The management of B3 lesions with emphasis on lobular neoplasia
|
|
|
- Sharyl Casey
- 6 years ago
- Views:
Transcription
1 The management of B3 lesions with emphasis on lobular neoplasia Abeer Shaaban Queen Elizabeth Hospital Birmingham
2 NHSBSP core biopsy categories B1 - Normal B2 - Benign B3 Uncertain malignant potential B4 Suspicious of Malignancy B5 Malignant
3 B3 category Proportion: 5-9% of core biopsy diagnoses Includes lesions of variable significance. Diagnostically challenging! Includes lesions with and without atypia. Requires further sampling: traditionally by surgery.
4 B3 lesions FEA AIDP Lobular in situ neoplasia Papilloma Radial scar Fibroaepithelial lesion Mucocoele like lesion Other: spindle cell lesions, apocrine atypia
5 Factors affecting frequency & upgrade rate Patient population: screening vs symptomatic Method of biopsy: NCB vs VAB (gauge of needle) Type and combination of B3 lesion Size of lesion Presence/absence of atypia
6 Papillary lesions Without atypia: 3.8% Noyak et al % Youk et al 2011 (age, size) With atypia 33% (vs 3%) McGhan et al 2013 Radial scar Without atypia (4-9%) With atypia Mucocoele - like lesion Without atypia 4% With atypia 21% (24-44%) Histopathology 2008;52:650, Brenner et al 2002 Rakha et al, Histopathology 2013
7 UPGRADE RATES: FEA + AIDP Study FEA FEA + AIDP Lee et al (2010) Rakha et al (2011a, b) Rajan et al (2011) AIDP 14% 29% 37% 21% 14% 29% 50.4% 40% 19% 29% 53% Total 18% 29% 44%
8 Why is there need for B3 management standardisation?
9 1. Management is inconsistent across screening units. 2. Increasing use of VAB 3. Over-treatment is a recognised issue 4. Local guidelines: Leeds, London QARC
10 National survey to all breast screening units in England 46 breast screening units responded (58% response rate) Filled out by: Radiologist 40 Clinician 4 Radiographer 2 28 units perform First line vacuum assisted biopsy (VAB) 37 units performed Second line VAB


11 B3 lesions with no atypia radial scar/papilloma with no atypia If conventional 14G core biopsy shows B3 lesion with no atypia 34 units responded 74% will offer second line VAB 26% will offer Surgical Diagnostic Biopsy If 1st line VAB shows B3 lesion with no atypia 27 units 41% will offer second line VAB 44% will offer Surgical biopsy 15% will discharge due to adequate sampling
12 Management of B3 lesion with atypia on 14G core biopsy 2 nd line VAB Surgical biopsy Discharge FEA AIDP AIDP + FEA ALH LCIS Radial scar + atypia Papilloma + atypia EC
13 Management of B3 lesion with atypia on VAB 2 nd line VAB Surgical biopsy Discharge FEA AIDP AIDP + FEA ALH LCIS Radial scar + atypia Papilloma + atypia EC
14 Benign open biopsy rate - prevalent (first) screens (per 1,000 women screened) Benign open biopsies Leeds prevalent open biopsy rate 0.9 UK benign open biopsy rates 1.73 per 1,000 women screened (Prevalent) 0.48 per 1,000 women screened (Incident) UK average: 1.74 Minimum std: 1.5 Target:
15 Increasing use of VAB

16 Core samples 1 st line VAB 2 nd line VAB With thanks to Dr Nisha Sharma
17 Vacuum-assisted core biopsy of breast lesions of uncertain malignant potential (B3) an alternative to surgery in selected cases Tennant et al. Breast 2008;17:456 Papillary lesions and radial scars without atypia
18 Over-treatment is a recognised issue
19 B3 Positive predictive value 21% Dillon et al 2007 (Ireland) 20% El-Sayed et al % Rakha et al (NCB) 21.2% Bianchi et al cases (VACNB Study group, Italy) 20% Strachan et al 2015, under review, 398
20 The majority of patients (75-80%) with B3 diagnosis will have a benign histology on further sampling. Is surgical excision necessary?
21 Local guidelines such as London QARC and Leeds pathway have been developed
22 Local guidelines


23

24 Leeds pathway for B3 lesion with atypia
25 Aim to adequately sample by VAB to rule out coexistent cancer Follow up
26 Lobular neoplasia Encompasses atypical lobular hyperplasia (ALH) and lobular in situ carcinoma (LCIS). LCIS: classical and variants
27 Classical LCIS Disease of premenopausal women (90%) Most LCIS diagnosed between yrs. Often multifocal (60-80%) and bilateral (up to 35%) True incidence is difficult to assess (reported between % (Haagenson 1978, Page 1991)
28 Classical LCIS Presents on mammographic screening but can also be incidental. Risk of malignancy is x3 likely to be unilateral than bilateral (Page et al 2003)

29 LCIS Marker of breast cancer risk: RR 8-10 Direct precursor: LOH: in LCIS and the associated lobular ca: 17q, 17p, 11q. Lakhani 1995, Nayae 1997 Mutation of the e-cadherin gene: in LCIS and invasive lobular ca, Berx et al., 1996
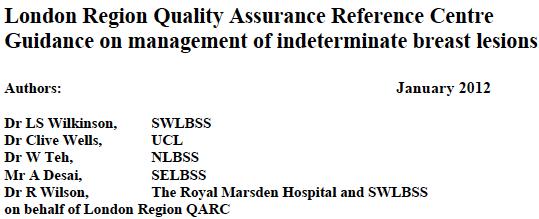
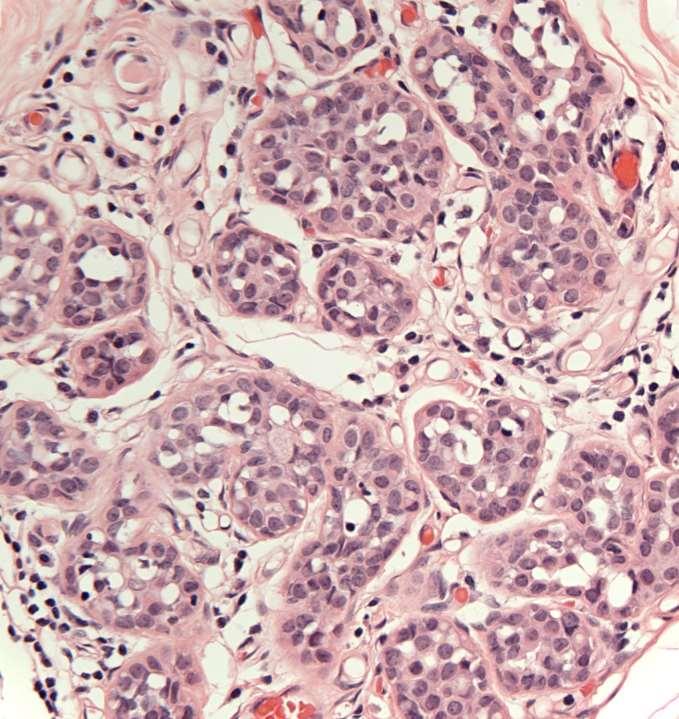
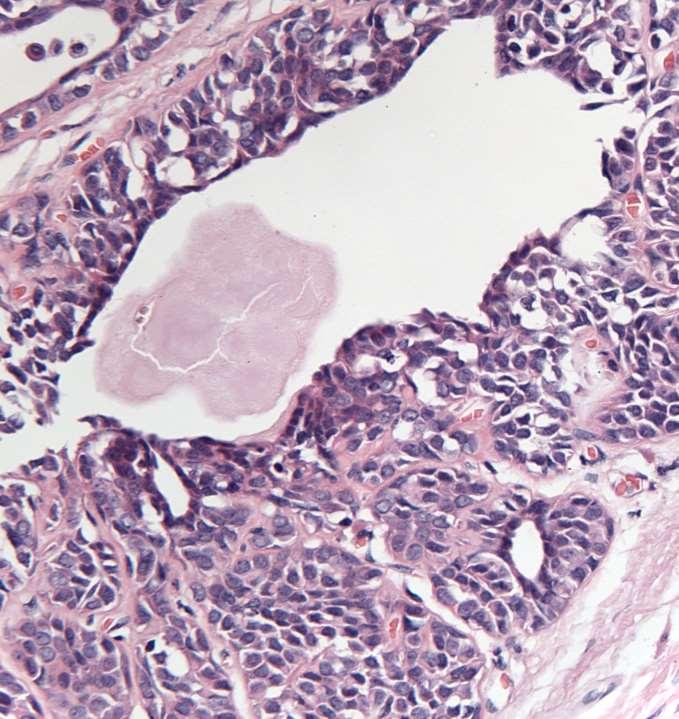
30 Histologically A monomorphic proliferation within TDLU of dyscohesive cells with uniform round nuclei, indistinct nucleoli and scant cytoplasm. Intracytoplasmic lumina are often present Pagetoid spread can be seen.
31 Type A cells: small uniform cells with bland nuclei and scant cytoplasm Type B cells: cells are larger, with more cytoplasm and mild to moderate atypia
32 Type A
33 Type B
34 Type B
35

