Breast: Difficulties in Core Biopsies
|
|
|
- Earl Rich
- 6 years ago
- Views:
Transcription


1 Breast: Difficulties in Core Biopsies Anna Marie Mulligan, MB, MSc, FRCPath University Health Network and University of Toronto
2 No conflicts of interest
3 Role of Core Needle Biopsy To eliminate need for surgical excision of benign lesions To definitively diagnose malignancy Allow surgical planning and consideration for possible neoadjuvant therapy Superior to FNA
4 Advantages Challenges no. of surgeries in women with IBC Less invasive Less expensive Less scarring on subsequent imaging Confirm multiple foci and determine appropriate surgical procedure Limited material Disruption frequent Sampling error
5 Accuracy Excellent agreement with open bx. Accuracy, sensitivity, specificity 0.98, 0.88, 0.98 (mostly palpable) 0.98, 0.91, 1.00 (non-palpable) when > 6 cores with experienced radiologist Original and review pathologist 96% concordance Wei et al, Med Onc, 2010 Fajardo et al, Acad Rad, 2004
6 False Negatives 1-15% for malignancy Lower with 11G/vacuum Causes: Sampling/Suspicious mass not explained by histologic findings Calcifications not identified in the core Calcs > mass DCIS > invasive
7 Key to success Does my diagnosis correlate with the radiologic findings? Know the indication for the biopsy!!!!!
8 Triple Test Clinical Radiology Pathology Must correlate! Important for pathologist to appreciate imaging categories and pathology correlation Multidisciplinary rounds Specimen x-ray
9 Role of the Pathologist in the Evaluation of Calcifications
10 Calcifications Specimen radiograph mandatory for any biopsy performed for calcifications Separate cores with calcs from those without If calcs seen on mammo but none in specimen x-ray: ability to make dx from 82 to 40% Dx more likely in cores bearing calcs on specimen x-ray than those without 84 vs 71%


11 Specimen radiograph is mandatory for image-guided biopsy for calcifications U/S-guided needle bx Must reconcile the findings in specimen radiograph and mammogram with microscopic findings
12 Calcifications Examine > 3 levels intervening unstained levels may be retained for ER/PR vs. other IHC If indication = Ca+2, must make every effort to find Pattern/distribution Always report if calcs are seen and where Number More numerous in radiograph or microscopically? Size Is the size of the observed calcs consistent with those targeted? (size threshold of 100µm on imaging)
13 Audience participation 1 58 y.o woman with linear branching calcifications on mammography Stereotactic core biopsy Calcifications are reported as being present in the specimen x-ray

14
15 True or false Pathology correlates with radiology Findings are benign Patient returns to screening programme
16 False Calcifications not in keeping with linear branching morphology Cut deeper levels
17 No Calcs? Polarize -? calcium oxalate X-ray blocks Cut deeper levels Still none? Lost calcs Loss during processing/sectioning Destruction by fixatives Dislodged by microtome Rupture of cyst during biopsy fall-out
18 Microcalcifications: calcium oxalate
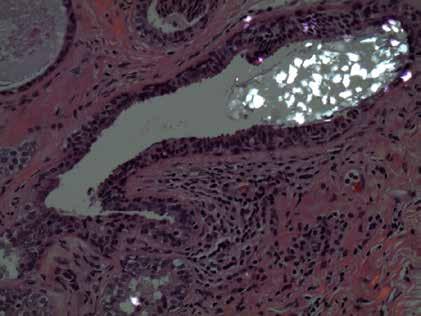


19 Microcalcifications: calcium oxalate
20 Categories Benign Malignant Uncertain Suspicious
21 Fibroadenoma Hamartoma Lactating adenoma Nodular adenosis Proliferative breast disease Benign Non-proliferative breast changes Cysts
22 Hamartoma Highlights importance of rad-path correlation Circumscribed/encapsulated Ducts, lobules, fibrous tissue, fat (variable) Typical mammographic appearance Obviating need for CNB in most
23
24 Hamartoma - CNB Benign fibrous and fatty breast tissue Was the lesion sampled? Are the characteristic imaging features present? If yes consider hamartoma
25 DCIS with microinvasion DCIS Malignant Invasive carcinoma Other Malignant

26 Beware: Pitfalls DCIS with obliterative sclerosis Displacement of calcs Displacement of atypical cells

27 Beware: Pitfalls DCIS with obliterative sclerosis Displacement of calcs Displacement of atypical cells

28 Beware: Pitfalls DCIS with obliterative sclerosis Displacement of calcs Displacement of atypical cells
29 DCIS 20% upgraded to IBC Mass lesions > microcalcs Younger patients Greater extent on mammo High grade Comedo necrosis Consider SLN Report: grade, comedonecrosis, calcifications, architecture, microinvasion
30 IBC - What to report? How much information is required pre-op? Neo-adjuvant therapy Proceeding direct to surgery Full range of prognostic and predictive information Provision of one set of results only? Avoids misleading/conflicting findings

 Size If entire tumour removed on biopsy Prone to inaccuracies")
31 What to report? Type May influence pre-op work-up and extent of surgery Good correlation with excision (72-82%) Grade Can be discordant; still useful Underestimate (less mitoses) (84% for high grade) Size If entire tumour removed on biopsy Prone to inaccuracies (underestimate in 79%) LVI Only if unequivocal; beware retraction, 8% sensitivity
32 Audience Participation 2 65 year old woman, screening detected mass, 1.3 cm Ultrasound-guided core biopsy

33
34

35

36
37 Which action is most appropriate? A. Observation, lesion is benign B. Excise, lesion is probably benign C. Re-biopsy, findings not concordant D. Wide local excision with sentinel node E. I m not sure..i think I need help
38 Which action is most appropriate? A. Observation, lesion is benign B. Excise, lesion is probably benign C. Re-biopsy, findings not concordant D. Wide local excision with sentinel node E. I m not sure..i think I need help

39

40 Radial Scar
41 Invasive Carcinoma Pitfalls on CNB Is it malignant of a benign mimic? e.g. tubular carcinoma vs radial scar Imaging not helpful

42

43

44



45 p63 SMMHC calponin
46 Pitfalls Radial Scar Entrapped distorted glands Tubules resembling those of tubular ca. Rare absence of MEC IHC staining Perineural invasion Necrosis present in 10% with UEH More challenging on CNB
47 Invasive Carcinoma Pitfalls on CNB Overcalling ILC In the setting of a well-circumscribed lesion SA, myoid hamartoma

