Oxygen Workbook. Produced by the Oxygen Steering Group, 2018
|
|
|
- Mary Neal
- 5 years ago
- Views:
Transcription

1 Oxygen Workbook 1 Produced by the Oxygen Steering Group, 2018
2 Contents 1. Pre-workbook Quiz Understanding breathing... 4 Anatomy of the Lung... 4 Respiratory Tract... 5 Function of the Lungs... 5 Exercise Mechanics of Breathing... 8 Inspiration and Expiration... 9 Gaseous exchange Composition of Gases in Air Lung Volumes and Capacities Vital Capacity Work of Breathing Exercise 2 Respiratory Anatomy & Physiology Quiz Exercise 3 Respiratory Anatomy & Physiology Quiz Exercise 4 Respiratory Anatomy & Physiology Quiz Indications for Oxygen Therapy Hypoxemia Oxygen Saturations Fraction of inspired oxygen (FiO 2 ) Respiratory Failure Type I Hypoxaemic Respiratory Failure Type II Hypercapnic Respiratory Failure Exercise Risks Prescribing oxygen therapy Via MedChart Administration of Oxygen Therapy Oxygen Administration flowchart Devices Fixed (controlled) oxygen delivery devices Weaning Humidified High Flow Nasal Prongs Variable (uncontrolled) oxygen delivery devices Titrating and weaning Oxygen Weaning flow chart Home oxygen Short Term Oxygen Therapy (STOT) and Long Term Oxygen Therapy (LTOT) Scenarios Scenario - Mrs Brown Scenario Steve Scenario - Olivia Scenario - Meredith Scenario - Adam Scenario - Jennifer Key messages Glossary / Terms References
3 1. Pre-workbook Quiz 1. Oxygen is a drug? Y N maybe 2. Oxygen is a treatment for? breathlessness hypoxia high carbon dioxide 3. Humidified High Flow Nasal O 2 Therapy should be documented as Oxygen percentage? Y N maybe 4. Can oxygen be given in an emergency without prescription? Y N maybe 5. The maximum amount of oxygen to be given through nasal prongs is? 2L 3L 5L 6. What type of oxygen delivery system would normally be used in a self-ventilating patient with SaO 2 < 60%? nasal cannula Venturi mask Reservoir mask Hudson mask 7. A patient presents to ED with a 60 pack year smoking history, obesity and swollen ankles, his target saturations should be? % 90-95% 88-92% 92-96% 8. What is the target oxygen saturations for a 20 year old asthmatic patient who presents with an acute exacerbation of asthma? 94-98% 88-92% 90-99% 92-96% year old man with no previous medical history having ankle surgery is on a PCA, what are his target saturations? 88-92% % 92-96% 10. A Venturi mask can be used as alternative to HHFNP? Y N 11. Which of the following devices can give controlled oxygen (ie with a fixed FiO 2 )? Venturi mask Hudson mask Humidified High Flow Nasal Prongs (Airvo) nasal prongs 3
4 2. Understanding breathing Anatomy of the Lung The respiratory system is made up of organs related to the exchange and interchange of gases, they consist of the following: Nose The most important functions of the nose are to filter the atmospheric air before passing it further into the respiratory system, and to provide the sense of smell. Pharynx Is a common passageway for air and food; the pharynx opens into two pathways, one that leads to the oesophagus, the other trachea or air passage. The pharynx continually removes dust and warms inhaled air. Larynx Protects the airway from food and liquid; also protects the vocal chords. Trachea Continuously cleans air and is lined with goblet cells and ciliated epithelial cells which produce mucus and carry dirt and particles back up to the pharynx. The mucus moistens the air when it passes through the respiratory tract. Lungs Contain alveoli and bronchi. They are responsible for transporting oxygen from the atmosphere into blood and releasing carbon dioxide from blood back to the atmosphere. Bronchi One of the primary functions of bronchi is to allow air to pass through it. As the trachea splits into two parts, the inhaled air then enters the bronchi. From here, it passes through further divisions of the bronchi; these divisions are known as bronchioles. The bronchioles then divide to form alveolar ducts which eventually end into alveolar air sacs or alveoli. Thus, the bronchi basically act as a passage for air to pass through. Alveoli The functional unit of the lungs are tiny air sacs that arise from bronchioles called alveoli. These terminal air sacs are the area where the exchange of gases takes place within the lungs. This air exchange consists of absorption of oxygen and removal of carbon dioxide. Source: 4

5 Respiratory Tract The respiratory tract is divided into two main parts: the upper respiratory tract consisting of the nose, nasal cavity and the pharynx; and the lower respiratory tract consisting of the larynx, trachea, bronchi and the lungs. The trachea, which begins at the edge of the larynx, divides into two bronchi and continues into the lungs. The trachea allows air to pass from the larynx to the bronchi and then to the lungs. The bronchi divide into smaller bronchioles, which branch in the lungs forming passageways for air. The terminal parts of the bronchi are the alveoli. The alveoli are the functional units of the lungs and they form the site of gaseous exchange. Source: Function of the Lungs Lungs take in oxygen, which cells need to live and carry out normal functions. The lungs also get rid of carbon dioxide (travels in the blood as bicarbonate), a waste product of the body s cells. Lungs are enveloped in a membrane called the pleura. Visceral pleura lines the lungs and parietal pleura lines the thoracic cavity. Between the two is a potential space which contains a lubricating fluid, this allows pleural layers to slide against each other easily during respiration. The pleura keeps the lung next to the chest wall, to allow for optimum inflation of the alveoli during respiration. It directly transmits pressures from the chest wall to the lung. Therefore, movements of the chest wall during breathing are coupled closely with movement of the lungs. 5
 lung one to the R) lung. In the lungs, the main-stem bronchus divide into smaller bronchi Then into bronchioles, bronchioles end in alveoli.")
6 When you inhale Air enters the body through the nose and/or mouth Travels down the throat through the larynx and trachea Air enters into the lungs through tubes called main stem bronchus One main stem bronchus leads to L) lung one to the R) lung. In the lungs, the main-stem bronchus divide into smaller bronchi Then into bronchioles, bronchioles end in alveoli. It is here where the exchange of oxygen and carbon dioxide between air and the blood in the lungs occurs. Blood enters the lungs via the pulmonary arteries. It then proceeds through arterioles and into the alveolar capillaries. Oxygen and carbon dioxide are exchanged between blood and the air. This blood then flows out of the alveolar capillaries, through venuoles, and back to the heart via the pulmonary veins. 6
7 Exercise 1 Review the Respiratory System diagram (You can find images on Google for Respiratory tract) Identify each of the numbered areas; enter your answers in the table below. ANSWERS
8 3. Mechanics of Breathing What is a Respiration? Respiration is the transport of oxygen from ambient air to the tissue cells and the transport of carbon dioxide in the opposite direction. It consists of: Inspiration (inhaling) Expiration (exhaling) Inspiration Inspiration is an active process requiring 75% diaphragmatic muscular effort. During inspiration The diaphragm moves downwards increasing the volume of the thoracic cavity. Intercostal muscles pull the ribs up expanding the rib cage and further increasing this volume. Through this there is a fall in intra-pleural pressure and a fall in alveolar pressure (below atmospheric pressure). This is negative pressure. Air always flows from a region of high pressure to a region of lower pressure. In inspiration the pressure gradient is from the mouth to the alveoli (ie gas follows the pressure gradient). Air is sucked in through the respiratory tract and into the alveoli. This is called negative pressure breathing. Expiration In expiration the diaphragm and intercostal muscles relax. This is usually a passive process. This relaxation of the muscles and diaphragm causes: The intra-pleural pressure to become less negative. The alveolar pressure rises (above atmospheric pressure). The gas flows from high pressure gradient to a low pressure gradient. The gas is forced out into the air. 8

9 Inspiration and Expiration Source: 9

10 Gaseous exchange SOURCE: Address&dcr=0&source=lnms&tbm=isch&sa=X&ved=0ahUKEwiytrS_g5LYAhUJXLwKHdWfBKYQ_AUICigB&biw=1 280&bih=879#imgrc=W9JCUrvaLJyPxM:&spf=

11 Composition of Gases in Air Source: 11

12 Lung Volumes and Capacities Source: Go to site volumes 12