36 E-cadherin
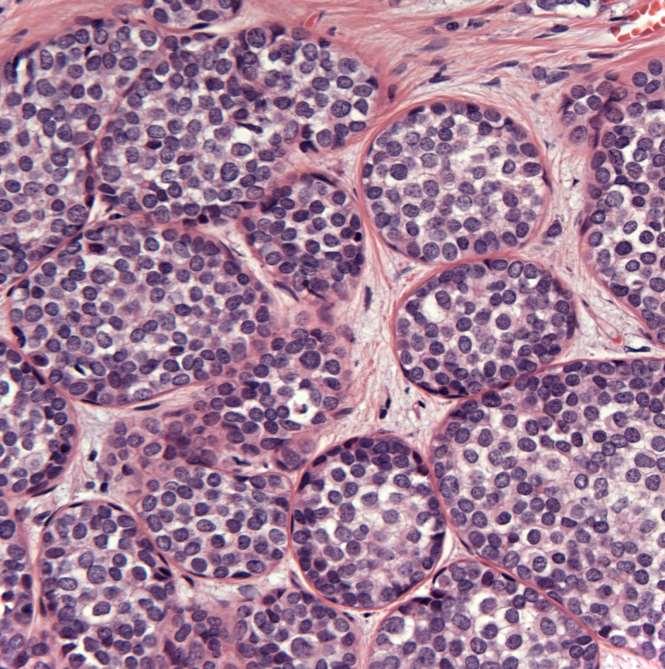
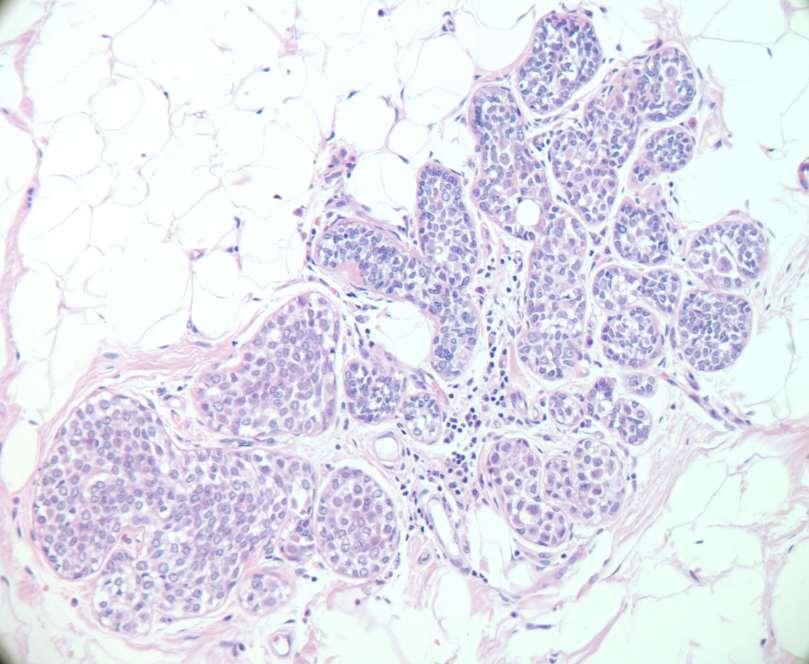
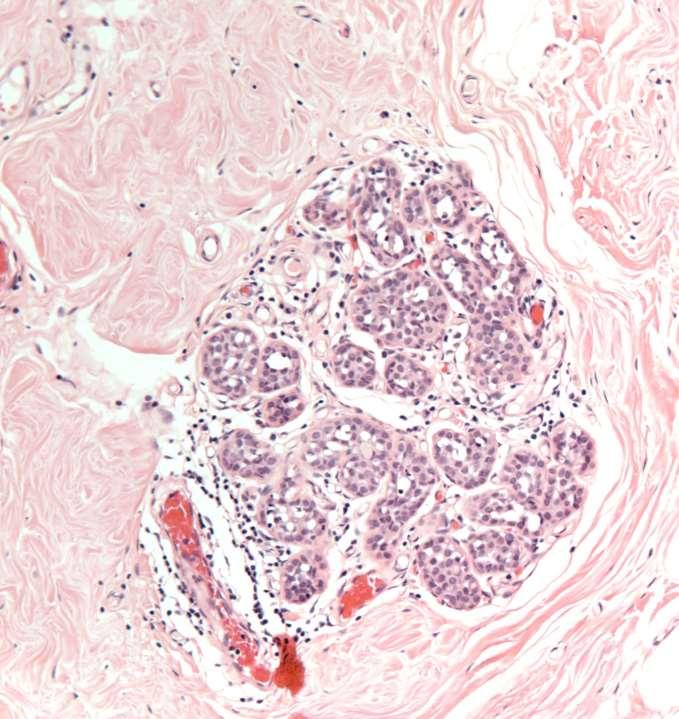
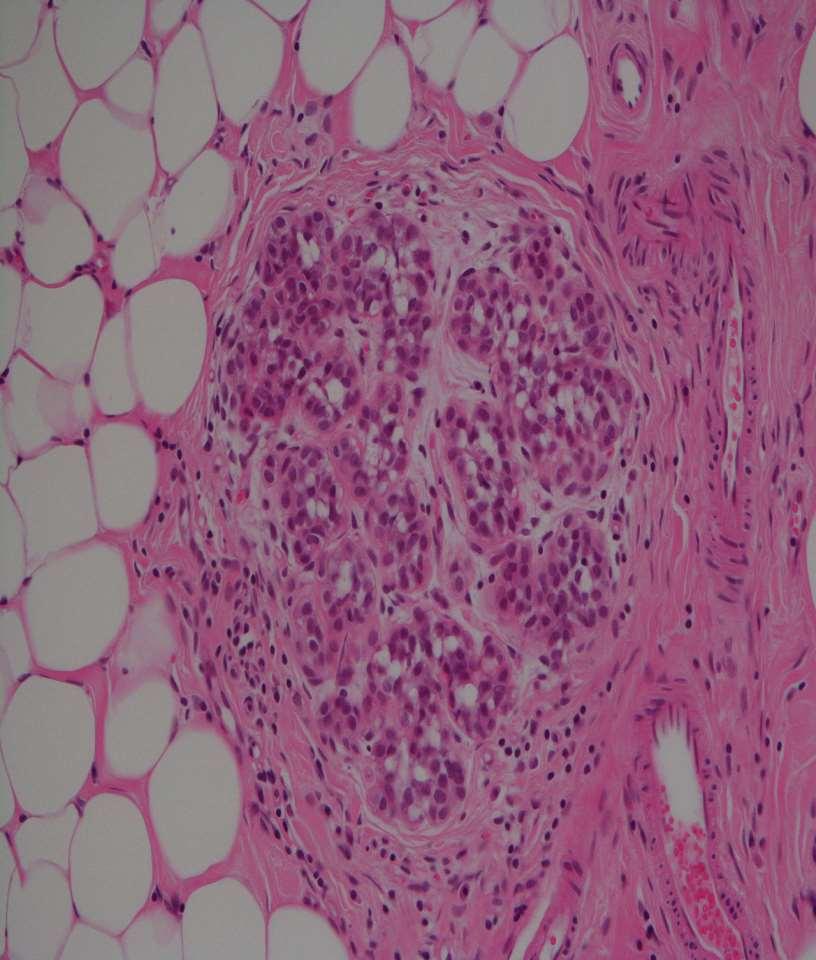
37 ALH vs LCIS Depends on extent of lesion LCIS: more than half of the acini are filled, distended and distorted by the dyscohesive lobular cells.
38 ALH
39 ALH
40 DD: LCIS vs DCIS Cellular cohesion Look for architectural pattern of DCIS E-cadherin

