In Situ Breast Carcinoma. James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA
|
|
|
- Alicia McCormick
- 5 years ago
- Views:
Transcription
1 In Situ Breast Carcinoma James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA
2 Content In Situ Ductal Carcinoma In Situ Lobular Carcinoma Carcinoma with Mixed Ductal and Lobular Features/Pleomorphic Lobular Carcinoma In Situ Encysted Papillary Carcinoma
3 Ductal Carcinoma in Situ: Differential Diagnosis, Clinical Significance, and Prognostic Factors Traditional (Architectural) Classification Controversies & Problems Biologic Differences Segmental Distribution New Classification Systems Treatment
4 Classification of DCIS Traditional classification based primarily on architecture Comedo, solid, cribriform, papillary micropapillary, clinging





5





6





7



8





9





10
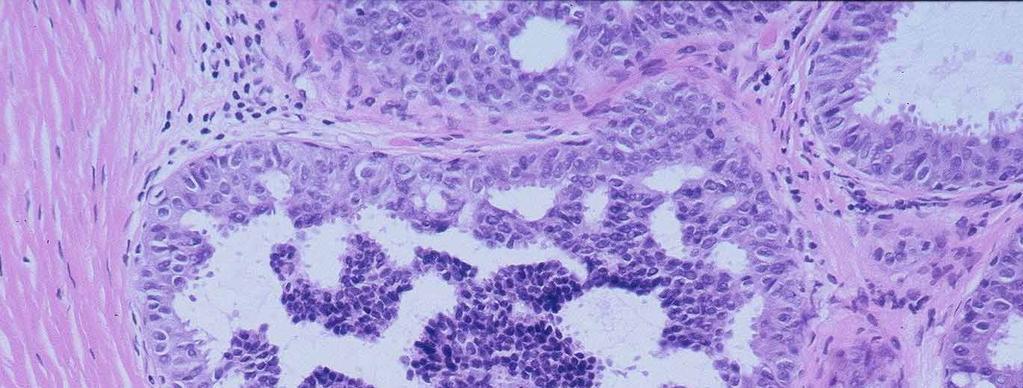
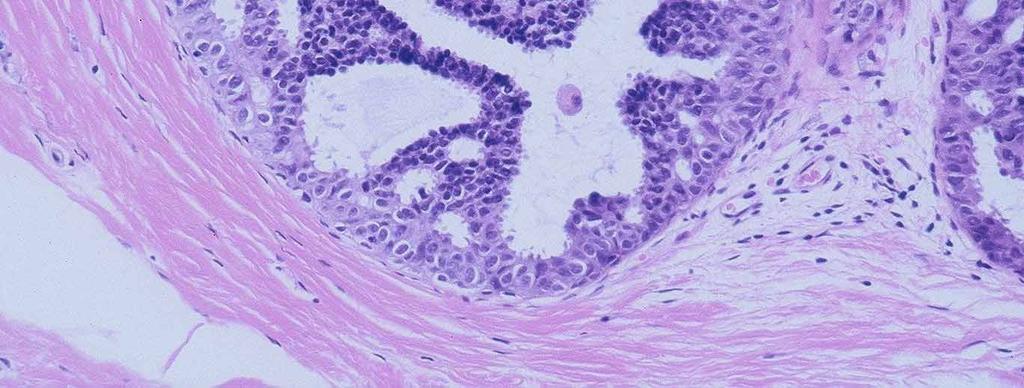
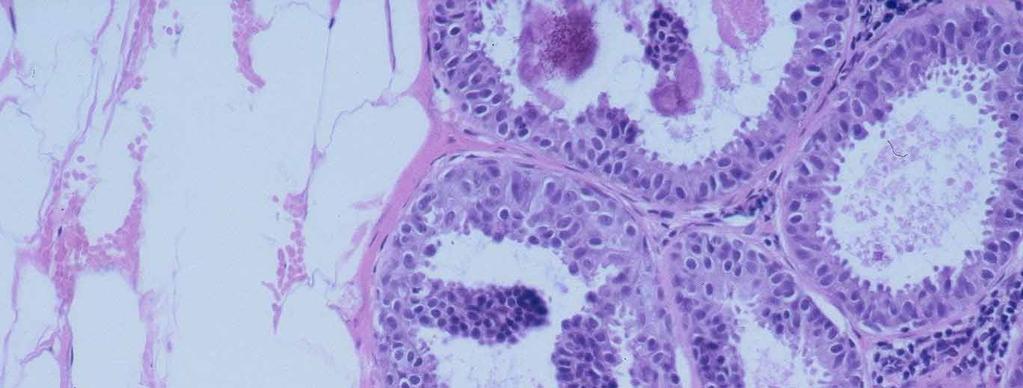
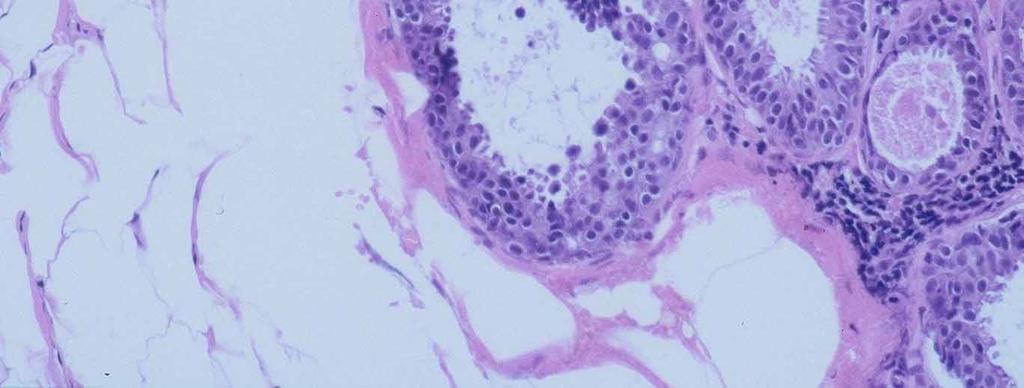
11 Papillary Ductal Carcinoma In Situ In contrast to papillomas, a uniform cell population Hyperchromatic cuboidal to columnar cells +/- clear epithelial cells near the base (globoid cells), which may mimic myoepithelial cells





