GI Grand Rounds. A A Lifetime of Abdominal Pain 12/9/2004 Tim Edwards
|
|
|
- Charlene Franklin
- 6 years ago
- Views:
Transcription
1 GI Grand Rounds A A Lifetime of Abdominal Pain 12/9/2004 Tim Edwards
2 PMH Aug 25, year old male presents to a pediatric gastroenterologist for primary complaint of anorexia, intermittent abdominal pain which occasionally awakens him at night These problems have been present for >1 year Negative UGI study EGD with mild gastritis Rx with tagamet 40mg/kg/day and caffeine free diet
3 May 19,1994 Seen for c/o abdominal pain with vomiting at bedtime Been doing well off all medications for 1 year Weight 44 lbs; height 43 inches Exam within normal limits GES T1/2 prolonged at 135 minutes Rx with Cisapride 5mg 20minutes QAC+HS for gastroparesis.
4 October 19, 1994 Seen in f/u for gastritis and GERD Doing well on Tagament and Propulsid No abdominal pain Recently started with loose stools Height 46 in, weight 47.5 lbs Exam within normal limits Propulsid stopped with recurrence of severe abdominal pain within several days
5 September 21, 1998 F/U of GERD and gastroparesis Prilosec 20mg/day and Propulsid 10mg BID-TID C/O crampy abdominal pain No vomiting 2-33 loose stools per day without blood or mucus No weight loss Height 55 inches; weight 90 lbs
6 February 25, 2003 Seen for recurrent abdominal pain associated with vomiting for three weeks Off medications for 2 years Daily epigastric/substernal pain. Pain usually postprandial. Emesis is nonbilious,, previously ingested food Lost 6 lbs Weight 121 lbs; Height 65 in Exam within normal limits Placed on bland diet and Nexium for recurrent GERD
7 August 18, 2003 Recent EGD within normal limits Biopsies normal, no celiac disease No improvement with Zelnorm 3mg BID Once per week with severe crampy abdominal pain relieved with nonbilious vomiting Weight 112 lb; height 66 inches Exam within normal limits 4H GES with T1/2 161 minutes
8 January 27, 2004 F/U GERD and gastroparesis Recurrent abdominal pain has returned Prominent regurgitation Frequent nausea No diarrhea Decreased appetite; lost 4 lbs since October Increased Nexium 40mg BID; Increased Reglan to 5 mg TID
9 February 8, 2004 Still with epigastric/substernal pain 2-2 3X/wk Will vomit when pain is severe Reglan increased to 7.5mg TID Referred to Dr Wo for evaluation and potential use of Domperidone
10 April 20, 2004 Doing well on Nexium QAM and reglan BID No N/V/abdominal pain Repeated UGI with SBFT and CT abd/pelvis were without evidence of obstruction, stricture, or IBD Blood tests were without suggestion of secondary causes of gastroparesis Trial of Domperidone 10mg TID
11 July 30, 2004 Admitted to U of L Hospital from Dr Wo s clinic for 2 days of sharp, constant, nonradiating,, epigastric pain which was relieved with vomiting No PO intake for 2 days Increase in typical GERD pain No diarrhea
12 PMH: As outlined previously. O/W negative. PSHx: : None FmHx: : Noncontributory Social Hx: Does well in school, no ETOH, drugs All: NKDA Meds: Nexium 40mg PO BID, Domperidone 10 mg PO BID ROS: 11 lb weight loss previous 3 weeks
13 Physical Exam VS: 112/ Gen: NAD HEENT: NC/AT, EOMI, anicteric, o/p without lesion Neck: No TM, no LAN CV: RRR Lungs: CTA B Abd: S/ND/minimal TTP mid epigastrium, no HSM, no masses Ext: No c/c/e Neuro: AAOX3, nonfocal.
14 Laboratory Hgb/Hct 16/46 WBC 7 Plt 284 Na 137 Cl 94 BUN 18 K 3.6 CO2 30 Cr 1.1 Ca 9 Tp 8.1 Alb 4.7 Amylase 53 Lipase 110 AST 25 ALT 24 Tbili 0.08
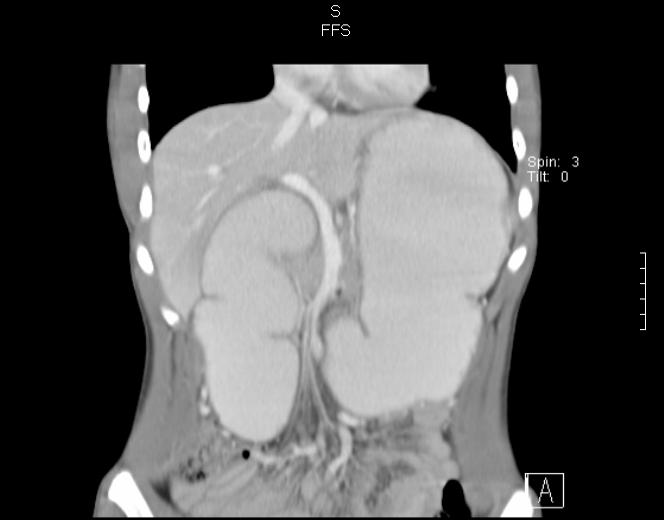
15 Imaging 7/30/2004 CT Abdomen Marked dilatation of the stomach and proximal duodenum with a transition point near the third portion of the duodenum. May be secondary to focal dysmotility versus obstruction secondary to the mesentary and its vascular structures simulating a SMA syndrome.

