Endometrial pathology. Dr Tom Dodd and Dr Georgina England
|
|
|
- Merry Gladys Parsons
- 6 years ago
- Views:
Transcription
1 Endometrial pathology Dr Tom Dodd and Dr Georgina England
2 Case 1 Female age 35
3
4

5
6 Case 1 Proliferative endometrium
7 Case 2 Female age 38

8

9

10

11
12 Case 2 Secretory endometrium
13 Dating endometrium Assessed on the functional layer of the endometrium (superficial stratum compactum & deeper stratum spongiosum). Isthmic endometrium, with fibrous stroma & flattened & slit-like glands, is not representative. Dated to the most advanced area. Abnormal endometrium should not be dated. Inactive or atrophic endometrium. Endometritis. Polyps Hyperplasia.
14 Dating endometrium Functional layer of the endometrium superficial stratum compactum Decidualised stromal cells more prominent. Deeper stratum spongiosum. Stroma more oedematous in secretory phase. Basal layer Stroma relatively more prominent. No secretory activity.
15 Dating endometrium Proliferative endometrium can be divided into three phases: early, middle and late. Secretory phase broadly divided into two stages: Earlier predominantly glandular Cytoplasmic vacuolation, later saw-tooth pattern Later stromal Oedema and latter stromal cell decidualisation. inc. endometrial lymphocytes (CD 3 -, CD 56+). Spiral arterioles. Menstrual phase Disruption of glands Condensation of stroma Stromal leukocyte infiltration. Trap: Collapsing glands back to back pattern not to confused with hyperplasia or carcinoma. Clue : look for secretory features and decidual change in stroma.
16 Normal endometrium Trap: Late secretory pattern endometrium with sawtooth glands not to be confused with hyperplasia or carcinoma. Clues: Marked gland crowding or complexity Nuclear stratification and enlargement and vesicular nuclei. Stromal predecidualised cells
17 Further pitfalls Dissociation of glands and stroma False crowding Misdiagnose hyperplasia or carcinoma Don't diagnose complex hyperplasia without intact stroma Telescoping artefact Intussusception of glands producing a gland within gland pattern. Recognised as each gland is surrounded by a circle of epithelium.
18 Case 3 Female age 28

19

20

21

22

23

24
25 Case 3 Arias-Stella reaction
26 Arias-Stella reaction Nuclear atypia with nuclear enlargement, hyperchromasia and pleomorphism and vacuolated cytoplasm. Trap: confuse nuclei bulging into gland lumen with hobnail cells of clear cell carcinoma. Clues Hypersecretory features. Decidual stromal changes. Mitoses +/- p53 & MIB 1 (vs clear cell carcinoma) Marker of pregnancy intrauterine or extrauterine. Also may be induced with hormones especially progestational drugs.
27 Case 4 Female age 40

28

29

30

31

32
33 Case 4 Non-specific chronic endometritis
34 Non-specific chronic endometritis Variable features Prominent lymphoid aggregates within functionalis Especially if germinal centres present. Plasma cells (CD 138 positive) +/- neutrophils glands & stroma Neutrophils should not be present in endometrium until menstruation established. Disturbance in glands and stroma effecting dating of endometrium. Aetiology includes: Pregnancy related, post abortion etc. specific infections e.g. Chlamydia in association with polyps & tumours.
35 Case 6 Female age 37

36

37

38

39

40

41

42
43 Case 6 Syncytial papillary change / Papillary syncytial metaplasia
44 Syncytial papillary change (Papillary syncytial metaplasia) Cuboidal epithelial cells with eosinophilic cytoplasm typically heaped up to give a papillary appearance. Neutrophils are commonly present. Relatively common, and may be seen with menstrual breakdown and in infarcted polyps. Clue to the presence of non-menstrual endometrial shedding. Regarded as not a true metaplasia but a change associated with menstrual breakdown. Clue vs carcinoma Confinement to surface, bland cytology, low MIB 1 & menstrual change
45 Endometrial metaplasia Diverse range of changes Recognised by cytoplasmic changes. Squamous, tubal, eosinophilic, mucinous & clear cell. Frequently associated with hyperplasia, but is not diagnostic of hyperplasia or indicative of endometrial atypia. Clue: attention to the low power architectural pattern will assist in separating metaplasia alone from hyperplasia or carcinoma.
46 Case 7 Female age 45

47

48

49
50 Case 7 Endometrial hyperplasia (hyperplasia without atypia)
51 Case 8 Female age 48

52

53

54
55 Case 8 Endometrial hyperplasia and squamous metaplasia
56 Endometrial hyperplasia Assessment of endometrium may be difficult and to a degree is subjective and a variety of nomenclatures have been proposed. WHO 2014 system Hyperplasia without atypia Atypical hyperplasia / endometrioid intraepithelial neoplasia Serous endometrial intraepithelial carcinoma (SEIC) WHO 1994 system Simple hyperplasia Complex hyperplasia Atypical hyperplasia
57 Hyperplasia without atypia Typically thickened endometrium Endometrial glands show variation in size with cystically dilated glands being typical. Problem: Separation from disordered proliferative endometrium. Clues: Hyperplasia typically diffuse vs focal & variable. Gland to stromal ratio increases greater 1 : 1 in hyperplasia. Glands lack infolding, budding and branching. Lining epithelium resembles proliferative endometrium Columnar pseudostratified cells. Nuclei are oval with even chromatin and inconspicuous nucleoli. Problem: separation from postmenopausal cystic atrophy Clues: atrophic epithelium lacking mitoses in glands & stroma.
58 Complex hyperplasia No longer used Either classified as hyperplasia without atypia or atypical hyperplasia
59 Atypical hyperplasia Cellular features of malignancy Loss of polarity Increase in N:C ratio Nuclear pleomorphism & hyperchromasia Coarse chromatin Prominent nucleoli Irregular nuclear membranes Degree of atypia is not usually graded (some recommend grading mild, moderate severe), and may be focal. Architectural features must be considered to separate from carcinoma.
60 Differential diagnosis Atypical polypoid adenomyoma Frequently younger premenopausal women with a polyp often in lower uterus. Polypoid biphasic lesion cellular smooth muscle stroma. Variable glandular complexity, atypia and squamous morules. Absence of severe cytological atypia & low architectural complexity. Usually some benign proliferative or secretory endometrium in sample.
61 Case 9 Female age 55

62

63

64

65

66

67
68 Case 9 Endometrioid adenocarcinoma
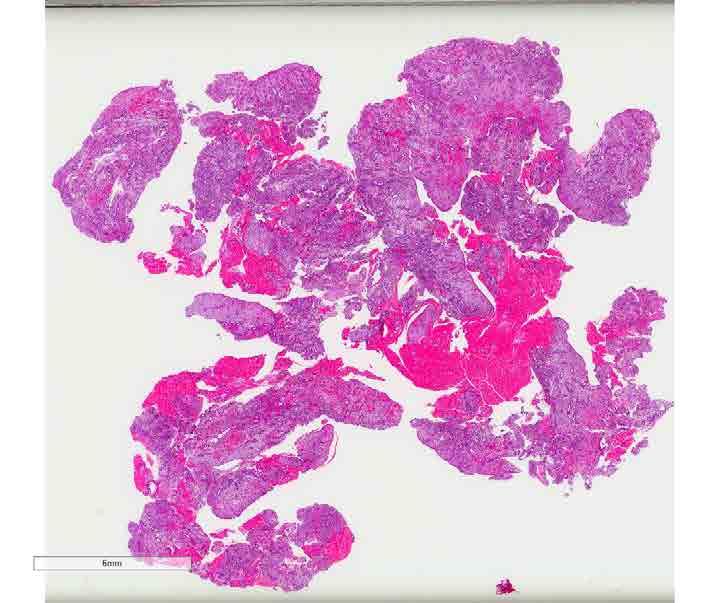
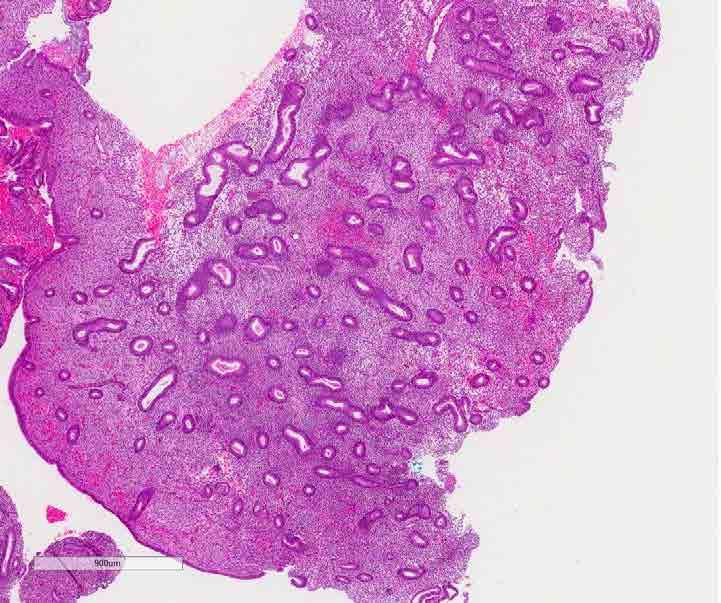
69 Endometrioid adenocarcinoma Problem: Distinction between atypical endometrial hyperplasia and endometrioid adenocarcinoma may be difficult on curettage specimens. Clues: include: Confluent glands with a cribriform architecture or labyrinth pattern Total absence of stroma between neoplastic glands. Prominent surface villous or papillary growth pattern particularly with second and third degree branching or cribriform budding. Irregular glands infiltrating fibrotic stroma.
70 Endometrioid adenocarcinoma Grading should be undertaken FIGO architectural and cytological features. Grade 1 < 6% non-gland forming growth. Grade 2 < 6 50 % non-gland forming growth Grade 3 > 50% non-gland forming growth Grade 1 & 2 increase one grade I if grade 3 nuclei present. Nuclear grade Oval -> round Marked variation in size & shape Hypochromasia - > hyperchromasia Variation in staining intensity Even chromatin - > Coarse clumped chromatin Nucleoli not prominent - > prominent nucleoli. Sparse mitoses - > frequent and abnormal mitoses. Concordance with curette & hysterectomy specimen 45 75% prove to have a higher grade. (Mitchard,J Hirschowitz, l Histopathology. 42(4): , April 2003). Reflecting sampling and reproducibility of grading.
71 Lynch syndrome 2-5% of endometrial carcinomas Approx 10% of endometrial ca at < 40 years Surveillance for colorectal carcinoma in Lynch syndrome reduces mortality by 65% Occurs in 3 settings: Germline mutations in: MSH2, MSH6, MLH1, PMS2 MSH6 mutations most common in EC Germline EPCAM mutation downregulation of MSH2 Constitutive epimuation widespread methylation of genes including MLH1 MMR IHC followed by sequencing is the most cost effective approach BRAF of limited utility in EC
72 Case 10 Female age 64

73

74

75

76

77
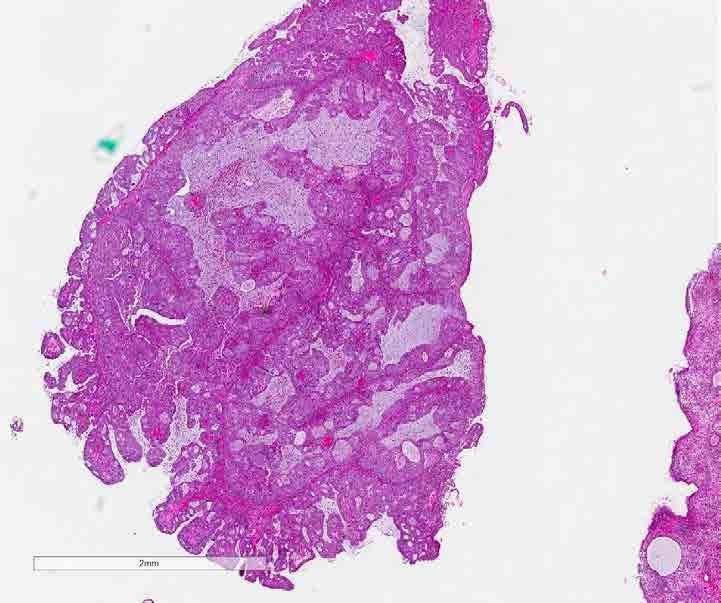
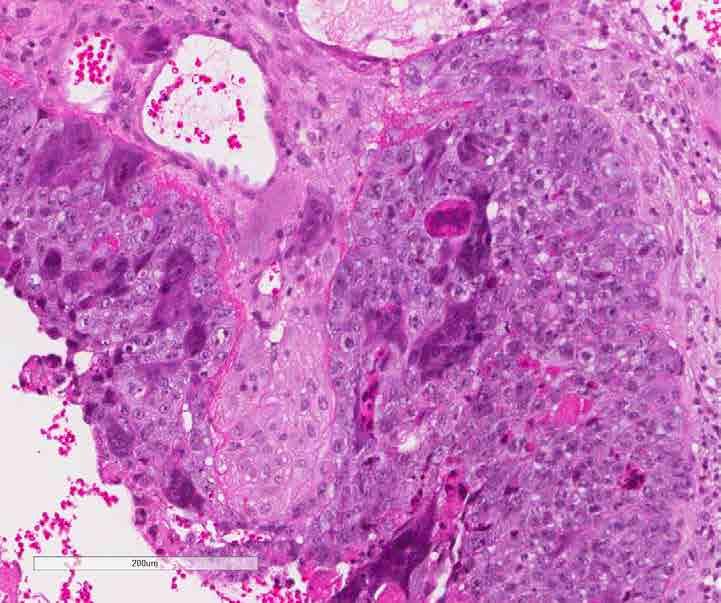
78 Case 10 Serous carcinoma
79 Serous carcinoma May occur in association with endometrioid and clear cell components. Background endometrium may show surface epithelium exhibiting high grade malignant cells referred to as endometrial intraepithelial carcinoma.
80 Serous carcinoma - histology Analogous to ovarian equivalent. Complex papillary architecture, Cellular budding High grade cytology Psammoma bodies (25%)
81 Pitfalls in serous carcinoma Problem: Separating tumours with a glandular pattern from endometrioid carcinoma. Clues: the epithelium is pleomorphic with rounded nuclei and prominent nucleoli. polarity of endometrioid carcinoma is absent. ICC All or nothing staining with p53 Usually negative ER/PR/beta catenin High MIB 1 > 75% of cells

82
83 Case 11 Female age 65

84

85

86

87

88
89 Case 11 Clear cell carcinoma
90 Clear cell carcinoma Uncommon, occurs in older women. Background atrophic pattern, but some cases show endometrial hyperplasia. Identical to ovarian counterpart. Histological appearances: Clear cells with a solid, tubulocystic or papillary growth pattern. Hobnail cells are characteristic. +/-Oncocytic cytology with eosinophilic cytoplasm High grade by definition May occur in association with serous or endometrioid pattern carcinomas.
91 Uterine clear cell tumours Clear cell carcinoma HNF1b positive, ki 67 50% Endometrioid carcinoma Secretory variant Clear cell change Squamous metaplasia with clear cells Serous carcinoma with clear cells P16 and P53 positive, Ki67 >75% PEComas HMB45, Melan A and SMA positive
92 Bokhman classification of endometrial carcinomas Type 1 70% Endometrioid carcinoma Post menopausal High oestrogen states: Obese, PCOS, Granulosa cell tumours Background of endometrial hyperplasia / endometrial intraepithelial neoplasia PTEN, KRAS, CTNNB1, PIK3CA, MSI Type 2 30% Serous and clear cell carcinomas Atrophic endometrium +/- endometrial intraepithelial carcinoma HER2 TP53
93 Case 12 Female age 55

94
95

96

97

98




99 ER P16 CEA Vimentin
100 Case 12 Endometrial carcinoma with a microglandular-like pattern (aka Low grade mucinous microglandular adenocarcinoma)

101
102 Endometrial carcinoma with a microglandular-like pattern Low aggressive endometrial carcinoma resembling endocervical microglandular hyperplasia. Postmenopausal women Numerous neutrophils in gland lumens, scattered mitoses, mild nuclear atypia. IHC: Positive: CD10, vimentin, CEA, ER, p16. Negative: PAX2, p63, CD34 Ki67 >10% DDx - microglandular hyperplasia negative for these antibodies.
103 Endometrioid vs endocervical Endocervical carcinoma typically: Greater nuclear atypia & mitoses. Mucinous differentiation may occur in both sites Immunohistochemistry: Endometrial: vimentin +, ER +,CEA Cervical: vimentin -, ER weak + or -, CEA + p16 strong in endocervical, (negative in unusual subtypes). endometrial endometrioid ca weak/focal, strong in rare cases
104 Case 16 Female age 73

105

106

107

108

109

110
111 Case 16 Endometrial adenosarcoma
112 Endometrial adenosarcoma Biphasic tumour with benign epithelial component and sarcomatous stroma. Polypoid mass Histology: Glands: compressed with a branched leaf-like pattern and lined typically with endometrioid-type epithelium. Stroma IHC: Sarcomatous Periglandular condensation. Variable degree of nuclear pleomorphism, and mitotic activity 20% may have heterologous elements +/- sarcomatous overgrowth prognostic signifciant. Positive: oestrogen receptor (ER), progesterone receptor (PR), CD10, WT1 and smooth muscle actin 80% no or limited myometrial invasion Sarcomatous overgrowth worse prognosis.
113 Case 13 Female age 71

114

115

116

117

118

119
120 Case 13 Malignant Mixed Mullerian Tumour / carcinosarcoma
121 Malignant Mixed Mullerian Tumour carcinosarcoma Malignant epithelial and stromal elements. Ratio of components varies, and curettage specimens may be composed entirely of sarcoma Presence of heterologous elements may be particularly helpful. Immunohistochemistry: Epithelial and mesenchymal elements may stain with cytokeratins. Pattern of carcinoma should be noted. Metastases may be purely carcinoma, biphasic or rarely purely sarcoma.
122 WHO classification of mixed epithelial and mesenchymal tumours 2014 Adenomyoma Atypical polypoid adenomyoma Adenofibroma Adenosarcoma Carcinosarcoma

123
124 Case 14 Female age 55

125

126

127

128




129 CK ER GCDFP Mammoglobin
130 Case 14 Metastatic lobular carcinoma
131 Metastatic malignancies Metastatic carcinoma may represent a major diagnostic challenge. Common sites: Breast, G.I. tract, lung and melanoma Mimics for endometrial stromal sarcoma. Mimics for endometrial stromal sarcoma Lobular breast carcinoma mucin vacuoles, cytokeratin +, & breast associated antigens + Lymphoma CD 45 +
132 Case 15 Female age 60

133

134

135

136

137

138
139 Case 15 Leiomyosarcoma
140 Leimyosarcoma Typically, non-specific symptoms of pain and abnormal bleeding. Smooth muscle differentiation usually straight forward and aided with ICC for desmin. Care with assessing necrosis, mitotic index and cytological atypia prior to diagnosing malignancy on limited curettings. atypical smooth muscle tumour Differential diagnosis Combined stromal and smooth muscle tumours Epithelioid tumours Spindle cell carcinoma (Cytokeratin positive)
141 Case 17 Female age 52

142

143

144

145


146 Immunohistochemical stains CD10 Cytokeratin
147 Case 17 Endometrial Stromal Sarcoma
148 Endometrial Stromal Sarcoma (ESS) WHO classification of stromal tumours 2014 Endometrial stromal nodule Endometrial stromal sarcoma, low grade Endometrial stromal sarcoma, high grade Undifferentiated endometrial sarcoma high grade pleomorphic, mitotically active and show necrosis and lack specific differentiation. Sarcoma composed of cells resembling proliferative endometrial stroma and myometrial or vascular invasion. Small regular cells with oval nuclei fine stippled chromatin and inconspicuous nucleoli. Highly vascular with arterioles and a network of slit like capillaries. Hyaline fibrosis and foamy macrophages.
149 Problems with diagnosis of ESS Curettings containing cellular proliferating endometrial stromal tissue. Endometrial biopsy specimen may not allow distinction between endometrial stromal nodule and low-grade endometrial stromal sarcoma. Depends on assessment of margin. May show occasional benign glands. Smooth muscle differentiation. CD10 immunohistochemistry may be of assistance. Raise possibility of stromal tumour & further assessment including imaging.
150 Case 5 Female age 28

151

152

153

154

155


156 Immunohistochemical stains Cytokeratin Inhibin
157 Case 5 Placental site nodule
158 Placental site nodules Indicative of past pregnancy & incidental finding. Paucicellular circumscribed eosinophilic nodule within endometrium Composed of chorionic type intermediate (extravillous trophoblast) and may be hyalinised. Positive for cytokeratin, hpl and inhibin. Ki 67 < 5% Trap: Differential diagnosis with epithelioid trophoblastic tumour. Clues: Superficial, small, circumscribed and lack atypia. Proliferative index < 8%
159 Case 18 Female age 22

160

161

162

163
164 Case 18 Hydatidiform mole
165 Hydatidiform mole Gross vesicles significantly larger in complete mole Mole shape Hydrops increase with increasing gestational age, but scalloping of villi is more common in partial mole Polypoid villi complete mole Implantation site trophoblastic atypia focal & mild in partial mole vs diffuse & marked in complete mole. Villous stromal karyorrhexis Feature of complete mole Vascularity can be detected with CD 34 of most moles. Partial mole generally present. Complete mole inconspicuous.
166 Further investigation P57 Immunohistochemistry Paternally imprinted (ie not expressed) maternally transcribed gene, therefore complete loss of labelling of cytotrophoblast in complete moles Partial moles Labelling of cytotrophoblast villous stomal cells in & hydropic abortions. Ploidy Partial moles generally triploid Complete moles generally diploid (some tetraploid) with only paternal chromosomes.
167 What is the significance? 2-3% of complete moles will develop choriocarcinoma 0.5% of partial moles will develop choriocarcinoma
168 Case 19 Female age 28

169

170

171

172

173

174

175
176

177
178 Case 19 Choriocarcinoma
179 Choriocarcinoma Trimorphic population of intermediate trophoblastic cells, syncytiotrophoblast and cytotrophoblast with ABSENT chorionic villi Historically: ~ 50% hydatidiform mole ~ 25% normal pregnancy ~ 25% abortion Currently: 50% follow normal pregnancy Pathology Haemorrhagic mass Dismorphic cytotrophoblast & syncytiotrophoblast Haemorrhage, necrosis & mitoses +++ Cytokeratin, hcg, inhibin +
180 Differential diagnosis Complete mole Placental site trophoblastic tumour Biphasic pattern of choriocarcinoma hpl positive hcg levels (typically lower in PSTT) and ICC staining. Exaggerated placental site reaction Similar cellular population Occasional villi may be present. MIB 1 near 0% in placental site reaction vs high in choriocarcinoma. Placental site nodule Bland cytology of intermediate trophoblast No haemorrhagic necrosis. Carcinoma Leiomyosarcoma
181 WHO classification of gestational trophoblastic disease 2014 Neoplasms Choriocarcinoma Placental site trophoblastic tumour Epithelioid trophoblastic tumour Non-neoplastic lesions Placental site nodule and plaque Exaggerated placental site Molar pregnancies Hydatidiform mole Complete Partial Invasive Abnormal villous lesions (nonmolar)
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
6/5/2010. Outline of Talk. Endometrial Alterations That Mimic Cancer & Vice Versa: Metaplastic / reactive changes. Problems in Biopsies/Curettages
 Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus
 Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience
 Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS
 ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Trophoblastic tumors
 Trophoblastic tumors Uterus tumor course Oslo, 21-22/1/16 Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway Cases 45 38 39 4 Case 45
Trophoblastic tumors Uterus tumor course Oslo, 21-22/1/16 Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway Cases 45 38 39 4 Case 45
Atypical Hyperplasia/EIN
 EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
Disclosure. Case. Mixed Tumors of the Uterine Corpus and Cervix. I have nothing to disclose
 Mixed Tumors of the Uterine Corpus and Cervix Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Department of Pathology Brigham and Women s Hospital Boston, MA UCSF Current Issues in Anatomic
Mixed Tumors of the Uterine Corpus and Cervix Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Department of Pathology Brigham and Women s Hospital Boston, MA UCSF Current Issues in Anatomic
Index. Cytoplasm, nonepithelial malignant tumor features 70
 Accurette device 23 Adenosarcoma, differential diagnosis 80, 81 Arias-Stella reaction 65 Atypical endocervical cells 8 Atypical endometrial cells 8 Atypical glandular cells (AGC) 8, 9 Atypical glandular
Accurette device 23 Adenosarcoma, differential diagnosis 80, 81 Arias-Stella reaction 65 Atypical endocervical cells 8 Atypical endometrial cells 8 Atypical glandular cells (AGC) 8, 9 Atypical glandular
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Page # 1. Endometrium. Cellular Components. Anatomical Regions. Management of SIL Thomas C. Wright, Jr. Most common diseases:
 Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Diagnostically Challenging Cases in Gynecologic Pathology
 Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Department of Pathology, Royal Group of Hospitals Trust, Belfast, Northern Ireland.
 UTERINE ADENOSARCOMA W Glenn McCluggage Department of Pathology, Royal Group of Hospitals Trust, Belfast, Northern Ireland. Definition of Adenosarcoma: A mixed tumor composed of benign neoplastic glandular
UTERINE ADENOSARCOMA W Glenn McCluggage Department of Pathology, Royal Group of Hospitals Trust, Belfast, Northern Ireland. Definition of Adenosarcoma: A mixed tumor composed of benign neoplastic glandular
Dr Sanjiv Manek Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Demystifying Endometrial Hyperplasia
 Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate
Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate
of 20 to 80 and subsequently declines [2].
![of 20 to 80 and subsequently declines [2].](/thumbs/80/81450506.jpg "of 20 to 80 and subsequently declines [2].") - - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
- - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box?
 When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
Pathology of the female genital tract
 Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
CINtec p16 INK4a Staining Atlas
 CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo. Case Discussions. 60 year old woman Routine gynecologic control LBC
 BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix
 The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
Female genital tract II.
 Female genital tract II. Pathology of the uterine corpus Lilla Madaras 2 nd Department Of Pathology Semmelweis University Budapest 9 th April 2018 Anatomy 2 The normal endometrium Histology Regulation
Female genital tract II. Pathology of the uterine corpus Lilla Madaras 2 nd Department Of Pathology Semmelweis University Budapest 9 th April 2018 Anatomy 2 The normal endometrium Histology Regulation
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden
 and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden") What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000
 Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Histologic diagnosis of gestational trophoblastic diseases (GTD)
") 1 Histologic diagnosis of gestational trophoblastic diseases (GTD) Masaharu Fukunaga, M.D. Department of Pathology, the Jikei University Daisan Hospital, Tokyo, Japan Hydatidiform moles With the increased
1 Histologic diagnosis of gestational trophoblastic diseases (GTD) Masaharu Fukunaga, M.D. Department of Pathology, the Jikei University Daisan Hospital, Tokyo, Japan Hydatidiform moles With the increased
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Intravascular Endometrium Mimicking Vascular Invasion
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 A Papanicolau, G Lin Citation A Papanicolau, G Lin.. The Internet Journal of Pathology. 2010 Volume 12 Number 1. Abstract Intravascular endometrium
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 A Papanicolau, G Lin Citation A Papanicolau, G Lin.. The Internet Journal of Pathology. 2010 Volume 12 Number 1. Abstract Intravascular endometrium
What really matters When and Why. Pathology of Uterine Mesenchymal Lesions. Nafisa Wilkinson London
 What really matters When and Why Pathology of Uterine Mesenchymal Lesions Nafisa Wilkinson London Patient centred approach immunohistochemistry Histological diagnosis Next generation sequencing Genetic
What really matters When and Why Pathology of Uterine Mesenchymal Lesions Nafisa Wilkinson London Patient centred approach immunohistochemistry Histological diagnosis Next generation sequencing Genetic
Case year female. Routine Pap smear
 Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
5 Mousa Al-Abbadi. Ola Al-juneidi & Obada Zalat. Ahmad Al-Tarefe
 5 Mousa Al-Abbadi Ola Al-juneidi & Obada Zalat Ahmad Al-Tarefe Abnormal Uterine Bleeding (AUB) AUB is a very common scenario or symptom where women complain of menorrhagia (heavy and/or for long periods),
5 Mousa Al-Abbadi Ola Al-juneidi & Obada Zalat Ahmad Al-Tarefe Abnormal Uterine Bleeding (AUB) AUB is a very common scenario or symptom where women complain of menorrhagia (heavy and/or for long periods),
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Case 3 - GYN. History: 66 year old, routine Pap test. Dr. Stelow
 Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Pathology Slides. [Pathology]
![Pathology Slides. [Pathology]](/thumbs/94/120604575.jpg "Pathology Slides. [Pathology]") Pathology Slides MedicoNotes provides real laboratory pathological slides to aid you to differentiate between different pathological structures under microscope. www.mediconotes.com Histology slides example
Pathology Slides MedicoNotes provides real laboratory pathological slides to aid you to differentiate between different pathological structures under microscope. www.mediconotes.com Histology slides example
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
1 NORMAL HISTOLOGY AND METAPLASIAS
 1 NORMAL HISTOLOGY AND METAPLASIAS, MD Anatomy and Histology 1 Metaplasias 2 ANATOMY AND HISTOLOGY The female breast is composed of a branching duct system, which begins at the nipple with the major lactiferous
1 NORMAL HISTOLOGY AND METAPLASIAS, MD Anatomy and Histology 1 Metaplasias 2 ANATOMY AND HISTOLOGY The female breast is composed of a branching duct system, which begins at the nipple with the major lactiferous
Problems in the Differential Diagnosis of Endometrial Hyperplasia and Carcinoma
 THE 1999 LONG COURSE ON PATHOLOGY OF THE UTERINE CORPUS AND CERVIX Problems in the Differential Diagnosis of Endometrial Hyperplasia and Carcinoma Steven G. Silverberg, M.D. Department of Pathology, University
THE 1999 LONG COURSE ON PATHOLOGY OF THE UTERINE CORPUS AND CERVIX Problems in the Differential Diagnosis of Endometrial Hyperplasia and Carcinoma Steven G. Silverberg, M.D. Department of Pathology, University
3/28/2017. Disclosure of Relevant Financial Relationships. GU Evening Subspecialty Case Conference. Differential Diagnosis:
 GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
Endometrial Stromal Tumors
 Endometrial Stromal Tumors WHO Categories: Endometrial Stromal Nodule (ESN) Endometrial Stromal Sarcoma, low grade (LGESS) Endometrial Stromal Sarcoma, high grade (HGESS) Undifferentiated Uterine Sarcoma
Endometrial Stromal Tumors WHO Categories: Endometrial Stromal Nodule (ESN) Endometrial Stromal Sarcoma, low grade (LGESS) Endometrial Stromal Sarcoma, high grade (HGESS) Undifferentiated Uterine Sarcoma
Prepared By Jocelyn Palao and Layla Faqih
 Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
Macro- and microacinar proliferations of the prostate
 Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
The incidence of cervical adenocarcinoma (ADC) has
 has") Cervical Adenocarcinoma of Human Papillomavirus Positive and Human Papillomavirus Negative Tumors Edyta C. Pirog, MD, PhD Context. Cervical adenocarcinomas span a diverse group of tumors with several distinct
Cervical Adenocarcinoma of Human Papillomavirus Positive and Human Papillomavirus Negative Tumors Edyta C. Pirog, MD, PhD Context. Cervical adenocarcinomas span a diverse group of tumors with several distinct
Ovarian Clear Cell Carcinoma
 Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Pathology of Ovarian Tumours. Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh
 AFMC Pune PDCC (Cytopathology) PGI Chandigarh") Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY
 UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY SCIENTIFIC COORDINATOR: PROF. DR. MIHAI B. BRĂILA, Ph.D. Ph.D. Graduand:
UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY SCIENTIFIC COORDINATOR: PROF. DR. MIHAI B. BRĂILA, Ph.D. Ph.D. Graduand:
Endometrial line thickness in different conditions.
 Endometrial line thickness in different conditions 1 Endometrial thickens in response to Rising estrogen levels during the menstrual cycle and then shedding endometrial at the times of menses 2 The thickens
Endometrial line thickness in different conditions 1 Endometrial thickens in response to Rising estrogen levels during the menstrual cycle and then shedding endometrial at the times of menses 2 The thickens
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
OUTLINE. Case History 1/28/2013. Endometrial Neoplasia, Including Endometrial Intraepithelial Neoplasia (EIN)
") Endometrial Neoplasia, Including Endometrial Intraepithelial Neoplasia (EIN) TEXAS SOCIETY OF PATHOLOGISTS ANNUAL MEETING Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Brigham and Women
Endometrial Neoplasia, Including Endometrial Intraepithelial Neoplasia (EIN) TEXAS SOCIETY OF PATHOLOGISTS ANNUAL MEETING Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Brigham and Women
CASE 4 21/07/2017. Ectopic Prostatic Tissue in Cervix. Female 31. LLETZ for borderline nuclear abnormalities
 Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
JMSCR Vol 05 Issue 11 Page November 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.78 A Histomorphological Study of Carcinoma
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.78 A Histomorphological Study of Carcinoma
Ovarian carcinoma classification. Robert A. Soslow, MD
 Ovarian carcinoma classification Robert A. Soslow, MD soslowr@mskcc.org WHO classification Serous Mucinous Endometrioid Clear cell Transitional Squamous Mixed epithelial Undifferentiated Introduction Rationale
Ovarian carcinoma classification Robert A. Soslow, MD soslowr@mskcc.org WHO classification Serous Mucinous Endometrioid Clear cell Transitional Squamous Mixed epithelial Undifferentiated Introduction Rationale
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Section 1. Biology of gynaecological cancers: our current understanding
 Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Proliferative Epithelial lesions of the Breast. Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London
 Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
ESS: Pathologic Insights
 GEIS XVI INTERNATIONAL SYMPOSIUM Seville 4th October 2018 ESS: Pathologic Insights Sílvia Bagué The Royal Marsden Hospital London (United Kingdom) I have no conflicts of interest Endometrial stromal sarcoma
GEIS XVI INTERNATIONAL SYMPOSIUM Seville 4th October 2018 ESS: Pathologic Insights Sílvia Bagué The Royal Marsden Hospital London (United Kingdom) I have no conflicts of interest Endometrial stromal sarcoma
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Tinh hoàn
 Tinh hoàn Tinh hoàn Tinh hoàn Tiền liệt tuyến Tiền liệt tuyến Mào tinh hoàn Mào tinh hoàn Túi tinh Túi tinh Túi tinh Túi tinh So-called cystadenoma of seminal vesicle. Gross appearance of granulomatous
Tinh hoàn Tinh hoàn Tinh hoàn Tiền liệt tuyến Tiền liệt tuyến Mào tinh hoàn Mào tinh hoàn Túi tinh Túi tinh Túi tinh Túi tinh So-called cystadenoma of seminal vesicle. Gross appearance of granulomatous
PRM Associated Endometrial Change Introduction & Illustrations 12-Feb-2012
 Introductory Remarks: These images are from clinical trial endometrial samples collected by catheter biopsy. They are presented with a low power section view with selected higher power images to show detailed
Introductory Remarks: These images are from clinical trial endometrial samples collected by catheter biopsy. They are presented with a low power section view with selected higher power images to show detailed
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
EQA circulation 35 educational cases. Dr. A Graham Aberdeen Royal Infirmary
 EQA circulation 35 educational cases Dr. A Graham Aberdeen Royal Infirmary Case E1 Female 52 Polypoid mass right side of cervix, adjacent to os 70 Biphasic lesion 4 No answer 3 Prolapsed tube 2 Endometriosis
EQA circulation 35 educational cases Dr. A Graham Aberdeen Royal Infirmary Case E1 Female 52 Polypoid mass right side of cervix, adjacent to os 70 Biphasic lesion 4 No answer 3 Prolapsed tube 2 Endometriosis
3/24/2017. Disclosure of Relevant Financial Relationships. Mixed Epithelial Endometrial Carcinoma. ISGyP Endometrial Cancer Project
 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Diagnostic problems in uterine smooth muscle tumors
 Diagnostic problems in uterine smooth muscle tumors Marina Kos Ljudevit Jurak Clinical Department of Pathology, Clinical Hospital Center Sestre milosrdnice, Zagreb Institute of Pathology, University of
Diagnostic problems in uterine smooth muscle tumors Marina Kos Ljudevit Jurak Clinical Department of Pathology, Clinical Hospital Center Sestre milosrdnice, Zagreb Institute of Pathology, University of
Pathological Classification of Hepatocellular Carcinoma
 3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Cytology and Surgical Pathology of Gynecologic Neoplasms
 Cytology and Surgical Pathology of Gynecologic Neoplasms Current Clinical Pathology ANTONIO GIORDANO, MD, PHD SERIES EDITOR For further titles published in this series, go to http://www.springer.com/springer/series/7632
Cytology and Surgical Pathology of Gynecologic Neoplasms Current Clinical Pathology ANTONIO GIORDANO, MD, PHD SERIES EDITOR For further titles published in this series, go to http://www.springer.com/springer/series/7632
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis
 In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis Rouba Ali-Fehmi,MD The Karmanos Cancer Institute, Wayne State University School of Medicine Global incidence of cervical
In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis Rouba Ali-Fehmi,MD The Karmanos Cancer Institute, Wayne State University School of Medicine Global incidence of cervical
Enterprise Interest None
 Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas. W Glenn McCluggage Belfast, Northern Ireland
 The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas W Glenn McCluggage Belfast, Northern Ireland Enterprise Interest None OVARIAN SEROUS CARCINOMA (OSC) RECENT DEVELOPMENTS
The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas W Glenn McCluggage Belfast, Northern Ireland Enterprise Interest None OVARIAN SEROUS CARCINOMA (OSC) RECENT DEVELOPMENTS
Female Genital Tract Lab. Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan
 Female Genital Tract Lab Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan Ovarian Pathology A 20-year-old female presented with vague left pelvic pain. Pelvic exam revealed
Female Genital Tract Lab Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan Ovarian Pathology A 20-year-old female presented with vague left pelvic pain. Pelvic exam revealed
CLINICAL SIGNIFICANCE OF BENIGN EPITHELIAL CHANGES
 Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Mesothelioma: diagnostic challenges from a pathological perspective. Naseema Vorajee August 2016
 Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens
 How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
Recent advances in breast cancers
 Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Recent advances in breast cancers Breast cancer is a hetrogenous disease due to distinct genetic alterations. Similar morphological subtypes show variation in clinical behaviour especially in response
Histopathology: Cervical HPV and neoplasia
 Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
PAPILLARY PROLIFERATION OF THE ENDOMETRIUM: A BENIGN LESION SIMULATING ADENOCARCINOMA.
 PAPILLARY PROLIFERATION OF THE ENDOMETRIUM: A BENIGN LESION SIMULATING ADENOCARCINOMA. Teresa Pusiol, Maria Grazia Zorzi, Doriana Morichetti U.O. Anatomia Patologica Ospedale S. Maria del Carmine Rovereto
PAPILLARY PROLIFERATION OF THE ENDOMETRIUM: A BENIGN LESION SIMULATING ADENOCARCINOMA. Teresa Pusiol, Maria Grazia Zorzi, Doriana Morichetti U.O. Anatomia Patologica Ospedale S. Maria del Carmine Rovereto
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Important Recent Advances in Gynaecological Pathology
 Important Recent Advances in Gynaecological Pathology Sanjiv Manek Consultant Gynaecological Pathologist Oxford, UK In recent years there have been a significant number of changes in gynaecological pathology
Important Recent Advances in Gynaecological Pathology Sanjiv Manek Consultant Gynaecological Pathologist Oxford, UK In recent years there have been a significant number of changes in gynaecological pathology
CYSTIC TUMORS OF THE KIDNEY JOHN N. EBLE, M.D. CYSTIC NEPHROMA
 Page 1 CYSTIC TUMORS OF THE KIDNEY JOHN N. EBLE, M.D. Department of Pathology & Laboratory Medicine Phone (317) 274-4806 Medical Science A-128 FAX: (317) 278-2018 635 Barnhill Drive jeble @iupui.edu Indianapolis,
Page 1 CYSTIC TUMORS OF THE KIDNEY JOHN N. EBLE, M.D. Department of Pathology & Laboratory Medicine Phone (317) 274-4806 Medical Science A-128 FAX: (317) 278-2018 635 Barnhill Drive jeble @iupui.edu Indianapolis,
Received, June 29, 1904; accepted for publication
 THE AMEBICAN JOURNAL OF CLINICAL PATHOLOGY Copyright 1964 by The Williams & Wilkins Co. Vol. 42, No. 0 Printed in U.S.A. CARCINOMA IN SITU OF THE ENDOMETRIUM ISABELLE A. BUEHL, M.D., PRANK VELLIOS, M.D.,
THE AMEBICAN JOURNAL OF CLINICAL PATHOLOGY Copyright 1964 by The Williams & Wilkins Co. Vol. 42, No. 0 Printed in U.S.A. CARCINOMA IN SITU OF THE ENDOMETRIUM ISABELLE A. BUEHL, M.D., PRANK VELLIOS, M.D.,
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Spindle Cell Lesions Of The Breast. Emad Rakha Professor of Breast Pathology and Consultant Pathologist
 Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
SMOOTH MUSCLE TUMOURS
 SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as