12





13





14
15 Papillary Ductal Carcinoma In Situ Differential includes papilloma/invasive carcinoma It has fibrovascular cores There are no myoepithelial cells in the fibrovascular cores The blood vessels mark with smooth muscle markers p63 is negative in the cores It has myoepithelial cells around the periphery of the duct
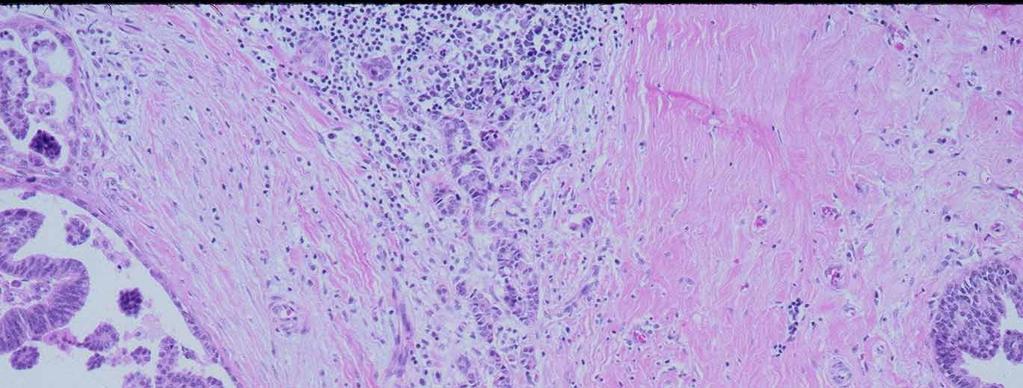
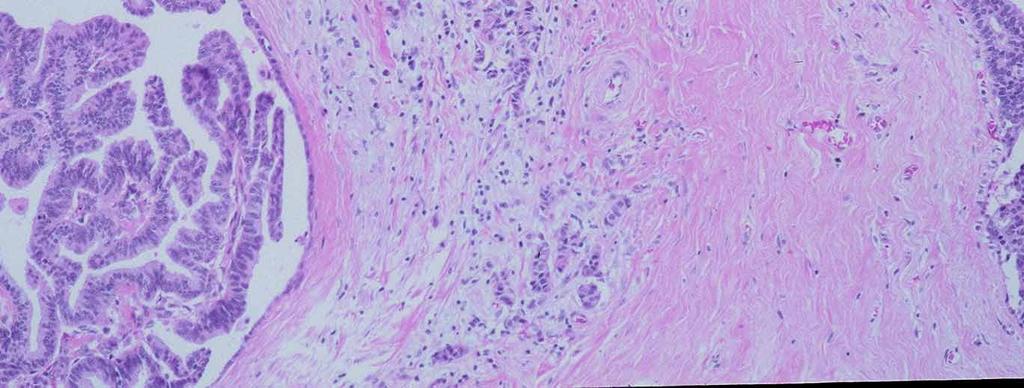
16 Papillary Ductal Carcinoma In Situ The associated invasive carcinoma usually NOS/NST Occasionally invasive in nests maintaining fibrovascular cores Invasive papillary carcinoma may metastasize maintaining a nested papillary appearance mimicking DCIS
17 Biphasic DCIS
18 Problems with the Architectural Classification System Definitions for subtypes not uniform Many lesions have mixtures of subtypes





19





20





21
22 Heterogeneity of DCIS 100 consecutive cases 76 non-comedo lesions mixture of patterns in 30% most commonly crib + mp 24 comedo lesions Non-comedo areas in 42% (Lennington, 1994)





23





24
25 DCIS While architecture varies considerably within an individual case Nuclear morphology is much more constant
26 DCIS Most newly proposed classification systems rely primarily on Nuclear morphology And have 3 grades