41 E-cadherin
42 Variants of LCIS Pleomorphic LCIS (PLCIS)

43 PLCIS A more recently recognized variant of Lobular Carcinoma In Situ (LCIS) May calcify hence present through breast screening Biology and natural history uncertain Histologically: mimics high grade DCIS

44

45

46

47 E-cadherin
48 Rare variant of LCIS LCIS with comedo necrosis A study of 18 cases reported a strong association with invasive ca (67% of cases) Fadare et al Am J Surg Pathol :

49

50
51 LCIS upgrade rate Ranged from 0-60%, (majority 2-25%), Buckley et al 2014 systematic review, Murray et al 2013 Upgrade rate 3% in concordant and 38% if imaging-pathological discordant, Murray et al ALH upgrade rate (27%) not significantly different from LCIS (33%), Ibrahim et al 2012
52 Reasons for variation Screening vs symptomatic Radiological correlation Amount of tissue : core vs VAB LCIS in structured lesions Family history vs sporadic Inclusion of PLCIS Co-existing other lesions as ADH
53 Upgrade rate of PLCIS 41%, range 30-60%, Hussain and Cunnick 2011, Carder et al 2011
54 Variability in LN management Surgical excision: as some patients may have a co-existing invasive malignancy (ABS/BASO guidelines 2009) Observation/radiological monitoring: LN without radiological pathological discordance (Meroni et AL 2014) Surgical excision mandatory only if radiological-pathological discordance (Capobiancoet al 2014) VAB as alternative to surgical excision (Parkin et al 2014)
55 B3 guidelines group Commissioned by NHSBSP Invited members representing imaging, surgery and pathology
56 Composition of the B3 group Chair: Prof Sarah Pinder Radiologists: Louise Wilkinson, Nisha Sharma Surgeons: Simon Pain, Anil Desai, Ashu Gandhi Pathologists: Sarah Pinder, Andrew Lee, Abeer Shaaban
57 B3 Guidelines Group Remit To undertake review of the literature on lesions categorised as B3 To come up with guideline document for a practical approach to management of these for the NHS BSP.
58 Progress First meeting: October 2014 Management recommendations lesion by lesion. Use of diagrams/flow charts General principles: radiological/pathological concordance Draft for discussion/consultation
59 Recommendations 2 nd line VAB as method of choice for further sampling of B3 lesions, following either conventional core or 1 st line VAB B3 diagnosis. All cases should be discussed at MDT meeting Centres should plan to acquire 2 nd line VAB or refer to a centre that can do it Diagnostic excision for fibroepithelial lesions, spindle cell lesions, papilloma with atypia
60 B3 Lobular Neoplasia pathway B3 Lobular neoplasia on 14g or 1 st line VAB 2 nd line VAB >3.5g MDT discussion No further disease or LN only, rad/path concordance No further disease or LN only, rad/path non-concordance DCIS, PLCIS, Invasive MDT Meeting Annual mammography Diagnostic surgery & subsequent management as per findings Therapeutic surgery
61 Advantages of 2 nd line VAB For patients Targeted sampling: less tissue removed. Outpatient procedure, well tolerated by patients. Avoid complication of anaesthesia and surgery No scarring, easier further imaging and assessment. Rapid turnaround of results.
62 Advantages of 2 nd line VAB For MDT Improves pre-operative diagnosis rate. Reduces benign surgical biopsy rate. Planning therapeutic surgery for cancer patients. Reducing the risk of over-treatment

63 Reduction in benign diagnostic surgery From Dr S Rajan
64 Lobular neoplasia on core biopsy ALH/Classical LCIS: code as B3 and recommend further tissue examination by VAB PLCIS: code as B5a and manage as DCIS LCIS with necrosis: rare, best coded as B4, recommend surgical excision.
65 B3 management FAQ How to deal with extensive calcification?
66 Sample two ends/areas of the lesion by 1 st line VAB If B3, proceed to 2 nd line VAB
67 Does the management vary in presence/absence of atypia?
68 49 cases of radial scar without atypia In 9 cases (18.3%): atypia on surgical excision. Conclusion: diagnosis of RS without atypia does not exclude malignancy. Further sampling by VAB or surgical excision is required

69 Rakha et al 2014
70 Does the management vary if B3 lesion shows atypia vs no atypia? Overall : No Further sampling is required for papillomas/radial scars without atypia (unless lesion completely removed radiologically) Guidelines recommend excision of papilloma with atypia to assess size (for DCIS size cut off)
71 Does the pathway differ if first sample is by conventional core or VAB?
72 No The purpose of the first biopsy (14 g core or VAB) is to obtain a small sample to make a diagnosis
73 If a centre is doing first line VAB sampling, should they still do 2 nd line VAB for B3 lesions?
74 Yes First line VAB is a limited sample for initial diagnosis. An adequate, representative sample to exclude malignancy cannot be achieved by 1 st line VAB
75 22 Italian centres 3107 B3 VAB diagnoses 1644 (54.2%) underwent surgical excision Overall PPV: 21.2 %
76 VAB upgrade Lesion PPV (%) Pure ADH 27.3 FEA 12.7 ALH 24.2 LIN 22 RS 10.6 All B3 21.2
77 What if a unit cannot implement 2 nd line VAB?
78 Units should try to implement 2 nd line VAB Otherwise, they should refer to another centre that provides the service. The group felt they should recommend what is best for patients.
79 Majority of UK units have 1 st line VAB It is hoped that the guidelines will be a catalyst to enable units to justify a business case and implement the pathway
80 Should 2nd line VAB aim to excise the whole lesion?
81 Not necessarily, depending on size The aim is to obtain further tissue and a representative sample to exclude coexistent malignancy The group will provide guidance on what represents adequate sampling
82 Should we therefore aim to always extensively sample on 1 st line VAB/sample all calcification?
83 No. 1 st line VAB/cores are meant to provide a small sample for diagnosis and not to remove the whole abnormality It may be feasible to fully sample a small area of calcification However, it would not be justified to excessively sample all patients by 1 st line VAB
84 How much tissue should be taken by second line VAB?
85 Standard is: cores, 7 or 8g needle, or equivalent to 3.5 gm 2 nd line VAB is targeted sampling. While tissue taken is less than a diagnostic excision, it is likely to be more representative
86 Should incidental lesions such as incidental ALH, LCIS, ADH be managed using the same pathway?
87 Yes Evidence show that those lesions are associated with upgrade to malignancy on further tissue sampling

88 1025 core biopsies Two UK regions: West Midlands and South Central region Final histology : 25% malignant
89 Lesion PPV (%) Pure ADH 50.4 LCIS 15 ALH 24.2 LN (unspecified) 25 LN+ADH 61.5 LN+CSL/RS 60 Papilloma with atypia 36.7 Papilloma without 12.9 atypia RS with atypia 39.2 RS without atypia 8.9
90 How should small incidental papilloma and/or radial scar without atypia be managed?
91 If no atypia and the lesion is small and fully excised on core/vab, categorise as B2. If not sure is completely excised, code as B3 and discuss at MDT meeting. If confirmed wholly excised, no further action is needed. If not wholly excised, follow the management pathway by 2 nd line VAB
92 Summary Current management of B3 lesions is not uniform and likely to represent overtreatment. The majority of lesions are benign on excision. MDT discussion and radiologicalpathological correlation are essential for planning management.
93 B3 guidelines are pending and recommend the use of 2 nd line VAB for further sampling as alternative to diagnostic surgery, except if lesion is completely removed by 1 st line VAB
94 THANK YOU
Management of B3 lesions
 Management of B3 lesions Pathological view Abeer Shaaban Queen Elizabeth Hospital Birmingham FEA AIDP B3 lesions In situ Lobular neoplasia Papilloma Radial scar Fibroaepithelial lesion Mucocoele like lesion
Management of B3 lesions Pathological view Abeer Shaaban Queen Elizabeth Hospital Birmingham FEA AIDP B3 lesions In situ Lobular neoplasia Papilloma Radial scar Fibroaepithelial lesion Mucocoele like lesion
B3 lesions: A Practical Approach. Dr Nisha Sharma
 B3 lesions: A Practical Approach Dr Nisha Sharma B3 lesions NHS BSP 6.7% (3.3%-12.6%) of diagnostic core biopsies will be categorised as B3 El Sayed et al (2008) 8 centres in UK and B3 ranged from 2.3
B3 lesions: A Practical Approach Dr Nisha Sharma B3 lesions NHS BSP 6.7% (3.3%-12.6%) of diagnostic core biopsies will be categorised as B3 El Sayed et al (2008) 8 centres in UK and B3 ranged from 2.3
Guidance on the management of B3 lesions
 Guidance on the management of B3 lesions Lesion diagnosed on 14g or vacuumassisted biopsy (VAB) Risk of upgrade Recommended investigation Suggested approach for follow-up if no malignancy on VAE awaiting
Guidance on the management of B3 lesions Lesion diagnosed on 14g or vacuumassisted biopsy (VAB) Risk of upgrade Recommended investigation Suggested approach for follow-up if no malignancy on VAE awaiting
Atypical Ductal Hyperplasia and Papillomas: A Comparison of Ultrasound Guided Breast Biopsy and Stereotactic Guided Breast Biopsy
 Atypical Ductal Hyperplasia and Papillomas: A Comparison of Ultrasound Guided Breast Biopsy and Stereotactic Guided Breast Biopsy Breast Cancer is the most common cancer diagnosed in women in the United
Atypical Ductal Hyperplasia and Papillomas: A Comparison of Ultrasound Guided Breast Biopsy and Stereotactic Guided Breast Biopsy Breast Cancer is the most common cancer diagnosed in women in the United
04/10/2018 HIGH RISK BREAST LESIONS. Pathology Perspectives of High Risk Breast Lesions ELEVATED RISK OF BREAST CANCER HISTORICAL PERSPECTIVES
 Pathology Perspectives of High Risk Breast Lesions Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head Director of Clinical Trials, Research and Development The University of Texas MD
Pathology Perspectives of High Risk Breast Lesions Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head Director of Clinical Trials, Research and Development The University of Texas MD
Treatment options for the precancerous Atypical Breast lesions. Prof. YOUNG-JIN SUH The Catholic University of Korea
 Treatment options for the precancerous Atypical Breast lesions Prof. YOUNG-JIN SUH The Catholic University of Korea Not so benign lesions? Imaging abnormalities(10% recall) lead to diagnostic evaluation,
Treatment options for the precancerous Atypical Breast lesions Prof. YOUNG-JIN SUH The Catholic University of Korea Not so benign lesions? Imaging abnormalities(10% recall) lead to diagnostic evaluation,
Disclosures 5/27/2012. Outline of Talk. Outline of Talk. When Is LCIS Clinically Significant? Classic LCIS. Classic LCIS
 When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation
When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation
CLINICAL SIGNIFICANCE OF BENIGN EPITHELIAL CHANGES
 Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Proliferative Breast Disease: implications of core biopsy diagnosis. Proliferative Breast Disease
 Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
3/27/2017. Disclosure of Relevant Financial Relationships. Papilloma???
 Management of Papillary Lesions Diagnosed at Rad Path Concordant Core Biopsy (CNB) Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Management of Papillary Lesions Diagnosed at Rad Path Concordant Core Biopsy (CNB) Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
CNB vs Surgical Excision
 Update on Core Needle Biopsy of Non-palpable Breast Lesions Nour Sneige, M.D. UT MD Anderson Cancer Center Houston, Tx Image-Guided CNB of Breast Lesions An alternative to surgical biospy CNB vs Surgical
Update on Core Needle Biopsy of Non-palpable Breast Lesions Nour Sneige, M.D. UT MD Anderson Cancer Center Houston, Tx Image-Guided CNB of Breast Lesions An alternative to surgical biospy CNB vs Surgical
Proliferative Epithelial lesions of the Breast. Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London
 Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
Emad A Rakha, Bernard Chi-Shern Ho, Veena K Naik, Soumadri Sen, Lisa Hamilton, Zsolt Hodi, Ian Ellis, Andrew Hs Lee
 Outcome of breast lesions diagnosed as lesion of uncertain malignant potential (B3) or suspicious of malignancy (B4) on needle core biopsy including detailed review of epithelial atypia Emad A Rakha, Bernard
Outcome of breast lesions diagnosed as lesion of uncertain malignant potential (B3) or suspicious of malignancy (B4) on needle core biopsy including detailed review of epithelial atypia Emad A Rakha, Bernard
6/3/2010. Outline of Talk. Lobular Breast Cancer: Definition of lobular differentiation. Common Problems in Diagnosing LCIS in Core Biopsies
 Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Columnar Cell Lesions
 Columnar Cell Lesions Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Question? Columnar cell lesions are: a) Annoying lesions
Columnar Cell Lesions Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Question? Columnar cell lesions are: a) Annoying lesions
Image guided core biopsies:
 Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Advocating Nonsurgical Management of Patients With Small, Incidental Radial Scars at the Time of Needle Core Biopsy. A Study of 77 Cases
 Advocating Nonsurgical Management of Patients With Small, Incidental Radial Scars at the Time of Needle Core Biopsy A Study of 77 Cases Cathleen Matrai, MD; Timothy M. D Alfonso, MD; Lindsay Pharmer, MD;
Advocating Nonsurgical Management of Patients With Small, Incidental Radial Scars at the Time of Needle Core Biopsy A Study of 77 Cases Cathleen Matrai, MD; Timothy M. D Alfonso, MD; Lindsay Pharmer, MD;
High risk lesions of the breast : Review of the current diagnostic and management strategies
 High risk lesions of the breast : Review of the current diagnostic and management strategies Poster No.: C-1204 Congress: ECR 2016 Type: Educational Exhibit Authors: P. Jagmohan, F. J. Pool, P. G. Pillay,
High risk lesions of the breast : Review of the current diagnostic and management strategies Poster No.: C-1204 Congress: ECR 2016 Type: Educational Exhibit Authors: P. Jagmohan, F. J. Pool, P. G. Pillay,
Columnar Cell Lesions. Columnar Cell Lesions and Flat Epithelial Atypia
 Columnar Cell Lesions and Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Columnar Cell Lesions Lesions characterized by columnar epithelial cells
Columnar Cell Lesions and Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Columnar Cell Lesions Lesions characterized by columnar epithelial cells
Cytyc Corporation - Case Presentation Archive - March 2002
 FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
Histological Type. Morphological and Molecular Typing of breast Cancer. Nottingham Tenovus Primary Breast Cancer Study. Survival (%) Ian Ellis
 Ian Ellis") Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Epithelial Columnar Breast Lesions: Histopathology and Molecular Markers
 29th Annual International Conference Advances in the Application of Monoclonal Antibodies in Clinical Oncology and Symposium on Cancer Stem Cells 25 th -27t h June, 2012, Mykonos, Greece Epithelial Columnar
29th Annual International Conference Advances in the Application of Monoclonal Antibodies in Clinical Oncology and Symposium on Cancer Stem Cells 25 th -27t h June, 2012, Mykonos, Greece Epithelial Columnar
Case study 1. Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research
 NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Enterprise Interest None
 Enterprise Interest None B3 lesions of the breast What are they at surgery? Case 4 Edi Brogi MD PhD Attending Pathologist - Director of Breast Pathology Memorial Sloan Kettering Cancer Center New York
Enterprise Interest None B3 lesions of the breast What are they at surgery? Case 4 Edi Brogi MD PhD Attending Pathologist - Director of Breast Pathology Memorial Sloan Kettering Cancer Center New York
Columnar Cell Lesions and Flat Epithelial Atypia
 Columnar Cell Lesions and Flat Epithelial Atypia Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Terminology for Columnar Cell
Columnar Cell Lesions and Flat Epithelial Atypia Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Terminology for Columnar Cell
LOBULAR CARCINOMA IN SITU: WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE
 : WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE Benjamin O. Anderson, M.D. Director, Breast Health Clinic Professor of Surgery and Global Health, University of Washington Joint Member, Fred Hutchinson Cancer
: WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE Benjamin O. Anderson, M.D. Director, Breast Health Clinic Professor of Surgery and Global Health, University of Washington Joint Member, Fred Hutchinson Cancer
Promise of a beautiful day
 Promise of a beautiful day Ductal carcinoma in Situ Lobular Carcinoma in Situ Natural History Manosmed Tartous Oct 2009 Gérard ABADJIAN MD Pathology Department Hôtel-Dieu de France. Associate Professor
Promise of a beautiful day Ductal carcinoma in Situ Lobular Carcinoma in Situ Natural History Manosmed Tartous Oct 2009 Gérard ABADJIAN MD Pathology Department Hôtel-Dieu de France. Associate Professor
Atypical proliferative lesions diagnosed on core biopsy - 6 year review
 Atypical proliferative lesions diagnosed on core biopsy - 6 year review Dr Angela Harris, Dr Julie Weigner & Dr Ricardo Vilain NSW Health Pathology Pathology North, Hunter Anatomical Pathology & Cytology
Atypical proliferative lesions diagnosed on core biopsy - 6 year review Dr Angela Harris, Dr Julie Weigner & Dr Ricardo Vilain NSW Health Pathology Pathology North, Hunter Anatomical Pathology & Cytology
Controversies on the Management of High Risk Breast Lesions on Core Biopsy: An Update on the Literature
 Controversies on the Management of High Risk Breast Lesions on Core Biopsy: An Update on the Literature Dianne Georgian- Smith MD Brigham and Women s Hospital Associate Professor of Radiology, Harvard
Controversies on the Management of High Risk Breast Lesions on Core Biopsy: An Update on the Literature Dianne Georgian- Smith MD Brigham and Women s Hospital Associate Professor of Radiology, Harvard
Excisional biopsy or long term follow-up results in breast high-risk lesions diagnosed at core needle biopsy
 Excisional biopsy or long term follow-up results in breast high-risk lesions diagnosed at core needle biopsy Poster No.: C-2515 Congress: ECR 2015 Type: Authors: Scientific Exhibit Ö. S. Okcu 1, A. Oktay
Excisional biopsy or long term follow-up results in breast high-risk lesions diagnosed at core needle biopsy Poster No.: C-2515 Congress: ECR 2015 Type: Authors: Scientific Exhibit Ö. S. Okcu 1, A. Oktay
Interpretation of Breast Pathology in the Era of Minimally Invasive Procedures
 Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine Jacksonville Medical Director, UF Health Breast Center Chief of Pathology
Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine Jacksonville Medical Director, UF Health Breast Center Chief of Pathology
IBCM 2, April 2009, Sarajevo, Bosnia and Herzegovina
 Preoperative diagnosis and treatment planning in breast cancer The pathologist s perspective L. Mazzucchelli Istituto Cantonale di Patologia Locarno, Switzerland IBCM 2, 23-25 April 2009, Sarajevo, Bosnia
Preoperative diagnosis and treatment planning in breast cancer The pathologist s perspective L. Mazzucchelli Istituto Cantonale di Patologia Locarno, Switzerland IBCM 2, 23-25 April 2009, Sarajevo, Bosnia
Diagnostic benefits of ultrasound-guided. CNB) versus mammograph-guided biopsy for suspicious microcalcifications. without definite breast mass
 versus mammograph-guided biopsy for suspicious microcalcifications. without definite breast mass") Volume 118 No. 19 2018, 531-543 ISSN: 1311-8080 (printed version); ISSN: 1314-3395 (on-line version) url: http://www.ijpam.eu ijpam.eu Diagnostic benefits of ultrasound-guided biopsy versus mammography-guided
Volume 118 No. 19 2018, 531-543 ISSN: 1311-8080 (printed version); ISSN: 1314-3395 (on-line version) url: http://www.ijpam.eu ijpam.eu Diagnostic benefits of ultrasound-guided biopsy versus mammography-guided
Quality ID #263: Preoperative Diagnosis of Breast Cancer National Quality Strategy Domain: Effective Clinical Care
 Quality ID #263: Preoperative Diagnosis of Breast Cancer National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
Quality ID #263: Preoperative Diagnosis of Breast Cancer National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
Surgical Pathology Issues of Practical Importance
 Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
PURPOSE IMAGE-GUIDANCE MODALITIES IMAGE-GUIDED BREAST BIOPSY. US-Techniques. Ultrasound. US guided NLOBB. TH. Helbich
 IMAGE-GUIDED BREAST BIOPSY PURPOSE TH. Helbich Department of Radiology Division of Molecular & Gender Imaging Medical University of Vienna Imaging techniques Interventional procedures Quality management
IMAGE-GUIDED BREAST BIOPSY PURPOSE TH. Helbich Department of Radiology Division of Molecular & Gender Imaging Medical University of Vienna Imaging techniques Interventional procedures Quality management
Controversies and Problematic Issues in Core Needle Biopsies (To excise or not to excise)
") Controversies and Problematic Issues in Core Needle Biopsies (To excise or not to excise) Laura C. Collins, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Schematic Representation
Controversies and Problematic Issues in Core Needle Biopsies (To excise or not to excise) Laura C. Collins, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Schematic Representation
Classic lobular neoplasia on core biopsy: a clinical and radio-pathologic correlation study with follow-up excision biopsy
 762 & 2013 USCAP, Inc All rights reserved 0893-3952/13 $32.00 Classic lobular neoplasia on core biopsy: a clinical and radio-pathologic correlation study with follow-up excision biopsy Shweta Chaudhary
762 & 2013 USCAP, Inc All rights reserved 0893-3952/13 $32.00 Classic lobular neoplasia on core biopsy: a clinical and radio-pathologic correlation study with follow-up excision biopsy Shweta Chaudhary
Breast: Difficulties in Core Biopsies
 Breast: Difficulties in Core Biopsies Anna Marie Mulligan, MB, MSc, FRCPath University Health Network and University of Toronto E-mail: annamarie.mulligan@uhn.ca No conflicts of interest Role of Core Needle
Breast: Difficulties in Core Biopsies Anna Marie Mulligan, MB, MSc, FRCPath University Health Network and University of Toronto E-mail: annamarie.mulligan@uhn.ca No conflicts of interest Role of Core Needle
Sami Shousha Editor. Breast Pathology. Problematic Issues
 Breast Pathology Editor Breast Pathology Problematic Issues Editor Charing Cross Hospital Imperial College Healthcare NHS Trust & Imperial College London United Kingdom ISBN 978-3-319-28653-2 ISBN 978-3-319-28655-6
Breast Pathology Editor Breast Pathology Problematic Issues Editor Charing Cross Hospital Imperial College Healthcare NHS Trust & Imperial College London United Kingdom ISBN 978-3-319-28653-2 ISBN 978-3-319-28655-6
Good afternoon everyone. First of all many thanks to Dr. Bonaventura and Dr. Arn for inviting
 PATHOLOGY IN-SITU CARCINOMA, ROHIT BHARGAVA, MD 1 Good afternoon everyone. First of all many thanks to Dr. Bonaventura and Dr. Arn for inviting me here, it s great to be here and I m going to talk about
PATHOLOGY IN-SITU CARCINOMA, ROHIT BHARGAVA, MD 1 Good afternoon everyone. First of all many thanks to Dr. Bonaventura and Dr. Arn for inviting me here, it s great to be here and I m going to talk about
Chief Investigator Adele Francis University of Birmingham UK. Prof MWR Reed (CoI) University of Sheffield
 University of Sheffield") The LORIS Trial: A multicentre, randomised phase III trial of standard surgery versus active monitoring in women with newly diagnosed low risk ductal carcinoma in situ. Chief Investigator Adele Francis
The LORIS Trial: A multicentre, randomised phase III trial of standard surgery versus active monitoring in women with newly diagnosed low risk ductal carcinoma in situ. Chief Investigator Adele Francis
Pathology of Lobular & Ductal Preneoplasia. Syed A Hoda, MD Weill-Cornell, New York, NY
 Pathology of Lobular & Ductal Preneoplasia Syed A Hoda, MD Weill-Cornell, New York, NY Proliferative Epithelial Changes in Breast A wide range of proliferative epithelial changes occur in the breast There
Pathology of Lobular & Ductal Preneoplasia Syed A Hoda, MD Weill-Cornell, New York, NY Proliferative Epithelial Changes in Breast A wide range of proliferative epithelial changes occur in the breast There
Incidence of ductal lesions
 Ductal Proliferative Lesions of the Breast: From FEA to ADH to DCIS Incidence of ductal lesions Pre-mammography: DCIS < 3% of breast cancers, large palpable masses, with invasion Mammography: DCIS 25%
Ductal Proliferative Lesions of the Breast: From FEA to ADH to DCIS Incidence of ductal lesions Pre-mammography: DCIS < 3% of breast cancers, large palpable masses, with invasion Mammography: DCIS 25%
Flat Epithelial Atypia
 Flat Epithelial Atypia Richard Owings, M.D. University of Arkansas for Medical Sciences Department of Pathology Flat epithelial atypia can be a difficult lesion May be a subtle diagnosis Lots of changes
Flat Epithelial Atypia Richard Owings, M.D. University of Arkansas for Medical Sciences Department of Pathology Flat epithelial atypia can be a difficult lesion May be a subtle diagnosis Lots of changes
Papillary lesions of the breast - Imaging findings and diagnostic challenges
 Papillary lesions of the breast - Imaging findings and diagnostic challenges Poster No.: R-0146 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: P. Jagmohan, F. J. Pool Keywords: Breast, Mammography,
Papillary lesions of the breast - Imaging findings and diagnostic challenges Poster No.: R-0146 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: P. Jagmohan, F. J. Pool Keywords: Breast, Mammography,
Benign Breast Disease and Breast Cancer Risk
 Benign Breast Disease and Breast Cancer Risk Jean F. Simpson, M.D. Vanderbilt University Nashville, Tennessee December 1, 2011 Nashville Nashville Lebanon 1 Cedars of Lebanon State Park The American University
Benign Breast Disease and Breast Cancer Risk Jean F. Simpson, M.D. Vanderbilt University Nashville, Tennessee December 1, 2011 Nashville Nashville Lebanon 1 Cedars of Lebanon State Park The American University
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Mammographic features and correlation with biopsy findings using 11-gauge stereotactic vacuum-assisted breast biopsy (SVABB)
") Original article Annals of Oncology 14: 450 454, 2003 DOI: 10.1093/annonc/mdh088 Mammographic features and correlation with biopsy findings using 11-gauge stereotactic vacuum-assisted breast biopsy (SVABB)
Original article Annals of Oncology 14: 450 454, 2003 DOI: 10.1093/annonc/mdh088 Mammographic features and correlation with biopsy findings using 11-gauge stereotactic vacuum-assisted breast biopsy (SVABB)
Breast Pathology. Breast Development
 Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
Management of Patients Diagnosed With Lobular Carcinoma in Situ at Needle Core Biopsy at a Community-Based Outpatient Facility
 Women s Imaging Original Research Destounis et al. Management of LCIS Diagnosed at Core Needle Biopsy Women s Imaging Original Research FOCUS ON: Stamatia V. Destounis 1 Philip F. Murphy Posy J. Seifert
Women s Imaging Original Research Destounis et al. Management of LCIS Diagnosed at Core Needle Biopsy Women s Imaging Original Research FOCUS ON: Stamatia V. Destounis 1 Philip F. Murphy Posy J. Seifert
Breast Lesion Excision System-Intact (BLES): A Stereotactic Method of Biopsy of Suspicius Non-Palpable Mammographic Lesions.
: A Stereotactic Method of Biopsy of Suspicius Non-Palpable Mammographic Lesions.") Breast Lesion Excision System-Intact (BLES): A Stereotactic Method of Biopsy of Suspicius Non-Palpable Mammographic Lesions. Poster No.: C-1595 Congress: ECR 2014 Type: Authors: Scientific Exhibit I. Georgiou
Breast Lesion Excision System-Intact (BLES): A Stereotactic Method of Biopsy of Suspicius Non-Palpable Mammographic Lesions. Poster No.: C-1595 Congress: ECR 2014 Type: Authors: Scientific Exhibit I. Georgiou
Lobular Carcinoma In Situ Variants in Breast Cores
 Lobular Carcinoma In Situ Variants in Breast Cores Potential for Misdiagnosis, Upgrade Rates at Surgical Excision, and Practical Implications Megan E. Sullivan, MD; Seema A. Khan, MD; Yurdanur Sullu, MD;
Lobular Carcinoma In Situ Variants in Breast Cores Potential for Misdiagnosis, Upgrade Rates at Surgical Excision, and Practical Implications Megan E. Sullivan, MD; Seema A. Khan, MD; Yurdanur Sullu, MD;
HHS Public Access Author manuscript Am J Surg Pathol. Author manuscript; available in PMC 2016 September 06.
 Radial Scar at Image-guided Needle Biopsy: Is Excision Necessary? Niamh Conlon, MB, FRCPath *, Clare D Arcy, MB, FRCPath *, Jennifer B. Kaplan, MD, Zenica L. Bowser, MS *, Anibal Cordero, BS *, Edi Brogi,
Radial Scar at Image-guided Needle Biopsy: Is Excision Necessary? Niamh Conlon, MB, FRCPath *, Clare D Arcy, MB, FRCPath *, Jennifer B. Kaplan, MD, Zenica L. Bowser, MS *, Anibal Cordero, BS *, Edi Brogi,
Surgical Management of High- Risk Breast Lesions
 Surgical Management of High- Risk Breast Lesions Amy C. Degnim, MD a, Tari A. King, MD b, * KEYWORDS High-risk lesion Atypical hyperplasia Lobular carcinoma in situ Percutaneous breast biopsy Breast cancer
Surgical Management of High- Risk Breast Lesions Amy C. Degnim, MD a, Tari A. King, MD b, * KEYWORDS High-risk lesion Atypical hyperplasia Lobular carcinoma in situ Percutaneous breast biopsy Breast cancer
Review Article. ISSN: (Print) ISSN: (Online)
 ISSN: (Online)") Scholars International Journal of Obstetrics and Gynecology Abbreviated key title: Sch. Int. J. Obstet. Gynec. A Publication by Scholars Middle East Publishers Dubai, United Arab Emirates ISSN: 2616-8235
Scholars International Journal of Obstetrics and Gynecology Abbreviated key title: Sch. Int. J. Obstet. Gynec. A Publication by Scholars Middle East Publishers Dubai, United Arab Emirates ISSN: 2616-8235
Breast Disease: What PCPs Need to Know. Eunice Cho MD FACS
 Breast Disease: What PCPs Need to Know Eunice Cho MD FACS New Breast Cancer Screening Guideline for women with average risk Every other year AGE 40 AGE 45 AGE 55 AGE 55 + Talk with your doctor about when
Breast Disease: What PCPs Need to Know Eunice Cho MD FACS New Breast Cancer Screening Guideline for women with average risk Every other year AGE 40 AGE 45 AGE 55 AGE 55 + Talk with your doctor about when
Performance Indices of Needle Biopsy Procedures for the Assessment of Screen Detected Abnormalities in Services Accredited by BreastScreen Australia
 DOI:http://dx.doi.org/10.7314/APJCP.2014.15.24.10665 RESEARCH ARTICLE Performance Indices of Needle Biopsy Procedures for the Assessment of Screen Detected Abnormalities in Services Accredited by BreastScreen
DOI:http://dx.doi.org/10.7314/APJCP.2014.15.24.10665 RESEARCH ARTICLE Performance Indices of Needle Biopsy Procedures for the Assessment of Screen Detected Abnormalities in Services Accredited by BreastScreen
Diagnostic accuracy of ultrasonography-guided core needle biopsy for breast lesions
 Singapore Med J 01; 5(1) 40 Diagnostic accuracy of ultrasonography-guided core needle biopsy for breast lesions Wiratkapun Cl, MD, Treesit T1, MD, Wibulpolprasert E1, MD, Lertsithichai P, MD, MSc INTRODUCTION
Singapore Med J 01; 5(1) 40 Diagnostic accuracy of ultrasonography-guided core needle biopsy for breast lesions Wiratkapun Cl, MD, Treesit T1, MD, Wibulpolprasert E1, MD, Lertsithichai P, MD, MSc INTRODUCTION
MEDICAL IMAGING AND BREAST DISEASE HOW CAN WE HELP YOU?
 MEDICAL IMAGING AND BREAST DISEASE HOW CAN WE HELP YOU? Barbara M. Preston, M.D. SCREENING MAMMOGRAPHY AVERAGE RISK PATIENTS KAISER RECOMMENDATION: ALL WOMEN (INCLUDING TRANSGENDER FEMALES) Every 1-21
MEDICAL IMAGING AND BREAST DISEASE HOW CAN WE HELP YOU? Barbara M. Preston, M.D. SCREENING MAMMOGRAPHY AVERAGE RISK PATIENTS KAISER RECOMMENDATION: ALL WOMEN (INCLUDING TRANSGENDER FEMALES) Every 1-21
Current issues in diagnostic breast pathology
 1 Cancer Studies and Molecular Medicine, University of Leicester, Leicester, UK 2 Academic Unit of Pathology, Leeds University, Leeds, UK 3 Academic Oncology/Breast Pathology, King s College London, London,
1 Cancer Studies and Molecular Medicine, University of Leicester, Leicester, UK 2 Academic Unit of Pathology, Leeds University, Leeds, UK 3 Academic Oncology/Breast Pathology, King s College London, London,
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
ACRIN 6666 Therapeutic Surgery Form
 S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
Poster No.: C-0466 Congress: ECR 2010 Scientific Exhibit
 Up-right stereotactic vacuum-assisted biopsy (UP-VAB) of non palpable breast lesions: Results and correlations with radiological suspicion (BI-RADS classification) Poster No.: C-0466 Congress: ECR 2010
Up-right stereotactic vacuum-assisted biopsy (UP-VAB) of non palpable breast lesions: Results and correlations with radiological suspicion (BI-RADS classification) Poster No.: C-0466 Congress: ECR 2010
Public Health Agency NORTHERN IRELAND BREAST SCREENING PROGRAMME ANNUAL REPORT & STATISTICAL BULLETIN QUALITY ASSURANCE REFERENCE CENTRE
 Public Health Agency Improving Your Health and Wellbeing NORTHERN IRELAND BREAST SCREENING PROGRAMME ANNUAL REPORT & STATISTICAL BULLETIN 2010-2011 QUALITY ASSURANCE REFERENCE CENTRE August 2012 1 2 Contents
Public Health Agency Improving Your Health and Wellbeing NORTHERN IRELAND BREAST SCREENING PROGRAMME ANNUAL REPORT & STATISTICAL BULLETIN 2010-2011 QUALITY ASSURANCE REFERENCE CENTRE August 2012 1 2 Contents
Anatomic Pathology / Mucocele-like Lesions on Breast Core Biopsy. Mucocele-like Lesions Diagnosed on Breast Core Biopsy
 Anatomic Pathology / Mucocele-like Lesions on Breast Core Biopsy Mucocele-like Lesions Diagnosed on Breast Core Biopsy Assessment of Upgrade Rate and Need for Surgical Excision Brian Sutton, MD, 1 Simone
Anatomic Pathology / Mucocele-like Lesions on Breast Core Biopsy Mucocele-like Lesions Diagnosed on Breast Core Biopsy Assessment of Upgrade Rate and Need for Surgical Excision Brian Sutton, MD, 1 Simone
Imaging in breast cancer. Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since
 Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
BI-RADS CATEGORIZATION AND BREAST BIOPSY categorization in the selection of appropriate breast biopsy technique is also discussed. Patients and method
 Original Article Positive Predictive Value of BI-RADS Categorization in an Asian Population Yah-Yuen Tan, Siew-Bock Wee, Mona P.C. Tan and Bee-Kiang Chong, 1 Departments of General Surgery and 1Diagnostic
Original Article Positive Predictive Value of BI-RADS Categorization in an Asian Population Yah-Yuen Tan, Siew-Bock Wee, Mona P.C. Tan and Bee-Kiang Chong, 1 Departments of General Surgery and 1Diagnostic
Breast Lesions of Uncertain Malignant Potential: A Challenge for Surgeons
 Breast Lesions of Uncertain Malignant Potential: A Challenge for Surgeons Deslauriers Nancy 1, Sidéris Lucas 1, Dufresne Michel-Pierre 2, Mitchell Andrew 3, Drolet Pierre 4, Dubé Pierre 1, Leclerc Yves
Breast Lesions of Uncertain Malignant Potential: A Challenge for Surgeons Deslauriers Nancy 1, Sidéris Lucas 1, Dufresne Michel-Pierre 2, Mitchell Andrew 3, Drolet Pierre 4, Dubé Pierre 1, Leclerc Yves
Atypical And Suspicious Categories In Fine Needle Aspiration Cytology Of The Breast
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-853, p-issn: 2279-861.Volume 15, Issue 1 Ver. III (October. 216), PP 57-61 www.iosrjournals.org Atypical And Suspicious Categories in
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-853, p-issn: 2279-861.Volume 15, Issue 1 Ver. III (October. 216), PP 57-61 www.iosrjournals.org Atypical And Suspicious Categories in
Benign and preinvasive breast lesions
 58 Benign and preinvasive breast lesions Anke Kleine-Tebbe 1, Aurelia Noske 2 1 DRK Clinics Berlin Köpenick, Berlin, Germany 2 Institute for pathology, Charité Campus Mitte, Charité University Medical
58 Benign and preinvasive breast lesions Anke Kleine-Tebbe 1, Aurelia Noske 2 1 DRK Clinics Berlin Köpenick, Berlin, Germany 2 Institute for pathology, Charité Campus Mitte, Charité University Medical
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
NORTHERN IRELAND BREAST SCREENING PROGRAMME ANNUAL REPORT & STATISTICAL BULLETIN
 Improving Your Health and Wellbeing NORTHERN IRELAND BREAST SCREENING PROGRAMME ANNUAL REPORT & STATISTICAL BULLETIN 211-212 QUALITY ASSURANCE REFERENCE CENTRE August 213 1 2 Contents Page Summary 4 Introduction
Improving Your Health and Wellbeing NORTHERN IRELAND BREAST SCREENING PROGRAMME ANNUAL REPORT & STATISTICAL BULLETIN 211-212 QUALITY ASSURANCE REFERENCE CENTRE August 213 1 2 Contents Page Summary 4 Introduction
Original Report. Mucocele-Like Tumors of the Breast: Mammographic and Sonographic Appearances. Katrina Glazebrook 1 Carol Reynolds 2
 Katrina Glazebrook 1 Carol Reynolds 2 Received January 2, 2002; accepted after revision August 28, 2002. 1 Department of Radiology, Mayo Clinic, 200 First St. S.W., Rochester, MN 55905. Address correspondence
Katrina Glazebrook 1 Carol Reynolds 2 Received January 2, 2002; accepted after revision August 28, 2002. 1 Department of Radiology, Mayo Clinic, 200 First St. S.W., Rochester, MN 55905. Address correspondence
Ductal Carcinoma in Situ. Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA
 Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Aspects of quality in breast pathology. Andrew Lee Nottingham University Hospitals
 Aspects of quality in breast pathology Andrew Lee Nottingham University Hospitals British breast pathology EQA: performance issues Ian Ellis Friday 8.30 am National breast screening pathology audit 2015
Aspects of quality in breast pathology Andrew Lee Nottingham University Hospitals British breast pathology EQA: performance issues Ian Ellis Friday 8.30 am National breast screening pathology audit 2015
Macrobiopsy under X-Ray Guidance
 Macrobiopsy under X-Ray Guidance C. Balleyguier, B. Boyer Radiology Gustave Roussy, Villejuif, France Breast Intervention Imaging Major domain in breast imaging European guidelines recommend a pre surgical
Macrobiopsy under X-Ray Guidance C. Balleyguier, B. Boyer Radiology Gustave Roussy, Villejuif, France Breast Intervention Imaging Major domain in breast imaging European guidelines recommend a pre surgical
Ductal Proliferations of the Breast: The Good, the Bad, and the Ugly
 Ductal Proliferations of the Breast: The Good, the Bad, and the Ugly Melinda F. Lerwill, MD CRITERIA FOR DISTINGUISHING LOW-GRADE DUCTAL CARCINOMA IN SITU FROM USUAL DUCTAL HYPERPLASIA CYTOLOGY Low-grade
Ductal Proliferations of the Breast: The Good, the Bad, and the Ugly Melinda F. Lerwill, MD CRITERIA FOR DISTINGUISHING LOW-GRADE DUCTAL CARCINOMA IN SITU FROM USUAL DUCTAL HYPERPLASIA CYTOLOGY Low-grade
The Hot Topic for today is a biopsy from a 58-year-old woman who had worrisome mammographic calcifications on screening.
 The Hot Topic for today is a biopsy from a 58-year-old woman who had worrisome mammographic calcifications on screening. 1 My name is Dan Visscher; I am a consultant in the Division of Anatomic Pathology
The Hot Topic for today is a biopsy from a 58-year-old woman who had worrisome mammographic calcifications on screening. 1 My name is Dan Visscher; I am a consultant in the Division of Anatomic Pathology
Mammographic imaging of nonpalpable breast lesions. Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand
 Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Breast core needle biopsy: issues and controversies
 S36 & 2010 USCAP, Inc. All rights reserved 0893-3952/10 $32.00 Breast core needle biopsy: issues and controversies Michael Bilous Institute of Clinical Pathology and Medical Research, Westmead Hospital
S36 & 2010 USCAP, Inc. All rights reserved 0893-3952/10 $32.00 Breast core needle biopsy: issues and controversies Michael Bilous Institute of Clinical Pathology and Medical Research, Westmead Hospital
Original Articles. Clinical Implications of Margin Involvement by Pleomorphic Lobular Carcinoma In Situ
 Original Articles Clinical Implications of Margin Involvement by Pleomorphic Lobular Carcinoma In Situ Erinn Downs-Kelly, DO; Diana Bell, MD; George H. Perkins, MD; Nour Sneige, MD; Lavinia P. Middleton,
Original Articles Clinical Implications of Margin Involvement by Pleomorphic Lobular Carcinoma In Situ Erinn Downs-Kelly, DO; Diana Bell, MD; George H. Perkins, MD; Nour Sneige, MD; Lavinia P. Middleton,
Benign Breast Disease. David Anderson, MD Assistant Professor of Clinical Surgery
 Benign Breast Disease David Anderson, MD Assistant Professor of Clinical Surgery Overview Nipple Discharge Breast infection Breast Pain Gynecomastia Fibroepithelial lesions High Risk Lesions-Papilloma,
Benign Breast Disease David Anderson, MD Assistant Professor of Clinical Surgery Overview Nipple Discharge Breast infection Breast Pain Gynecomastia Fibroepithelial lesions High Risk Lesions-Papilloma,
In Situ Breast Carcinoma. James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA
 In Situ Breast Carcinoma James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA Content In Situ Ductal Carcinoma In Situ Lobular Carcinoma
In Situ Breast Carcinoma James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA Content In Situ Ductal Carcinoma In Situ Lobular Carcinoma
Atypical papillary lesions after core needle biopsy and subsequent breast carcinoma
 Asian Biomedicine Vol. 5 No. 2 April 2011; 243-248 DOI: 10.5372/1905-7415.0502.031 Original article Atypical papillary lesions after core needle biopsy and subsequent breast carcinoma Tuenchit Khamapirad
Asian Biomedicine Vol. 5 No. 2 April 2011; 243-248 DOI: 10.5372/1905-7415.0502.031 Original article Atypical papillary lesions after core needle biopsy and subsequent breast carcinoma Tuenchit Khamapirad
TRIAL SYNOPSIS LORIS. The Low Risk DCIS Trial. Chief Investigator. Miss Adele Francis
 TRIAL SYNOPSIS LORIS Chief Investigator The Low Risk DCIS Trial Miss Adele Francis ISRCTN No. 27544579 Sponsor University of Birmingham, United Kingdom Trial Design Objectives of Feasibility Study A multi-centre,
TRIAL SYNOPSIS LORIS Chief Investigator The Low Risk DCIS Trial Miss Adele Francis ISRCTN No. 27544579 Sponsor University of Birmingham, United Kingdom Trial Design Objectives of Feasibility Study A multi-centre,
CPC 4 Breast Cancer. Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast.
 CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
Stereotactic 11-Gauge Vacuum- Assisted Breast Biopsy: A Validation Study
 Georg Pfarl 1 Thomas H. Helbich 1 Christopher C. Riedl 1 Teresa Wagner 2 Michael Gnant 3 Margaretha Rudas 4 Laura Liberman 5 Received March 11, 2002; accepted after revision May 17, 2002. 1 Department
Georg Pfarl 1 Thomas H. Helbich 1 Christopher C. Riedl 1 Teresa Wagner 2 Michael Gnant 3 Margaretha Rudas 4 Laura Liberman 5 Received March 11, 2002; accepted after revision May 17, 2002. 1 Department
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Texas Society of Pathologists 2013 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical
Papillary Lesions of the Breast Texas Society of Pathologists 2013 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical
Protocol for the Examination of Biopsy Specimens From Patients With Invasive Carcinoma of the Breast
 Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: BreastInvasive 1.0.0.0 Protocol Posting Date: February 2019 Accreditation Requirements The use of
Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: BreastInvasive 1.0.0.0 Protocol Posting Date: February 2019 Accreditation Requirements The use of
Disclosures. Premalignant Lesions of the Breast: What Clinicians Want and Why. NY Times: Prone to Error: Earliest Steps to Find Cancer.
 Disclosures Premalignant Lesions of the Breast: What Clinicians Want and Why I have nothing to disclose Rick Baehner, MD Assistant Professor, UCSF Pathology NY Times: Prone to Error: Earliest Steps to
Disclosures Premalignant Lesions of the Breast: What Clinicians Want and Why I have nothing to disclose Rick Baehner, MD Assistant Professor, UCSF Pathology NY Times: Prone to Error: Earliest Steps to
1 NORMAL HISTOLOGY AND METAPLASIAS
 1 NORMAL HISTOLOGY AND METAPLASIAS, MD Anatomy and Histology 1 Metaplasias 2 ANATOMY AND HISTOLOGY The female breast is composed of a branching duct system, which begins at the nipple with the major lactiferous
1 NORMAL HISTOLOGY AND METAPLASIAS, MD Anatomy and Histology 1 Metaplasias 2 ANATOMY AND HISTOLOGY The female breast is composed of a branching duct system, which begins at the nipple with the major lactiferous
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node
 Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY
 EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School Breast Cancer Screening Early detection of
EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School Breast Cancer Screening Early detection of
EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY
 EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School Breast Cancer Screening Early detection of
EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School Breast Cancer Screening Early detection of
Mammo-50 Eligibility Queries
 Mammo-50 Eligibility Queries Are patients who have received either neo-adjuvant or adjuvant chemo, radiotherapy or been part of another trial, ie OPTIMA, FAST FORWARD excluded from entry? Any patients
Mammo-50 Eligibility Queries Are patients who have received either neo-adjuvant or adjuvant chemo, radiotherapy or been part of another trial, ie OPTIMA, FAST FORWARD excluded from entry? Any patients
Minimizing Errors in Diagnostic Pathology
 Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville Medical Director, Shands Jacksonville Breast Health Center
Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville Medical Director, Shands Jacksonville Breast Health Center
Non-mass Enhancement on Breast MRI. Aditi A. Desai, MD Margaret Ann Mays, MD
 Non-mass Enhancement on Breast MRI Aditi A. Desai, MD Margaret Ann Mays, MD Breast MRI Important screening and diagnostic tool, given its high sensitivity for breast cancer detection Breast MRI - Indications
Non-mass Enhancement on Breast MRI Aditi A. Desai, MD Margaret Ann Mays, MD Breast MRI Important screening and diagnostic tool, given its high sensitivity for breast cancer detection Breast MRI - Indications