13 Vital Capacity Vital capacity is maximal inspiration followed by maximal expiration and this is the volume measured in simple spirometry. Vital Capacity is affected by factors such as: Gender (eg 20-25% less in adult females) Age (maximum in young adults) Body size. Vital Capacity is also affected by illness and disease such as: Paralysis eg: Muscular dystrophy/motor neuron disease Polio Spinal cord injury. Lung inflation problems/restrictive disorders eg: Pulmonary fibrosis/silicosis Scoliosis/kyphosis. Obstructive disorders eg: Asthma COPD Collapse of bronchi/emphysema Tumour. Work of Breathing Work of breathing (WOB) is how much work that the body has to do to breath. WOB accounts for 5% of total body oxygen consumption in a normal resting state but can increase dramatically during acute illness. Most of this is used to overcome the lung and chest wall stiffness during inspiration (called compliance ) Work to overcome airway resistance is usually very small, except during exercise or in unusual situations like asthmatics. Patients with respiratory diseases have increased respiratory workloads, which may be due to: o High respiratory rates o Stiff lungs o High airway resistances. When a patient becomes so exhausted that they can no longer keep up workload respiratory failure results. 13
14 Exercise 2 Respiratory Anatomy & Physiology Quiz Match by drawing a line between the pulmonary measurement and the correct definition. Tidal Volume Total volume of air in the lung Inspiratory Capacity Volume of air inspired or expired in a normal breath Total Lung Capacity Expiratory reserve volume + residual volume Vital Capacity The maximal amount of air that can be inspired after a tidal expiration Residual Volume Maximal volume of air expired forcefully after a maximal inspiration inspiration followed by maximal expiration Functional Residual Capacity Air remaining in the lungs after forced expiration Expiratory Reserve Volume Volume of air that can be forcefully inspired after a normal tidal exhalation 14
15 Exercise 3 Respiratory Anatomy & Physiology Quiz Write your answers using the word bank below: 1. pleura lines the thoracic cavity. 2. volume is the volume that remains after the most forceful exhalation (1200 ml). 3. A disease of the lungs in which the walls of alveoli lose elasticity and remain filled causing increased chest size (barrel-chested) is called. 4. Breathing in; or inhaling is called. 5. Breathing out; exhaling is called. 6. Difficult expiration caused by contraction in the muscles surrounding the bronchioles, often caused by allergic reactions, is called. 7. Inflammation of the bronchi is called. 8. Inflammation of the pleura is called. 9. Mucus in the respiratory system is pushed upward by. 10. Normal breathing volume (normally about 500 ml. per breath) is called. 11. Oxygen deficiency is called. 12. Secondary bronchi branch into smaller tubes called. 13. Sputum is another term for. 14. The pleura covers the lungs. 15. The is the narrow portion at the top of the lungs. 16. The is the volume that can be inhaled after normal inspiration Word Bank - Apex, asthma, bronchioles, bronchitis, cilia, emphysema, expiration, hypoxia, inspiration, inspiratory reserve volume, mucous, pleurisy, residual, tidal volume, visceral. parietal. 15
16 Exercise 4 Respiratory Anatomy & Physiology Quiz Write your answers using the word bank below 1. The exchange of oxygen from blood to cells is called respiration. 2. The exchange of oxygen from air to blood is called respiration. 3. The machine used to measure breathing volume is called a.. 4. The maximum breathing volume is called capacity. 5. The membrane that lines the tubes in the respiratory system is called the respiratory.. 6. The millions of tiny sacs that exchange oxygen and carbon dioxide are called. 7. The substance that coats the inside of the alveoli is called. 8. The two tubes that branch off the trachea are called the. 9. The volume that can be exhaled after expiring tidal volume ( ml) is called volume Word Bank - Alveoli, expiratory reserve, external, internal, mucosa, primary bronchi, spirometer, surfactant, vital. 16
17 4. Indications for Oxygen Therapy The rationale for using oxygen therapy in the acute setting is prevention of cellular hypoxia caused by hypoxemia (low pa0 2 ) and thus, prevention of potentially irreversible damage to vital organs. Oxygen therapy does not relieve breathlessness in the absence of hypoxaemia. For example, there is no clinical benefit with short burst oxygen therapy in COPD patients with breathlessness. Hypoxemia Hypoxemia is defined by the British Thoracic Society (2017) as low partial pressure of oxygen (pa0 2 ) in the blood. The normal pa0 2 is between kpa. Arterial Blood Gas monitoring is the gold standard for measurement as it provides critical information about ventilation, pulmonary gas exchange and acid/base status. Oxygen Saturations For an initial, safe, simple and continuous measurement of Hypoxaemia, we can use Oxyhaemaglobin Saturation (Sp0 2 ). This can be measured non-invasively and is an approximation of arterial oxygenation. This does not give us detailed information about ventilation of a patient. It is further limited by having less accuracy in certain situations such as poor peripheral perfusion, nail polish, movement artefact, cold temperatures, digital clubbing, skin colour. The Thoracic Society of Australia and New Zealand recommend an oxygen saturation range of 92-96% for most patient, and 88-92% for patients at risk of hypercapnic respiratory failure (Type 2 Respiratory Failure). Fraction of inspired oxygen (FiO 2 ) Fraction of Inspired Oxygen (FiO 2 ) represents the percentage of oxygen a person inhales with each breath. Room air contains a FiO 2 of 21%; therefore the FiO 2 of a patient without supplemental oxygen is 21%. As we increase the amount of oxygen a patient gets, we increase the FiO 2. Devices used for the delivery of oxygen can either provide a variable FiO 2, or a fixed FiO 2. Respiratory Failure The respiratory system basically consists of a gas exchanging organ (lungs) and a ventilatory pump (respiratory muscles and thorax). Either or both of these can fail and cause respiratory failure. Respiratory failure is defined as a failure to maintain adequate gas exchange and is characterised by abnormalities of arterial blood gas tensions. Type 1 failure is defined by a Pa0 2 of <8kPa with a normal or low PaC0 2 <6.0kPa eg pneumonia/ pulmonary oedema. Type 2 failure is defined by a Pa0 2 of <8kPa and a PaC0 2 of >6kPa, eg COPD. Respiratory failure can be acute, acute-on-chronic or chronic. 17
18 Type I Hypoxaemic Respiratory Failure It can be defined as hypoxaemia without hypercapnia; the carbon dioxide (CO 2 ) level may be normal or low. To put it another way, this time with values; type I respiratory failure is a PaO 2 < 8 kpa (60 mmhg) with a normal to low PaCO 2 (<6.0 kpa (45 mmhg). Therefore this type of respiratory failure is seen as an oxygenation failure but overall ventilation has been maintained. This is the most common form of respiratory failure. Causes Low inspired FiO 2 Low atmospheric gas (seen in ventilated patients) High altitude Cardiac shunt Left to right cardiac shunt (as seen in atrial or ventricular septum defect) Diffusion limitation Such as seen in interstitial lung diseases V/Q mismatch Perfused but not ventilated (intra pulmonary shunt) eg consolidation (pneumonia) atelectasis Perfused but partially ventilated eg COPD, severe asthma, pneumonia, pulmonary oedema Ventilated and partially perfused eg hypoxaemia, shock, pulmonary vasoconstriction Ventilated but unperfused eg pulmonary embolism. Type II Hypercapnic Respiratory Failure It can be defined as hypercapnia with or without hypoxaemia (more likely with hypoxaemia unless supplemental O 2 has been given). To put it another way, this time with values; Type II respiratory failure is PaO 2 < 8kPa (60 mmhg) and PaCO 2 > 6.0 kpa (50 mmhg). Type II respiratory failure may be acute or chronic in nature. Where type II is chronic HCO 3 (bicarbonate) will also be high as the kidneys have had time to retain HCO 3. If the ph is normal this is known as compensated Type II respiratory failure and where the ph remains low (acidosis) this is partially compensated Type II respiratory failure and known as acute-on- chronic respiratory failure. 18
19 Normal ARTERIAL BLOOD GAS Values Causes Parameter Normal Arterial Values ph PaCO kpa ( mmhg) HCO3 (Bi-carbonate) mmol/l PaO kpa ( mmhg) Base excess -3 to +3 Oxygen Saturation >95% Respiratory centre problems: CVA Tumour Central hypoventilation Over sedation with drugs. Muscle weakness: Guillian-Barré syndrome Motor neuron disease Myasthenia gravis Muscular dystrophy Polio Spinal injuries Muscular fatigue as seen in obesity hypoventilation. Chest wall / pleural diseases: Pneumothorax Kyphoscoliosis Massive pleural effusion Diaphragmatic paralysis. Airway disorder: Asthma Pneumonia COPD Bronchiectasis/cystic fibrosis. 19
