What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden
|
|
|
- Esther Cunningham
- 5 years ago
- Views:
Transcription
 Serous Clear cell Immunohistochemistry Rarer tumours Diagnostic difficulties Staging problems Other important")
 Risk factors oestrogen++, insulin resistance, LS Wide variation in")
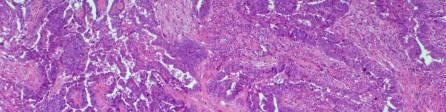
1 What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common) Serous Clear cell Immunohistochemistry Rarer tumours Diagnostic difficulties Staging problems Other important considerations when reporting uterine carcinomas Endometrioid adenocarcinoma I have no conflicts of interest to declare Grade 1-2 is the archetypal low grade uterine carcinoma Arises from atypical hyperplasia (complex atypical hyperplasia/ein) Risk factors oestrogen++, insulin resistance, LS Wide variation in morphology 1


 Kendall et al, AJSP 1998 Most useful criteria: Glandular confluence Stromal alterations")
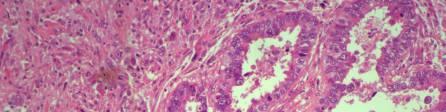
2 Differentiating hyperplasia from G1 endometrioid adenocarcinoma Differentiating atypical hyperplasia from G1 endometrioid adenocarcinoma In the absence of myometrial invasion (biopsy, endometriumconfined 1A cancers), diagnosis of adenocarcinoma is based on architecture Interobserver variation has been shown to be low in diagnosis of G1 endometrioid adenocarcinoma by expert gynae pathologists (kappa value = 0.83) Kendall et al, AJSP 1998 Most useful criteria: Glandular confluence Stromal alterations Assessment of atypia in hyperplasia was the most difficult area Longacre et al, AJSP 1995; 19:








3 Endometrioid adenocarcinoma variants (WHO 2014) Squamous differentiation Secretory variant Villoglandular variant Ciliated cell variant Mucinous carcinoma >50% DPAS+ intracytoplasmic mucin?higher rate of pelvic nodal metastases but no difference in overall survival (Rauh-Hain et al, Am J Clin Onc. 2016) 3



")



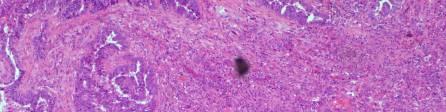
4 MELF (Microcystic, elongated and fragmented) Particular pattern of invasion in endometrioid adenocarcinomas (generally low grade) Typical morphology Associated with lymphovascular space invasion Can be difficult to delineate (single/small groups of cells overlooked) AE1/3 ER Adenoma malignum pattern 4







5 Grading endometrioid adenocarcinoma FIGO GRADING SYSTEM Grade 1 = <5% solid Grade 2 = 5-50% solid Grade 3 = >50% solid Caveat 1: Don t include morular/squamous differentiation Caveat 2: Marked nuclear atypia upgrades by one 5
6 Immunohistochemistry of endometrioid adenocarcinoma Immunohistochemistry of endometrioid adenocarcinoma p53 wild-type p16 p53 wild-type p16 Immunohistochemistry of endometrioid adenocarcinoma Immunohistochemistry of endometrioid adenocarcinoma Mismatch repair immunohistochemistry more later p53 wild-type p16 p53 wild-type p16 6

 Generally seen in")

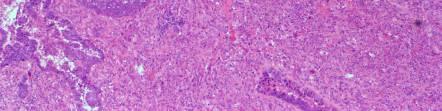
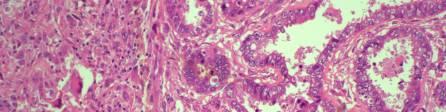
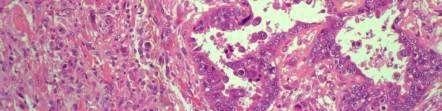
7 Uterine serous carcinoma Precursor lesion is endometrial intraepithelial carcinoma May be associated with BRCA mutation (de Jonge et al, EJC 2017) Generally seen in atrophic background (Usually) the epithelial component of carcinosarcoma Morphology EIC 7




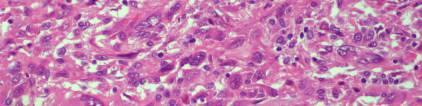
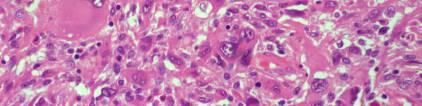
8 Immunohistochemistry p53 Carcinosarcoma A biphasic tumour in which the epithelial component has undergone epithelial to mesenchymal transition (usually) The sarcomatous component can be homologous or heterologous Rhabdomyosarcoma Chondrosarcoma Liposarcoma May be useful to comment on the proportion of adenocarcinoma:sarcoma Comment on the composition of any metastatic deposits usually epithelial unless there is extensive rhabdomyosarcomatous differentiation Immunohistochemistry cont 8

9 9

 Report all histological subtypes in main body of report, especially if there is a minor high")
10 Rare (1-5% of all uterine carcinomas) May be associated with Lynch syndrome Aggressive Clear cell carcinoma Other rare types Undifferentiated/dedifferentiated carcinoma Mesonephric carcinoma Squamous cell carcinoma Neuroendocrine carcinoma Peripheral neuroectodermal tumour Choriocarcinoma Immunohistochemistry Mixed carcinomas p53 wild-type WT1 negative ER negative Patchy or block p16 Napsin often positive (less reliable than in the ovary) E.g. mixed serous and endometrioid There should be at least 10% of the second component (WHO 2014) Report all histological subtypes in main body of report, especially if there is a minor high grade component Consider underlying genetic abnormality such as MMR deficiency in cases which are difficult to classify 10
11 Diagnostic difficulties (subtyping) IA/IB problems Immunohistochemistry can help with: Differentiating endometrioid from serous subtypes (usually) Differentiating serous from clear cell Identifying rhabdomyosarcoma in carcinosarcoma Immunohistochemistry is not useful for: Differentiating atypical hyperplasia from Grade 1 endometrioid carcinoma Grading endometrioid carcinoma Smooth muscle metaplasia within the exophytic part of the tumour can mimic myometrium Myometrium may be thinned due to compression by slow-growing tumour Tumour in the cornua Adenomyosis Problems with staging/reporting What problems? It s so simple! Where does the inner half end? How do you assess cervical stromal invasion? Does cervical glandular involvement matter? Does this tumour in the ovary represent metastatic carcinoma or a synchronous primary? When is LVSI not LVSI? Tips Tumour by the arcuate vascular plexus indicates outer half Try to find tumour adjacent to uninvolved endometrium for accuracy Rounded edges may suggest adenomyosis 11



12 Lymphovascular space invasion Cervical stromal invasion Longitudinal sections of cervix/lus are most helpful for accurate detection Pseudovascular space invasion Robotic and laparoscopic surgery uterine manipulation Glandular involvement does not upstage but may direct adjuvant treatment (depends on centre) 12

13 Metastasis versus Synchronous primaries endometrioid adenocarcinoma Evaluated 18 organ-confined synchronous ovarian/endometrial low-grade endometrioid adenocarcinomas 17/18 demonstrated a clonal relationship Scully criteria (in the absence of routine genomic sequencing (!) include: histological dissimilarity, no LVSI, superficial myometrial invasion, evidence of precursor lesions (atypical hyperplasia/ovarian endometriosis) Pseudovascular space invasion Metastasis versus synchronous primaries serous carcinoma Kommoss et al, AJSP 2017: Uterine serous carcinomas can metastasise to tubal epithelium and mimic STIC Useful IHC to differentiate includes p53 if divergent patterns (early driving mutation), WT1, ER Caveat: the reverse can occur (ovarian/tubal primary with secondary uterine involvement) 13


14 Other considerations Tumour size >25mm was a risk factor for local recurrence How to assess? How to report? Significance of ITCs? Other considerations Sentinel lymph node sampling Mismatch repair immunohistochemistry Who to target? Biopsies or resections? How to interpret? Which patterns are most significant? 14

15 Mismatch repair continued Take home messages Mutation Loss of expression (IHC) Significance MLH1 MLH1, PMS2 Sporadic (approximately 50%, promoter methylation), remainder LS PMS2 PMS2 Usually LS MSH2 MSH2, MSH6 Usually LS MSH6 MSH6 Rarest, usually LS Criteria can be applied to make differentiation between atypical hyperplasia and G1 endometrioid adenocarcinoma more robust and reproducible Staging can be difficult and is crucial for determining adjuvant treatment Consider your policy for mismatch repair testing Thank you! Questions? Helpful reference: Pathologic Staging of EndometrialCarcinomas: Selected Areas of Difficulty. McCluggage WG. Adv Anat Pathol Mar;25(2): doi: /PAP PMID:
Atypical Hyperplasia/EIN
 EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas. W Glenn McCluggage Belfast, Northern Ireland
 The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas W Glenn McCluggage Belfast, Northern Ireland Enterprise Interest None OVARIAN SEROUS CARCINOMA (OSC) RECENT DEVELOPMENTS
The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas W Glenn McCluggage Belfast, Northern Ireland Enterprise Interest None OVARIAN SEROUS CARCINOMA (OSC) RECENT DEVELOPMENTS
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus
 Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience
 Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Index. B Bilateral salpingo-oophorectomy (BSO), 69
, 69") A Advanced stage endometrial cancer diagnosis, 92 lymph node metastasis, 92 multivariate analysis, 92 myometrial invasion, 92 prognostic factors FIGO stage, 94 histological grade, 94, 95 histologic cell
A Advanced stage endometrial cancer diagnosis, 92 lymph node metastasis, 92 multivariate analysis, 92 myometrial invasion, 92 prognostic factors FIGO stage, 94 histological grade, 94, 95 histologic cell
Standards and datasets for reporting cancers. Dataset for histological reporting of endometrial cancer. December 2017
 Standards and datasets for reporting cancers Dataset for histological reporting of endometrial cancer December 2017 Authors: Dr Raji Ganesan, Birmingham Women s NHS Foundation Trust Dr Naveena Singh, Barts
Standards and datasets for reporting cancers Dataset for histological reporting of endometrial cancer December 2017 Authors: Dr Raji Ganesan, Birmingham Women s NHS Foundation Trust Dr Naveena Singh, Barts
Department of Pathology, Royal Group of Hospitals Trust, Belfast, Northern Ireland.
 UTERINE ADENOSARCOMA W Glenn McCluggage Department of Pathology, Royal Group of Hospitals Trust, Belfast, Northern Ireland. Definition of Adenosarcoma: A mixed tumor composed of benign neoplastic glandular
UTERINE ADENOSARCOMA W Glenn McCluggage Department of Pathology, Royal Group of Hospitals Trust, Belfast, Northern Ireland. Definition of Adenosarcoma: A mixed tumor composed of benign neoplastic glandular
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS
 ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis
 In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis Rouba Ali-Fehmi,MD The Karmanos Cancer Institute, Wayne State University School of Medicine Global incidence of cervical
In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis Rouba Ali-Fehmi,MD The Karmanos Cancer Institute, Wayne State University School of Medicine Global incidence of cervical
Current Concept in Ovarian Carcinoma: Pathology Perspectives
 Current Concept in Ovarian Carcinoma: Pathology Perspectives Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine Current Concept in Ovarian
Current Concept in Ovarian Carcinoma: Pathology Perspectives Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine Current Concept in Ovarian
of 20 to 80 and subsequently declines [2].
![of 20 to 80 and subsequently declines [2].](/thumbs/80/81450506.jpg "of 20 to 80 and subsequently declines [2].") - - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
- - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
Ovarian carcinoma classification. Robert A. Soslow, MD
 Ovarian carcinoma classification Robert A. Soslow, MD soslowr@mskcc.org WHO classification Serous Mucinous Endometrioid Clear cell Transitional Squamous Mixed epithelial Undifferentiated Introduction Rationale
Ovarian carcinoma classification Robert A. Soslow, MD soslowr@mskcc.org WHO classification Serous Mucinous Endometrioid Clear cell Transitional Squamous Mixed epithelial Undifferentiated Introduction Rationale
Important Recent Advances in Gynaecological Pathology
 Important Recent Advances in Gynaecological Pathology Sanjiv Manek Consultant Gynaecological Pathologist Oxford, UK In recent years there have been a significant number of changes in gynaecological pathology
Important Recent Advances in Gynaecological Pathology Sanjiv Manek Consultant Gynaecological Pathologist Oxford, UK In recent years there have been a significant number of changes in gynaecological pathology
Endometrial cancer. Szabolcs Máté MD. I. St. Department of Obstetrics and Gyneacology.
 Endometrial cancer Szabolcs Máté MD. I. St. Department of Obstetrics and Gyneacology dr.mate.szabolcs@gmail.com Epidemiology Developing countries Cervical cancer is the most common gyn. malignant tumor
Endometrial cancer Szabolcs Máté MD. I. St. Department of Obstetrics and Gyneacology dr.mate.szabolcs@gmail.com Epidemiology Developing countries Cervical cancer is the most common gyn. malignant tumor
Endometrial hyperplasia vs. Intraepithelial neoplasia. Martin Chang, MD PhD FRCPC Pathology Update Friday November 9, 2012
 Endometrial hyperplasia vs. Intraepithelial neoplasia Martin Chang, MD PhD FRCPC Pathology Update Friday November 9, 2012 Disclosure No relevant financial conflicts to declare. Case 1 Gland crowding Gland
Endometrial hyperplasia vs. Intraepithelial neoplasia Martin Chang, MD PhD FRCPC Pathology Update Friday November 9, 2012 Disclosure No relevant financial conflicts to declare. Case 1 Gland crowding Gland
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box?
 When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
3/25/2019. Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates
 Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates") J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates Signs
J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates Signs
Low-grade serous neoplasia. Robert A. Soslow, MD
 Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Case 1. Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno
 Luca Mazzucchelli Istituto cantonale di patologia Locarno") Case 1 Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno SAMO Interdisciplinary Workshop on Gynecological Tumors Lucern, October
Case 1 Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno SAMO Interdisciplinary Workshop on Gynecological Tumors Lucern, October
A randomised trial of non-selective versus selective adjuvant Therapy in high risk Apparent stage 1 Endometrial Cancer QA MANUAL
 A randomised trial of non-selective versus selective adjuvant Therapy in high risk Apparent stage 1 Endometrial Cancer QA MANUAL For Surgical Specimen Processing and Microscopy Central Pathology Quality
A randomised trial of non-selective versus selective adjuvant Therapy in high risk Apparent stage 1 Endometrial Cancer QA MANUAL For Surgical Specimen Processing and Microscopy Central Pathology Quality
Section 1. Biology of gynaecological cancers: our current understanding
 Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Management of Endometrial Hyperplasia
 Management of Endometrial Hyperplasia I have nothing to disclose. Stefanie M. Ueda, M.D. Assistant Clinical Professor UCSF Division of Gynecologic Oncology Female Malignancies in the United States New
Management of Endometrial Hyperplasia I have nothing to disclose. Stefanie M. Ueda, M.D. Assistant Clinical Professor UCSF Division of Gynecologic Oncology Female Malignancies in the United States New
UTERINE SARCOMA EXAMPLE OF A UTERINE SARCOMA USING PROPOSED TEMPLATE
 UTERINE SARCOMA EXAMPLE OF A UTERINE SARCOMA USING PROPOSED TEMPLATE Case: Adenosarcoma with heterologous elements and stromal overgrowth o TAH, BSO, omentectomy, staging biopsies of cul-de-sac, bladder
UTERINE SARCOMA EXAMPLE OF A UTERINE SARCOMA USING PROPOSED TEMPLATE Case: Adenosarcoma with heterologous elements and stromal overgrowth o TAH, BSO, omentectomy, staging biopsies of cul-de-sac, bladder
ACCME/Disclosures. Risk of Gyne Ca in HBOC. Molecular basis of HBOC. Hereditary Ovarian and Breast Cancer Syndrome
 Hereditary Ovarian and Breast Cancer Syndrome C. Blake Gilks, MD Dept of Pathology Vancouver General Hospital University of British Columbia Blake.gilks@vch.ca The USCAP requires that anyone in a position
Hereditary Ovarian and Breast Cancer Syndrome C. Blake Gilks, MD Dept of Pathology Vancouver General Hospital University of British Columbia Blake.gilks@vch.ca The USCAP requires that anyone in a position
JMSCR Vol 05 Issue 11 Page November 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.78 A Histomorphological Study of Carcinoma
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.78 A Histomorphological Study of Carcinoma
CASE 4 21/07/2017. Ectopic Prostatic Tissue in Cervix. Female 31. LLETZ for borderline nuclear abnormalities
 Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
Disclosure. Case. Mixed Tumors of the Uterine Corpus and Cervix. I have nothing to disclose
 Mixed Tumors of the Uterine Corpus and Cervix Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Department of Pathology Brigham and Women s Hospital Boston, MA UCSF Current Issues in Anatomic
Mixed Tumors of the Uterine Corpus and Cervix Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Department of Pathology Brigham and Women s Hospital Boston, MA UCSF Current Issues in Anatomic
Adenocarcinoma of the Cervix
 Question 1. Each of the following statements about cervical adenocarcinoma is true except: Adenocarcinoma of the Cervix SAMS a) A majority of women with cervical adenocarcinoma have stage I tumors at diagnosis.
Question 1. Each of the following statements about cervical adenocarcinoma is true except: Adenocarcinoma of the Cervix SAMS a) A majority of women with cervical adenocarcinoma have stage I tumors at diagnosis.
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer
 status in Colorectal Cancer") Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer Start date: May 2015 Review date: April 2018 1 Background Mismatch repair (MMR) deficiency is seen in approximately 15%
Demystifying Endometrial Hyperplasia
 Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate
Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate
The molecular genetics of endometrial cancer
 The molecular genetics of endometrial cancer Lora Hedrick Ellenson, M.D. Department of Pathology and Laboratory Medicine Weill Medical College of Cornell University Introduction Classification of endometrial
The molecular genetics of endometrial cancer Lora Hedrick Ellenson, M.D. Department of Pathology and Laboratory Medicine Weill Medical College of Cornell University Introduction Classification of endometrial
Villoglandular adenocarcinoma of cervix a tumour with bland cytological features: report of a case missed on cytology
 Malaysian J Pathol 2003; 25(2) : CERVICAL 139 143 VILLOGLANDULAR ADENOCARCINOMA CYTOLOGY CASE REPORT Villoglandular adenocarcinoma of cervix a tumour with bland cytological features: report of a case missed
Malaysian J Pathol 2003; 25(2) : CERVICAL 139 143 VILLOGLANDULAR ADENOCARCINOMA CYTOLOGY CASE REPORT Villoglandular adenocarcinoma of cervix a tumour with bland cytological features: report of a case missed
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017
 Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Index. Cytoplasm, nonepithelial malignant tumor features 70
 Accurette device 23 Adenosarcoma, differential diagnosis 80, 81 Arias-Stella reaction 65 Atypical endocervical cells 8 Atypical endometrial cells 8 Atypical glandular cells (AGC) 8, 9 Atypical glandular
Accurette device 23 Adenosarcoma, differential diagnosis 80, 81 Arias-Stella reaction 65 Atypical endocervical cells 8 Atypical endometrial cells 8 Atypical glandular cells (AGC) 8, 9 Atypical glandular
Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Pr
 Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Professor Yong Loo Lin School of Medicine, National University
Case Presentation Diana Lim, MBBS, FRCPA, FRCPath Senior Consultant Department of Pathology, National University Health System, Singapore Assistant Professor Yong Loo Lin School of Medicine, National University
Intravascular Endometrium Mimicking Vascular Invasion
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 A Papanicolau, G Lin Citation A Papanicolau, G Lin.. The Internet Journal of Pathology. 2010 Volume 12 Number 1. Abstract Intravascular endometrium
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 A Papanicolau, G Lin Citation A Papanicolau, G Lin.. The Internet Journal of Pathology. 2010 Volume 12 Number 1. Abstract Intravascular endometrium
ACCME/Disclosures. Case History 4/13/2016. USCAP GU Specialty Conference Case 3. Ann Arbor, MI
 USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
VULVAR CARCINOMA. Page 1 of 5
 VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type)
") Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
New Cancer Cases By Site Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3%
 Uterine Malignancy New Cancer Cases By Site 2010 Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3% Cancer Deaths By Site 2010 Lung 26% Breast 15% Colo-Rectal 9% Pancreas 7%
Uterine Malignancy New Cancer Cases By Site 2010 Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3% Cancer Deaths By Site 2010 Lung 26% Breast 15% Colo-Rectal 9% Pancreas 7%
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") C ORPUS UTERI C ARCINOMA STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery Tis * T1 I T1a IA NX N0 N1 N2
C ORPUS UTERI C ARCINOMA STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery Tis * T1 I T1a IA NX N0 N1 N2
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications. Andres A. Roma, MD Cleveland Clinic
 Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications Andres A. Roma, MD Cleveland Clinic No Disclosures In the past 12 months, I have not had
Session Number: 1020 Session: Adenocarcinoma of the Cervix: Diagnostic Pitfalls and New Prognostic Implications Andres A. Roma, MD Cleveland Clinic No Disclosures In the past 12 months, I have not had
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Small diagnostic biopsies Handling and reporting issues. Dr Varsha Shah Consultant Histopathologist Royal Gwent Hospital Newport
 Small diagnostic biopsies Handling and reporting issues Dr Varsha Shah Consultant Histopathologist Royal Gwent Hospital Newport RCPath 2017 Biopsy vs. resection specimens Smaller Tissues: Larger Issues
Small diagnostic biopsies Handling and reporting issues Dr Varsha Shah Consultant Histopathologist Royal Gwent Hospital Newport RCPath 2017 Biopsy vs. resection specimens Smaller Tissues: Larger Issues
ARRO Case: Early-stage Endometrial Cancer
 ARRO Case: Early-stage Endometrial Cancer Ankit Modh, MD (PGY-4) Faculty Advisor: Mohamed A Elshaikh, MD Department of Radiation Oncology Henry Ford Cancer Institute Case Presentation 70 y/o African American
ARRO Case: Early-stage Endometrial Cancer Ankit Modh, MD (PGY-4) Faculty Advisor: Mohamed A Elshaikh, MD Department of Radiation Oncology Henry Ford Cancer Institute Case Presentation 70 y/o African American
Mousa. Najat kayed &Renad Al-Awamleh. Nizar Alkhlaifat
 6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
3/24/2017. Disclosure of Relevant Financial Relationships. Mixed Epithelial Endometrial Carcinoma. ISGyP Endometrial Cancer Project
 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Interpretation of p53 Immunostains. P53 Mutations are Ubiquitous in High Grade Serous Carcinoma. Diffuse strong positive nuclear staining
 Stains for Tumor Classification p53 p16 WT1 HMGA2 P53 Mutations are Ubiquitous in High Grade Serous Carcinoma Source Ahmed et al Australian Ovarian Cancer Study Cancer Genome Atlas Research Network Cases
Stains for Tumor Classification p53 p16 WT1 HMGA2 P53 Mutations are Ubiquitous in High Grade Serous Carcinoma Source Ahmed et al Australian Ovarian Cancer Study Cancer Genome Atlas Research Network Cases
6/5/2010. Outline of Talk. Endometrial Alterations That Mimic Cancer & Vice Versa: Metaplastic / reactive changes. Problems in Biopsies/Curettages
 Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
ACCME/Disclosures. Diagnosing Mesothelioma in Limited Tissue Samples. Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016
 Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Page # 1. Endometrium. Cellular Components. Anatomical Regions. Management of SIL Thomas C. Wright, Jr. Most common diseases:
 Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Staging. Carcinoma confined to the corpus. Carcinoma confined to the endometrium. Less than ½ myometrial invasion. Greater than ½ myometrial invasion
 5 th of June 2009 Background Most common gynaecological carcinoma in developed countries Most cases are post-menopausal Increasing incidence in certain age groups Increasing death rates in the USA 5-year
5 th of June 2009 Background Most common gynaecological carcinoma in developed countries Most cases are post-menopausal Increasing incidence in certain age groups Increasing death rates in the USA 5-year
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
This protocol is intended to assist pathologists in providing
 Protocol for the Examination of Specimens From Patients With Carcinomas of the Endometrium A Basis for Checklists Steven G. Silverberg, MD, for the Members of the Cancer Committee, College of American
Protocol for the Examination of Specimens From Patients With Carcinomas of the Endometrium A Basis for Checklists Steven G. Silverberg, MD, for the Members of the Cancer Committee, College of American
What is endometrial cancer?
 Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer March 2017 1 Background Mismatch repair (MMR) deficiency is seen in approximately
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact
 Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER. Guidelines for the assessment of mismatch. Colorectal Cancer
 COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
COLORECTAL PATHWAY GROUP, MANCHESTER CANCER Guidelines for the assessment of mismatch repair (MMR) status in Colorectal Cancer January 2015 1 Background Mismatch repair (MMR) deficiency is seen in approximately
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
This peer-reviewed article can be downloaded, printed and distributed freely for any purposes (see copyright notice below).
.") Diagnostic Pathology This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Endometrioid adenocarcinoma
Diagnostic Pathology This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Endometrioid adenocarcinoma
Gynecologic Malignancies. Kristen D Starbuck 4/20/18
 Gynecologic Malignancies Kristen D Starbuck 4/20/18 Outline Female Cancer Statistics Uterine Cancer Adnexal Cancer Cervical Cancer Vulvar Cancer Uterine Cancer Endometrial Cancer Uterine Sarcoma Endometrial
Gynecologic Malignancies Kristen D Starbuck 4/20/18 Outline Female Cancer Statistics Uterine Cancer Adnexal Cancer Cervical Cancer Vulvar Cancer Uterine Cancer Endometrial Cancer Uterine Sarcoma Endometrial
3 cell types in the normal ovary
 Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix
 The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
Ovarian cancer: 2012 Update Srini Prasad MD Univ Texas MD Anderson Cancer Center
 Ovarian cancer: 2012 Update Srini Prasad MD Univ Texas MD Anderson Cancer Center Ovarian cancer is not a single disease Ovarian Epithelial Tumors: Histological Spectrum* Type Frequency Histology High-Grade
Ovarian cancer: 2012 Update Srini Prasad MD Univ Texas MD Anderson Cancer Center Ovarian cancer is not a single disease Ovarian Epithelial Tumors: Histological Spectrum* Type Frequency Histology High-Grade
Case 3 - GYN. History: 66 year old, routine Pap test. Dr. Stelow
 Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
HISTOLOGICAL TYPES OF UTERINE CANCER IN THE DR. SALVATOR VUIA CLINICAL OBSTETRICS AND GYNECOLOGY HOSPITAL ARAD DURING THE PERIOD
 HISTOLOGICAL TYPES OF UTERINE CANCER IN THE DR. SALVATOR VUIA CLINICAL OBSTETRICS AND GYNECOLOGY HOSPITAL ARAD DURING THE 2000-2009 PERIOD Gheorghe Furău 1), Voicu Daşcău 1), Cristian Furău 1), Lucian
HISTOLOGICAL TYPES OF UTERINE CANCER IN THE DR. SALVATOR VUIA CLINICAL OBSTETRICS AND GYNECOLOGY HOSPITAL ARAD DURING THE 2000-2009 PERIOD Gheorghe Furău 1), Voicu Daşcău 1), Cristian Furău 1), Lucian
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Ovarian Clear Cell Carcinoma
 Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
Type I. Type II. Excess estrogen Lynch Endometrioid adenocarcinoma PTEN. High grade More aggressive Serous, Clear Cell p53
 Type I Excess estrogen Lynch Endometrioid adenocarcinoma PTEN Type II High grade More aggressive Serous, Clear Cell p53 Stage I IA IB Stage II Stage III IIIA IIIB IIIC IIIC1 IIIC2 Stage IV IVA IVB nodes
Type I Excess estrogen Lynch Endometrioid adenocarcinoma PTEN Type II High grade More aggressive Serous, Clear Cell p53 Stage I IA IB Stage II Stage III IIIA IIIB IIIC IIIC1 IIIC2 Stage IV IVA IVB nodes
Endometrial pathology. Dr Tom Dodd and Dr Georgina England
 Endometrial pathology Dr Tom Dodd and Dr Georgina England Case 1 Female age 35 Case 1 Proliferative endometrium Case 2 Female age 38 Case 2 Secretory endometrium Dating endometrium Assessed on the
Endometrial pathology Dr Tom Dodd and Dr Georgina England Case 1 Female age 35 Case 1 Proliferative endometrium Case 2 Female age 38 Case 2 Secretory endometrium Dating endometrium Assessed on the
Diagnostically Challenging Cases in Gynecologic Pathology
 Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Clonal evolution of human cancers
 Clonal evolution of human cancers -Pathology-based microdissection and genetic analysis precisely demonstrates molecular evolution of neoplastic clones- Hiroaki Fujii, MD Ageo Medical Laboratories, Yashio
Clonal evolution of human cancers -Pathology-based microdissection and genetic analysis precisely demonstrates molecular evolution of neoplastic clones- Hiroaki Fujii, MD Ageo Medical Laboratories, Yashio
Dall istologia alla caratterizzazione biomolecolare
 Il carcinoma ovarico: approccio multidisciplinare e prospettive terapeutiche Dall istologia alla caratterizzazione biomolecolare Anna Pesci Ospedale SC Don Calabria, Negrar anna.pesci@sacrocuore.it Ovarian
Il carcinoma ovarico: approccio multidisciplinare e prospettive terapeutiche Dall istologia alla caratterizzazione biomolecolare Anna Pesci Ospedale SC Don Calabria, Negrar anna.pesci@sacrocuore.it Ovarian
Cervical Cancer: 2018 FIGO Staging
 Cervical Cancer: 2018 FIGO Staging Jonathan S. Berek, MD, MMS Laurie Kraus Lacob Professor Stanford University School of Medicine Director, Stanford Women s Cancer Center Senior Scientific Advisor, Stanford
Cervical Cancer: 2018 FIGO Staging Jonathan S. Berek, MD, MMS Laurie Kraus Lacob Professor Stanford University School of Medicine Director, Stanford Women s Cancer Center Senior Scientific Advisor, Stanford
OUTLINE. Case History 1/28/2013. Endometrial Neoplasia, Including Endometrial Intraepithelial Neoplasia (EIN)
") Endometrial Neoplasia, Including Endometrial Intraepithelial Neoplasia (EIN) TEXAS SOCIETY OF PATHOLOGISTS ANNUAL MEETING Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Brigham and Women
Endometrial Neoplasia, Including Endometrial Intraepithelial Neoplasia (EIN) TEXAS SOCIETY OF PATHOLOGISTS ANNUAL MEETING Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Brigham and Women
UTERINE SARCOMAS CURRENT THERAPEUTIC OPTIONS
 Review Journal of Translational Medicine and Research, volume 19, no. 1-2, 2014 UTERINE SARCOMAS CURRENT THERAPEUTIC OPTIONS N. Bacalbaæa 1, A. Traistaru 2, I. Bãlescu 3 1 Carol Davila University of Medicine
Review Journal of Translational Medicine and Research, volume 19, no. 1-2, 2014 UTERINE SARCOMAS CURRENT THERAPEUTIC OPTIONS N. Bacalbaæa 1, A. Traistaru 2, I. Bãlescu 3 1 Carol Davila University of Medicine
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens
 How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
5/26/2016. Pelvic Serous Carcinoma: 2014 W.H.O. Update. Outline of Talk. Changes to 2014 WHO system for pelvic serous tumors
 Pelvic Serous Carcinoma: 2014 W.H.O. Update Outline of Talk Practical Implications for Pathologists Changes to 2014 WHO system for pelvic serous tumors High grade serous carcinoma versus low grade serous
Pelvic Serous Carcinoma: 2014 W.H.O. Update Outline of Talk Practical Implications for Pathologists Changes to 2014 WHO system for pelvic serous tumors High grade serous carcinoma versus low grade serous
Endometrium. Protocol applies to all carcinomas of the endometrium. Procedures Cytology (No Accompanying Checklist) Biopsy Curettage Hysterectomy
 Biopsy Curettage Hysterectomy") Endometrium Protocol applies to all carcinomas of the endometrium. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Endometrium Protocol applies to all carcinomas of the endometrium. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Pathology of the female genital tract
 Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY
 UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY SCIENTIFIC COORDINATOR: PROF. DR. MIHAI B. BRĂILA, Ph.D. Ph.D. Graduand:
UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY SCIENTIFIC COORDINATOR: PROF. DR. MIHAI B. BRĂILA, Ph.D. Ph.D. Graduand:
Endometrial Cancer Histopathology Reporting Guide
 Endometrial Cancer Histopathology Reporting Guide Family/Last name Given name(s) Date of birth DD MM YYYY Patient identifiers Date of request Accession/Laboratory number DD MM YYYY Elements in black text
Endometrial Cancer Histopathology Reporting Guide Family/Last name Given name(s) Date of birth DD MM YYYY Patient identifiers Date of request Accession/Laboratory number DD MM YYYY Elements in black text
Factors predictive of myoinvasion in cases of Complex Atypical Hyperplasia diagnosed on endometrial biopsy or curettage
 Factors predictive of myoinvasion in cases of Complex Atypical Hyperplasia diagnosed on endometrial biopsy or curettage Jessica Johns, MD Jeffrey Killeen, MD Robert Kim, MD Hyeong Jun Ahn, PhD None Disclosures
Factors predictive of myoinvasion in cases of Complex Atypical Hyperplasia diagnosed on endometrial biopsy or curettage Jessica Johns, MD Jeffrey Killeen, MD Robert Kim, MD Hyeong Jun Ahn, PhD None Disclosures
New Developments in Immunohistochemistry for Gynecologic Pathology
 New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
Gynaecological Malignancies
 Gynaecological Malignancies Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea Division of Pathology School of Medicine & Health Sciences Overview Genital tract tumors
Gynaecological Malignancies Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea Division of Pathology School of Medicine & Health Sciences Overview Genital tract tumors
Shina Oranratanaphan, Tarinee Manchana*, Nakarin Sirisabya
 Comparison of Synchronous Endometrial and Ovarian Cancers versus Primary with Metastasis RESEARCH COMMUNICATION Clinicopathologic Variables and Survival Comparison of Patients with Synchronous Endometrial
Comparison of Synchronous Endometrial and Ovarian Cancers versus Primary with Metastasis RESEARCH COMMUNICATION Clinicopathologic Variables and Survival Comparison of Patients with Synchronous Endometrial
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES CASE 1: FEMALE REPRODUCTIVE
 Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
RESEARCH COMMUNICATION
 RESEARCH COMMUNICATION Clinicopathologic Analysis of Women with Synchronous Primary Carcinomas of the Endometrium and Ovary: 10- Year Experience from Chiang Mai University Hospital Jiraprapa Natee 1 *,
RESEARCH COMMUNICATION Clinicopathologic Analysis of Women with Synchronous Primary Carcinomas of the Endometrium and Ovary: 10- Year Experience from Chiang Mai University Hospital Jiraprapa Natee 1 *,
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Carcinoma of the Cervix Histopathology Reporting Guide
 Carcinoma of the Cervix Histopathology Reporting Guide Family/Last name Given name(s) Date of birth DD MM YYYY Patient identifiers Date of request Accession/Laboratory number DD MM YYYY Elements in black
Carcinoma of the Cervix Histopathology Reporting Guide Family/Last name Given name(s) Date of birth DD MM YYYY Patient identifiers Date of request Accession/Laboratory number DD MM YYYY Elements in black