48


49 SA mimicking ILC pattern
50 Invasive Carcinoma Pitfalls on CNB Under calling ILC Paucicellular infiltrate Chronic inflammation/histiocytes

51 Stroma appears more cellular than usual

52


53


54 Inflammatory vs. ILC Pan-CK
55 Radial Scar Papillary L N Uncertain CCLs with atypia ADH Spindle cell lesions FELCS

56 Uncertain 7.7% of screening biopsies Clinical dilemma Need excision to exclude malignancy Hayes et al, J Clin Pathol Dec;62(12):
57 Papillary Lesions Heterogeneous Finger-like projections Central FV core Lined by epithelium IDP vs. IDP with atypia/dcis vs. EPC


58 Benign intraductal papilloma with FEHUT




59 SMM-HC
60 Intraductal Papilloma Sclerosis Obscure papillary nature Entrapment Mimics invasion ID MECs Stroma hyalinized Underlying lesion is benign

61 Benign intraductal papilloma with sclerosis and entrapment

62
63 Atypia in Papilloma IP with: Low grade cytologic atypia Architectural atypia Extent < 3mm If > 3mm DCIS in IP DDx UEH ER CK5 Page et al. Cancer.,1996 Jul 15;78(2): Grin et al. AJSP, 2009 Nov;33(11):

64 Atypia within a papilloma

65
66 Encapsulated Papillary Carcinoma Papillary carcinoma, surrounded by fibrous capsule FV cores Single population Low to intermediate grade MECs lacking from periphery In situ vs invasive?


67

68


69 Fibrovascular Core p63/smms No MEC lining FV cores or periphery
70 Diagnosing Invasive Ca Difficult! EPC lack MEC around periphery IHC not useful Pseudoinvasion True invasion Recognisable pattern of invasive carcinoma Beyond capsule, into fat/normal breast May not be included in biopsy


71
72 Management Atypia in IP excise EPC excise Benign IP? Risk of upgrade to malignancy (0-36%) Sampling or difficult dx.? Preventive? Excise all vs. prolonged follow-up vs. VACB Consider: Small, no atypia, generously sampled by VACB, no residual lesion post-core imaging Beware epithelial displacement
73 Study Benign papillomas on CNB Upgrade Rate Benign Excised Benign on Excision Atypical on excision Malignant on excision Total Upgrade N(%) Jakate et al, (17.8%) Kim et al, (12%) Bennett et al Jung et al (6%) Chang et al (17%) Ahmadiyeh et al (3%) Jaffer et al (16%) Bernik et al (36%) Shandarajah et al (19%) Sakr et al (8%) Rizzo et al (24%) Kil et al (8%) Total (86%) 62 (6%) 81 (8%) 143 (14%)
74 Audience Participation 3 47 year old woman, fine pleomorphic calcifications Stereotactic core biopsy performed Very little tissue obtained, mostly fat, with focal epithelial element.multiple additional levels cut

75
76 Most appropriate action A. Benign, continue routine screening B. Re-biopsy patient C. Excise, it s at least atypical D. Excise, it s malignant E. I m not sure..help needed!!
77 Most appropriate action A. Benign, continue routine screening B. Re-biopsy patient C. Excise, it s at least atypical D. Excise, it s malignant E. I m not sure..help needed!!

78 FEHUT ADH

79

80
81 Core Biopsy Diagnosis Atypical Ductal Hyperplasia
82 ADH Dx. depends on quantitative features => can t be diagnosed reliably on core biopsy Atypical intraductal epithelial proliferation o r...at least amounting to ADH... Be conservative in borderline cases Should pass bilateral mastectomy test
83 Management - ADH Excise mammographic abnormality Not infrequently part of larger DCIS Nature of biopsy => quantitative criteria not met Underestimation of malignancy Rates of upgrade to DCIS or invasive cancer (18-87% using 14G) Vacuum-assisted methods 11G Lower underestimation rate (10-39%) Removal of entire lesion DCIS>>IBC (25%)
84 Audience Participation 4 53 year old woman Mammo: asymmetric density U/S: mass with microlobulation of margins U/S-guided core biopsy

85
86 What next? Patient follow-up, no surgery necessary Complete excision Complete excision with sentinel node Additional work-up of case None of the above
87 What next? Patient follow-up, no surgery necessary Complete excision Complete excision with sentinel node Additional work-up of case None of the above

88 LCIS within sclerosing adenosis E-cadherin
89 LCIS vs DCIS - An Important Distinction? Yes Clinical significance and management considerations LN indicator of increased risk (traditional) 4-5x - ALH 8-10x LCIS Bilateral Page et al, Human Pathology 1991; 22; LG DCIS risk is ipsilateral direct precursor Data shows that LN can act as a non-obligate precursor of IBC Risk of ipsilateral x3 ILC overrepresented LCIS and ILC shared genetic alterations
90 Should LN be Excised? Co-existent high risk lesion e.g. ADH Rad-path discordance Indeterminate features Variant LCIS Liberman et al, AM J Roentgenol 1999;173: Reviewed in : Jacobs et al, Am J Surg Patholol 2002;26:


91 Pleomorphic LCIS Classic LCIS with necrosis
92 Should LN be Excised? Classic LN only Upgrade 17-36% Studies retrospective, selection bias Small numbers Larger studies, rad-path correlation 1-3.4% Murray et al, Cancer, 2013, Chaudhary et al, Mod Path, 2013, Hwang et al. Mod Pathol 2008;21: Nagi et al. Cancer May 15;112(10):

93 Schnitt and Vincent-Salomon Columnar cell change Columnar cell hyperplasia atypia atypia Flat Epithelial Atypia

94

95

96 FEA
97 CCL - Management Non-atypical Excision not required If calcs are accounted for Atypical lesions Very low risk of progression Red flag Excise
98 Study CNB and Excision FEA N Upgrade N(%) Invasive N(%) DCIS N(%) LN N(%) Bonnett et al Guerra-Wallace et al Kunju and Kleer David et al Noel et al Piubello et al Ingegnoli et al Chivukula et al Senetta et al Noske et al Lavoue et al Rakha et al, N/A N/A Peres et al, Biggar et al, Khoumais, ADH N(%) Total (30%) 24 (4.2%) 37(6%) 45 (8%) 68 (12%)
99 Radial Scar/CSL Ducts radiating from central sclerotic core Fibrotic/elastotic centre FEHUT SA Papillary change DCIS ADH LN IMC Usually associated BPD; 10% AH/CIS, 1-5% IMC
100 Radial Scar Results of Outcome Studies Following CNB Majority of Studies recommend all RS be excised based on associated atypia in 10-15% of cases Carefully performed studies suggests: Rates of missed carcinomas (benign on CNB) 0-5% Majority of upgrades had at least AH on Bx Virtually no upgrades if : RS < 1.0 cm, esp if < 6-7 mm Sampled by 11 gauge needle or larger > 12 cores taken Brenner 2002 Sohn 2010 Cawson 2003 Rajan 2011
101 RS Treatment Approach Incidental Finding No Further Treatment Mammo Lesion of Interest No Atypia Mammo < 6-7 mm Well sampled 11 or 8 gauge needle No Atypia Limited Sample Atypia Malignancy Mammo discordant Excision
102 Take Home Messages Radiologic correlation pivotal Does the pathology explain the imaging? If not reconcile Still discordant? Re-biopsy Uncertain category? Appropriate mgt. CNB has limits Be conservative
Proliferative Breast Disease: implications of core biopsy diagnosis. Proliferative Breast Disease
 Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Controversies and Problematic Issues in Core Needle Biopsies (To excise or not to excise)
") Controversies and Problematic Issues in Core Needle Biopsies (To excise or not to excise) Laura C. Collins, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Schematic Representation
Controversies and Problematic Issues in Core Needle Biopsies (To excise or not to excise) Laura C. Collins, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Schematic Representation
3/27/2017. Disclosure of Relevant Financial Relationships. Papilloma???
 Management of Papillary Lesions Diagnosed at Rad Path Concordant Core Biopsy (CNB) Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Management of Papillary Lesions Diagnosed at Rad Path Concordant Core Biopsy (CNB) Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Treatment options for the precancerous Atypical Breast lesions. Prof. YOUNG-JIN SUH The Catholic University of Korea
 Treatment options for the precancerous Atypical Breast lesions Prof. YOUNG-JIN SUH The Catholic University of Korea Not so benign lesions? Imaging abnormalities(10% recall) lead to diagnostic evaluation,
Treatment options for the precancerous Atypical Breast lesions Prof. YOUNG-JIN SUH The Catholic University of Korea Not so benign lesions? Imaging abnormalities(10% recall) lead to diagnostic evaluation,
04/10/2018 HIGH RISK BREAST LESIONS. Pathology Perspectives of High Risk Breast Lesions ELEVATED RISK OF BREAST CANCER HISTORICAL PERSPECTIVES
 Pathology Perspectives of High Risk Breast Lesions Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head Director of Clinical Trials, Research and Development The University of Texas MD
Pathology Perspectives of High Risk Breast Lesions Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head Director of Clinical Trials, Research and Development The University of Texas MD
CNB vs Surgical Excision
 Update on Core Needle Biopsy of Non-palpable Breast Lesions Nour Sneige, M.D. UT MD Anderson Cancer Center Houston, Tx Image-Guided CNB of Breast Lesions An alternative to surgical biospy CNB vs Surgical
Update on Core Needle Biopsy of Non-palpable Breast Lesions Nour Sneige, M.D. UT MD Anderson Cancer Center Houston, Tx Image-Guided CNB of Breast Lesions An alternative to surgical biospy CNB vs Surgical
Columnar Cell Lesions
 Columnar Cell Lesions Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Question? Columnar cell lesions are: a) Annoying lesions
Columnar Cell Lesions Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Question? Columnar cell lesions are: a) Annoying lesions
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Image guided core biopsies:
 Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Enterprise Interest None
 Enterprise Interest None B3 lesions of the breast What are they at surgery? Case 4 Edi Brogi MD PhD Attending Pathologist - Director of Breast Pathology Memorial Sloan Kettering Cancer Center New York
Enterprise Interest None B3 lesions of the breast What are they at surgery? Case 4 Edi Brogi MD PhD Attending Pathologist - Director of Breast Pathology Memorial Sloan Kettering Cancer Center New York
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Texas Society of Pathologists 2013 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical
Papillary Lesions of the Breast Texas Society of Pathologists 2013 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical
Ductal Carcinoma in Situ. Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA
 Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Columnar Cell Lesions and Flat Epithelial Atypia
 Columnar Cell Lesions and Flat Epithelial Atypia Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Terminology for Columnar Cell
Columnar Cell Lesions and Flat Epithelial Atypia Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Terminology for Columnar Cell
Benign Mimics of Malignancy in Breast Pathology
 Arthur Purdy Stout Society of Surgical Pathologists Companion Meeting Benign Mimics of Malignancy in Breast Pathology Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School,
Arthur Purdy Stout Society of Surgical Pathologists Companion Meeting Benign Mimics of Malignancy in Breast Pathology Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School,
Flat Epithelial Atypia
 Flat Epithelial Atypia Richard Owings, M.D. University of Arkansas for Medical Sciences Department of Pathology Flat epithelial atypia can be a difficult lesion May be a subtle diagnosis Lots of changes
Flat Epithelial Atypia Richard Owings, M.D. University of Arkansas for Medical Sciences Department of Pathology Flat epithelial atypia can be a difficult lesion May be a subtle diagnosis Lots of changes
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Guidance on the management of B3 lesions
 Guidance on the management of B3 lesions Lesion diagnosed on 14g or vacuumassisted biopsy (VAB) Risk of upgrade Recommended investigation Suggested approach for follow-up if no malignancy on VAE awaiting
Guidance on the management of B3 lesions Lesion diagnosed on 14g or vacuumassisted biopsy (VAB) Risk of upgrade Recommended investigation Suggested approach for follow-up if no malignancy on VAE awaiting
Proliferative Epithelial lesions of the Breast. Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London
 Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
IBCM 2, April 2009, Sarajevo, Bosnia and Herzegovina
 Preoperative diagnosis and treatment planning in breast cancer The pathologist s perspective L. Mazzucchelli Istituto Cantonale di Patologia Locarno, Switzerland IBCM 2, 23-25 April 2009, Sarajevo, Bosnia
Preoperative diagnosis and treatment planning in breast cancer The pathologist s perspective L. Mazzucchelli Istituto Cantonale di Patologia Locarno, Switzerland IBCM 2, 23-25 April 2009, Sarajevo, Bosnia
Disclosures 5/27/2012. Outline of Talk. Outline of Talk. When Is LCIS Clinically Significant? Classic LCIS. Classic LCIS
 When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation
When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Excisional biopsy or long term follow-up results in breast high-risk lesions diagnosed at core needle biopsy
 Excisional biopsy or long term follow-up results in breast high-risk lesions diagnosed at core needle biopsy Poster No.: C-2515 Congress: ECR 2015 Type: Authors: Scientific Exhibit Ö. S. Okcu 1, A. Oktay
Excisional biopsy or long term follow-up results in breast high-risk lesions diagnosed at core needle biopsy Poster No.: C-2515 Congress: ECR 2015 Type: Authors: Scientific Exhibit Ö. S. Okcu 1, A. Oktay
Imaging in breast cancer. Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since
 Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
The management of B3 lesions with emphasis on lobular neoplasia
 The management of B3 lesions with emphasis on lobular neoplasia Abeer Shaaban Queen Elizabeth Hospital Birmingham NHSBSP core biopsy categories B1 - Normal B2 - Benign B3 Uncertain malignant potential
The management of B3 lesions with emphasis on lobular neoplasia Abeer Shaaban Queen Elizabeth Hospital Birmingham NHSBSP core biopsy categories B1 - Normal B2 - Benign B3 Uncertain malignant potential
Atypical proliferative lesions diagnosed on core biopsy - 6 year review
 Atypical proliferative lesions diagnosed on core biopsy - 6 year review Dr Angela Harris, Dr Julie Weigner & Dr Ricardo Vilain NSW Health Pathology Pathology North, Hunter Anatomical Pathology & Cytology
Atypical proliferative lesions diagnosed on core biopsy - 6 year review Dr Angela Harris, Dr Julie Weigner & Dr Ricardo Vilain NSW Health Pathology Pathology North, Hunter Anatomical Pathology & Cytology
Interpretation of Breast Pathology in the Era of Minimally Invasive Procedures
 Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine Jacksonville Medical Director, UF Health Breast Center Chief of Pathology
Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine Jacksonville Medical Director, UF Health Breast Center Chief of Pathology
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node
 Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Incidence of ductal lesions
 Ductal Proliferative Lesions of the Breast: From FEA to ADH to DCIS Incidence of ductal lesions Pre-mammography: DCIS < 3% of breast cancers, large palpable masses, with invasion Mammography: DCIS 25%
Ductal Proliferative Lesions of the Breast: From FEA to ADH to DCIS Incidence of ductal lesions Pre-mammography: DCIS < 3% of breast cancers, large palpable masses, with invasion Mammography: DCIS 25%
Controversies on the Management of High Risk Breast Lesions on Core Biopsy: An Update on the Literature
 Controversies on the Management of High Risk Breast Lesions on Core Biopsy: An Update on the Literature Dianne Georgian- Smith MD Brigham and Women s Hospital Associate Professor of Radiology, Harvard
Controversies on the Management of High Risk Breast Lesions on Core Biopsy: An Update on the Literature Dianne Georgian- Smith MD Brigham and Women s Hospital Associate Professor of Radiology, Harvard
Atypical Ductal Hyperplasia and Papillomas: A Comparison of Ultrasound Guided Breast Biopsy and Stereotactic Guided Breast Biopsy
 Atypical Ductal Hyperplasia and Papillomas: A Comparison of Ultrasound Guided Breast Biopsy and Stereotactic Guided Breast Biopsy Breast Cancer is the most common cancer diagnosed in women in the United
Atypical Ductal Hyperplasia and Papillomas: A Comparison of Ultrasound Guided Breast Biopsy and Stereotactic Guided Breast Biopsy Breast Cancer is the most common cancer diagnosed in women in the United
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Case study 1. Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research
 NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Non-mass Enhancement on Breast MRI. Aditi A. Desai, MD Margaret Ann Mays, MD
 Non-mass Enhancement on Breast MRI Aditi A. Desai, MD Margaret Ann Mays, MD Breast MRI Important screening and diagnostic tool, given its high sensitivity for breast cancer detection Breast MRI - Indications
Non-mass Enhancement on Breast MRI Aditi A. Desai, MD Margaret Ann Mays, MD Breast MRI Important screening and diagnostic tool, given its high sensitivity for breast cancer detection Breast MRI - Indications
6/3/2010. Outline of Talk. Lobular Breast Cancer: Definition of lobular differentiation. Common Problems in Diagnosing LCIS in Core Biopsies
 Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Surgical Pathology Issues of Practical Importance
 Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Advocating Nonsurgical Management of Patients With Small, Incidental Radial Scars at the Time of Needle Core Biopsy. A Study of 77 Cases
 Advocating Nonsurgical Management of Patients With Small, Incidental Radial Scars at the Time of Needle Core Biopsy A Study of 77 Cases Cathleen Matrai, MD; Timothy M. D Alfonso, MD; Lindsay Pharmer, MD;
Advocating Nonsurgical Management of Patients With Small, Incidental Radial Scars at the Time of Needle Core Biopsy A Study of 77 Cases Cathleen Matrai, MD; Timothy M. D Alfonso, MD; Lindsay Pharmer, MD;
Ana Sofia Preto 19/06/2013
 Ana Sofia Preto 19/06/2013 Understanding the underlying pathophysiologic processes leading to the various types of calcifications Description and illustration of the several types of calcifications, according
Ana Sofia Preto 19/06/2013 Understanding the underlying pathophysiologic processes leading to the various types of calcifications Description and illustration of the several types of calcifications, according
High risk lesions of the breast : Review of the current diagnostic and management strategies
 High risk lesions of the breast : Review of the current diagnostic and management strategies Poster No.: C-1204 Congress: ECR 2016 Type: Educational Exhibit Authors: P. Jagmohan, F. J. Pool, P. G. Pillay,
High risk lesions of the breast : Review of the current diagnostic and management strategies Poster No.: C-1204 Congress: ECR 2016 Type: Educational Exhibit Authors: P. Jagmohan, F. J. Pool, P. G. Pillay,
Diagnostic benefits of ultrasound-guided. CNB) versus mammograph-guided biopsy for suspicious microcalcifications. without definite breast mass
 versus mammograph-guided biopsy for suspicious microcalcifications. without definite breast mass") Volume 118 No. 19 2018, 531-543 ISSN: 1311-8080 (printed version); ISSN: 1314-3395 (on-line version) url: http://www.ijpam.eu ijpam.eu Diagnostic benefits of ultrasound-guided biopsy versus mammography-guided
Volume 118 No. 19 2018, 531-543 ISSN: 1311-8080 (printed version); ISSN: 1314-3395 (on-line version) url: http://www.ijpam.eu ijpam.eu Diagnostic benefits of ultrasound-guided biopsy versus mammography-guided
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Management of B3 lesions
 Management of B3 lesions Pathological view Abeer Shaaban Queen Elizabeth Hospital Birmingham FEA AIDP B3 lesions In situ Lobular neoplasia Papilloma Radial scar Fibroaepithelial lesion Mucocoele like lesion
Management of B3 lesions Pathological view Abeer Shaaban Queen Elizabeth Hospital Birmingham FEA AIDP B3 lesions In situ Lobular neoplasia Papilloma Radial scar Fibroaepithelial lesion Mucocoele like lesion
CLINICAL SIGNIFICANCE OF BENIGN EPITHELIAL CHANGES
 Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Mammographic imaging of nonpalpable breast lesions. Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand
 Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Breast Pathology. Breast Development
 Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
Benign, Reactive and Inflammatory Lesions of the Breast
 Benign, Reactive and Inflammatory Lesions of the Breast Marilin Rosa, MD Associate Member Section Head of Breast Pathology Department of Anatomic Pathology Program Director, Breast Pathology Fellowship
Benign, Reactive and Inflammatory Lesions of the Breast Marilin Rosa, MD Associate Member Section Head of Breast Pathology Department of Anatomic Pathology Program Director, Breast Pathology Fellowship
Epithelial Columnar Breast Lesions: Histopathology and Molecular Markers
 29th Annual International Conference Advances in the Application of Monoclonal Antibodies in Clinical Oncology and Symposium on Cancer Stem Cells 25 th -27t h June, 2012, Mykonos, Greece Epithelial Columnar
29th Annual International Conference Advances in the Application of Monoclonal Antibodies in Clinical Oncology and Symposium on Cancer Stem Cells 25 th -27t h June, 2012, Mykonos, Greece Epithelial Columnar
Original Report. Mucocele-Like Tumors of the Breast: Mammographic and Sonographic Appearances. Katrina Glazebrook 1 Carol Reynolds 2
 Katrina Glazebrook 1 Carol Reynolds 2 Received January 2, 2002; accepted after revision August 28, 2002. 1 Department of Radiology, Mayo Clinic, 200 First St. S.W., Rochester, MN 55905. Address correspondence
Katrina Glazebrook 1 Carol Reynolds 2 Received January 2, 2002; accepted after revision August 28, 2002. 1 Department of Radiology, Mayo Clinic, 200 First St. S.W., Rochester, MN 55905. Address correspondence
Columnar Cell Lesions. Columnar Cell Lesions and Flat Epithelial Atypia
 Columnar Cell Lesions and Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Columnar Cell Lesions Lesions characterized by columnar epithelial cells
Columnar Cell Lesions and Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Columnar Cell Lesions Lesions characterized by columnar epithelial cells
COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST
 COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST Aberrations of Normal Development and Involution (ANDI). The basic principles underlying the aberrations of normal development and involution (ANDI) classification
COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST Aberrations of Normal Development and Involution (ANDI). The basic principles underlying the aberrations of normal development and involution (ANDI) classification
Disclosures. Premalignant Lesions of the Breast: What Clinicians Want and Why. NY Times: Prone to Error: Earliest Steps to Find Cancer.
 Disclosures Premalignant Lesions of the Breast: What Clinicians Want and Why I have nothing to disclose Rick Baehner, MD Assistant Professor, UCSF Pathology NY Times: Prone to Error: Earliest Steps to
Disclosures Premalignant Lesions of the Breast: What Clinicians Want and Why I have nothing to disclose Rick Baehner, MD Assistant Professor, UCSF Pathology NY Times: Prone to Error: Earliest Steps to
Breast Imaging Lexicon
 9//201 200 BI RADS th Edition 201 BI RADS th Edition Breast Imaging Lexicon Mammographic Pathology and Assessment Categories Deborah Thames, R.T.(R)(M)(QM) The Advanced Health Education Center Nonmember:
9//201 200 BI RADS th Edition 201 BI RADS th Edition Breast Imaging Lexicon Mammographic Pathology and Assessment Categories Deborah Thames, R.T.(R)(M)(QM) The Advanced Health Education Center Nonmember:
Classic lobular neoplasia on core biopsy: a clinical and radio-pathologic correlation study with follow-up excision biopsy
 762 & 2013 USCAP, Inc All rights reserved 0893-3952/13 $32.00 Classic lobular neoplasia on core biopsy: a clinical and radio-pathologic correlation study with follow-up excision biopsy Shweta Chaudhary
762 & 2013 USCAP, Inc All rights reserved 0893-3952/13 $32.00 Classic lobular neoplasia on core biopsy: a clinical and radio-pathologic correlation study with follow-up excision biopsy Shweta Chaudhary
The Hot Topic for today is a biopsy from a 58-year-old woman who had worrisome mammographic calcifications on screening.
 The Hot Topic for today is a biopsy from a 58-year-old woman who had worrisome mammographic calcifications on screening. 1 My name is Dan Visscher; I am a consultant in the Division of Anatomic Pathology
The Hot Topic for today is a biopsy from a 58-year-old woman who had worrisome mammographic calcifications on screening. 1 My name is Dan Visscher; I am a consultant in the Division of Anatomic Pathology
Benign Breast Disease and Breast Cancer Risk
 Benign Breast Disease and Breast Cancer Risk Jean F. Simpson, M.D. Vanderbilt University Nashville, Tennessee December 1, 2011 Nashville Nashville Lebanon 1 Cedars of Lebanon State Park The American University
Benign Breast Disease and Breast Cancer Risk Jean F. Simpson, M.D. Vanderbilt University Nashville, Tennessee December 1, 2011 Nashville Nashville Lebanon 1 Cedars of Lebanon State Park The American University
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR
 INTERNAL MAMMARY SUPRACLAVICULAR") BREAST LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR HISTOLOGY LOBE: (10 in whole breast) LOBULE: (many per lobe) ACINUS/I, aka ALVEOLUS/I: (many per lobule) DUCT(S): INTRA- or
BREAST LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR HISTOLOGY LOBE: (10 in whole breast) LOBULE: (many per lobe) ACINUS/I, aka ALVEOLUS/I: (many per lobule) DUCT(S): INTRA- or
Promise of a beautiful day
 Promise of a beautiful day Ductal carcinoma in Situ Lobular Carcinoma in Situ Natural History Manosmed Tartous Oct 2009 Gérard ABADJIAN MD Pathology Department Hôtel-Dieu de France. Associate Professor
Promise of a beautiful day Ductal carcinoma in Situ Lobular Carcinoma in Situ Natural History Manosmed Tartous Oct 2009 Gérard ABADJIAN MD Pathology Department Hôtel-Dieu de France. Associate Professor
Atypical papillary lesions after core needle biopsy and subsequent breast carcinoma
 Asian Biomedicine Vol. 5 No. 2 April 2011; 243-248 DOI: 10.5372/1905-7415.0502.031 Original article Atypical papillary lesions after core needle biopsy and subsequent breast carcinoma Tuenchit Khamapirad
Asian Biomedicine Vol. 5 No. 2 April 2011; 243-248 DOI: 10.5372/1905-7415.0502.031 Original article Atypical papillary lesions after core needle biopsy and subsequent breast carcinoma Tuenchit Khamapirad
CPC 4 Breast Cancer. Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast.
 CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
Ultrasound of the Breast BASICS FOR THE ORDERING CLINICIAN
 Ultrasound of the Breast BASICS FOR THE ORDERING CLINICIAN Breast Ultrasound Anatomy Skin Breast Parenchyma Pectoralis Fascia Pectoralis Breast Ultrasound Anatomy Indications for Breast Ultrasound Palpable
Ultrasound of the Breast BASICS FOR THE ORDERING CLINICIAN Breast Ultrasound Anatomy Skin Breast Parenchyma Pectoralis Fascia Pectoralis Breast Ultrasound Anatomy Indications for Breast Ultrasound Palpable
Pathology of Lobular & Ductal Preneoplasia. Syed A Hoda, MD Weill-Cornell, New York, NY
 Pathology of Lobular & Ductal Preneoplasia Syed A Hoda, MD Weill-Cornell, New York, NY Proliferative Epithelial Changes in Breast A wide range of proliferative epithelial changes occur in the breast There
Pathology of Lobular & Ductal Preneoplasia Syed A Hoda, MD Weill-Cornell, New York, NY Proliferative Epithelial Changes in Breast A wide range of proliferative epithelial changes occur in the breast There
Pitfalls and Limitations of Breast MRI. Susan Orel Roth, MD Professor of Radiology University of Pennsylvania
 Pitfalls and Limitations of Breast MRI Susan Orel Roth, MD Professor of Radiology University of Pennsylvania Objectives Review the etiologies of false negative breast MRI examinations Discuss the limitations
Pitfalls and Limitations of Breast MRI Susan Orel Roth, MD Professor of Radiology University of Pennsylvania Objectives Review the etiologies of false negative breast MRI examinations Discuss the limitations
Imaging-Guided Core Needle Biopsy of Papillary Lesions of the Breast
 Eric L. Rosen 1 Rex C. Bentley 2 Jay A. Baker 1 Mary Scott Soo 1 Received January 30, 2002; accepted after revision April 12, 2002. 1 Department of Radiology, Breast Imaging Division, Duke University Medical
Eric L. Rosen 1 Rex C. Bentley 2 Jay A. Baker 1 Mary Scott Soo 1 Received January 30, 2002; accepted after revision April 12, 2002. 1 Department of Radiology, Breast Imaging Division, Duke University Medical
RSNA, /radiol Appendix E1. Methods
 RSNA, 2016 10.1148/radiol.2016151097 Appendix E1 Methods US and Near-infrared Data Acquisition Four optical wavelengths (740 nm, 780 nm, 808 nm, and 830 nm) were used to sequentially deliver the light
RSNA, 2016 10.1148/radiol.2016151097 Appendix E1 Methods US and Near-infrared Data Acquisition Four optical wavelengths (740 nm, 780 nm, 808 nm, and 830 nm) were used to sequentially deliver the light
The role of the cytologist in breast cancer screening
 The role of the cytologist in breast cancer screening I.Seili-Bekafigo, MD, PhD Clinical cytologist KBC Rijeka Croatian Society for Clinical Cytology Fine needle aspiration (FNA, FNAB, FNAC) Fine needle
The role of the cytologist in breast cancer screening I.Seili-Bekafigo, MD, PhD Clinical cytologist KBC Rijeka Croatian Society for Clinical Cytology Fine needle aspiration (FNA, FNAB, FNAC) Fine needle
Mammographic features and correlation with biopsy findings using 11-gauge stereotactic vacuum-assisted breast biopsy (SVABB)
") Original article Annals of Oncology 14: 450 454, 2003 DOI: 10.1093/annonc/mdh088 Mammographic features and correlation with biopsy findings using 11-gauge stereotactic vacuum-assisted breast biopsy (SVABB)
Original article Annals of Oncology 14: 450 454, 2003 DOI: 10.1093/annonc/mdh088 Mammographic features and correlation with biopsy findings using 11-gauge stereotactic vacuum-assisted breast biopsy (SVABB)