20 Exercise 5 Hypercapnic respiratory failure can be defined as PaO 2 < 8 kpa and PaCO 2 > 6.0 kpa. True False Treatments for respiratory failure include: Bronchodilators Antibiotics oxygen All of the above Type II respiratory failure is the most common form of failure. True False Name four causes for Type I respiratory failure. Which are treatments for respiratory failure? Treat underlying cause Control any airway obstruction Control secretions Give controlled oxygen as required Consider NIV for carbon dioxide control All of the above 20
21 Name four causes for Type II respiratory failure. Name four signs and symptoms for respiratory failure
22 5. Risks Fire Hazard Oxygen is an accelerant of fire. Administration of prophylactic oxygen to a patient who is not hypoxaemic may cause a delay in recognising clinical deterioration. Not recommended in the absence of hypoxaemia for treatment of ACS and CVA. High concentration oxygen in myocardial infarction is associated with greater infarct size. Oxygen toxicity. For patients with type II respiratory failure the administration of high concentration of oxygen (above 2L/minute) may result in hypercapnia, respiratory acidosis, reduced GCS and poorer outcomes. 6. Prescribing oxygen therapy As oxygen is considered a drug at concentrations higher than ambient air, it must be prescribed by a doctor or independent prescriber, except in emergency situations. Oxygen is used to alleviate hypoxaemia (low arterial oxygen content). It is not a treatment for breathlessness and should therefore not be prescribed or administered if the oxygen saturation is > 92% on air. Oxygen must be prescribed on MedChart according to a specific oxygen delivery device and target saturation range. In an emergency situation with severe hypoxia oxygen administration without a prescription is appropriate while waiting for medical assessment of the patient. In these situations, use high concentration oxygen (15L/min via non-rebreathe mask). 22


23 Via MedChart 23
24 7. Administration of Oxygen Therapy Oxygen Administration flowchart Patient with suspected Hypoxaemia: Obtain oximetry Consider ABG in: Critically ill patients with cardiorespiratory or metabolic dysfunction In patients with an SpO 2 of <92% in whom Hypoxia may be present Deteriorating SpO 2 requiring increased FiO 2 outside treatment parameters Patients at risk of Hypercapnia Breathless patient in whom an accurate SpO 2 cannot obtained Is the patient at risk of hypercapnic respiratory failure? Yes No SpO 2 <88% SpO 2 > 88% SpO 2 <85% SpO % Start O 2 therapy Venturi 24% set at 2L/min OR Venturi 28% set at 4L/min OR Humidified High Flow Nasal Prongs Titrate O 2 to achieve SpO % target Give Bronchodilator (if prescribed) by air driven nebuliser or MDI with spacer No O 2 therapy Continue monitoring Consider ABG Start O 2 4L/min nasal cannula, 5-10L/min via mask, 15L/min via a reservoir mask Titrate O 2 to achieve SpO % target range Obtain ABG Start 2-4L/min via standard nasal prongs and/or Titrate O 2 to achieve SpO % target range Consider ABG Obtain ABG ph <7.35 and pco 2 >6.0kpa ph >7.35 PaCO 2 >6kpa or pao 2 < 8kpa PaCO 2 <6kpa and PaO 2 >8kpa Consult COPD pathway and refer to ICU/HDU Controlled O 2 as needed to maintain SpO % target saturations range. Controlled O 2 as needed to maintain Sp % target Senior medical review Controlled O 2 as needed to maintain target saturations range 92-96%. Monitor SpO 2 Titrate O 2 to maintain SpO % Consider medical review 24
25 Devices Oxygen therapy can be administered in many different ways, and should be determined by clinical indications and assessment of the patient s needs. There are many devices available in the various inpatient settings which can be utilised based on clinical indications and the intended use of the device. These must be charted as the flow rate and device, with an appropriate target saturation range. Oxygen delivery devices can be divided into those which provide a fixed percentage of oxygen (FiO 2 ) and those which provide a variable amount of oxygen (FiO 2 ) depending on the patient s minute volume. Any patient who is at risk of carbon dioxide retention, or who is a known co 2 retainer, must use a controlled oxygen delivery device to ensure we do not over oxygenate the patient causing type II respiratory failure. Fixed (controlled) oxygen delivery devices Venturi mask Aim to deliver constant oxygen concentration within and between breaths. This is a good mask for patients with raised C0 2 (patients with a target of 88-92%) With TACHYPNOEA (RR >30/min) the oxygen supply should be increased by 50%. Increasing flow does not increase oxygen concentration. Delivers 24-60% oxygen Different colours deliver different rates Flow rate: Varies with colour. The correct flow rate to use with each colour is shown on mask, along with the percentage of oxygen delivered. Types: Blue = 3L/min = 24% O 2 Yellow = 6L/min = 28% O 2 White = 8L/min = 31% O2 Green = 12L/min = 35% O 2 Pink = 15L/min = 40% O 2 Orange = 15L/min = 60% O 2 Venturi masks are used in COPD, where it is important not to over-oxygenate the patient. 25
 via wide bore nasal cannulae, providing low-level (mean) positive airway pressure and a fixed concentration (%) of oxygen.")

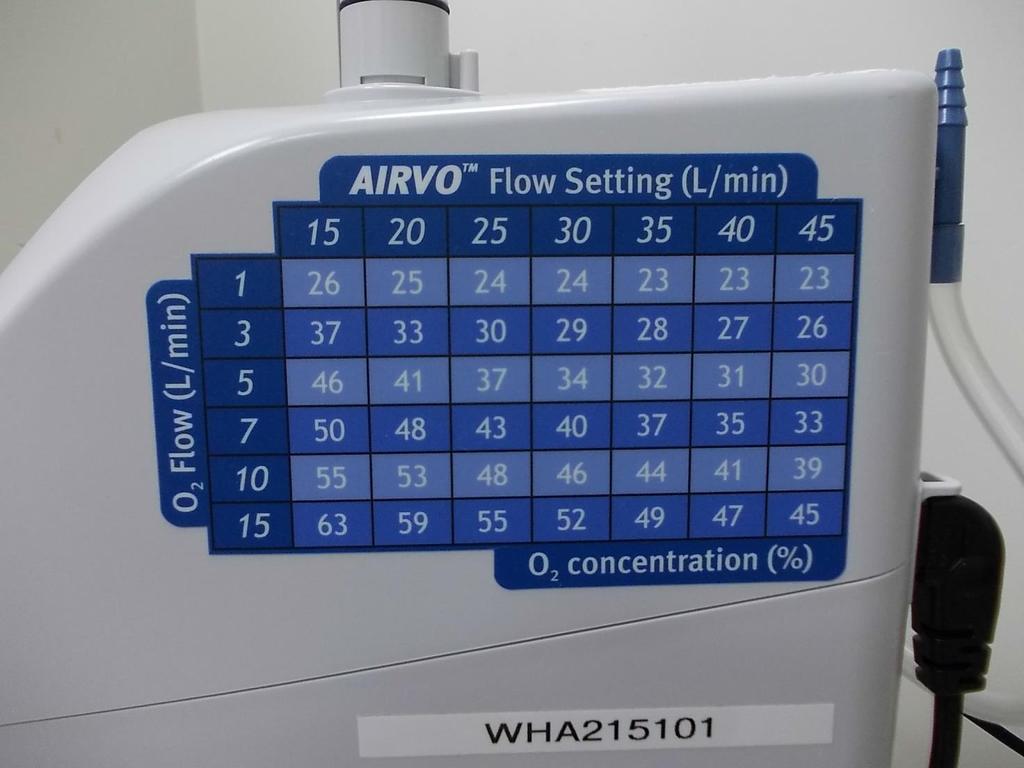
26 Humidified High Flow Nasal Prongs Humidified High Flow Nasal Prongs differ significantly from standard oxygen delivery devices. It delivers a fast humidified gas flow (blended air and oxygen) via wide bore nasal cannulae, providing low-level (mean) positive airway pressure and a fixed concentration (%) of oxygen. Air flow is usually set at 35L/min. Mean positive airway pressure increases with higher air flows. Oxygen concentrations of 21% - 52% can be delivered. Fixed delivery of oxygen concentration HHFNP meets inspiratory demand, reducing room air entrainment Reduced work of breathing due to delivery of high flow inspired gas Optimal humidification to aid expectoration Ability to eat, drink and communicate Allows the patient to self-administer inhaler therapy with a spacer. Waitemata DHB Policy [P] Oxygen Humidified High Flow Nasal Prongs - Adult 26


27 27
28 Weaning Humidified High Flow Nasal Prongs Note: Oxygen should be administered at the lowest flow that achieves the prescribed SpO 2 parameter. Nurse-led weaning of oxygen is encouraged. Oxygen flow may be weaned when patient meets following criteria: 1. Respiratory rate < 24 per minute 2. No signs of increased work of breathing (eg accessory muscle use) 3. Meeting prescribed target SpO 2 percentage. If criteria are met, commence weaning as per flow chart 28

29 Variable (uncontrolled) oxygen delivery devices Nasal cannulae Nasal prongs are variable delivery devices, as the exact amount of oxygen (FiO 2 ) the patient is receiving changes due to the patient s minute volume. Nasal prongs can be used for a flow rate up to 4L/min, and deliver FiO 2 at approximately: 1 litre/min 24% 2 litres/min 28% 3 litres/min 32% Note: These are approximations only and cannot be relied upon. Nasal prongs allow the patient to eat and drink while in use. They can also feel less intrusive than a mask. Nasal prongs work best when the curve of the prongs is aimed towards the back of the nasal cavity. They are best suited to otherwise stable patients. Nasal prongs are not recommended for patients with nose bleeds, and can dry out nasal mucosa. Deliver 24-30% oxygen Flow rate 1-4L/min (4L will dry the nose, 2L is more comfortable) Used in non-acute situations or if only mildly hypoxic (e. saturations stable at 92% in a patient without lung disease). 29


30 Simple face mask (Hudson) A simple face mask (Hudson) mask is a Variable delivery device, as the amount of oxygen a patient receives changes as the patient s breathing rate changes. Oxygen delivery via a Hudson mask is not recommended as a long term therapy. If the patient requires a longer period of oxygen, humidity may be needed. Oxygen via a Hudson mask can be delivered in an emergency when higher amounts of oxygen are required. A minimum of 5 litres/min is used, as the high flow prevents the patient from rebreathing CO 2. A hudson mask can be used to deliver up to 10 litres/min of oxygen before a different device is required. Hudson masks come in different sizes, and the correct size is important for appropriate delivery of oxygen. The mask adds a reservoir of mls where oxygen can be inhaled from, along with room air. Oxygen delivered via a hudson mask can deliver approximately: 5 litres/min 40% 6 litres/min 45-50% 8 litres/min 55-60% 10 litres/min 60% 30
, a reservoir bag can be used.")
31 Reservoir Bag Mask This is a Variable delivery device, as the patients breathing rate changes the amount of oxygen they draw in with each breath. Where a patient requires higher amounts of oxygen than a Hudson mask can deliver (>60% FiO 2 ), a reservoir bag can be used. Prior to using this, the reservoir bag needs to inflate to give a reservoir of oxygen. This is then inhaled along with the supplemental oxygen and room air, to give a higher FiO 2. To inflate the bag, place your finger over the hole and let the bag inflate. Do not over inflate the bag, as it will burst. Patients who are in shock or showing severe respiratory distress will require a higher FiO2. If you are considering applying a reservoir bag mask, consider urgently contacting the team, or calling an Adult Resus call (777). A reservoir bag mask can be used with oxygen flow at 15 litres/min. Delivers 85-90% oxygen 15L flow rate Bag on mask with valves stopping almost all rebreathing of expired air Used for acutely unwell patients Note that saturations should be maintained at 92-96%, not 100%. Do not keep patients on 15L for longer than necessary as over-oxygenating for prolonged periods can be harmful. 31

32 Ambubag In an emergency situation, where the patient requires more than 80% Fi0 2, or where the patient requires support with ventilating, an Ambubag can be used. This device can be used to deliver 100% oxygen to the patient if required. Valves in the device control the flow of oxygen from the reservoir to the patient, and prevent the exhaled carbon dioxide from entering the reservoir and diluting the oxygen concentration. The flow rate applied to the bag should be more than 10litres/min to prevent the bag from fully deflating on inhalation litres/min % An ambubag can be used for oxygen delivery alone. It cannot be used as a long term device, and your patient will need urgent review. In order to ensure the patient is receiving what is in the reservoir, you will need to hold the mask firmly over the patient s nose and mouth. Remember your target saturations range. 32
33 8. Titrating and weaning Oxygen In most cases of acute illness, oxygen therapy will be reduced gradually as the patient recovers. The need for continuing oxygen therapy must be assessed on a daily basis by the medical team and documented in the medical notes. In stable patients, if the oxygen saturations exceed the desired target range, active weaning is appropriate and encouraged. With low levels of supplemental oxygen (1L/min nasal prongs or 24% by venturi mask), stop oxygen and re-check saturations after the patient has been breathing room air for 5 minutes, then again after 15 minutes. If saturation remains in the target range on air, the health professional can discontinue oxygen therapy. Should oxygen saturations subsequently fall below the target range, oxygen may be re-started. 33
34 Weaning flow chart 34
35 9. Home oxygen Short Term Oxygen Therapy (STOT) and Long Term Oxygen Therapy (LTOT) The aim of long term oxygen therapy is to prolong life by improving organ function and reducing the risk of right sided heart failure. This needs to be prescribed by a specialist after clinical assessment with blood gases showing hypoxia of <7.3 Pa0 2 or <8.0 Pa0 2, if there is any evidence of end organ failure such as right sided heart strain, or pulmonary hypertension. Patients who have this prescribed are required to use it for a minimum of 16 hours a day to prevent R) heart strain. They can obtain most of their time on oxygen overnight whilst they are sleeping and we recommend this due to nocturnal shallow breathing. Sometime patients who meet this criteria in hospital will be sent home with Short Term Oxygen Therapy (STOT) for a period of around six weeks while they recover. They then require specialist assessment after that period to see if they still meet the criteria and can go on to have LTOT. It is important that the discharging team refer the patient to Respiratory Outpatients Clinic for review six weeks post discharge. When patients receive oxygen at home they use an oxygen concentrator. This machine extracts air and 0 2 from the atmosphere and delivers oxygen to the patient. When patients receive STOT at home, they will receive a concentrator which runs on power and is about the size of a dehumidifier. They are issued with 7.5m tubing which will allow them to mobilise around their home with their oxygen on. This allows them to keep the concentrator outside their bedroom as it can be noisy. If, after review, the patient is put on LTOT, they will receive a longer tube of 15m and also a D size back up oxygen cylinder in the event of a power cut. They can also use this this cylinder if required for appointments. Patients are entitled to have their cylinder replaced every three weeks if required. 35
36 10. Scenarios Scenario - Mrs Brown Mrs Brown is a 67 year old lady who has been admitted to your ward for supportive treatment of her COPD. Her blood gases in ED indicate that she is at risk of CO 2 retention. At the beginning of the shift her vitals were within normal range with an unaltered NEWS of 0, and she was comfortable on room air, with no shortness of breath. At 1100hrs you check in on her and notice that she is pursed lip breathing, and showing signs of accessory muscle use. You record her vitals and note the following: Heart Rate: 106 bpm, regular Blood Pressure: 152/95 Respiratory rate: 28 breaths per minute SpO 2 : 82% on room air Temperature: 36.7 o C You discuss this with the team house officer who suggests she may benefit from oxygen therapy. Which device do you think would be most appropriate, and what flow rate/settings? What would be the target saturations range for Mrs Brown? Explain your rationale. How would you document the oxygen therapy in her notes? What would be your next steps if her oxygen requirements increase/decrease? Increase Decrease 36
37 Scenario Steve Steve is a 35 year old admitted to your ward, with a history of asthma. While on the ward he mentions that he feels tightness in his chest and shortness of breath. He takes multiple breaths to tell you this information and there is an audible inspiratory wheeze. His respiratory rate is 28 breaths per minute, prior to receiving nebulised salbutamol and ipratropium. You re-check on him 15 minutes after he has finished his nebuliser and note the following: Respiratory rate: 34 breaths / minute, audible wheeze Heart rate: 123 beats/minute SpO2: 89% on room air Blood pressure: 124/78 Temperature: 36.4 o C Steve is for full Resus, and as per the NEWS algorithm you place a 777 call, and notify the ICU outreach team. What actions can you take while waiting for the team to respond? Which device do you think would be most appropriate, and what flow rate/settings? What would be the target saturations range for Steve? Explain your rationale. How would you document the oxygen therapy in his notes? What would be your next steps if his oxygen requirements increase/decrease? Increase Decrease 37
38 Scenario - Olivia Olivia is a 42 year old healthcare worker who was admitted with bilateral pneumonia. She has been receiving Q8hrly IVAB s and has been on oxygen therapy, 2 litres/min via nasal prongs. You go to administer her morning IVAB s and note that her respiratory rate is 24 resps / minute. You note that there is dry areas around her nostrils, and her e-prescribing record shows that her oxygen has been on for the past 24 hours since her admission, consistent at the rate prescribed. You note that her respiratory rate has been within normal limits after her admission to the ward, and the record from ED shows that she had a respiratory rate of 25 on admission, which resolved with oxygen. Her SpO 2 has been consistent in the low 90 s for the past 12 hours, but her increased respiratory rate has only just been noted. Her current observations are: Respiratory rate - 24 breaths/minute Heart rate - 86 beats / minute Blood Pressure 132/76 mmhg SpO 2 92% on 2 litres/minute oxygen via Nasal Prongs Temperature 37.2 o C You power-page the House Officer and advise them of the change in respiratory rate, and accompanying vitals. Which device do you think would be most appropriate, and what flow rate/settings? What would be the target saturations range for Olivia? Explain your rationale. How would you document the oxygen therapy in her notes? What would be your next steps if her oxygen requirements increase/decrease? Increase Decrease 38
39 Scenario - Meredith Meredith has been admitted to your ward with a plan for comfort cares, as she has end stage COPD, and has reached the ceiling of care provided. Her family have been involved in this decision, and have agreed to symptomatic care and support, including IVAB s and oxygen therapy. She is not for NEWS or vital signs. You are advised by her daughter (next of kin), that she is sounding rattly, and seems to be in some discomfort. You support the family to turn her, and give her some suctioning for the secretions you can hear causing the rattling that the daughter reported. She is receiving oxygen via a face mask at 6 litres/minute, which she has been receiving continuously for the past 36 hours. You notice that she is using accessory muscles, and, despite the secretions, you note that she is dry on the lips and around the mouth. You count her respiratory rate, which is 32 respirations per minute and find that her SpO 2 is 80% You page the house officer to advise them of what you have observed. Which device do you think would be most appropriate, and what flow rate/settings? What would be the target saturations range for Meredith? Explain your rationale. How would you document the oxygen therapy in her notes? What would be your next steps if her oxygen requirements increase/decrease? Increase Decrease 39
