Fever of Unknown Origin
|
|
|
- Darcy Nicholson
- 5 years ago
- Views:
Transcription
1 Fever of Unknown Origin Dr. Kaya Süer Near East University Faculty of Medicine Infectious Diseases and Clinical Microbiology
2 FUO Most episodes of fever in humans are short-lived do not require diagnostic investigation or specific therapy. Some episodes of fever in humans can be readily diagnosed and effectively treated However, a small but important subgroups of fever are persistent and difficult to diagnose.
3 FUO Such puzzling fevers have fascinated and frustrated clinicians since the earliest days of clinical studies Prolonged and Perplexing Fevers, published by Keefer and Leard in 1955 Fever of Unknown Origin: Report on 100 cases, by Petersdorf and Beeson in 1961
4 Terminology and Definition In the United States, The term fever of unknown origin (FUO) is generally used. In other countries an alternative term, pyrexia of unknown origin (PUO), is often used.
5 Terminology and Definition The first formal definition of FUO by Petersdorf and Beeson nearly five decades ago: fever higher than 38.3 C persisting without diagnosis for at least 3 weeks persisting at least 1 week s investigation in hospital
6 Terminology and Definition Investigators have modified and extended this classical definition Classical FUO Health Care Associated FUO Immune-deficient FUO HIV-related FUO Computed axial tomography, magnetic resonance imaging, ultrasound imaging, nucleic acid based diagnostic testing, and rapid tests for pathogens have changed the landscape of FUO.
7 Four Subtypes of FUO Classical FUO Health care associated FUO Immune- Deficient FUO HIV-Related FUO Definition >38.0 C, >3 wk, >2 visits or 3 days in hospital >38.0 C, >3 days, not present or incubating on admission >38.0 C, >3 days, negative cultures after 48 hr 38.0 C, >3 wk for outpatients, >3 days for inpatients, HIV infection confirmed Leading causes Cancer, infections, inflammatory conditions, undiagnosed habitual hyperthermia Health care associated infections, postoperative complications, drug fever Majority due to infections, but cause documented in only 40%-60% HIV (primary infection), typical and atypical mycobacteria, CMV, lymphomas, toxoplasmosis, cryptococcosis, immune reconstitution inflammatory syndrome (IRIS)
8 Classical fever of unknown origine Most patients with classical FUO have subacute or chronic symptoms and therefore can be safely investigated as outpatients. In a series of 53 FUO patients; the median duration of fever before diagnosis was 40 days.
9 Classical fever of unknown origine Disorders causing classical FUO in five categories: Infections Neoplasms Connective tissue diseases Miscellaneous other disorders Undiagnosed illnesses
10 Classical fever of unknown origine In most series, infections are the largest category, accounting for 25% to 50% of cases However, if patients older than 65 years, infections become less common, falling into second or third place as a cause of classical FUO
11 Classical fever of unknown origine Among the infections responsible for classical FUO : abscesses endocarditis tuberculosis complicated urinary tract infections have consistently been among the most important. Infections tend to vary in incidence according to locale. Visceral leishmaniasis, 8% of cases reported from Spain. Familial Mediterranean fever in Ashkenazi Jews Kikuchi s disease (an unusual form of necrotizing lymphadenitis) primarily in Japan TRAPS (TNF-receptor associated periodic fever), formerly called familial Hibernian fever in Ireland
12 Classical fever of unknown origine The miscellaneous category rare causes of classical FUO: Addison s disease Adult Still s disease Alcoholic hepatitis Aortic dissectionytosis X Behçet s syndrome Chronic meningitis Erythema multiforme Fabry s disease Granulomatous hepatitis Histiocytosis X Inflammatory bowel disease Pheochromocytoma Sarcoidiosis Vitamin B12 deficiency and more specific diseases
13 Classical fever of unknown origine Allergic alveolitis Atrial myxoma Autoimmune cholangitis Bartonellosis Carcinomatous meningitis Castleman s disease Cirrhotic fever Cyclic neutropenia Drug fever and other Hypersensitivities Factitious fever Familial Hibernian fever Familial Mediterranean fever Giant coronary aneurysm Granulomatous peritonitis Hantavirus infection Hemoglobinopathies Hemolytic anemias Hemophagocytic syndrome Human picornavirus infection
14 Hypereosinophilic syndrome Immunoblastic lymphadenopathy Infected urachal cyst Kikuchi-Fujimoto disease Lofgren syndrome Lymphomatoid granulomatosis Metal fume fever Myeloproliferative syndromes Pancreatitis Parathyroid apoplexy Paroxysmal hemoglobinurias Pericarditis Periodic fever Polyarteritis nodosa Postpericardiotomy syndrome Pulmonary emboli Resorbing hematoma Retroperitoneal fibrosis Rosai-Dorfman disease Schnitzler s syndrome Sinusitis Serum sickness Sjögren s syndrome Subacute necrotizing lymphadenitis Thrombotic thrombocytopenic purpura Thyroiditis and thyrotoxicosis Veno-occlusive disease Wegener s granulomatosis Whipple s disease
15 Classical fever of unknown origine Connective tissue diseases responsible for classical FUO, Still s disease (juvenile rheumatoid arthritis) other variants of rheumatoid arthritis systemic lupus erythematosus predominate in younger patients, Whereas temporal arteritis polymyalgia rheumatica syndromes are more common in elderly patients.
16 Classical fever of unknown origine Malignant neoplasms, can induce fever directly through the production and release of pyrogenic cytokines (lymphomas) They can also generate fevers indirectly by undergoing spontaneous or induced necrosis or by creating conditions to secondary infections, such as postobstructive pneumonia
17 Classical fever of unknown origine Infants and children : The diseases responsible for classical FUO in infants differ from those in older children and adults. Respiratory infections cause classical FUO in infants more often than in children older than 12 months or in adults. The relative frequency of infections as the cause of FUO in infants is high, connective tissue diseases and cancers are rare in this age group.
18 Classical fever of unknown origine Kawasaki disease occurs in children younger than 5 years. Connective tissue diseases are rarely seen in children younger than 12 months, Still s disease is a leading cause of FUO in older children and young adults. Joint involvement in children with FUO usually signifies a serious underlying disorder, such as Connective tissue disease, Endocarditis, Leukemia.
19 Classical fever of unknown origine In a series of 146 pediatric cases of FUO, established a specific diagnosis in only 84(57.5%). Of these, 64 (43.8%) Infections, 11 (7.5%) Autoimmune disorders, 4 (2.7%) Malignant neoplasms, 5 (3.4%) a variety of other disorders, such as druginduced fever, sarcoidosis, and mercury poisoning.
20 Classical fever of unknown origine The most common infectious diseases diagnosed in this series were Epstein-Barr virus (EBV) infection (15%), Osteomyelitis (10%), Bartonellosis (5%), Urinary tract infections (4%).
21 Classical fever of unknown origine Elderly person : Classical FUO in patients older than 65 years is the relatively high frequency with which connective tissue diseases are identified as the cause of the illness In developed countries, connective tissue diseases surpass even infections as the leading cause of classical FUO in the elderly temporal arteritis polymyalgia rheumatica syndromes
22 Classical fever of unknown origine In elderly patients infections are identified as the cause of FUO, Intra-abdominal abscesses, Complicated urinary tract infections, Tuberculosis, Endocarditis
23 Classical fever of unknown origine DİAGNOSİS < 65 YEARS n: 152 > 65 YEARS n:201 Infections 72 (%35) 33 ( %21) Tumors 8 (%5) 37 (%19) Multisystem diseases 27 (%17) 57 (%28) Miscellaneous 39 (%26) 17 (% 8) No diagnosis 45 (%29) 18 (%9)
24 UNDİAGNOSED DİAGNOSİS Mac Lean et al n:587 Doherty et al n:195 Classical fever of unknown origin Malaria Hepatitis 6 3 Respiratory infections UTİ / Pyelonephritis Dysentry Dengue fever Enteric fever Tuberculosis 1 2 Rickettsial infections Acute HIV infection Amebic liver abscess 1 0 Other miscallenous infections Miscallenous noninfectious diseases 6 1
25 Classical fever of unknown origine Fever in returned travelers is most often due to common infections, such as Malaria Respiratory tract Infections Urinary tract infections
26 Health Care-Associated FUO Health care associated FUO is a condition in which patients first manifest fever during active medical treatment for some other illness. Such FUO cases are frequently attributable to risk factors encountered in the health care environment, Surgical procedures Urinary and Respiratory tract instrumentation Intravascular devices Drug therapy Immobilization
27 Immune-Deficient FUO Various forms of immunosuppression predispose more or less strongly to a wide variety of infectious complications. Thus, immunosuppressed patients have perhaps the highest incidence of FUO of any group of patients.
28 Immune-Deficient FUO In patients with impaired cell-mediated immunity, FUO is often due to : Infections % 58 Non-infectious %25 Undetermined % 17
29 Immune-Deficient FUO Neutropenic FUO : Neutropenia is a dangerous condition that can be considered a special subclass of immunodeficiency. The number of patients with episodes of neutropenia resulting from Cytotoxic therapy Malignancies affecting the bone marrow
30 Immune-Deficient FUO Episodes of fever are common in patients with neutropenia. Many such episodes are short-lived, because either respond quickly to treatment or rapidly fatal infections.
31 Immune-Deficient FUO Bacteremia and sepsis are frequent causes, empirical broad-spectrum antibiotics should be administered promptly, without waiting for the results of cultures, when fever develops in neutropenic patients. However, only about 35% of prolonged episodes of febrile neutropenia respond to broad-spectrum antibiotic therapy.
32 Immune-Deficient FUO If fever does not respond promptly to antibacterial therapy, fungal infection must be responsible, other causes are equally likely to be identified Resistant bacterial infections Tuberculosis, Toxoplasma gondii Greft-Versus-Host disease Drug fever Toxic effect of chemotherapy
33 HIV- Related FUO The primary phase of HIV infection is characterized by a mononucleosis-like illness in which fever is a prominent feature. Once symptoms of the primary phase of the HIV infection resolve, HIV-infected patients enter a long period of subclinical infection during which they are usually afebrile
34 HIV- Related FUO However, in the later phases of untreated HIV infection, episodes of fever become common, often signifying a superimposed illness. Many of these are potentially devastating opportunistic infections
35 Clinical Evaluation of FUO The evaluation of a patient with FUO typically includes : comprehensive history, verification that the patient actually has fever, consideration of the fever pattern, repeated physical examinations, every day laboratory investigations, imaging studies, invasive diagnostic procedures
36 Clinical Evaluation of FUO/ History History is a cornerstone of the evaluation of FUO. The history can be especially important in determining the choice of the initial laboratory investigations. Particular attention should be given to : recent travel, exposure to pets and other animals, the work environment, recent contact with people exhibiting similar symptoms. family history (FMF) past medical history (lymphoma, rheumatic fever, intraabdominal disorders) obtained medications
37 Clinical Evaluation of FUO/ Fever Next step is to verify the presence of fever. In fact, in a series of 347 patients admitted to the National Institutes of Health for investigation of prolonged fever, 35% were ultimately determined either not to have significant fever at all, or to have fever of factitious origin.
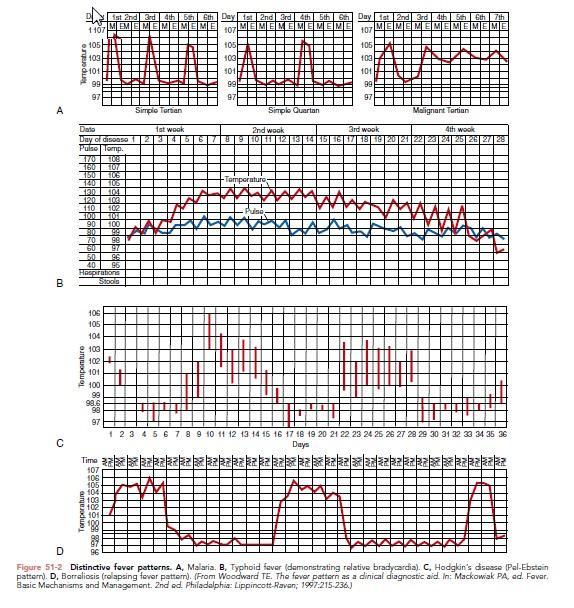
38 Clinical Evaluation of FUO/ Fever Febris continue Febris recurrens Intermittent (Hectic) Febris undulens (Pel - Ebstein) Remittent Subfebril fever

39
40
41 Clinical Evaluation of FUO/ Fever Pulse-temperature disassociation sometimes seen in typhoid fever, atypic pneumoniae 1 degree elevated fever, resulted with elevated 20 heart beats
42 Clinical Evaluation of FUO/ physical examination Frequently, key physical abnormalities in patients with FUO are so subtle as to require repeated examinations to be appreciated. Examples include the nodular or weakly pulsatile temporal artery of temporal arteritis, oral ulcers of disseminated histoplasmosis or Behçet s syndrome, choroid granuloma or epididymal nodule of extrapulmonary tuberculosis, the testicular nodule of polyarteritis nodosa, Rectal fluctuance of a perirectal abscess.
43 Clinical Evaluation of FUO/ physical BODY SITE PHYSICAL FINDING DIAGNOSIS examination HEAD Sinus tenderness Sinusitis TEMPORAL ARTERY Nodules,reduced pulsation Temporal arteritis OROPHARYNX FUNDUS CONJUNCTİVA Ulceration Tender tooth Choroid Tubercule Petechiaei,Roth spot s Histoplasmotosis Periapical abscees THYROİD Enlargment,tenderness Thyroiditis Dissemine granulomatosis Endocarditis HEART Murmur Infective endocarditis ABDOMEN LAP, Splenomegaly Lymphoma,endocarditis, Dissemine granulomatosis RECTUM Perirectal fluctuance Abscess GENİTALİA Testicular nodule Epididymal nodule Periarteritis nodosa Dissemine granulomatosis LOWER EXTREMİTİES Deep venous tenderness Thrombosis,thromboflebitis SKİN AND NAİLS Petechiae, clubbing, splinter hemorhages, subcutaneous nodule Vasculitis, endocarditis
44 Clinical Evaluation of FUO/ Laboratory Investigations In most series, noninvasive laboratory tests have yielded the diagnosis in approximately a quarter of the cases. The most useful of these serologic tests blood smears microbial culture
45 Clinical Evaluation of FUO/ Laboratory Investigations Bone marrow examination should be considered for diagnosis of suspected granulomatous diseases Tuberculosis, Histoplasmosis, Sarcoidosis, Carcinomatosis Hemophagocytic syndrome
46 Clinical Evaluation of FUO/ Laboratory Investigations Ultrasound imaging (USG) Computed tomography imaging(ct) Magnetic resonans imaging (MR) Scanning with labeled autologous leukocytes Gallium 67 scanning Positron emission tomography (PET)
47 Clinical Evaluation of FUO/Invasive Diagnostic Procedures Histopathologic examination of tissues obtained by Excisional biopsy, Needle biopsy, Laparoscopy Laparotomy, But in most published series of FUO patients, biopsy gave the final answer in less than half.
48 Clinical Evaluation of FUO/Invasive Diagnostic Procedures The diagnostic yield of operative and CTguided biopsies is higher than that of old-style bedside biopsy procedures. For this reason, bedside biopsies should rarely be performed todaytoday
49 Clinical Evaluation of FUO/Invasive Diagnostic Procedures Exploratory laparotomy, once a prominent procedure in the workup of FUO, is rarely performed today, unless localized abdominal physical signs or imaging findings, or both, are present. This is because few abdominal anatomic abnormalities are currently missed by CT scanning or MRI, vasculitis, polyarteritis nodosa, granulomatous disease, chronic cholecystitis
50
51 Therapeutic Trials of FUO In the past, empirical therapy with antiinflammatory agents, such as corticosteroids, aspirin, antimicrobial agents, In rare cases, even antineoplastic drugs were used for this purpose. Today such trials are seldom indicated.
52 Therapeutic Trials of FUO The limitations and risks of empirical therapeutic trials are obvious. Underlying diseases may remit spontaneously during the course of ineffective therapy, giving the false impression of success. Furthermore, empirical treatment is rarely specific. Rifampin, for example, is likely to be included in empirical therapeutic regimens for tuberculosis, but is highly active against numerous bacterial species other than Mycobacterium tuberculosis.
53 Therapeutic Trials of FUO Similarly, fevers caused by malignant neoplasms have been reported to respond better to nonsteroidal anti-inflammatory agents such as naproxen than fevers of infectious origin, but the action of naproxen is nonspecific; the ability of the so-called naproxen test to differentiate malignant from nonmalignant causes of FUO remains unvalidated.
54 Therapeutic Trials of FUO For these reasons, therapeutic trials, even when successful in reducing fever, may delay the correct diagnosis and thus the appropriate treatment of FUO.
55 Management A fundamental principle in the management of classical FUO is that therapy should be withheld, whenever possible, until the cause of the fever has been determined, so that treatment can be tailored to a specific diagnosis. In febrile neutropenic patients, the principles of treatment are entirely different. Neutropenic patients should generally receive broad-spectrum antimicrobial therapy immediately after samples for appropriate cultures have been obtained
56 Prognosis Elderly patients with malignant neoplasms have the poorest prognosis. Diagnostic delay affects the prognosis adversely in intra-abdominal infections, miliary tuberculosis, disseminated fungal infections, recurrent pulmonary emboli
57 General diagnostic evaluation of patients with FUO Comprehensive history Repeated physical examinations Complete blood count Routine blood chemistry determinations Urinalysis, including microscopic examination Chest radiograph Erythrocyte sedimentation rate Antinuclear antibodies Rheumatoid factor Blood cultures: three or more separate specimens obtained in absence of antimicrobial therapy Cytomegalovirus IgM antibodies or viral detection in blood Heterophile antibody test in children and young adults Tuberculin skin test Computed tomography of abdomen, pelvis, or other sites Magnetic resonance imaging Radionuclide scans Human immunodeficiency virus antibodies or viral detection assay Further evaluation of any abnormality detected by above tests Venous duplex imaging of lower limbs

58
FEVER OF UNKNOWN ORIGIN. Cristian Baicus Internal Medicine, Colentina Hospital
 FEVER OF UNKNOWN ORIGIN Cristian Baicus Internal Medicine, Colentina Hospital www.baicus.ro 1961 definition 1. Ilness> 3 weeks 2. Fever>38.3 C (>101 F), on several occasions 3. Diagnosis uncertain after
FEVER OF UNKNOWN ORIGIN Cristian Baicus Internal Medicine, Colentina Hospital www.baicus.ro 1961 definition 1. Ilness> 3 weeks 2. Fever>38.3 C (>101 F), on several occasions 3. Diagnosis uncertain after
Vasculitis and Vasculitides. OMONDI OYOO Physician/Rheumatologist; Senior Lecturer, Department of Medicine University of Nairobi
 Vasculitis and Vasculitides OMONDI OYOO Physician/Rheumatologist; Senior Lecturer, Department of Medicine University of Nairobi Definition Presence of leucocytes in the vessel wall with reactive damage
Vasculitis and Vasculitides OMONDI OYOO Physician/Rheumatologist; Senior Lecturer, Department of Medicine University of Nairobi Definition Presence of leucocytes in the vessel wall with reactive damage
NUCLEAR MEDICINE IMAGING IN FUO
 NUCLEAR MEDICINE IMAGING IN FUO Christophe Van de Wiele, M.D., Ph.D. Department of Nuclear Medicine, University Hospital, Ghent, Belgium NUCLEAR MEDICINE IMAGING IN FUO Definitions and classifications
NUCLEAR MEDICINE IMAGING IN FUO Christophe Van de Wiele, M.D., Ph.D. Department of Nuclear Medicine, University Hospital, Ghent, Belgium NUCLEAR MEDICINE IMAGING IN FUO Definitions and classifications
Mohammad Reza Shakibi M.D Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward
 Shafa Hospital, Rheumatology ward") VASCULITIS SYNDROMES Mohammad Reza Shakibi M.D Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward ILLUSTRATED CASE 1 A 56 years old lady refered me for prolonged fever, arthritis
VASCULITIS SYNDROMES Mohammad Reza Shakibi M.D Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward ILLUSTRATED CASE 1 A 56 years old lady refered me for prolonged fever, arthritis
CHAPTER 11 FEVER. Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University
 CHAPTER 11 FEVER Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University DEFINITION OF FEVER Fever is an elevation of body temperature that exceeds the normal daily variation,
CHAPTER 11 FEVER Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University DEFINITION OF FEVER Fever is an elevation of body temperature that exceeds the normal daily variation,
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
 MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
Atlas of the Vasculitic Syndromes
 CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
Diagnostic approach to fever of unknown origin. Steven Vanderschueren General Internal Medicine University Hospitals Leuven Belgium
 Diagnostic approach to fever of unknown origin Steven Vanderschueren General Internal Medicine University Hospitals Leuven Belgium FUO A Case Definitions Causes Diagnostic Approach Prognosis Conclusion
Diagnostic approach to fever of unknown origin Steven Vanderschueren General Internal Medicine University Hospitals Leuven Belgium FUO A Case Definitions Causes Diagnostic Approach Prognosis Conclusion
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Pathomechanism of fever. Fever of unknown origin. Fever and rash
 Pathomechanism of fever. Fever of unknown origin. Fever and rash Dr. Szathmári Miklós Semmelweis University 1st Department of Medicine 11 April 2014. Regulation of body temperature Controlled by the hypothalamus
Pathomechanism of fever. Fever of unknown origin. Fever and rash Dr. Szathmári Miklós Semmelweis University 1st Department of Medicine 11 April 2014. Regulation of body temperature Controlled by the hypothalamus
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acalculous cholecystitis, postoperative, 190 191 Acute cardiac failure, hypoxic liver injury and, in critically ill and postoperative patients,
Note: Page numbers of article titles are in boldface type. A Acalculous cholecystitis, postoperative, 190 191 Acute cardiac failure, hypoxic liver injury and, in critically ill and postoperative patients,
GOALS AND OBJECTIVES INFECTIOUS DISEASE
 GOALS AND OBJECTIVES INFECTIOUS DISEASE Infectious Disease and HIV Overview: The Infectious Diseases Program at the University of Southern California prepares trainees for the management of problems in
GOALS AND OBJECTIVES INFECTIOUS DISEASE Infectious Disease and HIV Overview: The Infectious Diseases Program at the University of Southern California prepares trainees for the management of problems in
Scottish Surveillance of Healthcare Associated Infection Programme (SSHAIP) Health Protection Scotland (HPS) SSI Surveillance Protocol 7th Edition
 Health Protection Scotland (HPS) SSI Surveillance Protocol 7th Edition") 1 Contents Female reproductive system operations (Abdominal hysterectomy and Caesarean section)... 3 Intra-abdominal infections... 3 Endometritis... 4 Other infections of the female reproductive tract...
1 Contents Female reproductive system operations (Abdominal hysterectomy and Caesarean section)... 3 Intra-abdominal infections... 3 Endometritis... 4 Other infections of the female reproductive tract...
Fever in Lupus. 21 st April 2014
 Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
The Naproxen Test as a Diagnostic Tool in the Causative Differentiation of Fever
 The Naproxen Test as a Diagnostic Tool in the Causative Differentiation of Fever Emmanuel Edwin R. Dy, M.D.,* Patrick Gerard L. Moral, M.D.** and Sandra Teresa G. Victorio-Navarra, M.D.*** (*Fellow, Section
The Naproxen Test as a Diagnostic Tool in the Causative Differentiation of Fever Emmanuel Edwin R. Dy, M.D.,* Patrick Gerard L. Moral, M.D.** and Sandra Teresa G. Victorio-Navarra, M.D.*** (*Fellow, Section
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
Lahey Clinic Internal Medicine Residency Program: Curriculum for Infectious Disease
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Infectious Disease Faculty representative: Eva Piessens, MD, MPH Resident representative: Karen Ganz, MD Revision date: February 1, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Infectious Disease Faculty representative: Eva Piessens, MD, MPH Resident representative: Karen Ganz, MD Revision date: February 1, 2006
PAEDIATRIC Point Prevalence Survey. Ward Form
 Appendix 1 PAEDIATRIC Point Prevalence Survey Ward Form Please fill in one form for each ward included in PPS Date of survey Person completing form (Auditor code) Hospital Name Department/Ward Paediatric
Appendix 1 PAEDIATRIC Point Prevalence Survey Ward Form Please fill in one form for each ward included in PPS Date of survey Person completing form (Auditor code) Hospital Name Department/Ward Paediatric
Dr Rodney Itaki Lecturer Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology
 Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Internal Medicine End of Rotation
 Internal Medicine End of Rotation EXAM TOPIC LIST CARDIOVASCULAR Angina pectoris Cardiac arrhythmias/conduction disorders Cardiomyopathy Congestive heart failure Coronary vascular disease Endocarditis
Internal Medicine End of Rotation EXAM TOPIC LIST CARDIOVASCULAR Angina pectoris Cardiac arrhythmias/conduction disorders Cardiomyopathy Congestive heart failure Coronary vascular disease Endocarditis
APPROACH TO FEVER OF UNKNOWN ORIGIN IN CHILDREN
 APPROACH TO FEVER OF UNKNOWN ORIGIN IN CHILDREN Adriana ONDRUŠOVÁ Faculty of Healthcare, Alexander Dubček University of Trenčín, Študentská 2, 911 50 Trenčín, Slovak Republic Abstract Fever is a common
APPROACH TO FEVER OF UNKNOWN ORIGIN IN CHILDREN Adriana ONDRUŠOVÁ Faculty of Healthcare, Alexander Dubček University of Trenčín, Študentská 2, 911 50 Trenčín, Slovak Republic Abstract Fever is a common
HELPING YOU AND YOUR PATIENTS TALK OPENLY ABOUT MODERATELY TO SEVERELY ACTIVE RA
 SIMPONI ARIA (golimumab) is indicated for the treatment of adults with moderately to severely active rheumatoid arthritis (RA) in combination with MTX, active psoriatic arthritis, and active ankylosing
SIMPONI ARIA (golimumab) is indicated for the treatment of adults with moderately to severely active rheumatoid arthritis (RA) in combination with MTX, active psoriatic arthritis, and active ankylosing
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
Role of imaging (images) in my practice. Dr P Senthur Nambi Consultant Infectious Diseases
 in my practice. Dr P Senthur Nambi Consultant Infectious Diseases") Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Role of imaging (images) in my practice Dr P Senthur Nambi Consultant Infectious Diseases Medical images: My thoughts Images are just images Subject to the intellect of the interpreter View it in conjuction
Vasculitides in Surgical Neuropathology Practice
 Vasculitides in Surgical Neuropathology Practice USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Vasculitides in Surgical Neuropathology Practice USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Lemuel Shattuck Hospital Consultation Service
 Lemuel Shattuck Hospital Consultation Service a) Goals, Objectives, and ACGME Competencies Goals Learn how to manage complicated infectious disease problems in a public health setting. Learn how to provide
Lemuel Shattuck Hospital Consultation Service a) Goals, Objectives, and ACGME Competencies Goals Learn how to manage complicated infectious disease problems in a public health setting. Learn how to provide
Case Presentation VASCULITIS. Case Presentation. Case Presentation. Vasculitis
 Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Contents. 3 Diagnostic Tests and Studies Introduction Examination... 27
 Contents 1 Normal Anatomy... 1 1.1 Introduction... 1 1.2 Surface Landmarks... 1 1.3 Oral Mucosa... 3 1.4 Tongue... 5 1.5 Floor of Mouth... 6 1.6 Palate... 6 1.7 Dentition... 7 1.8 Temporomandibular Joint...
Contents 1 Normal Anatomy... 1 1.1 Introduction... 1 1.2 Surface Landmarks... 1 1.3 Oral Mucosa... 3 1.4 Tongue... 5 1.5 Floor of Mouth... 6 1.6 Palate... 6 1.7 Dentition... 7 1.8 Temporomandibular Joint...
INDEX NEUROLOGIC MANIFESTATIONS OF SYSTEMIC DISEASE. Note: Page numbers of article titles are in boldface type.
 NEUROLOGIC MANIFESTATIONS OF SYSTEMIC DISEASE INDEX Note: Page numbers of article titles are in boldface type. Abuse, drug, CNS vasculopathy and, 130 131 Acromegaly, 46 48 causes of, 46 47 clinical presentation
NEUROLOGIC MANIFESTATIONS OF SYSTEMIC DISEASE INDEX Note: Page numbers of article titles are in boldface type. Abuse, drug, CNS vasculopathy and, 130 131 Acromegaly, 46 48 causes of, 46 47 clinical presentation
Rayos Prior Authorization Program Summary
 Rayos Prior Authorization Program Summary FDA APPROVED INDICATIONS AND DOSAGE FDA-Approved Indications: 1 Agent Indication Dosage Rayos (prednisone delayedrelease tablet) as an anti-inflammatory or immunosuppressive
Rayos Prior Authorization Program Summary FDA APPROVED INDICATIONS AND DOSAGE FDA-Approved Indications: 1 Agent Indication Dosage Rayos (prednisone delayedrelease tablet) as an anti-inflammatory or immunosuppressive
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Vasculitis. Edward Dwyer, M.D. Division of Rheumatology. Vasculitis
 Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
VASCULITIS. Case Presentation. Case Presentation
 VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
IS IT INFECTIOUS OR IMMUNE-MEDIATED: APPROACH TO FEVER OF UNDETERMINED ORIGIN
 IS IT INFETIOUS OR IMMUNE-MEIATE: APPROAH TO FEVER OF UNETERMINE ORIGIN. Guillermo outo, VM, ip. AVIM outo Veterinary onsultants Hilliard, OH 43026 coutovetconsultants@gmail.com www.coutovetconsultants.com
IS IT INFETIOUS OR IMMUNE-MEIATE: APPROAH TO FEVER OF UNETERMINE ORIGIN. Guillermo outo, VM, ip. AVIM outo Veterinary onsultants Hilliard, OH 43026 coutovetconsultants@gmail.com www.coutovetconsultants.com
ORIGINAL INVESTIGATION. From Prolonged Febrile Illness to Fever of Unknown Origin
 From Prolonged Febrile Illness to Fever of Unknown Origin The Challenge Continues ORIGINAL INVESTIGATION Steven Vanderschueren, MD, PhD; Daniël Knockaert, MD, PhD; Tom Adriaenssens, MD; Wim Demey, MD;
From Prolonged Febrile Illness to Fever of Unknown Origin The Challenge Continues ORIGINAL INVESTIGATION Steven Vanderschueren, MD, PhD; Daniël Knockaert, MD, PhD; Tom Adriaenssens, MD; Wim Demey, MD;
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Cimzia (certolizumab pegol) Data Showed Broad and Rapid Relief From Burden of Symptoms In Rheumatoid Arthritis Patients
 Data Showed Broad and Rapid Relief From Burden of Symptoms In Rheumatoid Arthritis Patients") Cimzia (certolizumab pegol) Data Showed Broad and Rapid Relief From Burden of Symptoms In Rheumatoid Arthritis Patients Rapid, sustained and clinically meaningful improvement in wideranging patient-reported
Cimzia (certolizumab pegol) Data Showed Broad and Rapid Relief From Burden of Symptoms In Rheumatoid Arthritis Patients Rapid, sustained and clinically meaningful improvement in wideranging patient-reported
Form 2033 R3.0: Wiskott-Aldrich Syndrome Pre-HSCT Data
 Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Has this patient's data been previously reported to USIDNET? USIDNET ID: Today's Date: - - Date of HSCT for which
Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Has this patient's data been previously reported to USIDNET? USIDNET ID: Today's Date: - - Date of HSCT for which
Clinical Aspect and Application of Laboratory Test in Herpes Virus Infection. Masoud Mardani M.D,FIDSA
 Clinical Aspect and Application of Laboratory Test in Herpes Virus Infection Masoud Mardani M.D,FIDSA Shahidhid Bh BeheshtiMdi Medical lui Universityit Cytomegalovirus (CMV), Epstein Barr Virus(EBV), Herpes
Clinical Aspect and Application of Laboratory Test in Herpes Virus Infection Masoud Mardani M.D,FIDSA Shahidhid Bh BeheshtiMdi Medical lui Universityit Cytomegalovirus (CMV), Epstein Barr Virus(EBV), Herpes
GIANT CELL ARTERITIS. Page 1 of 6 Reproduction of this material requires written permission of the Vasculitis Foundation. Copyright 2018.
 What is giant cell arteritis (GCA)? Giant cell arteritis (GCA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
What is giant cell arteritis (GCA)? Giant cell arteritis (GCA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
The EM Educator Series
 The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
Index. B Biological factors, 2 Brain stem encephalitis, Burkitt s lymphoma, 83, 105
 Index A Acquired immunodeficiency syndrome (AIDS) abdomen gallbladder complications, 97, 107 109 gastrointestinal complications, 96, 105 106 liver complications, 97, 107 109 neoplasm, 99, 110 111 pancreas
Index A Acquired immunodeficiency syndrome (AIDS) abdomen gallbladder complications, 97, 107 109 gastrointestinal complications, 96, 105 106 liver complications, 97, 107 109 neoplasm, 99, 110 111 pancreas
Emerging Infections. David V. Condoluci, DO.,F.A.C.O.I.
 Emerging Infections David V. Condoluci, DO.,F.A.C.O.I. Declaratives I have no conflicts of interest. I do not speak for any companies I have no grants other than Ryan White and AETC from the federal government
Emerging Infections David V. Condoluci, DO.,F.A.C.O.I. Declaratives I have no conflicts of interest. I do not speak for any companies I have no grants other than Ryan White and AETC from the federal government
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
There are two main causes of a low platelet count
 Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
What prescribers need to know
 HUMIRA Citrate-free presentations in an Electronic Medical Record (EMR) What prescribers need to know 2 / This is your guide to identifying HUMIRA Citrate-free presentations in your Electronic Medical
HUMIRA Citrate-free presentations in an Electronic Medical Record (EMR) What prescribers need to know 2 / This is your guide to identifying HUMIRA Citrate-free presentations in your Electronic Medical
ESCMID Online Lecture Library. by author
 Therapies or diseases predisposing to infection Congenital immunodeficiences Acquired conditions Common variable immunedeficiency particular diseases (e.g. HIV, cancer,leukemia, lymphoma, diabetes, cystic
Therapies or diseases predisposing to infection Congenital immunodeficiences Acquired conditions Common variable immunedeficiency particular diseases (e.g. HIV, cancer,leukemia, lymphoma, diabetes, cystic
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Interstitial syndrome
 Interstitial syndrome Ground-glass attenuation Miliary and nodular images linear images Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
Interstitial syndrome Ground-glass attenuation Miliary and nodular images linear images Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
InterQual Level of Care 2018 Index
 InterQual Level of Care 2018 Index Long-Term Acute Care (LTAC) Criteria The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where a specific
InterQual Level of Care 2018 Index Long-Term Acute Care (LTAC) Criteria The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where a specific
Announcing HUMIRA. Psoriasis Starter Package
 Announcing HUMIRA (adalimumab) Psoriasis Starter Package HUMIRA is indicated for the treatment of adult patients with moderate to severe chronic plaque psoriasis who are candidates for systemic therapy
Announcing HUMIRA (adalimumab) Psoriasis Starter Package HUMIRA is indicated for the treatment of adult patients with moderate to severe chronic plaque psoriasis who are candidates for systemic therapy
OSTEOMYELITIS. If it occurs in adults, then the axial skeleton is the usual site.
 OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
WISKOTT-ALDRICH SYNDROME. An X-linked Primary Immunodeficiency
 WISKOTT-ALDRICH SYNDROME An X-linked Primary Immunodeficiency WHAT IS WISKOTT ALDRICH SYNDROME? Wiskott-Aldrich Syndrome (WAS) is a serious medical condition that causes problems both with the immune system
WISKOTT-ALDRICH SYNDROME An X-linked Primary Immunodeficiency WHAT IS WISKOTT ALDRICH SYNDROME? Wiskott-Aldrich Syndrome (WAS) is a serious medical condition that causes problems both with the immune system
Internal Medicine Certification Examination Blueprint
 Internal Medicine Certification Examination Blueprint What Does the Examination Cover? The exam is designed to evaluate the extent of the candidate s knowledge and clinical judgment in the areas in which
Internal Medicine Certification Examination Blueprint What Does the Examination Cover? The exam is designed to evaluate the extent of the candidate s knowledge and clinical judgment in the areas in which
Resident, PGY1 David Geffen School of Medicine at UCLA. Los Angeles Society of Pathology Resident and Fellow Symposium 2013
 Resident, PGY1 David Geffen School of Medicine at UCLA Los Angeles Society of Pathology Resident and Fellow Symposium 2013 85 year old female with past medical history including paroxysmal atrial fibrillation,
Resident, PGY1 David Geffen School of Medicine at UCLA Los Angeles Society of Pathology Resident and Fellow Symposium 2013 85 year old female with past medical history including paroxysmal atrial fibrillation,
DRAFT. Remission rates, calculated using observed case (OC) analyses were as follows: Year 1 Year 2 Year 3 Year 4 All patients 62.
 analyses were as follows: Year 1 Year 2 Year 3 Year 4 All patients 62.") DRAFT New Efficacy Data Shows Cimzia (certolizumab pegol) Provides Long-Term Remission of Moderate to Severe Crohn s Disease Regardless of Prior Anti-TNF Exposure, According to Data Presented at DDW Oral
DRAFT New Efficacy Data Shows Cimzia (certolizumab pegol) Provides Long-Term Remission of Moderate to Severe Crohn s Disease Regardless of Prior Anti-TNF Exposure, According to Data Presented at DDW Oral
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Management of Immune Reconstitution Inflammatory Syndrome (IRIS)
") Management of Immune Reconstitution Inflammatory Syndrome (IRIS) Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the IRIS Guideline
Management of Immune Reconstitution Inflammatory Syndrome (IRIS) Adult Clinical Guideline from the New York State Department of Health AIDS Institute www.hivguidelines.org Purpose of the IRIS Guideline
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
A number of factors point to the likelihood of a person with RA developing RV:
 What is rheumatoid vasculitis (RV)? Rheumatoid vasculitis (RV) is a rare but serious complication of rheumatoid arthritis (RA) an inflammatory disease that causes severe joint pain and damage, and can
What is rheumatoid vasculitis (RV)? Rheumatoid vasculitis (RV) is a rare but serious complication of rheumatoid arthritis (RA) an inflammatory disease that causes severe joint pain and damage, and can
Supplementary Online Content
 Supplementary Online Content Lee C-C, Lee M-tG, Chen Y-S. Risk of aortic dissection and aortic aneurysm in patients taking oral fluoroquinolone. JAMA Internal Medicine. Published online October 5, 2015.
Supplementary Online Content Lee C-C, Lee M-tG, Chen Y-S. Risk of aortic dissection and aortic aneurysm in patients taking oral fluoroquinolone. JAMA Internal Medicine. Published online October 5, 2015.
Clinical cases and pitfalls using FDG-PET. François Jamar Université Catholique de Louvain, Brussels, Belgium
 Clinical cases and pitfalls using FDG-PET François Jamar Université Catholique de Louvain, Brussels, Belgium Case history (1) sepsis 60 yr old female Diabetes (1)- hypertension, alcohol Renal failure,
Clinical cases and pitfalls using FDG-PET François Jamar Université Catholique de Louvain, Brussels, Belgium Case history (1) sepsis 60 yr old female Diabetes (1)- hypertension, alcohol Renal failure,
Remicade (infliximab) DRUG.00002
 DRUG.00002") Applicability/Effective Date *- Florida Healthy Kids Remicade (infliximab) DRUG.00002 Override(s) Prior Authorization Step Therapy Medications Remicade (infliximab) Approval Duration 1 year Comment Intravenous
Applicability/Effective Date *- Florida Healthy Kids Remicade (infliximab) DRUG.00002 Override(s) Prior Authorization Step Therapy Medications Remicade (infliximab) Approval Duration 1 year Comment Intravenous
Fever of unknown origin
 Fever of unknown origin Case B History of the present illness 75 years old women presented at our hospital with since months daily fevers between 38 to 39.5 Celsius (100.4-103.1 F) with night sweats. Her
Fever of unknown origin Case B History of the present illness 75 years old women presented at our hospital with since months daily fevers between 38 to 39.5 Celsius (100.4-103.1 F) with night sweats. Her
Fever and rash in children. Haider Arishi MD Consultant, pediatrics and infectious diseases Director, infection control program
 Fever and rash in children Haider Arishi MD Consultant, pediatrics and infectious diseases Director, infection control program objectives To understand importance of fever and rash. To discuss the clinical
Fever and rash in children Haider Arishi MD Consultant, pediatrics and infectious diseases Director, infection control program objectives To understand importance of fever and rash. To discuss the clinical
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
Post Travel Fever. Dr. Eyal Leshem. Center for Geographic Medicine Sheba Medical Center Tel Hashomer, Israel
 Post Travel Fever Dr. Eyal Leshem Center for Geographic Medicine Sheba Medical Center Tel Hashomer, Israel Introduction Fever in returned traveler: Trivial vs. life threatening infections Tropical and
Post Travel Fever Dr. Eyal Leshem Center for Geographic Medicine Sheba Medical Center Tel Hashomer, Israel Introduction Fever in returned traveler: Trivial vs. life threatening infections Tropical and
Title: Author: Speciality / Division: Directorate:
 Antifungal guidelines for CANDIDIASIS INFECTIONS (Adults) Proven infection: Targeted antifungal therapy should be prescribed for: o Positive cultures from a sterile site with clinical or radiological abnormality
Antifungal guidelines for CANDIDIASIS INFECTIONS (Adults) Proven infection: Targeted antifungal therapy should be prescribed for: o Positive cultures from a sterile site with clinical or radiological abnormality
ST - segment Elevation Myocardial Infarction complicating an atypical Kawasaki disease
 ST - segment Elevation Myocardial Infarction complicating an atypical Kawasaki disease Raluca PRISECARU, Marc VINCENT, Steven VERCAUTEREN Brussels Heart Center, Brussels, Belgium Disclosure None Clinical
ST - segment Elevation Myocardial Infarction complicating an atypical Kawasaki disease Raluca PRISECARU, Marc VINCENT, Steven VERCAUTEREN Brussels Heart Center, Brussels, Belgium Disclosure None Clinical
Abscess. A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body.
 Abscess A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body. Ethyology Bacteria causing cutaneous abscesses are typically indigenous
Abscess A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body. Ethyology Bacteria causing cutaneous abscesses are typically indigenous
New Cimzia data, with sites in the US, demonstrate safety and efficacy, increased participation in social activities for adult RA patients
 Long-term Cimzia (certolizumab pegol) data demonstrated rapid sustained improvements in clinical outcomes and quality of life in moderate to severe rheumatoid arthritis (RA) patients New Cimzia data, with
Long-term Cimzia (certolizumab pegol) data demonstrated rapid sustained improvements in clinical outcomes and quality of life in moderate to severe rheumatoid arthritis (RA) patients New Cimzia data, with
2/23/18. Disclosures. Rheumatic Diseases of Childhood. Making Room for Rheumatology. I have nothing to disclose. James J.
 Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adaptive immune response biologic response modifiers and, 735 737 S-Adenosylmethionine (SAMe) for hepatitis, 825 826 Albinterferon for hepatitis,
Note: Page numbers of article titles are in boldface type. A Adaptive immune response biologic response modifiers and, 735 737 S-Adenosylmethionine (SAMe) for hepatitis, 825 826 Albinterferon for hepatitis,
EBV and Infectious Mononucleosis. Infectious Disease Definitions. Infectious Diseases
 Infectious Disease Definitions Infection when a microorganism invades a host and multiplies enough to disrupt normal function by causing signs and symptoms Pathogencity ability of an organism to cause
Infectious Disease Definitions Infection when a microorganism invades a host and multiplies enough to disrupt normal function by causing signs and symptoms Pathogencity ability of an organism to cause
Kawasaki Disease. 1:45 2:30 p.m. James Nocton, MD Benjamin Goot, MD. Children s Specialty Group. All rights reserved.
 Kawasaki Disease 1:45 2:30 p.m. James Nocton, MD Benjamin Goot, MD Disclosures We have no relevant financial relationships to disclose. Objectives Describe the characteristic signs and symptoms of Kawasaki
Kawasaki Disease 1:45 2:30 p.m. James Nocton, MD Benjamin Goot, MD Disclosures We have no relevant financial relationships to disclose. Objectives Describe the characteristic signs and symptoms of Kawasaki
lung, as evidenced on chest radiography. This pattern is seen in 1-3% of all TB cases.
 http://emedicine.medscape.com/article/221777-overview Miliary Tuberculosis uthor: Klaus-Dieter Lessnau, MD, FCCP; Chief Editor: Burke A Cunha, MD more... Sep 13, 2013 Updated: Sep 13, 2013 Overview of
http://emedicine.medscape.com/article/221777-overview Miliary Tuberculosis uthor: Klaus-Dieter Lessnau, MD, FCCP; Chief Editor: Burke A Cunha, MD more... Sep 13, 2013 Updated: Sep 13, 2013 Overview of
The Role of Invasive and Non-Invasive Procedures in Diagnosing Fever of Unknown Origin
 Ivyspring International Publisher Research Paper 682 International Journal of Medical Sciences 2012; 9(8):682-689. doi: 10.7150/ijms.4591 The Role of Invasive and Non-Invasive Procedures in Diagnosing
Ivyspring International Publisher Research Paper 682 International Journal of Medical Sciences 2012; 9(8):682-689. doi: 10.7150/ijms.4591 The Role of Invasive and Non-Invasive Procedures in Diagnosing
Scleritis LEN V KOH OD
 Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2
Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2
Infliximab/Infliximab-dyyb DRUG.00002
 Infliximab/Infliximab-dyyb DRUG.00002 Override(s) Prior Authorization Step Therapy Medications Remicade (infliximab) Inflectra (inflectra-dyyb) Approval Duration 1 year Comment Intravenous administration
Infliximab/Infliximab-dyyb DRUG.00002 Override(s) Prior Authorization Step Therapy Medications Remicade (infliximab) Inflectra (inflectra-dyyb) Approval Duration 1 year Comment Intravenous administration
REFERRAL GUIDELINES: RHEUMATOLOGY
 Outpatient Page 1 1 REFERRAL GUIDELINES: RHEUMATOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential Referral Content Referring
Outpatient Page 1 1 REFERRAL GUIDELINES: RHEUMATOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential Referral Content Referring
Heart on Fire: Infective Endocarditis. Objectives. Disclosure 8/27/2018. Mary McGreal DNP, RN, ANP-c, CCRN
 Heart on Fire: Infective Endocarditis Mary McGreal DNP, RN, ANP-c, CCRN Objectives Discuss the incidence of infective endocarditis? Discuss the pathogenesis of infective endocarditis? Discuss clinical
Heart on Fire: Infective Endocarditis Mary McGreal DNP, RN, ANP-c, CCRN Objectives Discuss the incidence of infective endocarditis? Discuss the pathogenesis of infective endocarditis? Discuss clinical
Inflectra (infliximab-dyyb), Remicade (infliximab), Renflexis (infliximab-abda) DRUG CG-DRUG-64
, Remicade (infliximab), Renflexis (infliximab-abda) DRUG CG-DRUG-64") Inflectra (infliximab-dyyb), Remicade (infliximab), Renflexis (infliximab-abda) DRUG.00002 CG-DRUG-64 Override(s) Prior Authorization *Washington Medicaid See State Specific Mandates Medications Inflectra
Inflectra (infliximab-dyyb), Remicade (infliximab), Renflexis (infliximab-abda) DRUG.00002 CG-DRUG-64 Override(s) Prior Authorization *Washington Medicaid See State Specific Mandates Medications Inflectra
number Done by Corrected by Doctor موسى العبادي
 number 12 Done by Corrected by Doctor موسى العبادي Morphology of Granulomatous Inflammations The first image (left) shows a lung alveolus in which necrosis is taking place. The image below it shows the
number 12 Done by Corrected by Doctor موسى العبادي Morphology of Granulomatous Inflammations The first image (left) shows a lung alveolus in which necrosis is taking place. The image below it shows the
December 3, 2015 Severe Sepsis and Septic Shock Antibiotic Guide
 Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Cerebral Toxoplasmosis in HIV-Infected Patients. Ahmed Saad,MD,FACP
 Cerebral Toxoplasmosis in HIV-Infected Patients Ahmed Saad,MD,FACP Introduction Toxoplasmosis: Caused by the intracellular protozoan, Toxoplasma gondii. Immunocompetent persons with primary infection
Cerebral Toxoplasmosis in HIV-Infected Patients Ahmed Saad,MD,FACP Introduction Toxoplasmosis: Caused by the intracellular protozoan, Toxoplasma gondii. Immunocompetent persons with primary infection
CENTRAL NERVOUS SYSTEM VASCULITIS
 What is central nervous system (CNS) vasculitis? Central nervous system (CNS) vasculitis is among a family of rare disorders characterized by inflammation of the blood vessels, which restricts blood flow
What is central nervous system (CNS) vasculitis? Central nervous system (CNS) vasculitis is among a family of rare disorders characterized by inflammation of the blood vessels, which restricts blood flow
Case Report Traumatic Haemorrhagic Cervical Lymphadenopathy with Underlying Infectious Mononucleosis
 Hindawi Case Reports in Radiology Volume 2017, Article ID 3097414, 4 pages https://doi.org/10.1155/2017/3097414 Case Report Traumatic Haemorrhagic Cervical Lymphadenopathy with Underlying Infectious Mononucleosis
Hindawi Case Reports in Radiology Volume 2017, Article ID 3097414, 4 pages https://doi.org/10.1155/2017/3097414 Case Report Traumatic Haemorrhagic Cervical Lymphadenopathy with Underlying Infectious Mononucleosis
Fever of Unknown Origin (FUO) Clinical Presentation. Author: Sandra G Gompf, MD, FACP, FIDSA; Chief Editor: Michael Stuart Bronze, MD
 Clinical Presentation. Author: Sandra G Gompf, MD, FACP, FIDSA; Chief Editor: Michael Stuart Bronze, MD") Updated: Mar 20, 2017 Fever of Unknown Origin (FUO) Clinical Presentation Author: Sandra G Gompf, MD, FACP, FIDSA; Chief Editor: Michael Stuart Bronze, MD Sandra G Gompf, MD, FACP, FIDSA Associate Professor
Updated: Mar 20, 2017 Fever of Unknown Origin (FUO) Clinical Presentation Author: Sandra G Gompf, MD, FACP, FIDSA; Chief Editor: Michael Stuart Bronze, MD Sandra G Gompf, MD, FACP, FIDSA Associate Professor
Present Status of Lab oratory Diagnosis o f Sarcoidosis
 A n n a l s o f C l i n i c a l L a b o r a t o r y S c i e n c e, Vol. 3, No. 2 Copyright 1 9 7 3, Institute for Clinical Science Present Status of Lab oratory Diagnosis o f Sarcoidosis HAROLD L. ISRAEL,
A n n a l s o f C l i n i c a l L a b o r a t o r y S c i e n c e, Vol. 3, No. 2 Copyright 1 9 7 3, Institute for Clinical Science Present Status of Lab oratory Diagnosis o f Sarcoidosis HAROLD L. ISRAEL,
PROPAEDEUTICS OF INTERNAL DISEASES EXAMINATION SYLLABUS. Part I - General
 PROPAEDEUTICS OF INTERNAL DISEASES EXAMINATION SYLLABUS Part I - General 1. History taking plan of history taking, sections, questions. 2. History taking - rules. 3. Current state of health - study plan.
PROPAEDEUTICS OF INTERNAL DISEASES EXAMINATION SYLLABUS Part I - General 1. History taking plan of history taking, sections, questions. 2. History taking - rules. 3. Current state of health - study plan.
Evaluation of Neck Mass. Disclosure. Learning Objectives 3/24/2014. Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ. Nothing to disclose
 Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Does this child have fever > 7 days with no obvious source despite in depth investigation?
 1 Does this child have fever > 7 days with no obvious source despite in depth investigation? Stabilise toxic/septic looking child using resuscitation guidelines, call for senior help YES YES Is this child
1 Does this child have fever > 7 days with no obvious source despite in depth investigation? Stabilise toxic/septic looking child using resuscitation guidelines, call for senior help YES YES Is this child
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
ACCME/Disclosures. Two Patients and a Caveat 4/13/2016. Patient #1: 13 y/o boy with IPEX syndrome; s/p BMT
 Two Patients and a Caveat The Use and Misuse of Molecular Methods in Mycobacterial Infections Gary W. Procop, MD Director, Molecular Microbiology Infectious Disease Pathologist Cleveland Clinic ACCME/Disclosures
Two Patients and a Caveat The Use and Misuse of Molecular Methods in Mycobacterial Infections Gary W. Procop, MD Director, Molecular Microbiology Infectious Disease Pathologist Cleveland Clinic ACCME/Disclosures
I-Brite - Ocular/Medical/General Information
 I-Brite - Ocular/Medical/General Information Na me Date Gender (First) (Middle) (Last) Date of Birth Age Occupation Phone No. Address City State Zip Please describe what is abnormal about the appearance
I-Brite - Ocular/Medical/General Information Na me Date Gender (First) (Middle) (Last) Date of Birth Age Occupation Phone No. Address City State Zip Please describe what is abnormal about the appearance
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
CUMULATIVE ILLNESS RATING SCALE (CIRS)
") CUMULATIVE ILLNESS RATING SCALE (CIRS) The CIRS used in this protocol is designed to provide an assessment of recurrent or ongoing chronic comorbid conditions, classified by 14 organ systems. Using the
CUMULATIVE ILLNESS RATING SCALE (CIRS) The CIRS used in this protocol is designed to provide an assessment of recurrent or ongoing chronic comorbid conditions, classified by 14 organ systems. Using the
Luke Droney IMMUNOGLOBULIN LEVELS AND FUNCTION
 IMMUNOGLOBULIN LEVELS AND FUNCTION Interpret changes in immunoglobulin levels within the clinical context including - Immunodeficiency - Disorders characterised by hypergammaglobulinaemia, rheumatoid arthritis,
IMMUNOGLOBULIN LEVELS AND FUNCTION Interpret changes in immunoglobulin levels within the clinical context including - Immunodeficiency - Disorders characterised by hypergammaglobulinaemia, rheumatoid arthritis,