16
17
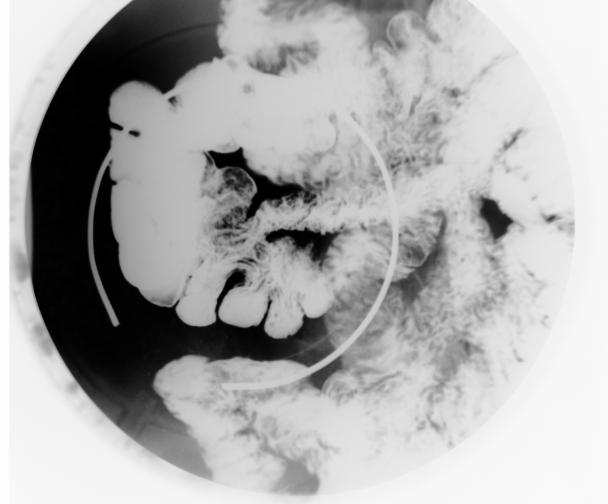
18 Upper GI limited August 3, 2004 There is a filling defect seen in the second or third portion of the duodenum which may be c/w intrinsic vs extrinsic defect, but intrinsic defect is favored. The etiology may be ectopic pancreatic tissue, large adenomatous polyp, small bowel tumor or other multiple extrinsic causes such as SMA syndrome. Non-obstructive obstructive bowel pattern

19 EGD
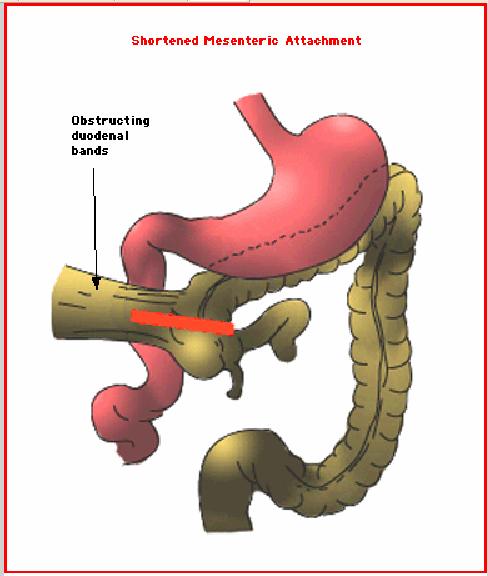
20 Definitive Therapy Given endoscopic and radiologic evidence of extrinsic lesion resulting in obstruction a surgical consultation was obtained. On 8/4/2004 the patient was taken to the OR for exploratory laparotomy for diagnosis of source of duodenal obstruction
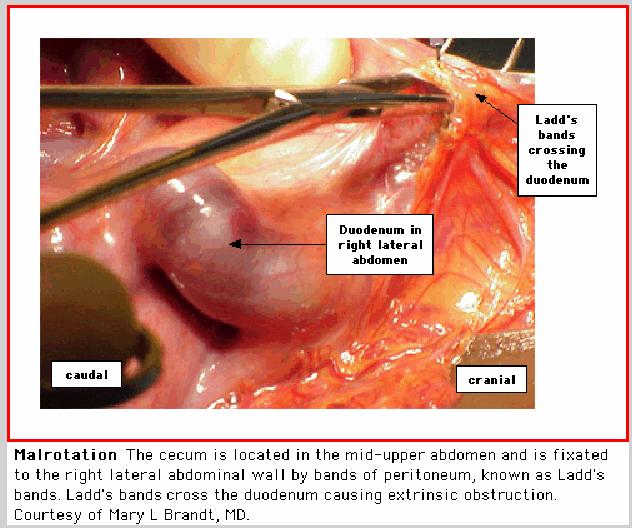
21 Operative Findings Liver, gallbladder, spleen, and stomach appeared normal Unable to locate the ligament of Trietz The duodenum was not fixed in usual retroperitoneal position Thick fibrous band of tissue crossed the 4 th portion of the duodenum as an obstruction point Cecum and ascending colon were mobile and not attached to the lateral abdominal wall This was c/w intestinal malrotation
22
23 Intestinal Malrotation in the Adolescent Midgut malrotation is estimated to occur in approximately 1/500 live births The true incidence is unknown owing to those who remain asymptomatic and go undiagnosed Surgical series estimate 50-80% present in the first month of life 20% present within first year 10-20% present older than 1 year
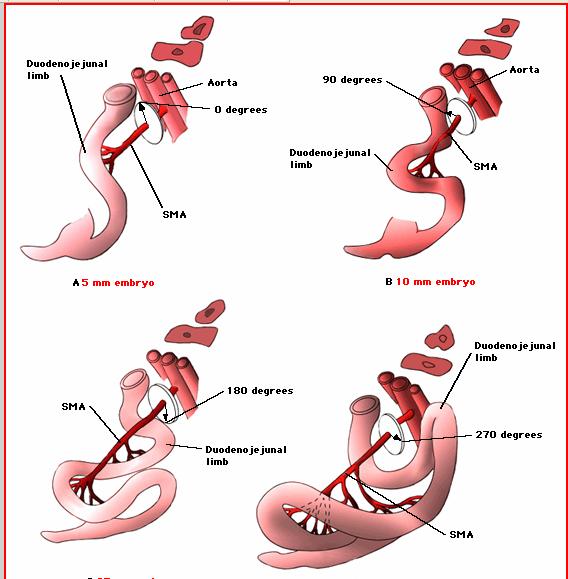
24 Pathophysiology Intestinal malrotation can be simply defined as any deviation from the normal 270 degree counterclockwise rotation of the midgut during embryonic development
25 Normal Rotation In the first two months of development the growth of the intestines exceeds the capacity of the abdomen to contain them The bowel develops outside the abdomen in the yolk sac Normal counterclockwise rotation of the bowel is driven by the greater rate of proximal bowel growth as compared to distal bowel and the rapid growth of the fetal liver
26 Return to the Abdomen First the duodenojejunal junction passes behind the SMA and becomes fixed to the upper left retroperitoneum. This forms the ligament of Trietz Second, the cecocolic junction passes from the left side of the abdomen, anterior to the SMA, assuming its position right of midline Overall, the bowel rotates 270 degrees counterclockwise from the original primary loop
27 Duodenojejunal Rotation

28 Cecocolic Limb
29 Normal Fixation At the completion of the rotation the intestines become fixed to the retroperitoneum by a broad based mesentery The mesentery extends from the ligament of Trietz to the ileocecal junction

30 Normal Mesenteric Fixation
31 Nonrotation Nonrotation occurs when the duodenojejunal and cecocolic limbs return the abdomen without any rotation The small bowel is located in the right abdomen The colon is located in the left abdomen
32
33 Malrotation Malrotation occurs with the duodenojejunal limb having no rotation. The cecocolic limb has partial rotation The cecum will be fixed to the right central abdominal wall by thick peritoneal bands. These bands may cause extrinsic compression of the duodenum This configuration results in a very narrow mesenteric attachment The narrow vascular pedicle predisposes to volvulus with subsequent ischemia and necrosis
34
35 Clinical Presentation Majority of symptomatic malrotation is diagnosed within the first week of life The presentation of malrotation in adolescents and adults is highly variable Most will have intermittent abdominal pain The pain has an unusual nature in the it will be transient, vague, and not necessarily associated with any physical findings Often the pain is postprandial and may or may not be associated with vomiting Less common presentations include failure to thrive, malabsorption, diarrhea, motility disorders, and biliary obstruction
36 Clinical Presentation Case studies report the time to diagnosis ranging from months to 17 years Common misdiagnoses include cyclic vomiting, food allergy, IBS, and motility disorders Often malrotation is first suspected in adolescents due to abnormal imaging studies or at laparotomy
37 Plain Films Conventional radiography is neither sensitive nor specific for malrotation Right sided jejunal markings and absence of stool filled colon in the right lower quadrant can be suggestive of malrotation Plain radiographs may be completely normal
38 Upper GI Series A limited Upper gastrointestinal barium series remains the most accurate tool for detection of malrotation Findings include failure of the duodenojejunal junction to cross the midline and lying below the level of the duodenal bulb and a clearly misplaced duodenum that has a corkscrew appearance 75% of cases have obvious signs of malrotation

39
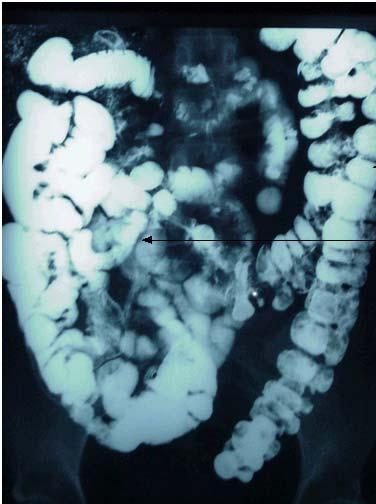
40 Barium Enema Contrast enema examination usually shows malposition of the right colon Contrast enema findings are nonspecific because the cecal location can be variable without malrotation 20% of patients with malrotation will have a cecum which assumes a normal position giving a false negative study
41
42 Ultrasound The role of ultrasound for diagnosing malrotation is not established A normal U/S does not rule out malrotation Findings which suggest malrotation are an abnormal relationship of the SMV and SMA; either anterior or to the left of the SMA The whirlpool sign of volvulus caused by the twisting of the vessels around the narrow mesenteric pedicle
43 CT Imaging Many cases of quiescent malrotation in adolescents and adults are detected by CT s obtained for other reasons CT can depict extra-intestinal findings not seen on conventional imaging Deviation of the normal SMV to SMA relationship (vertical or left-right inversion is suspicious for malrotation) The pancreas may show underdevelopment or absence of the uncinate process

44
45 Treatment The treatment for malrotation, whether asymptomatic, related to acute duodenal obstruction, or incidentally found is surgical The Ladd procedure is used for treatment of duodenal obstruction secondary to malrotation He wrote his paper on this procedure in 1932
46
47 Outcome Overall mortality rate is related to the presence or absence of volvulus and intestinal necrosis at the time of surgery Mortality approaches 0% in healthy patients without intestinal ischemia Recurrent volvulus can not be eliminated due to the inability to correct the underlying defect of malrotation. Estimated recurrence is 2-5% 2
48 Summary The clinical diagnosis of malrotation in adolescents and adults is rarely considered Adolescents/adults most often present with chronic abdominal pain with or without vomiting or chronic diarrhea Malrotation should be considered in any adolescent with intermittent abdominal pain, vomiting, diarrhea, or malabsorption Surgery is indicated in all cases of malrotation regardless of the discovery to reduce risk of volvulus and associated complications
Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help. Print this Page Add to my Bookmarks Page 3 of 10
 Welcome Kristin Ingstrup [ Logout ] SEARCH Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help Overview Editorial Board My Learning Plan January February March May June July August
Welcome Kristin Ingstrup [ Logout ] SEARCH Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help Overview Editorial Board My Learning Plan January February March May June July August
Hirschprung s. Meconium plug R/S >1 R/S <1
 NEONATAL ABDOMINAL EMERGENCIES LOW OBSTRUCTION HIGH OBSTRUCTION INTESTINAL OBSTRUCTION High obstruction - proximal to mid-ileumileum Few dilated, air filled bowel loops Complete obstruction diagnosed by
NEONATAL ABDOMINAL EMERGENCIES LOW OBSTRUCTION HIGH OBSTRUCTION INTESTINAL OBSTRUCTION High obstruction - proximal to mid-ileumileum Few dilated, air filled bowel loops Complete obstruction diagnosed by
Neonatal intestinal obstruction: how to make etiological diagnosis?
 Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. Mnari, M. Zguidi, A. Zrig, M. Maatouk, B. Hmida, R. Salem,
Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. Mnari, M. Zguidi, A. Zrig, M. Maatouk, B. Hmida, R. Salem,
Intestinal Malrotation
 Intestinal Malrotation Poster No.: C-1368 Congress: ECR 2015 Type: Educational Exhibit Authors: K. Carpentier, B. De Foer, F. Deckers, P. Leyman, M. 1 1 1 2 1 1 1 2 Pouillon, P. M. Parizel ; Wilrijk/BE,
Intestinal Malrotation Poster No.: C-1368 Congress: ECR 2015 Type: Educational Exhibit Authors: K. Carpentier, B. De Foer, F. Deckers, P. Leyman, M. 1 1 1 2 1 1 1 2 Pouillon, P. M. Parizel ; Wilrijk/BE,
Neonatal intestinal obstruction: how to make etiological diagnosis?
 Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. MNARI, M. Zguidi, A. Zrig, M. MAATOUK, B. Hmida, R. Salem,
Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. MNARI, M. Zguidi, A. Zrig, M. MAATOUK, B. Hmida, R. Salem,
Perforation of a Duodenal Diverticulum. Elective Student S. C.
 Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Objectives. Pediatric Mortality. Another belly pain. Gastroenteritis. Spewing & Pooing Child 4/18/16
 Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011
 Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus
 A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
Cecal Volvulus: Case Presentation and Review of CT Findings
 August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
Case Whirlpool sign in midgut volvulus
 Case 11454 Whirlpool sign in midgut volvulus Emad El-din Althamer 1, Shagufta Jabeen 2, Nada Al-Assaf 1, Akram Jawad 1, Muhammad Hassan 1, Muhammad Fatani 1, Rumayan Al-Rumyan 1, A Aziz Mosabihi 1, Ahmeduddin
Case 11454 Whirlpool sign in midgut volvulus Emad El-din Althamer 1, Shagufta Jabeen 2, Nada Al-Assaf 1, Akram Jawad 1, Muhammad Hassan 1, Muhammad Fatani 1, Rumayan Al-Rumyan 1, A Aziz Mosabihi 1, Ahmeduddin
B Papaziogas, A Patsas, G Paraskevas, P Tsiaousis, I Koutelidakis, C Christoforakis, K Atmatzidis
 ISPUB.COM The Internet Journal of Surgery Volume 19 Number 2 B Papaziogas, A Patsas, G Paraskevas, P Tsiaousis, I Koutelidakis, C Christoforakis, K Atmatzidis Citation B Papaziogas, A Patsas, G Paraskevas,
ISPUB.COM The Internet Journal of Surgery Volume 19 Number 2 B Papaziogas, A Patsas, G Paraskevas, P Tsiaousis, I Koutelidakis, C Christoforakis, K Atmatzidis Citation B Papaziogas, A Patsas, G Paraskevas,
Volvulus of the Gastrointestinal Tract: x-ray and CT imaging
 Volvulus of the Gastrointestinal Tract: x-ray and CT imaging Poster No.: C-0076 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Papadaki, S. Paschalidou, S. GIANNOU ; Rethymno, CR/ 1 2 2 3 1 3
Volvulus of the Gastrointestinal Tract: x-ray and CT imaging Poster No.: C-0076 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Papadaki, S. Paschalidou, S. GIANNOU ; Rethymno, CR/ 1 2 2 3 1 3
Development of pancreas and Small Intestine. ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama
 Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Adults intestinal malrotations: a simple approach to recognize the most frequent types with MDCT
 Adults intestinal malrotations: a simple approach to recognize the most frequent types with MDCT Poster No.: C-2484 Congress: ECR 2012 Type: Educational Exhibit Authors: F. Macrì, R. Argirò, B. SACCONI,
Adults intestinal malrotations: a simple approach to recognize the most frequent types with MDCT Poster No.: C-2484 Congress: ECR 2012 Type: Educational Exhibit Authors: F. Macrì, R. Argirò, B. SACCONI,
ABDOMEN - GI. Duodenum
 TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
Good morning! July 24, 2014
 Good morning! July 24, 2014 Prep #1 A 2-year-old boy presents to your office with a 2-day history of swelling of the right eye. He has been otherwise well. There are scattered insect bites on his body,
Good morning! July 24, 2014 Prep #1 A 2-year-old boy presents to your office with a 2-day history of swelling of the right eye. He has been otherwise well. There are scattered insect bites on his body,
Morning Report. Allison Haden, MD October 1, 2002
 Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
A Rare but Serious Complication of Ladd s Procedure: Recurrent Midgut Volvulus
 130 A Rare but Serious Complication of Ladd s Procedure: Recurrent Midgut Volvulus Murat Alkan a Pelin Oğuzkurt a Ozlem Alkan b Semire Serin Ezer a Akgün Hiçsönmez a Departments of a Pediatric Surgery
130 A Rare but Serious Complication of Ladd s Procedure: Recurrent Midgut Volvulus Murat Alkan a Pelin Oğuzkurt a Ozlem Alkan b Semire Serin Ezer a Akgün Hiçsönmez a Departments of a Pediatric Surgery
Midgut malrotation presenting as acute bowel obstruction in an adult with literature review
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 3 Ver.9 March. (2018), PP 76-82 www.iosrjournals.org Midgut malrotation presenting as acute
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 3 Ver.9 March. (2018), PP 76-82 www.iosrjournals.org Midgut malrotation presenting as acute
Key words: anomaly of intestine, reversed rotation, adult
 Key words: anomaly of intestine, reversed rotation, adult n92+ 4 n Fig. 1 Barium enema obstruction of the arrows) and mobile seen. (prone position, : Extrinsic transvers colon (between cecum (round arrow)
Key words: anomaly of intestine, reversed rotation, adult n92+ 4 n Fig. 1 Barium enema obstruction of the arrows) and mobile seen. (prone position, : Extrinsic transvers colon (between cecum (round arrow)
Vomiting in children: The good coordination between radiologists and pediatricians is the key to success
 Vomiting in children: The good coordination between radiologists and pediatricians is the key to success C. Santos Montón 1, M. T. Garzon Guiteria 2, A. Hortal Benito-Sendín 1, K. El Karzazi 1, P. Sanchez
Vomiting in children: The good coordination between radiologists and pediatricians is the key to success C. Santos Montón 1, M. T. Garzon Guiteria 2, A. Hortal Benito-Sendín 1, K. El Karzazi 1, P. Sanchez
Case Report Carcinoma of the Colon in an Adult with Intestinal Malrotation
 Case Reports in Surgery Volume 2013, Article ID 525081, 4 pages http://dx.doi.org/10.1155/2013/525081 Case Report Carcinoma of the Colon in an Adult with Intestinal Malrotation Michael Donaire, James Mariadason,
Case Reports in Surgery Volume 2013, Article ID 525081, 4 pages http://dx.doi.org/10.1155/2013/525081 Case Report Carcinoma of the Colon in an Adult with Intestinal Malrotation Michael Donaire, James Mariadason,
Case Report Intestinal Malrotation: A Rare Cause of Small Intestinal Obstruction
 Case Reports in Surgery, Article ID 453128, 4 pages http://dx.doi.org/10.1155/2014/453128 Case Report Intestinal Malrotation: A Rare Cause of Small Intestinal Obstruction Mesut Sipahi, 1 Kasim Caglayan,
Case Reports in Surgery, Article ID 453128, 4 pages http://dx.doi.org/10.1155/2014/453128 Case Report Intestinal Malrotation: A Rare Cause of Small Intestinal Obstruction Mesut Sipahi, 1 Kasim Caglayan,
Flouroscopy CT. Principal Modality (2): Case Report # [] Date accepted: 14 May 2015
![Flouroscopy CT. Principal Modality (2): Case Report # [] Date accepted: 14 May 2015](/thumbs/85/92263701.jpg "Flouroscopy CT. Principal Modality (2): Case Report # [] Date accepted: 14 May 2015") Radiological Category: Emergency Principal Modality (1): Principal Modality (2): Flouroscopy CT Case Report # [] Submitted by: Haider Virani, M.D. Faculty reviewer: Naga Chinapuvvula, MD Date accepted:
Radiological Category: Emergency Principal Modality (1): Principal Modality (2): Flouroscopy CT Case Report # [] Submitted by: Haider Virani, M.D. Faculty reviewer: Naga Chinapuvvula, MD Date accepted:
Anatomy of the SMALL INTESTINE. Dr. Noman Ullah Wazir PMC
 Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 09/17/2011 Radiology Quiz of the Week # 38 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 09/17/2011 Radiology Quiz of the Week # 38 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Barber Pole Sign in CT Angiography, Adult Presentation of Midgut Malrotation: A Case Report
 Iran J Radiol. 2015 July; 12(3): e17853. Published online 2015 July 22. ABDOMINAL IMAGING DOI: 10.5812/iranjradiol.17853v2 Case Report Barber Pole Sign in CT Angiography, Adult Presentation of Midgut Malrotation:
Iran J Radiol. 2015 July; 12(3): e17853. Published online 2015 July 22. ABDOMINAL IMAGING DOI: 10.5812/iranjradiol.17853v2 Case Report Barber Pole Sign in CT Angiography, Adult Presentation of Midgut Malrotation:
What is Your Diagnosis?
 What is Your Diagnosis? Izabela Ragan, Class of 2014 Signalment Species: Canine Breed: English Bulldog Sex: Male castrated Date of birth: 04/14/11 Presenting Complaint Dog was presented for vomiting and
What is Your Diagnosis? Izabela Ragan, Class of 2014 Signalment Species: Canine Breed: English Bulldog Sex: Male castrated Date of birth: 04/14/11 Presenting Complaint Dog was presented for vomiting and
Chapter 48 Anomalies of Intestinal Rotation
 Chapter 48 Anomalies of Intestinal Rotation François I. Luks Rotational anomalies of the intestinal tract refer to the failure of the primitive midgut to establish its normal anatomical relationships and
Chapter 48 Anomalies of Intestinal Rotation François I. Luks Rotational anomalies of the intestinal tract refer to the failure of the primitive midgut to establish its normal anatomical relationships and
Pediatric abdominal emergencies In the first year of life
 Common Pediatric abdominal emergencies In the first year of life Kristian Stien Thomassen Section of Pediatric Radiology Dept. of Radiology and Nuclear Medicine Oslo University Hospital Understand the
Common Pediatric abdominal emergencies In the first year of life Kristian Stien Thomassen Section of Pediatric Radiology Dept. of Radiology and Nuclear Medicine Oslo University Hospital Understand the
Midgut. Over its entire length the midgut is supplied by the superior mesenteric artery
 Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the
Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the
A 34 year old woman with Vomiting and abdominal pain
 A 34 year old woman with Vomiting and abdominal pain The patient was a 34 y/o woman admitted because of epigastric pain developed from 2 months ago. It was a crampy pain without radiation that became better
A 34 year old woman with Vomiting and abdominal pain The patient was a 34 y/o woman admitted because of epigastric pain developed from 2 months ago. It was a crampy pain without radiation that became better
Reverse rotation of gut with small bowel volvulus
 International Surgery Journal Narayanasamy SN et al. Int Surg J. 2015 May;2(2):295-299 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Case Report DOI: 10.5455/2349-2902.isj20150537 Reverse rotation
International Surgery Journal Narayanasamy SN et al. Int Surg J. 2015 May;2(2):295-299 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Case Report DOI: 10.5455/2349-2902.isj20150537 Reverse rotation
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Abdominal Pain in Pediatric Patients Image Gently
 Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
Deep Enteroscopy Methods to Diagnose Small Bowel IBD
 Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Procedure for Duodenal Stricture With Malrotation Masquerading as Superior Mesenteric Artery Syndrome in an Adult Patient
 CASE REPORT Procedure for Duodenal Stricture With Malrotation Masquerading as Superior Mesenteric Artery Syndrome in an Adult Patient Naoki Takahashi, PhD, Kazuyuki Gyoten, PhD, Kiyoshi Narita, MD, Rie
CASE REPORT Procedure for Duodenal Stricture With Malrotation Masquerading as Superior Mesenteric Artery Syndrome in an Adult Patient Naoki Takahashi, PhD, Kazuyuki Gyoten, PhD, Kiyoshi Narita, MD, Rie
Abdominal Assessment
 Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Discharge Summary-Page 1
 Discharge Summary-Page 1 Admission diagnosis: 1. Gastritis. 2. Alcoholic cirrhosis, ascites, grade 1 esophageal varices. 3. Recent left knee arthroplasty. 4. Osteoporosis naqmq : 1. Three chest X-rays
Discharge Summary-Page 1 Admission diagnosis: 1. Gastritis. 2. Alcoholic cirrhosis, ascites, grade 1 esophageal varices. 3. Recent left knee arthroplasty. 4. Osteoporosis naqmq : 1. Three chest X-rays
But.. Capsule Endoscopy. Guidelines (OMED ECCO) Why is Enteroscopy so Important? 4/19/2017
 Why is Enteroscopy so Important? 4/19/2017") Dr. Elizabeth Odstrcil Digestive Health Associates of Texas April 22, 2017 But.. Capsules fail to reach the cecum in as many as 25% of patients Patients with known CD have a risk of capsule retention of
Dr. Elizabeth Odstrcil Digestive Health Associates of Texas April 22, 2017 But.. Capsules fail to reach the cecum in as many as 25% of patients Patients with known CD have a risk of capsule retention of
Gastrointestinal Tract Imaging. Objectives. Reference. VMB 960 April 6, Stomach Small Intestine Colon. Radiography & Ultrasound
 Gastrointestinal Tract Imaging VMB 960 April 6, 2009 Stomach Small Intestine Colon Objectives Radiography & Ultrasound Contrast Examination of the Small Intestine Reference Chapters 45 47 Pages 750 805
Gastrointestinal Tract Imaging VMB 960 April 6, 2009 Stomach Small Intestine Colon Objectives Radiography & Ultrasound Contrast Examination of the Small Intestine Reference Chapters 45 47 Pages 750 805
Dr. Zahiri. In the name of God
 Dr. Zahiri In the name of God small intestine = small bowel is the part of the gastrointestinal tract Boundaries: Pylorus Ileosecal junction Function: digestion and absorption of food It receives bile
Dr. Zahiri In the name of God small intestine = small bowel is the part of the gastrointestinal tract Boundaries: Pylorus Ileosecal junction Function: digestion and absorption of food It receives bile
Barium Studies of the Small Intestine
 Chin J Radiol 2004; 29: 309-314 309 Barium Studies of the Small Intestine JEN-HUEY CHIANG RHEUN-CHUAN LEE TSIU-SHAN TSENG YI-YOU CHIOU CHENG-YEN CHANG Department of Radiology, Taipei Veterans General Hospital
Chin J Radiol 2004; 29: 309-314 309 Barium Studies of the Small Intestine JEN-HUEY CHIANG RHEUN-CHUAN LEE TSIU-SHAN TSENG YI-YOU CHIOU CHENG-YEN CHANG Department of Radiology, Taipei Veterans General Hospital
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
General Data. 王 X 村 78 y/o 男性
 General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
Postgastrectomy Syndromes
 Postgastrectomy Syndromes Postgastrectomy syndromes are iatrogenic conditions that may arise from partial gastrectomies, independent of whether the gastric surgery was initially performed for peptic ulcer
Postgastrectomy Syndromes Postgastrectomy syndromes are iatrogenic conditions that may arise from partial gastrectomies, independent of whether the gastric surgery was initially performed for peptic ulcer
KK College of Nursing Peptic Ulcer Badil D ass Dass, Lecturer 25th July, 2011
 KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
Suspected Foreign Body Ingestion
 Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015
 ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015 CASE PRESENTATION 41 yo woman presented one day hx abdominal pain, worsening nausea/vomiting denied flatus/bm
ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015 CASE PRESENTATION 41 yo woman presented one day hx abdominal pain, worsening nausea/vomiting denied flatus/bm
The jejunum and the Ileum. Prof. Oluwadiya KS
 The jejunum and the Ileum Prof. Oluwadiya KS www.oluwadiya.siteled.com Introduction Introduction The small intestine (SI) comprises of the duodenum, jejunum and the ileum The jejunum is the second part
The jejunum and the Ileum Prof. Oluwadiya KS www.oluwadiya.siteled.com Introduction Introduction The small intestine (SI) comprises of the duodenum, jejunum and the ileum The jejunum is the second part
Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies. Author(s): Joseph House (University of Michigan), MD 2012
: Joseph House (University of Michigan), MD 2012") Project: Ghana Emergency Medicine Collaborative Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies Author(s): Joseph House (University of Michigan), MD 2012 License: Unless otherwise noted,
Project: Ghana Emergency Medicine Collaborative Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies Author(s): Joseph House (University of Michigan), MD 2012 License: Unless otherwise noted,
CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST
 CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST IDENTIFICATION DATA ผ ป วยเด กชายไทย อาย 13 ว น เช อชาต ไทย ส ญชาต ไทย ภ ม ล าเนา จ งหว ด อ ท ยธาน เข าร บการร กษาท รพ.มหาว ทยาล ยนเรศวรว
CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST IDENTIFICATION DATA ผ ป วยเด กชายไทย อาย 13 ว น เช อชาต ไทย ส ญชาต ไทย ภ ม ล าเนา จ งหว ด อ ท ยธาน เข าร บการร กษาท รพ.มหาว ทยาล ยนเรศวรว
The Physician as Medical Illustrator
 The Physician as Medical Illustrator Francois Luks Arlet Kurkchubasche Division of Pediatric Surgery Wednesday, December 9, 2015 Week 5 A good picture is worth a 1,000 bad ones How to illustrate an operation
The Physician as Medical Illustrator Francois Luks Arlet Kurkchubasche Division of Pediatric Surgery Wednesday, December 9, 2015 Week 5 A good picture is worth a 1,000 bad ones How to illustrate an operation
Case 1- B.N. 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids.
 Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
PEDIATRIC EMERGENCY DEPARTMENT CLINICAL GUIDELINE: GI SURGICAL EMERGENCIES: VOMITING
 GI SURGICAL EMERGENCIES: VOMITING PYLORIC STENOSIS Population: Infants: onset between 2-5 weeks of age 1 in 250 births Male: female ratio 4:1 Familial incidence History: No vomiting in the first few weeks
GI SURGICAL EMERGENCIES: VOMITING PYLORIC STENOSIS Population: Infants: onset between 2-5 weeks of age 1 in 250 births Male: female ratio 4:1 Familial incidence History: No vomiting in the first few weeks
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Gastrointestinal Pathology. August 2007
 Gastrointestinal Pathology August 2007 Case 1 Dysphagia and halitosis Case 1 Dilatation of the oesophagus with a smooth narrowing of its lower end. The large volume of contained fluid indicates delayed
Gastrointestinal Pathology August 2007 Case 1 Dysphagia and halitosis Case 1 Dilatation of the oesophagus with a smooth narrowing of its lower end. The large volume of contained fluid indicates delayed
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Imaging Children with Acute Abdominal Pain -- Role/Protocols of US, CT, MR
 Imaging Children with Acute Abdominal Pain -- Role/Protocols of US, CT, MR Kimberly E. Applegate, MD, MS Emory University Financial disclosures: AIM (American Imaging Management) radiation protection advisory
Imaging Children with Acute Abdominal Pain -- Role/Protocols of US, CT, MR Kimberly E. Applegate, MD, MS Emory University Financial disclosures: AIM (American Imaging Management) radiation protection advisory
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Nasogastric tube. Stomach. Pylorus. Duodenum 1. Duodenum 2. Duodenum 3. Duodenum 4
 Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
THE mainstay of the radiographic study of the upper gastrointestinal tract has
 BARIUM-SPRAY EXAMINATION OF THE STOMACH- PRELIMINARY REPORT OF A NEW ROENTGENOGRAPHIC TECHNIC EDWARD BUONOCORE, M.D., and THOMAS F. MEANEY, M.D. Department of Hospital Radiology THE mainstay of the radiographic
BARIUM-SPRAY EXAMINATION OF THE STOMACH- PRELIMINARY REPORT OF A NEW ROENTGENOGRAPHIC TECHNIC EDWARD BUONOCORE, M.D., and THOMAS F. MEANEY, M.D. Department of Hospital Radiology THE mainstay of the radiographic
A rare case of intestinal obstruction due to internal hernia. Dr. Jayanth 3 rd year PG Dept. Of General Surgery
 A rare case of intestinal obstruction due to internal hernia Dr. Jayanth 3 rd year PG Dept. Of General Surgery One of the common cause of acute abdomen May lead to high morbidity and mortality if not treated
A rare case of intestinal obstruction due to internal hernia Dr. Jayanth 3 rd year PG Dept. Of General Surgery One of the common cause of acute abdomen May lead to high morbidity and mortality if not treated
Heterotaxia syndrome: The role of screening for intestinal rotation. abnormalities
 ADC Online First, published on May 12, 2005 as 10.1136/adc.2004.067504 Heterotaxia syndrome: The role of screening for intestinal rotation abnormalities Matthew Choi, Steven H Borenstein, Lisa Hornberger
ADC Online First, published on May 12, 2005 as 10.1136/adc.2004.067504 Heterotaxia syndrome: The role of screening for intestinal rotation abnormalities Matthew Choi, Steven H Borenstein, Lisa Hornberger
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
PMH: DM HTN Colon cancer s/p left hemicolectomy, chemo Now with mets to liver and peritoneum. Restarted on chemo 2/4/13 oxaliplatin, cepecitabine
 3.5.2013 75 y.o M with PMH of HTN, DM II with nephropathy, CKD stage III(b/l cr 1.5), colon cancer s/p hemicolectomy (8/2011) now with recurrence and mets to liver and peritoneum undergoing chemo at woodhull,
3.5.2013 75 y.o M with PMH of HTN, DM II with nephropathy, CKD stage III(b/l cr 1.5), colon cancer s/p hemicolectomy (8/2011) now with recurrence and mets to liver and peritoneum undergoing chemo at woodhull,
Sonographic Appearances of Common Gut Pathology in Paediatric Patients: Comparison with Plain Abdominal Radiography
 3668 Radiographer Text 1/4/04 2:57 PM Page 11 The Radiographer vol. 51: 11-17 Sonographic Appearances of Common Gut Pathology in Paediatric Patients: Comparison with Plain Abdominal Radiography Lino Piotto
3668 Radiographer Text 1/4/04 2:57 PM Page 11 The Radiographer vol. 51: 11-17 Sonographic Appearances of Common Gut Pathology in Paediatric Patients: Comparison with Plain Abdominal Radiography Lino Piotto
Volvulus characterization in radiology: A review
 Volvulus characterization in radiology: A review Poster No.: C-1677 Congress: ECR 2010 Type: Topic: Educational Exhibit GI Tract Authors: C. Antunes, M. Seco, A. Canelas, C. Ruivo, C. Paulino, F. Cruz,
Volvulus characterization in radiology: A review Poster No.: C-1677 Congress: ECR 2010 Type: Topic: Educational Exhibit GI Tract Authors: C. Antunes, M. Seco, A. Canelas, C. Ruivo, C. Paulino, F. Cruz,
Hernia Advisory Panel. Ethicon, Johnson & Johnson. Funding
 Acute Abdomen Andreas M Kluftinger MD FRCSC Kelowna General Hospital Disclosure Hernia Advisory Panel Ethicon, Johnson & Johnson Funding nil, zilch, zippo, nada, zero Objectives Understand the Pathophysiology
Acute Abdomen Andreas M Kluftinger MD FRCSC Kelowna General Hospital Disclosure Hernia Advisory Panel Ethicon, Johnson & Johnson Funding nil, zilch, zippo, nada, zero Objectives Understand the Pathophysiology
Chronic abdominal pain after RYGB A management guide
 OBES 21 st October 2017 Chronic abdominal pain after RYGB A management guide Dr Chun-Hai Tan MBBS, Masters of Medicine (Surgery), FRCS (Edinburgh) Consultant Surgeon Metabolic & Bariatric Surgery, Minimally
OBES 21 st October 2017 Chronic abdominal pain after RYGB A management guide Dr Chun-Hai Tan MBBS, Masters of Medicine (Surgery), FRCS (Edinburgh) Consultant Surgeon Metabolic & Bariatric Surgery, Minimally
GIANT DUODENAL DIVERTICULA*
 JUNE, 1974 GIANT DUODENAL DIVERTICULA* By JACK R. MILLARD, M.D., FRED M. H. ZITER, JR., M.D., and WILLIAM P. SLOVER, M.D. HARTFORD, D UODENAL diverticula are common incidental findings on barium examinations
JUNE, 1974 GIANT DUODENAL DIVERTICULA* By JACK R. MILLARD, M.D., FRED M. H. ZITER, JR., M.D., and WILLIAM P. SLOVER, M.D. HARTFORD, D UODENAL diverticula are common incidental findings on barium examinations
Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER
 1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy?
 January 2013 Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy? Johanna Sheu, Harvard Medical School Year III 1 Agenda Menu of tests Definition/anatomy/classification Pediatrics
January 2013 Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy? Johanna Sheu, Harvard Medical School Year III 1 Agenda Menu of tests Definition/anatomy/classification Pediatrics
USMLE Step 1 Problem Drill 17: Gastrointestinal System
 USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
USMLE Step 1 Problem Drill 17: Gastrointestinal System Question No. 1 of 10 1. A surgeon is planning to remove a patient s gallbladder endoscopically. During the procedure, the endoscope will traverse
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
53 year old Female with Hypoglycemia. Colleen Flynn, MD April 5, 2012
 53 year old Female with Hypoglycemia Colleen Flynn, MD April 5, 2012 HPI 53 yo F referred to the endocrine clinic for hypoglycemia x 1 year. History of a non secreting metastatic neuroendocrine tumor diagnosed
53 year old Female with Hypoglycemia Colleen Flynn, MD April 5, 2012 HPI 53 yo F referred to the endocrine clinic for hypoglycemia x 1 year. History of a non secreting metastatic neuroendocrine tumor diagnosed
Pediatric Radiology Update
 Pediatric Radiology Update Douglas Rivard, DO Vice Chairman, Radiology Dept Children s Mercy Hospital Asst Professor of Radiology University of Missouri-Kansas City Objectives Review radiation biology
Pediatric Radiology Update Douglas Rivard, DO Vice Chairman, Radiology Dept Children s Mercy Hospital Asst Professor of Radiology University of Missouri-Kansas City Objectives Review radiation biology
Critically Ill Children in Pediatric Surgery. No disclosures to report.
 Critically Ill Children in Pediatric Surgery Hillary J. Collyer RN, MSN, CPNP, CCRN Pediatric Surgery Nurse Practitioner Hasbro Children s Hospital Disclosure Information Speaker: Hillary Collyer No disclosures
Critically Ill Children in Pediatric Surgery Hillary J. Collyer RN, MSN, CPNP, CCRN Pediatric Surgery Nurse Practitioner Hasbro Children s Hospital Disclosure Information Speaker: Hillary Collyer No disclosures
Adult Intussusception
 Bahrain Medical Bulletin, Vol. 27, No. 3, September 2005 Adult Intussusception Suhair Alsaad, MBCHB, CABS, FRCSI* Mariam Al-Muftah, MBCHB** Objectives: Adult intussusception is a rare entity. We present
Bahrain Medical Bulletin, Vol. 27, No. 3, September 2005 Adult Intussusception Suhair Alsaad, MBCHB, CABS, FRCSI* Mariam Al-Muftah, MBCHB** Objectives: Adult intussusception is a rare entity. We present
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
I. Intussusception in Children: Diagnostic Imaging and Treatment
 1 I. Intussusception in Children: Diagnostic Imaging and Treatment II. Author Kimberly E. Applegate, MD, MS Indiana University Department of Radiology Riley Hospital for Children 702 Barnhill Rd., Rm 1053b
1 I. Intussusception in Children: Diagnostic Imaging and Treatment II. Author Kimberly E. Applegate, MD, MS Indiana University Department of Radiology Riley Hospital for Children 702 Barnhill Rd., Rm 1053b
X-ray Corner. Imaging of the Small Bowel. Pantongrag-Brown L. Case 1. A 63-year-old man presented with abdominal pain, nausea and vomiting.
 THAI J 42 Imaging of the Small Bowel GASTROENTEROL 2015 X-ray Corner Imaging of the Small Bowel Pantongrag-Brown L Small bowel is the longest tubular organ in the body, about 18-22 feet. It is anchored
THAI J 42 Imaging of the Small Bowel GASTROENTEROL 2015 X-ray Corner Imaging of the Small Bowel Pantongrag-Brown L Small bowel is the longest tubular organ in the body, about 18-22 feet. It is anchored
Exploring Anatomy: the Human Abdomen
 Exploring Anatomy: the Human Abdomen PERITONEUM AND PERITONEAL CAVITY PERITONEUM The peritoneum is a thin serous membrane that lines the abdominal cavity and covers, in variable amounts, the viscera within
Exploring Anatomy: the Human Abdomen PERITONEUM AND PERITONEAL CAVITY PERITONEUM The peritoneum is a thin serous membrane that lines the abdominal cavity and covers, in variable amounts, the viscera within
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Development of the Digestive System. W.S. O The University of Hong Kong
 Development of the Digestive System W.S. O The University of Hong Kong Plan for the GI system Then GI system in the abdomen first develops as a tube suspended by dorsal and ventral mesenteries. Blood
Development of the Digestive System W.S. O The University of Hong Kong Plan for the GI system Then GI system in the abdomen first develops as a tube suspended by dorsal and ventral mesenteries. Blood
Case Cholecystoduodenal fistula with migrated gallstone leading to gastric outlet obstruction: Bouveret's syndrome
 Case 14613 Cholecystoduodenal fistula with migrated gallstone leading to gastric outlet obstruction: Bouveret's syndrome Eva De Backer 1, Filip Vanhoenacker 2, 3, 4, Adelard De Backer5 1: Ghent University,
Case 14613 Cholecystoduodenal fistula with migrated gallstone leading to gastric outlet obstruction: Bouveret's syndrome Eva De Backer 1, Filip Vanhoenacker 2, 3, 4, Adelard De Backer5 1: Ghent University,
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
Inflammatory Bowel Disease When is diarrhea not just diarrhea?
 Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Case 1307 Mesothelial cysts
 Case 1307 Mesothelial cysts Vinhais S, Monteiro M, Cunha TM INSTITUTO PORTUGUÊS DE ONCOLOGIA de Francisco Gentil de LISBOA Section: Gastro-Intestinal Imaging Published: 2001, Nov. 23 Patient: 44 year(s),
Case 1307 Mesothelial cysts Vinhais S, Monteiro M, Cunha TM INSTITUTO PORTUGUÊS DE ONCOLOGIA de Francisco Gentil de LISBOA Section: Gastro-Intestinal Imaging Published: 2001, Nov. 23 Patient: 44 year(s),
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus
 Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
Medical application of transabdominal ultrasound in gastrointestinal diseases
 Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
The "whirl sign". Diagnostic accuracy for intestinal volvulus.
 The "whirl sign". Diagnostic accuracy for intestinal volvulus. Poster No.: C-0670 Congress: ECR 2014 Type: Scientific Exhibit Authors: M. Pire, M. Marti, A. Borobia, A. Verón; Madrid/ES Keywords: Abdomen,
The "whirl sign". Diagnostic accuracy for intestinal volvulus. Poster No.: C-0670 Congress: ECR 2014 Type: Scientific Exhibit Authors: M. Pire, M. Marti, A. Borobia, A. Verón; Madrid/ES Keywords: Abdomen,
A Case of Carcinoma Colon Presenting As Intestinal Malrotation
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 9 Ver. XI (September. 2017), PP 25-29 www.iosrjournals.org A Case of Carcinoma Colon Presenting
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 9 Ver. XI (September. 2017), PP 25-29 www.iosrjournals.org A Case of Carcinoma Colon Presenting
Abdominal Imaging: Luminal organs. Rowland Illing MA BMBCh DM FLS MRCS(Eng) FRCR
 FRCR") Abdominal Imaging: Luminal organs Rowland Illing MA BMBCh DM FLS MRCS(Eng) FRCR Aims Reference text & resources Management of a patient Imaging what and when to use What to ask and how to describe Segments
Abdominal Imaging: Luminal organs Rowland Illing MA BMBCh DM FLS MRCS(Eng) FRCR Aims Reference text & resources Management of a patient Imaging what and when to use What to ask and how to describe Segments
ABDOMINAL PAIN AND DIARRHEA - IT S NOT (ALWAYS) WHAT YOU THINK. Yakov Wainer, MD Gastroenterology and Hepatology Meir Medical Center
 WHAT YOU THINK. Yakov Wainer, MD Gastroenterology and Hepatology Meir Medical Center") ABDOMINAL PAIN AND DIARRHEA - IT S NOT (ALWAYS) WHAT YOU THINK Yakov Wainer, MD Gastroenterology and Hepatology Meir Medical Center 1 ST ADMISSION - 2015 38 y/o female Abdominal pain, diarrhea - intermittent
ABDOMINAL PAIN AND DIARRHEA - IT S NOT (ALWAYS) WHAT YOU THINK Yakov Wainer, MD Gastroenterology and Hepatology Meir Medical Center 1 ST ADMISSION - 2015 38 y/o female Abdominal pain, diarrhea - intermittent
CASE #1. 39M with HIV/AIDS (CD4 24, VL 93,000) rarely taking HAART or OI prophylaxis for several months
 rarely taking HAART or OI prophylaxis for several months") CASE #1 39M with HIV/AIDS (CD4 24, VL 93,000) rarely taking HAART or OI prophylaxis for several months Presented with acute onset abdominal pain Diffuse, constant, non-positional Reported nausea/vomiting
CASE #1 39M with HIV/AIDS (CD4 24, VL 93,000) rarely taking HAART or OI prophylaxis for several months Presented with acute onset abdominal pain Diffuse, constant, non-positional Reported nausea/vomiting