40 Scenario - Adam Adam is a 45 year old man admitted to your ward for pain management. You are looking after him for an afternoon shift, and have just taken handover from the morning nurse. For his pain he is charted: IV Morphine, as per protocol 0.5mg-2.0mg every 5 minutes, PRN Sevredol, 20mg, PO, Q1hrly, PRN Paracetemol, 1gm, Q6hrly, regularly Codeine, 60mg, PO, Q6hrly, PRN During the handover the morning nurse tells you that he has required regular morphine throughout the shift for his pain, as well as having Sevredol. The nurse states that he was consistently complaining of 8/10 pain throughout the shift, which is why he was having these doses. When rounding was done half an hour ago he was in 5/10 pain, and alert. His e-vitals record shows that his respiratory rate has been between 15 and 18 throughout the shift. His vitals have all been within normal limits. You go with the morning nurse to the bedside to introduce yourself to the patient, and find that he is unresponsive, has a respiratory rate of 6 breaths per minute, and is cyanosed on the lips. You press the emergency bell and the morning nurse goes to call 777. What actions can you take while waiting for the team to respond? Which device do you think would be most appropriate, and what flow rate/settings? What would be the target saturations range for Steve? Explain your rationale. How would you document the oxygen therapy in his notes? What would be your next steps if his oxygen requirements increase/decrease? Increase Decrease 40
41 Scenario - Jennifer Jennifer is a 67 year old female who has a L) NOF repair following mechanical fall and fracture. Her medical history consists of osteoporosis, hypertension and diverticulitis. She is on the ward 4 hours post op, she has a PCA in situ and is drowsy with a GCS of 15/15. She hasn t used her PCA for the last half hour and claims her pain is 2/10 on the pain scale. She has oxygen prescribed via the NOF protocol and has O 2, 2L via simple nasal cannulae in situ. Her current observations are: Respiratory rate - 24 breaths/minute Heart rate - 90 beats / minute Blood Pressure 127/65 mmhg SpO 2 96% on 2 litres/minute oxygen via Nasal Prongs Temperature 36.0 o C What is the most appropriate course of action in this situation? What would be the target saturations range for Jennifer? Explain your rationale. How would you document the oxygen therapy in her notes? What would be your next steps if her oxygen requirements increase/decrease? Increase Decrease 41
42 11. Key messages Oxygen is a drug which must be prescribed. A fixed delivery of oxygen device is recommended for patients at risk of C0 2 retention. In an emergency situation oxygen administration without a prescription is appropriate while waiting for medical assessment of the patient. Oxygen must be prescribed for a specific oxygen delivery device and target saturations range. If it is necessary to increase the oxygen flow rate to maintain the desired target saturation range in a previously stable patient, then a review of the patient s clinical condition by the medical team and ICU outreach is required as per the NEWS algorithm. Oxygen administration should be documented on e-vitals with the fi0 2 the patient is receiving from a controlled delivery device and the Litres of oxygen at the flow metre for variable rate (uncontrolled) delivery devices. Any patient requiring oxygen administration during transit requires the attendance of a registered nurse. Oxygen should be administered at the lowest flow that achieves the prescribed SpO 2 parameter. Nurse-led weaning of oxygen is encouraged. 42
43 12. Glossary / Terms ABGs Arterial Blood Gases ADLs Assisted Daily Living skills AH Absolute Humidity AIRVO Humidifier with PEEP ARDS Adult Respiratory Distress Syndrome b/m Breaths per Minute BiPAP Bi-level Positive Airway Pressure CHF Congestive Heart Failure cmh 2 O Centimetres of Water CNS Central Nervous System CO 2 Carbon Dioxide COPD Chronic Obstructive Pulmonary Disease CPAP Continuous Positive Airway Pressure CT Computed Tomography CVA Cerebral Vascular Accident CVS Cardio Vascular System EPAP Expiratory Positive Airway Pressure FEV1 Forced Expiratory Volume in 1 Second FiO 2 Fraction of Inspired Oxygen in a gas mixture HCO 3 Bicarbonate HMEs Heat and Moisture Exchangers Hz Hertz IPAP Inspiratory Positive Airway Pressure kpa Kilopascal LOC Level of Consciousness M3 Muscarinic acetylcholine receptor also known as the cholinergic receptors mg/l Milligrams per Litre mmhg Millimetre of Mercury mmol/l Millimoles per Litre NIPPV Non Invasive Positive Pressure Ventilation NIV Non Invasive Ventilation O 2 Oxygen PaCO 2 PaCO 2 is the partial pressure or CO2 in the alveolus PaO 2 Symbol for partial pressure of oxygen in arterial blood. pco 2 pco 2 is the partial pressure of CO 2 in blood. (There will be a small difference to PaCo 2 because of the pressure gradient across the membrane that causes CO 2 to diffuse from the blood into the lungs) ph Hydrogen Ion Measure (Acid or Alkaline) po2 Total Pressure Oxygen Gas Component R Rate RH Relative Humidity S Spontaneous S/T Spontaneous / Timed SaO 2 SaO 2 can be measured either by ABG analysis or by pulse oximetry. (SaO 2 refers to the amount o oxygen bound to haemoglobin in arterial blood.) SpO 2 SpO 2 simply means that the SaO 2 was measured using pulse oximetry. TV Tidal Volume V/Q Ventilation / Perfusion Ratio VC Vital Capacity WOB Work of Breathing β Beta2 Adrenergic Agonist 43
44 13. References Beasley, R., Chien, J., Douglas, J., Eastlake, L., Farah, C., King, G., Moore, R., Pilcher, J., Richards, M, Smith, S and Walters, H.(2015). Thoracic Society of Australia and New Zealand oxygen guidelines for acute oxygen use in adults: Swimming between the flags. Respirology.20: Cuvelier, A., & Muir, J.F. (2007). Obesity-hypoventilation syndrome and non-invasive mechanical ventilation: new insights in the Pickwick papers? Chest 131, 7-8. Higgs, D. (n.d.). Guidelines for the use of Non Invasive Ventilation (NIV) in acute respiratory failure. East Kent Hospitals NHS Trust. Masa, J.F., Celli, B. R., Riesco, J. A., Hernandez, M., Sanchez De Cos, J., & Disdier, C. (2001). The obesity hypoventilation syndrome can be treated with non-invasive mechanical ventilation. Chest 119(4), Masip, J., Roque, M., Sanchez, B., Fernandez, R., Subirana, M., & Exposito, J. A. (2005). Noninvasive ventilation in acute cardiogenic pulmonary oedema: systematic review and meta-analysis. JAMA: Journal of the American Medical Association, 294(24), Moritz, F., Brousse, B., Gellee, B., Chajara, A., L Her, E., Hellot, M. F., Bénichouet, J., al. (2007). Continuous positive airway pressure versus bi-level non-invasive ventilation in acute cardiogenic pulmonary oedema: a randomized multicentre trial. Annals of Emergency Medicine, Vol 50 issue (6), Nottingham University Hospital NHS Trust (2016), Inpatient Oxygen Therapy Policy. O Driscoll, B., Howard, L., Davison, A. (2008). Guidelines for emergency oxygen use in adult patients. Thorax.63, supplement VI. Waitemata District Health Board (2016) Oxygen Therapy Humidified High Flow Nasal Prongs. Available on WDHB Intranet Waitemata District Health Board (2016) Oxygen Therapy Inpatient and STOT ordering. Available on WDHB Intranet Williams, R., Rankin, N., Smith, T., Galler, D., & Seakins, P. Relationship between the humidity and temperature of inspired gas and the function of the airway mucosa. Crit Care Med 1996; 24(11):

45 V
Oxygen Workbook Answer book
 Oxygen Workbook Answer book 1 Produced by the Oxygen Steering Group, 2018 2 1. Pre-workbook Quiz 1. Oxygen is a drug? Y N maybe 2. Oxygen is a treatment for? breathlessness hypoxia high carbon dioxide
Oxygen Workbook Answer book 1 Produced by the Oxygen Steering Group, 2018 2 1. Pre-workbook Quiz 1. Oxygen is a drug? Y N maybe 2. Oxygen is a treatment for? breathlessness hypoxia high carbon dioxide
Chapter 10 The Respiratory System
 Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
Anatomy & Physiology 2 Canale. Respiratory System: Exchange of Gases
 Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
Oxygen: Is there a problem? Tom Heaps Acute Physician
 Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
LUNGS. Requirements of a Respiratory System
 Respiratory System Requirements of a Respiratory System Gas exchange is the physical method that organisms use to obtain oxygen from their surroundings and remove carbon dioxide. Oxygen is needed for aerobic
Respiratory System Requirements of a Respiratory System Gas exchange is the physical method that organisms use to obtain oxygen from their surroundings and remove carbon dioxide. Oxygen is needed for aerobic
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM
 CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
CHAPTER 7.1 STRUCTURES OF THE RESPIRATORY SYSTEM Pages 244-247 DO NOW What structures, do you think, are active participating in the breathing process? 2 WHAT ARE WE DOING IN TODAY S CLASS Finishing Digestion
Chapter 10. The Respiratory System Exchange of Gases. Copyright 2009 Pearson Education, Inc.
 Chapter 10 The Respiratory System Exchange of Gases http://www.encognitive.com/images/respiratory-system.jpg Human Respiratory System UPPER RESPIRATORY TRACT LOWER RESPIRATORY TRACT Nose Passageway for
Chapter 10 The Respiratory System Exchange of Gases http://www.encognitive.com/images/respiratory-system.jpg Human Respiratory System UPPER RESPIRATORY TRACT LOWER RESPIRATORY TRACT Nose Passageway for
Chapter 10 Respiration
 1 Chapter 10 Respiration Introduction/Importance of the Respiratory System All eukaryotic organisms need oxygen to perform cellular respiration (production of ATP), either aerobically or anaerobically.
1 Chapter 10 Respiration Introduction/Importance of the Respiratory System All eukaryotic organisms need oxygen to perform cellular respiration (production of ATP), either aerobically or anaerobically.
Chapter 10. Respiratory System and Gas Exchange. Copyright 2005 Pearson Education, Inc. publishing as Benjamin Cummings
 Chapter 10 Respiratory System and Gas Exchange Function of the Respiratory System To obtain oxygen (O 2 ) for all cells in the body. To rid the cells of waste gas (CO 2 ). Oxygen (O 2 ) is vital chemical
Chapter 10 Respiratory System and Gas Exchange Function of the Respiratory System To obtain oxygen (O 2 ) for all cells in the body. To rid the cells of waste gas (CO 2 ). Oxygen (O 2 ) is vital chemical
Tuesday, December 13, 16. Respiratory System
 Respiratory System Trivia Time... What is the fastest sneeze speed? What is the surface area of the lungs? (hint... think of how large the small intestine was) How many breaths does the average person
Respiratory System Trivia Time... What is the fastest sneeze speed? What is the surface area of the lungs? (hint... think of how large the small intestine was) How many breaths does the average person
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Respiratory System. Chapter 9
 Respiratory System Chapter 9 Air Intake Air in the atmosphere is mostly Nitrogen (78%) Only ~21% oxygen Carbon dioxide is less than 0.04% Air Intake Oxygen is required for Aerobic Cellular Respiration
Respiratory System Chapter 9 Air Intake Air in the atmosphere is mostly Nitrogen (78%) Only ~21% oxygen Carbon dioxide is less than 0.04% Air Intake Oxygen is required for Aerobic Cellular Respiration
The Respiratory System
 13 PART A The Respiratory System PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB Organs of the Respiratory
13 PART A The Respiratory System PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB Organs of the Respiratory
CARDIOVASCULAR AND RESPIRATORY SYSTEMS
 CARDIOVASCULAR AND RESPIRATORY SYSTEMS KEY TERMS: Cardiovascular System, cardio, vascular, blood vessels, valves, arteries, capillaries, veins, systemic circulation, pulmonary circulation Your Cardiovascular
CARDIOVASCULAR AND RESPIRATORY SYSTEMS KEY TERMS: Cardiovascular System, cardio, vascular, blood vessels, valves, arteries, capillaries, veins, systemic circulation, pulmonary circulation Your Cardiovascular
The respiratory system structure and function
 Name: Class: Date: Active reading 11A + Biology Gr11A The respiratory system structure and function The function of the respiratory system is to bring oxygen into the body and eliminate carbon dioxide
Name: Class: Date: Active reading 11A + Biology Gr11A The respiratory system structure and function The function of the respiratory system is to bring oxygen into the body and eliminate carbon dioxide
The Respiratory System Structures of the Respiratory System Structures of the Respiratory System Structures of the Respiratory System Nose Sinuses
 CH 14 D.E. Human Biology The Respiratory System The Respiratory System OUTLINE: Mechanism of Breathing Transport of Gases between the Lungs and the Cells Respiratory Centers in the Brain Function Provides
CH 14 D.E. Human Biology The Respiratory System The Respiratory System OUTLINE: Mechanism of Breathing Transport of Gases between the Lungs and the Cells Respiratory Centers in the Brain Function Provides
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
THE RESPIRATORY SYSTEM. Pages and
 THE RESPIRATORY SYSTEM Pages 103-105 and 146-150 1 When the respiratory system is mentioned, people generally think of breathing, but breathing is only one of the activities of the respiratory system.
THE RESPIRATORY SYSTEM Pages 103-105 and 146-150 1 When the respiratory system is mentioned, people generally think of breathing, but breathing is only one of the activities of the respiratory system.
Non-invasive Ventilation protocol For COPD
 NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
Chapter 11 The Respiratory System
 Biology 12 Name: Respiratory System Per: Date: Chapter 11 The Respiratory System Complete using BC Biology 12, page 342-371 11.1 The Respiratory System pages 346-350 1. Distinguish between A. ventilation:
Biology 12 Name: Respiratory System Per: Date: Chapter 11 The Respiratory System Complete using BC Biology 12, page 342-371 11.1 The Respiratory System pages 346-350 1. Distinguish between A. ventilation:
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
About the Respiratory System. Respiratory System. Human Respiratory System. Cellular Respiration. Nostrils. Label diagram
 Respiratory System Human Respiratory System A system to deliver oxygen (O2) to body cells & get rid of carbon dioxide (CO2) as a waste through cellular respiration. Two systems involved: Respiratory &
Respiratory System Human Respiratory System A system to deliver oxygen (O2) to body cells & get rid of carbon dioxide (CO2) as a waste through cellular respiration. Two systems involved: Respiratory &
B Unit III Notes 6, 7 and 8
 The Respiratory System Why do we breathe? B. 2201 Unit III Notes 6, 7 and 8 Respiratory System We know that our cells respire to produce ATP (energy). All organisms need energy to live, so that s why we
The Respiratory System Why do we breathe? B. 2201 Unit III Notes 6, 7 and 8 Respiratory System We know that our cells respire to produce ATP (energy). All organisms need energy to live, so that s why we
5/5/2013. The Respiratory System. Chapter 16 Notes. The Respiratory System. Nasal Cavity. Sinuses
 The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
The Respiratory System Chapter 16 Notes The Respiratory System Objectives List the general functions of the respiratory system. Identify the organs of the respiratory system. Describe the functions of
ADVANCED ASSESSMENT Respiratory System
 ONTARIO BASE HOSPITAL GROUP QUIT ADVANCED ASSESSMENT Respiratory System 2007 Ontario Base Hospital Group ADVANCED ASSESSMENT Respiratory System AUTHOR(S) Mike Muir AEMCA, ACP, BHSc Paramedic Program Manager
ONTARIO BASE HOSPITAL GROUP QUIT ADVANCED ASSESSMENT Respiratory System 2007 Ontario Base Hospital Group ADVANCED ASSESSMENT Respiratory System AUTHOR(S) Mike Muir AEMCA, ACP, BHSc Paramedic Program Manager
Phases of Respiration. Chapter 18: The Respiratory System. Structures of the Respiratory System. Structures of the Respiratory System
 Phases of Respiration Chapter 18: The Respiratory System Respiration Process of obtaining oxygen from environment and delivering it to cells Phases of Respiration 1. Pulmonary ventilation between air and
Phases of Respiration Chapter 18: The Respiratory System Respiration Process of obtaining oxygen from environment and delivering it to cells Phases of Respiration 1. Pulmonary ventilation between air and
Chapter 10 Lecture Outline
 Chapter 10 Lecture Outline See separate PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright 2016 McGraw-Hill Education. Permission required for reproduction
Chapter 10 Lecture Outline See separate PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright 2016 McGraw-Hill Education. Permission required for reproduction
The primary function of the respiratory system is to supply the blood with oxygen in order for the blood to deliver oxygen to all parts of the body.
