Principles of Surgical Oncology ศาสตราจารย นายแพทย ธนพล ไหมแพง
|
|
|
- Brice Percival Lynch
- 5 years ago
- Views:
Transcription

1 Principles of Surgical Oncology ศาสตราจารย นายแพทย ธนพล ไหมแพง
2 Surgery is the oldest treatment for cancer and, until recently, was the only treatment that could cure patients with cancer.
3 Ancient history of surgery for cancer treatment 1600 BC First recorded description of the surgical treatment of cancer (in Egypt) 400 BC Hippocrates describes the stages of cancer and advises against surgery for terminal disease; he coins the terms carcinoma (crab-leg tumor) and sarcoma (fleshy tumor) 200 AD Galen identifies cancer as a systemic disease (primary and metastasis)
4 Historical eras of surgery to treat cancer Before 1850 Early heroic attempts to resect cancer Development of standard surgical resection techniques Development of extended radical surgical procedures
5 Historical eras of surgery to treat cancer Exploration of combinedmodality treatment Multimodality therapy improves organ preservation and survival 2000-present Surgical practice incorporates improved understanding of the molecular basis of tumor biology
6 Roles for Surgery Prevention of cancer Diagnosis of cancer Treatment of cancer Rehabilitation
7 Surgery that can prevent cancer Underlying Associated cancer Prophylactic surgery Cryptorchidism Polyposis coli Familial colon cancer Ulcerative colitis Multiple endocrines Neoplasm (type II and III) Familial breast cancer Familial ovarian cancer Testicular Colon Colon Colon Medullary cancer of the thyroid Breast Ovary Orchiopexy Colectomy Colectomy Colectomy Thyroidectomy Mastectomy Oophorectomy
8 Roles for Surgery Prevention of cancer Diagnosis of cancer Treatment of cancer Rehabilitation
9 Surgical detection and biopsy for tissue diagnosis Fine Needle Aspiration (FNA) cytology Core needle biopsy Incisional biopsy Excisional biopsy Surgical staging

10
11 Pitfalls in Biopsy Techniques

12
13 Specialized techniques of cancer management Laparoscopy UGI endoscopy Colonoscopy Bronchoscopy Mediastinoscopy Thoracoscopy Needle localization and breast biopsy

14


15


16
17 Roles for Surgery Prevention of cancer Diagnosis of cancer Treatment of cancer Rehabilitation
18 Surgical Treatment of Cancer Surgery for primary cancer Surgery for residual disease Surgery for metastatic disease Surgery for oncologic emergencies Surgery for palliation Surgery for reconstruction and rehabilitation
19 Principles of surgical resection of tumor Adequate margin of resection Prevention of tumor spillage Minimal manipulation Reconstruction
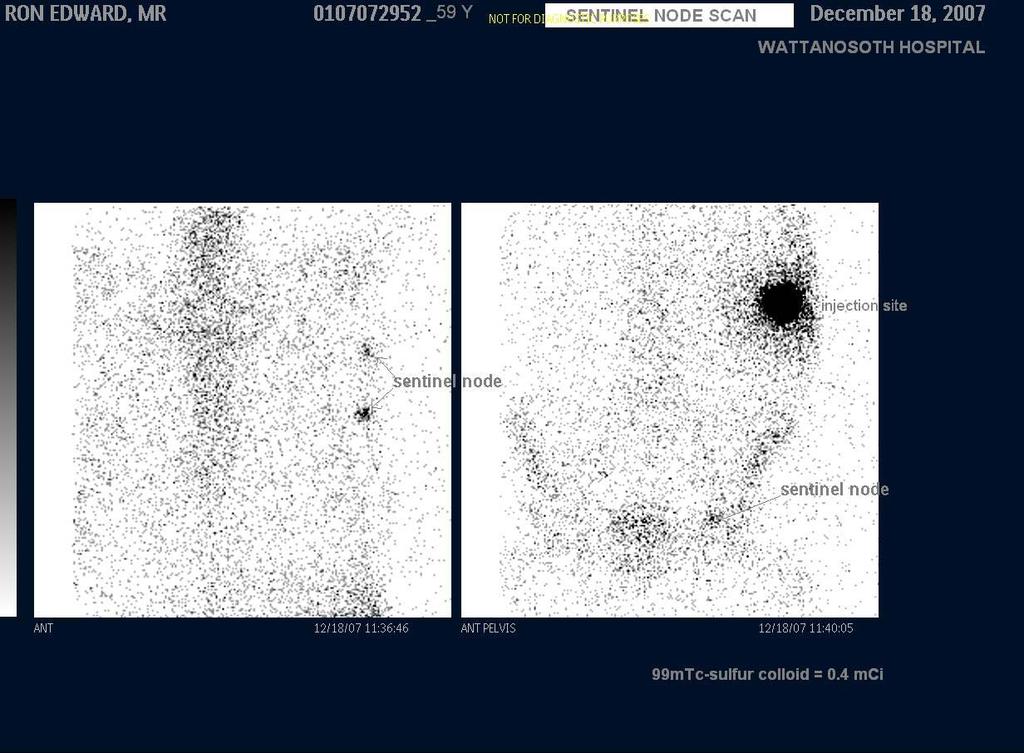
20 New Concepts in Cancer Management Conservative breast surgery (Sentinel node biopsy) Limb salvage surgery in sarcoma Major ablative surgery in head & neck cancer

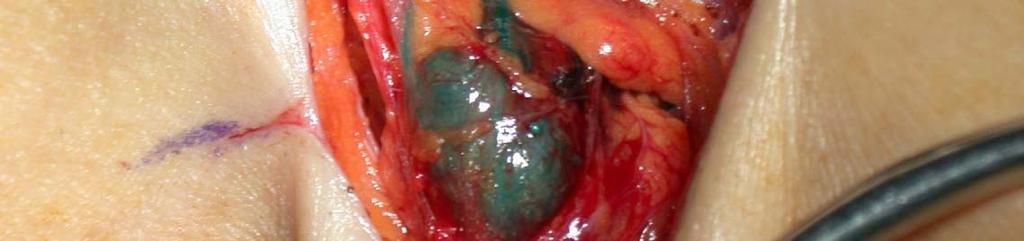

21 Sentinel node biopsy
22




23




24

25
26 Perioperative management of patient with cancer
27 Effects of cancer Anatomical Tumors Cancer therapy Physiological Tumors Cancer therapy
28 Anatomical effects of tumors Airway consideration in patient with advanced head and neck tumors - Preoperative CT scan - Awake intubation using fiberoptic guidance - Beware of post operative airway obstruction

29


30
31 Anatomical Effects of Tumors (cont.) Mediastinal Masses History of dyspnea, stridor, wheezing, orthopnea Patient with possible mediastinal compression should be avoid from general anesthesia (biopsy under local anesthesia) Neuman GG, et al. Anesthesiology 1984; 60:

32
33 Mediastinal Masses (cont.) Patients who require general anesthesia despite tracheobronchial tree compression should undergo the following 1. Awake fiberoptic intubation 2. Spontaneous ventilation throughout the procedure
34 Mediastinal masses (cont.) 3. Ability to quickly reposition the patient to lateral, prone or sitting position in the event of cardiovascular collapse or airway obstruction 4. Available rigid bronchoscopy to open, a collapsed airway 5. Standby femoro-femoral bypass In: Lefor AT, ed. Surgical problems affecting the patient with cancer. Philadelphia, PA: Lippincott-Raven, 1996;
35 Physiologic effects of tumors Pheochromocytoma - Preoperative pharmacologic manipulation - Intraoperative monitoring Hypertensive crisis Hypotension
36 Physiologic effects of tumors Carcinoid Tumors 5 hydroxytryptamine (serotonin) Diarrhea with abdominal cramping Respiratory distress Bronchospasm Hypertension
37 Carcinoid Tumor (cont.) Preoperative Preparation Adequate hydration Cardiac evaluation (Right sided heart failure)
38 Anatomical effects of cancer therapy Effects of radiation therapy to the head and neck Distortion of airway anatomy Edema and swelling of tissue


39
40 Effects of radiation therapy to the GI Tract Stricture Obstruction Perforation Bleeding Fistula formation Radiation induced bowel injury
41 Physiologic effects of cancer therapy Bleomycin Pulmonary fibrosis Dry non productive cough Dyspnea Fever Tachypnea
42 Physiologic effects of cancer therapy (cont.) Cardiac toxicity Doxorubicin Daunorubicin Epirubicin ECG change or Chronic cardiomyopathy Herceptin

43
44 Hepatic Toxicity After Chemotherapy Steatosis Vascular Lesions (Centrolobular Necrosis) Steatohepatitis (CASH : Chemotherapy - Associated Steatohepatitis)
45 Physiologic effects of cancer therapy (cont.) Steroid administration Received > 2 weeks in the past year Risk of adrenal suppression
46 Poor Nutritional status Effects of tumor and therapy Eating and Drinking impaired by pain, nausea, stomatitis Tumor involving oropharynx or GI tract Metabolic aberrations may induce anorexia and weight loss
47 Poor nutritional status (cont.) Perioperative nutritional support Fewer operative complications Shorter length of hospital stay
48 Oncogeriatric patients Two thirds of all solid tumors occur in patients aged 65 years or older and most cancer related deaths occur within this age group 1. Alexander HR, et al., J Surg Oncol 1991; 47: Wallach CB, et al., Gastroenterol Clin North Am 1990; 19: Brookes B. Ann Surg 1937; 105:
49 Oncogeriatric patients (cont.) There is considerable evidence that this steadily expanding population receives substandard treatment when compared with younger age groups Samet J, et al., JAMA 1986; 255:
50 Surgical Treatment of Cancer Surgery for primary cancer Surgery for residual disease Surgery for metastatic disease Surgery for oncologic emergencies Surgery for palliation Surgery for reconstruction and rehabilitation
51 Surgical Treatment of Metastatic Disease Pulmonary metastases Liver metastases Bone metastases Brain metastases
52 Criteria for resection of pulmonary metastasis The disease at the primary site must be controlled No metastases outside of the lungs are demonstrable All apparent disease in the chest must be completely resectable The risk of the resection must not be excessive


53

54
55 Metastasectomy Complete resection of distant metastases improves five-year overall survival rates 40% for colorectal cancer with resection of liver metastases 30% for sarcoma with resection of lung metastases 16% for breast cancer with resection of brain metastases
56 Surgical Treatment of Cancer Surgery for primary cancer Surgery for residual disease Surgery for metastatic disease Surgery for oncologic emergencies Surgery for palliation Surgery for reconstruction and rehabilitation
57 Surgery for palliation Goals of palliative surgery Relieve symptoms for patients beyond cure when non-surgical measures are not feasible, not effective, or not expedient Palliation means patient should be better at the completion of the procedure It is axiomatic that one cannot palliatively improve an asymptomatic patient using a scalpel. R. G. Martin, 1982
58 Palliative improvement of function and quality of life Adequate control of pain Relief gastrointestinal and biliary obstruction Stop hemorrhage Supplement poor nutrition Airway obstruction Renal failure Rectal or urinary incontinence
59 Surgery for reconstruction and rehabilitation Restoration of form Restoration of function Care of ostomies Psychological treatment and support Maintenance and improvement of quality of life
60 Treatment-related complications Gastrointestinal and genitourinary strictures Fistulae Tissue necrosis of bone (osteonecrosis) or skin Proctitis and cystitis Radiation-induced secondary cancer
61 The surgeon who treats cancer must be familiar with the natural history of diseases and with the principles of multimodality treatment of surgery, radiation therapy, chemotherapy, immunotherapy and other new treatment modalities.
62 Surgical Oncologist is well qualified surgeon who has obtained additional training and experience in multidisciplinary approach to Prevention Diagnosis Treatment Cancer patients Rehabilitation Devotes a major portion of their professional practice to these activities and cancer research.
63 Multidisciplinary teams and collaborative environment Teams include not only clinicians and nurses but also support staff and basic and applied scientists. All aiming toward improved outcomes and higher quality of care and of life.
64 Training of Surgical Oncologist Two years training program on a surgical oncology service Training from approved program Training at a center with sufficient basic science resources Training at an institution that will provide adequate operative experience Full-time assignment to radiation and medical oncology
65 Surgical Oncology in the Future Preemptive surgery in populations at genetic risk for the development of cancer Tissue and function-preserving improvements Minimally invasive and robotic surgery Implantable monitors Treatment sensitizers Tissue-engineered, implantable spare parts Refinements in surgical practice will be driven by the underlying molecular basis of tumor biology

66
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Therapeutic Bronchoscopy Etiology - Benign Stenosis Post - intubation Trauma Post - operative Inflammatory Idiopathic
 Endobronchial Palliation of Airway Disease Douglas E. Wood, MD Professor and Chief Division of Cardiothoracic Surgery Vice-Chair, Department of Surgery Endowed Chair in Lung Cancer Research University
Endobronchial Palliation of Airway Disease Douglas E. Wood, MD Professor and Chief Division of Cardiothoracic Surgery Vice-Chair, Department of Surgery Endowed Chair in Lung Cancer Research University
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
So, we already talked about that recognition is the key to optimal treatment and outcome.
 Hi, I m Dr. Anthony Lucci from the University of Texas MD Anderson Cancer Center in Houston. And today, I d like to talk to you about the role of surgery in inflammatory breast cancer patients. So, there
Hi, I m Dr. Anthony Lucci from the University of Texas MD Anderson Cancer Center in Houston. And today, I d like to talk to you about the role of surgery in inflammatory breast cancer patients. So, there
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Faster Cancer Treatment Indicators: Use cases
 Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine
 What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
Advances in Breast Surgery. Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015
 Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
PET IMAGING (POSITRON EMISSION TOMOGRAPY) FACT SHEET
 FACT SHEET") Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
National Breast Cancer Audit next steps. Martin Lee
 National Breast Cancer Audit next steps Martin Lee National Cancer Audits Current Bowel Cancer Head & Neck Cancer Lung cancer Oesophagogastric cancer New Prostate Cancer - undergoing procurement Breast
National Breast Cancer Audit next steps Martin Lee National Cancer Audits Current Bowel Cancer Head & Neck Cancer Lung cancer Oesophagogastric cancer New Prostate Cancer - undergoing procurement Breast
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018)
 Test Content Outline (Effective 2018)") Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018) I. Coordination of Care - 26% A. Breast health, screening, early detection, risk assessment and reduction 1. Issues related to
Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018) I. Coordination of Care - 26% A. Breast health, screening, early detection, risk assessment and reduction 1. Issues related to
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
The Role of Surgery in Inflammatory Bowel Disease. Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health
 The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: SURGICAL ONCOLOGY 5-May-2013 DEVELOPED BY: Bruce
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: SURGICAL ONCOLOGY 5-May-2013 DEVELOPED BY: Bruce
2/3/2015. Anterior Mediastinal Masses and Lower Airway Problems
 es and Lower Airway Problems es and Lower Airway Problems 25 y.o. Female Ant. Mediastinal Mass Cervical Mediastinoscopy + Biopsy Most Important History? A) Dysphagia B) Fever C) Orthopnea D) Chest pain
es and Lower Airway Problems es and Lower Airway Problems 25 y.o. Female Ant. Mediastinal Mass Cervical Mediastinoscopy + Biopsy Most Important History? A) Dysphagia B) Fever C) Orthopnea D) Chest pain
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Colon, or Colorectal, Cancer Information
 Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
Patient Name Date of Birth Age. Other phone ( ) . Other
 . Other") GASTROINTESTINAL & MINIMALLY INVASIVE SURGERY HEALTH HISTORY QUESTIONNAIRE Date Patient Name _ Date of Birth Age Daytime phone ( ) Other phone ( ) Email How did you hear about us? My doctor Yellow pages
GASTROINTESTINAL & MINIMALLY INVASIVE SURGERY HEALTH HISTORY QUESTIONNAIRE Date Patient Name _ Date of Birth Age Daytime phone ( ) Other phone ( ) Email How did you hear about us? My doctor Yellow pages
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
Multidisciplinary management of retroperitoneal sarcomas
 Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
PEDIATRIC & ADOLESCENT CANCER SURVIVORSHIP. Denise Rokitka, MD, MPH
 PEDIATRIC & ADOLESCENT CANCER SURVIVORSHIP Denise Rokitka, MD, MPH Objectives Describe incidence of childhood cancer and survival rates and causes of early mortality. Understand the late effects of cancer
PEDIATRIC & ADOLESCENT CANCER SURVIVORSHIP Denise Rokitka, MD, MPH Objectives Describe incidence of childhood cancer and survival rates and causes of early mortality. Understand the late effects of cancer
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Animal chemotherapy Film radiotherapy Music cancer treatment
 Cancer treatments Animal chemotherapy Film radiotherapy Music cancer treatment What are the main treatments? Hormone therapy Surgery Chemotherapy Radiotherapy Targeted anti-cancer therapy (immunotherapy)
Cancer treatments Animal chemotherapy Film radiotherapy Music cancer treatment What are the main treatments? Hormone therapy Surgery Chemotherapy Radiotherapy Targeted anti-cancer therapy (immunotherapy)
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Radiation Treatment for Breast. Cancer. Melissa James Radiation Oncologist August 2015
 Radiation Treatment for Breast Cancer Melissa James Radiation Oncologist August 2015 OUTLINE External Beam Radiation treatment. (What is Radiation, doctor?) Role of radiation. (Why am I getting radiation,
Radiation Treatment for Breast Cancer Melissa James Radiation Oncologist August 2015 OUTLINE External Beam Radiation treatment. (What is Radiation, doctor?) Role of radiation. (Why am I getting radiation,
Caring for a Patient with Colorectal Cancer. Objectives. Poll question. UNC Cancer Network Presented on 10/15/18. For Educational Use Only 1
 Caring for a Patient with Colorectal Cancer Tammy Triglianos RN, APRN-BC, AOCNP Nurse Practitioner, GI Oncology 10/15/2018 Objectives Describe common signs and symptoms of colorectal cancer Understand
Caring for a Patient with Colorectal Cancer Tammy Triglianos RN, APRN-BC, AOCNP Nurse Practitioner, GI Oncology 10/15/2018 Objectives Describe common signs and symptoms of colorectal cancer Understand
DEPARTMENT OF ONCOLOGY ELECTIVE
 DEPARTMENT OF ONCOLOGY ELECTIVE 2015-2016 www.uwo.ca/oncology Oncology Elective Program Administrator: Ms. Kimberly Trudgeon Room A4-901C (Admin) LHSC London Regional Cancer Centre (Victoria Campus) Phone:
DEPARTMENT OF ONCOLOGY ELECTIVE 2015-2016 www.uwo.ca/oncology Oncology Elective Program Administrator: Ms. Kimberly Trudgeon Room A4-901C (Admin) LHSC London Regional Cancer Centre (Victoria Campus) Phone:
When do you delay surgery?
 Cancer BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University of Chicago I have no disclosures 2 nd leading
Cancer BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University of Chicago I have no disclosures 2 nd leading
Laparoscopic Colorectal Surgery
 Laparoscopic Colorectal Surgery 20 th November 2015 Dr Adam Cichowitz General Surgeon Laparoscopic Colorectal Surgery Introduced in early 1990s Uptake slow Steep learning curve Requirement for equipment
Laparoscopic Colorectal Surgery 20 th November 2015 Dr Adam Cichowitz General Surgeon Laparoscopic Colorectal Surgery Introduced in early 1990s Uptake slow Steep learning curve Requirement for equipment
ANNEX 1 OBJECTIVES. At the completion of the training period, the fellow should be able to:
 1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Oncologic Emergencies
 Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory
Oncologic Emergencies Peter Bjerkerot RN, OCN 1339 Normandy Drive Atlanta, GA 30306-2574 404.754.5952 WebPage http://boyrn.com peter.bjerkerot@mindspring.com Full Disclosure Statement Celgene Nurse Advisory
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
Oncologic Emergencies: When to call the Radiation Oncologist
 Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Oncologic Emergencies: When to call the Radiation Oncologist Dr. Shrinivas Rathod Radiation Oncologist Radiation Oncology Program CancerCare Manitoba and University of Manitoba Disclosures Speaker s name:
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Maria João Cardoso, MD, PhD
 Locally Advanced Breast Cancer Specific Issues in LocorregionalTreatment Surgery, MD, PhD Head Breast Surgeon Breast Unit, Champalimaud Foundation Lisbon, Portugal 1 Conflict of Interest Disclosure No
Locally Advanced Breast Cancer Specific Issues in LocorregionalTreatment Surgery, MD, PhD Head Breast Surgeon Breast Unit, Champalimaud Foundation Lisbon, Portugal 1 Conflict of Interest Disclosure No
Principles of Surgical Oncology. Winnie Achilles Tierklinik Hollabrunn Lastenstrasse Hollabrunn
 Principles of Surgical Oncology Winnie Achilles Tierklinik Hollabrunn Lastenstrasse 2 2020 Hollabrunn boexi@gmx.de The first surgery provides the best chance for a cure in an animal with a tumor Clinical
Principles of Surgical Oncology Winnie Achilles Tierklinik Hollabrunn Lastenstrasse 2 2020 Hollabrunn boexi@gmx.de The first surgery provides the best chance for a cure in an animal with a tumor Clinical
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age. Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010
 Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
BCCA Protocol Summary for Combined Modality Adjuvant Therapy for High Risk Rectal Carcinoma using Capecitabine and Radiation Therapy
 BCCA Protocol Summary for Combined Modality Adjuvant Therapy for High Risk Rectal Carcinoma using Capecitabine and Radiation Therapy Protocol Code: Tumour Group: Contact Physician: GIRCRT Gastrointestinal
BCCA Protocol Summary for Combined Modality Adjuvant Therapy for High Risk Rectal Carcinoma using Capecitabine and Radiation Therapy Protocol Code: Tumour Group: Contact Physician: GIRCRT Gastrointestinal
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM
 OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation *
 ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
RECTUM/SIGMOID COLON/BOWEL,
 EMBRACE Follow-up Patient ID: Day Month Year Physician (initials) RECTUM/SIGMOID COLON/BOWEL, morbidity scoring CTC v3.0 1. Diarrhea 1: Increase of
EMBRACE Follow-up Patient ID: Day Month Year Physician (initials) RECTUM/SIGMOID COLON/BOWEL, morbidity scoring CTC v3.0 1. Diarrhea 1: Increase of
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Cancer of Unknown Primary (CUP) Protocol
 Protocol") 1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type)
") Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
BRLAACDT. Protocol Code. Breast. Tumour Group. Dr. Karen Gelmon. Contact Physician
 BCCA Protocol Summary for Treatment of Locally Advanced Breast Cancer using DOXOrubicin and Cyclophosphamide followed by DOCEtaxel and Trastuzumab (HERCEPTIN) Protocol Code Tumour Group Contact Physician
BCCA Protocol Summary for Treatment of Locally Advanced Breast Cancer using DOXOrubicin and Cyclophosphamide followed by DOCEtaxel and Trastuzumab (HERCEPTIN) Protocol Code Tumour Group Contact Physician
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Cancer is a group of more than 100 different diseases that are characterized by uncontrolled cellular growth,
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Cancer is a group of more than 100 different diseases that are characterized by uncontrolled cellular growth,
HEPATIC METASTASES. We can state 3 types of metastases depending on their treatment options:
 HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction
 The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction Alaa Gaafar-MD, Ahmed Youssef-MD, Mohamed Elhadidi-MD A l e x a n d r i a F a c u l t y o f
The use of metallic expandable tracheal stents in the management of inoperable malignant tracheal obstruction Alaa Gaafar-MD, Ahmed Youssef-MD, Mohamed Elhadidi-MD A l e x a n d r i a F a c u l t y o f
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Appendix 4 Urology Care Pathways
 Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Gastrointestinal obstruction Dr Iain Lawrie
 Gastrointestinal obstruction Dr Iain Lawrie Consultant and Honorary Clinical Senior Lecturer in Palliative Medicine The Pennine Acute Hospitals NHS Trust / The University of Manchester iain.lawrie@pat.nhs.uk
Gastrointestinal obstruction Dr Iain Lawrie Consultant and Honorary Clinical Senior Lecturer in Palliative Medicine The Pennine Acute Hospitals NHS Trust / The University of Manchester iain.lawrie@pat.nhs.uk
THE COLLEGE OF SURGEONS OF HONG KONG
 CRITERIA FOR RECOGNITION OF SUBSPECIALTIES IN GENERAL KEY ESSENTIAL FOR THE IN THE POST Total Mastectomy / MRM * 10 BREAST Breast Conserving Surgery * 10 2 (The Axillary Dissection # 10 minimum number
CRITERIA FOR RECOGNITION OF SUBSPECIALTIES IN GENERAL KEY ESSENTIAL FOR THE IN THE POST Total Mastectomy / MRM * 10 BREAST Breast Conserving Surgery * 10 2 (The Axillary Dissection # 10 minimum number
Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery
 Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery Goal The goal of the Breast Surgery rotation is to develop the knowledge, skills and attitudes necessary to evaluate,
Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery Goal The goal of the Breast Surgery rotation is to develop the knowledge, skills and attitudes necessary to evaluate,
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Cancer. University of Illinois at Chicago College of Nursing
 Cancer University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Develop a basic understanding of cancer 2. Describe
Cancer University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Develop a basic understanding of cancer 2. Describe
Wilms Tumor and Neuroblastoma
 Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
Wilms Tumor and Neuroblastoma Wilm s Tumor AKA: Nephroblastoma the most common intra-abdominal cancer in children. peak incidence is 2 to 3 years of age Biology somatic mutations restricted to tumor tissue
The Itracacies of Staging Patients with Suspected Lung Cancer
 The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Classification System
 Classification System A graduate of the Breast Oncology training program should be able to care for all aspects of disease and/or provide comprehensive management. When referring to a discipline of training
Classification System A graduate of the Breast Oncology training program should be able to care for all aspects of disease and/or provide comprehensive management. When referring to a discipline of training
Structured Follow-Up after Colorectal Cancer Resection: Overrated. R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007
 Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018
 Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Calcitonin. 1
 Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Esophageal Cancer. What is esophageal cancer?
 Scan for mobile link. Esophageal Cancer Esophageal cancer occurs when cancer cells develop in the esophagus. The two main types are squamous cell carcinoma and adenocarcinoma. Esophageal cancer may not
Scan for mobile link. Esophageal Cancer Esophageal cancer occurs when cancer cells develop in the esophagus. The two main types are squamous cell carcinoma and adenocarcinoma. Esophageal cancer may not
Rectal Cancer. About the Colon and Rectum. Symptoms. Colorectal Cancer Screening
 Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
3/9/2017. Chapter 56. Care of the Patient with Cancer. Cancer Rates in the US. Carcinogenesis
 Chapter 56 Care of the Patient with Cancer All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Cancer Rates in the US 1 in 2 men and 1 in 3 women
Chapter 56 Care of the Patient with Cancer All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Cancer Rates in the US 1 in 2 men and 1 in 3 women
Thoracoscopy for Lung Cancer
 Thoracoscopy for Lung Cancer Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your doctor may have recommended an operation to remove your lung cancer. The
Thoracoscopy for Lung Cancer Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your doctor may have recommended an operation to remove your lung cancer. The
BRAJACTT. Protocol Code. Breast. Tumour Group. Dr. Karen Gelmon. Contact Physician
 BC Cancer Protocol Summary for Adjuvant Therapy for Breast Cancer using DOXOrubicin and Cyclophosphamide followed by PACLitaxel and Trastuzumab (HERCEPTIN) Protocol Code Tumour Group Contact Physician
BC Cancer Protocol Summary for Adjuvant Therapy for Breast Cancer using DOXOrubicin and Cyclophosphamide followed by PACLitaxel and Trastuzumab (HERCEPTIN) Protocol Code Tumour Group Contact Physician
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Thoracic Surgery. Treating a wide range of chest disorders
 Thoracic Surgery Treating a wide range of chest disorders Thoracic Surgery at UCLA The UCLA Division of Cardiothoracic Surgery is among the nation s leaders in providing care for a wide range of chest
Thoracic Surgery Treating a wide range of chest disorders Thoracic Surgery at UCLA The UCLA Division of Cardiothoracic Surgery is among the nation s leaders in providing care for a wide range of chest
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
ENDPOINTS IN ONCOLOGY- HOW LONG WILL A CANCER PATIENT SURVIVE? DR GUNJAN BAIJAL CONSULTANT RADIATION ONCOLOGY MANIPAL GOA
 ENDPOINTS IN ONCOLOGY- HOW LONG WILL A CANCER PATIENT SURVIVE? DR GUNJAN BAIJAL CONSULTANT RADIATION ONCOLOGY MANIPAL GOA Why so much of cancer today? Times have changed HISTORICAL PERSPECTIVE CANCER as
ENDPOINTS IN ONCOLOGY- HOW LONG WILL A CANCER PATIENT SURVIVE? DR GUNJAN BAIJAL CONSULTANT RADIATION ONCOLOGY MANIPAL GOA Why so much of cancer today? Times have changed HISTORICAL PERSPECTIVE CANCER as
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
COUGH Dr. A m A it i e t sh A g A garwa w l Le L ctu t rer Departm t ent t o f f M e M dic i in i e
 COUGH Dr. Amitesh Aggarwal Lecturer Department of Medicine Cough is an explosive expiration that provides a normal protective mechanism for clearing the tracheobronchial tree of secretions and foreign
COUGH Dr. Amitesh Aggarwal Lecturer Department of Medicine Cough is an explosive expiration that provides a normal protective mechanism for clearing the tracheobronchial tree of secretions and foreign
ISPUB.COM. Rare Cases: Tracheal/bronchial Obstruction. O Wenker, L Moehn, C Portera, G Walsh HISTORY ADMISSION
 ISPUB.COM The Internet Journal of Radiology Volume 1 Number 1 O Wenker, L Moehn, C Portera, G Walsh Citation O Wenker, L Moehn, C Portera, G Walsh.. The Internet Journal of Radiology. 1999 Volume 1 Number
ISPUB.COM The Internet Journal of Radiology Volume 1 Number 1 O Wenker, L Moehn, C Portera, G Walsh Citation O Wenker, L Moehn, C Portera, G Walsh.. The Internet Journal of Radiology. 1999 Volume 1 Number
Summary of Operative Experience
 Summary of Operative Experience (Remarks: Programme Directors of respective Specialty Boards will conduct random check of the trainee s Logbook Summary and Logbook Summary Report against the operation
Summary of Operative Experience (Remarks: Programme Directors of respective Specialty Boards will conduct random check of the trainee s Logbook Summary and Logbook Summary Report against the operation
Clinical Management of Obscure- Overt Gastrointestinal Bleeding. Presented by Dr. 張瀚文
 Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
came from a carcinoma and in 12 from a sarcoma. Ninety lesions were intrapulmonary and the as the chest wall and pleura. Details of the primary
 Thorax 1982;37:366-370 Thoracic metastases MARY P SHEPHERD From the Thoracic Surgical Unit, Harefield Hospital, Harefield ABSTRACI One hundred and four patients are reviewed who were found to have thoracic
Thorax 1982;37:366-370 Thoracic metastases MARY P SHEPHERD From the Thoracic Surgical Unit, Harefield Hospital, Harefield ABSTRACI One hundred and four patients are reviewed who were found to have thoracic
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
2018 OCN Keywords January 22, 2018 Subject Area Weight Keywords
 Subject Area Weight Keywords Care Continuum 19% Care Continuum Coordination of Care Navigation Psychosocial Symptom Management Health Promotion/Screening and Early Detection Disease Prevention High-Risk
Subject Area Weight Keywords Care Continuum 19% Care Continuum Coordination of Care Navigation Psychosocial Symptom Management Health Promotion/Screening and Early Detection Disease Prevention High-Risk