Interstitial syndrome
|
|
|
- Coleen Jewel Green
- 5 years ago
- Views:
Transcription

1 Interstitial syndrome Ground-glass attenuation Miliary and nodular images linear images Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology


2 Acinus and primary lobule 1Terminal bronchiol; 2,3,4. respiratory bronchioli (BR1, BR2, BR3); 5. alveolar canal; 6. alveola sac; 7. alveola. There are 14 divisions between the trachea and terminal bronchiol Lobule: morphological unit. Dimension: 10 to 25 mm. It is composed of 3 to 5 acini (functional unit) (7.5 mm); 30 to 50 primary lobules (0.5 to 1 mm). 1 et 1'.centrolobular Bronchiol and artery; 2. terminal bronchiol and artery; 3. respiratory bronchiol; 4. canal; 5. sac; 6. alveolar; 7.perilobular vena and lymphatic vessels.
3 Under-pleural tissue The different parts of intersticial tissue: Intra-lobular tissue Peri-lobular tissue Under-pleural tissue Axial tissue Axial or peri-broncho vascular tissue Peri-lobular tissue (according to Dr. Bernadac) Intra-lobular tissue
4 Under-pleural tissue The different parts of interstitial tissue: Intra-lobular Axial tissue (according to Pr. Bernadac ) Peri-lobular tissue Intra-lobular tissue
5 Intra-lobular interstitial tissue images: -Ground glass attenuation -Miliary: micronodules <3mm -Nodules: between 3 and 7 mm -Macronodules > 7mm


6 Ground glass attenuation Normal chest X ray Easy to recognise on scanner, it is more difficult on CXR
7 Ground glass attenuation Main etiologies: Cardiac failure (initial phase before alveolar oedema) Viral or atypical bacterial infections Lyphoma, haemopatologic malignancies. Pneumocystosis

8 Pneumocystosis: one of the main opportunistic lung diseases in AIDS cases

9 Ground glass attenuation: pneumocystosis
10 Man, HIV+ severe dyspnea, normal auscultation, Sa02 86 % It is a pneumocystosis. CXR features in acute phase: Ground glass attenuation and or alveolar pictures Diffuse and bilateral picture No retraction, no systematisation


11 1 2 3 Improvment after 3 weeks of treatment with cotrimoxazole.


12


13 Miliary: diffuse micronodules < 3mm Normal CXR Easy to recognise on scanner, it is more difficult on CXR

14 It can be difficult to distinguish miliary from ground glass attenuation




15 miliary Ground glass attenuation


16 Miliary is sometimes barely visible

17 And sometimes the diagnosis is obvious


18 AFB+ in bronchial aspiration. Note the assymetry of the miliary M, 68 y African, t 40 C, weight loss, dyspnea, miliary left predominant, AFB negative in sputum



19 M, 25 years old Non-productive cough T 39 C Dyspnea with effort AFB in sputum Miliary. Improvement with anti-tb treatment


20 Man, 30 years old, non-smoker, dyspnea and cough progressively increasing. 2 chest x-ray with 2-month interval. AFB - In countries with high incidence, TB is the most probable diagnosis, But it could be also a sarcoïdosis


21



22 Man, 53 years old, refugee from mauritania. Cough and worsening condition. AFB neg.. Headache (notice the unequal size of nodules which is unusual in TB miliary)



23 Previous case: carcinomatous miliary with metastatic adenopathies, bone and brain metastasis


24 Woman, 20y HIV+ Cough, dyspnea, t 38 5C Miliary AFB - BAL: Histoplasmosis
 in case of TB AFB in sputum is usually negative The primary diagnosis is TB Main")
 sarcoidosis (incidence in your countries?")
25 Diagnostic of miliary : Requires an excellent quality CXR and very attentive analysis by the physician Negatoscope Pictures often barely visible, in contrast with the importance of general signs (asthenia, dyspnea, fever, weight loss) in case of TB AFB in sputum is usually negative The primary diagnosis is TB Main differential diagnosis (miliary and nodules<7mm) are: fungal infection, particularly in cases of AIDS, (histoplasmosis, cryptococcosis,...) sarcoidosis (incidence in your countries?) carcinomatosis miliary pneumoconiosis (probably frequent in your countries / Mines) auto-immune affection, haemotologic malignancies, immuno-allergic pneumopathy
26 In countries with high incidence of TB and HIV, If X-ray shows miliary pattern - First diagnostic suspect is TB - If not clinical response after 3 weeks of treatment, in PLHIV, consider adding anti-fungal treatment - BUT DO NOT INTERRUPT TB TREATMENT! - Among PLHIV, If severe clinical picture with X-ray ground glass attenuation picture and hypoxemia, consider PCP and start treatment
27 Nodules
28 Main etiologies of diffused nodules>7mm Tuberculosis Pulmonary metastasis Less frequent etiologies: silicosis sarcoidosis lymphoma fungal infection multiple abcesses by septic emboly hydatid cyst bronchiolo-alveolar cancer and multiple bronchial cancers vascularitis, Wegener, auti-immune disease, histiocytosis

29 Man, 55 years old Antecedent of left pleural effusion Hemoptoic sputum AFB+



30 Notice the excavation. This explains why this patient is AFB positive


31 Woman 55 years old, cough and dyspnea with effort. Tobacco >1pack/ day

32 Bronchial adenocarcinoma with lung metastis

33 Bronchial carcinoma with carcinomatous miliary

34 Lung metastasis ( uterus leiomyosarcoma)

35 Man, 65 years old, Asthenia, no respiratory symptoms except light cough. Antecedent of rectal cancer treated by surgery

36 Chest radio 6 months later

37 Balloon release: pulmonary metastasis of rectum cancer

38 Silicosis in an older mineworker


39 Silicosis in an older mineworker
40 Under-pleural tissue The different parts of intesticial tissue: Under-pleural tissue Axial tissue Peri-lobular tissue ( according to Pr. Bernadac ) Intra-lobular tissue


41 The pathology of under-pleural tissue is characterized by linear images called Kerley A or B lines. Kerley B lines Kerley A lines
42 Kerley lines: main etiologies Cardiac failure (B kerley lines) Viral infections Less frequent: - carcinomatous lymphangitis - Fibrosis, regardless of the etiology (toxic, auto-immune, allergic, idiopathic..) - pneumoconiosis - haemopathy -
43 Under-pleural tissue The different parts of intersticial tissue: Peri-lobular tissue Axial tissue ( according to Pr. Bernadac ) Peri-lobular tissue Intra-lobular tissue



44 The increasing thickness of the peri-lobular septa and their intersection produce reticular opacities which line polyedric spaces: «Meshed net» aspect. The main etiology is pulmonary fibrosis, regardless of the etiology ( idiopathic, toxic, autoimmun )


45 Idiopathic fibrosis
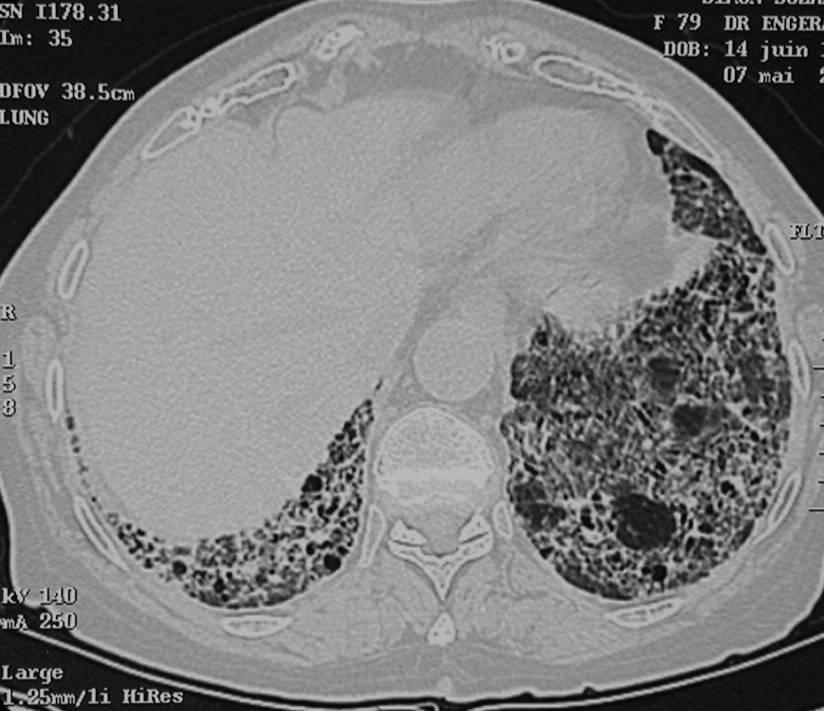
46 Idiopathic fibrosis

47 Under-pleural tissue The different parts of intersticial tissue: Axial or peribronchovascular tissue Axial tissue Peri-lobular tissue (according to Dr. Bernadac ) Intra-lobular tissue
 -Sarcoidosis -Viral and fungal infection The association of nodular and")
48 The pathology of peribronchovascular tissue is characterised by linear opacities from the hilus to the periphery of the lungs. Main etiologies are: -Carcinomatous lymphangitis -Fibrosis regardless of the etiology (idiopathic, autoimmune, allergic, toxic) -Sarcoidosis -Viral and fungal infection The association of nodular and linear images is highly suggestive of carcinomatous lymphangitis Carcinomatous lymphangitis


49 Man, 60 years old. Dyspnea with effort, poor condition and jaundice. The association of nodular and linear images suggests in this context a carcinomatous lymphangitis (pancreatic origin)

50 Previous case
51 Conclusions The Interstitial pathology is complicated The etiologies are numerous The intrication with alveolar pictures is frequent (cardiac failure, TB, infections..) The interpretation requires a very good quality chest radiography (especially for miliary) CT scan is much more performant but not always easily accessible
Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images
 Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology
Interstitial Syndrome Ground glass attenuation miliary and nodular images Linear images Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology
Alveolar condensation syndrome
 Alveolar condensation syndrome Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Lobule: morphological unit. Dimension: 10 to
Alveolar condensation syndrome Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Lobule: morphological unit. Dimension: 10 to
Pulmonary TB aspects
 Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Radiological syndroms. Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome
 Radiological syndroms Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome Alveolar syndrome Pulmonary architecture : Morphological unit is the lobule 15-25mm
Radiological syndroms Alveolar syndrome Bronchial syndrome Interstitial syndrome Vascular syndrome Mediastinal Syndrome Alveolar syndrome Pulmonary architecture : Morphological unit is the lobule 15-25mm
Key messages. CXR interpretation in TB/HIV setting. Training course
 Key messages CXR interpretation in TB/HIV setting Training course Normal CXR Front view and lateral view Good notions of technical conditions to obtain a good CXR Good knowledge of criteria for quality
Key messages CXR interpretation in TB/HIV setting Training course Normal CXR Front view and lateral view Good notions of technical conditions to obtain a good CXR Good knowledge of criteria for quality
Man, 65 years old, heavy smoker, cough, dyspnea and weight loss. AFB negative in sputum. Is TB possible?
 Chapter 10 Man, 65 years old, heavy smoker, cough, dyspnea and weight loss. AFB negative in sputum. Is TB possible? The opacity of the left upper lobe is not cavited and looks like a tissular mass, not
Chapter 10 Man, 65 years old, heavy smoker, cough, dyspnea and weight loss. AFB negative in sputum. Is TB possible? The opacity of the left upper lobe is not cavited and looks like a tissular mass, not
Cardio-vascular syndrome. Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology
 Cardio-vascular syndrome Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Left pulmonary artery Right pulmonary artery OFCP Left
Cardio-vascular syndrome Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Left pulmonary artery Right pulmonary artery OFCP Left
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
CARDIO-VASCULAR SYNDROME
 CARDIO-VASCULAR SYNDROME Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) OFCP Right pulmonary artery Left pulmonary artery
CARDIO-VASCULAR SYNDROME Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) OFCP Right pulmonary artery Left pulmonary artery
Case N 1. Anterior thoracic paint with increasing dyspnea for few days. No cough. Decrease of cardiac sounds. Courtesy Dr Van den Homberg-Tanzania
 Case N 1 Anterior thoracic paint with increasing dyspnea for few days. No cough. Decrease of cardiac sounds Courtesy Dr Van den Homberg-Tanzania Case N 1 Enlargment of cardiac silhouette. Notice the symetry
Case N 1 Anterior thoracic paint with increasing dyspnea for few days. No cough. Decrease of cardiac sounds Courtesy Dr Van den Homberg-Tanzania Case N 1 Enlargment of cardiac silhouette. Notice the symetry
Man 70 years old, chronic chonic exercice dyspnea, and past history of HTA. Acute and severe dyspnea, with non purulent sputum.
 Chapter 7 Man 70 years old, chronic chonic exercice dyspnea, and past history of HTA. Acute and severe dyspnea, with non purulent sputum. Auscultation: crepitant bilateral rales. Chest Xray: cardiomegaly
Chapter 7 Man 70 years old, chronic chonic exercice dyspnea, and past history of HTA. Acute and severe dyspnea, with non purulent sputum. Auscultation: crepitant bilateral rales. Chest Xray: cardiomegaly
Case N 1. Dyspnea and cough. Right thoracic paint. AFB in sputum not yet available. Courtesy Dr Van Den Homberg
 Case N 1 Dyspnea and cough. Right thoracic paint. AFB in sputum not yet available Courtesy Dr Van Den Homberg Case N 1 CXR: Right abundant pleural effusion. Notice the typical concave aspect of the superior
Case N 1 Dyspnea and cough. Right thoracic paint. AFB in sputum not yet available Courtesy Dr Van Den Homberg Case N 1 CXR: Right abundant pleural effusion. Notice the typical concave aspect of the superior
HRCT in Diffuse Interstitial Lung Disease Steps in High Resolution CT Diagnosis. Where are the lymphatics? Anatomic distribution
 Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Steps in High Resolution CT Diagnosis Pattern of abnormality Distribution of disease Associated findings Clinical history Tomás Franquet MD What is the diagnosis? Hospital de Sant Pau. Barcelona Secondary
Case 1: Question. 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule
 HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
Pleural syndrome Tuberculous pleurisy
 Pleural syndrome Tuberculous pleurisy Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Pleural effusion: Findings of fluid between
Pleural syndrome Tuberculous pleurisy Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Pleural effusion: Findings of fluid between
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations
 Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
I particularly want to thank: -Pr Pierre L Her who has been my nearest partner in this adventure which began in Cambodia many years ago.
 Introduction and advices for users: CXR interpretation in TB/HIV high burden settings Clinical and radiological cases for training to positive and differential diagnosis Here are collected 144 clinical
Introduction and advices for users: CXR interpretation in TB/HIV high burden settings Clinical and radiological cases for training to positive and differential diagnosis Here are collected 144 clinical
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Resident Case Review CHEST. Daria Manos CAR 2016
 Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
Resident Case Review CHEST CAR 2016 Daria Manos Disclosure Speakers bureau, Roche CAR 2016 Daria Manos 1. Recognize common and critical chest radiograph and computed tomography signs and use these clues
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
Pleural syndrome. Tubercular pleurisy
 Pleural syndrome. Tubercular pleurisy Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Pleurisy: Findings of fluid between visceral
Pleural syndrome. Tubercular pleurisy Dr Etienne Leroy-Terquem Centre hospitalier de Meulan les Mureaux. France French-cambodian association for pneumology (OFCP) Pleurisy: Findings of fluid between visceral
Bronchiectasis: An Imaging Approach
 Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Bronchiectasis: An Imaging Approach Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco Large Middle Small 1 Bronchiectasis
Radiologists toolbox to differentiate alveolar versus interstitial lung diseases
 Radiologists toolbox to differentiate alveolar versus interstitial lung diseases Dr Sumer Shikhare, Dr Trishna Shimpi, Dr Ashish Chawla Khoo Teck Puat Hospital Singapore. Relevant financial disclosures
Radiologists toolbox to differentiate alveolar versus interstitial lung diseases Dr Sumer Shikhare, Dr Trishna Shimpi, Dr Ashish Chawla Khoo Teck Puat Hospital Singapore. Relevant financial disclosures
The Dr. Jae Yang Lecture: An Overview of the Radiographic Picture of TB
 The Dr. Jae Yang Lecture: An Overview of the Radiographic Picture of TB Harvey H. Wong, MD FRCPC MScCH Assistant Professor Department of Medicine Division of Respirology University of Toronto Financial
The Dr. Jae Yang Lecture: An Overview of the Radiographic Picture of TB Harvey H. Wong, MD FRCPC MScCH Assistant Professor Department of Medicine Division of Respirology University of Toronto Financial
Acute and Chronic Lung Disease
 KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
KATHOLIEKE UNIVERSITEIT LEUVEN Faculty of Medicine Acute and Chronic Lung Disease W De Wever, JA Verschakelen Department of Radiology, University Hospitals Leuven, Belgium Clinical utility of HRCT To detect
Micronodular Lung Disease an algorithm
 Micronodular Lung Disease an algorithm H. Page McAdams, MD Department of Radiology Duke University Medical Center Durham, NC USA page.mcadams@duke.edu Question Which of the following lung diseases is MOST
Micronodular Lung Disease an algorithm H. Page McAdams, MD Department of Radiology Duke University Medical Center Durham, NC USA page.mcadams@duke.edu Question Which of the following lung diseases is MOST
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Introduction to Radiology for TB Nurses
 Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
Introduction to Radiology for TB Nurses Juzar Ali, MD; FRCP(C); FCCP May 4, 2018 Essential Skills for the TB Nurse Case Manager Little Rock, AR May 3 4, 2017 Juzar Ali, MD; FRCP(C); FCCP has the following
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
The Imaging Analysis of Pulmonary Sarcodiosis
 www.cancercellresearch.org ISSN: 2161-2609 Article The Imaging Analysis of Pulmonary Sarcodiosis Xin He, Chuanyu Zhang* Department of Radiology, Affiliated Hospital of Qingdao University, Qingdao, China
www.cancercellresearch.org ISSN: 2161-2609 Article The Imaging Analysis of Pulmonary Sarcodiosis Xin He, Chuanyu Zhang* Department of Radiology, Affiliated Hospital of Qingdao University, Qingdao, China
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
Pulmonary Sarcoidosis - Radiological Evaluation
 Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer
 Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer Poster No.: C-2297 Congress: ECR 2012 Type: Educational Exhibit Authors: Y.
Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer Poster No.: C-2297 Congress: ECR 2012 Type: Educational Exhibit Authors: Y.
Daria Manos RSNA 2016 RC 401. https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html
 Daria Manos RSNA 2016 RC 401 https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html STEP1: Is this fibrotic lung disease? STEP 2: Is this a UIP pattern? If yes:
Daria Manos RSNA 2016 RC 401 https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html STEP1: Is this fibrotic lung disease? STEP 2: Is this a UIP pattern? If yes:
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Radiologic-pathologic correlation of pulmonary diseases
 The 1578 th Chest Conference/ 3 rd Biennial Clinical- Radiologic-Pathologic Correlation Radiologic-pathologic correlation of pulmonary diseases Harumi Itoh, M.D. University of Fukui, Japan Centriacinar
The 1578 th Chest Conference/ 3 rd Biennial Clinical- Radiologic-Pathologic Correlation Radiologic-pathologic correlation of pulmonary diseases Harumi Itoh, M.D. University of Fukui, Japan Centriacinar
An Image Repository for Chest CT
 An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
An Image Repository for Chest CT Francesco Frajoli for the Chest CT in Antibody Deficiency Group An Image Repository for Chest CT he Chest CT in Antibody Deficiency Group is an international and interdisciplinary
Differential diagnosis
 Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings
 Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings Poster No.: C-1425 Congress: ECR 2017 Type: Educational
Pneumocystis jirovecci pneumonia: from mild disease to a real disaster. A pictorial review of the different radiologic patterns in acute settings Poster No.: C-1425 Congress: ECR 2017 Type: Educational
Comparison of High-resolution CT Findings between Miliary Metastases and Miliary Tuberculosis 1
 Comparison of High-resolution CT Findings between Miliary Metastases and Miliary Tuberculosis 1 Chan Sung Kim, M.D., Ki-Nam Lee, M.D., Jin Hwa Lee, M.D. Purpose: To compare the findings of high-resolution
Comparison of High-resolution CT Findings between Miliary Metastases and Miliary Tuberculosis 1 Chan Sung Kim, M.D., Ki-Nam Lee, M.D., Jin Hwa Lee, M.D. Purpose: To compare the findings of high-resolution
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
I have no relevant conflicts of interest to disclose
 I have no relevant conflicts of interest to disclose Diffuse parenchymal lung disease (DPLD) and its associations Secondary lobular anatomy DPLD History, clinical findings, temporal evolution, and exposures
I have no relevant conflicts of interest to disclose Diffuse parenchymal lung disease (DPLD) and its associations Secondary lobular anatomy DPLD History, clinical findings, temporal evolution, and exposures
Lung Metastases Imaging
 Lung Metastases Imaging Updated: Oct 23, 2015 Author: Tanay Patel, MD; Chief Editor: Eugene C Lin, MD more... OVERVIEW Overview Pulmonary metastasis is seen in 20-54% of extrathoracic malignancies. [1]
Lung Metastases Imaging Updated: Oct 23, 2015 Author: Tanay Patel, MD; Chief Editor: Eugene C Lin, MD more... OVERVIEW Overview Pulmonary metastasis is seen in 20-54% of extrathoracic malignancies. [1]
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Immunocompromised patients. Immunocompromised patients. Immunocompromised patients
 Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
Value of CT in Early Pneumonia in Immunocompromised Patients Nantaka Kiranantawat, PSU Preventative Factors Phagocyts Cellular immunity Humoral immunity Predisposing Factors Infection, Stress, Poor nutrition,
INTERSTITIAL LUNG DISEASE Dr. Zulqarnain Ashraf
 Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
Indep Rev Jul-Dec 2018;20(7-12) Dr. Zulqarnain Ashraf IR-653 Abstract: ILD is a group of diseases affect interstitium of the lung. Repeated insult to the lung cause the interstitium to be damaged. Similarly
and localized ground glass opacities, or bronchiolar focal or multifocal micronodules;
 E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
E1 Chest CT scan and Pneumoniae_YE Claessens et al- Supplementary methods Level of CAP probability according to CT scan - definite CAP: systematic alveolar condensation, or alveolar condensation with peripheral
Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma
 Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Article ID: WMC005047 ISSN 2046-1690 Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma Peer review status: No Corresponding Author: Dr. Mohammad Fawad Khattak,
Excavated pulmonary nodule: steps to diagnosis?
 Excavated pulmonary nodule: steps to diagnosis? Poster No.: C-1044 Congress: ECR 2014 Type: Authors: Keywords: DOI: Educational Exhibit W. Mnari, M. MAATOUK, A. Zrig, B. Hmida, M. GOLLI; Monastir/ TN Metastases,
Excavated pulmonary nodule: steps to diagnosis? Poster No.: C-1044 Congress: ECR 2014 Type: Authors: Keywords: DOI: Educational Exhibit W. Mnari, M. MAATOUK, A. Zrig, B. Hmida, M. GOLLI; Monastir/ TN Metastases,
Pulmonary fibrosis on the lateral chest radiograph: Kerley D lines revisited
 Insights Imaging (2017) 8:483 489 DOI 10.1007/s13244-017-0565-2 PICTORIAL REVIEW Pulmonary fibrosis on the lateral chest radiograph: Kerley D lines revisited Daniel B. Green 1 & Alan C. Legasto 1 & Ian
Insights Imaging (2017) 8:483 489 DOI 10.1007/s13244-017-0565-2 PICTORIAL REVIEW Pulmonary fibrosis on the lateral chest radiograph: Kerley D lines revisited Daniel B. Green 1 & Alan C. Legasto 1 & Ian
Uses, limitations and interpretation of CT in pulmonary infections: A practical approach
 Uses, limitations and interpretation of CT in pulmonary infections: A practical approach Canadian Association of Radiologists 2013 DISCLOSURES Speakers honorarium, Siemens Canada Objectives 1. Recognize
Uses, limitations and interpretation of CT in pulmonary infections: A practical approach Canadian Association of Radiologists 2013 DISCLOSURES Speakers honorarium, Siemens Canada Objectives 1. Recognize
Case Presentations in ILD. Harold R. Collard, MD Department of Medicine University of California San Francisco
 Case Presentations in ILD Harold R. Collard, MD Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Definition/Classification High-resolution CT scan Multidisciplinary
Case Presentations in ILD Harold R. Collard, MD Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Definition/Classification High-resolution CT scan Multidisciplinary
Mimics in chest disease: interstitial opacities
 Insights Imaging (2013) 4:9 27 DOI 10.1007/s13244-012-0207-7 PICTORIAL REVIEW Mimics in chest disease: interstitial opacities Anastasia Oikonomou & Panos Prassopoulos Received: 19 June 2012 / Revised:
Insights Imaging (2013) 4:9 27 DOI 10.1007/s13244-012-0207-7 PICTORIAL REVIEW Mimics in chest disease: interstitial opacities Anastasia Oikonomou & Panos Prassopoulos Received: 19 June 2012 / Revised:
5/9/2015. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. No, I am not a pulmonologist! Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Imaging of the Lung. István Battyány
 Imaging of the Lung István Battyány Anatomy of airways: (asszimetric dichotomy) trachea Main bronchus Lobar bronchus }lung, lobe 1. segmental bronchus subsegmental bronchus bronchus lobularis bronchiolus
Imaging of the Lung István Battyány Anatomy of airways: (asszimetric dichotomy) trachea Main bronchus Lobar bronchus }lung, lobe 1. segmental bronchus subsegmental bronchus bronchus lobularis bronchiolus
Respiratory Pathology. Kristine Krafts, M.D.
 Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Respiratory Pathology Kristine Krafts, M.D. Normal lung: alveolar spaces Respiratory Pathology Outline Acute respiratory distress syndrome Obstructive lung diseases Restrictive lung diseases Vascular
Case presentation. Dr REESAUL R
 Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
September 2014 Imaging Case of the Month. Michael B. Gotway, MD. Department of Radiology Mayo Clinic Arizona Scottsdale, AZ
 September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
Manish Powari Regional Training Day 10/12/2014
 Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts
 Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Nov 2003 Radiological Aspects of Pulmonary Tuberculosis in Immunocompetent Hosts Josh Rempell, Harvard Medical School Year III Tuberculosis: the captain of all (wo)men of death Overall, one third of the
Outline Definition of Terms: Lexicon. Traction Bronchiectasis
 HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
RADIOLOGICALL ANALYSIS OF INTERSTITIAL LUNG DISEASES
 Original Research Article RADIOLOGICALL ANALYSIS OF INTERSTITIAL LUNG DISEASES Meraj Rentia 1*, Himanshu Singla 1, Divya Malpani 2, Tushar Vaishnav 3, Pradeep Jhala 3 1 1 st year Resident, 2 3 rd year
Original Research Article RADIOLOGICALL ANALYSIS OF INTERSTITIAL LUNG DISEASES Meraj Rentia 1*, Himanshu Singla 1, Divya Malpani 2, Tushar Vaishnav 3, Pradeep Jhala 3 1 1 st year Resident, 2 3 rd year
Index. B Biological factors, 2 Brain stem encephalitis, Burkitt s lymphoma, 83, 105
 Index A Acquired immunodeficiency syndrome (AIDS) abdomen gallbladder complications, 97, 107 109 gastrointestinal complications, 96, 105 106 liver complications, 97, 107 109 neoplasm, 99, 110 111 pancreas
Index A Acquired immunodeficiency syndrome (AIDS) abdomen gallbladder complications, 97, 107 109 gastrointestinal complications, 96, 105 106 liver complications, 97, 107 109 neoplasm, 99, 110 111 pancreas
Nitrofurantoin-Induced Lung Toxicity
 Severe Nitrofurantoin-Induced Lung Toxicity Rami Jambeih, M.D. 1, John Flesher, M.D. 1,3, Joe J. Lin, M.D. 2,4 University of Kansas School of Medicine Wichita 1 Department of Internal Medicine 2 Department
Severe Nitrofurantoin-Induced Lung Toxicity Rami Jambeih, M.D. 1, John Flesher, M.D. 1,3, Joe J. Lin, M.D. 2,4 University of Kansas School of Medicine Wichita 1 Department of Internal Medicine 2 Department
100 Chest X Rays for Study Group. by Dr. Suneet Khurana
 100 Chest X Rays for Study Group by Dr. Suneet Khurana Approach to - Chest X Ray (shadow of the viscera on a photographic plate) Gas appears Black Fat appears Dark Grey Water Appears as Light Grey Bone
100 Chest X Rays for Study Group by Dr. Suneet Khurana Approach to - Chest X Ray (shadow of the viscera on a photographic plate) Gas appears Black Fat appears Dark Grey Water Appears as Light Grey Bone
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Thoracic Imaging: A Case of Metastatic Adenocarcinoma of Unknown Primary
 January 28, 2009 Thoracic Imaging: A Case of Metastatic Adenocarcinoma of Unknown Primary Kristina Mirabeau-Beale, Harvard Medical School Year III Gillian Lieberman, MD Agenda Introduce Patient RS Discuss
January 28, 2009 Thoracic Imaging: A Case of Metastatic Adenocarcinoma of Unknown Primary Kristina Mirabeau-Beale, Harvard Medical School Year III Gillian Lieberman, MD Agenda Introduce Patient RS Discuss
Typical and atypical findings of pulmonary sarcoidosis at high resolution CT
 Typical and atypical findings of pulmonary sarcoidosis at high resolution CT Poster No.: C-0169 Congress: ECR 2013 Type: Educational Exhibit Authors: L. Raposo Rodríguez, C. Mejía, B. Escobar Mallada,
Typical and atypical findings of pulmonary sarcoidosis at high resolution CT Poster No.: C-0169 Congress: ECR 2013 Type: Educational Exhibit Authors: L. Raposo Rodríguez, C. Mejía, B. Escobar Mallada,
* MILIARY MOTTLING --
 * MILIARY MOTTLING -- RARE CAUSE DR ARATHI SRINIVASAN FELLOW IN PEDIATRIC HEMATO ONCOLOGY DR A ANDAL DEPARTMENT OF PEDIATRICS DR JULIUS XAVIER SCOTT DEPARTMENT OF PEDIATRIC HEMATO ONCOLOGY KANCHI KAMAKOTI
* MILIARY MOTTLING -- RARE CAUSE DR ARATHI SRINIVASAN FELLOW IN PEDIATRIC HEMATO ONCOLOGY DR A ANDAL DEPARTMENT OF PEDIATRICS DR JULIUS XAVIER SCOTT DEPARTMENT OF PEDIATRIC HEMATO ONCOLOGY KANCHI KAMAKOTI
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I. December 5, 2012
 SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Chest imaging III: Nodular pulmonary disease. Ádám Domonkos Tárnoki, MD, PhD Assistant professor Department of Radiology, Semmelweis University 1
 Chest imaging III: Nodular pulmonary disease Ádám Domonkos Tárnoki, MD, PhD Assistant professor Department of Radiology, Semmelweis University 1 Pattern 2 Nodular pattern Several round opacity, typically
Chest imaging III: Nodular pulmonary disease Ádám Domonkos Tárnoki, MD, PhD Assistant professor Department of Radiology, Semmelweis University 1 Pattern 2 Nodular pattern Several round opacity, typically
Respiratory Interactive Session. Elaine Borg
 Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Chest Radiology LYMPHANGITIC CARCINOMATOSIS CERTAIN CANCERS SPREAD BY PLUGGING THE LYMPHATICS
 2 Chest Radiology Includes plain film diagnosis, CT, MRI, and interventional techniques used in the diagnosis of diseases of the lungs, pleura, and mediastinum including the heart and great vessels. LYMPHANGITIC
2 Chest Radiology Includes plain film diagnosis, CT, MRI, and interventional techniques used in the diagnosis of diseases of the lungs, pleura, and mediastinum including the heart and great vessels. LYMPHANGITIC
Complicated echinococcal cyst to Biopsy or not to biopsy. V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center
 Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
Complicated echinococcal cyst to Biopsy or not to biopsy V. Rusanov MR Kramer Pulmonary Institute, Rabin medical center Case 1 84 y.o. Male, Iraq descend, past smoker 40 PY Medical History- HTN, Rheumatoid
HIV-associated Pulmonary Disease. Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond QUESTION: HIV-associated Pulmonary Diseases
 Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond Laurence Huang, MD Professor of Medicine University of California San Francisco Chief, HIV/AIDS Chest Clinic Zuckerberg San Francisco General
Classic and Challenging Cases from the HIV/AIDS Clinic and Beyond Laurence Huang, MD Professor of Medicine University of California San Francisco Chief, HIV/AIDS Chest Clinic Zuckerberg San Francisco General
Radiation Pneumonitis Joseph Junewick, MD FACR
 Radiation Pneumonitis Joseph Junewick, MD FACR 03/19/2010 History 16 year old with history of relapsed stage IV-A Hodgkin disease. Prior pulmonary involvement was irradiated. Diagnosis Radiation Pneumonitis
Radiation Pneumonitis Joseph Junewick, MD FACR 03/19/2010 History 16 year old with history of relapsed stage IV-A Hodgkin disease. Prior pulmonary involvement was irradiated. Diagnosis Radiation Pneumonitis
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Long Case Set 02. Dr Raviraj Uppoor. Dr Sameer Shamshuddin. Consultant Radiologist Cumberland Infirmary, Carlisle, UK
 Long Case Set 02 www.frcrtutorials.com Dr Raviraj Uppoor MBBS, DMRD, DNB, FRCR Consultant Radiologist Cumberland Infirmary, Carlisle, UK Dr Sameer Shamshuddin MBBS, DMRD, FRCR Consultant Radiologist Royal
Long Case Set 02 www.frcrtutorials.com Dr Raviraj Uppoor MBBS, DMRD, DNB, FRCR Consultant Radiologist Cumberland Infirmary, Carlisle, UK Dr Sameer Shamshuddin MBBS, DMRD, FRCR Consultant Radiologist Royal
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia. Nitra and the Gangs.
 Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
General History. 林陳 珠 Female 69 years old 住院期間 : ~ Chief Complaint : sudden loss of conscious 5 minutes in the morning.
 General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
General History 林陳 珠 Female 69 years old 住院期間 : 93.5.8~93.5.15 Chief Complaint : sudden loss of conscious for 2-52 5 minutes in the morning. General History DM under regular medical control for 10 years.
Diffuse Interstitial Lung Diseases: Is There Really Anything New?
 : Is There Really Anything New? Sujal R. Desai, MBBS, MD ESTI SPEAKER SUNDAY Society of Thoracic Radiology San Antonio, Texas March 2014 Diffuse Interstitial Lung Disease The State of Play DILDs Is There
: Is There Really Anything New? Sujal R. Desai, MBBS, MD ESTI SPEAKER SUNDAY Society of Thoracic Radiology San Antonio, Texas March 2014 Diffuse Interstitial Lung Disease The State of Play DILDs Is There