 Respiratory System The primary function of the respiratory system is to supply the blood with oxygen in order for the blood to deliver oxygen to all parts of the body. The respiratory system does this
Respiratory System The primary function of the respiratory system is to supply the blood with oxygen in order for the blood to deliver oxygen to all parts of the body. The respiratory system does this
The Respiratory System
 BIOLOGY OF HUMANS Concepts, Applications, and Issues Fifth Edition Judith Goodenough Betty McGuire 14 The Respiratory System Lecture Presentation Anne Gasc Hawaii Pacific University and University of Hawaii
BIOLOGY OF HUMANS Concepts, Applications, and Issues Fifth Edition Judith Goodenough Betty McGuire 14 The Respiratory System Lecture Presentation Anne Gasc Hawaii Pacific University and University of Hawaii
Energy is needed for cell activities: growth,reproduction, repair, movement, etc...
 Respiration Energy is needed for cell activities: growth,reproduction, repair, movement, etc... Metabolism refers to all of the chemical reactions in the body, where molecules are synthesized (anabolism)
Respiration Energy is needed for cell activities: growth,reproduction, repair, movement, etc... Metabolism refers to all of the chemical reactions in the body, where molecules are synthesized (anabolism)
Circulatory System. and. Respiratory System. Ari Min, Yerim Lee and Min Ji Song THE HEART LUNGS. Monday, May 23, 2011
 Human Anatomy Circulatory System and THE HEART Respiratory System LUNGS Ari Min, Yerim Lee and Min Ji Song Purpose of the Circulatory System Function of circulatory system: exchange gases with cardiovascular
Human Anatomy Circulatory System and THE HEART Respiratory System LUNGS Ari Min, Yerim Lee and Min Ji Song Purpose of the Circulatory System Function of circulatory system: exchange gases with cardiovascular
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Unit 9. Respiratory System 16-1
 Unit 9 Respiratory System 16-1 Works together with the circulatory system Exchange of gases between atmosphere, blood, and cells If respiratory system and/or circulatory system fails, death will occur
Unit 9 Respiratory System 16-1 Works together with the circulatory system Exchange of gases between atmosphere, blood, and cells If respiratory system and/or circulatory system fails, death will occur
The Respiratory System. Dr. Ali Ebneshahidi
 The Respiratory System Dr. Ali Ebneshahidi Functions of The Respiratory System To allow gases from the environment to enter the bronchial tree through inspiration by expanding the thoracic volume. To allow
The Respiratory System Dr. Ali Ebneshahidi Functions of The Respiratory System To allow gases from the environment to enter the bronchial tree through inspiration by expanding the thoracic volume. To allow
COPD Challenge CASE PRESENTATION
 Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE
 VAPOTHERM POCKET GUIDE") Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Overview. The Respiratory System. Chapter 18. Respiratory Emergencies 9/11/2012
 Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Respiratory System. Introduction. Atmosphere. Some Properties of Gases. Human Respiratory System. Introduction
 Introduction Respiratory System Energy that we consume in our food is temporarily stored in the bonds of ATP (adenosine triphosphate) before being used by the cell. Cells use ATP for movement and to drive
Introduction Respiratory System Energy that we consume in our food is temporarily stored in the bonds of ATP (adenosine triphosphate) before being used by the cell. Cells use ATP for movement and to drive
Respiratory System. Student Learning Objectives:
 Respiratory System Student Learning Objectives: Identify the primary structures of the respiratory system. Identify the major air volumes associated with ventilation. Structures to be studied: Respiratory
Respiratory System Student Learning Objectives: Identify the primary structures of the respiratory system. Identify the major air volumes associated with ventilation. Structures to be studied: Respiratory
Chapter 16. Respiratory System
 Chapter 16 Respiratory System Introduction Respiration = the entire process of exchanging gases between the atmosphere and body cells 1. Ventilation 2. Gas exchange 3. Gas transport : 4. Cellular respiration
Chapter 16 Respiratory System Introduction Respiration = the entire process of exchanging gases between the atmosphere and body cells 1. Ventilation 2. Gas exchange 3. Gas transport : 4. Cellular respiration
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4
 INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients
 Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Function: to supply blood with, and to rid the body of
 1 2 3 4 5 Bio 1102 Lec. 7 (guided): Chapter 10 The Respiratory System Respiratory System Function: to supply blood with, and to rid the body of Oxygen: needed by cells to break down food in cellular respiration
1 2 3 4 5 Bio 1102 Lec. 7 (guided): Chapter 10 The Respiratory System Respiratory System Function: to supply blood with, and to rid the body of Oxygen: needed by cells to break down food in cellular respiration
Respiratory System. December 20, 2011
 Respiratory System December 20, 2011 Nasal Cavity: Contains cilia (hair cells) to prevent particles from entering the respiratory tract Mucus does the same, in addition to warming and moistening the air
Respiratory System December 20, 2011 Nasal Cavity: Contains cilia (hair cells) to prevent particles from entering the respiratory tract Mucus does the same, in addition to warming and moistening the air
The respiratory system
 The respiratory system Practical 1 Objectives Respiration, ventilation Intrapleural and intrapulmonary pressure Mechanism of inspiration and expiration Composition of the atmosphere and the expired air
The respiratory system Practical 1 Objectives Respiration, ventilation Intrapleural and intrapulmonary pressure Mechanism of inspiration and expiration Composition of the atmosphere and the expired air
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Questions 1-3 refer to the following diagram. Indicate the plane labeled by the corresponding question number.
 Name: Grade: ANATOMY TEST Questions 1-3 refer to the following diagram. Indicate the plane labeled by the corresponding question number. 1. Plane #1 is the... 2. Plane #2 is the... 3. Plane #3 is the...
Name: Grade: ANATOMY TEST Questions 1-3 refer to the following diagram. Indicate the plane labeled by the corresponding question number. 1. Plane #1 is the... 2. Plane #2 is the... 3. Plane #3 is the...
Respiratory System Functions. Respiratory System Organization. Respiratory System Organization
 Respiratory System Functions Functions of Respiratory System Gas exchange between blood and air Move air to and from exchange surfaces Protect exchange surfaces from environmental variations and pathogens
Respiratory System Functions Functions of Respiratory System Gas exchange between blood and air Move air to and from exchange surfaces Protect exchange surfaces from environmental variations and pathogens
Indications for Respiratory Assistance. Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer
 Indications for Respiratory Assistance Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer Respiratory Assistance Non-invasive - Nasal specs - Facemask/ Resevoir
Indications for Respiratory Assistance Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer Respiratory Assistance Non-invasive - Nasal specs - Facemask/ Resevoir
Chapter 13. The Respiratory System.
 Chapter 13 The Respiratory System https://www.youtube.com/watch?v=hc1ytxc_84a https://www.youtube.com/watch?v=9fxm85fy4sq http://ed.ted.com/lessons/what-do-the-lungs-do-emma-bryce Primary Function of Breathing
Chapter 13 The Respiratory System https://www.youtube.com/watch?v=hc1ytxc_84a https://www.youtube.com/watch?v=9fxm85fy4sq http://ed.ted.com/lessons/what-do-the-lungs-do-emma-bryce Primary Function of Breathing
Chronic inflammation of the airways Hyperactive bronchi Shortness of breath Tightness in chest Coughing Wheezing
 Chronic inflammation of the airways Hyperactive bronchi Shortness of breath Tightness in chest Coughing Wheezing Components of the respiratory system Nasal cavity Pharynx Trachea Bronchi Bronchioles Lungs
Chronic inflammation of the airways Hyperactive bronchi Shortness of breath Tightness in chest Coughing Wheezing Components of the respiratory system Nasal cavity Pharynx Trachea Bronchi Bronchioles Lungs
10/17/2016 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT COURSE OBJECTIVES COMMON CAUSES OF RESPIRATORY FAILURE
 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
Phases of Respiration
 Phases of Respiration We get oxygen from the environment and it goes to our cells, there. Pulmonary ventilation External exchange of gases Internal exchange of gases Overview of respiration. In ventilation,
Phases of Respiration We get oxygen from the environment and it goes to our cells, there. Pulmonary ventilation External exchange of gases Internal exchange of gases Overview of respiration. In ventilation,
1.1.2 CPAP therapy is used for patients who are suffering from an acute type 1 respiratory failure (Pa02 <8kPa with a normal or low Pac02).
.") Guidelines for initiating and managing CPAP (Continuous Positive Airway Pressure) on a general ward. B25/2006 1.Introduction and Who Guideline applies to 1.1.1 This document provides guidance for Healthcare
Guidelines for initiating and managing CPAP (Continuous Positive Airway Pressure) on a general ward. B25/2006 1.Introduction and Who Guideline applies to 1.1.1 This document provides guidance for Healthcare
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
(To be filled by the treating physician)
") CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
The Respiratory System
 The Respiratory System By Mr. Danilo Villar Rogayan Jr. Instructor I, Department of Natural Sciences RMTU San Marcelino Introduction Function Move air in an out of lungs (ventilation) Delivers oxygen (O
The Respiratory System By Mr. Danilo Villar Rogayan Jr. Instructor I, Department of Natural Sciences RMTU San Marcelino Introduction Function Move air in an out of lungs (ventilation) Delivers oxygen (O
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy
 Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy Disclaimer This material is intended for use by trained family members and caregivers of children with tracheostomies who are
Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy Disclaimer This material is intended for use by trained family members and caregivers of children with tracheostomies who are
Anatomy. The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs.
 Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning
 CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
The Human Respiration System
 The Human Respiration System Nasal Passage Overall function is to filter, warm and moisten air as it enters the body. The nasal passages are the primary site of air movement we tend to be nose breathers.
The Human Respiration System Nasal Passage Overall function is to filter, warm and moisten air as it enters the body. The nasal passages are the primary site of air movement we tend to be nose breathers.
Chapter 16. The Respiratory System. Mosby items and derived items 2010, 2006, 2002, 1997, 1992 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 16 The Respiratory System Objectives Discuss the generalized functions of the respiratory system List the major organs of the respiratory system and describe the function of each Compare, contrast,
Chapter 16 The Respiratory System Objectives Discuss the generalized functions of the respiratory system List the major organs of the respiratory system and describe the function of each Compare, contrast,
Your Lungs and COPD. Patient Education Pulmonary Rehabilitation. A guide to how your lungs work and how COPD affects your lungs
 Patient Education Your Lungs and COPD A guide to how your lungs work and how COPD affects your lungs Your lungs are organs that process every breath you take. They provide oxygen (O 2 ) to the blood and
Patient Education Your Lungs and COPD A guide to how your lungs work and how COPD affects your lungs Your lungs are organs that process every breath you take. They provide oxygen (O 2 ) to the blood and
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Respiratory Failure in the Pediatric Patient
 Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Respiratory System Mechanics
 M56_MARI0000_00_SE_EX07.qxd 8/22/11 3:02 PM Page 389 7 E X E R C I S E Respiratory System Mechanics Advance Preparation/Comments 1. Demonstrate the mechanics of the lungs during respiration if a bell jar
M56_MARI0000_00_SE_EX07.qxd 8/22/11 3:02 PM Page 389 7 E X E R C I S E Respiratory System Mechanics Advance Preparation/Comments 1. Demonstrate the mechanics of the lungs during respiration if a bell jar
NHS Training for Physiotherapy Support Workers. Workbook 14 The respiratory system
 NHS Training for Physiotherapy Support Workers Workbook 14 The respiratory system Contents Workbook 14 The respiratory system 1 14.1 Aim 3 14.2 Learning outcomes 3 14.3 The respiratory system 4 14.4 Breathing
NHS Training for Physiotherapy Support Workers Workbook 14 The respiratory system Contents Workbook 14 The respiratory system 1 14.1 Aim 3 14.2 Learning outcomes 3 14.3 The respiratory system 4 14.4 Breathing
Respiratory system. Applied Anatomy &Physiology
 Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
Respiratory system Applied Anatomy &Physiology Anatomy The respiratory system consists of 1)The Upper airway : Nose, mouth and larynx 2)The Lower airways Trachea and the two lungs. Within the lungs,
The RESPIRATORY System. Unit 3 Transportation Systems
 The RESPIRATORY System Unit 3 Transportation Systems Functions of the Respiratory System Warm, moisten, and filter incoming air Resonating chambers for speech and sound production Oxygen and Carbon Dioxide
The RESPIRATORY System Unit 3 Transportation Systems Functions of the Respiratory System Warm, moisten, and filter incoming air Resonating chambers for speech and sound production Oxygen and Carbon Dioxide
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
The RESPIRATORY System. Unit 3 Transportation Systems
 The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
The RESPIRATORY System Unit 3 Transportation Systems The Respiratory System Functions of the Respiratory System Warms, moistens, and filters incoming air Nasal cavity Resonating chambers for speech and
Respiratory System. BSC 2086 A&P 2 Professor Tcherina Duncombe Palm Beach State College
 Respiratory System BSC 2086 A&P 2 Professor Tcherina Duncombe Palm Beach State College Respiration Ventilation of lungs Gas exchange between air/bld and bld/tissue Use of oxygen in cellular respiration
Respiratory System BSC 2086 A&P 2 Professor Tcherina Duncombe Palm Beach State College Respiration Ventilation of lungs Gas exchange between air/bld and bld/tissue Use of oxygen in cellular respiration
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Tissue Hypoxia and Oxygen Therapy
 Tissue Hypoxia and Oxygen Therapy ก ก ก ก ก ก 1. ก ก 2. ก ก 3. tissue hypoxia 4. ก ก ก 5. ก ก ก 6. ก กก ก 7. ก ก tissue hypoxia ก ก ก ก 1. Pathway of oxygen transport 2. Causes of tissue hypoxia 3. Effect
Tissue Hypoxia and Oxygen Therapy ก ก ก ก ก ก 1. ก ก 2. ก ก 3. tissue hypoxia 4. ก ก ก 5. ก ก ก 6. ก กก ก 7. ก ก tissue hypoxia ก ก ก ก 1. Pathway of oxygen transport 2. Causes of tissue hypoxia 3. Effect
? Pulmonary Respiratory System
 The Structure of The Respiratory System The respiratory system is composed of groups of organelles that filters and transports air into the lungs. The organs comprising of the respiratory system include
The Structure of The Respiratory System The respiratory system is composed of groups of organelles that filters and transports air into the lungs. The organs comprising of the respiratory system include
Respiratory Physiology
 Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Bronchospasm & SOB. Kim Kilmurray Senior Clinical Teaching Fellow
 Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Chapter 11. The respiratory system. Glossary. Anthony Wheeldon
 Chapter 11 The respiratory system Anthony Wheeldon Glossary Accessory muscles Muscles not normally involved in respiration that can be utilised to increase inspiration. Acid base balance The mechanisms
Chapter 11 The respiratory system Anthony Wheeldon Glossary Accessory muscles Muscles not normally involved in respiration that can be utilised to increase inspiration. Acid base balance The mechanisms
OXYGEN USE IN PHYSICAL THERAPY PRACTICE. Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR
 OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
Unit 14: The Respiratory System
 Unit 14: The Respiratory System See what you already know! 1. Fill in the diagram on your own 2. Collaborate with your partner The Respiratory System The major function of the respiratory system is gas
Unit 14: The Respiratory System See what you already know! 1. Fill in the diagram on your own 2. Collaborate with your partner The Respiratory System The major function of the respiratory system is gas
Asthma Management Introduction, Anatomy and Physiology
 Asthma Management Introduction, Anatomy and Physiology University of Utah Center for Emergency Programs and The Utah Asthma Program Incidence, Impact and Goals of Asthma Management Prevalence, Morbidity
Asthma Management Introduction, Anatomy and Physiology University of Utah Center for Emergency Programs and The Utah Asthma Program Incidence, Impact and Goals of Asthma Management Prevalence, Morbidity
Respiratory System. Organization of the Respiratory System
 Respiratory System In addition to the provision of oxygen and elimination of carbon dioxide, the respiratory system serves other functions, as listed in (Table 15 1). Respiration has two quite different
Respiratory System In addition to the provision of oxygen and elimination of carbon dioxide, the respiratory system serves other functions, as listed in (Table 15 1). Respiration has two quite different
Firefighter Pre-Hospital Care Program Recruit Presentation. Respiratory Emergencies
 Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
Firefighter Pre-Hospital Care Program Recruit Presentation Respiratory Emergencies The Respiratory System Anatomy Pharynx Nasopharynx Oropharynx Epiglottis Larynx Trachea Right main bronchus Left main
The respiratory system has multiple organs, we will begin with the nose and nasal cavity.
 Respiratory System (Peer reviewed and edited) Slide 1: Respiratory System Slide 2: Functions Functions of respiratory system include gas exchange, communication, olfaction, and ph regulation. Gas exchange
Respiratory System (Peer reviewed and edited) Slide 1: Respiratory System Slide 2: Functions Functions of respiratory system include gas exchange, communication, olfaction, and ph regulation. Gas exchange
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
The Respiratory System
 Essentials of Human Anatomy & Physiology Elaine N. Marieb Seventh Edition Chapter 13 The Respiratory System Slides 13.1 13.30 Lecture Slides in PowerPoint by Jerry L. Cook Copyright 2003 Pearson Education,
Essentials of Human Anatomy & Physiology Elaine N. Marieb Seventh Edition Chapter 13 The Respiratory System Slides 13.1 13.30 Lecture Slides in PowerPoint by Jerry L. Cook Copyright 2003 Pearson Education,
Lab Activity 27. Anatomy of the Respiratory System. Portland Community College BI 233
 Lab Activity 27 Anatomy of the Respiratory System Portland Community College BI 233 1 Terminology Pulmonary Ventilation: aka breathing, is the movement of air into and out of the lungs External Respiration:
Lab Activity 27 Anatomy of the Respiratory System Portland Community College BI 233 1 Terminology Pulmonary Ventilation: aka breathing, is the movement of air into and out of the lungs External Respiration:
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory