A RANDOMISED, OPEN LABEL STUDY OF GUIDELINE DRIVEN TARGETED ANTIEMETIC THERAPY VERSUS SINGLE AGENT ANTIEMETIC THERAPY
|
|
|
- Amie Barrett
- 5 years ago
- Views:
Transcription

1
2 A RANDOMISED, OPEN LABEL STUDY OF GUIDELINE DRIVEN TARGETED ANTIEMETIC THERAPY VERSUS SINGLE AGENT ANTIEMETIC THERAPY Patsy Yates, Janet Hardy, Peter Martin, Jennifer Philip, Peter Hudson, David Currow, Geoff Mitchel, Helen Skerman, Paul Glare Queensland Univrsity of Technology, PaCCSC
3 In the last year of life 51% of cancer patients 27% of patients with non malignant disease experience nausea and vomiting
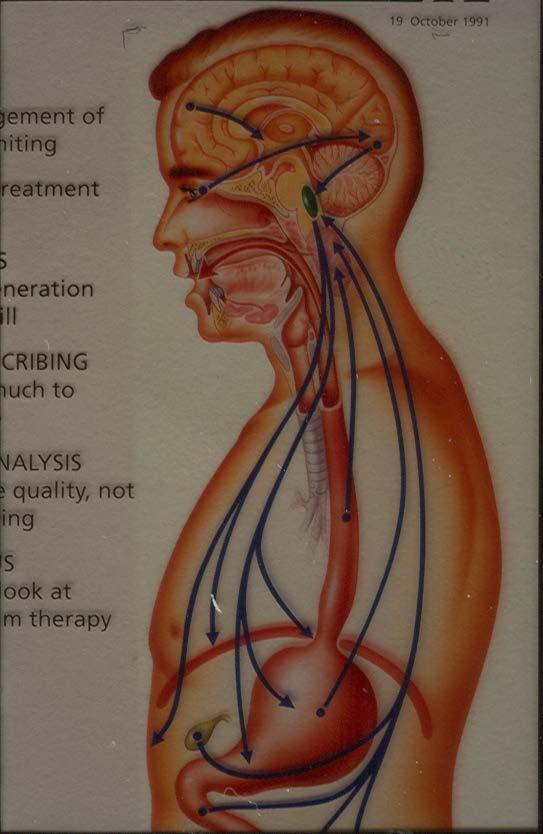
4 Common causes GI problems pharyngeal irritation drugs metabolic toxic brain metastases psychosomatic factors pain
5 Nausea and vomiting in patients with advanced disease often multifactorial often no obvious cause Kennett et al, 65 pts -mulifactorial 35 (56%) -unknown 22 (33%) -specific cause 6 (10%)
6 Correct reversible causes if possible severe pain infection cough hypercalcaemia tense ascites raised ICP stop emetogenic drugs
7 Non drug treatments control of malodour calm reassuring environment away from sight/smell of food small snacks someone else doing cooking complementary therapies/acupressure bands counselling

8
9
10 Drug approaches to emetic control 1. mechanistic or targeted - use patient s clinical picture to determine the likely pathophysiological abnormality - select antiemetic based on understanding of neuropharmacology
11
12 Receptor site affinities of selected anti-emetics D 2 antag H 1 antag ACh antag 5HT 2 antag 5HT 3 antag Metoclopromide (+) ++ Domperidone ++a Cisapride Ondansetron b Cyclizine Hyoscine hydrobromide 5HT 4 antag Haloperidol Prochlorperazine Chlorpromazine Levomepromazine
13
14
15 Mechanistic approach supported by 2 prospective audits -Bently, Pall med Lichter, J Pall Care1993 success claimed for 80-90% pts
16 Approaches to emetic control 2. empirical use any antiemetic without regard to underlying cause
17 Empirical approach trying various antiemetics without regard to underlying cause supported by Bruera, Bruera, Mystakidou, Corli (Glare, Supp Care Cancer 2004) success claimed for 80-90% pts 2 approaches had not been directly compared
18 Study details A randomised, open label study of guideline driven targeted antiemetic therapy versus single agent antiemetic therapy (haloperidol) Funding: NHMRC grant Sponsor: PACCSC (Flinders University) Nausea management program (NS1-3) Lead Investigators : Patsy Yates, Janet Hardy
19 Aim To determine whether guideline driven aetiology based anti-emetic therapy (targeted therapy) is more effective than single agent therapy with haloperidol in patients with cancer and nausea not related to anticancer therapy.
20 Treatment schedule: Guideline driven antiemetic therapy, given orally or parenterally (subcutaneous or intravenous), according to presumed cause of nausea using freely available PBS listed antiemetics in a 3 step dose escalation schedule or Haloperidol, in a 3 step dose escalation schedule from 1mg/24 hours to 3mg/24hours orally or parenterally (subcutaneously).
21 Definition of response: A minimum two point improvement from baseline and end score <3 on an 11 point NRS for average nausea for the previous 24 hours, measured 72 hours after the first study antiemetic administered. Primary endpoint: Response to treatment, defined as at least a two point improvement from baseline and a score < 3 for average nausea over the preceding 24 hours, measured at 72 hours using an 11-point (0-10) numeric rating scale.
22 Secondary endpoints best and worst nausea scores vomiting number of rescue antiemetic doses adverse events number treated at each dose level refractory nausea
23 Null hypothesis: For cancer patients with nausea, the response at 72 hours to aetiology based guideline driven antiemetics and haloperidol do not differ
24 Study population Patients who: are >18 years have a clinical diagnosis of cancer have nausea with an average score of 3 on an 11 point NRS are not currently receiving antiemetics or are already receiving antiemetics but these are inappropriate as defined by the antiemetic guidelines or are at a suboptimal dose are able to comply with all trial requirements are able to provide fully informed consent 24
25 Study population exclusions: nausea related to the treatment of cancer where acute treatment with 5HT3 antagonists is indicated nausea for which a specific antiemetic is indicated and randomisation to haloperidol would not be appropriate (e.g. dexamethasone for acutely raised ICP) undergone a procedure with the potential to affect nausea within 2 days prior to study or are likely to undergo a procedure or intervention with the potential to affect nausea during the 3 day study period
26 Exclusions (contd) unstable corticosteroids, within 48 hours prior to study definite contraindication to any of guideline drugs (Parkinson s disease, QTc prolongation, uncontrolled seizures) prior serious adverse event following any of the guideline drugs (dystonic reaction, neuroleptic malignant syndrome)
27 Clinical practice guidelines for the management of nausea (Modified from the original Glare CPGs according to expert consensus) 3 step treatment as determined by cause Code A B C D E F G H Dominant cause Central/ CTZ stimulation CNS disease Vestibular involvement Gastric stasis Ileus Mechanical obstruction Gastritis Cause undetermined (or multifactorial) 1. Glare P et al. Systematic review of the efficacy of antiemetics in the treatment of nausea in patients with far advanced cancer. Support Care Cancer 2004; 12:432-40
28 Dominant cause Treatment Step 1 Treatment Step 2 Treatment Step 3 A: Central/CTZ stimulation Prochlorperazine 5mg tds po or 25mg PR then 5mg tds po or 12.5mg bd IM/iv Haloperidol 1.5mg/24hrs po or sc Haloperidol 3mg/24hrs po or sc B: CNS disease Dex 8mg/24hrs po/sc/iv Dex 12mg/24hrs po/sc/iv Dex 16mg/24hrs po/sc/iv Clinical practice guidelines for the management of nausea C: Vestibular involvement Prochlorperazine 5mg tds po or 25mg PR then 5mg tds po or 12.5mg bd IM/iv Prochlorperazine 10mg tds po or 25mg PR then 10mg tds po or 12.5mg tds IM/iv Promethazine 25 mg tds po or 12.5mg sc then 10mg tds po D: Gastric stasis Metoclopramide 10mg qid po/sc/iv Metoclopramide 10mg Q4h po/sc/iv Metoclopramide 10mg Q4h po/sc/iv Dex 8mg/24hrs po/sc/iv E: Ileus Metoclopramide 10mg qid po/sc/iv F: Mechanical obstruction Haloperidol 1.5mg/24hrs po/sc Dex 8mg/24hrs po/sc/v Metoclopramide 10mg Q4h po/sc/iv Haloperidol 3mg/24hrs po/sc Dex 8mg/24hrs po/sc/iv Metoclopramide 10mg Q4h po/sc/iv Dexamethasone 8mg/24hrs po/sc/iv Haloperidol 3mg/24hrs po/sc Dex 8mg/24hrs po/sc/iv Hyoscine butylbromide 80mg/24hrs sc or Ranitidine 200mg/24hrs sc G: Gastritis Metoclopramide 10mg qid po/sc/iv PPI min dose H: Cause undetermined (or multifactorial) Metoclopramide 10mg qid po/sc/iv Metoclopramide 10mg qid po/sc/iv PPI max dose Metoclopramide 10mg qid po/sc/iv Haloperidol 1.5mg/24hrs po/sc Metoclopramide 10mg Q4h po/sc/iv PPI max dose Metoclopramide 10mg Q4h po/sc/iv Haloperidol 3mg/24hrs po/sc 28
29 Sample size a sample size of 75 per arm, after attrition, to detect a statistically significant difference in response of 25% between haloperidol and standard guidelines, with 90% power
30 Results (preliminary) 185 recruits between Oct 2010 and April F (69%) median age 70 yrs (28-91) most common cancers : breast, GI tract, lung, prostate median average nausea score at baseline: 5/10 median worst nausea score at baseline : 8/10 median baseline nausea interference score : 5/10 (range 0-10)
31 Results (preliiminary) 185 randomised 181 commenced study medication 152 participants (84%) completed the 3 planned days of treatment 7 withdrew because of unacceptable toxicty
32 Results preliminary, subject to change Randomisations Pre screened Randomised Completed Therapy arm distribution Therapy arm Guideline Haloperidol TOTAL Randomised Completed
33 Results preliminary data Dominant cause selected (missing data = 1) A B C D E F G H TOTA L * 23.2% 0.5% 3.2% 11.9% 7.0% 4.9% 3.8% 44.9% 100% Dominant cause A Central/ CTZ stimulation B CNS disease C Vestibular involvement D Gastric stasis E Ileus F Mechanical obstruction G Gastritis H Cause undetermined (or multifactorial)
34 CPG interim data If randomised to guideline therapy, which category? Category A B C D E F G H TOTAL Randomised % 0.0% 4.2% 12.6% 7.4% 4.2% 4.2% 38.9% 100.0% Dominant cause A Central/ CTZ stimulation B CNS disease C Vestibular involvement D Gastric stasis E Ileus F Mechanical obstruction G Gastritis H Cause undetermined (or multifactorial)
35 Response rate all randomised patients: 54% (targeted 55.8%, single agent 53.3%) completed 3 days: 65.1% (targeted 66.7%, single agent 63.5%)
36 Conclusion the response to antiemetic therapy was high in both arms guideline driven therapy did not result in greater control of nausea than single agent therapy with haloperidol regular use of currently available PBS-listed antiemetics results in good nausea control in the majority of patients
37 Nausea study 3 Nausea study 2 refractory N/V Nausea study 3 : Methotrimeprazine vs haloperidol 3 day study response: 2 point reduction in nausea score complete response: 2 point reduction in nausea score and final score <3/10 End point: response end day 3 Recruiting well

38
Hardy et al. BMC Cancer (2018) 18:510 https://doi.org/ /s
 18:510 https://doi.org/ /s") Hardy et al. BMC Cancer (2018) 18:510 https://doi.org/10.1186/s12885-018-4404-8 RESEARCH ARTICLE Open Access A randomized open-label study of guideline-driven antiemetic therapy versus single agent antiemetic
Hardy et al. BMC Cancer (2018) 18:510 https://doi.org/10.1186/s12885-018-4404-8 RESEARCH ARTICLE Open Access A randomized open-label study of guideline-driven antiemetic therapy versus single agent antiemetic
Nausea and Vomiting in Palliative Care
 Nausea and Vomiting in Palliative Care Definitions Nausea - an unpleasant feeling of the need to vomit Vomiting - the expulsion of gastric contents through the mouth, caused by forceful and sustained contraction
Nausea and Vomiting in Palliative Care Definitions Nausea - an unpleasant feeling of the need to vomit Vomiting - the expulsion of gastric contents through the mouth, caused by forceful and sustained contraction
We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients.
 We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients. The closing date for responses is 19th December The results
We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients. The closing date for responses is 19th December The results
Nausea & Vomiting. Dr Eve Lyn TAN Liverpool Hospital NSW, AUSTRALIA
 Nausea & Vomiting Dr Eve Lyn TAN Liverpool Hospital NSW, AUSTRALIA Prevalence prevalence varies *, systemic review 2007 : overall prevalence : nausea 30%, vomiting 20% in last 1-2 weeks of life : nausea
Nausea & Vomiting Dr Eve Lyn TAN Liverpool Hospital NSW, AUSTRALIA Prevalence prevalence varies *, systemic review 2007 : overall prevalence : nausea 30%, vomiting 20% in last 1-2 weeks of life : nausea
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
What else is new (other symptoms) DR ANDREW DAVIES
 DR ANDREW DAVIES") What else is new (other symptoms) DR ANDREW DAVIES Outline Nausea & vomiting Petroleum jelly (and oxygen) Nausea & vomiting MASCC / ESMO recommendations MASCC / ESMO recommendations General: The anti-emetic
What else is new (other symptoms) DR ANDREW DAVIES Outline Nausea & vomiting Petroleum jelly (and oxygen) Nausea & vomiting MASCC / ESMO recommendations MASCC / ESMO recommendations General: The anti-emetic
Palliative Patient in Emergency Department
 Palliative Patient in Emergency Department Dr Thiru Thirukkumaran Palliative Care Services NW THO Northwest Regional Hospital, Burnie Northwest Tasmania Outline the Session Introduction What is palliative
Palliative Patient in Emergency Department Dr Thiru Thirukkumaran Palliative Care Services NW THO Northwest Regional Hospital, Burnie Northwest Tasmania Outline the Session Introduction What is palliative
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Inpatient Palliative Medicine Update
 Inpatient Palliative Medicine Update David Dupere MD, FRCPC Head, Division of Palliative Medicine Department of Medicine QEII Health Sciences Centre Halifax, Nova Scotia Disclosures Book chapter in Compendium
Inpatient Palliative Medicine Update David Dupere MD, FRCPC Head, Division of Palliative Medicine Department of Medicine QEII Health Sciences Centre Halifax, Nova Scotia Disclosures Book chapter in Compendium
Updates in Chemotherapy-Induced Nausea and Vomiting (CINV) 2017
 2017") Updates in Chemotherapy-Induced Nausea and Vomiting (CINV) 2017 MELISSA C. MACKEY, PHARMD, BCPS, BCOP ONCOLOGY CLINICAL PHARMACIST DUKE UNIVERSITY HOSPITAL AUGUST 5, 2017 Objectives Review risk factors
Updates in Chemotherapy-Induced Nausea and Vomiting (CINV) 2017 MELISSA C. MACKEY, PHARMD, BCPS, BCOP ONCOLOGY CLINICAL PHARMACIST DUKE UNIVERSITY HOSPITAL AUGUST 5, 2017 Objectives Review risk factors
Syringe driver in Palliative Care
 Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Part 2: Pain and Symptom Management Nausea and Vomiting
 Part 2: Pain and Symptom Management Nausea and Vomiting Effective Date: February 22, 2017 Key Recommendations Select anti-nausea medication based on the etiology of the nausea and vomiting. Assessment
Part 2: Pain and Symptom Management Nausea and Vomiting Effective Date: February 22, 2017 Key Recommendations Select anti-nausea medication based on the etiology of the nausea and vomiting. Assessment
Symptom Management. Thomas McKain, MD, ABFM, ABHPM Medical Director
 Symptom Management Nausea & Vomiting Thomas McKain, MD, ABFM, ABHPM Medical Director Mr. Jones has nausea and vomiting. May I initiate Compazine from the Comfort Pak? Objectives 1. Delineate the Differential
Symptom Management Nausea & Vomiting Thomas McKain, MD, ABFM, ABHPM Medical Director Mr. Jones has nausea and vomiting. May I initiate Compazine from the Comfort Pak? Objectives 1. Delineate the Differential
Study No: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Antiemetics in chemotherapy
 Antiemetics in chemotherapy Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of submission Date
Antiemetics in chemotherapy Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of submission Date
Using syringe pumps in palliative care
 Using syringe pumps in palliative care Facilitator: Barbara Stone RN Ground rules Medication matching game Learning outcomes To identify the indications for using a syringe pump To discuss the general
Using syringe pumps in palliative care Facilitator: Barbara Stone RN Ground rules Medication matching game Learning outcomes To identify the indications for using a syringe pump To discuss the general
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
Algorithms for Symptom Management. In End of Life Care
 Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
9/20/2017. Effectively Managing Nausea and Vomiting. Disclosure. Objectives
 Effectively Managing Nausea and Myra Belgeri, Pharm.D, BCGP, BCPS, FASCP Clinical Pharmacist, Optum Hospice Pharmacy Services October 2017 1 Disclosure I have no relevant financial relationships with manufacturers
Effectively Managing Nausea and Myra Belgeri, Pharm.D, BCGP, BCPS, FASCP Clinical Pharmacist, Optum Hospice Pharmacy Services October 2017 1 Disclosure I have no relevant financial relationships with manufacturers
B.C. INTER-PROFESSIONAL PALLIATIVE SYMPTOM MANAGEMENT GUIDELINES
 B.C. INTER-PROFESSIONAL PALLIATIVE SYMPTOM MANAGEMENT GUIDELINES Copyright BC Centre for Palliative Care. 2017. 300-601 Sixth St. New Westminster, B.C. V3L 3C1. office@bc-cpc.ca please see Introduction
B.C. INTER-PROFESSIONAL PALLIATIVE SYMPTOM MANAGEMENT GUIDELINES Copyright BC Centre for Palliative Care. 2017. 300-601 Sixth St. New Westminster, B.C. V3L 3C1. office@bc-cpc.ca please see Introduction
Approach to Nausea & Vomi2ng
 Approach to Nausea & Vomi2ng Med 3 Seminar 2017 Dr. Robin Grant Division of Pallia2ve Medicine robin.grant@nshealth.ca Why nausea and vomi2ng? Pain 80-90+ % Fa2gue / asthenia 75-90% Cons2pa2on 70% Dyspnea
Approach to Nausea & Vomi2ng Med 3 Seminar 2017 Dr. Robin Grant Division of Pallia2ve Medicine robin.grant@nshealth.ca Why nausea and vomi2ng? Pain 80-90+ % Fa2gue / asthenia 75-90% Cons2pa2on 70% Dyspnea
Job title: Consultant Pharmacist/Advanced Practice Pharmacist
 Title : Guidelines for the Use of Antiemetics Purpose: To provide trust-wide guidance on the safe and effective use of antiemetics for the prevention and treatment of chemotherapy and radiotherapy induced
Title : Guidelines for the Use of Antiemetics Purpose: To provide trust-wide guidance on the safe and effective use of antiemetics for the prevention and treatment of chemotherapy and radiotherapy induced
Prevention of Antineoplastic Medication induced Nausea and Vomiting in Pediatric Cancer Patients
 Prevention of Antineoplastic Medication induced Nausea and Vomiting in Pediatric Cancer Patients Done by :Meznah Zaid Al-Mutairi Pharm.D Candidate PNU University College of Pharmacy Introduction Nausea
Prevention of Antineoplastic Medication induced Nausea and Vomiting in Pediatric Cancer Patients Done by :Meznah Zaid Al-Mutairi Pharm.D Candidate PNU University College of Pharmacy Introduction Nausea
End of life prescribing guidance
 End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
Managing Adverse Events in the Cancer Patient. Learning Objectives. Chemotherapy-Induced Nausea/Vomiting
 Managing Adverse Events in the Cancer Patient Lisa A Thompson, PharmD, BCOP Assistant Professor University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences Learning Objectives Describe
Managing Adverse Events in the Cancer Patient Lisa A Thompson, PharmD, BCOP Assistant Professor University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences Learning Objectives Describe
STEROID GUIDELINES AUDIT RESULTS
 STEROID GUIDELINES AUDIT RESULTS 27 patients were under active follow up between the audit dates. Notes for all these were audited. 59% (163) were not on steroids during this time 21% (57) were already
STEROID GUIDELINES AUDIT RESULTS 27 patients were under active follow up between the audit dates. Notes for all these were audited. 59% (163) were not on steroids during this time 21% (57) were already
SYRINGE DRIVER MEDICATIONS
 SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
End Stage Liver Disease Regional Audit Casenote Survey
 1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
Pancreatic cancer Palliative Care
 Pancreatic cancer Palliative Care Snežana Bošnjak Institute for Oncology and Radiology of Serbia Dept. Supportive Oncology & Pall Care Serbia, Belgrade Pancreatic Cancer: Palliative Care Abdominal / epigastric
Pancreatic cancer Palliative Care Snežana Bošnjak Institute for Oncology and Radiology of Serbia Dept. Supportive Oncology & Pall Care Serbia, Belgrade Pancreatic Cancer: Palliative Care Abdominal / epigastric
Guidelines for the Use of Anti-Emetics with Chemotherapy
 Guidelines for the Use of Anti-Emetics with The purpose of this document is to provide guidance on the rational use of anti-emetics for prevention and treatment of chemotherapy-induced nausea and vomiting
Guidelines for the Use of Anti-Emetics with The purpose of this document is to provide guidance on the rational use of anti-emetics for prevention and treatment of chemotherapy-induced nausea and vomiting
Doncaster & Bassetlaw Cancer Locality. Palliative Care Core Formulary
 Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
Palliative Care. Pocketbook 4
 Nottinghamshire STP EOL Programme Board 2019 Review 2022 Palliative Care Pocketbook 4 Contents Pain Guidelines page 2 Nausea and Vomiting page 9 Inoperable Bowel Obstruction page 10 Constipation page 11
Nottinghamshire STP EOL Programme Board 2019 Review 2022 Palliative Care Pocketbook 4 Contents Pain Guidelines page 2 Nausea and Vomiting page 9 Inoperable Bowel Obstruction page 10 Constipation page 11
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Nausea and Vomiting. Principles and Practice in End of Life Care November 2018
 Nausea and Vomiting Principles and Practice in End of Life Care November 2018 Overview Aims and Objectives Why is managing nausea and vomiting important? Definitions Causes Interventions pharmacological
Nausea and Vomiting Principles and Practice in End of Life Care November 2018 Overview Aims and Objectives Why is managing nausea and vomiting important? Definitions Causes Interventions pharmacological
Acute management of in-patient Parkinson s Disease patients
 Acute management of in-patient Parkinson s Disease patients Contents Pages Introduction and Admission advice 2 Nil by Mouth Guidance 3 5 Complex therapy advice (Apomorphine, DBS, Duodopa) 6 Surgical peri-operative
Acute management of in-patient Parkinson s Disease patients Contents Pages Introduction and Admission advice 2 Nil by Mouth Guidance 3 5 Complex therapy advice (Apomorphine, DBS, Duodopa) 6 Surgical peri-operative
Trust Guideline for Prevention and Control of Chemotherapy and Radiotherapy Induced Nausea and Vomiting in Adults
 A Clinical Guideline For Use in: Organisation-wide By: For: Key words: Name of document author: Job title of document author: Name of document author s Line Manager: Job title of author s Line Manager:
A Clinical Guideline For Use in: Organisation-wide By: For: Key words: Name of document author: Job title of document author: Name of document author s Line Manager: Job title of author s Line Manager:
Management of Nausea and Vomiting
 June 01, 2015 By Rudolph M. Navari, MD, PhD, FACP [1] Although marked progress in controlling chemotherapy-induced emesis has occurred over the past 25 years, nausea and vomiting remain among the most
June 01, 2015 By Rudolph M. Navari, MD, PhD, FACP [1] Although marked progress in controlling chemotherapy-induced emesis has occurred over the past 25 years, nausea and vomiting remain among the most
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
Gastroparesis and other upper GI problems DR ANDREW DAVIES
 Gastroparesis and other upper GI problems DR ANDREW DAVIES Outline Gastroparesis Hiccoughs Gastroparesis Gastroparesis Definition: A syndrome of objectively delayed gastric emptying in the absence of mechanical
Gastroparesis and other upper GI problems DR ANDREW DAVIES Outline Gastroparesis Hiccoughs Gastroparesis Gastroparesis Definition: A syndrome of objectively delayed gastric emptying in the absence of mechanical
Palliative Care Emergencies. Additional module if needed
 Palliative Care Emergencies Additional module if needed Learning objectives Understand emergency /urgent / important Describe common emergencies in PC Explore principles of essential management Outline
Palliative Care Emergencies Additional module if needed Learning objectives Understand emergency /urgent / important Describe common emergencies in PC Explore principles of essential management Outline
West of Scotland Cancer Network Guideline for Managing Chemotherapy Induced Nausea and Vomiting
 West of Scotland Cancer Network Guideline for Managing Chemotherapy Induced Nausea and Vomiting Definitions Acute nausea and vomiting Delayed nausea and vomiting Anticipatory nausea and vomiting Initial
West of Scotland Cancer Network Guideline for Managing Chemotherapy Induced Nausea and Vomiting Definitions Acute nausea and vomiting Delayed nausea and vomiting Anticipatory nausea and vomiting Initial
Drug Class Review on Newer Antiemetics
 Drug Class Review on Newer Antiemetics Final Report January 2006 A literature scan of this topic is done periodically The purpose of this report is to make available information regarding the comparative
Drug Class Review on Newer Antiemetics Final Report January 2006 A literature scan of this topic is done periodically The purpose of this report is to make available information regarding the comparative
Clinical Policy: Ondansetron (Zuplenz) Reference Number: CP.PMN.45 Effective Date: Last Review Date: Line of Business: Medicaid
 Reference Number: CP.PMN.45 Effective Date: Last Review Date: Line of Business: Medicaid") Clinical Policy: (Zuplenz) Reference Number: CP.PMN.45 Effective Date: 09.01.06 Last Review Date: 02.19 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Zuplenz) Reference Number: CP.PMN.45 Effective Date: 09.01.06 Last Review Date: 02.19 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
BJF Acute Pain Team Formulary Group
 Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Clatterbridge Centre for Oncology
 Clatterbridge Centre for Oncology CONTENTS 1. Why and when to use a syringe driver 2. Siting the syringe driver 3. Mixing and measuring 4. Setting up the syringe driver 5. Drug information 6. Common problems
Clatterbridge Centre for Oncology CONTENTS 1. Why and when to use a syringe driver 2. Siting the syringe driver 3. Mixing and measuring 4. Setting up the syringe driver 5. Drug information 6. Common problems
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life
 MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
TRANSPARENCY COMMITTEE OPINION. 31 January Date of marketing authorisation: 22 March 2005 (centralised marketing authorisation)
") The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 31 January 2007 ALOXI 250 µg solution for injection B/1 CIP 375,482-8 Applicant: THERABEL LUCIEN PHARMA palonosetron
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 31 January 2007 ALOXI 250 µg solution for injection B/1 CIP 375,482-8 Applicant: THERABEL LUCIEN PHARMA palonosetron
PERUGIA INTERNATIONAL CANCER CONFERENCE VII MULTINATIONAL ASSOCIATION FOR SUPPORTIVE CARE IN CANCER
 June 2004 PERUGIA INTERNATIONAL CANCER CONFERENCE VII MULTINATIONAL ASSOCIATION FOR SUPPORTIVE CARE IN CANCER CONSENSUS CONFERENCE ON ANTIEMETIC THERAPY PERUGIA, March 29-31, 2004 DELAYED EMESIS WORKING
June 2004 PERUGIA INTERNATIONAL CANCER CONFERENCE VII MULTINATIONAL ASSOCIATION FOR SUPPORTIVE CARE IN CANCER CONSENSUS CONFERENCE ON ANTIEMETIC THERAPY PERUGIA, March 29-31, 2004 DELAYED EMESIS WORKING
CLINICAL GUIDANCE FOR THE PREVENTION AND MANAGEMENT OF CHEMOTHERAPY AND RADIOTHERAPY INDUCED NAUSEA AND VOMITING IN ADULTS
 CLINICAL GUIDANCE FOR THE PREVENTION AND MANAGEMENT OF CHEMOTHERAPY AND RADIOTHERAPY INDUCED NAUSEA AND VOMITING IN ADULTS Procedure reference: Document owner: 2196 Version: V2.1 Robert Duncombe, The Director
CLINICAL GUIDANCE FOR THE PREVENTION AND MANAGEMENT OF CHEMOTHERAPY AND RADIOTHERAPY INDUCED NAUSEA AND VOMITING IN ADULTS Procedure reference: Document owner: 2196 Version: V2.1 Robert Duncombe, The Director
Symptom Management Pocket Guides: DELIRIUM
 Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
10/08/59 CAUSES OF BOWEL OBSTRUCTION IN MALIGNANCY INCIDENCE OF BOWEL OBSTRUCTION BEWARE! SYMPTOM PROFILE RADIOLOGY
 MANAGEMENT OF MALIGNANT BOWEL OBSTRUCTION PALLIATIVE CARE IN ONCOLOGY 2016 A/Professor Ghauri Aggarwal FRACP, FAChPM, FFPMANZCA Palliative Medicine Physician Sydney, Australia INCIDENCE OF BOWEL OBSTRUCTION
MANAGEMENT OF MALIGNANT BOWEL OBSTRUCTION PALLIATIVE CARE IN ONCOLOGY 2016 A/Professor Ghauri Aggarwal FRACP, FAChPM, FFPMANZCA Palliative Medicine Physician Sydney, Australia INCIDENCE OF BOWEL OBSTRUCTION
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Palliative Care. Anticipatory Prescribing Guidelines & June Gippsland Region Palliative Care Consortium Clinical Practice Group
 Palliative Care Anticipatory Prescribing Guidelines June 2016 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy No. Title Keywords Ratified GRPCC-CPG008_1.1_2016 Anticipatory Prescribing
Palliative Care Anticipatory Prescribing Guidelines June 2016 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy No. Title Keywords Ratified GRPCC-CPG008_1.1_2016 Anticipatory Prescribing
CLINICAL GUIDELINE FOR ANTIEMETIC USE IN PAEDIATRIC ONCOLOGY 1. Aim/Purpose of this Guideline
 CLINICAL GUIDELINE FOR ANTIEMETIC USE IN PAEDIATRIC ONCOLOGY 1. Aim/Purpose of this Guideline 1.1. This guideline applies to medical and nursing staff working with paediatric oncology patients. 2. The
CLINICAL GUIDELINE FOR ANTIEMETIC USE IN PAEDIATRIC ONCOLOGY 1. Aim/Purpose of this Guideline 1.1. This guideline applies to medical and nursing staff working with paediatric oncology patients. 2. The
Respiratory Secretions. Care in the last 72 hours of life Paul Tait, pharmacist
 Respiratory Secretions Care in the last 72 hours of life Paul Tait, pharmacist 50% Why? Inability to swallow & clear secretions Ineffective cough Reduced consciousness Pooling of secretions in the throat
Respiratory Secretions Care in the last 72 hours of life Paul Tait, pharmacist 50% Why? Inability to swallow & clear secretions Ineffective cough Reduced consciousness Pooling of secretions in the throat
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Anzemet) Reference Number: CP.PMN.141 Effective Date: 09.01.06 Last Review Date: 08.18 Line of Business: Commercial, HIM, Medicaid Revision Log See Important Reminder at the end of this
Clinical Policy: (Anzemet) Reference Number: CP.PMN.141 Effective Date: 09.01.06 Last Review Date: 08.18 Line of Business: Commercial, HIM, Medicaid Revision Log See Important Reminder at the end of this
This survey aims to look at individual practice and can be completed by any healthcare professional.
 This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
Grace Ma and Andrea Weiss FMF 2018
 Grace Ma and Andrea Weiss FMF 2018 Presenter: Grace Ma Relationships with financial sponsors: none Presenter: Andrea Weiss Relationships with financial sponsors: none This program has not received any
Grace Ma and Andrea Weiss FMF 2018 Presenter: Grace Ma Relationships with financial sponsors: none Presenter: Andrea Weiss Relationships with financial sponsors: none This program has not received any
EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
ALLERGIES/ SENSITIVITIES This section must be completed before prescribing/administering any drug
 COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
DOMPERIDONE BNF 4.6. Domperidone is a dopamine type 2-receptor antagonist. It is structurally related to the
 DOMPERIDONE BNF 4.6 Class: Prokinetic anti-emetic. Indications: Nausea and vomiting, dysmotility dyspepsia, gastro-oesophageal reflux. Pharmacology Domperidone is a dopamine type 2-receptor antagonist.
DOMPERIDONE BNF 4.6 Class: Prokinetic anti-emetic. Indications: Nausea and vomiting, dysmotility dyspepsia, gastro-oesophageal reflux. Pharmacology Domperidone is a dopamine type 2-receptor antagonist.
Drug: Aprepitant (Emend ) Date of Review: 4/01/10
 Date of Review: 4/01/10") CAMBRIDGESHIRE JOINT PRESCRIBING GROUP Business Case Evaluation and Recommendation Document Drug: Aprepitant (Emend ) Date of Review: 4/01/10 Business Case Decision and date: DOUBLE RED, 20 January 2010
CAMBRIDGESHIRE JOINT PRESCRIBING GROUP Business Case Evaluation and Recommendation Document Drug: Aprepitant (Emend ) Date of Review: 4/01/10 Business Case Decision and date: DOUBLE RED, 20 January 2010
The last days of life in hospital and at home
 The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
ATTUALITÀ NEL CONTROLLO DELL EMESI
 ATTUALITÀ NEL CONTROLLO DELL EMESI Dr Claudio Lotesoriere Dipartimento di Oncoematologia S.C. di Oncologia Medica P.O. San G. Moscati TARANTO email oncologia.taranto@gmail.com Types of CINV: Definitions
ATTUALITÀ NEL CONTROLLO DELL EMESI Dr Claudio Lotesoriere Dipartimento di Oncoematologia S.C. di Oncologia Medica P.O. San G. Moscati TARANTO email oncologia.taranto@gmail.com Types of CINV: Definitions
CONSORT 2010 checklist of information to include when reporting a randomised trial*
 Supplemental Figures for: Ramosetron Versus Ondansetron in Combination with Aprepitant and Dexamethasone for the Prevention of Highly Emetogenic Chemotherapy-induced Nausea and Vomiting: A Multicenter,
Supplemental Figures for: Ramosetron Versus Ondansetron in Combination with Aprepitant and Dexamethasone for the Prevention of Highly Emetogenic Chemotherapy-induced Nausea and Vomiting: A Multicenter,
Five Centers of Nausea. Linda Tavel, MD Program Medical Director VistaCare Hospice
 Five Centers of Nausea Linda Tavel, MD Program Medical Director VistaCare Hospice Objectives Prevalence of nausea and vomiting Anatomic and physiologic paths to nausea Evaluation of nausea Treatment of
Five Centers of Nausea Linda Tavel, MD Program Medical Director VistaCare Hospice Objectives Prevalence of nausea and vomiting Anatomic and physiologic paths to nausea Evaluation of nausea Treatment of
Pediatric Trials 23/04/2018. Disclosures. Nausea and Vomiting Control in Adults and Children: Mind the Gap! Learning Objectives
 Nausea and Vomiting Control in Adults and Children: Mind the Gap! Disclosures No relevant conflicts of interest Lee Dupuis, RPh, PhD May 5, 2018 2 Learning Objectives At the end of this presentation, attendees
Nausea and Vomiting Control in Adults and Children: Mind the Gap! Disclosures No relevant conflicts of interest Lee Dupuis, RPh, PhD May 5, 2018 2 Learning Objectives At the end of this presentation, attendees
Long Term Care Formulary HCD - 08
 1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
Medications used for symptom control in palliative care
 Learning Objectives used for symptom control in palliative care Luis Viana, R. Ph., M.Ed., CGP 1. For common symptoms experienced by the person managed with palliative care: Recognize the symptom to be
Learning Objectives used for symptom control in palliative care Luis Viana, R. Ph., M.Ed., CGP 1. For common symptoms experienced by the person managed with palliative care: Recognize the symptom to be
Symptom Control in Heart Failure. Dr Claire L Hookey
 Symptom Control in Heart Failure Dr Claire L Hookey Heart Failure symptoms Class III/IV CHF, mean 67.1 years, mean EF 22.3% Most prevalent symptoms:- lack of energy (66%) dry mouth (62%) shortness of breath
Symptom Control in Heart Failure Dr Claire L Hookey Heart Failure symptoms Class III/IV CHF, mean 67.1 years, mean EF 22.3% Most prevalent symptoms:- lack of energy (66%) dry mouth (62%) shortness of breath
Vomiting Approach to diagnosis
 Vomiting Approach to diagnosis By Dr. Sahar El-Gharabawy Associate professor of internal medicine Hepato-gastroenterology Unit )SMH ) Mansoura University Definitions: Nausea: Feeling "sick to the stomach",
Vomiting Approach to diagnosis By Dr. Sahar El-Gharabawy Associate professor of internal medicine Hepato-gastroenterology Unit )SMH ) Mansoura University Definitions: Nausea: Feeling "sick to the stomach",
Nausea. Assessment & Management. R J Crossno, MD, CMD, FAAFP, FAAHPM. Disclosures
 Nausea Assessment & Management R J Crossno, MD, CMD, FAAFP, FAAHPM Disclosures Dr. Crossno discloses his employment as Area Medical Director for VistaCare VistaCare has provided commercial support for
Nausea Assessment & Management R J Crossno, MD, CMD, FAAFP, FAAHPM Disclosures Dr. Crossno discloses his employment as Area Medical Director for VistaCare VistaCare has provided commercial support for
Clinical Policy: Nabilone (Cesamet) Reference Number: ERX.NPA.35 Effective Date:
 Reference Number: ERX.NPA.35 Effective Date:") Clinical Policy: (Cesamet) Reference Number: ERX.NPA.35 Effective Date: 09.01.17 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Cesamet) Reference Number: ERX.NPA.35 Effective Date: 09.01.17 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Using a Simple Diary for Management of Nausea and Vomiting During Chemotherapy
 Using a Simple Diary for Management of Nausea and Vomiting During Chemotherapy Problem identification Nausea and vomiting (N&V) are frequent complications following chemotherapy, even when taking 5-HT3
Using a Simple Diary for Management of Nausea and Vomiting During Chemotherapy Problem identification Nausea and vomiting (N&V) are frequent complications following chemotherapy, even when taking 5-HT3
Disclosures 9/17/2018. Best Practices in the Treatment of Nausea and Vomiting
 Best Practices in the Treatment of Nausea and Vomiting Jennifer Gabbard, MD Wake Forest School of Medicine jgabbard@wakehealth.edu 42 nd Annual Hospice & Palliative Care Conference September 2018 Charlotte,
Best Practices in the Treatment of Nausea and Vomiting Jennifer Gabbard, MD Wake Forest School of Medicine jgabbard@wakehealth.edu 42 nd Annual Hospice & Palliative Care Conference September 2018 Charlotte,
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Isle of Wight Syringe Driver Compatibility Guidelines
 Isle of Wight Syringe Driver Compatibility Guidelines Produced by The Earl Mountbatten Hospice, Isle of Wight Written January 2015, revision due January 2018 This guideline is available as a paper pocketbook
Isle of Wight Syringe Driver Compatibility Guidelines Produced by The Earl Mountbatten Hospice, Isle of Wight Written January 2015, revision due January 2018 This guideline is available as a paper pocketbook
Palliative care for patients with brain cancer
 Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Clinical Policy: Dolasetron (Anzemet) Reference Number: ERX.NPA.83 Effective Date:
 Reference Number: ERX.NPA.83 Effective Date:") Clinical Policy: (Anzemet) Reference Number: ERX.NPA.83 Effective Date: 09.01.18 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Anzemet) Reference Number: ERX.NPA.83 Effective Date: 09.01.18 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
CHEMOTHERAPY-INDUCED NAUSEA AND VOMITING
 CHEMOTHERAPY-INDUCED NAUSEA AND VOMITING Jennifer Shamai MS, RN, AOCNS, BMTCN Professional Practice Leader Department of Clinical Practice And Professional Education Click How to the edit Experts Master
CHEMOTHERAPY-INDUCED NAUSEA AND VOMITING Jennifer Shamai MS, RN, AOCNS, BMTCN Professional Practice Leader Department of Clinical Practice And Professional Education Click How to the edit Experts Master
European Medicines Agency
 European Medicines Agency SCIENTIFIC DISCUSSION 1. Introduction Emend is an oral substance P, aka human neurokinin 1 (NK-1)-receptor antagonist. Mammalian tachykinin substance P (SP) that binds to the
European Medicines Agency SCIENTIFIC DISCUSSION 1. Introduction Emend is an oral substance P, aka human neurokinin 1 (NK-1)-receptor antagonist. Mammalian tachykinin substance P (SP) that binds to the
Prevention and Management of cancer disease and of chemo-and radiotherapyinduced nausea and vomiting
 Prevention and Management of cancer disease and of chemo-and radiotherapyinduced nausea and vomiting Focusing on the updated MASCC/ESMO guidelines Karin Jordan Department of Hematology and Oncology, University
Prevention and Management of cancer disease and of chemo-and radiotherapyinduced nausea and vomiting Focusing on the updated MASCC/ESMO guidelines Karin Jordan Department of Hematology and Oncology, University
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
ESMO HIGHLIGHTS SUPPORTIVE AND PALLIATIVE CARE
 ESMO 2016 - HIGHLIGHTS SUPPORTIVE AND PALLIATIVE CARE FLORIAN SCOTTE Cancer Department Supportive Care in Cancer Unit Georges Pompidou European Hospital Paris France esmo.org DISCLOSURE SLIDE Consultant
ESMO 2016 - HIGHLIGHTS SUPPORTIVE AND PALLIATIVE CARE FLORIAN SCOTTE Cancer Department Supportive Care in Cancer Unit Georges Pompidou European Hospital Paris France esmo.org DISCLOSURE SLIDE Consultant
Drug Name: Aprepitant (Emend ) Manufacturer: Merck & Co., Inc.
 Manufacturer: Merck & Co., Inc.") Drug Name: Aprepitant (Emend ) Manufacturer: Merck & Co., Inc. Pharmacology: Aprepitant (previously known as MK-0839 and L-754030) is a new molecular entity that is the first in a new therapeutic class,
Drug Name: Aprepitant (Emend ) Manufacturer: Merck & Co., Inc. Pharmacology: Aprepitant (previously known as MK-0839 and L-754030) is a new molecular entity that is the first in a new therapeutic class,
Incidence and aetiology:
 A pilot randomised cross-over double blinded controlled efficacy study of Octreotide versus hyoscine hydrobromide in controlling respiratory secretions at the end of life Katherine Clark, David Currow,
A pilot randomised cross-over double blinded controlled efficacy study of Octreotide versus hyoscine hydrobromide in controlling respiratory secretions at the end of life Katherine Clark, David Currow,
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth)
") Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
FINAL CDEC RECOMMENDATION
 FINAL CDEC RECOMMENDATION PALONOSETRON CAPSULE (Aloxi Eisai Limited) Indication: Chemotherapy-Induced Nausea and Vomiting Recommendation: The Canadian Drug Expert Committee (CDEC) recommends that oral
FINAL CDEC RECOMMENDATION PALONOSETRON CAPSULE (Aloxi Eisai Limited) Indication: Chemotherapy-Induced Nausea and Vomiting Recommendation: The Canadian Drug Expert Committee (CDEC) recommends that oral
DECONTAMINATION AGENTS and ANTIEMETICS *** This material won t be covered in lecture, but you are responsible for it***
 Decontamination and Antiemetics Med 5724 Page 1 of 8 DECONTAMINATION AGENTS and ANTIEMETICS *** This material won t be covered in lecture, but you are responsible for it*** REFERENCES: Katzung (9th ed.)
Decontamination and Antiemetics Med 5724 Page 1 of 8 DECONTAMINATION AGENTS and ANTIEMETICS *** This material won t be covered in lecture, but you are responsible for it*** REFERENCES: Katzung (9th ed.)
Gastrointestinal obstruction Dr Iain Lawrie
 Gastrointestinal obstruction Dr Iain Lawrie Consultant and Honorary Clinical Senior Lecturer in Palliative Medicine The Pennine Acute Hospitals NHS Trust / The University of Manchester iain.lawrie@pat.nhs.uk
Gastrointestinal obstruction Dr Iain Lawrie Consultant and Honorary Clinical Senior Lecturer in Palliative Medicine The Pennine Acute Hospitals NHS Trust / The University of Manchester iain.lawrie@pat.nhs.uk
ECN Protocol Book. Antiemetic Guidelines for Adult Patients Receiving Chemotherapy and Radiotherapy
 ECN Protocol Book Antiemetic Guidelines f Adult Patients Receiving Chemotherapy and Radiotherapy Name of person presenting document: Reason f document development: Names of development team: Specify groups
ECN Protocol Book Antiemetic Guidelines f Adult Patients Receiving Chemotherapy and Radiotherapy Name of person presenting document: Reason f document development: Names of development team: Specify groups
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
Management of Chemotherapy Induced Nausea/Vomiting(CINV) in Adult Cancer Patients
 in Adult Cancer Patients") Management of Chemotherapy Induced Nausea/Vomiting(CINV) in Adult Cancer Patients By Zahra Shaghaghi, Pharm-D, BCOP, PhC Prepared for 2018 NMSHP Balloon Fiesta Symposium Goals and Objectives: Describe
Management of Chemotherapy Induced Nausea/Vomiting(CINV) in Adult Cancer Patients By Zahra Shaghaghi, Pharm-D, BCOP, PhC Prepared for 2018 NMSHP Balloon Fiesta Symposium Goals and Objectives: Describe