Op#mizing)Management)in)IBD:) Mucosal)Healing)
|
|
|
- Stella Griffin
- 5 years ago
- Views:
Transcription


1 Op#mizing)Management)in)IBD:) Mucosal)Healing) Vipul&Jairath&MD&PhD& Associate&Professor&of&Medicine,&Epidemiology&and& Biosta=s=cs& Western&University&&& Division&of&Gastroenterology,&& London&Health&Sciences&Network&
2 Biological)importance)of)mucosal)healing)
3 Mucosal)healing)in)UC:) Known)Knowns ) Associated&with&improved&clinical&outcomes& No&causal&proof&beJer&than&trea=ng&to&symptoms& Objec=ve&and&reliable&measure&of&disease&ac=vity& Discordance&between&symptoms&and&endoscopy& Will&soon&inform®ulatory&approval,&claims& labelling&and&reimbursement&
 60 40 20 0 46 0 (n=120) 34 1 (n=175) 11 2")
 Endoscopic score at Week 8 (ACT 1 & 2) Colombel JF")
4 Early)Mucosal)Healing)with)IFX)and)Steroid) Free)Remission) Patients (%) (n=120) 34 1 (n=175) 11 2 (n=114) p< (n=57) Endoscopic score at Week 8 (ACT 1 & 2) Colombel JF et al. Gastroenterology 2011;141:
5 Early)Mucosal)Healing)with)IFX)is)Associated) with)reduced)risk)of)colectomy) 1.00) Propor#on)with)colectomy) 0.75) 0.50) 0) p=0.0004) Endoscopy)subscore)=)0) Endoscopy)subscore)=)1) Endoscopy)subscore)=)2) Endoscopy)subscore)=)3) 10) 20) 30) 40) 50) Time)to)colectomy)(weeks)) Colombel)JF)et#al.)Gastroenterology#2011;141: )
& Ardizzone S, et al.")
6 Early)Response)to)Steroids)and)5\year)Outcome) #& *& *& #& #& *& *& *p<0.05&vs.&clinical&and&endoacopic&remission& #&p<0.05&vs.&clinical&remission&(+ /X&endoscopic&remission)& Ardizzone S, et al. Clin Gastroenterol Hepatol. 2011;9:483-9
7 Severity)of)Inflamma#on)is)a)Risk)Factor)for) Variable) Colorectal)Neoplasia)in)UC) Controls) (n=136)) Cases) (n=68)) 2.22& (0.78)& 2.38& (0.56)& Odds)ra#o)(95%) confidence)interval)) P)value) Colonoscopy) inflamma#on)score) 1.89&(0.52)& 2.54&( )& 0.001& Histological) inflamma#on)score) 2.05&(0.41)& 5.13&( )& <0.001& Family)history)of)CRC) (%)) 18&(14)& 7&(12)& 1.09&( )& 0.17& PSC)(%)) 2&(2)& 4&(6)& 4.00&( )& 0.11& Mesalamine)use)(%)) 122&(90)& 65&(96)& 2.38&( )& 0.32& Azathioprine)use)(%)) 37&(28)& 12&(18)& 0.73&( )& 0.22& Folate)supplement)(%)) 5&(4)& 1&(1)& 0.40&( )& 0.40& Current)smoker)(%)) 9&(7)& 2&(4)& 0.43&( )& 0.37& Segmental colonoscopic and histological inflammation was recorded by using a simple score (0, normal; 1, quiescent/chronic inflammation; and 2, 3, and 4, mild, moderate, and severe active inflammation, respectively). Rutter M et al. Gastroenterology. 2004;126:451-9
8 Mucosal)Healing)in)UC:) Known)Knowns ) Associated&with&improved&clinical&outcomes& No&causal&proof&beJer&than&trea=ng&to&symptoms& Objec=ve&and&reliable&measure&of&disease&ac=vity& Discordance&between&symptoms&and&endoscopy& Will&soon&inform®ulatory&approval,&claims& labelling&and&reimbursement&
9 Reliability)of)UC)Endoscopic)Assessment) Indices) UCDAI) Sigmoidoscopy) Score) Intraobserver)Agreement) All)7) Central) Readers) Instrument) Modified)Baron) Score) Ulcera#ve)Coli#s) Endoscopic)Index) of)severity) Visual)Analogue) Scale) 0.89)(0.85\0.92)) 0.88)(0.84\0.92)) 0.89)(0.85\0.93)) 0.91)(0.88) )0.94)) Es#mates)of)Intra\rater)and)Inter\rater)Agreement)Based)on)Data)from)50)Random) Videos)Evaluated)3)Times)by)7)Blinded,)off\site)readers) Feagan)BG.)et)al.)Gastroenterology)2013;145:149\157))
10 Mucosal)Healing)in)UC:) Known)Knowns ) Associated&with&improved&clinical&outcomes& No&causal&proof&beJer&than&trea=ng&to&symptoms& Objec=ve&and&reliable&measure&of&disease&ac=vity& Discordance&between&symptoms&and&endoscopy& Will&soon&inform®ulatory&approval,&claims& labelling&and&reimbursement&


11 Discrepancy)Between)Symptoms,)Endoscopy) and)histology) Colombel)J,)Gut)Sept)2016)
12 Mucosal)Healing)in)UC:) Known)Knowns ) Associated&with&improved&clinical&outcomes& No&causal&proof&beJer&than&trea=ng&to&symptoms& Objec=ve&and&reliable&measure&of&disease&ac=vity& Discordance&between&symptoms&and&endoscopy& Will&soon&inform®ulatory&approval,&claims& labelling&and&reimbursement&

13
14 Regulatory)Considera#ons) Mucosal&healing&has&been&included&as&a&secondary&endpoint&in& many&clinical&trials.&&in&many&clinical&trials,&mucosal&healing&has&been& defined&as&mayo&endoscopic&subscore&of&less&than&or&equal&to&1& point.&&however,(a(claim(of(mucosal((healing(would(not(be(supported( through(endoscopy(that(provides(only(an(assessment(of(the(visual( appearance(of(the(mucosa.&any&claim&related&to&findings&on& endoscopy,&in&the&absence&of&validated&histological&assessment&of& the&mucosa,&would&be&limited&to&the&endoscopic&appearance&of&the& mucosa & FDA&Drai&Guidance&2016&
15 Mucosal)Healing)in)CD:) Known)Knowns ) Associated&with&improved&clinical&outcomes& Surgery,&hospitaliza=on,&longterm&remission& Severity&of&lesions&correlates&with&prognosis& A&predictor&or&relapse&aier&withdrawal&of&an=XTNF& therapy&
16 Early)Mucosal)Healing:)Long\Term)Remission) EXTEND: Endoscopic response at week 12 and 1 year remission Patients (%) p< (n=31) >5 (n=31) SES-CD score at Week 12 Clinical remission defined as a CDAI score <150 EXTEND subanalysis; primary endpoint was complete mucosal healing at Week 12 (p=0.056); all patients received adalimumab induction therapy from Week 0, before being randomised to placebo or adalimumab maintenance therapy at Week 4 Rutgeerts P et al. Gastroenterology May;142(5):
Year)3)and)Year)4)(SUTD) P<0.05 P<0.05 Baert F, et al.")
17 Predic#ve)Factors)at)Year)2)for)Remission) During)Year)3)and)Year)4)(SUTD) P<0.05 P<0.05 Baert F, et al. Gastroenterology 2010; 138:463-8
18 Mucosal)Healing)and)Resec#on)in)CD) IBSEN Study: risk of future surgery in patients with mucosal healing at 1 year (n=146) 1.0 Proportion of patients not resected No mucosal healing Mucosal healing HR = 0.42, 95% CI ; p=0.027 Adjusted for age and disease extent at diagnosis 83% 69% Time in years after 1-year visit 9 Solberg IC et al. Clin Gastroenterol Hepatol. 2007;5:
19 Mucosal)Healing)in)CD:) Known)Knowns ) Associated&with&improved&clinical&outcomes& Surgery,&hospitaliza=on,&longterm&remission& Severity&of&lesions&correlates&with&prognosis& A&predictor&or&relapse&aier&withdrawal&of&an=XTNF& therapy&

20 Severity)of)Endoscopic)Lesions)and)Long) Term)Outcome)in)CD) Development of fistulizing disease Colectomy P=0.02 6/53 Allez M et al. Am J Gastroenterol 2002;97:
21 Endoscopic)Scoring)System)for) Postopera#ve)Recurrence)(Rutgeerts)Score) Post-operative recurrence after ileo-colonic resection Percent Survival without: Endoscopic lesions Laboratory recurrence Years Symptoms Surgery Symptom free survival (%) Years i4 i2 i3 i0 + i1 Rutgeerts P, et al. Gastroenterology 1990;99:
22 Relapse)Upon)Infliximab)Discon#nua#on)(STORI) Treated with combined scheduled infliximab+immunosuppressive therapy for at least 1 year. In stable remission without steroid for more than 6 months CDESI=0, low CRP, Normal HB = sustained clinical remission in 80% patients 1 Index # relapse Proportion /19 =5 10/36 Global 40/107 =6 13/24 =7 25/ Months since inclusion # at risk: Louis E et al Gastroenterology 2012;142:63 70
23 Known)Unknowns :)Defini#ons!) UC& Absence&of&friability,& blood,&erosions,&ulcers& Severity&of&bleeding& without&considering& ulcers& Mayo&0&or&1& UCDAI& 1& CD& Absence&of&ulcera=on& No&ulcera=on&in&any& segment& SESXCD& 5& CDEIS& 2,& 3& Rutgeerts& i1&

24 Peyrin-Birolet et al. Am J Gastro
Target?) Peyrin-Birolet et al.")
25 Ulcera#ve)Coli#s:)What)is)the) Consensus)Target?) Peyrin-Birolet et al. Am J Gastro
what)is)the)consensus)target?")
26 Crohn s:)what)is)the)consensus)target?) Peyrin-Birolet et al. Am J Gastro
27 Measuring)the)Score)

")
 3 =")
 Schroeder&KW,&et(al.")
28 The)Mayo)Endoscopic)Subscore) Findings of flexible proctosigmoidoscopy 0 = Normal or inactive disease 1 = Mild disease (erythema, decreased vascular pattern, mild friability) 2 = Moderate disease (marked erythema, absent vascular pattern, friability, erosions) 3 = Severe disease (spontaneous bleeding, ulceration) Schroeder&KW,&et(al.(N(Engl(J(Med(1987;317: &
vascular)paoern)with)arboriza#on)of)capillaries)clearly) defined)or)with)blurring)or)patchy)loss)of)capillary)margins) Patchy)oblitera#on)(1)& Patchy)oblitera#on)of)vascular)paoern)")
29 UCEIS:)Reliability)and)Ini#al)Valida#on) Descriptor) (score&most&severe& lesions)) Likert)scale)anchor) points) Defini#on) Vascular)paoern) Normal)(0)& Normal)vascular)paoern)with)arboriza#on)of)capillaries)clearly) defined)or)with)blurring)or)patchy)loss)of)capillary)margins) Patchy)oblitera#on)(1)& Patchy)oblitera#on)of)vascular)paoern) Obliterated)(2)& Complete)oblitera#on)of)vascular)paoern) Bleeding) None)(0)& No)visible)blood) Mucosal)(1)& Some)spots)or)streaks)of)coagulated)blood)on)the)surface)of) the)mucosa)ahead)of)the)scope)that)can)be)washed)away) Luminal)mild)(2)& Some)free)liquid)blood)in)the)lumen) Luminal)moderate)or) severe)(3)& Frank)blood)in)the)lumen)ahead)of)the)endoscope)or)visible) oozing)from)a)haemorrhagic)mucosa) Erosions)and)ulcers) None)(0)& Normal)mucosa,)no)visible)erosions)or)ulcers) Erosions)(1)& Tiny)( 5&mm)&defects)in)the)mucosa)of)a)white)or)yellow)colour) with)a)flat)edge) Superficial)ulcer)(2)& Larger)(>5&mm)&defects)in)the)mucosa.)Which)are)discrete) fibrin\covered)ulcers)when)compared)with)erosions)but) remain)superficial) Deep)ulcer)(3)& Deeper)excavated)defects)in)the)mucosa)with)a)slightly)raised) Vascular&paJern&provide&discrimina=on&for&lower&levels&of&severity& edge) Bleeding&discriminate&between&higher&levels&of&severity& NOTE. The worst affected area of the colon visible at sigmoidoscopy was scored. Although the original version of UCEIS gave a score of 1 to the normal appearance of a descriptor, a collective decision was made to change the numbering of the levels with normality awarded a score of 0, so that the simple sum of the UCEIS ranges from 0 to 8 Travis S, et al. Gut 2012;61:535 42;
 Vascular pattern V0: Normal; V1: Patchy")


30 UCEIS:)Examples) UCEIS 0 (V0, B0, E0) UCEIS 5 (V2, B1, E0) UCEIS 8 (V2, B3, E3) Vascular pattern V0: Normal; V1: Patchy obliteration; V2: Obliterated Bleeding B0: None; B1: Mucosal; B2: Luminal mild; B3: Luminal moderate or severe Erosions and ulcers E0: None; E1: Erosions; E2: Superficial ulcer; E3: Deep ulcer Walsh A, et al. Gastrointest Endosc Clin N Am 2014;:
31 CDEIS) Numerical grading system: 0-44
cm)) Presence)and)size)of)ulcers)(0\3)) Extent)of)ulcerated)surface)(0\3)) Extent)of)affected)surface)(0\3)) Ileum& SES\CD)Score)")
cm)) Very)large)ulcers) (>)2)cm)) Ulcerated)surface) None) <)10%) 10\30%) >)30%) Affected)surface) Unaffected)segment) <)50%) 50\75%)")



32 Simple)Endoscopic)Score)for)CD:)SES\CD) Numerical grading system: 0-56 Variable) Size)of)ulcers) None) Aphthous)ulcers) (0.1)to)0.5)cm)) Presence)and)size)of)ulcers)(0\3)) Extent)of)ulcerated)surface)(0\3)) Extent)of)affected)surface)(0\3)) Ileum& SES\CD)Score) Right& colon& SES\CD)values) 0) 1) 2) 3) Transverse& colon& Large)ulcers) (0.5)to)2.0)cm)) Very)large)ulcers) (>)2)cm)) Ulcerated)surface) None) <)10%) 10\30%) >)30%) Affected)surface) Unaffected)segment) <)50%) 50\75%) >)75%) Presence)of)narrowing) None) Single,) Can)be)passed) Mul#ple,) Can)be)passed) Cannot)be)passed) Lei&colon& Rectum& Total& Every segment of the bowel is scored on a scale from 0 to 3 using the endoscopic variables. If a segment was not seen due to nonpassable stenosis or was removed due to the previous surgery it scores 0. The sum of the scores for each endoscopic variable ranges from 0 to 15, except for stenosis, where it varies between 0 and 11, because 3 represents a stenosis through which a colonoscope cannot be passed and that can be observed only once. Patients with ileo-rectal anastomosis should be excluded as there are only 2 segments to consider. Presence)and)type)of)narrowings) (0\3)) SES\CD= Adult 8 mm Size references Adult endoscope D=13.6 mm Pediatric endoscope D=11.6 mm Pediatric ~ 7mm With fully open jaws Daperno M,. Gastrointest Endosc Oct;60(4):
 flat defect of the mucosa")

 of whitish, yellowish or greyish color with flat or excavated")



33 SES\CD:)Example) Variable: Ulcer Variable: Ulcerated and Affected Surface Aphthous ulcer - a tiny (< 5mm) flat defect of the mucosa of whitish, yellowish or greyish color with erythematous halo 10-30% ulcerated surface < 50% affected surface Large ulcer a discrete, fibrin-covered defect of the mucosa (>5mm but less< 2cm ) of whitish, yellowish or greyish color with flat or excavated edges > 30% ulcerated surface 50-75% affected surface Very large ulcer - a discrete, fibrin-covered defect of the mucosa (> 2cm) of whitish, yellowish or greyish color with flat or excavated edges > 30% ulcerated surface > 75% affected surface These are the single frames of the endoscopic video. Assessment of the sequences of video frames is required to score the entire segment/s of the bowel.

34 SES\CD:)Example) Aphthous ulcers ( cm) are present in the ileum Score = 1.0 for the ileum Extent of ulcerated surface is 10-30% in the ileum Score = 2.0 for the ileum Extent of affected surface is >75% in the ileum Score = 3.0 for the ileum There is no narrowing/s in the ileum Score = 0.0 for the ileum TOTAL SCORE FOR THE SEGMENT: 6.0 Aphthous ulcers in the ileum
Endoscopic)Score)for)Recurrence)of)")




35 Rutgeerts )Endoscopic)Score)for)Recurrence)of) CD)in)Neoterminal)Ileum) Score Criteria No lesions < 5 Aphtoid ulcers > 5 aphtoid ulcers with normal mucosa in between or skip areas of larger lesions or lesions confined to the ileocolonic anastomosis 3 4 Difuse ileates with large ulcers, normal mucosa in between Difuse ileitis with large ulcers, nodules/narrowing without normal mucosa in between
Can)Score)Just)as)Well) Dubenco, E.")