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
CURRICULUM FOR THE BREAST PATHOLOGY ROTATION UNIVERSITY OF FLORIDA DEPARTMENT OF PATHOLOGY
 CURRICULUM FOR THE BREAST PATHOLOGY ROTATION UNIVERSITY OF FLORIDA DEPARTMENT OF PATHOLOGY JULY, 2003 The following is a conceptual curriculum and set of guidelines for Pathology Residents on the Breast
CURRICULUM FOR THE BREAST PATHOLOGY ROTATION UNIVERSITY OF FLORIDA DEPARTMENT OF PATHOLOGY JULY, 2003 The following is a conceptual curriculum and set of guidelines for Pathology Residents on the Breast
In Situ Breast Carcinoma. James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA
 In Situ Breast Carcinoma James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA Content In Situ Ductal Carcinoma In Situ Lobular Carcinoma
In Situ Breast Carcinoma James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA Content In Situ Ductal Carcinoma In Situ Lobular Carcinoma
Good afternoon everyone. First of all many thanks to Dr. Bonaventura and Dr. Arn for inviting
 PATHOLOGY IN-SITU CARCINOMA, ROHIT BHARGAVA, MD 1 Good afternoon everyone. First of all many thanks to Dr. Bonaventura and Dr. Arn for inviting me here, it s great to be here and I m going to talk about
PATHOLOGY IN-SITU CARCINOMA, ROHIT BHARGAVA, MD 1 Good afternoon everyone. First of all many thanks to Dr. Bonaventura and Dr. Arn for inviting me here, it s great to be here and I m going to talk about
Utility of Adequate Core Biopsy Samples from Ultrasound Biopsies Needed for Today s Breast Pathology
 Utility of Adequate Core Biopsy Samples from Ultrasound Biopsies Needed for Today s Breast Pathology Ugur Ozerdem, M.D. 1 Abstract Background: There is a paradigm shift in breast biopsy philosophy. In
Utility of Adequate Core Biopsy Samples from Ultrasound Biopsies Needed for Today s Breast Pathology Ugur Ozerdem, M.D. 1 Abstract Background: There is a paradigm shift in breast biopsy philosophy. In
STEREOTACTIC BREAST BIOPSY: CORRELATION WITH HISTOLOGY
 3-rd Baltic Congress of Radiology, October 8-9, 2010 Riga Rūta Briedienė, Rūta Grigienė, Raimundas Meškauskas Institute of Oncology Vilnius University, National Centre of Pathology STEREOTACTIC BREAST
3-rd Baltic Congress of Radiology, October 8-9, 2010 Riga Rūta Briedienė, Rūta Grigienė, Raimundas Meškauskas Institute of Oncology Vilnius University, National Centre of Pathology STEREOTACTIC BREAST
DIAGNOSIS. Biopsy, Pathology and Subtypes. Knowledge Summary
 DIAGNOSIS Biopsy, Pathology and Subtypes Knowledge Summary DIAGNOSIS Biopsy, Pathology and Subtypes INTRODUCTION The success of an effective breast health care program is directly related to the availability
DIAGNOSIS Biopsy, Pathology and Subtypes Knowledge Summary DIAGNOSIS Biopsy, Pathology and Subtypes INTRODUCTION The success of an effective breast health care program is directly related to the availability
Breast core needle biopsy: issues and controversies
 S36 & 2010 USCAP, Inc. All rights reserved 0893-3952/10 $32.00 Breast core needle biopsy: issues and controversies Michael Bilous Institute of Clinical Pathology and Medical Research, Westmead Hospital
S36 & 2010 USCAP, Inc. All rights reserved 0893-3952/10 $32.00 Breast core needle biopsy: issues and controversies Michael Bilous Institute of Clinical Pathology and Medical Research, Westmead Hospital
Evaluation of Breast Specimens Removed by Needle Localization Technique
 Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Post Neoadjuvant therapy: issues in interpretation
 Post Neoadjuvant therapy: issues in interpretation Disclosure: Overview D Prognostic features in assessment of post treatment specimens: Tumor size Cellularity Grade Receptors LN Neoadjuvant chemotherapy:
Post Neoadjuvant therapy: issues in interpretation Disclosure: Overview D Prognostic features in assessment of post treatment specimens: Tumor size Cellularity Grade Receptors LN Neoadjuvant chemotherapy:
Low-grade Adenosquamous Carcinoma Coexisting with Sclerosing Adenosis of the Breast: A Case Report
 31 Case Report J. St. Marianna Univ. Vol. 8, pp. 31 35, 2017 Low-grade Adenosquamous Carcinoma Coexisting with Sclerosing Adenosis of the Breast: A Case Report Ryoko Oi 1, 2, Ichiro Maeda 1, Yoshio Aida
31 Case Report J. St. Marianna Univ. Vol. 8, pp. 31 35, 2017 Low-grade Adenosquamous Carcinoma Coexisting with Sclerosing Adenosis of the Breast: A Case Report Ryoko Oi 1, 2, Ichiro Maeda 1, Yoshio Aida
Breast Disease: What PCPs Need to Know. Eunice Cho MD FACS
 Breast Disease: What PCPs Need to Know Eunice Cho MD FACS New Breast Cancer Screening Guideline for women with average risk Every other year AGE 40 AGE 45 AGE 55 AGE 55 + Talk with your doctor about when
Breast Disease: What PCPs Need to Know Eunice Cho MD FACS New Breast Cancer Screening Guideline for women with average risk Every other year AGE 40 AGE 45 AGE 55 AGE 55 + Talk with your doctor about when
ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER. B.Zandi Professor of Radiology
 ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER B.Zandi Professor of Radiology Introduction In the USA, Breast Cancer is : The Most Common Non-Skin Cancer The Second Leading cause of
ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER B.Zandi Professor of Radiology Introduction In the USA, Breast Cancer is : The Most Common Non-Skin Cancer The Second Leading cause of
Breast Lesion Excision System-Intact (BLES): A Stereotactic Method of Biopsy of Suspicius Non-Palpable Mammographic Lesions.
: A Stereotactic Method of Biopsy of Suspicius Non-Palpable Mammographic Lesions.") Breast Lesion Excision System-Intact (BLES): A Stereotactic Method of Biopsy of Suspicius Non-Palpable Mammographic Lesions. Poster No.: C-1595 Congress: ECR 2014 Type: Authors: Scientific Exhibit I. Georgiou
Breast Lesion Excision System-Intact (BLES): A Stereotactic Method of Biopsy of Suspicius Non-Palpable Mammographic Lesions. Poster No.: C-1595 Congress: ECR 2014 Type: Authors: Scientific Exhibit I. Georgiou
Papillary Lesions in Breast Pathology Practice: Diagnostic Challenges and Practical Approach. A Six- Year Experience from a Tertiary Care Hospital
 Open Access Journal Research Article DOI: 10.23958/ijirms/vol02-i05/12 Papillary Lesions in Breast Pathology Practice: Diagnostic Challenges and Practical Approach. A Six- Year Experience from a Tertiary
Open Access Journal Research Article DOI: 10.23958/ijirms/vol02-i05/12 Papillary Lesions in Breast Pathology Practice: Diagnostic Challenges and Practical Approach. A Six- Year Experience from a Tertiary
Outline (1) Outline (2) Concepts in Prostate Pathology. Peculiarities of Prostate Cancer. Peculiarities of Prostate Cancer
 Outline (2) Concepts in Prostate Pathology. Peculiarities of Prostate Cancer. Peculiarities of Prostate Cancer") Concepts in Prostate Pathology Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Outline (1) Peculiarities of prostate cancer Peculiarities of prostate needle biopsy Needle bx vs. TURP Prostate
Concepts in Prostate Pathology Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Outline (1) Peculiarities of prostate cancer Peculiarities of prostate needle biopsy Needle bx vs. TURP Prostate
Diagnostic Dilemmas of Breast Imaging
 Diagnostic Dilemmas of Breast Imaging Common Causes of Error in Breast Cancer Detection By: Jason Cord, M.D. Mammography: Initial Imaging The standard for detection of breast cancer Screening mammography
Diagnostic Dilemmas of Breast Imaging Common Causes of Error in Breast Cancer Detection By: Jason Cord, M.D. Mammography: Initial Imaging The standard for detection of breast cancer Screening mammography
Quality ID #263: Preoperative Diagnosis of Breast Cancer National Quality Strategy Domain: Effective Clinical Care
 Quality ID #263: Preoperative Diagnosis of Breast Cancer National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
Quality ID #263: Preoperative Diagnosis of Breast Cancer National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
Diagnostic Problems in Breast Pathology How to avoid the pitfalls
 FORUM OF PATHOLOGY Diagnostic Problems in Breast Pathology How to avoid the pitfalls Professor C W Elston City Hospital Nottingham, United Kingdom Introduction Almost any breast lesion may produce diagnostic
FORUM OF PATHOLOGY Diagnostic Problems in Breast Pathology How to avoid the pitfalls Professor C W Elston City Hospital Nottingham, United Kingdom Introduction Almost any breast lesion may produce diagnostic
1 NORMAL HISTOLOGY AND METAPLASIAS
 1 NORMAL HISTOLOGY AND METAPLASIAS, MD Anatomy and Histology 1 Metaplasias 2 ANATOMY AND HISTOLOGY The female breast is composed of a branching duct system, which begins at the nipple with the major lactiferous
1 NORMAL HISTOLOGY AND METAPLASIAS, MD Anatomy and Histology 1 Metaplasias 2 ANATOMY AND HISTOLOGY The female breast is composed of a branching duct system, which begins at the nipple with the major lactiferous
BI-RADS CATEGORIZATION AND BREAST BIOPSY categorization in the selection of appropriate breast biopsy technique is also discussed. Patients and method
 Original Article Positive Predictive Value of BI-RADS Categorization in an Asian Population Yah-Yuen Tan, Siew-Bock Wee, Mona P.C. Tan and Bee-Kiang Chong, 1 Departments of General Surgery and 1Diagnostic
Original Article Positive Predictive Value of BI-RADS Categorization in an Asian Population Yah-Yuen Tan, Siew-Bock Wee, Mona P.C. Tan and Bee-Kiang Chong, 1 Departments of General Surgery and 1Diagnostic
Cystic Hypersecretory Carcinoma of the Breast:
 J Korean Soc Radiol 2010;62:287-294 Cystic Hypersecretory Carcinoma of the Breast: Sonographic Features with a Histological Correlation 1 Sang Yu Nam, M.D., Boo-Kyung Han, M.D., Jung Hee Shin, M.D., Eun
J Korean Soc Radiol 2010;62:287-294 Cystic Hypersecretory Carcinoma of the Breast: Sonographic Features with a Histological Correlation 1 Sang Yu Nam, M.D., Boo-Kyung Han, M.D., Jung Hee Shin, M.D., Eun
Diagnostic accuracy of ultrasonography-guided core needle biopsy for breast lesions
 Singapore Med J 01; 5(1) 40 Diagnostic accuracy of ultrasonography-guided core needle biopsy for breast lesions Wiratkapun Cl, MD, Treesit T1, MD, Wibulpolprasert E1, MD, Lertsithichai P, MD, MSc INTRODUCTION
Singapore Med J 01; 5(1) 40 Diagnostic accuracy of ultrasonography-guided core needle biopsy for breast lesions Wiratkapun Cl, MD, Treesit T1, MD, Wibulpolprasert E1, MD, Lertsithichai P, MD, MSc INTRODUCTION
BREAST MRI. VASILIKI FILIPPI RADIOLOGIST CT MRI & PET/CT Departments Hygeia Hospital, Athens, Greece
 BREAST MRI VASILIKI FILIPPI RADIOLOGIST CT MRI & PET/CT Departments Hygeia Hospital, Athens, Greece Breast ΜR Imaging (MRM) Breast MR imaging is an extremely powerful diagnostic tool, that when used in
BREAST MRI VASILIKI FILIPPI RADIOLOGIST CT MRI & PET/CT Departments Hygeia Hospital, Athens, Greece Breast ΜR Imaging (MRM) Breast MR imaging is an extremely powerful diagnostic tool, that when used in
Spindle Cell Lesions Of The Breast. Emad Rakha Professor of Breast Pathology and Consultant Pathologist
 Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
PAAF vs Core Biopsy en Lesiones Mamarias Case #1
 5/19/2014 PAAF vs Core Biopsy en Lesiones Mamarias Case #1 Fine Needle Aspiration Cytology of Breast: Correlation with Needle Core Biopsy 64-year-old woman Mass in breast Syed Hoda, MD CD31 Post-Radiation
5/19/2014 PAAF vs Core Biopsy en Lesiones Mamarias Case #1 Fine Needle Aspiration Cytology of Breast: Correlation with Needle Core Biopsy 64-year-old woman Mass in breast Syed Hoda, MD CD31 Post-Radiation
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
MEDICAL IMAGING AND BREAST DISEASE HOW CAN WE HELP YOU?
 MEDICAL IMAGING AND BREAST DISEASE HOW CAN WE HELP YOU? Barbara M. Preston, M.D. SCREENING MAMMOGRAPHY AVERAGE RISK PATIENTS KAISER RECOMMENDATION: ALL WOMEN (INCLUDING TRANSGENDER FEMALES) Every 1-21
MEDICAL IMAGING AND BREAST DISEASE HOW CAN WE HELP YOU? Barbara M. Preston, M.D. SCREENING MAMMOGRAPHY AVERAGE RISK PATIENTS KAISER RECOMMENDATION: ALL WOMEN (INCLUDING TRANSGENDER FEMALES) Every 1-21
BI-RADS Update. Martha B. Mainiero, MD, FACR, FSBI Brown University Rhode Island Hospital
 BI-RADS Update Martha B. Mainiero, MD, FACR, FSBI Brown University Rhode Island Hospital No Disclosures BI-RADS History 1980s Quality Issues ACR Accreditation BI-RADS 1994 2003 4 th Edition MRI, US January
BI-RADS Update Martha B. Mainiero, MD, FACR, FSBI Brown University Rhode Island Hospital No Disclosures BI-RADS History 1980s Quality Issues ACR Accreditation BI-RADS 1994 2003 4 th Edition MRI, US January