Nutn but a Small Biopsy How to approach small biopsy samples of the sinonasal tract
|
|
|
- Brenda Cross
- 5 years ago
- Views:
Transcription



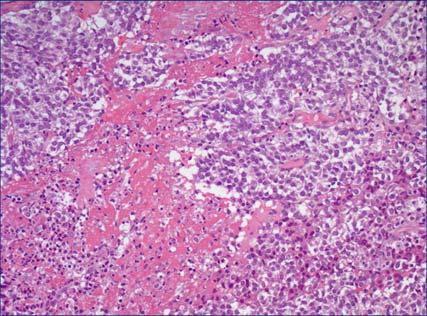
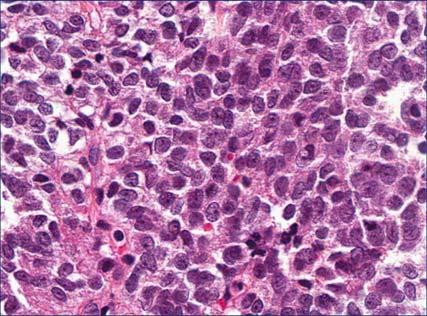
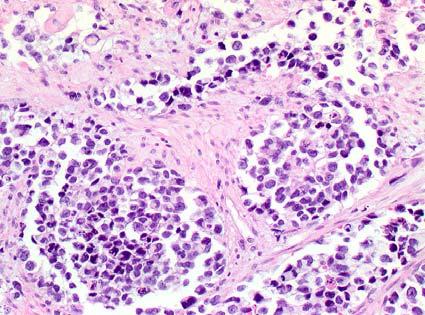
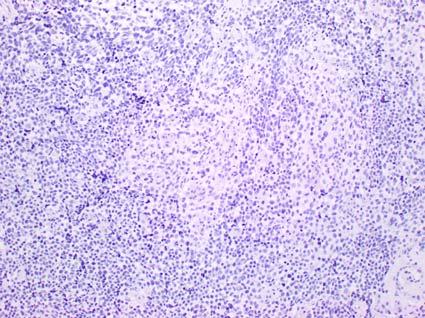
1 California Society of Pathology Saturday Slide Seminar Nutn but a Small Biopsy How to approach small biopsy samples of the sinonasal tract Lester D. R. Thompson Learning Objectives Following the presentation, participants should be able to: 1. Interpret and incorporating radiology findings into determining the best diagnosis for small biopsies. 2. Create a hierarchy of immunohistochemistry evaluation to achieve the best diagnosis with limited material. 3. Learn which entities can be combined versus separated into groups for management purposes. 2 Case 28 year old woman Presented with progressive sinus pain with recent onset of diplopia and headaches Left proptosis and exophthalmos were noted By computed tomography, there is a 1.8 x 1.1 cm left frontoethmoid sinus mass that involved the medial superior bony orbital wall, and extends to involve the soft tissues of the orbit and maxillary sinus During physical exam, there was a palpable mass through the left upper eyelid nasal side At biopsy there was a soft, somewhat necrotic to degenerated appearance to the tissue removed 3 5 6




2 7 8 Best diagnosis based on the H&E findings: 1. Melanoma 2. Mesenchymal chondrosarcoma 3. Rhabdomyosarcoma 4. Sinonasal undifferentiated carcinoma 5. Poorly differentiated squamous cell carcinoma 6. Lymphoma 7. Olfactory neuroblastoma 8. Ewing sarcoma 9. Pituitary adenoma 9 Differential Diagnosis: Mesenchymal Chondrosarcoma Malignant mesenchymal tumor with cartilaginous differentiation Rare, but 2 nd -3 rd decades Cartilage is frequently limited, requiring many sections or levels Biphasic microscopic pattern: Abrupt islands of cellular hyaline cartilage Small, undifferentiated round to spindled cells Cell arranged in a solid pattern with staghornshaped vessels Positive: CD99, Sox9; Negative: S100 protein HEY1-NCOA2 fusion detected by FISH in ~80% 11 12



")

 EWSR1/FLI1")
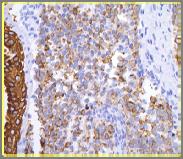
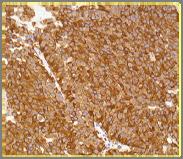
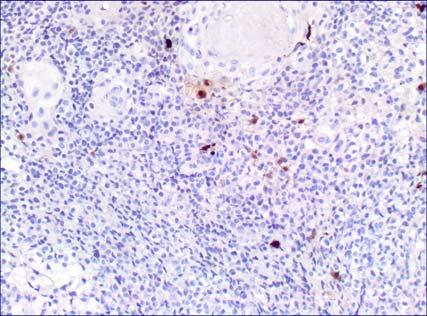
3 13 14 Differential Diagnosis: Ewing/PNET High-grade primitive small round cell sarcoma with (variable) neuroectodermal differentiation defined by presence of translocation (EWSR1) Small round blue cell tumor, sheets, tumor necrosis, finely distributed chromatin, mitoses Positive: CD99, FLI1, Erg, SNF5, p63 (~20%) Variable: NSE, S100 protein, synaptophysin, chromogranin, NFP or GFAP Negative: myogenic; hematolymphoid, keratin (focal up to 30%) EWSR1/FLI1 translocation most often EWS/FLI1 CD



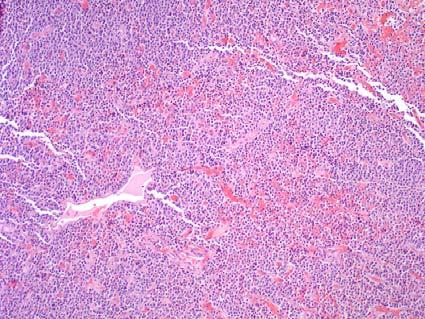
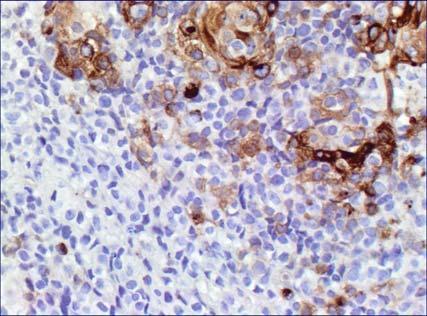
4 Differential Diagnosis: NK/T-cell lymphoma, Sinonasal Type Extranodal, NK/T cell lymphoma, sinonasal type Cytologic atypia, perivascular distribution, geographic necrosis Often shows pseudoepitheliomatous hyperplasia Positive: CD3, CD56, CD138, granzyme, EBER Negative: CD20, CK-pan, desmin, vascular markers CD3ε 23 24





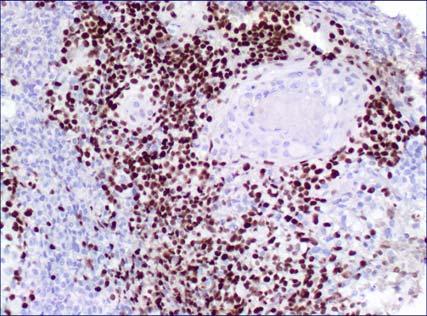
5 CD year old Woman Congestion, difficulty breathing Imaging showed a sphenoid sinus mass Biopsy performed
")



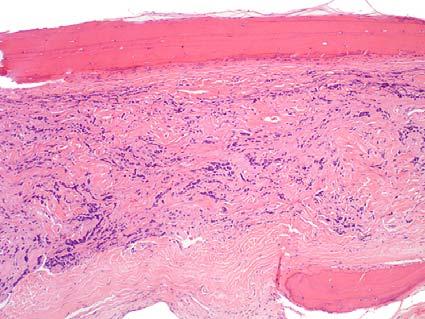
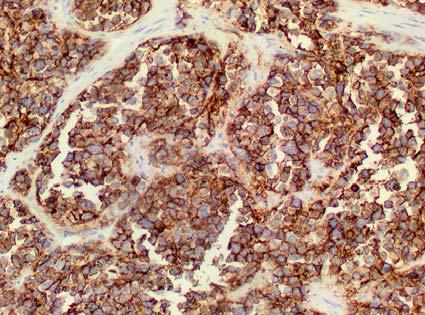
6 Synaptophysin Ectopic Sphenoid Sinus Pituitary Adenoma Clinical Benign pituitary gland neoplasm occurring separately from and without involvement of sella turcica (a normal anterior pituitary gland) Direct extension from intrasellar pituitary tumors in about 2% should be excluded Incidence: Rare in ectopic locations Age: Wide range: years Mean: 54 years Gender Female > Male (1.3:1) Symptoms: Obstruction, sinusitis, pain, discharge, headache, visual disturbances, endocrine syndrome Ectopic Sphenoid Sinus Pituitary Adenoma Imaging Findings Intrasphenoidal mass with expansion and/or erosion Sella may be involved by upward extension, but usually normal Strong enhancement post contrast Define extent and location of tumor Imaging usually suggests chordoma, nasopharyngeal carcinoma, or metastatic tumor 35 36

 Intact surface epithelium Submucosal location,")
; pleomorphism No perineural or")



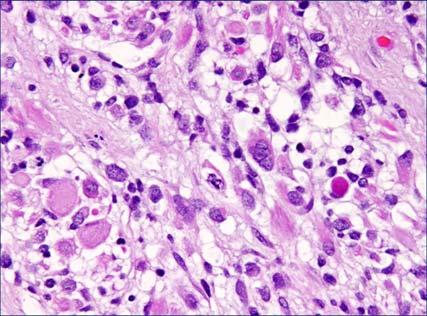
7 Pituitary Adenoma Pathology Findings Polypoid and pedunculated mass within sphenoid sinus, bone erosion Size: Range: 0.5 to 8.0 cm (mean, 2.9 cm) Intact surface epithelium Submucosal location, unencapsulated tumor Invades into subepithelial stroma and bone Necrosis (up to 25%); pleomorphism No perineural or vascular invasion; No atypical mitoses Many patterns Solid, organoid, glandular, insular, festoons, ribbons, single file, rosettes pseudorosettes, papillary, cystic Epithelial cells Polygonal, plasmacytoid, cuboidal, spindled, round or oval nuclei with salt-and-pepper, clumped chromatin, small nucleoli, intranuclear inclusions and variable cytoplasm Profound pleomorphism Polypoid

8 Immunohistochemistry Positive: CK-Pan (AE1/AE3) 79% Synaptophysin: 97% CD56: 91% NSE: 76% Chromogranin-A: 71% CD99: 40% Prolactin 59% FSH 47% LH 37% ACTH 33% TSH 29% GH 26% Neuroendocrine + Epithelial markers + CK-Pan CD56 Chromo 47 48
, corticosteroids (hydrocortisone, prednisone), thyroxine Stereotactic")
 4% died with disease (0.8 years) 14% persistence/recurrence (mean, 2.")


9 Treatment Surgery is treatment of choice Medical/hormonal manipulation Dopamine-agonists (bromocriptine), somatostatin analogs (octreotide), corticosteroids (hydrocortisone, prednisone), thyroxine Stereotactic radioablation For larger or incompletely removed tumors Excellent prognosis 96% have no evidence of disease (mean follow-up: 10.5 years) 4% died with disease (0.8 years) 14% persistence/recurrence (mean, 2.1 years) Managed with surgery or radiation Prolactin year old female Presented with seizure The computed tomography scan and the MRI demonstrate a 4.3 x 3.7 x 2.5 cm mass pushing the left frontal brain lobe, extends through the left ethmoid sinus Calcifications noted Small Round Blue Cell Tumors Small Blue Round Cell: MRS LEEP Melanoma Rhabdomyosarcoma Sinonasal undifferentiated carcinoma (SNUC) Lymphoma Esthesioneuroblastoma (Olfactory neuroblastoma) Ewing sarcoma Pituitary adenoma 53 54




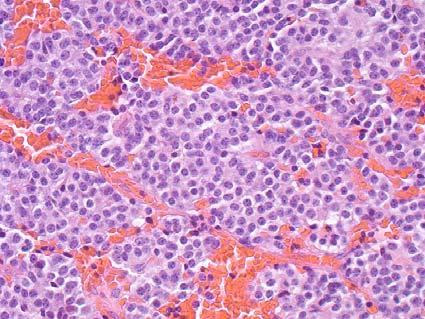
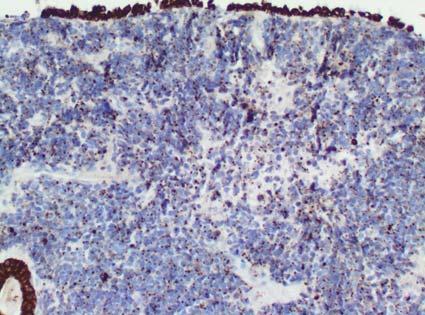
10 Olfactory Neuroblastoma Clinical and Imaging Arises from the specialized sensory neuroepithelial (neuroectodermal) olfactory cells Normally in upper part of the nasal cavity Superior nasal concha, upper part of septum, roof of nose, cribriform plate of ethmoid sinus Age: Bimodal age presentation (young or old) Sex: Equal gender Symptoms: Non-specific; Anosmia <5% Imaging: A dumbbell-shaped mass Extends across the cribriform plate of ethmoid sinus Bone erosion of the lamina papyracea CT may show speckled calcifications MR T1-weighted images after gadolinium show marked enhancement Olfactory Neuroblastoma Microscopic features Circumscribed lobules or nests of tumor in syncytial arrangement with neural processes Intact mucosa (olfactory mucosa in many cases) Tumor cells are small, round, blue cells Slightly larger than mature lymphocytes High nuclear to cytoplasmic ratio Nuclei are small and uniform with hyperchromatic, delicate nuclear chromatin distribution Nucleoli are inconspicuous




 less common")
11 Olfactory Neuroblastoma Microscopic features Two types of rosettes, although only in up to 30% of cases Pseudorosettes (Homer Wright) common The delicate, neurofibrillary and edematous stroma forms in the center of a cuffed or palisaded arrangement True rosettes (Flexner-Wintersteiner) less common Gland-like tight, annular arrangement 65 66




12 Olfactory Neuroblastoma Grading Grade based on the degree of differentiated, presence of neural stroma, mitotic figures, and necrosis Grade I to Grade IV Grade correlates with prognosis Increased grade of the tumor is more difficult to diagnose Olfactory Neuroblastoma Hyams Grading Feature Grade 1 Grade 2 Grade 3 Grade 4 Architec. L L L L Mitoses Anaplasia Matrix /- Rosettes HW HW FW FW Necrosis ±




13 Positive Olfactory Neuroblastoma Immunohistochemistry Synaptophysin, chromogranin, neuron specific enolase, NFP, CD56, calretinin S100 protein or GFAP found at the periphery of the tumor lobules and correspond to Schwann (sustentacular) cells Rarely, focal reactions with keratin (especially LMW cytokeratin Cam 5.2) Olfactory Neuroblastoma Immunohistochemistry Negative Desmin SMA MSA Myogenin HMB45 Melan A CD45RB CD99 75 Synaptophysin 76 Chromogranin CD

 metastasis: 10% Overall 5-year survival: 60 80% (stage & grade dependent) Low grade: High grade: 80% 5-year survival 40% 5-year survival")

14 S100 protein GFAP Positive Olfactory Neuroblastoma Immunohistochemistry to Order Synaptophysin/CD56/Chromogranin S-100 protein Negative CK-pan Myogenin/MYOD1/Desmin Calretinin Olfactory Neuroblastoma Management and Outcome Complete radical surgical eradication Craniofacial resection including cribriform plate by trephination or by endoscopic approach Combined with radiotherapy or chemotherapy Outcome: Recurrence rate 15 30% Lymph node metastasis: 10 20% Distant (lung/bone) metastasis: 10% Overall 5-year survival: 60 80% (stage & grade dependent) Low grade: High grade: 80% 5-year survival 40% 5-year survival Differential Diagnosis: Mucosal Melanoma Dyscohesive epithelioid to spindled tumor cells, junctional proliferation, pigmented, intranuclear cytoplasmic inclusions, eccentric nuclei, mitoses, peritheliomatous growth Positive: S100 protein, HMB-45, Melan-A Negative: Keratin, neuroendocrine markers, pituitary hormones and transcription factors 83 84




 and CD56 5-year")
15 85 86 S100 protein Rhabdomyosarcoma Looks like a polyp Can be embryonal, alveolar, or undifferentiated types Small round cells to ribbon or strap shaped cells to large cells Desmin, myogenin, myoglobin, MYOD1, SMA, MSA reactive Also positive with CK-pan (8%) and CD56 5-year survival dependent upon stage 89 90


16 CD56 CK-pan 95 96






17 Myogenin Immunohistochemistry Evaluation Initial panel for poorly differentiated tumor: CK-pan Desmin CD56 S100 protein CD45RB Actin Desmin year old Man Congestion, difficulty breathing Epistaxis Imaging showed a nasal cavity centered mass Biopsy performed CK: HWM & LMW





18 p63 CD p16 S100 protein, CK5/6, CD45RB, myogenin Sinonasal Undifferentiated Carcinoma High grade carcinoma without squamous or glandular differentiation Older patients Men > Women Rapidly growing clinically Midline destructive with bone destruction, necrosis and lymph-vascular invasion High frequency of metastatic disease Poor outcome




19 Sinonasal Undifferentiated Carcinoma Undifferentiated histologic appearance May have rosettes High mitotic index Positive: CK-pan, EMA, CK7 (~50%), NSE, Ki-67, p16, CD117 Sometimes: Synaptophysin, chromogranin, CD56, p63 Negative: CK5/6, desmin, CD34, HPV, S100 protein, HMB45, EBER Neuroendocrine carcinoma Tends to have more salt-and-pepper nuclear chromatin Slightly different immunohistochemistry Positive: CK-pan/CAM5.2: Dot/punctate; neuroendocrine markers CD56, synaptophysin, chromogranin, NSE Negative: p16, HPV, NUT, CD CK-pan 114
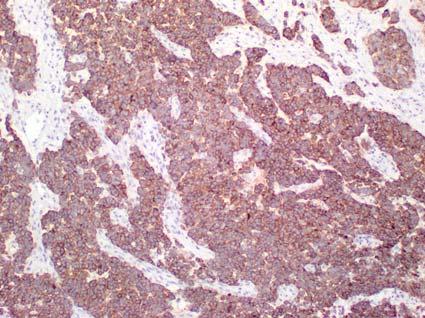

20 Synaptophysin CD CK5/6, S100 protein, Prolactin, Desmin, CD34 S100 protein CK5/6 p




21 CD34 CD45RB, Desmin, MSA, Synaptophysin Best classification after studies: 1. Nasopharyngeal carcinoma 2. Poorly differentiated squamous cell carcinoma, pending IHC 3. Poorly differentiated squamous cell carcinoma 4. Sinonasal undifferentiated carcinoma Additional Considerations There is abrupt squamous differentiation or keratinization Otherwise poorly differentiated Negative sarcoma and neuroendocrine markers Additional evaluation can be done NUT midline carcinoma 125 NUT 126
 gene Most common (70%) rearrangements are BRD4-NUTM1 fusion, although NUT-variant fusions are well recognized ~35% affect the head and neck area Most in sinonasal tract > orbit")

 may yield growth arrest Targeted therapies increase survival to >18 mo 129 130")
 H&E features are often characteristic Let H&E guide ancillary/pertinent studies There will be immunohistochemistry overlap Targeted molecular studies as needed Take Home Points Always")
22 NUT Midline Carcinoma NUT midline carcinoma (NMC) is an aggressive subset of squamous cell carcinoma, genetically defined by rearrangement of the NUTM1 gene Nuclear protein in testis (NUT, aka NUTM1) gene Most common (70%) rearrangements are BRD4-NUTM1 fusion, although NUT-variant fusions are well recognized ~35% affect the head and neck area Most in sinonasal tract > orbit Majority in mediastinum Generally younger patients Usually midline but can be anywhere Squamous cell carcinoma NUT midline carcinoma NUT1 Midline Carcinoma Prognosis is usually poor (median 6.7 months) Diagnosis is only confirmed by nuclear immunoreactivity to NUT protein Specific fusion oncogenes for clinical trials Conventional chemotherapeutic regimens are ineffective Molecular targeted therapies (bromodomain inhibitors [BETi] and histone deacetylase inhibitors [HDACi]) may yield growth arrest Targeted therapies increase survival to >18 mo Conclusion Think very broadly when confronted with Sinonasal Tract Small Round Blue Cell tumors (MR. SLEEP) H&E features are often characteristic Let H&E guide ancillary/pertinent studies There will be immunohistochemistry overlap Targeted molecular studies as needed Take Home Points Always use radiology and/or clinical findings Consider what will be done with + or findings when ordering special studies Preferentially and sequentially order studies Wide differential diagnoses are common, but they can be narrowed significantly with clinical, imaging and laboratory findings
Small (and large) Blue Cell Tumors of the Skull Base
 Blue Cell Tumors of the Skull Base") Small (and large) Blue Cell Tumors of the Skull Base Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Small (and large) Blue Cell Tumors of the Skull Base Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Case 2. Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset
 Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Nasal Cavity and Paranasal Sinuses
 Chapter 2 Nasal Cavity and Paranasal Sinuses Introduction Included in this chapter are nasal cavities, frontal sinus, ethmoid complex, sphenoid sinus, and maxillary sinuses. These cavities and sinuses
Chapter 2 Nasal Cavity and Paranasal Sinuses Introduction Included in this chapter are nasal cavities, frontal sinus, ethmoid complex, sphenoid sinus, and maxillary sinuses. These cavities and sinuses
Disclosures. The Thin Red Line Between Neuropathology and Head & Neck Pathology. Introduction CASE 1. Current Issues Tihan
 Disclosures I have nothing to disclose The Thin Red Line Between Neuropathology and Head & Neck Pathology Tarik Tihan, MD, PhD UCSF, Department of Pathology Neuropathology Division Introduction Three cases
Disclosures I have nothing to disclose The Thin Red Line Between Neuropathology and Head & Neck Pathology Tarik Tihan, MD, PhD UCSF, Department of Pathology Neuropathology Division Introduction Three cases
Financial disclosures
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
1/10/2018. Soft Tissue Tumors Showing Melanocytic Differentiation. Overview. Desmoplastic/ Spindle Cell Melanoma
 2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Special slide seminar
 Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Case Presentation. Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD. Department of Pathology Jordan University Hospital Amman, Jordan
 Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
J of Evolution of Med and Dent Sci/ eissn , pissn / Vol. 3/ Issue 30/July 28, 2014 Page 8403
 BENIGN TUMOR OF NOSE AND PARANASAL SINUS IN A CHILD: A CASE REPORT Mujtaba Khan 1, S. Muneeruddin Ahmed 2, A. Sesha Prasad 3, M. Mahendra Kumar 4, G. Shahul Hameed 5 HOW TO CITE THIS ARTICLE: Mujtaba Khan,
BENIGN TUMOR OF NOSE AND PARANASAL SINUS IN A CHILD: A CASE REPORT Mujtaba Khan 1, S. Muneeruddin Ahmed 2, A. Sesha Prasad 3, M. Mahendra Kumar 4, G. Shahul Hameed 5 HOW TO CITE THIS ARTICLE: Mujtaba Khan,
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Pitfalls in Sinonasal Pathology
 Pitfalls in Sinonasal Pathology Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences jhunt2@uams.edu
Pitfalls in Sinonasal Pathology Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences jhunt2@uams.edu
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Case Studies in the Skull Base
 Case Studies in the Skull Base Amy C Tsai, MD Neuroradiology Fellow Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA No disclosures related
Case Studies in the Skull Base Amy C Tsai, MD Neuroradiology Fellow Department of Radiology and Imaging Sciences University of Utah Health Sciences Center Salt Lake City, Utah, USA No disclosures related
04/13/2017. Sinonasal Pathology. Sinonasal Tract Pathology Outline. 24 th Annual Seminar in Pathology Pittsburgh, PA April 27, 2017
 Sinonasal Pathology 24 th Annual Seminar in Pathology Pittsburgh, PA April 27, 2017 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL Sinonasal Tract Pathology Outline Sinonasal (Schneiderian) papillomas
Sinonasal Pathology 24 th Annual Seminar in Pathology Pittsburgh, PA April 27, 2017 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL Sinonasal Tract Pathology Outline Sinonasal (Schneiderian) papillomas
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Neuroendocrine Carcinoma. Lebanon Neuroendocrine Neoplasms of H&N Nov /7/2011. Broad Classification:
 H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Founders Seminar. Handout material. Challenging Cases in Head and Neck Surgical Pathology
 Founders Seminar Handout material Challenging Cases in Head and Neck Surgical Pathology Robert A. Robinson Department of Pathology University of Iowa American Academy of Oral and Maxillofacial Pathology
Founders Seminar Handout material Challenging Cases in Head and Neck Surgical Pathology Robert A. Robinson Department of Pathology University of Iowa American Academy of Oral and Maxillofacial Pathology
Immunohistochemistry in Bone and Soft Tissue Tumors. Sahar Rassi Zankoul, MD
 Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Sinonasal Tumors. Objectives. Objectives. Incidence of Paranasal Sinus Tumors. Demographics of Paranasal Sinus Tumors. Paranasal Sinus Tumors
 Sinonasal Tumors Objectives Incidence and demographics of sinonasal tumors Separating tumors from inflammatory changes Common and notable histologic types of sinonasal tumors Staging of sinonasal tumors
Sinonasal Tumors Objectives Incidence and demographics of sinonasal tumors Separating tumors from inflammatory changes Common and notable histologic types of sinonasal tumors Staging of sinonasal tumors
3/27/2017. Pulmonary Pathology Specialty Conference. Disclosure of Relevant Financial Relationships. Clinical History:
 Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Financial disclosures
 Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP
 What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
Difficult Diagnoses and Controversial Entities in Neoplastic Lung
 Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia
 Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia Sílvia Bagué Servei de Patologia Hospital de Sant Pau Barcelona Soft tissue sarcomas Heterogeneous group
Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia Sílvia Bagué Servei de Patologia Hospital de Sant Pau Barcelona Soft tissue sarcomas Heterogeneous group
Case Report SMARCB1 (INI1)-deficient sinonasal carcinoma: a newly described entity
-deficient sinonasal carcinoma: a newly described entity") Int J Clin Exp Pathol 2016;9(3):3454-3458 www.ijcep.com /ISSN:1936-2625/IJCEP0024095 Case Report SMARCB1 (INI1)-deficient sinonasal carcinoma: a newly described entity Ming Zeng 1*, Changrong Chen 2*,
Int J Clin Exp Pathol 2016;9(3):3454-3458 www.ijcep.com /ISSN:1936-2625/IJCEP0024095 Case Report SMARCB1 (INI1)-deficient sinonasal carcinoma: a newly described entity Ming Zeng 1*, Changrong Chen 2*,
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology
 IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
Differential Diagnosis of Oral Masses. Palatal Lesions
 Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
SMALL CELL NEUROENDOCRINE CARCINOMA OF ETHMOID SINUS: CASE REPORT AND LITERATURE REVIEW
 Therapeut Radiol Oncol 2003; 10(3): 175-179 175 SMALL CELL NEUROENDOCRINE CARCINOMA OF ETHMOID SINUS: CASE REPORT AND LITERATURE REVIEW Forn-Chia Lin 1, Li-Ching Lin 1, Chang-Chuan Su 2, Kuei-Li Lin 1,
Therapeut Radiol Oncol 2003; 10(3): 175-179 175 SMALL CELL NEUROENDOCRINE CARCINOMA OF ETHMOID SINUS: CASE REPORT AND LITERATURE REVIEW Forn-Chia Lin 1, Li-Ching Lin 1, Chang-Chuan Su 2, Kuei-Li Lin 1,
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Mojca Velikonja Jože Pižem
 Mojca Velikonja Jože Pižem An 81-year old woman presented with an exophytic, wart-like skin lesion on her neck that she had observed for one year. Cryotherapy had been applied twice, but proved unsuccessful.
Mojca Velikonja Jože Pižem An 81-year old woman presented with an exophytic, wart-like skin lesion on her neck that she had observed for one year. Cryotherapy had been applied twice, but proved unsuccessful.
59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain
 December 2016 59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain Contributed by: Divya Sharma, MD. Fellow, Gastrointestinal Pathology, Department of Pathology
December 2016 59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain Contributed by: Divya Sharma, MD. Fellow, Gastrointestinal Pathology, Department of Pathology
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Scotland and Northern Ireland EQA Scheme. Circulation 46
 Scotland and Northern Ireland EQA Scheme Circulation 46 Special Educational Cases E1 and E2 Presented by Dr K Robertson Case E1 Female 42 year old with heavy menstrual and intermenstrual bleeding. IUS
Scotland and Northern Ireland EQA Scheme Circulation 46 Special Educational Cases E1 and E2 Presented by Dr K Robertson Case E1 Female 42 year old with heavy menstrual and intermenstrual bleeding. IUS
Pathology Mystery and Surprise
 Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Financial disclosures
 An update on immunohistochemical markers in mesenchymal neoplasms By Konstantinos Linos MD, FCAP, FASDP Assistant Professor of Pathology Geisel School of Medicine at Dartmouth Dartmouth-Hitchcock Medical
An update on immunohistochemical markers in mesenchymal neoplasms By Konstantinos Linos MD, FCAP, FASDP Assistant Professor of Pathology Geisel School of Medicine at Dartmouth Dartmouth-Hitchcock Medical
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Sinonasal carcinomas ARTICLE IN PRESS. Lester D.R. Thompson MINI-SYMPOSIUM: HEAD AND NECK PATHOLOGY. Introduction
 Current Diagnostic Pathology (2006) 12, 40 53 www.elsevier.com/locate/cdip MINI-SYMPOSIUM: HEAD AND NECK PATHOLOGY Sinonasal carcinomas Lester D.R. Thompson Southern California Permanente Medical Group,
Current Diagnostic Pathology (2006) 12, 40 53 www.elsevier.com/locate/cdip MINI-SYMPOSIUM: HEAD AND NECK PATHOLOGY Sinonasal carcinomas Lester D.R. Thompson Southern California Permanente Medical Group,
Basaloid neoplasms of the head and neck. Basaloid SCC. Clinico-pathologic features 5/5/11. Basaloid Tumors Head and Neck
 Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
Rare Presentation Of Adenoidcystic Carcinoma Of External Auditory Canal With Subcutaneous Metastasis In Temporal Region
 ISPUB.COM The Internet Journal of Otorhinolaryngology Volume 13 Number 2 Rare Presentation Of Adenoidcystic Carcinoma Of External Auditory Canal With Subcutaneous Metastasis In Temporal Region S Kaushik,
ISPUB.COM The Internet Journal of Otorhinolaryngology Volume 13 Number 2 Rare Presentation Of Adenoidcystic Carcinoma Of External Auditory Canal With Subcutaneous Metastasis In Temporal Region S Kaushik,
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
The Differential Diagnosis of Sinonasal/Nasopharyngeal Neuroendocrine/Neuroectodermally Derived Tumors
 The Differential Diagnosis of Sinonasal/Nasopharyngeal Neuroendocrine/Neuroectodermally Derived Tumors Kathleen T. Montone, MD Context. The differential diagnosis of neuroendocrine neoplasms arising in
The Differential Diagnosis of Sinonasal/Nasopharyngeal Neuroendocrine/Neuroectodermally Derived Tumors Kathleen T. Montone, MD Context. The differential diagnosis of neuroendocrine neoplasms arising in
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology
 David M. Parham, MD Chief of Anatomic Pathology") Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology Tumors of skeletal muscle: Rhabdomyomas and rhabdomyosarcomas Embryonal muscle 2 3 4 5 6 7 8 Rhabdomyoma Benign
Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology Tumors of skeletal muscle: Rhabdomyomas and rhabdomyosarcomas Embryonal muscle 2 3 4 5 6 7 8 Rhabdomyoma Benign
Case Report Endocrine Mucin-Producing Sweat Gland Carcinoma, a Histological Challenge
 Hindawi Volume 2017, Article ID 6343709, 4 pages https://doi.org/10.1155/2017/6343709 Case Report Endocrine Mucin-Producing Sweat Gland Carcinoma, a Histological Challenge Mary Anne Brett, Samih Salama,
Hindawi Volume 2017, Article ID 6343709, 4 pages https://doi.org/10.1155/2017/6343709 Case Report Endocrine Mucin-Producing Sweat Gland Carcinoma, a Histological Challenge Mary Anne Brett, Samih Salama,
Metaplastic carcinoma of the breast with neuroglial differentiation
 The Breast (]]]]) ], ]]] ]]] THE BREAST www.elsevier.com/locate/breast CASE REPORT Metaplastic carcinoma of the breast with neuroglial differentiation Mehra Golshan a,, Adam Kuten b, Jacquleine William
The Breast (]]]]) ], ]]] ]]] THE BREAST www.elsevier.com/locate/breast CASE REPORT Metaplastic carcinoma of the breast with neuroglial differentiation Mehra Golshan a,, Adam Kuten b, Jacquleine William
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
FINALIZED SEER SINQ QUESTIONS
 0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
The Small Round Blue Cell Tumors of the Sinonasal Area
 Head and Neck Pathol (2010) 4:84 93 DOI 10.1007/s12105-009-0158-6 PROCEEDINGS OF THE 2010 NORTH AMERICAN SOCIETY OF HEAD AND NECK PATHOLOGY COMPANION MEETING (WASHINGTON, DC) The Small Round Blue Cell
Head and Neck Pathol (2010) 4:84 93 DOI 10.1007/s12105-009-0158-6 PROCEEDINGS OF THE 2010 NORTH AMERICAN SOCIETY OF HEAD AND NECK PATHOLOGY COMPANION MEETING (WASHINGTON, DC) The Small Round Blue Cell
DIAGNOSTIC DILEMMA. Case Reports Clinical history. Materials and Methods
 DIAGNOSTIC DILEMMA A Metastatic Renal Carcinoid Tumor Presenting as Breast Mass: A Diagnostic Dilemma Farnaz Hasteh, M.D., 1 Robert Pu, M.D., Ph.D., 2 and Claire W. Michael, M.D. 2 * We present clinicopathological
DIAGNOSTIC DILEMMA A Metastatic Renal Carcinoid Tumor Presenting as Breast Mass: A Diagnostic Dilemma Farnaz Hasteh, M.D., 1 Robert Pu, M.D., Ph.D., 2 and Claire W. Michael, M.D. 2 * We present clinicopathological
NASAL SEPTUM ADENOID CYSTIC CARCINOMA: A CASE REPORT
 NASAL SEPTUM ADENOID CYSTIC CARCINOMA: A CASE REPORT Shu-Yu Tai, 1 Chen-Yu Chien, 2 Chih-Feng Tai, 2,4 Wen-Rei Kuo, 2,4 Wan-Ting Huang, 3 and Ling-Feng Wang 2,4 Departments of 1 Family Medicine, 2 Otolaryngology
NASAL SEPTUM ADENOID CYSTIC CARCINOMA: A CASE REPORT Shu-Yu Tai, 1 Chen-Yu Chien, 2 Chih-Feng Tai, 2,4 Wen-Rei Kuo, 2,4 Wan-Ting Huang, 3 and Ling-Feng Wang 2,4 Departments of 1 Family Medicine, 2 Otolaryngology
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
CNS TUMORS. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
Disclosure of Relevant Financial Relationships
 Ewing and Ewing like sarcomas Using Genetic Signatures in Refining Small Blue Round Cell Tumor Classification Cristina Antonescu, MD Department of Pathology Disclosure of Relevant Financial Relationships
Ewing and Ewing like sarcomas Using Genetic Signatures in Refining Small Blue Round Cell Tumor Classification Cristina Antonescu, MD Department of Pathology Disclosure of Relevant Financial Relationships
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
number Done by Corrected by Doctor Maha Shomaf
 number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
University Journal of Pre and Para Clinical Sciences
 ISSN 2455 2879 Volume 2 Issue 1 2016 Metaplastic carcinoma breast a rare case report Abstract : Metaplastic carcinoma of the breast is a rare malignancy with two distinct cell lines described as a breast
ISSN 2455 2879 Volume 2 Issue 1 2016 Metaplastic carcinoma breast a rare case report Abstract : Metaplastic carcinoma of the breast is a rare malignancy with two distinct cell lines described as a breast
Salivary Gland FNA ATYPICAL : Criteria and Controversies
 Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
DISCUSSION: PLGA accounts for about 2% of all salivary gland tumours and occurs almost exclusively in the minor salivary glands.
 SWELLING ON THE HARD PALATE PRESENTING AS POLYMORPHOUS LOW GRADE ADENOCARCINOMA: A AND REVIEW OF LITERATURE Swapnil D. Chandekar 1, Sunita S. Dantkale 2, Rahul R. Narkhede 3, Snehal V. Chavhan 4, Khushboo
SWELLING ON THE HARD PALATE PRESENTING AS POLYMORPHOUS LOW GRADE ADENOCARCINOMA: A AND REVIEW OF LITERATURE Swapnil D. Chandekar 1, Sunita S. Dantkale 2, Rahul R. Narkhede 3, Snehal V. Chavhan 4, Khushboo
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Nasal Cavity and Paranasal Sinuses
 2017 Head and Neck Tumors Selected Topics Lester D. R. Thompson 1 2 Inclusion Criteria Nasal Cavity and Paranasal Sinuses 2005 edition: 76 diagnoses 2017 edition: 39 diagnoses 3 1. The tumor occurs exclusively
2017 Head and Neck Tumors Selected Topics Lester D. R. Thompson 1 2 Inclusion Criteria Nasal Cavity and Paranasal Sinuses 2005 edition: 76 diagnoses 2017 edition: 39 diagnoses 3 1. The tumor occurs exclusively
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
MALIGNANT TUMOURS OF THE JAWS
 MALIGNANT TUMOURS OF THE JAWS MALIGNANT TUMOURS OF THE JAWS Squamous cell carcinoma Osteogenic sarcoma Chondrosarcoma Fibrosarcoma Malignant lymphomas (incl. Burkitt s) Multiple myeloma Ameloblastoma Secondary
MALIGNANT TUMOURS OF THE JAWS MALIGNANT TUMOURS OF THE JAWS Squamous cell carcinoma Osteogenic sarcoma Chondrosarcoma Fibrosarcoma Malignant lymphomas (incl. Burkitt s) Multiple myeloma Ameloblastoma Secondary
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Diagnostically Challenging Cases in Gynecologic Pathology
 Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Rhabdomyosarcoma. Yueh-Lan Huang, Chin-Feng Tseng, Li-King Yang, and Chen-Hua Tsai
 2005 16 146-150 Rhabdomyosarcoma of the Adult Nasopharynx A Case Report Yueh-Lan Huang, Chin-Feng Tseng, Li-King Yang, and Chen-Hua Tsai Division of Oncology, Department of Internal Medicine, Cardinal
2005 16 146-150 Rhabdomyosarcoma of the Adult Nasopharynx A Case Report Yueh-Lan Huang, Chin-Feng Tseng, Li-King Yang, and Chen-Hua Tsai Division of Oncology, Department of Internal Medicine, Cardinal
Part 1. Slides 1-38, Rita Alaggio Soft tissue tumors Trondheim 14. mars 2013
 Part 1 Slides 1-38, Rita Alaggio Soft tissue tumors Trondheim 14. mars 2013 Pediatric Pathology Soft Tissue Tumors AN UPDATE Rita Alaggio Azienda Ospedaliera Università di Padova Soft Tissue Tumors More
Part 1 Slides 1-38, Rita Alaggio Soft tissue tumors Trondheim 14. mars 2013 Pediatric Pathology Soft Tissue Tumors AN UPDATE Rita Alaggio Azienda Ospedaliera Università di Padova Soft Tissue Tumors More
Ocular Neoplasia What s Common? What s New? Richard R Dubielzig
 Ocular Neoplasia What s Common? What s New? Richard R Dubielzig Orbit 288 6% Tumors of the globe make up 3225 out of 6110 total neoplasms = 53%. Tumors of the conjunctiva make up 1192 out of 6110 total
Ocular Neoplasia What s Common? What s New? Richard R Dubielzig Orbit 288 6% Tumors of the globe make up 3225 out of 6110 total neoplasms = 53%. Tumors of the conjunctiva make up 1192 out of 6110 total
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
A 25 year old female with a palpable mass in the right lower quadrant of her abdomen
 May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
General: Brain tumors are lesions that have mass effect distorting the normal tissue and often result in increased intracranial pressure.
 1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
1 Lecture Objectives Know the histologic features of the most common tumors of the CNS. Know the differences in behavior of the different tumor types. Be aware of the treatment modalities in the various
My Journey into the World of Salivary Gland Sebaceous Neoplasms
 My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
Case Report Paranasal Sinus Neuroendocrine Carcinoma: A Case Report and Review of the Literature
 Hindawi Publishing Corporation Case Reports in Oncological Medicine Volume 2013, Article ID 728479, 5 pages http://dx.doi.org/10.1155/2013/728479 Case Report Paranasal Sinus Neuroendocrine Carcinoma: A
Hindawi Publishing Corporation Case Reports in Oncological Medicine Volume 2013, Article ID 728479, 5 pages http://dx.doi.org/10.1155/2013/728479 Case Report Paranasal Sinus Neuroendocrine Carcinoma: A
Disclosure. Case. Mixed Tumors of the Uterine Corpus and Cervix. I have nothing to disclose
 Mixed Tumors of the Uterine Corpus and Cervix Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Department of Pathology Brigham and Women s Hospital Boston, MA UCSF Current Issues in Anatomic
Mixed Tumors of the Uterine Corpus and Cervix Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Department of Pathology Brigham and Women s Hospital Boston, MA UCSF Current Issues in Anatomic
-The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
- In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Disclosures. An update on ancillary techniques in the diagnosis of soft tissue tumors. Ancillary techniques. Introduction
 Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources
 Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
ONCOLOGY. Csaba Bödör. Department of Pathology and Experimental Cancer Research november 19., ÁOK, III.
 ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
EQA Circulation 43 Educational Cases
 EQA Circulation 43 Educational Cases E1-E2 Monica Agarwal Monklands Hospital E1 38 yrs male Submandibular gland tumour E1 Formal excision following diagnosis of poorly differentiated carcinoma on core
EQA Circulation 43 Educational Cases E1-E2 Monica Agarwal Monklands Hospital E1 38 yrs male Submandibular gland tumour E1 Formal excision following diagnosis of poorly differentiated carcinoma on core
(CYLINDROMA) ATLAS OF HEAD AND NECK PATHOLOGY ADENOID CYSTIC CARCINOMA
 ATLAS OF HEAD AND NECK PATHOLOGY ADENOID CYSTIC CARCINOMA") (CYLINDROMA) This malignant tumor is poorly encapsulated and while seemingly well defined within the affected gland, there is usually infiltration of surrounding tissue on closer examination. The cut surface
(CYLINDROMA) This malignant tumor is poorly encapsulated and while seemingly well defined within the affected gland, there is usually infiltration of surrounding tissue on closer examination. The cut surface
Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case
 Kobe J. Med. Sci., Vol. 49, No. 2, pp. 45-49, 2003 Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case MASAHIRO UMEDA 1), SATOSHI YOKOO 1), YASUYUKI SHIBUYA 1), TAKAHIDE KOMORI
Kobe J. Med. Sci., Vol. 49, No. 2, pp. 45-49, 2003 Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case MASAHIRO UMEDA 1), SATOSHI YOKOO 1), YASUYUKI SHIBUYA 1), TAKAHIDE KOMORI
3/24/2017 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS. Disclosure of Relevant Financial Relationships
 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
I have nothing to disclose
 A 47 year old female with multiple lung nodules Disclosure of Relevant Financial Relationships Tamar Giorgadze, MD, PhD Professor of Pathology Medical College of Wisconsin Milwaukee, Wisconsin USCAP requires
A 47 year old female with multiple lung nodules Disclosure of Relevant Financial Relationships Tamar Giorgadze, MD, PhD Professor of Pathology Medical College of Wisconsin Milwaukee, Wisconsin USCAP requires
Epithelial tumors. Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev
 Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate