Advances in Lipid Management
|
|
|
- Cornelia Flowers
- 5 years ago
- Views:
Transcription
1 Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
2 Prevention of Cardiovascular Disease Essence of prevention is lifestyle-related. Diet high in fruits and vegetables, and lifestyle with aerobic exercise INTERHEART STUDY
3 INTERHEART Nine risk factors accounted for 90% of the risk of heart disease internationally Smoking Hypertension Diabetes Waist/hip ratio Lack of daily consumption of fruits and vegetables Physical activity Lack of consumption of alcohol Dyslipidemia Psychosocial factors Yusef Lancet. 2004;364:
4 Dyslipidemia Dyslipidemia is a major modifiable risk factor for CVD
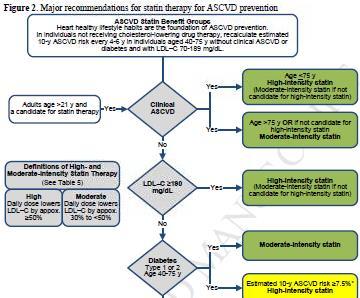
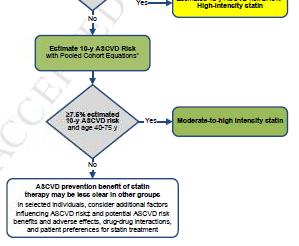
5 ASCVD Risk Benefit Groups Adults > 21 years and able to tolerate statins YES Clinical ASCVD YES Age < 75 years of age; High NO YES Intensity statin LDL > 190 mg/dl Age > 75 years; Moderate Intensity statin High Intensity statin NO Diabetes NO Moderate intensity statin ASCVD risk score is > 7.5%; High intensity statin ASCVD risk score > 7.5% and age YES Moderate to high intensity statin NO ASCVD risk benefit of statins may be less clear in other groups

6 J Am Coll Cardiol 2014;64:485 94)
7 How Does Dyslipidemia Cause Coronary Artery Disease? Complex interplay between lipids and the endothelium of the vasculature

8 Progression of Atherothrombotic Vascular Events Moore KJ, Tobas I, Cell April ; 145(3):
9 How do statins work? J Am Coll Cardiol. 2000;35(1):1-10. doi: /s (99)
10 Statins reduce MI and CVD mortality by 25-40% in the secondary prevention population and MI/CVA risk by similar numbers in the primary prevention population Statins should NOT be used in pregnancy and lactation
11 Statin intolerance Statin intolerance is a clinical syndrome characterized by: The inability to tolerate at least 2 statins: one statin at the lowest starting daily dose AND another statin at any daily dose, due to either objectionable symptoms (real or perceived) or abnormal lab determinations which are temporally related to statin treatment and reversible upon statin discontinuation, but reproducible by re-challenge with other known determinants being excluded* *such as hypothyroidism, interacting drugs, concurrent illnesses, significant changes in physical activity or exercise, or underlying muscle disease Guyton JR et al. J Clin Lipid : S72-S81
12 PCSK9 inhibitors Two major companies- Amgen and Sanofi/Regeneron
13 J Am Coll Cardiol. 2013;62(16): doi: /j.jacc
14 Dramatic Reductions in LDL They lower LDL cholesterol by dramatic levels, down 50% to 70% reductions of LDL cholesterol, and this effect lasts for 2 to 4 weeks of treatment. Ongoing Phase III clinical trials Outcome trial in progress
15 Familial Hypercholesterolemias (FH) Group of genetic conditions resulting in severe elevations of blood cholesterol levels FH is among the most commonly occurring genetic metabolic disorders The heterozygous form occurs in approximately 1 in people in many populations (estimated current US prevalence is 620,000) Homozygous form is quite rare, occurring in approximately 1/1 million individuals
16 Total cholesterol in heterozygous FH patients (genetic defect inherited from one parent) are typically in the range of 300 to 550 mg/dl (but sometimes lower) In homozygous FH (genetic defects inherited from both parents), range from 650 to 1000 mg/dl Hypercholesterolemia is present from childhood, leading to early development of coronary heart disease The risk of premature coronary heart disease is elevated about 20-fold in untreated FH patients FH is underdiagnosed and undertreated
17 Suspect FH when fasting LDL in adults > 20 years is > 190 (mg/dl) or non-hdl > 220 mg/dl In those < 20 years, suspect FH when LDL-C > 160 mg/dl or non-hdl > 190 mg/dl
18 Treatment of FH Individuals with FH have a very high lifetime risk of coronary heart disease and are at very high risk of premature coronary heart disease Early treatment is highly beneficial. Long-term drug therapy of patients with FH can substantially reduce or remove the excess lifetime risk of coronary heart disease due to the genetic disorder and can lower coronary heart disease event rates in FH patients to levels similar of those in the general population
19 FH requires lifelong treatment and regular follow up Both children and adults with LDL-C >190 mg/dl (or non-hdl > 220 mg/dl) after lifestyle changes will require drug therapy. For adult FH patients (> 20 years of age), drug treatment to achieve an LDL-C reduction of > 50% should be initiated. Statins should be the initial treatment for all adults with FH
20 For adult FH patients, initial treatment is the use of moderate to high doses of high potency statins (rosuvastatin, atorvastatin). Low potency statins are generally inadequate for FH patients For patients who cannot use a statin, most will require combination therapy (ezetimibe, niacin, bile acid sequestrants) Intensify drug treatment in higher risk patients (diabetes, current smoking, clinically evident coronary heart disease, a FH of early coronary heart disease, high lipoprotein (a)).
21 Homozygous FH Lomitapide (oral microsomal triglyceride transfer protein inhibitor) approved for the treatment of patients with homozygous FH. MTP plays a role in the assembly and secretion of triglyceride-rich apolipoprotein B-containing lipoproteins Mipomersen is a second-generation antisense oligonucleotide that inhibits production of apolipoprotein B. Given as a weekly injection, it lowers LDL-C levels in humans and is approved for use in patients with homozygous FH
22 LDL-Apheresis LDL-apheresis is a US FDA-approved medical therapy for FH patients who are not at their LDL-C treatment goal or who have ongoing symptomatic disease LDL apheresis is done weekly or biweekly and lowers LDL-C levels by up to 80% acutely and 30% chronically.
23 Residual risk
24 New Data Demonstrating that VLDL-c (remnant cholesterol) is associated with a two-fold greater risk than LDL-c Varbo et al. Journal of the American College of Cardiology
25 Management of High TG Limited data on who to treat Mild to moderate hypertg ( , even up to 1000), main indication for therapy is reduction of CVD risk Lifestyle Statins not most effective at lowering TG, most effective agents at lowering CVD risk No trial of statins has looked specifically at patients with normal LDL and elevated TG.
26 Reduce TG, reduce CVD risk? Uncertain whether pharmacologic therapy targeted at reducing TG levels will reduce CVD risk. Several trials raise the possibility that pharmacologic treatment targeting TG will provide benefit Helsinki Heart Study, CVD risk was highest in the cohort with a TG > 201 and an LDL/HDL > 5.0; a benefit from gemfibrozil was confined to this high risk group 1 1. Manninen Circulation. 1992;85(1):37.
27 VA-HIT- assessed efficacy of gemfibrozil in patients with low HDL (<40), relatively low LDL (<140) and TG levels <300. Gemfibrozil raised HDL by 6%, lowered TG by 31%, and had no significant effect on LDL. At five years, there was an absolute risk reduction of 4.4% in nonfatal MI or death from coronary cause, more than could be explained by the increase in HDL 1 ACCORD Lipid fenofibrate showed no overall benefit when added to a statin in patients with DM2, but did improve outcomes in a subset of patients with both elevated TG (>204) and low HDL 2 Similar suggestions of benefit in such subgroups in the FIELD trial 3 and the Bezafibrate Infarction Prevention trial 4 1. Rubins HB, N Engl J Med. 1999;341(6): ACCORD Study Group, N Engl J Med. 2010;362(17): Keech A Lancet. 2005;366(9500): Bezafibrate Infarction Prevention (BIP) study Circulation. 2000;102(1):21.
28 Do patients with elevated TG at baseline benefit from pharmocologic monotherapy? In statin trials, subgoups with high TG had higher risk in 4S, the CARE trial, WOSCOPS, AFCAPS- TEXCAPS and TNT and to have greater CVD risk reduction with lipid therapy in 4S and CARE. But CVD risk reduction similar across TG levels in LIPID, HPS and WOSCOPS and actually worse in patients with metabolic syndrome in the Anglo- Scandinavian Cardiac Outcome Trial. Thus, in patients with hypertg, statin therapy may be beneficial in the setting of an LDL level that merits treatment. Triglycerides and Cardiovascular Disease: A Scientific Statement from the American Heart Association; Circulation 2011
29 Statins benefit regardless of TG level, however fibrates more commonly show more benefit in those with high TG These high CVD risk subgroups benefited in Helsinki Heart Study, Bezafibrate trial and FIELD. In VA-HIT, fibrates reduced CVD risk across all categories of baseline TG The ACCORD trial (negative overall in the addition of fibrate to statin) did show benefit in the subgroup with elevated TG > 204 and low HDL Therefore, the aggregate data suggest that statin or fibrate may be beneficial in patients with high TG levels, low HDL or both
30 Is a high TG level in individuals receiving pharmacologic monotherapy associated with increased CVD risk? In LIPID, each 89 mg decrease in TG in on treatment patients with pravastatin significantly decreased CVD risk by 11% In PROVE-IT TIMI 22, achieving TG < 150 was associated with a 27% decrease in CVD risk Post hoc analysis of combined data from IDEAL and TNT, CVD risk was 30% higher when ontreatment TG> 150 and 63% higher in patients in the top quintile of high TG than those in the lowest However, after adjusting for HDL, ratio of apob/apoa1, baseline glucose, BMI, HTN, T2DM and smoking eliminated the association. Thus high risk statin treated patients who continue to have elevated TG levels display an increased risk for CVD but these patients also have other metabolic abnormalities and adjustment for measures of these associated abnormalities such as non-hdl and apob decreases the predictive effect of TG.
31 Do patients with elevated TG levels while undergoing statin therapy receive additional CVD risk reduction by the addition of a second drug that targets TG or TRL? Subgroup analysis in the JELIS trial which patients received EPA vs placebo on top of a statin, indicated those with TG > 150 had high CVD risk and those combination therapy with a statin plus EPA in this high risk subgroup reduced CVD risk by 53% compared with statin monotherapy. This was despite the fact that the dose of EPA was 1.8 g/d which translated into minimal TG reduction (5% between groups) Therefore the benefit in JELIS was not a TG mediated effect
32 Trials that used statin plus niacin combination therapy have shown a reduction in coronary arteriographic progression and regression as well as a reduction in CIMT Reduction in CVD outcomes were observed in several of these studies although the event rates were low, a statin placebo group was not used and the studies were not powered nor prespecified to address CVD outcomes Limited data on the addition of a second drug to a statin; ACCORD did not show an overall benefit to the addition of a fibrate to a statin, although there was benefit in a subgroup of high TG, low HDL Stage set for AIM-HIGH and HPS2-THRIVE
33 No Trials Done To Lower TG There are no prospective trials results proving that decreasing TG prevents atherosclerosis or improves outcomes. No trial requiring hyper-tg as part of the entry criteria and specifically addressing whether a TG-decrease intervention compared to placebo reduces CV events. All we have to date are post-hoc subset analyses of CV outcomes trials that did not require elevated TG at baseline. There has never been a statin trial that addressed whether reduction of TG provided additional benefit
34 A Long-Term Outcomes Study to Assess STatin Residual risk reduction with EpaNova in high cardiovascular risk patients with Hypertriglyceridemia (STRENGTH) Patients with TG mg/dl and HDL-c < 40mg/dl at high risk for CVD. N=13,000 R EPANOVA 4 g/day Corn Oil 4 g/day Lead in 5-year follow-up 34
35 Lee, Pate et al Impact of Running 55, 137 adults in the Cooper Clinic in Texas Participants followed for 15 years Running was assessed by physical activity questionnaire Interestingly, runners had lower all-cause and CVD mortality (30% and 45% lower risk) with a 3-year life expectancy benefit. In addition, even running at slower speeds, at lower doses, defined as < 51 minutes, < 6 miles, 1 to 2 times, < 6 miles/hour, was associated with significant and similar benefit. Persistent runners over an average of 5.9 years had the most significant mortality benefit with 29% and 50% lower risk of all-cause and CVD mortality.
36 Impact of a healthy lifestyle Healthy lifestyle is associated with decreased risk for incident coronary heart disease in young women followed from 1991 to 2011 in the Nurse s Health Study. 88,940 women were followed from 1991 to Six factors were considered to define optimal lifestyle (no smoking, healthy diet, 2.5 hours a week physical activity, < 7 hours/ week television watching, healthy BMI and moderate alcohol intake). Women who engaged in all 6 healthy lifestyle choices had a 92% lower risk for coronary heart disease and a 66% lower risk for a clinical cardiovascular risk factor (diabetes, hypertension or hypercholesterolemia). (Chomistek, Chiuve et al. 2015


37 Hot off the press! Dietary Guidelines Advisory Committee
38 Conclusions 90% of MI s globally can be explained by nine risk factors LDL is causally linked to CVD PCSK9 inhibitors Familial hypercholesterolemia Statins 2013 ACC/AHA guidelines Residual risk- elevated non-hdl, high TG Lifestyle or medications for residual risk?
39 Severe hypertriglyceridemia TG > 1000 TG carried in chylomicrons and large VLDLstatins less effective at reduction Fibrates and/or fish oil preferable Higher risk patients with CVD and very high TG statin and fibrate or fish oil Lower risk patients with very high TG evidence is less clear; combination therapy versus statin alone

40 AIM-HIGH AIM-HIGH Investigators, NEJM 2011 Dec 15; 365(24):
41 ACCORD- LIPID The ACCORD Study Group N Engl J Med 2010; 362:
42
43 HPS2-THRIVE The HPS2-THRIVE Collaborative Group N Engl J Med 2014;371:
44 Outcome Data on Non-statins Drug Cholestyramine Colestipol Ezetimibe Results Effective in primary prevention (Lipid Research Clinics 1984) and secondary prevention in men (Watts 1992) Significantly reduces cardiovascular events compared to placebo (Insull 2006) No cardiac outcomes data and ezetimibe did not cause regression of carotid intima-media thickness (surrogate marker) when added to a statin (Kastelein 2008, Taylor 2009)
45 Fenofibrate Gemfibrozil In type 2 diabetics, did not reduce primary outcome of fatal MI or CHD mortality. Improved secondary outcomes of non-fatal MI and coronary revascularization, a reduction in albuminuria, reduced laser treatments for retinopathy (FIELD 2005) Added on to statin, did not lower risk of non-fatal MI, non-fatal stroke, or CV death, more than statin alone in patients with type 2 diabetes at high risk for CV disease. May be a subgroup (high TG, low HDL) that benefits (ACCORD 2010) Effective in primary prevention in men (Helsinki Heart Study 1987) and in secondary prevention in men with low HDL (VA-HIT 1999)
46 Niacin Omega-3 fatty acids Effective in secondary prevention (Coronary Drug Project 1975) Niacin and simvastatin decreased atherosclerosis, coronary death, MI, stroke, or revascularization (HATS 2001) Added on to statin, niacin decreased CIMT (ARBITER , ARBITER-6 HALTS 2009) In patients with stable CVD and LDL < 70, no benefit to addition of niacin to statin therapy (AIM-HIGH 2011) In patients with DM, CVD, PAD, the addition of niacin + laropiprant + statin vs statin did not reduce MI or CV death and increased side effects (HPS2- THRIVE) Effective in secondary prevention (GISSI-Prevenzione 2002); however, recent meta-analysis did not show that omega-3 fatty acids reduce cardiovascular events or mortality (Rizos 2012)
47 What do the guidelines say in managing hypertg
48 ATP III TG > 500- risk for pancreatitis; primary problem to address. Elevated triglycerides are an independent risk factor for CVD. Reflects atherogenic potential of triglyceride rich lipoproteins; i.e. VLDL Therefore the sum of LDL and VLDL (non-hdl) is a secondary goal of treatment. Goal non-hdl is 30 mg/dl higher than LDL goal. Management: Diet, weight loss, drug therapy (statins or addition of nicotinic acid or fibrate). NCEP ATP III
49 2013 ACC/AHA Blood Cholesterol Guidelines
50
51
52 NLA Lipid Guidelines- Draft A drug targeting triglyceride reduction should be considered for first-line therapy in those with triglycerides 500 mg/dl. Triglyceride lowering drug therapies include fibrates, high-dose omega-3 fatty acids and nicotinic acid A statin may be a reasonable first-line agent if the triglyceride concentration is 500 mg/dl but <1000 mg/dl, if no history of pancreatitis When used, drug therapy should be adequate to attain levels of atherogenic cholesterol (non-hdl-c and LDL-C) that are below the goal cut points.
53 European Guidelines 2012 Primary goal will be to achieve the LDL target based on the total CV risk As compared with the overwhelming evidence for the benefits of LDL reduction, the evidence on the benefits of lowering elevated TG levels is modest. Lifestyle improves TG. Weight reduction, regular physical activity, can reduce TG by 20-30%, mandatory for all patients with obesity, metabolic syndrome, DM2 Although the CVD risk is increased if fasting TG are > 150, the use of drugs to lower TG should only be considered in subjects with TG > 200 who cannot lower them by lifestyle measures and if the subject is at high total CV risk The available pharmacologic interventions include statins, fibrates, nicotinic acid, and n-3 PUFAs. As statins have significant effects on mortality as well as most CVD outcome parameters, these drugs are the first choice to reduce both total CVD risk and moderately elevated TG levels
54 Nonpharmacologic therapy Weight loss in obese patients Aerobic exercise Avoidance of concentrated sugars Avoidance of medications that raise TG Strict glycemic control in diabetics
55 Dietary management of high TG Mild to moderate high TG Chylomicrons originate from dietary fat; VLDL from TG from the liver Usually chylomicrons deliver their TG load to periphery quickly and moderate TG elevation from high VLDL VLDL from lypolysis (augmented by obesity, diabetes, insulin resistance) and de novo synthesis of fatty acids and TG in the liver from carbohydrates Focus of diet should be reduction in total intake and reduction in carbohydrates; also moderate exercise
56 Moderate to severe high TG (TG above 500 or 1000), clearance of chylomicrons slow, such that chylomicrons are still present from last night s meal Crucial to restrict dietary fat Diet aimed at weight loss should be avoided in patients with severe high TG, because when weight loss diet ends and refeeding begins, patients likely to develop very high TG and resultant risk of pancreatitis.
57
58 Effect of Lipid-Lowering Therapies on Triglyceride Reduction Drug % Triglyceride Reduction Fibrates Immediate-release niacin Omega Extended-release niacin Statins Ezetimibe 5-10
59 HDL Ideal levels of HDL higher in women than men (50 vs. 40) Low HDL related to the presence of CVD Causal relationship between low HDL and CVD not established It has not been proven that raising HDL is of benefit in reducing CVD risk Assaying the cholesterol content of HDL (HDL- C) may fail to adequately measure its protective effects.
60 dal-outcomes Schwartz GG et al; for dal-outcomes Investigators. Effects of dalcetrapib in patients with a recent acute coronary syndrome. NEJM. 2012;367:
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk?
 There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode Island Cardiology Center
 Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
Non-Statin Lipid-Lowering Agents M Holler - Last updated: 10/2016
 Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology
 Lipid Management Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology Clinical Director, Lipid Clinics Assistant Professor Division of Cardiovascular Medicine The Ohio State University Wexner
Lipid Management Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology Clinical Director, Lipid Clinics Assistant Professor Division of Cardiovascular Medicine The Ohio State University Wexner
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID?
 Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Hyperlipidemia and Cardiovascular Disease. Kathmandu November 2010 Harold E. Lebovitz, MD, FACE
 Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
B. Patient has not reached the percentage reduction goal with statin therapy
 Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Cholesterol Treatment Update
 Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Zuhier Awan, MD, PhD, FRCPC
 Metabolism, Atherogenic Properties and Agents to Reduce Triglyceride-Rich Lipoproteins (TRL) The Fifth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 8-11, 2019 Zuhier
Metabolism, Atherogenic Properties and Agents to Reduce Triglyceride-Rich Lipoproteins (TRL) The Fifth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 8-11, 2019 Zuhier
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Presenter Disclosure Information
 1:45 2:45pm Lipid Management: A Primary Care Perspective Presenter Disclosure Information The following relationships exist related to this presentation: Richard F. Wright, MD, FACC, has no financial relationships
1:45 2:45pm Lipid Management: A Primary Care Perspective Presenter Disclosure Information The following relationships exist related to this presentation: Richard F. Wright, MD, FACC, has no financial relationships
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies
 1. Evidence from genetic, epidemiologic and clinical studies") Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC/AHA. See American College of Cardiology/ ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors American College of Cardiology/American
Index Note: Page numbers of article titles are in boldface type. A ACC/AHA. See American College of Cardiology/ ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors American College of Cardiology/American
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
Metabolism, Atherogenic Properties and Agents to reduce Triglyceride-Rich Lipoproteins Manfredi Rizzo, MD, PhD
 Metabolism, Atherogenic Properties and Agents to reduce Triglyceride-Rich Lipoproteins Manfredi Rizzo, MD, PhD Associate Professor of Internal Medicine Faculty of Medicine, University of Palermo, Italy
Metabolism, Atherogenic Properties and Agents to reduce Triglyceride-Rich Lipoproteins Manfredi Rizzo, MD, PhD Associate Professor of Internal Medicine Faculty of Medicine, University of Palermo, Italy
UPDATES IN LIPID MANAGEMENT
 UPDATES IN LIPID 2017 Cardiovascular Symposium MANAGEMENT SUDHA RAVILLA, MD, DIPLOMATE, ABCL MEDICAL DIRECTOR CLINICAL LIPIDOLOGY TMHPP METABOLIC HEALTH CENTER INTRODUCTION CVD is STILL the No. 1 cause
UPDATES IN LIPID 2017 Cardiovascular Symposium MANAGEMENT SUDHA RAVILLA, MD, DIPLOMATE, ABCL MEDICAL DIRECTOR CLINICAL LIPIDOLOGY TMHPP METABOLIC HEALTH CENTER INTRODUCTION CVD is STILL the No. 1 cause
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
Diabetic Dyslipidemia
 Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
The Cardiovascular Institute Mount Sinai School of Medicine, New York
 The Cardiovascular Institute Mount Sinai School of Medicine, New York HDL YES HDL NO Juan Jose Badimon, Ph.D Professor of Medicine Director, Atherothrombosis Research Unit The Mount Sinai School of Medicine
The Cardiovascular Institute Mount Sinai School of Medicine, New York HDL YES HDL NO Juan Jose Badimon, Ph.D Professor of Medicine Director, Atherothrombosis Research Unit The Mount Sinai School of Medicine
Management of LDL as a Risk Factor. Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil
 Management of LDL as a Risk Factor Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Consulting for: Merck, Astra Zeneca, ISIS- Genzyme, Novo-Nordisk, BMS, Pfizer,
Management of LDL as a Risk Factor Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Consulting for: Merck, Astra Zeneca, ISIS- Genzyme, Novo-Nordisk, BMS, Pfizer,
Comprehensive Treatment for Dyslipidemias. Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium
 Comprehensive Treatment for Dyslipidemias Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium Primary Prevention 41 y/o healthy male No Medications Normal BP, Glucose and BMI Social History:
Comprehensive Treatment for Dyslipidemias Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium Primary Prevention 41 y/o healthy male No Medications Normal BP, Glucose and BMI Social History:
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk
 Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Familial Hypercholesterolemia
 Familial Hypercholesterolemia Dr.Ramzi Al-Mohammadi Assistant Professor of Medicine Interventional Cardiologist, Advanced HF and Transplant Consultant Classification of Hyperlipedemia Primary hyperlipedemia:
Familial Hypercholesterolemia Dr.Ramzi Al-Mohammadi Assistant Professor of Medicine Interventional Cardiologist, Advanced HF and Transplant Consultant Classification of Hyperlipedemia Primary hyperlipedemia:
Ezetimibe and SimvastatiN in Hypercholesterolemia EnhANces AtherosClerosis REgression (ENHANCE)
") Ezetimibe and SimvastatiN in Hypercholesterolemia EnhANces AtherosClerosis REgression (ENHANCE) Thomas Dayspring, MD, FACP Clinical Assistant Professor of Medicine University of Medicine and Dentistry
Ezetimibe and SimvastatiN in Hypercholesterolemia EnhANces AtherosClerosis REgression (ENHANCE) Thomas Dayspring, MD, FACP Clinical Assistant Professor of Medicine University of Medicine and Dentistry
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Recent Advances & Emerging Data in the Treatment of Hypertriglyceridemia. Michael Miller, MD, FACC, FAHA, FNLA
 Recent Advances & Emerging Data in the Treatment of Hypertriglyceridemia Michael Miller, MD, FACC, FAHA, FNLA Professor of Medicine, Epidemiology & Public Health University of Maryland School of Medicine
Recent Advances & Emerging Data in the Treatment of Hypertriglyceridemia Michael Miller, MD, FACC, FAHA, FNLA Professor of Medicine, Epidemiology & Public Health University of Maryland School of Medicine
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital
 Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital 1. Importance of Lowering LDL-Cholesterol in Diabetes Patients & Lipid Guidelines Prevalence of dyslipidemia in Korea Prevalence
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital 1. Importance of Lowering LDL-Cholesterol in Diabetes Patients & Lipid Guidelines Prevalence of dyslipidemia in Korea Prevalence
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Management of Post-transplant hyperlipidemia
 Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
The American Diabetes Association estimates
 DYSLIPIDEMIA, PREDIABETES, AND TYPE 2 DIABETES: CLINICAL IMPLICATIONS OF THE VA-HIT SUBANALYSIS Frank M. Sacks, MD* ABSTRACT The most serious and common complication in adults with diabetes is cardiovascular
DYSLIPIDEMIA, PREDIABETES, AND TYPE 2 DIABETES: CLINICAL IMPLICATIONS OF THE VA-HIT SUBANALYSIS Frank M. Sacks, MD* ABSTRACT The most serious and common complication in adults with diabetes is cardiovascular
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Prospective Natural-History Study of Coronary Atherosclerosis
 Introduction Review of literature from April 2010 to present Concentrated on clinical studies Categories: Atherosclerosis, Lipids, Diabetes and CVD Risk Medical Therapy Statins really could there be anything
Introduction Review of literature from April 2010 to present Concentrated on clinical studies Categories: Atherosclerosis, Lipids, Diabetes and CVD Risk Medical Therapy Statins really could there be anything
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Qué factores de riesgo lipídicos debemos controlar? En qué medida?
 Qué factores de riesgo lipídicos debemos controlar? En qué medida? Risk category High risk: CHD or CHD risk equivalents (10- year risk >20%) Moderately high risk: two or more risk factors (10-year risk
Qué factores de riesgo lipídicos debemos controlar? En qué medida? Risk category High risk: CHD or CHD risk equivalents (10- year risk >20%) Moderately high risk: two or more risk factors (10-year risk
Lipid Lowering in Patients at High Risk for Cardiovascular Disease
 Lipid Lowering in Patients at High Risk for Cardiovascular Disease Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Novel
Lipid Lowering in Patients at High Risk for Cardiovascular Disease Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Novel
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
STATIN UTILIZATION MANAGEMENT CRITERIA
 STATIN UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: HMG Co-A Reductase Inhibitors & Combinations Agents which require prior review: Advicor (niacin extended-release/lovastatin) Crestor (rosuvastatin)(5mg,10mg,
STATIN UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: HMG Co-A Reductase Inhibitors & Combinations Agents which require prior review: Advicor (niacin extended-release/lovastatin) Crestor (rosuvastatin)(5mg,10mg,
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Copyright 2017 by Sea Courses Inc.
 Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
DYSLIPIDEMIA RECOMMENDATIONS
 DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
10/15/2012. Lessons Learned from Tim Russert: Investigating Residual Risk. Tim Russert: Residual CV Risk?
 Lessons Learned from Tim Russert: Investigating Residual Risk Peter H. Jones, MD, FACP Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Houston, Texas Tim Russert:
Lessons Learned from Tim Russert: Investigating Residual Risk Peter H. Jones, MD, FACP Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Houston, Texas Tim Russert:
Treating Lipids for Prevention of CAD in Women: Matching Therapy to Risk
 TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Cholesterol Medicines New & Old: What to Use When
 Cholesterol Medicines New & Old: What to Use When Patrick E. McBride, M.D., M.P.H. Division of Cardiovascular Medicine Preventive Cardiology Program Disclosures McBride no conflicts of interest Outline
Cholesterol Medicines New & Old: What to Use When Patrick E. McBride, M.D., M.P.H. Division of Cardiovascular Medicine Preventive Cardiology Program Disclosures McBride no conflicts of interest Outline
Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane
 Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane Kostner, 2007 2008 LDL Target depends on your level of Risk Acute Plaque Rupture ACS (UA/NSTEMI/STEMI)
Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane Kostner, 2007 2008 LDL Target depends on your level of Risk Acute Plaque Rupture ACS (UA/NSTEMI/STEMI)
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus
 Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Modern Lipid Management:
 Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Lipid Guidelines Who, What, and How Low. Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute
 Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Macrovascular Management. What s next beyond standard treatment?
 Macrovascular Management What s next beyond standard treatment? Are Lifestyle Modifications Still Relevant in Diabetic Patients? Diet Omega-6 and omega-3 fatty acids have been shown to improve CVD risk
Macrovascular Management What s next beyond standard treatment? Are Lifestyle Modifications Still Relevant in Diabetic Patients? Diet Omega-6 and omega-3 fatty acids have been shown to improve CVD risk
Prof. John Chapman, MD, PhD, DSc
 Prof. John Chapman, MD, PhD, DSc Director of the Dyslipidemia and Atherosclerosis Research Unit of the National Institute for Health and Medical Research (INSERM) at the Pitié-Salpétrière Hospital in Paris
Prof. John Chapman, MD, PhD, DSc Director of the Dyslipidemia and Atherosclerosis Research Unit of the National Institute for Health and Medical Research (INSERM) at the Pitié-Salpétrière Hospital in Paris
Statin Intolerance. Jason Evanchan DO, FACC April 20 th, 2018
 Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Lipid Management: Beyond LDL
 Lipid Management: Beyond LDL Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine University of Kentucky Overview Discuss the concept of residual risk Review current evidence-based medicine
Lipid Management: Beyond LDL Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine University of Kentucky Overview Discuss the concept of residual risk Review current evidence-based medicine
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Cardiovascular Controversies: Emerging Therapies for Lowering Cardiovascular Risk
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Familial hypercholesterolaemia
 Familial hypercholesterolaemia Jaimini Cegla MRCP FRCPath PhD Consultant in Chemical Pathology and Metabolic Medicine Hammersmith Hospital Lipid Clinic 20 April 2017 An unrecognised, potentially fatal,
Familial hypercholesterolaemia Jaimini Cegla MRCP FRCPath PhD Consultant in Chemical Pathology and Metabolic Medicine Hammersmith Hospital Lipid Clinic 20 April 2017 An unrecognised, potentially fatal,
Cardiovascular disease and diabetes Vascular harmony
 Cardiovascular disease and diabetes 2018 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics
Cardiovascular disease and diabetes 2018 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics
Financial Disclosures
 1 Lipids in Type 2 Diabetes July 20, 2013 Abhimanyu Garg, M.D. Professor of Internal Medicine Chief, Division of Nutrition and Metabolic Diseases Distinguished Chair in Human Nutrition Research UT Southwestern
1 Lipids in Type 2 Diabetes July 20, 2013 Abhimanyu Garg, M.D. Professor of Internal Medicine Chief, Division of Nutrition and Metabolic Diseases Distinguished Chair in Human Nutrition Research UT Southwestern
Attainment of Combined Optimal Lipid Values With the Use of Niacin
 www.medscape.com Attainment of Combined Optimal Lipid Values With the Use of Niacin Has AIM-HIGH Closed the Book on This Debate? Tyan Thomas Clin Lipidology. 2012;7(4):389-396. Abstract and Introduction
www.medscape.com Attainment of Combined Optimal Lipid Values With the Use of Niacin Has AIM-HIGH Closed the Book on This Debate? Tyan Thomas Clin Lipidology. 2012;7(4):389-396. Abstract and Introduction
nicotinic acid 375mg, 500mg, 750mg, 1000mg modified release tablet (Niaspan ) No. (93/04) Merck
 No. (93/04) Merck") Scottish Medicines Consortium Resubmission nicotinic acid 375mg, 500mg, 750mg, 1000mg modified release tablet (Niaspan ) No. (93/04) Merck New formulation 6 January 2006 The Scottish Medicines Consortium
Scottish Medicines Consortium Resubmission nicotinic acid 375mg, 500mg, 750mg, 1000mg modified release tablet (Niaspan ) No. (93/04) Merck New formulation 6 January 2006 The Scottish Medicines Consortium