27
28 Alternative Classification Proposal Ductal Intraepithelial Neoplasia (DIN) Is appealing at some level UDH through high grade DCIS as a spectrum (DIN1-DIN3) There is no scientific evidence that ductal lesions progress in the breast following this pathway
29 DCIS: Differentiation High Grade Low Grade Cytology High grade Low grade Necrosis Frequent Infrequent Aneuploidy Frequent Infrequent
30 DCIS: Differentiation High Grade Low Grade ER+, PR+ Infrequent Frequent Proliferative rate High Low
31 DCIS: Differentiation High Grade Low Grade HER2/neu+ Frequent Infrequent bcl2+ Frequent Infrequent P53 mutations Frequent Infrequent Angiogenesis Frequent Infrequent
32 DCIS: Differentiation High Grade Low Grade Microinvasion More common Less common Calcifications Course granular Linear branching Psammomatous Fine granular
33 Genetic Abnormalities In DCIS High Grade Intermediate Low Grade Amplifications 17q12, 11q13 >Losses on 16q Losses on 16q Buerger H. J Pathol 1999; 187:396
34 DCIS The molecular and genetic abnormalities seen with DCIS are the same seen with invasive cancer Low grade DCIS has changes of low grade invasive cancer and of the special types of invasive cancer High grade DCIS has changes seen in high grade invasive cancer
35 Microarray Profiling Numerous studies have now documented that ductal carcinoma in situ has the same subtypes previously identified for invasive carcinoma Luminal a Luminal b HER-2/neu over expressing Basal like
36 DCIS: Size > 10 mm HER2/neu+ 83% HER2/neu- 33% De Potter C. Hum Pathol 1995; 26:601
37 Mammographic Appearance of DCIS Microcalcifications alone most common (~70%) Other (~30%) Soft tissue abnormality with microcalcifications Soft tissue abnormality alone mass sometimes circumscribed architectural distortion
38 DISTRIBUTION OF DCIS The myth of multicentricity Most cases show unicentric (segmental) distribution Involved segment may be large
39 Segments of the Breast
40
41 Mammographic vs Histologic Size (using standard views without magnification) Size discrepancy > 2cm High Grade 8/50 (16%) Low Grade 15/32 (47%) Holland et al 1984
42 DCIS: Differentiation High Grade Low Grade + excision margin Less frequent More frequent
43 Mammographic vs Pathologic Size ( magnificaton views ) 59 mastectomy specimens with DCIS Maximum size discrepancy ~1.5 cm; similar in High and Low Grade lesions Holland et al 1994
44 Mammographic vs Pathologic Size Magnification Views High Grade 3/14 (21%) Intermediate Grade 1/7 (14%) Low Grade 2/14 (14%) (Holland 1994)
45 Mammographic vs Pathologic Size Mammography still underestimated size of DCIS Size discrepancy < 2cm in ~80-85% of cases (Holland,1994)
46 Is there a relationship between Grade of DCIS and Outcome?
47 Local Recurrence Related to Histologic Grade (Type) RX F/U DCIS Grade high low Lagios CS 124 mos 33% 2% Schwartz CS 47 mos 48% 2% Collins CS 62 mos 25% 5% Solin CS+RT 5 yr 11% 2% Solin CS+Rt 15 yr 18% 15% B-17 CS 8yr 34% 29% B-17 CS+RT 8yr 15% 12%
48 Low Grade or Non-Comedo Groups Lagios Silverstein Solin Fisher NG 1 without necrosis NG 1 or 2 without necrosis NG 1 or 2 with necrosis, NG 1 or 2 without necrosis, NG 3 without necrosis NG 1 or 2 with necrosis, NG 1 or 2 without necrosis, NG 3 without necrosis, NG 3 with necrosis in <1/3
49 DCIS In evaluating studies of histologic type and risk of local recurrence, it is essential to understand the composition of the groups being compared (NOT EVERYONE S LOW GRADE IS THE SAME)
50 Considerations Regarding Recurrence and Histologic Type Poorly differentiated lesions are associated with necrosis and calcification Poorly differentiated lesions grow more rapidly Studies have relatively short follow-up Well differentiated lesions can recur up to 4 decades after biopsy(sanders M., Cancer 2005)
51 The higher recurrence rate in poorly differentiated DCIS may be a function of short follow-up and ease of detection
52 Local Recurrence Related to Histologic Type Influence of Length of F/U (Solin et al, CS+RT) Follow-up (act) Local Recurrence high grade low grade 5 years 11% 2% 8 years 20% 5% 10 years 18% 15%
53 Importance of Margin Assessment: DCIS Positive margins identified in many studies as the most important risk factor for local recurrence However, margin status alone may be suboptimal in defining adequacy of excision
54 NSABP B-17 Pathologic Subset Analysis, 1995 Margins and Local Recurrence (mean f/u 48 mos) CS CS +RT Positive/unk 25% 10% Negative 11% 4%
55 Unicentric (Segmental) Involvement Continuous Multifocal (gaps)
56 ?negative margin
57 Gaps Between Foci of DCIS (Faverly, Holland; 1994) Gap Size # (%) No gap 30 (50%) <5mm 19 (32%) 5-10mm 6(10%) >10mm 5 (8%)
58 Gap Size Related to DCIS Grade (Faverly, Holland; 1994) Gap size Grade Low Int. High (n=27) (n=9) (n=19) None 30% 45% 90% <5mm 44% 33% 5% 5-10mm 11% 11% 5% >10mm 15% 11% 0%
59 Gaps in Low Grade DCIS Large histologic sections High grade DCIS usually unifocal Low grade DCIS often multifocal Foschini MP., Human Pathology 2007
60 Gaps in Low Grade DCIS In order to diagnose low grade DCIS you need cellular monomorphism and architectural change Some areas of low grade DCIS are diagnostic while other areas lack sufficient architectural change The Gaps may be diagnostic not biological
61
62
63 Clonal Analysis of DCIS 7 cases of predominantly intraductal carcinoma studied: all monoclonal 3 cases with multiple foci of DCIS: every sample monoclonal, and same allele of PGK gene inactivated in each case All cases comedo type
64 Breast Failure in Patients with Negative Margins: The Wm Beaumont Experience # of Ducts With DCIS Near Margin # Ducts with DCIS 12 yr Recurrence Rate >8 25
65 DCIS 33% of patients with negative excision margins who had post-operative mammography performed, which revealed microcalcifications, had residual DCIS Waddell B, 2000
66 Even with free margins, if there is a significant amount of DCIS near the margins, a re-excision should be considered
67 Margin Width and Local Recurrence (Silverstein, 1999) Margin width >10mm: low risk of local recurrence for patients treated with CS+RT or CS alone risk of local recurrence not affected by Use of radiotherapy nuclear grade presence of comedo necrosis lesion size
68 Margin Width and Local Recurrence (Silverstein,2006) Margin width >10mm: 12Year probability of local recurrence with CS alone 13.9% (3.4% invasive) with CS+RT 2.5% (1.6% invasive)
69 How Wide is Wide Enough? Not a resolved issue Wider excisions associated with lower local recurrence but poorer cosmetic outcome Optimal margin width likely differs for patients treated with CS+RT and CS alone
70 Margin Width and Local Recurrence Wong, 2006(JCRT) Prospective study for small ( 2.5 cm) non-hg DCIS Margin width 1 cm No RT Accrual closed early due to high LR rate 5year LR 12%
71 ECOG ES5194 Excision +/- Tam DCIS Excised minimum 3mm margin Two arms Low or intermediate grade 2.5 cm or smaller High grade (NG3 + necrosis 1 cm or smaller) Specimen sequentially sectioned and completely embedded Post excision Mag mammo negative for calcs
72 ECOG ES5194 Excision +/- Tam 2006 Ipsilateral Breast recurrence at 5 years High grade 14.8% ( %) Low or intermediate 6.1% ( %) The use of radiotherapy decreased recurrence in all groups
73 Size (Extent) of DCIS Size related to likelihood of finding occult invasion lymph node metastases Size related to ability to perform adequate excision and achieve satisfactory cosmesis
74 Problems in Determining Size Often underestimated by mammography Grossly evident tumor rarely present Microscopically, lesion often present on >1 slide Accurate assessment requires total, sequential embedding or some modification thereof
75 Estimation of Size If mammo-path discrepant, use larger size
76 INK
77 A B C D
78 The BIDMC Approach All tissue is placed in disposable cassettes Labeled numerically and sequentially If the calcifications are associated with benign findings,no more sampling If DCIS, additional cassettes can be submitted maintaining orientation
79 Estimation of Size Blocks 3 mm thick x # of involved blocks
80 First Generation Randomized Clinical Trials Radiation Therapy Excision Observation
81 First Generation Randomized Trials With Available Results NSABP-B17 EORTC 10853
82 Local Recurrence Rates in NSABP-B17 and EORTC Trials NSABP-B17 EORTC Excision 27% (3.6%/yr) 26% (3.8%/yr) Excision+RT 12% (1.6%/yr) 15% (2.1%/yr) % Red n 56% 47%
83 NSABP B17 8 Year Update Breast Recurrence LE LE+RT Margins Free 29% 13% Involved/unk 39% 17% p=ns
84 NSABP B17 8 Year Update Breast Recurrence LE LE+RT Comedo Necrosis Abs/SI 23% 13% Mod/marked 40% 14%
85 Risk Factors For Local Recurrence EORTC Age < or = 40 Palpable lesion No radiation Intermediate or high grade DCIS Solid or Cribriform v Micropapillary or Clinging attern Doubtful margin All groups benefited from Radiation ijker, N et. al. JCO, 2006
86 Second Generation Randomized Clinical Trials Tamoxifen Excision + RT Placebo
87 NSABP B-24 Trial (5 yr actuarial results) Placebo Tam %redn p LR 9.3% 6.0% 35% 0.04 Invasive LR 4.2% 2.1% 50% 0.03 Non-inv LR 5.1% 3.9% 24% 0.43 CBC 3.4% 2.0% 41% 0.01 Lancet, 1999
88 Comparison of the 5-Year Local Recurrence Rates in NSABP B17 and B24 Trials B24 Tamoxifen 7% B24 Placebo 12% B17 Lumpectomy+XRT 12% B17 Lumpectomy 25%
89 Reduction in Recurrence Seen only in ER+ cases For this reason we are currently testing our cases of DCIS for estrogen receptors
90 Mortality of DCIS Treated by Mastectomy Historically up to 2% of patients with DCIS developed metastatic disease For patients with mammographically detected disease the risk is lower
91 Axillary Node Involvement in DCIS (Pre-Sentinel) In the National Cancer Data Base 3.7% had positive nodes (10946 women) Other modern series 0-0.5%
92 Sentinel Lymph Node (SLN) Involvement in DCIS With the SNL procedure and IHC it is not unusual to find positive nodes In recent series 6 to 13 % of cases are positive Most of these cases are identified by IHC alone or first These patients are generally offered adjuvant therapy
93 Sentinel Lymph Node (SLN) Involvement in DCIS Given that fewer than 2% of patients with DCIS will develop distant metastasis it is clear that IHC identification does not translate to a known risk
94 SLN in DCIS Two large studies have shown no relationship between positive SLN and recurrence in patients with DCIS Marby H., Giuliano A. E. and Silverstein MJ, A J Surg 2006, 192 : 455 Broekhuizen LN, Eur J Surg Oncol,2006, 32: 502
95 Sentinel Lymph Node (SLN) Involvement in DCIS For this reason we do not generally advocate for the use of IHC in those rare patients who undergo a SLN procedure
96 DCIS Consensus Conferences The European Organization for Research and Treatment of Cancer (EORTC) has held a number of DCIS Consensus Meetings In addition Gordon Schwartz MD organized Meetings in the USA
97 DCIS Consensus Conferences Recommendations for Reporting Nuclear grade Necrosis Polarization Architectural pattern(s) Margins Size of DCIS
98 DCIS Consensus Conferences Recommendations for Reporting Location of Microcalcifications Correlation of tissue specimens with specimen x-ray and mammographic findings
99 DCIS Consensus Conferences In terms of Pathology Reporting the conclusions were essentially the same
100 Conclusions Distribution in breast, histologic features, size, and adequacy of excision appear to be important considerations in selecting appropriate therapy for patients with DCIS
101 Conclusions Difficulties in assessing each of these factors Relative importance and interactions among them not well defined
102 Where Do We Go From Here? Long term results from clinical trials Methods to assess full extent of lesion and to assure its removal Methods to assess biologic potential Agents to prevent or suppress progression to invasion
103 Final Pathology Report for DCIS Specimen size Nuclear grade Architectural pattern(s) Necrosis Lesion size/extent Location of calcifications Margins
104 Intracystic Carcinoma Stains for myoepithelial cells are generally negative Is it DCIS is an enlarged duct or an expansile invasive carcinoma If a single cystic space is involved, excision is generally curative Examine adjacent tissue If DCIS adjacent, prognosis same as any DCIS
105 Intracystic Carcinoma The proliferation may be papillary, cribriform or solid The wall is often thick and may have entrapped epithelium Entrapped epithelium does not qualify for invasive carcinoma





106
107





108
109 Intracystic Papillary Carcinoma 917 cases from the California Tumor Registry from % classified as having invasion At 10 years the relative cumulative survival Insitu 96.8% With invasion 94.4% P.NS Grabowski, J Cancer 2008, 113: 916
110 Lobular Neoplasia Atypical Lobular Hyperplasia Lobular Carcinoma insitu
111 Lobular Neoplasia (LCIS/ALH) Cytologically both lesions are identical Monomorphic cell population (usually small) May have signet ring cells Pagetoid spread common Hallmark is lack of cellular cohesion (ecadherin negative)
112 Lobular Neoplasia (LCIS/ALH) The difference between LCIS and ALH depends on the degree of lobular involvement and distention Both lesions are generally felt to indicate elevated risk for subsequent development of breast cancer. There is a greater risk associated with LCIS than ALH





113
114 Classical LCIS Type A- Small cells with uniform nuclei Type B- Larger cells with more variable nuclei; with or without prominent nucleoli
115 Markers in Classic LCIS ER Proliferation Rate HER2 p53 E-Cadherin Positive Low Negative Negative Negative
116 Lobular Neoplasia (LCIS/ALH) In most women it is thought of as a risk factor for development of any type of breast cancer In women who develop Invasive Lobular Carcinoma (ILC) it is a direct precursor
117 Lobular Neoplasia (LCIS/ALH) FREQUENCY Depends on definition Between % of biopsies done for a mass Much higher in mammographically driven biopsies ~ 5-15% 80-90% found in pre menopausal women
118 Lobular Neoplasia (LCIS/ALH) It is almost always an incidental finding While not usually a cause of microcalcifications frequently present near calcifications Multicentric in 60-80% of mastectomy specimens with LCIS/ALH Bilateral in ~ 25-35% of cases
119 Lobular Neoplasia (LCIS/ALH) NATURAL HISTORY Subsequent invasive carcinoma % Relative Risk 5-12 times control populations % invasive breast cancer per year of FU studies with greater than 5 years of follow up
120 Lobular Neoplasia (LCIS/ALH) MANAGEMENT NSABP trials show a 50% reduction in breast cancer when these patients receive Tamoxifen Bilateral Mastectomy Observation Some advocate Unilateral Subcutaneous Mastectomy
121 Pleomorphic LCIS A lesion that lacks cohesion It has major biologic differences from what is usually felt to be LCIS Often has necrosis and apoptosis Has a high proliferative rate
122 Pleomorphic LCIS An E cadherin negative in situ carcinoma High nuclear grade Usually ER positive High proliferative rate (47-92% of cases) Her2/neu positive (5-25% of cases)
123 LCIS with Comedo Necrosis 18 cases of E cadherin negative LIN Usually associated with mammographic calcifications Invasive carcinoma present in 67% of cases
124 Pleomorphic LCIS / LCIS with Comedo Necrosis More aggressive biological characteristics More frequently associated with invasive carcinoma
125 Pleomorphic LCIS We do not have outcome studies of observation alone with these lesions In order not to confuse the clinicians, at this time, I diagnose these lesions as insitu carcinoma with mixed ductal and lobular features And advise they be treated as one would a comparable DCIS
126 Histologic Differential Diagnosis between LCIS and Solid Small Cell DCIS Feature LCIS DCIS Loss of cohesion Yes No Intracytoplasmic Present Absent vacuoles Pagetoid ductal Present Absent spread Microacini Absent Present Polarity of cells at periphery Absent Present
127 Questions
Ductal Carcinoma in Situ. Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA
 Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
CLINICAL SIGNIFICANCE OF BENIGN EPITHELIAL CHANGES
 Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Columnar Cell Lesions
 Columnar Cell Lesions Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Question? Columnar cell lesions are: a) Annoying lesions
Columnar Cell Lesions Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Question? Columnar cell lesions are: a) Annoying lesions
Proliferative Epithelial lesions of the Breast. Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London
 Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
Surgical Pathology Issues of Practical Importance
 Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
6/3/2010. Outline of Talk. Lobular Breast Cancer: Definition of lobular differentiation. Common Problems in Diagnosing LCIS in Core Biopsies
 Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Columnar Cell Lesions. Columnar Cell Lesions and Flat Epithelial Atypia
 Columnar Cell Lesions and Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Columnar Cell Lesions Lesions characterized by columnar epithelial cells
Columnar Cell Lesions and Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Columnar Cell Lesions Lesions characterized by columnar epithelial cells
04/10/2018 HIGH RISK BREAST LESIONS. Pathology Perspectives of High Risk Breast Lesions ELEVATED RISK OF BREAST CANCER HISTORICAL PERSPECTIVES
 Pathology Perspectives of High Risk Breast Lesions Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head Director of Clinical Trials, Research and Development The University of Texas MD
Pathology Perspectives of High Risk Breast Lesions Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head Director of Clinical Trials, Research and Development The University of Texas MD
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006
 Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Texas Society of Pathologists 2013 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical
Papillary Lesions of the Breast Texas Society of Pathologists 2013 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical
Ductal Carcinoma-in-Situ: New Concepts and Controversies
 Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Disclosures. Premalignant Lesions of the Breast: What Clinicians Want and Why. NY Times: Prone to Error: Earliest Steps to Find Cancer.
 Disclosures Premalignant Lesions of the Breast: What Clinicians Want and Why I have nothing to disclose Rick Baehner, MD Assistant Professor, UCSF Pathology NY Times: Prone to Error: Earliest Steps to
Disclosures Premalignant Lesions of the Breast: What Clinicians Want and Why I have nothing to disclose Rick Baehner, MD Assistant Professor, UCSF Pathology NY Times: Prone to Error: Earliest Steps to
LOBULAR CARCINOMA IN SITU: WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE
 : WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE Benjamin O. Anderson, M.D. Director, Breast Health Clinic Professor of Surgery and Global Health, University of Washington Joint Member, Fred Hutchinson Cancer
: WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE Benjamin O. Anderson, M.D. Director, Breast Health Clinic Professor of Surgery and Global Health, University of Washington Joint Member, Fred Hutchinson Cancer
Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction
 Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction Aldona J. Spiegel, M.D., and Charles E. Butler, M.D. Houston, Texas Skin-sparing
Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction Aldona J. Spiegel, M.D., and Charles E. Butler, M.D. Houston, Texas Skin-sparing
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Cytyc Corporation - Case Presentation Archive - March 2002
 FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Radiation and DCIS. The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging
 Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Good afternoon everyone. First of all many thanks to Dr. Bonaventura and Dr. Arn for inviting
 PATHOLOGY IN-SITU CARCINOMA, ROHIT BHARGAVA, MD 1 Good afternoon everyone. First of all many thanks to Dr. Bonaventura and Dr. Arn for inviting me here, it s great to be here and I m going to talk about
PATHOLOGY IN-SITU CARCINOMA, ROHIT BHARGAVA, MD 1 Good afternoon everyone. First of all many thanks to Dr. Bonaventura and Dr. Arn for inviting me here, it s great to be here and I m going to talk about
Evaluation of Breast Specimens Removed by Needle Localization Technique
 Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Disclosures 5/27/2012. Outline of Talk. Outline of Talk. When Is LCIS Clinically Significant? Classic LCIS. Classic LCIS
 When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation
When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation
Management of Ductal Carcinoma In Situ
 Management of Ductal Carcinoma In Situ Stella Hetelekidis, MD Stuart J. Schnitt, MD Monica Morrow, MD Jay R. Harris, MD Introduction Ductal carcinoma in situ (DCIS), also known as intraductal carcinoma,
Management of Ductal Carcinoma In Situ Stella Hetelekidis, MD Stuart J. Schnitt, MD Monica Morrow, MD Jay R. Harris, MD Introduction Ductal carcinoma in situ (DCIS), also known as intraductal carcinoma,
Carcinoma mammario: le istologie non frequenti. Valentina Guarneri Università di Padova IOV-IRCCS
 Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Columnar Cell Lesions and Flat Epithelial Atypia
 Columnar Cell Lesions and Flat Epithelial Atypia Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Terminology for Columnar Cell
Columnar Cell Lesions and Flat Epithelial Atypia Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Terminology for Columnar Cell
Treatment options for the precancerous Atypical Breast lesions. Prof. YOUNG-JIN SUH The Catholic University of Korea
 Treatment options for the precancerous Atypical Breast lesions Prof. YOUNG-JIN SUH The Catholic University of Korea Not so benign lesions? Imaging abnormalities(10% recall) lead to diagnostic evaluation,
Treatment options for the precancerous Atypical Breast lesions Prof. YOUNG-JIN SUH The Catholic University of Korea Not so benign lesions? Imaging abnormalities(10% recall) lead to diagnostic evaluation,
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
A712(18)- Test slide, Breast cancer tissues with corresponding normal tissues
- Test slide, Breast cancer tissues with corresponding normal tissues") A712(18)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
A712(18)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
Diseases of the breast (2 of 2) Breast cancer
 Breast cancer") Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Epithelial Columnar Breast Lesions: Histopathology and Molecular Markers
 29th Annual International Conference Advances in the Application of Monoclonal Antibodies in Clinical Oncology and Symposium on Cancer Stem Cells 25 th -27t h June, 2012, Mykonos, Greece Epithelial Columnar
29th Annual International Conference Advances in the Application of Monoclonal Antibodies in Clinical Oncology and Symposium on Cancer Stem Cells 25 th -27t h June, 2012, Mykonos, Greece Epithelial Columnar
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine
 Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Promise of a beautiful day
 Promise of a beautiful day Ductal carcinoma in Situ Lobular Carcinoma in Situ Natural History Manosmed Tartous Oct 2009 Gérard ABADJIAN MD Pathology Department Hôtel-Dieu de France. Associate Professor
Promise of a beautiful day Ductal carcinoma in Situ Lobular Carcinoma in Situ Natural History Manosmed Tartous Oct 2009 Gérard ABADJIAN MD Pathology Department Hôtel-Dieu de France. Associate Professor
ACRIN 6666 Therapeutic Surgery Form
 S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
Speaker s Bureau. Travel expenses. Advisory Boards. Stock. Genentech Invuity Medtronic Pacira. Faxitron. Dune TransMed7 Genomic Health.
 Management of DCIS Shawna C. Willey, MD, FACS Professor of Surgery, Georgetown University Director, Medstar Regional Breast Health Program Chief, Department of Surgery Medstar Georgetown University Hospital
Management of DCIS Shawna C. Willey, MD, FACS Professor of Surgery, Georgetown University Director, Medstar Regional Breast Health Program Chief, Department of Surgery Medstar Georgetown University Hospital
Proliferative Breast Disease: implications of core biopsy diagnosis. Proliferative Breast Disease
 Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Mammographic imaging of nonpalpable breast lesions. Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand
 Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Case study 1. Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research
 NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node
 Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Interpretation of Breast Pathology in the Era of Minimally Invasive Procedures
 Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine Jacksonville Medical Director, UF Health Breast Center Chief of Pathology
Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine Jacksonville Medical Director, UF Health Breast Center Chief of Pathology
Invasive Papillary Breast Carcinoma
 410 This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the
410 This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Image guided core biopsies:
 Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Histological Type. Morphological and Molecular Typing of breast Cancer. Nottingham Tenovus Primary Breast Cancer Study. Survival (%) Ian Ellis
 Ian Ellis") Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Pathology of Lobular & Ductal Preneoplasia. Syed A Hoda, MD Weill-Cornell, New York, NY
 Pathology of Lobular & Ductal Preneoplasia Syed A Hoda, MD Weill-Cornell, New York, NY Proliferative Epithelial Changes in Breast A wide range of proliferative epithelial changes occur in the breast There
Pathology of Lobular & Ductal Preneoplasia Syed A Hoda, MD Weill-Cornell, New York, NY Proliferative Epithelial Changes in Breast A wide range of proliferative epithelial changes occur in the breast There
Breast Pathology. Breast Development
 Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
3/27/2017. Disclosure of Relevant Financial Relationships. Papilloma???
 Management of Papillary Lesions Diagnosed at Rad Path Concordant Core Biopsy (CNB) Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Management of Papillary Lesions Diagnosed at Rad Path Concordant Core Biopsy (CNB) Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Flat Epithelial Atypia
 Flat Epithelial Atypia Richard Owings, M.D. University of Arkansas for Medical Sciences Department of Pathology Flat epithelial atypia can be a difficult lesion May be a subtle diagnosis Lots of changes
Flat Epithelial Atypia Richard Owings, M.D. University of Arkansas for Medical Sciences Department of Pathology Flat epithelial atypia can be a difficult lesion May be a subtle diagnosis Lots of changes
A DEEPER DIVE INTO DUCTAL CARCINOMA IN SITU: CLINICAL AND PATHOLOGIC CONSIDERATIONS IN 2015
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 A DEEPER DIVE INTO DUCTAL CARCINOMA IN SITU: CLINICAL AND PATHOLOGIC CONSIDERATIONS IN 2015
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 A DEEPER DIVE INTO DUCTAL CARCINOMA IN SITU: CLINICAL AND PATHOLOGIC CONSIDERATIONS IN 2015
When do you need PET/CT or MRI in early breast cancer?
 When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
CPC 4 Breast Cancer. Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast.
 CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
CPC 4 Breast Cancer Rochelle Harwood, a 35 year old sales assistant, presents to her GP because she has noticed a painless lump in her left breast. 1. What are the most likely diagnoses of this lump? Fibroadenoma
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR
 INTERNAL MAMMARY SUPRACLAVICULAR") BREAST LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR HISTOLOGY LOBE: (10 in whole breast) LOBULE: (many per lobe) ACINUS/I, aka ALVEOLUS/I: (many per lobule) DUCT(S): INTRA- or
BREAST LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR HISTOLOGY LOBE: (10 in whole breast) LOBULE: (many per lobe) ACINUS/I, aka ALVEOLUS/I: (many per lobule) DUCT(S): INTRA- or
Resection Margins in Breast Conserving Surgery. Alberto Costa, MD Canton Ticino Breast Unit Lugano, Switzerland
 Resection Margins in Breast Conserving Surgery Alberto Costa, MD Canton Ticino Breast Unit Lugano, Switzerland Breast Conserving Surgery 1 Probably one of the most important innovation in cancer surgery
Resection Margins in Breast Conserving Surgery Alberto Costa, MD Canton Ticino Breast Unit Lugano, Switzerland Breast Conserving Surgery 1 Probably one of the most important innovation in cancer surgery
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
High risk lesions of the breast : Review of the current diagnostic and management strategies
 High risk lesions of the breast : Review of the current diagnostic and management strategies Poster No.: C-1204 Congress: ECR 2016 Type: Educational Exhibit Authors: P. Jagmohan, F. J. Pool, P. G. Pillay,
High risk lesions of the breast : Review of the current diagnostic and management strategies Poster No.: C-1204 Congress: ECR 2016 Type: Educational Exhibit Authors: P. Jagmohan, F. J. Pool, P. G. Pillay,
Triple Negative Breast Cancer
 Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Triple Negative Breast Cancer Prof. Dr. Pornchai O-charoenrat Division of Head-Neck & Breast Surgery Department of Surgery Faculty of Medicine Siriraj Hospital Breast Cancer Classification Traditional
Quality ID #263: Preoperative Diagnosis of Breast Cancer National Quality Strategy Domain: Effective Clinical Care
 Quality ID #263: Preoperative Diagnosis of Breast Cancer National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
Quality ID #263: Preoperative Diagnosis of Breast Cancer National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues
- Test slide, Breast cancer tissues with corresponding normal tissues") A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
The Hot Topic for today is a biopsy from a 58-year-old woman who had worrisome mammographic calcifications on screening.
 The Hot Topic for today is a biopsy from a 58-year-old woman who had worrisome mammographic calcifications on screening. 1 My name is Dan Visscher; I am a consultant in the Division of Anatomic Pathology
The Hot Topic for today is a biopsy from a 58-year-old woman who had worrisome mammographic calcifications on screening. 1 My name is Dan Visscher; I am a consultant in the Division of Anatomic Pathology
The management of B3 lesions with emphasis on lobular neoplasia
 The management of B3 lesions with emphasis on lobular neoplasia Abeer Shaaban Queen Elizabeth Hospital Birmingham NHSBSP core biopsy categories B1 - Normal B2 - Benign B3 Uncertain malignant potential
The management of B3 lesions with emphasis on lobular neoplasia Abeer Shaaban Queen Elizabeth Hospital Birmingham NHSBSP core biopsy categories B1 - Normal B2 - Benign B3 Uncertain malignant potential
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
It is a malignancy originating from breast tissue
 59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
Breast Cancer. Dr Rodney Itaki Anatomical Pathology Discipline Division of Pathology
 Breast Cancer Dr Rodney Itaki Anatomical Pathology Discipline Division of Pathology Muscles Muscles underneath the breasts separating them from the ribs Breast has no muscle tissue 2 Female Breast Anatomy
Breast Cancer Dr Rodney Itaki Anatomical Pathology Discipline Division of Pathology Muscles Muscles underneath the breasts separating them from the ribs Breast has no muscle tissue 2 Female Breast Anatomy
Lobular Carcinoma In Situ Variants in Breast Cores
 Lobular Carcinoma In Situ Variants in Breast Cores Potential for Misdiagnosis, Upgrade Rates at Surgical Excision, and Practical Implications Megan E. Sullivan, MD; Seema A. Khan, MD; Yurdanur Sullu, MD;
Lobular Carcinoma In Situ Variants in Breast Cores Potential for Misdiagnosis, Upgrade Rates at Surgical Excision, and Practical Implications Megan E. Sullivan, MD; Seema A. Khan, MD; Yurdanur Sullu, MD;
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation
 Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Disclosure. Objectives 03/19/2019. Current Issues in Management of DCIS Radiation Oncology Considerations
 Current Issues in Management of DCIS Radiation Oncology Considerations Fariba Asrari, M.D. Director. Johns Hopkins Breast Center at Green Spring Station Department of Radiation Oncology & Molecular Sciences
Current Issues in Management of DCIS Radiation Oncology Considerations Fariba Asrari, M.D. Director. Johns Hopkins Breast Center at Green Spring Station Department of Radiation Oncology & Molecular Sciences
Protocol for the Examination of Biopsy Specimens From Patients With Invasive Carcinoma of the Breast
 Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: BreastInvasive 1.0.0.0 Protocol Posting Date: February 2019 Accreditation Requirements The use of
Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: BreastInvasive 1.0.0.0 Protocol Posting Date: February 2019 Accreditation Requirements The use of
What are Adequate Margins of Resection for Breast-Conserving Therapy?
 What are Adequate Margins of Resection for Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School What are Adequate Margins
What are Adequate Margins of Resection for Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School What are Adequate Margins
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
Incidence of ductal lesions
 Ductal Proliferative Lesions of the Breast: From FEA to ADH to DCIS Incidence of ductal lesions Pre-mammography: DCIS < 3% of breast cancers, large palpable masses, with invasion Mammography: DCIS 25%
Ductal Proliferative Lesions of the Breast: From FEA to ADH to DCIS Incidence of ductal lesions Pre-mammography: DCIS < 3% of breast cancers, large palpable masses, with invasion Mammography: DCIS 25%
Benign Breast Disease and Breast Cancer Risk
 Benign Breast Disease and Breast Cancer Risk Jean F. Simpson, M.D. Vanderbilt University Nashville, Tennessee December 1, 2011 Nashville Nashville Lebanon 1 Cedars of Lebanon State Park The American University
Benign Breast Disease and Breast Cancer Risk Jean F. Simpson, M.D. Vanderbilt University Nashville, Tennessee December 1, 2011 Nashville Nashville Lebanon 1 Cedars of Lebanon State Park The American University
Imaging in breast cancer. Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since
 Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
CURRICULUM FOR THE BREAST PATHOLOGY ROTATION UNIVERSITY OF FLORIDA DEPARTMENT OF PATHOLOGY
 CURRICULUM FOR THE BREAST PATHOLOGY ROTATION UNIVERSITY OF FLORIDA DEPARTMENT OF PATHOLOGY JULY, 2003 The following is a conceptual curriculum and set of guidelines for Pathology Residents on the Breast
CURRICULUM FOR THE BREAST PATHOLOGY ROTATION UNIVERSITY OF FLORIDA DEPARTMENT OF PATHOLOGY JULY, 2003 The following is a conceptual curriculum and set of guidelines for Pathology Residents on the Breast
GOALS AND OBJECTIVES BREAST PATHOLOGY
 GOALS AND OBJECTIVES BREAST PATHOLOGY LEVEL: PGY2, PGY3, PGY5 A number of these rotations are introductory in nature, as they are major subspecialties, and are followed by two more blocks in PGY-3, during
GOALS AND OBJECTIVES BREAST PATHOLOGY LEVEL: PGY2, PGY3, PGY5 A number of these rotations are introductory in nature, as they are major subspecialties, and are followed by two more blocks in PGY-3, during
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
Atypical proliferative lesions diagnosed on core biopsy - 6 year review
 Atypical proliferative lesions diagnosed on core biopsy - 6 year review Dr Angela Harris, Dr Julie Weigner & Dr Ricardo Vilain NSW Health Pathology Pathology North, Hunter Anatomical Pathology & Cytology
Atypical proliferative lesions diagnosed on core biopsy - 6 year review Dr Angela Harris, Dr Julie Weigner & Dr Ricardo Vilain NSW Health Pathology Pathology North, Hunter Anatomical Pathology & Cytology
American Journal of Cancer Case Reports. Invasive Papillary Carcinoma of Male Breast: A Rare Case Report
 American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr SantraAetal. American Journal of Cancer Case Reports 2014, 3:56-61 Page 1 of 6 Vol 3 Article ID 20140617, 6 pages Case Report
American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr SantraAetal. American Journal of Cancer Case Reports 2014, 3:56-61 Page 1 of 6 Vol 3 Article ID 20140617, 6 pages Case Report
10 reasons why it makes sense to rename DCIS to minimise overtreatment? PRO: Mike Dixon OBE Edinburgh Breast Unit
 10 reasons why it makes sense to rename DCIS to minimise overtreatment? PRO: Mike Dixon OBE Edinburgh Breast Unit 10 reasons why it makes sense to rename DCIS to minimise overtreatment? PRO: Mike Dixon
10 reasons why it makes sense to rename DCIS to minimise overtreatment? PRO: Mike Dixon OBE Edinburgh Breast Unit 10 reasons why it makes sense to rename DCIS to minimise overtreatment? PRO: Mike Dixon
AMSER Case of the Month: November 2018
 AMSER Case of the Month: November 2018 52 year old female with an abnormal screening mammogram Areeg Rehman, MS 4 Nova Southeastern University Rebecca T. Sivarajah, MD Penn State University College of
AMSER Case of the Month: November 2018 52 year old female with an abnormal screening mammogram Areeg Rehman, MS 4 Nova Southeastern University Rebecca T. Sivarajah, MD Penn State University College of
259 Patients with DCIS of the breast applying USC/Van Nuys prognostic index: a retrospective review with long term follow up
 Breast Cancer Res Treat (2008) 109:405 416 DOI 10.1007/s10549-007-9668-7 REVIEW 259 Patients with DCIS of the breast applying USC/Van Nuys prognostic index: a retrospective review with long term follow
Breast Cancer Res Treat (2008) 109:405 416 DOI 10.1007/s10549-007-9668-7 REVIEW 259 Patients with DCIS of the breast applying USC/Van Nuys prognostic index: a retrospective review with long term follow
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer. Pathology. AGO e. V. in der DGGG e.v. sowie in der DKG e.v.
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Pathology Pathology Versions 2004 2017: Blohmer / Costa / Fehm / Friedrichs / Huober / Kreipe / Lück / Schneeweis / Sinn /
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Pathology Pathology Versions 2004 2017: Blohmer / Costa / Fehm / Friedrichs / Huober / Kreipe / Lück / Schneeweis / Sinn /
IBCM 2, April 2009, Sarajevo, Bosnia and Herzegovina
 Preoperative diagnosis and treatment planning in breast cancer The pathologist s perspective L. Mazzucchelli Istituto Cantonale di Patologia Locarno, Switzerland IBCM 2, 23-25 April 2009, Sarajevo, Bosnia
Preoperative diagnosis and treatment planning in breast cancer The pathologist s perspective L. Mazzucchelli Istituto Cantonale di Patologia Locarno, Switzerland IBCM 2, 23-25 April 2009, Sarajevo, Bosnia
Current issues in diagnostic breast pathology
 1 Cancer Studies and Molecular Medicine, University of Leicester, Leicester, UK 2 Academic Unit of Pathology, Leeds University, Leeds, UK 3 Academic Oncology/Breast Pathology, King s College London, London,
1 Cancer Studies and Molecular Medicine, University of Leicester, Leicester, UK 2 Academic Unit of Pathology, Leeds University, Leeds, UK 3 Academic Oncology/Breast Pathology, King s College London, London,
CNB vs Surgical Excision
 Update on Core Needle Biopsy of Non-palpable Breast Lesions Nour Sneige, M.D. UT MD Anderson Cancer Center Houston, Tx Image-Guided CNB of Breast Lesions An alternative to surgical biospy CNB vs Surgical
Update on Core Needle Biopsy of Non-palpable Breast Lesions Nour Sneige, M.D. UT MD Anderson Cancer Center Houston, Tx Image-Guided CNB of Breast Lesions An alternative to surgical biospy CNB vs Surgical