of post-germinal centre myeloma. DNA DAMAGE CXCR4 Homing to Lytic lesion activation CD38 CD138 CD56 Phenotypic markers Naive Secondary lymphoid organ Multiple myeloma is a malignancy of s caused
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Chapter 2 (pages 22 33): Cells and Tissues of the Immune System. Prepared by Kristen Dazy, MD, Scripps Clinic Medical Group
: Cells and Tissues of the Immune System. Prepared by Kristen Dazy, MD, Scripps Clinic Medical Group") Allergy and Immunology Review Corner: Cellular and Molecular Immunology, 8th Edition By Abul K. Abbas, MBBS; Andrew H. H. Lichtman, MD, PhD; and Shiv Pillai, MBBS, PhD. Chapter 2 (pages 22 33): Cells and
Allergy and Immunology Review Corner: Cellular and Molecular Immunology, 8th Edition By Abul K. Abbas, MBBS; Andrew H. H. Lichtman, MD, PhD; and Shiv Pillai, MBBS, PhD. Chapter 2 (pages 22 33): Cells and
WBCs Disorders. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent
 Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Lymphoid System: cells of the immune system. Answer Sheet
 Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
Lymphoid System: cells of the immune system Answer Sheet Q1 Which areas of the lymph node have most CD3 staining? A1 Most CD3 staining is present in the paracortex (T cell areas). This is towards the outside
Adaptive Immunity: Humoral Immune Responses
 MICR2209 Adaptive Immunity: Humoral Immune Responses Dr Allison Imrie 1 Synopsis: In this lecture we will review the different mechanisms which constitute the humoral immune response, and examine the antibody
MICR2209 Adaptive Immunity: Humoral Immune Responses Dr Allison Imrie 1 Synopsis: In this lecture we will review the different mechanisms which constitute the humoral immune response, and examine the antibody
PET Imaging in Langerhans Cell Histiocytosis
 PET Imaging in Langerhans Cell Histiocytosis Christiane Franzius Bremen, Germany Histiocytosis Histiocytosis Idiopathic proliferation of histiocytes Two types of histiocytes macrophages: antigen processing
PET Imaging in Langerhans Cell Histiocytosis Christiane Franzius Bremen, Germany Histiocytosis Histiocytosis Idiopathic proliferation of histiocytes Two types of histiocytes macrophages: antigen processing
Principles of Adaptive Immunity
 Principles of Adaptive Immunity Chapter 3 Parham Hans de Haard 17 th of May 2010 Agenda Recognition molecules of adaptive immune system Features adaptive immune system Immunoglobulins and T-cell receptors
Principles of Adaptive Immunity Chapter 3 Parham Hans de Haard 17 th of May 2010 Agenda Recognition molecules of adaptive immune system Features adaptive immune system Immunoglobulins and T-cell receptors
B cell activation and antibody production. Abul K. Abbas UCSF
 1 B cell activation and antibody production Abul K. Abbas UCSF 2 Lecture outline B cell activation; the role of helper T cells in antibody production Therapeutic targeting of B cells 3 Principles of humoral
1 B cell activation and antibody production Abul K. Abbas UCSF 2 Lecture outline B cell activation; the role of helper T cells in antibody production Therapeutic targeting of B cells 3 Principles of humoral