36 Experts )and) Non\Experts )Can)Score)Just)as)Well) Dubenco, E. JCC, 2016
37 Alterna#vely)\)Describe)what)You)See) Perineal&exam& Loca=on&and&extent&of&inflamma=on&(e.g.&%&surface&area)& If&the&bowel&involvement&is&con=nuous&or&patchy& Comment&on:& Erythema& loss&of&vascularity& bleeding&(spontaneous&or&contact)& erosions&or&ulcera=ons&(superficial&or&deep)& Strictures&or&fistulas& Overall&impression:& Endoscopically&quiescent&remission &
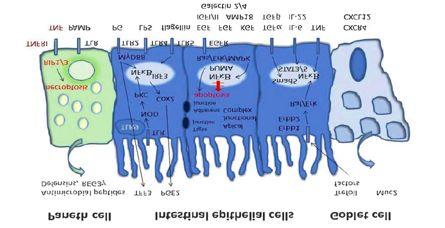
38 Looking)Beyond)the)Mucosa)
 Neurath and Travis, Gut")
39 How) Deep )is)remission?) Neurath and Travis, Gut 2012
40 )Predictors)of)Relapse)in)UC) Hazard)ra#o) (95%)CI)) P)value) Age) 0.4 a )( )) 0.003) Basal) plasmacytosis) No.)of)prior) relapses) (women)) No.)of)prior) relapses)(men)) 4.5)( )) 0.003) 1.6 b )( )) <0.001) 0.93))( )) 0.64) a Per&decade.& &b No&significant&differences&in&WBC,&Hb,&and&albumin.& Propor#on)of)pa#ents)in)remission) 1) 0.75) 0.5) 0.25) 0) 0) Basal)Plasmacytosis) Absence) Presence) 2) 4) 6) 8) 10) 12) Months)on)study) Bitton A, et al. Gastroenterology 2001;120:13 20
41 Histological)Remission)Predicts)Lower) Hospitaliza#on)Rates)and)steroid)use) Histological)remission)is)associated)with)a)4\fold)reduc#on)in) hospitalisa#on) Hospitaliza#on) 1) Clinical) 1) Endoscopic) 1) Histological) 0.5) 0.5) 0.5) 0) 0) 10) 20) 30) 40) Time)(months)) Clinical)remission) No)clinical)remission) 0) 0) 10) 20) 30) 40) Time)(months)) Endoscopic)remission) No)endoscopic)remission) 0) 0) 10) 20) 30) 40) Time)(months)) Histological)remission) No)histological)remission) Clinical)remission) Endoscopic)remission) Histological)remission) Hazard)Ra#o)(95%)CI)) 0.24)(0.05 )1.10) 0.53)( ) 0.27)( ) P)value) 0.07) 0.25) 0.048) Bryant RV, et al. Gut, 2015

42 Ultrastructural)Healing) Normal mucosa CDEIS<4 with endomicroscopic activity Active CD Mucosal healing at endomicroscopy Neurath and Travis, Gut 2012
43 Can)Our)Current)Armamentarium)Achieve) Mucosal)Healing?)
44 Crohn s UC 5-ASA - 44% 1 Steroids -? 30% 2 Azathioprine 53% 3 53% 4 Methotrexate 11% 5? Infliximab 48% 6 50% 7 Certolizumab 4% 8? Adalimumab 24% 9 41% 10 Vedolizumab? 51% Römkens TEH, et al. Inflamm Bowel Dis. 2012;18: Truelove SC, Witts LJ. Br Med J. 1954;4884: Lémann M, et al. Gastroenterology ;128: Ardizzone S, et al. Gut 2006;55: Laharie D, et al. Aliment Pharmacol Ther. 2011;33: Ferrante M et al. Gastroenterology. 2013;145: Rutgeerts P, et al. N Engl J Med. 2005;353: Hébuterne X, et al. Gut. 2013;62: Rutgeerts P et al. Gastroenterology. 2012;142: Sandborn WJ et al. Gastroenterology. 2012;142: Feagan BG et al. N Engl J Med. 2013;369:
45 Surrogates)for)endoscopic)disease)ac#vity)
46 Surrogates)for)endoscopic)disease)ac#vity) CRP& 20%&do¬&mount&a&response& Differs&in&CD&vs&UC& Confounded&by&age,&sex,&BMI& Calprotec=n& Higher&levels&in&colon&vs.&Ileum& CutXoffs&unclear& IntraXindividual&varia=on,&assay&standardiza=ons& Lactoferrin& Unstable&at&room&temperature& Unclear&cutXoffs&
47 Calprotec#n)to)detect)ac#ve)inflamma#on:UC) Variable) Sensi#vity) Specificity) CRP) IBD) Calprotec#n) CD) UC) &0.49&(0.34,&0.64)&& &0.87&(0.82,&0.91)&& &0.88&(0.84,&0.92)&& &0.92&(0.72,&0.98)&& 0.67&(0.58,&0.75)&& &0.79&(0.68,&0.87)&& Stool)Lactoferrin) IBD) 0.82&(0.73,&0.88)&& &0.79&(0.62,&0.89)&& Mosli et al; Am J Gastroenterol Jun:110(6):802-15
48 How)Important)is)Mucosal)Healing)in)the) Course)of)IBD?) Mucosal&healing,&which&can&be&achieved&by&several& drugs,&is&associated&with&bejer&outcomes& Lower&hospitaliza=on&rates,&relapse&rates& Mucosal&healing&may&be&associated&with&a&lower&risk& of&colorectal&cancer&in&uc& Mucosal&healing&is&associated&with&less&bowel& damage&in&cd& Mucosal&healing&is&a&predictor&of&relapse&aier&an=X TNF&withdrawal&
49 Unanswered)Ques#ons) How&much&mucosal&healing&is&needed&to&modify&disease& course?& Should&therapies&be&op=mized&to&achieve&MH&or&to&avoid& adverse&outcomes&in&the&absence&of&healing?& When&is&the&best&=ming&for&endoscopic&reXevalua=on&aier& interval&change&in&therapy&& Is&trea=ng&to&mucosal&healing&any&beJer&than&trea=ng&to& clinical&symptoms&(will&pa=ents&accept&this?)& Is&trea=ng&beyond&mucosal&healing&beJer&than&to&mucosal& healing&or&symptoms&(will&pa=ent&accept&this?)& Can&dose&deXescala=on&occur&aier&a&period&of&deep& remission?&
50 Randomized)Trials)in)the)Pipeline) REACT)2) Cluster&trial& Algorithmic&approach&of& trea=ng&to&symptoms& vs.&mucosal&healing& 24&months&follow&up&of& CD&related& hospitaliza=on/&& complica=ons/surgeries& CALM)Trial) Individual&randomized& Tight&disease&control& (CDAI,&CRP,&Calpro)&vs.& management&using&less& stringent&disease& criteria&(cdai)& Studies are needed in Ulcerative Colitis
51 Prac#cal)Recommenda#ons:)UC) Baseline)endoscopy:)first)presenta#on)of)significant)symptoms) Follow)up)colonoscopy))at)3\6)months:)Adjust)therapy)accordingly) Stra#fy)according)to)relapse)risk) High)Risk) o Flare<12)months) o Recent)therapy)change) o Persistent)lesions) o Persistent)neutrophils) o Smoking)cessa#on) o Poor)adherence) Low)Risk) o Remission>12)months) o Stable)maintenance) therapy) o Endoscopic)healing) o Histological)healing) o Smoker) o Good)adherence) Clinic)3\4)months) Calprotec#n)2\3)months) CRP)2\3)months) Re\scope)if)symptoms)or)abnormal) biomarkers) Clinic)6\12)months) Calprotec#n)3\6)months) CRP)3\6)months) Re\scope)if)symptoms)or)abnormal) biomarkers)
52 Stratify low / high risk: Age; disease location; disease behavior, smoking; deep ulceration TNF ; Immunosuppressants Other treatment options Complete Clinical remission Biomarker normalization at weeks + endoscopy Complete Clinical remission Biomarker normalization at weeks Yes No No Yes Monitor symptoms & biomarkers every 3-6 months When altered Endoscopy and / or cross-sectional imaging Adapt therapy and further monitoring according to drug class After 6months
Mucosal healing: does it really matter?
 Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Endoscopy in Inflammatory Bowel Disease DR. REENA KHANNA
 Endoscopy in Inflammatory Bowel Disease DR. REENA KHANNA ASSISTANT PROFESSOR, UNIVERSITY OF WESTERN ONTARIO Background Clinical trials in ulcerative colitis and Crohn s disease require validated instruments
Endoscopy in Inflammatory Bowel Disease DR. REENA KHANNA ASSISTANT PROFESSOR, UNIVERSITY OF WESTERN ONTARIO Background Clinical trials in ulcerative colitis and Crohn s disease require validated instruments
Activity and Endoscopic measures : Crohn s disease. Jean-Frederic COLOMBEL Justin Cote-Daigneault Icahn Medical School at Mount Sinai, New York
 Activity and Endoscopic measures : Crohn s disease Jean-Frederic COLOMBEL Justin Cote-Daigneault Icahn Medical School at Mount Sinai, New York J-F Colombel has served as consultant or advisory board member
Activity and Endoscopic measures : Crohn s disease Jean-Frederic COLOMBEL Justin Cote-Daigneault Icahn Medical School at Mount Sinai, New York J-F Colombel has served as consultant or advisory board member
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND. Fabrizio Parente
 NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
IBD Updates. Themes in IBD IBD management journey. New tools for therapeutic monitoring. First-line treatment in IBD
 IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease. David A. Schwartz, MD
 An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation?
 Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
September 12, 2015 Millie D. Long MD, MPH, FACG
 Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Implementation of disease and safety predictors during disease management in UC
 Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
IBD scoring systems. Lara Hart, MD FRCPC 1,2 Talat Bessissow, MD FRCPC 1 Mallory Chavannes, MD FRCPC 3,4
 IBD scoring systems Lara Hart, MD FRCPC 1,2 Talat Bessissow, MD FRCPC 1 Mallory Chavannes, MD FRCPC 3,4 1. McGill University Health Center, Montreal QC; 2. McMaster University Medical Center, Hamilton
IBD scoring systems Lara Hart, MD FRCPC 1,2 Talat Bessissow, MD FRCPC 1 Mallory Chavannes, MD FRCPC 3,4 1. McGill University Health Center, Montreal QC; 2. McMaster University Medical Center, Hamilton
5/2/2018 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD
 5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
Medical Management of Inflammatory Bowel Disease
 Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Personalized Medicine in IBD: Where Are We in 2013
 Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Recent Advances in the Management of Refractory IBD
 Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Biologics in IBD. Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College
 Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Evaluation of the severity of ulcerative colitis using endoscopic dual red imaging targeting deep vessels
 Evaluation of the severity of ulcerative colitis using endoscopic dual red imaging targeting deep vessels Authors Makoto Naganuma 1, 2, Naohisa Yahagi 3,RiekoBessho 1, Keiko Ohno 1, Mari Arai 1, Makoto
Evaluation of the severity of ulcerative colitis using endoscopic dual red imaging targeting deep vessels Authors Makoto Naganuma 1, 2, Naohisa Yahagi 3,RiekoBessho 1, Keiko Ohno 1, Mari Arai 1, Makoto
Disclosures. What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists
 What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
Anne Griffiths MD, FRCPC. SickKids Hospital, University of Toronto. Buenos Aires, August 16, 2014
 Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions. Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
 Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Clinical Study Clinical Study of the Relation between Mucosal Healing and Long-Term Outcomes in Ulcerative Colitis
 Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2013, Article ID 192794, 6 pages http://dx.doi.org/10.1155/2013/192794 Clinical Study Clinical Study of the Relation between
Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2013, Article ID 192794, 6 pages http://dx.doi.org/10.1155/2013/192794 Clinical Study Clinical Study of the Relation between
Impact of endoscopic monitoring in postoperative Crohn s disease patients already receiving pharmacological prevention of recurrence
 1130-0108/2015/107/10/586-590 Revista Española de Enfermedades Digestivas Copyright 2015 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid Vol. 107, N.º 10, pp. 586-590, 2015 ORIGINAL PAPERS Impact of endoscopic
1130-0108/2015/107/10/586-590 Revista Española de Enfermedades Digestivas Copyright 2015 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid Vol. 107, N.º 10, pp. 586-590, 2015 ORIGINAL PAPERS Impact of endoscopic
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease
 Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Endoscopy in IBD. F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M.
 Frankfurt/M.") F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
Moderately to severely active ulcerative colitis
 Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Treatment Goals. Current Therapeutic Pyramids Crohn s Disease Ulcerative Colitis 11/14/10
 Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
How do I choose amongst medicines for inflammatory bowel disease. Maria T. Abreu, MD
 How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
Narrow band imaging efficiency in evaluation of mucosal healing/ relapse of ulcerative colitis
 Original article Narrow band imaging efficiency in evaluation of mucosal healing/ relapse of ulcerative colitis Authors Seiko Sasanuma 1, Kazuo Ohtsuka 1, 2, Shin-ei Kudo 1, Noriyuki Ogata 1, Yasuharu
Original article Narrow band imaging efficiency in evaluation of mucosal healing/ relapse of ulcerative colitis Authors Seiko Sasanuma 1, Kazuo Ohtsuka 1, 2, Shin-ei Kudo 1, Noriyuki Ogata 1, Yasuharu
Preventing post-operative recurrence
 Oxford Inflammatory Bowel Disease MasterClass Preventing post-operative recurrence Dr Oliver Brain Oxford Disclosures Presented at IEE, Oxford 2013 AbbVie sponsored meeting Talk Outline Risk factors for
Oxford Inflammatory Bowel Disease MasterClass Preventing post-operative recurrence Dr Oliver Brain Oxford Disclosures Presented at IEE, Oxford 2013 AbbVie sponsored meeting Talk Outline Risk factors for
Randomised clinical trial: delayed-release oral mesalazine 4.8 g day vs. 2.4 g day in endoscopic mucosal healing ASCEND I and II combined analysis
 Alimentary Pharmacology and Therapeutics Randomised clinical trial: delayed-release oral mesalazine 4.8 g day vs. 2.4 g day in endoscopic mucosal healing ASCEND I and II combined analysis G. R. Lichtenstein*,
Alimentary Pharmacology and Therapeutics Randomised clinical trial: delayed-release oral mesalazine 4.8 g day vs. 2.4 g day in endoscopic mucosal healing ASCEND I and II combined analysis G. R. Lichtenstein*,
As clinicians we would all agree that the goal for our
 CURRENT CONTROVERSIES: PRO, CON, AND BALANCE Controversies in Mucosal Healing in Ulcerative Colitis Sunanda Kane, MD,* Frances Lu, MD, Asher Kornbluth, MD, Dahlia Awais, MD, and Peter D.R. Higgins, MD,
CURRENT CONTROVERSIES: PRO, CON, AND BALANCE Controversies in Mucosal Healing in Ulcerative Colitis Sunanda Kane, MD,* Frances Lu, MD, Asher Kornbluth, MD, Dahlia Awais, MD, and Peter D.R. Higgins, MD,
Achieving Success in Ulcerative Colitis: the Role of Infliximab
 Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Join the conversation at #GIFORUMCCFA
 1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
healing with methotrexate in Crohn s disease: a prospective comparative study with azathioprine infliximab
 Mucosal healing with methotrexate in Crohn s disease: a prospective comparative study with azathioprine and infliximab David Laharie, Armel Reffet, Genevieve Belleannée, Edouard Chabrun, Clement Subtil,
Mucosal healing with methotrexate in Crohn s disease: a prospective comparative study with azathioprine and infliximab David Laharie, Armel Reffet, Genevieve Belleannée, Edouard Chabrun, Clement Subtil,
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah
 John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts
 Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz The Mt. Sinai School of Medicine Refining our Management
Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz The Mt. Sinai School of Medicine Refining our Management
Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation
 ORIGINAL ARTICLE Annals of Gastroenterology (2019) 32, 1-6 Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation Dimitrios S. Politis a, Konstantinos
ORIGINAL ARTICLE Annals of Gastroenterology (2019) 32, 1-6 Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation Dimitrios S. Politis a, Konstantinos
The role of endoscopy in inflammatory bowel disease
 European Review for Medical and Pharmacological Sciences The role of endoscopy in inflammatory bowel disease M. DAPERNO, R. SOSTEGNI, A. LAVAGNA, L. CROCELLÀ, E. ERCOLE, C. RIGAZIO, R. ROCCA, A. PERA Center
European Review for Medical and Pharmacological Sciences The role of endoscopy in inflammatory bowel disease M. DAPERNO, R. SOSTEGNI, A. LAVAGNA, L. CROCELLÀ, E. ERCOLE, C. RIGAZIO, R. ROCCA, A. PERA Center
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Mono or Combination Therapy with. Individualized Approach
 Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Update on Biologics in Ulcerative Colitis. Scott Plevy, MD University of North Carolina Chapel Hill, NC
 Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Biologic Therapy for Inflammatory. Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida
 Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
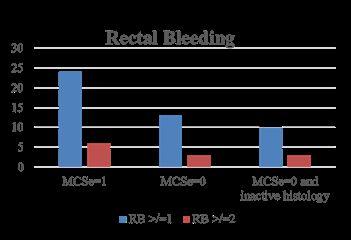
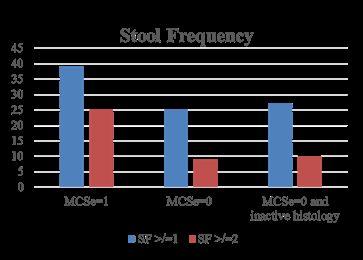
Mucosal Healing in Ulcerative Colitis When Zero is Better
 Journal of Crohn's and Colitis, 2016, 20 25 doi:10.1093/ecco-jcc/jjv180 Advance Access publication October 5, 2015 Original Article Original Article Mucosal Healing in Ulcerative Colitis When Zero is Better
Journal of Crohn's and Colitis, 2016, 20 25 doi:10.1093/ecco-jcc/jjv180 Advance Access publication October 5, 2015 Original Article Original Article Mucosal Healing in Ulcerative Colitis When Zero is Better
Title: Author: Journal:
 IMPORTANT COPYRIGHT NOTICE: This electronic article is provided to you by courtesy of Ferring Pharmaceuticals. The document is provided for personal usage only. Further reproduction and/or distribution
IMPORTANT COPYRIGHT NOTICE: This electronic article is provided to you by courtesy of Ferring Pharmaceuticals. The document is provided for personal usage only. Further reproduction and/or distribution
Op#mal Therapy in IBD: Where Are We Now?
 Op#mal Therapy in IBD: Where Are We Now? Brian G. Feagan MD Professor of Medicine, Epidemiology and Biosta;s;cs Western University Senior Scien;fic Director, Robarts Clinical Trials, London, Ontario, Canada
Op#mal Therapy in IBD: Where Are We Now? Brian G. Feagan MD Professor of Medicine, Epidemiology and Biosta;s;cs Western University Senior Scien;fic Director, Robarts Clinical Trials, London, Ontario, Canada
Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών. Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων
 Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων Conflict of interest By means of this, the speaker confirms that
Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων Conflict of interest By means of this, the speaker confirms that
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
CLINICAL INSIGHTS 01
 P2 Borrowing a Treatment Paradigm From Rheumatoid Arthritis P4 Antidrug Antibody Monitoring in Practice P6 Proactive Drug Monitoring Informs Therapeutic Dose Adjustments P7 Keeping Patients in Remission
P2 Borrowing a Treatment Paradigm From Rheumatoid Arthritis P4 Antidrug Antibody Monitoring in Practice P6 Proactive Drug Monitoring Informs Therapeutic Dose Adjustments P7 Keeping Patients in Remission
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Severe IBD: What to Do When Anti- TNFs Don t Work?
 Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
Immunogenicity of Biologic Agents and How to Prevent Sensitization
 Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy
 Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease
 Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
How to use infliximab?
 How to use infliximab? Séverine Vermeire, MD, PhD Division of Gastroenterology University Hospital Gasthuisberg Leuven The how to use infliximab rules Before starting IFX: try optimizing chances for response!
How to use infliximab? Séverine Vermeire, MD, PhD Division of Gastroenterology University Hospital Gasthuisberg Leuven The how to use infliximab rules Before starting IFX: try optimizing chances for response!
The small bowel capsule and management of patients
 The small bowel capsule and management of patients with inflammatory bowel disease Arnaud Bourreille Institut des maladies de l appareil digestif (Imad), CHU Hôtel Dieu, Nantes, France The management of
The small bowel capsule and management of patients with inflammatory bowel disease Arnaud Bourreille Institut des maladies de l appareil digestif (Imad), CHU Hôtel Dieu, Nantes, France The management of
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases
 Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art
 Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art David T. Rubin, MD The Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition
Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art David T. Rubin, MD The Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition
Results of the 2nd scientific workshop of the ECCO (IV): Therapeutic strategies to enhance intestinal healing in inflammatory bowel disease
: Therapeutic strategies to enhance intestinal healing in inflammatory bowel disease") Journal of Crohn's and Colitis (2012) 6, 492 502 Available online at www.sciencedirect.com SPECIAL ARTICLE Results of the 2nd scientific workshop of the ECCO (IV): Therapeutic strategies to enhance intestinal
Journal of Crohn's and Colitis (2012) 6, 492 502 Available online at www.sciencedirect.com SPECIAL ARTICLE Results of the 2nd scientific workshop of the ECCO (IV): Therapeutic strategies to enhance intestinal
ENTYVIO (VEDOLIZUMAB)
") ENTYVIO (VEDOLIZUMAB) UnitedHealthcare Community Plan Medical Benefit Drug Policy Policy Number: CS2017D0053F Effective Date: July 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
ENTYVIO (VEDOLIZUMAB) UnitedHealthcare Community Plan Medical Benefit Drug Policy Policy Number: CS2017D0053F Effective Date: July 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
New treatment options in UC. Rob Bryant IBD Consultant Royal Adelaide Hospital
 New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Disease Monitoring. Symptoms Activity. No Symptoms No Activity. What is the Problem with Dogma? What are the FACTS
 Heal the Mucosa or Heal the Patient (Data vs Dogma) Heal the Mucosa Cary G. Sauer MD MSCR Associate Professor, Emory University School of Medicine Clinical Director, IBD Program The Facts vs The Force
Heal the Mucosa or Heal the Patient (Data vs Dogma) Heal the Mucosa Cary G. Sauer MD MSCR Associate Professor, Emory University School of Medicine Clinical Director, IBD Program The Facts vs The Force
Endpoints for Stopping Treatment in UC
 Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Latest Treatment Updates for Ulcerative Colitis: Evolving Treatment Goals
 Latest Treatment Updates for Ulcerative Colitis: Evolving Treatment Goals Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker
Latest Treatment Updates for Ulcerative Colitis: Evolving Treatment Goals Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker
Outcomes of immunosuppressors and biologic drugs in inflammatory bowel diseases: a real life experience
 Outcomes of immunosuppressors and biologic drugs in inflammatory bowel Treatments and therapeutic approaches in IBD are constantly evolving. The newly emerged biologic treatments are one such evolving
Outcomes of immunosuppressors and biologic drugs in inflammatory bowel Treatments and therapeutic approaches in IBD are constantly evolving. The newly emerged biologic treatments are one such evolving
IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital
 IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital Aims To understand the aetiology of IBD To understand the impact that
IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital Aims To understand the aetiology of IBD To understand the impact that
Personalized Medicine in IBD
 Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Fistulizing Crohn s Disease: The Aggressive Approach
 Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
2nd Nottingham IBD Masterclass, 2017
 2nd Nottingham IBD Masterclass, 217 Positioning IL12/IL23 blockade in the Crohn s disease treatment algorithm Prof James Lindsay, Consultant Gastroenterologist, Barts Health NHS Trust Professor in Inflammatory
2nd Nottingham IBD Masterclass, 217 Positioning IL12/IL23 blockade in the Crohn s disease treatment algorithm Prof James Lindsay, Consultant Gastroenterologist, Barts Health NHS Trust Professor in Inflammatory
What do we need for diagnosis of IBD
 What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
Withdrawal of drug therapy in patients with quiescent Crohn s disease
 Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Selby Inflamm Bowel Dis. 2008:14:
 Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases?
 How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases? Alessandro Armuzzi Lead IBD Unit Complesso Integrato Columbus Fondazione Policlinico Gemelli Università
How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases? Alessandro Armuzzi Lead IBD Unit Complesso Integrato Columbus Fondazione Policlinico Gemelli Università
Inflammatory Bowel Disease: Clinical updates. Dr Jeff Chao Princess Alexandra Hospital
 Inflammatory Bowel Disease: Clinical updates Dr Jeff Chao Princess Alexandra Hospital Inflammatory bowel disease 2017 Clinical updates and future directions Pathogenesis Treatment targets Therapeutic agents
Inflammatory Bowel Disease: Clinical updates Dr Jeff Chao Princess Alexandra Hospital Inflammatory bowel disease 2017 Clinical updates and future directions Pathogenesis Treatment targets Therapeutic agents
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
ENTYVIO (VEDOLIZUMAB)
") ENTYVIO (VEDOLIZUMAB) UnitedHealthcare Commercial Medical Benefit Drug Policy Policy Number: 2017D0053F Effective Date: July 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
ENTYVIO (VEDOLIZUMAB) UnitedHealthcare Commercial Medical Benefit Drug Policy Policy Number: 2017D0053F Effective Date: July 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
Positioning Biologics in Ulcerative Colitis
 Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Inflammatory bowel disease (IBD), which includes both Crohn s
, which includes both Crohn s") Mucosal Healing in Inflammatory Bowel Disease A True Paradigm of Success? Maneesh Dave, MBBS, MPH, and Edward V. Loftus, Jr., MD Dr. Dave is a Fellow and Instructor of Medicine and Dr. Loftus is a Professor
Mucosal Healing in Inflammatory Bowel Disease A True Paradigm of Success? Maneesh Dave, MBBS, MPH, and Edward V. Loftus, Jr., MD Dr. Dave is a Fellow and Instructor of Medicine and Dr. Loftus is a Professor
Emerging g therapies for IBD: A practical approach to positioning. Sequential Therapies for IBD
 Emerging g therapies for IBD: A practical approach to positioning Stephen B. Hanauer, MD Sequential Therapies for IBD Disease Severity at Presentation Severe Anti-TNF +/IS Cyclosporine (UC) Colectomy (UC)
Emerging g therapies for IBD: A practical approach to positioning Stephen B. Hanauer, MD Sequential Therapies for IBD Disease Severity at Presentation Severe Anti-TNF +/IS Cyclosporine (UC) Colectomy (UC)
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
Medical Therapy for Pediatric IBD: Efficacy and Safety
 Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/38545 holds various files of this Leiden University dissertation. Author: Molendijk, Ilse Title: Mesenchymal stromal cell therapy for Crohn's disease :
Cover Page The handle http://hdl.handle.net/1887/38545 holds various files of this Leiden University dissertation. Author: Molendijk, Ilse Title: Mesenchymal stromal cell therapy for Crohn's disease :
Prevention and Management of Postoperative Crohn s disease
 Prevention and Management of Postoperative Crohn s disease Miguel Regueiro, M.D. Associate Professor of Medicine Associate Chief for Education Clinical Head and Co-Director, IBD Center Director, Gastroenterology,
Prevention and Management of Postoperative Crohn s disease Miguel Regueiro, M.D. Associate Professor of Medicine Associate Chief for Education Clinical Head and Co-Director, IBD Center Director, Gastroenterology,
Optimizing Management using CRP, Fecal Calprotectin and Ferritin. Peter Laszlo Lakatos 1st Department of Medicine Semmelweis University Budapest
 Optimizing Management using CRP, Fecal Calprotectin and Ferritin Peter Laszlo Lakatos 1st Department of Medicine Semmelweis University Budapest Objectives Overview of disease progression Old and new treatment
Optimizing Management using CRP, Fecal Calprotectin and Ferritin Peter Laszlo Lakatos 1st Department of Medicine Semmelweis University Budapest Objectives Overview of disease progression Old and new treatment
Once Daily Dosing for Induction and Maintenance of Remission in Ulcerative Colitis
 Once Daily Dosing for Induction and Maintenance of Remission in Ulcerative Colitis John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University JKM 2014 Svartz N. Acta Med Scand
Once Daily Dosing for Induction and Maintenance of Remission in Ulcerative Colitis John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University JKM 2014 Svartz N. Acta Med Scand
Treatment of ulcerative colitis with adalimumab or infliximab: long-term follow-up of a single-centre cohort
 Alimentary Pharmacology and Therapeutics Treatment of ulcerative colitis with adalimumab or infliximab: long-term follow-up of a single-centre cohort N. Gies, K. I. Kroeker, K. Wong & R. N. Fedorak Division
Alimentary Pharmacology and Therapeutics Treatment of ulcerative colitis with adalimumab or infliximab: long-term follow-up of a single-centre cohort N. Gies, K. I. Kroeker, K. Wong & R. N. Fedorak Division
Positioning New Therapies
 Positioning New Therapies Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker Disclosure Stephen Hanauer, MD has disclosed
Positioning New Therapies Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker Disclosure Stephen Hanauer, MD has disclosed
Diarrhoea for the Acute Physician
 Diarrhoea for the Acute Physician STEPHEN INNS GASTROENTEROLOGIST AND PHYSICIAN HUTT VALLEY DHB August 2013 Outline Case History 1 Initial assessment of acute diarrhoea Management of fulminant UC Management
Diarrhoea for the Acute Physician STEPHEN INNS GASTROENTEROLOGIST AND PHYSICIAN HUTT VALLEY DHB August 2013 Outline Case History 1 Initial assessment of acute diarrhoea Management of fulminant UC Management
ENTYVIO (VEDOLIZUMAB)
") ENTYVIO (VEDOLIZUMAB) UnitedHealthcare Oxford Clinical Policy Policy Number: PHARMACY 285.8 T2 Effective Date: November 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE... 1 CONDITIONS OF COVERAGE...
ENTYVIO (VEDOLIZUMAB) UnitedHealthcare Oxford Clinical Policy Policy Number: PHARMACY 285.8 T2 Effective Date: November 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE... 1 CONDITIONS OF COVERAGE...
Efficacy and Safety of Adalimumab in Ulcerative Colitis Refractory to Conventional Therapy in Routine Clinical Practice
 Journal of Crohn's and Colitis, 216, 26 3 doi:1.193/ecco-jcc/jjv169 Advance Access publication September 21, 215 Original Article Original Article Efficacy and Safety of Adalimumab in Ulcerative Colitis
Journal of Crohn's and Colitis, 216, 26 3 doi:1.193/ecco-jcc/jjv169 Advance Access publication September 21, 215 Original Article Original Article Efficacy and Safety of Adalimumab in Ulcerative Colitis
The Spectrum of IBD. Inflammatory Bowel Disease. Symptoms. Epidemiology. Tests for IBD. CD or UC? Inflamatory Bowel Disease. Fernando Vega, M.D.
 The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
Gionata Fiorino VEDOLIZUMAB E IBD. Un nuovo target terapeutico
 Gionata Fiorino VEDOLIZUMAB E IBD Un nuovo target terapeutico Anti cell adhesion molecules Danese S, NEJM 2011 6 Steps leukocyte recruitment Fiorino G. et al. 2010 Vedolizumab Blocks Fewer Biological Pathways
Gionata Fiorino VEDOLIZUMAB E IBD Un nuovo target terapeutico Anti cell adhesion molecules Danese S, NEJM 2011 6 Steps leukocyte recruitment Fiorino G. et al. 2010 Vedolizumab Blocks Fewer Biological Pathways
COPYRIGHT. Inflammatory Bowel Disease What Every Clinician Needs to Know. Adam S. Cheifetz, MD. Director, Center for Inflammatory Bowel Disease
 Inflammatory Bowel Disease What Every Clinician Needs to Know Adam S. Cheifetz, MD Director, Center for Inflammatory Bowel Disease Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard
Inflammatory Bowel Disease What Every Clinician Needs to Know Adam S. Cheifetz, MD Director, Center for Inflammatory Bowel Disease Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard