Paediatric Morphology
|
|
|
- Esmond Boone
- 6 years ago
- Views:
Transcription



1 Robyn Wells Core Haematology Pathology Queensland Central Laboratory 1
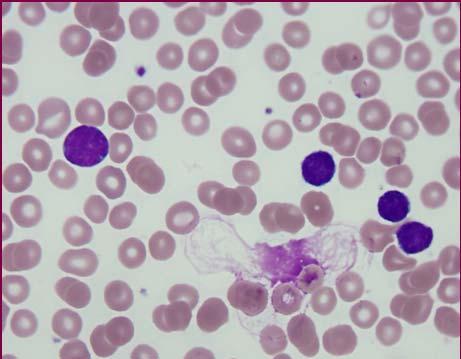
2 Normal paediatric films: Red blood cells are slightly hypochromic and microcytic in normal infants and children, compared to adult cells. Even when iron stores are normal, cells have this appearance Lower ranges for MCV and MCH for these age groups. Mild iron deficiency is common The lymphocyte count is often higher than the neutrophils (reversed differential) Majority of these are small dark normal lymphocytes. The larger, paler, granulated lymphocytes (large granular lymphocytes) are more numerous but remain at constant levels throughout childhood. Reactive lymphocytes may occur in small numbers in apparently healthy children especially in the first three years Response to subclinical viral infections and other immunological stimuli. The platelet morphology is similar to adult films. Red cell abnormalities: Low production nutritional, viral, hypoplasia Abnormal production - haemoglobinopathies, sideroblastic anaemia, CDAs, Haemolysis - AIHA, membrane disorders (HS, HE, MO), oxidative, enzyme deficiencies 2


3 Nutritional Fe deficiency Commonest anaemia of childhood Usually dietary but can be due to blood loss If not eating iron containing foods, will start at 5 6 months when iron from mum runs out This coincides with a 2-3 year period of rapid growth with peak iron requirements Megaloblastic anaemia is uncommon Can occur if nursing mother is strict vegan Also if intrinsic factor deficiency or Ab s for B12 deficiency Malabsorption may also be a cause for either B12 or folate deficiency 3


4 Parvovirus or other viruses can cause a red cell aplasia (and often neutropenia as well) EBV, viral hepatitis, HIV, varicella, and CMV also implicated Hypoplasia due to immune diseases such as SLE, syndromes such as Fanconi s and Diamond Blackfan Abnormal production includes the thalassemias and Hb defects, sideroblastic anaemia and CDA α chain disorders are detectable at birth whereas β chain variants will not manifest until 4-6 months. Other Hb opathies will be apparent at different ages moderate to severe anaemia will occur in HbSS from 4 months onwards, HbC will only cause a slight anaemia 4

5 Hereditary sideroblastic anaemia is rare with anaemia occurring from a few months to 7-8 years. It is either X-linked or autosomal recessive Acquired SA can be due to toxins such as lead, drugs or secondary to immune disorders CDA very rare, structural abnormalities of the rbc membrane Any increased RBC turnover is haemolysis may be slight (HE) or acute (AIHA) Inherited membrane disorders such as HE, HS and MO may have chronic haemolysis but also acute episodes HE spectrin defect. Precursor cells are normal in shape Usually mild except homozygous state HS - instability of the skeletal lipid bilayer results in loss of membrane as the red cell circulates through the microvasculature. Red cell picture of a mixture of normal looking cells and spherocytes it is not a really homogenous looking population unless the patient is asplenic. Can be hard to differentiate from AIHA especially in children in a haemolytic crisis 5



6 Melanesian Ovalocytosis Melanesia, Indonesia, SE Asia Oval stomatocytes with 1 or 2 transverse slits Cells are more rigid gives some protection against malaria 6
7 AIHA Relatively rare in children 1 in 80,000 Primary or secondary Primary warm reactive, PCH, cold agglutinin disease Secondary generalized auto-immune disease, immune deficiency, malignancy, medication, infection The most common primary AIHA is the warm reactive form Autoantibodies, usually IgG bind to RBC at 37 C May fix complement Extravascular haemolysis mainly in spleen Leads to splenomegaly, jaundice and anaemia Mechanism warm reactive IgG autoantibodies coat autologous red cells and may fix complement. Sensitized cells pass through spleen and RES Interact with Fc receptors and complement on macrophages Ingested by macrophages or part membrane removed spherocytes Paroxysmal cold haemoglobinuria (PCH) occurs after a viral-like illness IgG autoantibodies bind preferentially at colder temperatures Fix complement efficiently Cause intravascular haemolysis with haemoglobinuria, haemoglobinaemia and anaemia 7
 Antibody binds")

8 Cold agglutinin disease Rare can be after Mycoplasma infection IgM autoantibodies bind I/i antigens at colder temperatures Fix complement Complement-mediated intravascular or immune-mediated extravascular clearance Mechanism cold reactive (PCH and CAD) Antibody binds preferentially at 4 C and fixes complement efficiently If complement is activated to completion, intravascular haemolysis occurs If complement is deposited on the red cell but not fully activated, macrophages in the RES bind the rbc using complement receptors Clearance in the liver, rather than the spleen 8


9 Oxidative haemolysis can be due to chemicals, drugs, heavy metals Denatures the Hb which precipitates and then removed from the red cell by the RES Uncommon in children more in babies or adults Unstable Hb gives similar morphology but no oxidative cause as such Enzyme deficiencies - PK, G6PD G6PD X-linked Can have haemolytic crises triggered by oxidants or infections Favism ingestion of fava beans acute haemolysis PK highly variable with chronic haemolysis Prickle cells in film but many more after splenectomy 9




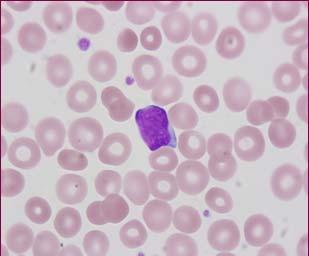
10 Childhood ALL can be very difficult to pick as the blasts can be small even microblasts Children s lymphocytes often have little cytoplasm, an inactive nucleoli or look a little clefted or convoluted 10
11 The WHO classification of precursor B- lymphoblastic leukaemia is equivalent to B-cell ALL L1 and L2 in the FAB classification and precursor T-lymphoblastic leukaemia encompasses the T-cell All L1 and L2 (FAB) Pre B-ALL occurs most commonly in children <6 years The B-cell type is the one that is harder to distinguish as it is more homogenous in appearance, small to moderately sized blasts, high N/C ratio with only a little scanty basophilic cytoplasm and inconspicuous nucleoli The T lineage blasts are larger and more heterogenous with more obvious nucleoli, varied chromatin patterns from fine to coarsely condensed and variable amounts of cytoplasm T-cell blasts can have very folded and cleaved nuclei The count is often high and the patients can present with a tumour mass The full blood count results and clinical notes may or may not be helpful. Usually at least one cell line is suppressed and anaemia and/or thrombocytopenia is a presenting feature. White cell counts can be anywhere from 1.0 to 1500 x 10 9 /L There is nearly always neutropenia 11



12 Differential diagnosis for children who present with severe cytopenias include such things as viral infections, red cell aplasia, aplastic anaemia, solid tumours, lymphomas or the rarer conditions such as Diamond Blackfan anaemia, Fanconi s anaemia or congenital dyserythropoietic anaemia 12



13 13






14 14




15 15




16 16



17 Reactive lymphocytes can vary from slightly larger round cells with basophilic cytoplasm to very large with abundant cytoplasm with basophilic rim. The chromatin pattern also varies from being diffuse to partly condensed There is always a range or spectrum of cells not a homogenous or clonal population 17







18 18






19 Acute myeloid leukaemias Morphology often misleading Flow, cytogenetics, molecular Sometimes clues in the company they keep Age, WCC, history can help 19







20 20




21 21


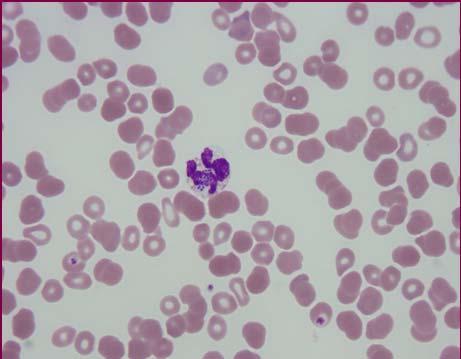
22 Definition of promyelocyte?? The malignant promyelocyte will have very variable granularity of the cytoplasm even the microgranular variant will have occasional heavily granulated cells and Auer rods or Faggott cells present. The majority of the promyelocytes will have some very fine granules often need to check under oil Nuclear shape that is distinctive (can be confused with monocytic) The microgranular variant will often have a higher WCC, but all have the tendency to DIC/bleeding presentation and complications. 22
 Both types have reniform or bilobed nuclei that can vary a lot in size The WCC for")

23 The typical or hypergranular APML features promyelocytes with densely packed granular cytoplasm and cells with Auer rods often multiple or in bundles (Faggot cells) Both types have reniform or bilobed nuclei that can vary a lot in size The WCC for hypogranular variant can be quite high up to 100 x 10 9 /L, so a lot of these reniform and bilobed cells are seen The typical form is easier to pick, but does present a challenge as they are nearly always pancytopenic on presentation, with the WCC below 4 x 10 9 /L 23




24 24




25 Other interesting stuff.. 25




26 26




27 27




28 28



29 29


30 PAEDIATRIC MORPHOLOGY WORKSHOP Case studies 1-12 Wednesday 10 th August 2011 Case 1: 12 mth M, gastro (D&V) Case 1: Other results: DAT neg, B. pertussis NR, CMV past infection, parvovirus B19 NR, toxoplasmosis NR 30




31 31



32 Blood film: Does it agree with the parameters? Yes - hypochromic, microcytic Other significant cells??elliptocytes?pencil cells?tear drops?polychromatic cells Possible causes & differential diagnosis: Fe deficiency Haemoglobinopathy 32
33 - Haemoglobinopathy RCC high/n Hb - N RDW - N MCHC - N - Iron deficiency RCC low Hb - low RDW - high MCHC - low - Fe studies: Iron 3 umol/l (9 22) Transferrin BC 109 umol/l (40-75) Transferrin 4.3 g/l ( ) Transferrin satn 3 % (115-45) Ferritin 6 ug/l (6-60) Case 2 2 yr F, CN haemolytic anaemia 33




34 34




35 35
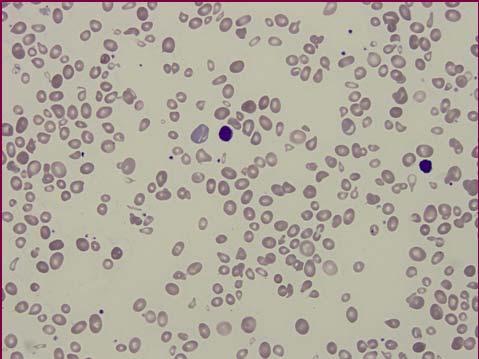
36 - Case 2 What cells are present in the film? Do they match the FBC results? What can be the cause of anaemia in a 2 yr old child? What does the presence of so many NRBC mean? - - Microcytes: Hb opathy or iron deficiency Stippling: Lead poisoning, Hb opathy, ineffective erythropoiesis Dimorphic Post transfusion, sideroblastic anaemia Spherocytes: Haemolysis, rbc membrane instability 36

37 - Increased polychromasia and NRBC: BM response, haemolysis, ineffective erythropoiesis Tear drops: Myelofibrosis, MDS, megaloblastic anaemia, HbH disease Hypochromia: Fe deficiency, Hb opathy - Fe studies: - Hb studies: Case 3: 5 y male Referred to paediatric haematology clinic No family history of anything haematological Mother: β thal minor Father: β thal minor 37


38 38



39 - Case 3: What are the significant abnormalities in the film? What might you see in the biochem results? 39
40 - Other results: Bili 34 umol/l (<20) Bili (conj) 5 umol/l (<4) LD 369 U/L ( ) - DAT: Poly 3+, IgG 3+, C3d negative Eosin-5-maleimide: Normal staining pattern consistent with haemolysis? further tests? Case 4: 2 yr F pancytopenia, Hb 30 yesterday?leukaemia 40



41 41


42 - Case 4: Causes of pancytopenia in a 2 yr old leukaemia viral aplastic anaemia nutritional drugs - - Any blasts? Any reactive lymphs? Any features of aa? Any signs of iron deficiency or megaloblastic anaemia? Any history of drugs? LD 5310 U/L ( ) 42
43 - - Extremely rare condition Imerslund- Gräsbeck syndrome Autosomal recessive Identical twin sister also has it Vitamin B12 deficiency due to selective malabsorption Megaloblastic anaemia occurs after 4 months (transplacental transfer runs out) - In about half the cases proteinuria also occurs with no signs of kidney disease Cause is defect in the receptor of the vitamin B12-intrinsic receptor complex of the ileal enterocyte. This receptor is also essential for renal protein reabsorption. Mutation is either cubilin (CUBN) gene on chr 10 or amnionless (AMN) on chr14. Responds to life-long B12 injections Case 5 2 yr M, chronic urticaria, vasculitis 43




44 44
, total bilirubin 55 umol/l (<20) mild numbers of spherocytes, moderate polychromasia and slight red")
 and AIHA.")
45 - Case 5 2 year old male presented with angioedema and hepatomegaly Hb 72 g/l and platelets 10 x 10 9 /L LD 1160 U/L ( ), total bilirubin 55 umol/l (<20) mild numbers of spherocytes, moderate polychromasia and slight red cell agglutination - - What could be causing this thrombocytopenia and haemolysis? Evan s syndrome is the combination of immune thrombocytopenic purpura (ITP) and AIHA. Autoimmune neutropenia also occurs in a minority of cases 45
46 - The clinical course is variable Often prolonged, with chronic haemolysis Relapses are common and significant mortality of 13% in a review of 99 patients Underlying causes have been proposed and include a variety of immune defects SLE, CVID and autoimmune lymphoproliferative syndrome (ALPS). - Recent evidence suggests that ALPS may be the underlying cause in a substantial proportion of cases. In ALPS there is a defect in the programmed cell death of lymphocytes which leads to massive lymphadenopathy and abnormal function of the T-cells. Other lymphoid malignancies (HD and lymphomas) and chronic infections (eg HIV and Hep C) need to be considered - Rx with T-cell immunosuppressive (mycophenolate) Now quite stable and well Blood film only occasional spherocyte and slight polychromasia Platelets normal Case 6 CN haemolysis and acute liver impairment 46



47 47



48 48


49 - Case 6 Film consistent with liver failure? Consistent with haemolysis? Which are the significant features in the film? Polychromasia, elliptocytes, target cells, spherocytes, Pappenheimer bodies, basophilic stippling, acanthocytes, blister cells, bite cells - Which are the significant features in the film? Polychromasia, elliptocytes, target cells, spherocytes, Pappenheimer bodies, basophilic stippling, acanthocytes, blister cells, bite cells What causes spherocytes, blister and bite cells? Oxidative haemolysis - - Oxidative haemolysis G6PD def, unstable Hb, chemicals, drugs, membrane damage Liver failure?wilson s disease 49


50 - Case 7 10 mth old, Haematology clinic patient First presented with pseudomonas sepsis when 8 weeks old 50




51 51

52 - Case 7 Severe neutropenia in an infant?cause - Leukaemia Viral Infection Toxins BM failure Familial/cyclical neutropenia Immune - Leukaemia blasts? Viral reactive lymphs? Infection any response? Toxins other cytopenias? BM failure other cytopenias? Familial/cyclical neutropenia -?? Immune underlying autoimmune disease? Age group? (alloimmune neonatal period) 52

53 - In this case there was infection, but no BM response G-CSF therapy response - Therefore there are stem cell precursors that are responsive to G-CSF BM no maturation beyond promyelocyte/myelocyte stage. No malignancy Kostmann s syndrome (infantile genetic agranulocytosis) Often compensatory monocytosis Infection is usual cause of death - Rx massive doses of G-CSF 30mg/kg (normal dose 5mg/kg) BMT No sibling Parents are talking about trying for nonaffected baby for cord cell donation Case 8 3y M fever, rash FBC results: Hb 118 g/l Ne x 109/L RCC 4.35 x 1012/L Ly x 109/L MCV 86 fl Mo x 109/L Hct 0.37 Eo x 109/L WBC 7.9 x 109/L Ba x 109/L Plats 104 x 109/L Meta x 109/L RDW 16.2 % Mye x 109/L MCH 27.1 pg Pro x 109/L MCHC 317 g/l Blasts x 109/L 53




54 54



55 - Case 8 What are the cells in the film? Homogeneous or pleomorphic population? Variable amounts of cytoplasm? Variable sized nucleus? Nasty or nice? 55

56 - FBC results: Hgb 118 g/l Ne 1.7 x 109/L RCC 4.35 x 1012/L Ly 6.0 x 109/L MCV 86 fl Mo 0.2 x 109/L Hct 0.37 Eo 0.1 x 109/L WBC 7.9 x 109/L Ba x 109/L Plats 104 x 109/L Meta x 109/L RDW 16.2 % Mye x 109/L MCH 27.1 pg Pro x 109/L MCHC 317 g/l Blasts x 109/L - Diagnosis? - - Diagnosis? Viral infection (EBV negative) 56



57 Case 9 14 mth F CN anaemia, Hx viral illness 57



58 - Case 9 Usual questions!! Do the cells look normal? Any signs of infection/malignancy/haemolysis/nutritional deficiency/viral infection? 58

59 - What can cause the anaemia and neutropenia??bm failure platelets normal?viral no reactive lymphs?drugs hope not BM aspirate Viral studies on BM: 59



60 - Case 10 2 y M, easy bruising Post transfusion and G-CSF Now completely well 6 months later TEC and immune neutropenia 60




61 61



62 - Case 10 - Any signs of infection/reactive process/haem disorder? Any characteristic features of a particular disorder? What could be the differential diagnosis? What are the abnormal FBC parameters? Cause in a 2 yr old for these results? 62




63 - Acute or chronic? What WHO classification? Is this usual in a 2 yr old? Case day M bronchiolitis/pneumonia 63



64 64

 Creat 148 (36-99) Haemolysis occurring LD 3610 (125-735) 3 days later")
65 - Case 11 WCC 65.4, Hb 63, plts 173, neuts 30, lymphs 21.8 Film features? High WCC reactive or disorder? RBC changes what can cause these? - Renal function not too bad. Worst results: Urea 14.0 ( ) Creat 148 (36-99) Haemolysis occurring LD 3610 ( ) 3 days later plats were Diagnosis?? 65


66 - - NPA B. pertussis DNA Detected HUS/TTP can occur secondary to malignancy, infections etc Cells fragmented as they push through thrombus formed due to exotoxin-induced endothelial damage Usually diarrhoea associated E. coli or S. dysenteriae Occasionally URTI <4 yrs age Case 12 4y F, pale, unwell 66




67 67



68 - FBC what is low? Neutrophils 9% or





69 - - What is most likely? Morphology? Appearance of cells?
70 - Precursor B-ALL Markers: positive for CD10, CD19, CD20 (v), CD34, CD38, HLA-DR, CD79a No cytogenetics abnormality detected, but very poor sample 70
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust
 Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Hematopathology Lab. Third year medical students
 Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Anemia (3).ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh
.ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh") Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi
.ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi") Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
EDUCATIONAL COMMENTARY BLOOD CELL IDENTIFICATION
 EDUCATIONAL COMMENTARY BLOOD CELL IDENTIFICATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
EDUCATIONAL COMMENTARY BLOOD CELL IDENTIFICATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES
 namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF BIOMEDICAL SCIENCES QUALIFICATION CODE: SOBBMS LEVEL: 6 COURSE
namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF BIOMEDICAL SCIENCES QUALIFICATION CODE: SOBBMS LEVEL: 6 COURSE
Year 2003 Paper two: Questions supplied by Tricia
 QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
Hematology Unit Lab 1 Review Material
 Hematology Unit Lab 1 Review Material - 2018 Objectives Laboratory instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Hematology Unit Lab 1 Review Material - 2018 Objectives Laboratory instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Drop of Blood Unravels Mysteries. Prof. Salma Afrose Department of Hematology Dhaka Medical College
 Drop of Blood Unravels Mysteries Prof. Salma Afrose Department of Hematology Dhaka Medical College Peripheral Blood Film (PBF) PBF is a laboratory workup that involves cytology of Peripheral blood cell
Drop of Blood Unravels Mysteries Prof. Salma Afrose Department of Hematology Dhaka Medical College Peripheral Blood Film (PBF) PBF is a laboratory workup that involves cytology of Peripheral blood cell
Blood Cell Identification Graded
 BCP-21 Blood Cell Identification Graded Case History The patient is a 37-year-old female with a history of multiple sickle cell crises. She now presents with avascular necrosis of the left hip. Laboratory
BCP-21 Blood Cell Identification Graded Case History The patient is a 37-year-old female with a history of multiple sickle cell crises. She now presents with avascular necrosis of the left hip. Laboratory
HAEMOLYTIC ANAEMIA. Dr. Hasan Fahmawi, MRCP(London), FRCP(Edin) Consultant Physician
, FRCP(Edin) Consultant Physician") HAEMOLYTIC ANAEMIA Dr. Hasan Fahmawi, MRCP(London), FRCP(Edin) Consultant Physician Haemolysis Definition shortening of the normal red blood lifespan of 120 days Increase in unconjugated bilirubin, increased
HAEMOLYTIC ANAEMIA Dr. Hasan Fahmawi, MRCP(London), FRCP(Edin) Consultant Physician Haemolysis Definition shortening of the normal red blood lifespan of 120 days Increase in unconjugated bilirubin, increased
Faculty of Medicine Dr. Tariq Aladily
 Iron deficiency anemia The most common anemia worldwide Only 10% of ingested iron is absorbed Most dietary iron occurs in meat products Absorbed in duodenum Hepcidin By inhibiting ferroportin, hepcidin
Iron deficiency anemia The most common anemia worldwide Only 10% of ingested iron is absorbed Most dietary iron occurs in meat products Absorbed in duodenum Hepcidin By inhibiting ferroportin, hepcidin
Extra Notes 3. Warm. In the core (center) of the body, where the temperature is 37 C.
 of the body, where the temperature is 37 C.") Extra Notes 3 *The numbers of the slides are according to the last year slides. Slide 33 Autoimmune hemolytic anemia : Abnormal circulating antibodies that target normal antigen on the RBC and cause lysis.
Extra Notes 3 *The numbers of the slides are according to the last year slides. Slide 33 Autoimmune hemolytic anemia : Abnormal circulating antibodies that target normal antigen on the RBC and cause lysis.
HEMATOLOGIC MORPHOLOGY- AECOM HEMATOLOGY COURSE
 Log Out Help current login :lcytryn@montefiore.org HEMATOLOGIC MORPHOLOGY- AECOM HEMATOLOGY COURSE Lawrence Cytryn, M.D. - Course Director 1998 Edward Burns, M.D. Images used by permission within AECOM
Log Out Help current login :lcytryn@montefiore.org HEMATOLOGIC MORPHOLOGY- AECOM HEMATOLOGY COURSE Lawrence Cytryn, M.D. - Course Director 1998 Edward Burns, M.D. Images used by permission within AECOM
Does Morphology Matter in 2017
 Does Morphology Matter in 2017 ISLH May 2017 Kathryn Foucar Distinguished Professor Emerita kfoucar@salud.unm.edu Objectives Recognize unique RBC and WBC abnormalities in non-neoplastic disorders Learn
Does Morphology Matter in 2017 ISLH May 2017 Kathryn Foucar Distinguished Professor Emerita kfoucar@salud.unm.edu Objectives Recognize unique RBC and WBC abnormalities in non-neoplastic disorders Learn
Evaluation of Anemia. Md. Shafiqul Bari Associate professor (Medicine) SOMC
 SOMC") Evaluation of Anemia Md. Shafiqul Bari Associate professor (Medicine) SOMC Definition Anemia is operationally defined as a reduction in one or more of the major RBC measurements Hemoglobin concentration
Evaluation of Anemia Md. Shafiqul Bari Associate professor (Medicine) SOMC Definition Anemia is operationally defined as a reduction in one or more of the major RBC measurements Hemoglobin concentration
Borderline cytopenias. Dr Taku Sugai Consultant Haematologist
 Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
EDUCATIONAL COMMENTARY DIFFERENTIATING IMMATURE PERIPHERAL BLOOD CELLS
 Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Continuing Education on the left side of the
Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Continuing Education on the left side of the
Blood Cell Identification Graded
 Blood Cell Identification Graded Case History The patient was a five-day-old girl with an elevated unconjugated bilirubin and a weakly positive direct antiglobulin test (DAT). Her CBC showed: WBC = 11.0
Blood Cell Identification Graded Case History The patient was a five-day-old girl with an elevated unconjugated bilirubin and a weakly positive direct antiglobulin test (DAT). Her CBC showed: WBC = 11.0
Anemia. A case-based approach. David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017
 Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
Tim R. Randolph. PhD, MT(ASCP) Chair and Associate Professor Department of Biomedical Laboratory Science Saint Louis University
 Chair and Associate Professor Department of Biomedical Laboratory Science Saint Louis University") Tim R. Randolph. PhD, MT(ASCP) Chair and Associate Professor Department of Biomedical Laboratory Science Saint Louis University Anemias Over 30 types Myeloproliferative Neoplasm Polycythemia Leukemia AML:M6
Tim R. Randolph. PhD, MT(ASCP) Chair and Associate Professor Department of Biomedical Laboratory Science Saint Louis University Anemias Over 30 types Myeloproliferative Neoplasm Polycythemia Leukemia AML:M6
EDUCATIONAL COMMENTARY MORPHOLOGIC CHANGES IN PERIPHERAL BLOOD CELLS
 EDUCATIONAL COMMENTARY MORPHOLOGIC CHANGES IN PERIPHERAL BLOOD CELLS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY MORPHOLOGIC CHANGES IN PERIPHERAL BLOOD CELLS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Haemolytic anaemias. Dr. J Potgieter Department of Haematology NHLS Tshwane Academic Division
 Haemolytic anaemias Dr. J Potgieter Department of Haematology NHLS Tshwane Academic Division Red Cell Destruction Extravascular in macrophages of RES (BM, liver, spleen) Haem to iron and protoporphyrin
Haemolytic anaemias Dr. J Potgieter Department of Haematology NHLS Tshwane Academic Division Red Cell Destruction Extravascular in macrophages of RES (BM, liver, spleen) Haem to iron and protoporphyrin
Red cell disorder. Dr. Ahmed Hasan
 Red cell disorder Dr. Ahmed Hasan Things to be learned in this lecture Definition and clinical feature of anemia. Classification of anemia. Know some details of microcytic anemia Question of the lecture:
Red cell disorder Dr. Ahmed Hasan Things to be learned in this lecture Definition and clinical feature of anemia. Classification of anemia. Know some details of microcytic anemia Question of the lecture:
General Characterisctics
 Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
Interpreting the CBC. Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired
 Interpreting the CBC Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired The CBC 3 Cell Lines RBCs WBCs Platelets Assess general health Make
Interpreting the CBC Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired The CBC 3 Cell Lines RBCs WBCs Platelets Assess general health Make
Interpreting Blood Tests Part 1. Dr Andrew Smith
 Interpreting Blood Tests Part 1 Dr Andrew Smith Outline Part 1 (This Week) Introduction Which Tube!?! FBCs U+Es Part 2 (Next Week): More Electrolytes LFTs Clotting Extras Introduction Bloods are a core
Interpreting Blood Tests Part 1 Dr Andrew Smith Outline Part 1 (This Week) Introduction Which Tube!?! FBCs U+Es Part 2 (Next Week): More Electrolytes LFTs Clotting Extras Introduction Bloods are a core
FBC interpretation. Dr. Gergely Varga
 FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TEST PROGRAM Glass Slide - November 2016
 NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TEST PROGRAM Glass Slide - November 2016 Results from this proficiency test event are available at: http://www.wadsworth.org/regulatory/clep/pt/summaries SLIDE
NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TEST PROGRAM Glass Slide - November 2016 Results from this proficiency test event are available at: http://www.wadsworth.org/regulatory/clep/pt/summaries SLIDE
Proper Slide Preparation
 Hematology Essentials: A Foundation for WBC Review Using Case Studies Christine Hinz, MS, MLS(ASCP) CM Proper Slide Preparation smooth, homogenous film 1/2 to 3/4 the slide length straight feather edge
Hematology Essentials: A Foundation for WBC Review Using Case Studies Christine Hinz, MS, MLS(ASCP) CM Proper Slide Preparation smooth, homogenous film 1/2 to 3/4 the slide length straight feather edge
Dairion Gatot, Soegiarto Ganie, Savita Handayani. Divisi Hematologi & Onkologi Medik Departemen Ilmu Penyakit Dalam FK-USU/RS H.Adam Malik Medan 2009
 HAEMOLYTIC ANAEMIA Dairion Gatot, Soegiarto Ganie, Savita Handayani. Divisi Hematologi & Onkologi Medik Departemen Ilmu Penyakit Dalam FK-USU/RS H.Adam Malik Medan 2009 WHEN BY THEN Hb 9 g% transfusion
HAEMOLYTIC ANAEMIA Dairion Gatot, Soegiarto Ganie, Savita Handayani. Divisi Hematologi & Onkologi Medik Departemen Ilmu Penyakit Dalam FK-USU/RS H.Adam Malik Medan 2009 WHEN BY THEN Hb 9 g% transfusion
SESSION 1 Reactive cytopenia and dysplasia
 SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
Rory McCulloch. Specialty Trainee Haematology Royal Devon & Exeter Hospital
 Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
MORPHOLOGY OF BONE MARROW ASPIRATES. Dr.Prasanna N Kumar Head Department of Pathology, Oman Medical College, Oman
 MORPHOLOGY OF BONE MARROW ASPIRATES Dr.Prasanna N Kumar Head Department of Pathology, Oman Medical College, Oman BONE MARROW ASPIRATION Sites Sternum Anterior or posterior iliac spines Aspiration from
MORPHOLOGY OF BONE MARROW ASPIRATES Dr.Prasanna N Kumar Head Department of Pathology, Oman Medical College, Oman BONE MARROW ASPIRATION Sites Sternum Anterior or posterior iliac spines Aspiration from
Participants Identification No. % Evaluation. Mitotic figure Educational Erythrocyte precursor, abnormal 1 0.
 Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
Kathleen Finnegan MS MT(ASCP)SHCM
SHCM") Kathleen Finnegan MS MT(ASCP)SHCM Discuss the history of hematology automation and digital differentials. Discuss the HemoFAXS Hematology Analysis System by Tissue Gnostics. Review automated microscopy
Kathleen Finnegan MS MT(ASCP)SHCM Discuss the history of hematology automation and digital differentials. Discuss the HemoFAXS Hematology Analysis System by Tissue Gnostics. Review automated microscopy
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Morphology Case Study. Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital
 Morphology Case Study Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital 41 year old male presented to GP for routine check-up in May 2011. FBC Results:
Morphology Case Study Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital 41 year old male presented to GP for routine check-up in May 2011. FBC Results:
Year 2002 Paper two: Questions supplied by Jo 1
 Year 2002 Paper two: Questions supplied by Jo 1 Question 70 A 25 year old previously well male student presents with recent exertional dyspnoea, epistaxis and bruising. There is no history of medication,
Year 2002 Paper two: Questions supplied by Jo 1 Question 70 A 25 year old previously well male student presents with recent exertional dyspnoea, epistaxis and bruising. There is no history of medication,
(anemia) ก hemoglobin concentration, hematocrit deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2
 ก hemoglobin concentration, hematocrit deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2") ก ก. ก ก.. ก (anemia) ก hemoglobin concentration, hematocrit ก ก ก 2 Standard deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2 Hemoglobin hematocrit MCV (g/dl) (%) (fl) ( ) 0.5-1.9
ก ก. ก ก.. ก (anemia) ก hemoglobin concentration, hematocrit ก ก ก 2 Standard deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2 Hemoglobin hematocrit MCV (g/dl) (%) (fl) ( ) 0.5-1.9
EDUCATIONAL COMMENTARY DISTINGUISHING MORPHOLOGIC LOOK-ALIKES
 EDUCATIONAL COMMENTARY DISTINGUISHING MORPHOLOGIC LOOK-ALIKES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY DISTINGUISHING MORPHOLOGIC LOOK-ALIKES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
MDS 101. What is bone marrow? Myelodysplastic Syndrome: Let s build a definition. Dysplastic? Syndrome? 5/22/2014. What does bone marrow do?
 101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
The patient had a mild splenomegaly but no obvious lymph node enlargement. The consensus phenotype obtained from part one of the exercise was:
 Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Hematologic changes in systemic diseases. Chittima Sirijerachai
 Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS
 QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS WHAT IS TRUE AND WHAT IS FALSE? Questions 1 Iron deficiency anemia a) Is usually associated with a raised MCV. b) The MCH is usually low. c) Is most commonly due
QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS WHAT IS TRUE AND WHAT IS FALSE? Questions 1 Iron deficiency anemia a) Is usually associated with a raised MCV. b) The MCH is usually low. c) Is most commonly due
Haematologist-reviewed peripheral blood smear in paediatric practice
 Singapore Med J 2018; 59(2): 64-68 https://doi.org/10.11622/smedj.2018013 Haematologist-ed peripheral blood smear in paediatric practice Anselm Chi-wai Lee, MBBS, FAMS ABSTRACT Manual examination of the
Singapore Med J 2018; 59(2): 64-68 https://doi.org/10.11622/smedj.2018013 Haematologist-ed peripheral blood smear in paediatric practice Anselm Chi-wai Lee, MBBS, FAMS ABSTRACT Manual examination of the
Acute Lymphoblastic Leukaemia
 Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology
Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology
Approach to a pale child
 Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Common Haematological Problems in Primary Care
 23 rd March 2019 GP Hot Topics In Primary Care Common Haematological Problems in Primary Care Dr Samar Kulkarni Consultant Haematologist-Oncologist and The Christie Private Care Manchester, UK. Haematology?
23 rd March 2019 GP Hot Topics In Primary Care Common Haematological Problems in Primary Care Dr Samar Kulkarni Consultant Haematologist-Oncologist and The Christie Private Care Manchester, UK. Haematology?
THE KENYA POLYTECHNIC UNIVERSITY COLLEGE
 THE KENYA POLYTECHNIC UNIVERSITY COLLEGE SCHOOL OF HEALTH SCIENCES AND TECHNOLOGY DEPARTMENT OF BIOMEDICAL LABORATORY SCIENCES AND TECHNOLOGY DIPLOMA IN MEDICAL LABORATORY SCIENCE END OF YEAR 1 EXAMINATION
THE KENYA POLYTECHNIC UNIVERSITY COLLEGE SCHOOL OF HEALTH SCIENCES AND TECHNOLOGY DEPARTMENT OF BIOMEDICAL LABORATORY SCIENCES AND TECHNOLOGY DIPLOMA IN MEDICAL LABORATORY SCIENCE END OF YEAR 1 EXAMINATION
AIHA The Laboratory Perspective on Testing. Tom Bullock Joint UK NEQAS (BTLP) & BBTS BBT SIG Annual Meeting 20 th November 2018
 & BBTS BBT SIG Annual Meeting 20 th November 2018") AIHA The Laboratory Perspective on Testing Tom Bullock Joint UK NEQAS (BTLP) & BBTS BBT SIG Annual Meeting 20 th November 2018 Auto Immune Haemolytic Anaemia (AIHA) BSH guideline (Hill et al. 2017): AIHA
AIHA The Laboratory Perspective on Testing Tom Bullock Joint UK NEQAS (BTLP) & BBTS BBT SIG Annual Meeting 20 th November 2018 Auto Immune Haemolytic Anaemia (AIHA) BSH guideline (Hill et al. 2017): AIHA
Hematology 101. Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD
 Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 93 A 16yo adolescent male presents with lethargy and lower respiratory tract infection. Physical examination shows him to be febrile, icteric
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 93 A 16yo adolescent male presents with lethargy and lower respiratory tract infection. Physical examination shows him to be febrile, icteric
Peripheral Blood Smear Examination. Momtazmanesh MD. Ped. Hematologist & Oncologist Loghman General Hospital
 1395 Peripheral Blood Smear Examination Momtazmanesh MD. Ped. Hematologist & Oncologist Loghman General Hospital Peripheral Blood Smear A peripheral blood smear is a snapshot of the cells that are present
1395 Peripheral Blood Smear Examination Momtazmanesh MD. Ped. Hematologist & Oncologist Loghman General Hospital Peripheral Blood Smear A peripheral blood smear is a snapshot of the cells that are present
PAEDIATRIC HAEMATOLOGY
 PAEDIATRIC HAEMATOLOGY AIMS National Scientific Meeting Sydney 2014 GILLIAN ROZENBERG Lymphocytes in a 1 day old neonate Lymphocyte in a 1 day old neonate DEVELOPMENT OF HAEMOPOIESIS RED CELL VALUES DURING
PAEDIATRIC HAEMATOLOGY AIMS National Scientific Meeting Sydney 2014 GILLIAN ROZENBERG Lymphocytes in a 1 day old neonate Lymphocyte in a 1 day old neonate DEVELOPMENT OF HAEMOPOIESIS RED CELL VALUES DURING
FBC CASES Vernon Louw Clinical Haematology 2010
 FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
Blood Cell Identification Graded
 Blood Cell Identification Graded Case History A 51-year-old female presented with dyspnea on exertion. Laboratory results were as follows: WBC=5.5 X 10 9 /L; Hgb=4.2 g/dl; Hct=13.9%; MCV=78.7fL; RDW=30;
Blood Cell Identification Graded Case History A 51-year-old female presented with dyspnea on exertion. Laboratory results were as follows: WBC=5.5 X 10 9 /L; Hgb=4.2 g/dl; Hct=13.9%; MCV=78.7fL; RDW=30;
Contents SECTION 1: PHYSIOLOGY OF BLOOD
 Contents SECTION 1: PHYSIOLOGY OF BLOOD Chapter 1: Overview of Physiology of Blood 1 Normal Haematopoiesis 1 Red Blood Cells 6 White Blood Cells 15 Immune System 27 Megakaryopoiesis 32 Normal Haemostasis
Contents SECTION 1: PHYSIOLOGY OF BLOOD Chapter 1: Overview of Physiology of Blood 1 Normal Haematopoiesis 1 Red Blood Cells 6 White Blood Cells 15 Immune System 27 Megakaryopoiesis 32 Normal Haemostasis
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Clinical & Laboratory Assessment
 Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
MORPHOLOGY IN ACTION. Description MINI-CASE ONE OBJECTIVES. Differential Diagnosis. Laboratory Results
 MORPHOLOGY IN ACTION Mini-case studies using morphology Bernadette Rodak, MS, MT, SH(ASCP) Professor emeritus Indiana University brodak@iupui.edu Description Mini-case studies will be used to integrate
MORPHOLOGY IN ACTION Mini-case studies using morphology Bernadette Rodak, MS, MT, SH(ASCP) Professor emeritus Indiana University brodak@iupui.edu Description Mini-case studies will be used to integrate
Haemopoiesis. Matthew Hazell Consultant Clinical Scientist Trainee
 Haemopoiesis Matthew Hazell Consultant Clinical Scientist Trainee Learning objectives Describe haemopoiesis and the development of blood cells from stem cells to mature cells Explain the roles of the different
Haemopoiesis Matthew Hazell Consultant Clinical Scientist Trainee Learning objectives Describe haemopoiesis and the development of blood cells from stem cells to mature cells Explain the roles of the different
Approaching Neutropenia in Children. SW Florida Osteopathic Medical Society: 39 th Annual Seminars in Family Practice
 Approaching Neutropenia in Children SW Florida Osteopathic Medical Society: 39 th Annual Seminars in Family Practice Approaching Neutropenia in Children Emad Salman M.D Golisano Children s Hospital of
Approaching Neutropenia in Children SW Florida Osteopathic Medical Society: 39 th Annual Seminars in Family Practice Approaching Neutropenia in Children Emad Salman M.D Golisano Children s Hospital of
Anaemia / SCD/ Bleeding disorders in Children
 Anaemia / SCD/ Bleeding disorders in Children Dr Neil Kennedy Handouts by Steve Graham Learning Outcomes Describe mechanisms of anaemia in Malawian children Discuss important causes of anaemia Describe
Anaemia / SCD/ Bleeding disorders in Children Dr Neil Kennedy Handouts by Steve Graham Learning Outcomes Describe mechanisms of anaemia in Malawian children Discuss important causes of anaemia Describe
Aplastic anamia & Sideroblastic anemia
 Hematology Lecture 7 كلية التقنيات الصحية والطبية قسم التحليالت المرضية Aplastic anamia & Sideroblastic anemia اإلعداد: ظفر جبار دهاق فؤاد APLASTIC ANEMIA What is Aplastic anemia? Aplastic anemia is a
Hematology Lecture 7 كلية التقنيات الصحية والطبية قسم التحليالت المرضية Aplastic anamia & Sideroblastic anemia اإلعداد: ظفر جبار دهاق فؤاد APLASTIC ANEMIA What is Aplastic anemia? Aplastic anemia is a
Anaemia due to a red blood cell membrane defect
 Anaemia due to a red blood cell membrane defect BHS training course 2013 1 Red blood cell membrane defect Pathologies Clinical signs Diagnostic criteria Treatment (HS) 2 The pathologies Structural organisation
Anaemia due to a red blood cell membrane defect BHS training course 2013 1 Red blood cell membrane defect Pathologies Clinical signs Diagnostic criteria Treatment (HS) 2 The pathologies Structural organisation
Microcytic Hypochromic Anemia An Approach to Diagnosis
 Microcytic Hypochromic Anemia An Approach to Diagnosis Decreased hemoglobin synthesis gives rise to microcytic hypochromic anemias. Hypochromic anemias are characterized by normal cellular proliferation
Microcytic Hypochromic Anemia An Approach to Diagnosis Decreased hemoglobin synthesis gives rise to microcytic hypochromic anemias. Hypochromic anemias are characterized by normal cellular proliferation
r). SUPPLEMENTARY/SECOND OPPORTUNITY EXAMINATION PAPER nnmlbih UNIVERSITY Sophia Blaauw INSTRUCTIONS FACULTY OF HEALTH AND APPLIED SCIENCES
. SUPPLEMENTARY/SECOND OPPORTUNITY EXAMINATION PAPER nnmlbih UNIVERSITY Sophia Blaauw INSTRUCTIONS FACULTY OF HEALTH AND APPLIED SCIENCES") r). nnmlbih UNIVERSITY OF SCIEFICE nnd TECHNOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF MEDICAL LABORATORY SCIENCES QUALIFICATION CODE: 08BMLS
r). nnmlbih UNIVERSITY OF SCIEFICE nnd TECHNOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF MEDICAL LABORATORY SCIENCES QUALIFICATION CODE: 08BMLS
Genetics of Thalassemia
 Genetics of Thalassemia Submitted by : Raya Samir Al- Hayaly Sura Zuhair Salih Saad Ghassan Al- Dulaimy Saad Farouq Kassir Sama Naal Salouha Zahraa Jasim Al- Aarajy Supervised by : Dr. Kawkab Adris Mahmod
Genetics of Thalassemia Submitted by : Raya Samir Al- Hayaly Sura Zuhair Salih Saad Ghassan Al- Dulaimy Saad Farouq Kassir Sama Naal Salouha Zahraa Jasim Al- Aarajy Supervised by : Dr. Kawkab Adris Mahmod
In adults, the predominant Hb (HbA) molecule has four chains: two α and two β chains. In thalassemias, the synthesis of either the α or the β chains
 molecule has four chains: two α and two β chains. In thalassemias, the synthesis of either the α or the β chains") Thalassaemias Thalassemia Thalassemia is an inherited autosomal recessive blood disease. Associated with absence or reduction in a or b globin chains. Reduced synthesis of one of the globin chains can
Thalassaemias Thalassemia Thalassemia is an inherited autosomal recessive blood disease. Associated with absence or reduction in a or b globin chains. Reduced synthesis of one of the globin chains can
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acute lymphoblastic leukemia, in India, 439 440 pediatric, global approach to, 420 424 core resources in low- and middle-income countries, 423
Note: Page numbers of article titles are in boldface type. A Acute lymphoblastic leukemia, in India, 439 440 pediatric, global approach to, 420 424 core resources in low- and middle-income countries, 423
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Classification of Anaemia
 Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities
 Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities Acute Myeloid Leukemia with recurrent cytogenetic Abnormalities -t(8;21)(q22;q22)(aml/eto) -inv(16) or t(16;16) -t(15;17) -11q23 Acute Myeloid
Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities Acute Myeloid Leukemia with recurrent cytogenetic Abnormalities -t(8;21)(q22;q22)(aml/eto) -inv(16) or t(16;16) -t(15;17) -11q23 Acute Myeloid
APPROACHING TO PANCYTOPENIA
 APPROACHING TO PANCYTOPENIA P A T C H A R E E K O M V I L A I S A K, M. D. A S S I S T A N T P R O F E S S O R D I V I S I O N O F P E D I A T R I C H E M A T O L O G Y O N C O L O G Y, D E P A R T M E
APPROACHING TO PANCYTOPENIA P A T C H A R E E K O M V I L A I S A K, M. D. A S S I S T A N T P R O F E S S O R D I V I S I O N O F P E D I A T R I C H E M A T O L O G Y O N C O L O G Y, D E P A R T M E
Case Report A Case of WarmAutoimmune HaemolyticAnaemiaPresenting with Intravascular Haemolysis
 IBIMA Publishing International Journal of Case Reports in Medicine http://www.ibimapublishing.com/journals/ijcrm/ijcrm.html Vol. 2014 (2014), Article ID 165588, 4 pages DOI: 10.5171/2014.165588 Case Report
IBIMA Publishing International Journal of Case Reports in Medicine http://www.ibimapublishing.com/journals/ijcrm/ijcrm.html Vol. 2014 (2014), Article ID 165588, 4 pages DOI: 10.5171/2014.165588 Case Report
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Red Cell Nomenclature
 Red Cell Nomenclature Prepared by Gillian Rozenberg on behalf of the RCPA Haematology QAP Date of Issue: May 2004 RED CELL NOMENCLATURE The morphological abnormalities seen in the red cell offer a key
Red Cell Nomenclature Prepared by Gillian Rozenberg on behalf of the RCPA Haematology QAP Date of Issue: May 2004 RED CELL NOMENCLATURE The morphological abnormalities seen in the red cell offer a key
Peripheral Blood Smear: Diagnostic Clues and Algorithms
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Anaemia. The symptoms of anaemia are tiredness, shortness of breath and being pale. The anaemia in CDA is very variable.
 Anaemia The symptoms of anaemia are tiredness, shortness of breath and being pale. The anaemia in CDA is very variable. In some patients, it is very mild and does not cause them significant symptoms. In
Anaemia The symptoms of anaemia are tiredness, shortness of breath and being pale. The anaemia in CDA is very variable. In some patients, it is very mild and does not cause them significant symptoms. In
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and
 Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
ADx Bone Marrow Report. Patient Information Referring Physician Specimen Information
 ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report
 Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
Adult Acute leukemia. Matthew Seftel. August
 Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
Bone marrow failure. By Zahraa Nasooh Al_Saaty
 Bone marrow failure By Zahraa Nasooh Al_Saaty Pancytopenia : Pancytopenia describes a reduction in the blood count of all the major cell lines-red cells,white cell and platelets. It has several causes
Bone marrow failure By Zahraa Nasooh Al_Saaty Pancytopenia : Pancytopenia describes a reduction in the blood count of all the major cell lines-red cells,white cell and platelets. It has several causes
Platelet and WBC disorders
 Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
THE UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PATHOLOGY HEMOLYTIC ANEMIAS. Dr. Tariq Aladily
 THE UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PATHOLOGY HEMOLYTIC ANEMIAS Third year medical students First semester Faculty 2018/2019 of Medicine Hereditary Spherocytosis Intrinsic defects
THE UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PATHOLOGY HEMOLYTIC ANEMIAS Third year medical students First semester Faculty 2018/2019 of Medicine Hereditary Spherocytosis Intrinsic defects
Laboratory Techniques. Tehran Medical Branch Islamic Azad University
 Anemia Laboratory Techniques Behzad Poopak, DCLS PhD Tehran Medical Branch Islamic Azad University bpoopak@yahoo.com Learning Objectives Review the anemia as a public health problem Review the lab tests
Anemia Laboratory Techniques Behzad Poopak, DCLS PhD Tehran Medical Branch Islamic Azad University bpoopak@yahoo.com Learning Objectives Review the anemia as a public health problem Review the lab tests
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Session 11 Disorders of Red cells. B.M.C.Randika Wimalasiri Lecturer(Probationary) Department of Medical Laboratory Sciences
 Department of Medical Laboratory Sciences") Session 11 Disorders of Red cells B.M.C.Randika Wimalasiri Lecturer(Probationary) Department of Medical Laboratory Sciences Red cells Biconcave cells carry oxygen to the peripheral tissues red colour-
Session 11 Disorders of Red cells B.M.C.Randika Wimalasiri Lecturer(Probationary) Department of Medical Laboratory Sciences Red cells Biconcave cells carry oxygen to the peripheral tissues red colour-
Candidates must answer ALL questions
 Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Indication of peripheral blood smear exmination:
 Indication of peripheral blood smear exmination: 1. For carried out differential WBC count. 2. For differential diagnosis of anemia. 3. For detection of parasites. 4. For diagnosis of leucemoid reaction.
Indication of peripheral blood smear exmination: 1. For carried out differential WBC count. 2. For differential diagnosis of anemia. 3. For detection of parasites. 4. For diagnosis of leucemoid reaction.
FLOW CYTOMETRY PRINCIPLES AND PRACTICE. Toby Eyre Consultant Haematologist Oxford University Hospitals NHS Foundation Trust June 2018
 FLOW CYTOMETRY PRINCIPLES AND PRACTICE Toby Eyre Consultant Haematologist Oxford University Hospitals NHS Foundation Trust June 2018 Aims and Objectives Principles of flow cytometry Preparation Steps involved
FLOW CYTOMETRY PRINCIPLES AND PRACTICE Toby Eyre Consultant Haematologist Oxford University Hospitals NHS Foundation Trust June 2018 Aims and Objectives Principles of flow cytometry Preparation Steps involved
2. Non- hemolytic anemias 3. Normocytic Normochromic Normocytic Normochromic Blood loss. (MCV<80 fl) (MCV fl) (MCV>100 fl)
 (MCV fl) (MCV>100 fl)") Definition of Anaemia of Anaemias Approach for diagnosis of Red cell disorders any condition resulting from a significant decrease in the total body erythrocyte mass due to decrease of Hb and or RBCs Hemoglobin
Definition of Anaemia of Anaemias Approach for diagnosis of Red cell disorders any condition resulting from a significant decrease in the total body erythrocyte mass due to decrease of Hb and or RBCs Hemoglobin
Diseases Of The Blood
 Diseases Of The Blood DR. Associate Professor Of Pathology Faculty Of Medicine Ain Shams University Red Blood Cells and Anemia RBC=4-6 million/mm 2 Hb=12-18 g/dl Oxygen Carrying Molecule Hemoglobin Tetramer:
Diseases Of The Blood DR. Associate Professor Of Pathology Faculty Of Medicine Ain Shams University Red Blood Cells and Anemia RBC=4-6 million/mm 2 Hb=12-18 g/dl Oxygen Carrying Molecule Hemoglobin Tetramer:
Laboratory for diagnosis of THALASSEMIA
 SCBM343 CLINICAL PATHOLOGY 2(1-2-3) Laboratory for diagnosis of THALASSEMIA PORNTHIP CHAICHOMPOO pornthip.chh@mahidol.ac.th Acknowledgements Dr. Pranee Winichagoon Fucharoen Ms. Pornnapa Khampan Thalassemia
SCBM343 CLINICAL PATHOLOGY 2(1-2-3) Laboratory for diagnosis of THALASSEMIA PORNTHIP CHAICHOMPOO pornthip.chh@mahidol.ac.th Acknowledgements Dr. Pranee Winichagoon Fucharoen Ms. Pornnapa Khampan Thalassemia
Normal Development. Normal Development 10/16/2012. Hematopoietic and Lymph Node Pathology. Red Blood Cell Maturation & Anemias
 Hematopoietic and Lymph Node Pathology Normal Development Red Blood Cell Maturation & Anemias Normal Development Differentiation of Hematopoietic Cells 1 Bone Marrow Bone Marrow Bone Marrow, RBC Precursors
Hematopoietic and Lymph Node Pathology Normal Development Red Blood Cell Maturation & Anemias Normal Development Differentiation of Hematopoietic Cells 1 Bone Marrow Bone Marrow Bone Marrow, RBC Precursors
Deconstructing the CBC
 Deconstructing the CBC Dr. Ann M. Wexler Solano Hematology Oncology September 10, 2017 What Are the Major Components of Blood? Red Blood Cells (also called erythrocytes) White Blood Cells (also called
Deconstructing the CBC Dr. Ann M. Wexler Solano Hematology Oncology September 10, 2017 What Are the Major Components of Blood? Red Blood Cells (also called erythrocytes) White Blood Cells (also called
Differential Blood Smear H3
 Verein für Association pour le Associazione per il medizinische Qualitätskontrolle contrôle de qualité médical controllo di qualità medico Report Differential Blood Smear H3 MQ 2015-4 MQ, Institut für
Verein für Association pour le Associazione per il medizinische Qualitätskontrolle contrôle de qualité médical controllo di qualità medico Report Differential Blood Smear H3 MQ 2015-4 MQ, Institut für