CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER
|
|
|
- Jonathan Spencer
- 5 years ago
- Views:
Transcription


1 CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011

2 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter
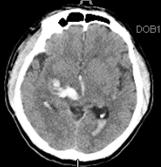
3 Imaging Studies for Etiology of Intracerebral Intraventricular Hemorrhage
4 Vascular Lesions and Etiology of ICH/IVH High prevalence in younger patients (up to 50% of cases < 50 years of age) May cause ICH/IVH at any age Distribution of blood and other features on diagnostic CT may suggest, but not totally establish/exclude May include cerebrovascular malformations, aneurysms, arterial dissection, venous occlusive disease, and other vasculopathies
5 Types of Lesions Delineated on CTA Aneurysms (>2-3mm) Cerebrovascular malformations (arterial, venous, maybe cavernous) Occlusive arterial lesions (Moyamoya, sickle cell arteriopathy) Dilated veins (fistulae)

6 Types of Lesions Delineated on MR (MRI, MRA, Gadolinium, special sequences)* Many of the same as the CTA Lesser sensitivity than CTA for AVMs and aneurysms Greater sensitivity than CTA for cavernous malformations Tumors Evidence of brain ischemia Hemorrhagic angiopathies * May be performed without Gadolinium if renal failure or allergies
7 Types of lesions found on Catheter Angiogram Aneurysms and AVMs too small to be seen on CTA/MRA (or to confirm CTA/MRA)
8 CLEAR Protocol CLEAR III is not designed to test safety/effectiveness of thrombolysis in the setting of known cerebrovascular lesion as the source of hemorrhage Excluding underlying cerebrovascular etiology is a requirement of the CLEAR protocol Investigators are given leeway (options) in choosing appropriate studies for individual case, but looking for and excluding an etiology are REQUIRED.
9 Take Home Message CTA is advised in EVERY case except: Renal failure Severe allergy MRI/MRA is advised if CTA not done, tumor, ischemia or cavernous angiomas are suspected, or if particular question remains after CTA Catheter angiogram is advised if there is a question on CTA or MRI/MRA (consider catheter angiogram in every young patient <40-50 years of age)
10 EXAMPLES (REAL CASES FROM FIRST 120 CASES IN CLEAR III) 177 cases were excluded because of vascular etiology among 3197 cases screened
11 Screen Failures by Category Group Category N % (by group) Vascular* % Tumor % Radiographically Identifiable Exclusions (n = 234) Midbrain / Infratentorial 13 6 % Severe SAH 9 4 % Hemorrhagic Conversion 9 4 % Non-radiographically Identifiable Exclusions (n = 2963) (other) Ɨ % *Vascular includes aneurysm, AVM, Moyamoya, Dural AV fistula, and other vascular lesions Ɨ (other) age, traumatic injury, pregnancy status, historical mrs score, etc. (current data as of 7/17/2011)

12 Radiologic Screen Failures by Category


13 Arteriovenous Malformation 1 51 year old female with suspicious CTA with asymmetric vessels and no clear nidus, so angiogram done revealing an AVM Right lenticulostriate AVM with early draining vein and intra-nidal aneurysm Excluded from CLEAR


14 Arteriovenous Malformation 2 26 year old, underwent MRI/MRA that did not reveal a definite lesion Catheter angiogram done in view of high likelihood of etiology in young patient Angiogram confirmed small thalamic AVM and treated with embolization. Excluded from CLEAR.

, had an")
15 Arteriovenous Malformation 3 61 year old hypertensive female with no definite parenchymal bleed source (primary IVH), had an abnormal CTA

16 Arteriovenous Malformation 3 Angiogram done confirming an AVM, with feeding artery aneurysm, emergently embolized Excluded from CLEAR; AGE IS NOT A GUARANTEE AGAINST VASCULAR ETIOLOGY


17 Moyamoya 39 year old with IVH, caudate bleed and hx of cocaine use enrolled without a CTA or other etiologic screen* CTA done after enrollment, and dosing, demonstrated basal arterial occlusions and Moyamoya collaterals Catheter angiogram confirmed diffuse Moyamoya and associated aneurysms. Dosing was stopped in patient and being followed up closely * A protocol deviation


18 ACom Aneurysm 34 year old patient with ICH and IVH, some basal subarachnoid extension Confirmed ACom aneurysm by angiogram and treated with coiling


19 Mycotic Aneurysm 50 year old with subtle abnormal contrast enhancement on CTA Mycotic aneurysm confirmed on angiogram and treated with coiling
20 Etiology of ICH/IVH You will not see if you don t look Help us not miss ANY case where thrombolysis might be unsafe You won t be blamed for screening, but you might regret short cuts


21 Midbrain Extension and Eligibility Nuances of exclusion criterion
22 Midbrain extension clarification A minor tail into the rostral midbrain is not an exclusion Thalamic bleeds with apparent midbrain extension that do not have overt midbrin signs (dilated nonreactive pupils, extensor posturing, downward gaze) are eligible for participation in the study. Patients with transient occulomotor dysfunction are eligible for participation. Note: Patients with a posterior fossa ICH or cerebellar hematomas are ineligible. This has been clarified in v3 of the protocol


23 Indications for first and second EVD placements
24 First EVD catheter placement indications Acute obstructive hydrocephalus following IVH causing high ICP Even though ICP can be managed medically with sedation and osmotic diuretics, such management is often insufficient to reduce ICP and those settings call for EVD placement Therefore, first catheter placements are often put into the less involved (contralateral) ventricle
25 Second catheter placement indications Clot producing trapped ventricles Clinically important shifts Pan-ventricular enlargement with effacement/ischemia Typically occurs with larger IVH > 40 ml
26 Catheter management
27 Management clarifications During screening If catheter clogs and the patient is in screening for the study, the patient cannot receive t-pa Saline flush is acceptable Use of t-pa during screening excludes patient from participation During dosing If catheter clogs and needs replacement: Try to wait 24 hours prior to removal, unless medically necessary Send post-replacement CT images for SC review
28 Subject excluded from CLEAR: t-pa given during screening the residents gave rt-pa and thought that was all that was needed to enroll a subject into CLEAR III yea we gave rt-pa to flush the catheter, where does that state that s exclusionary in the protocol? so the neurosurgical team gave rt-pa because they didn t want to place a second catheter and randomize the patient
29 Take home points for catheter management The use of rt-pa flushes in an EVD are not part of standard of care, and are not an FDA approved indication of rt-pa Intraventricular rt-pa is being tested in this trial, it is the experimental test article, and cannot be used off-protocol in an enrolled or eligible subject
30 Bleeding expansion/stabilization
31 IVH stability/expansion Width of the lateral ventricle most compromised by blood clot must not increase by > 2 mm (allowing for movement of blood under influence of gravity) If the clot is not stable (i.e., difference is > 2 mm), a repeat CT scan must be performed at least 12 hours after the scan revealing IVH expansion, and compared to demonstrate further stability/expansion
32 ICH stability/expansion ICH must be 30 ml on initial presentation Difference must be 5 cc on CT scan repeated for required 6h stability as determined by the (AxBxC)/2 method (total ICH volume must not exceed 35 ml on pre-randomization stability scans) If the clot is not stable (i.e., difference is > 5 ml), a repeat CT scan must be performed at least 12 hours later and compared to the CT scan revealing bleed expansion If the size stabilizes (i.e., enlargement 5 ml) and remains 35 ml, the patient is eligible
33 Catheter tract stability/expansion Catheter tract bleeding must be < 5 ml on CT scan for stability (including any bleeding at the entry site or along the catheter tract that is 5 mm in diameter seen on any CT slice, is seen on > 2 slices, or is > 5 ml) If a catheter tract hemorrhage is present on the CT scan done after EVD placement and is > 5 ml or > 5 mm, obtain a repeat CT scan 12 hours later. If the size stabilizes (i.e., enlargement < 5 ml or < 5 mm between 2 sequential CT scans), the patient is eligible.
34 Take home message- stability/expansion Importance of careful scrutinizing of ALL diagnostic and stability scans during screening period and filling out CT scan forms in real time
35 Research versus best clinical practice A review of the protocol
36 Best clinical practice Placement of initial EVD for obstructive IVH* Placement of second EVD in cases of casting/trapping/mass effect-shift Daily CT scans to assess clot for first few days after IVH (during test article administration) * Ziai et al., 2009
37 May be considered research-related Placement of second EVD, when first EVD functions for ICP control, but is otherwise suboptimal for administration of test article (catheter perforations not in ventricle) Required stabilization periods* 6 Hours: Between EVD placement(s) and stability CTs Replacement of catheter Second catheter placed 12 hours: Catheter tract hemorrhage > 5ml (wait 12 hours until next dose is given) 24 Hours: > 2 passes for catheter placement If dosing has begun, any catheter manipulation (removal, 2 nd catheter placement) * May be justified clinically
38 May be considered research-related What if patient looks good clinically despite obstructive IVH Widely varying practice patterns up front EVD versus EVD if/when patient worsens REMEMBER--- Obstructive IVH is correlated with worse ICH outcome, at all GCS strata; enhanced IVH clearance is the primary intervention being tested in CLEAR III to improve outcome If patient meets inclusion criteria otherwise, frank discussion with family about clinical equipoise Up front EVD is the only opportunity to benefit from potentially enhanced IVH clearance.
39 Questions?
Welcome to our MISTIE III Safety Forum September 12, 2016
 Welcome to our MISTIE III Safety Forum September 12, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Mario Zuccarello, MD, University of Cincinnati Revisiting the Importance of
Welcome to our MISTIE III Safety Forum September 12, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Mario Zuccarello, MD, University of Cincinnati Revisiting the Importance of
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Intracranial spontaneous hemorrhage mechanisms, imaging and management
 Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Intracranial spontaneous hemorrhage mechanisms, imaging and management Dora Zlatareva Department of Diagnostic Imaging Medical University, Sofia, Bulgaria Intracranial hemorrhage (ICH) ICH 15% of strokes
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD.
 Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Interventions in the Management of Acute Stroke. Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital
 Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical College NewYork-Presbyterian Hospital I have no financial disclosures Understand range of pathology that may present
Louisiana State University Health Sciences Center
 Louisiana State University Health Sciences Center Department of Neurosurgery Student Clerkship Guide 2017 2018 Introduction Welcome to LSUHSC New Orleans neurosurgery rotation. Our department is dedicated
Louisiana State University Health Sciences Center Department of Neurosurgery Student Clerkship Guide 2017 2018 Introduction Welcome to LSUHSC New Orleans neurosurgery rotation. Our department is dedicated
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
The management of ICH when to operate when not to?
 The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
The management of ICH when to operate when not to? Intracranial Hemorrhage High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
Hemorrhagic Stroke. Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
 Hemorrhagic Stroke Objectives: Introduction Etiology Pathophysiology Clinical presentation Diagnosis and Imaging Treatment Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
Hemorrhagic Stroke Objectives: Introduction Etiology Pathophysiology Clinical presentation Diagnosis and Imaging Treatment Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Vascular Malformations of the Brain: A Review of Imaging Features and Risks
 Vascular Malformations of the Brain: A Review of Imaging Features and Risks Comprehensive Neuroradiology: Best Practices October 27-30, 2016 Sudhakar R. Satti, MD Associate Director Neurointerventional
Vascular Malformations of the Brain: A Review of Imaging Features and Risks Comprehensive Neuroradiology: Best Practices October 27-30, 2016 Sudhakar R. Satti, MD Associate Director Neurointerventional
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins
 ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
General Data. Gender: Female Birthday and age: 1932/11/03, 73 y/o Occupation: house keeper Date of Admission: 2005/03/30
 General Data Gender: Female Birthday and age: 1932/11/03, 73 y/o Occupation: house keeper Date of Admission: 2005/03/30 Chief Complain Dizziness and light headache for recent 1 year. Present illness Hypertension
General Data Gender: Female Birthday and age: 1932/11/03, 73 y/o Occupation: house keeper Date of Admission: 2005/03/30 Chief Complain Dizziness and light headache for recent 1 year. Present illness Hypertension
Dural Arteriovenous Malformations and Fistulae (DAVM S DAVF S)
") Jorge Guedes Campos NEUROIMAGING DEPARTMENT HOSPITAL SANTA MARIA UNIVERSITY OF LISBON PORTUGAL DEFINITION region of arteriovenous shunting confined to a leaflet of packymeninges often adjacent to a major
Jorge Guedes Campos NEUROIMAGING DEPARTMENT HOSPITAL SANTA MARIA UNIVERSITY OF LISBON PORTUGAL DEFINITION region of arteriovenous shunting confined to a leaflet of packymeninges often adjacent to a major
A Case of Carotid-Cavernous Fistula
 A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
10 May Disclosure. + Outline. Case-based approach to nontraumatic intracranial hemorrhage. Kathleen R. Fink, MD University of Washington
 Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Outline Case-based
Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Outline Case-based
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016
 Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE
Welcome to our Quarterly MISTIE III Safety Forum April 6, 2016 Agenda: Update from our Surgical Centers: Where we stand surgically Issam Awad, MD, University of Chicago Vascular Defect Screening in MISTIE
Brain Arteriovenous Malformations Endovascular Therapy and Associated Therapeutic Protocols Jorge Guedes Cabral de Campos
 Endovascular Therapy and Associated Therapeutic Protocols Jorge Guedes Cabral de Campos Neuroradiology Department Hospital de Santa Maria University of Lisbon CEREBRAL AVM CLINICAL / EPIDEMIOLOGY Brain
Endovascular Therapy and Associated Therapeutic Protocols Jorge Guedes Cabral de Campos Neuroradiology Department Hospital de Santa Maria University of Lisbon CEREBRAL AVM CLINICAL / EPIDEMIOLOGY Brain
Advances in Acute stroke Management
 Advances in Acute stroke Management Sandra Ripper-Brown, DNP Neuroscience Nurse Practitioner St. Mary s Medical Center WPB, FL Palm Beach County Nurse Practitioner Council Annual Conference APRNs: Agents
Advances in Acute stroke Management Sandra Ripper-Brown, DNP Neuroscience Nurse Practitioner St. Mary s Medical Center WPB, FL Palm Beach County Nurse Practitioner Council Annual Conference APRNs: Agents
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Carotid Cavernous Fistula
 Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
NEURORADIOLOGY DIL part 3
 NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
CT angiography and its role in the investigation of intracranial haemorrhage
 CT angiography and its role in the investigation of intracranial haemorrhage RD Magazine, 39, 458, 29-30 Dr M Igra Radiology SPR Leeds General Infirmary Dr I Djoukhadar Research fellow Wolfson Molecular
CT angiography and its role in the investigation of intracranial haemorrhage RD Magazine, 39, 458, 29-30 Dr M Igra Radiology SPR Leeds General Infirmary Dr I Djoukhadar Research fellow Wolfson Molecular
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Vascular Malformations
 Vascular Malformations LTC Robert Shih Chief of Neuroradiology Walter Reed Medical Center Special thanks to LTC Alice Smith (retired) Disclosures: None. This presentation reflects the personal views of
Vascular Malformations LTC Robert Shih Chief of Neuroradiology Walter Reed Medical Center Special thanks to LTC Alice Smith (retired) Disclosures: None. This presentation reflects the personal views of
What Are We Going to Do? Fourth Year Meds Clinical Neuroanatomy. Hydrocephalus and Effects of Interruption of CSF Flow. Tube Blockage Doctrine
 Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Supratentorial cerebral arteriovenous malformations : a clinical analysis
 Original article: Supratentorial cerebral arteriovenous malformations : a clinical analysis Dr. Rajneesh Gour 1, Dr. S. N. Ghosh 2, Dr. Sumit Deb 3 1Dept.Of Surgery,Chirayu Medical College & Research Centre,
Original article: Supratentorial cerebral arteriovenous malformations : a clinical analysis Dr. Rajneesh Gour 1, Dr. S. N. Ghosh 2, Dr. Sumit Deb 3 1Dept.Of Surgery,Chirayu Medical College & Research Centre,
Explaining All of the Options for AVM: Cerebral Arteriovenous Malformation
 Explaining All of the Options for AVM: Cerebral Arteriovenous Malformation Recorded on: November 19, 2012 Bernard Bendok, M.D. Director of the Neurointerventional Program Northwestern Memorial Hospital
Explaining All of the Options for AVM: Cerebral Arteriovenous Malformation Recorded on: November 19, 2012 Bernard Bendok, M.D. Director of the Neurointerventional Program Northwestern Memorial Hospital
Dilemma in Imaging Diagnosis, Endovascular Management and Complications
 Vascular anomaly at the craniocervical junction presenting with sub arachnoid hemorrhage: Dilemma in Imaging Diagnosis, Endovascular Management and Complications Ajeet 1* 1. Department of Radiology, St
Vascular anomaly at the craniocervical junction presenting with sub arachnoid hemorrhage: Dilemma in Imaging Diagnosis, Endovascular Management and Complications Ajeet 1* 1. Department of Radiology, St
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD
 Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
NEURORADIOLOGY Part I
 NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
NEURORADIOLOGY Part I Vörös Erika University of Szeged Department of Radiology SZEGED BRAIN IMAGING METHODS Plain film radiography Ultrasonography (US) Computer tomography (CT) Magnetic resonance imaging
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
A few Neurosurgical Emergencies. Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015
 A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
Index. C Capillary telangiectasia, intracerebral hemorrhage in, 295 Carbon monoxide, formation of, in intracerebral hemorrhage, edema due to,
 Neurosurg Clin N Am 13 (2002) 395 399 Index Note: Page numbers of article titles are in boldface type. A Age factors, in intracerebral hemorrhage outcome, 344 Albumin, for intracerebral hemorrhage, 336
Neurosurg Clin N Am 13 (2002) 395 399 Index Note: Page numbers of article titles are in boldface type. A Age factors, in intracerebral hemorrhage outcome, 344 Albumin, for intracerebral hemorrhage, 336
Summary of some of the landmark articles:
 Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Ischemic Stroke Studies
 Ischemic Stroke Studies ADAPT registry of thrombectomy using first-pass aspiration technique POINT ASA and Clopidogrel vs ASA and placebo in acute minor ischemic stroke or TIA POSITIVE ineligible for tpa,
Ischemic Stroke Studies ADAPT registry of thrombectomy using first-pass aspiration technique POINT ASA and Clopidogrel vs ASA and placebo in acute minor ischemic stroke or TIA POSITIVE ineligible for tpa,
Overview of Cerebrovascular Malformations
 Overview of Cerebrovascular Malformations Pursuit of Neurovascular Excellence 8 th annual Barbara Albani, MD Chief, Neurointerventional Surgery Christiana Care Health Systems Newark, DE Financial Disclosures
Overview of Cerebrovascular Malformations Pursuit of Neurovascular Excellence 8 th annual Barbara Albani, MD Chief, Neurointerventional Surgery Christiana Care Health Systems Newark, DE Financial Disclosures
ORIGINAL ARTICLE COMPUTED TOMOGRAPHY EVALUATION OF SPONTANEOUS INTRACRANIAL HAEMORRHAGE
 Available online at www.journalijmrr.com INTERNATIONAL JOURNAL OF MODERN RESEARCH AND REVIEWS IJMRR ISSN: 2347-8314 Int. J. Modn. Res. Revs. Volume 3, Issue 4, pp 647-652, April, 2015 ORIGINAL ARTICLE
Available online at www.journalijmrr.com INTERNATIONAL JOURNAL OF MODERN RESEARCH AND REVIEWS IJMRR ISSN: 2347-8314 Int. J. Modn. Res. Revs. Volume 3, Issue 4, pp 647-652, April, 2015 ORIGINAL ARTICLE
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
What Is an Arteriovenous malformation (AVM)?
?") American Society of Neuroradiology What Is an Arteriovenous malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall
American Society of Neuroradiology What Is an Arteriovenous malformation (AVM)? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Diagnostic Cerebral Angiography in Spontaneous Intracranial Haemorrhage: A Guide for Developing Countries
 Original Article Diagnostic Cerebral Angiography in Spontaneous Intracranial Haemorrhage: A Guide for Developing Countries Ishak Abu Bakar, Ibrahim Lutfi Shuaib, Abdul Rahman Mohd Ariff, Nyi Nyi Naing
Original Article Diagnostic Cerebral Angiography in Spontaneous Intracranial Haemorrhage: A Guide for Developing Countries Ishak Abu Bakar, Ibrahim Lutfi Shuaib, Abdul Rahman Mohd Ariff, Nyi Nyi Naing
From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council
 American Society of Neuroradiology What Is a Stroke? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair
American Society of Neuroradiology What Is a Stroke? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair
The management of ICH when to operate when not to?
 The management of ICH when to operate when not to? ICH is a Bad Disease High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
The management of ICH when to operate when not to? ICH is a Bad Disease High Incidence o Accounts for 10-15% of all strokes 1,2,5 o 80,000 cases in US; 2 million WW 2,5 o Incidence doubles for African-
Ventriculostomy and Risk of Upward Herniation in Patients with Obstructive Hydrocephalus from Posterior Fossa Mass Lesions
 https://doi.org/10.1007/s12028-017-0487-3 ORIGINAL ARTICLE Ventriculostomy and Risk of Upward Herniation in Patients with Obstructive Hydrocephalus from Posterior Fossa Mass Lesions Sherri A. Braksick
https://doi.org/10.1007/s12028-017-0487-3 ORIGINAL ARTICLE Ventriculostomy and Risk of Upward Herniation in Patients with Obstructive Hydrocephalus from Posterior Fossa Mass Lesions Sherri A. Braksick
Medical Review Guidelines Magnetic Resonance Angiography
 Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Overview of imaging modalities for cerebral aneurysms
 Overview of imaging modalities for cerebral aneurysms Soroush Zaghi BIDMC PCE: Radiology August 2008 (Images from BIDMC, PACS.) Our Patient: Presentation Our patient is a 57 y/o woman who reports blowing
Overview of imaging modalities for cerebral aneurysms Soroush Zaghi BIDMC PCE: Radiology August 2008 (Images from BIDMC, PACS.) Our Patient: Presentation Our patient is a 57 y/o woman who reports blowing
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Stereotactic Burr Hole Aspiration Surgery for Spontaneous Hypertensive Cerebellar Hemorrhage
 Journal of Cerebrovascular and Endovascular Neurosurgery ISSN 2234-8565, EISSN 2287-3139, http://dx.doi.org/10.7461/jcen.2012.14.3.170 Original Article Stereotactic Burr Hole Aspiration Surgery for Spontaneous
Journal of Cerebrovascular and Endovascular Neurosurgery ISSN 2234-8565, EISSN 2287-3139, http://dx.doi.org/10.7461/jcen.2012.14.3.170 Original Article Stereotactic Burr Hole Aspiration Surgery for Spontaneous
Case Conference: Neuroradiology. Case 1: Tumor Case 1: 22yo F w/ HA and prior Seizures
 Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT
 Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
Pearls and Pitfalls in Neuroradiology of Cerebrovascular Disease The Essentials with MR and CT Val M. Runge, MD Wendy R. K. Smoker, MD Anton Valavanis, MD Control # 823 Purpose The focus of this educational
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM. Vikram Jadhav MD, PhD. 04/12/2018 CentraCare Health St.
 ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
VASCULAR MALFORMATIONS. Owen Samuels, MD Adam Webb, MD Emory University
 VASCULAR MALFORMATIONS Owen Samuels, MD Adam Webb, MD Emory University Introduction Brain and spinal cord vascular malformations can be separated into five main categories: 1) Arteriovenous malformation,
VASCULAR MALFORMATIONS Owen Samuels, MD Adam Webb, MD Emory University Introduction Brain and spinal cord vascular malformations can be separated into five main categories: 1) Arteriovenous malformation,
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Talent Abdominal Stent Graft
 Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
4/10/2018. The Surgical Treatment of Cerebral Aneurysms. Aneurysm Locations. Aneurysmal Subarachnoid Hemorrhage. Jerone Kennedy, M.D.
 The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite
 Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
Endovascular Treatment of Cerebral Arteriovenous Malformations. Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh
 Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial. Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD
 Trial. Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD") FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD Background Intracerebral hemorrhage (ICH) accounts for more than
FVIIa for Acute Hemorrhagic Stroke Administered at Earliest Time (FASTEST) Trial Joseph P. Broderick, MD James Grotta, MD Jordan Elm, PhD Background Intracerebral hemorrhage (ICH) accounts for more than
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
Symptoms of small vessel strokes. Small Vessel stroke. What is this? Treatment. Large Vessel stroke 6/1/2018
 Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage
 July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
Microsurgery for ruptured cerebellar arteriovenous malformations
 European Review for Medical and Pharmacological Sciences Microsurgery for ruptured cerebellar arteriovenous malformations S.-F. GONG 1,2, X.-B. WANG 1,3, Y.-Q. LIAO 1,2, T.-P. JIANG 1,2, J.-B. HE 1,2,
European Review for Medical and Pharmacological Sciences Microsurgery for ruptured cerebellar arteriovenous malformations S.-F. GONG 1,2, X.-B. WANG 1,3, Y.-Q. LIAO 1,2, T.-P. JIANG 1,2, J.-B. HE 1,2,
Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy
 ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease
 Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Cerebrovascular Malformations in the Elderly Indications for Treatment
 Cerebrovascular Malformations in the Elderly Indications for Treatment Johanna T. Fifi, MD, FAHA, FSVIN Director of Endovascular Ischemic Stroke Assistant Professor of Neurology, Neurosurgery, and Radiology
Cerebrovascular Malformations in the Elderly Indications for Treatment Johanna T. Fifi, MD, FAHA, FSVIN Director of Endovascular Ischemic Stroke Assistant Professor of Neurology, Neurosurgery, and Radiology
Historical perspective
 SPINAL AVM Introduction Vascular malformations of spinal cord are a rare clinical entity, representing 5% of all primary spinal cord lesions, with arteriovenous malformations(avm) & cavernous malformations
SPINAL AVM Introduction Vascular malformations of spinal cord are a rare clinical entity, representing 5% of all primary spinal cord lesions, with arteriovenous malformations(avm) & cavernous malformations
M555 Medical Neuroscience Blood Flow in CNS Meninges Blood Brain Barrier CSF
 M555 Medical Neuroscience Blood Flow in CNS Meninges Blood Brain Barrier CSF Arterial Blood Flow to CNS approximately % of what goes wrong within the skull that produces neurological deficits is vascular
M555 Medical Neuroscience Blood Flow in CNS Meninges Blood Brain Barrier CSF Arterial Blood Flow to CNS approximately % of what goes wrong within the skull that produces neurological deficits is vascular
Pediatric Neurointervention: Vein of Galen Malformations
 Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Classification of Stroke. CNA Neuroscience Nursing Course: Cerebrovascular Disorders. Stroke in Canada
 CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
Vascular Malformations of the Brain. William A. Cox, M.D. Forensic Pathologist/Neuropathologist. September 8, 2014
 Vascular Malformations of the Brain William A. Cox, M.D. Forensic Pathologist/Neuropathologist September 8, 2014 Vascular malformations of the brain are classified into four principal groups: arteriovenous
Vascular Malformations of the Brain William A. Cox, M.D. Forensic Pathologist/Neuropathologist September 8, 2014 Vascular malformations of the brain are classified into four principal groups: arteriovenous
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Idiopathic Lenticulostriate Artery Pseudoaneurysm Protruding into the Lateral Ventricle: A Case Report
 Journal of Cerebrovascular and Endovascular Neurosurgery ISSN 2234-8565, EISSN 2287-3139, http://dx.doi.org/10.7461/jcen.2013.15.3.246 Case Report Idiopathic Lenticulostriate Artery Pseudoaneurysm Protruding
Journal of Cerebrovascular and Endovascular Neurosurgery ISSN 2234-8565, EISSN 2287-3139, http://dx.doi.org/10.7461/jcen.2013.15.3.246 Case Report Idiopathic Lenticulostriate Artery Pseudoaneurysm Protruding
Cerebral Aneurysms. U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health
 Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an
Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an