Figurate Erythemas and Purpuras
|
|
|
- Chad Haynes
- 5 years ago
- Views:
Transcription
1 Figurate Erythemas and Purpuras Dr. Anna Karp D.O. Dr. Stephanie Lasky D.O. In collaboration with our co-residents Program Director: Suzanne Sirota Rozenberg D.O. St. Johns Episcopal Hospital Far Rockaway, New York 1
2 Disclosures None
3 Figurate Erythemas
4 Objectives Discuss the following figurate erythemas and treatments Erythema Annulare Centrifugum Erythema Marginatum Erythema Migrans Erythema Gyratum Repens Discuss the different types of purpuras and their etiologies Review basic methods of coagulation Review specific purpuric syndromes Discuss treatment modalities
5 Erythema Annulare Centrifugum Introduction Superficial and deep forms. More common in adults. Peak incidence in 5 th decade of life. Duration: days to months, often self-limiting Most commonly idiopathic, but can be related to infection or other exposures. Reaction pattern or hypersensitivity reaction to one of many antigens
6 Pathogenesis Infectious causes: Dermatophytes (Tinea Pedis) Fungal: Candida, Penicillium in blue cheese. Viruses (e.g. poxvirus, EBV, varicella-zoster virus, HIV) Parasites and Ectoparasites (e.g. Phthirus pubis). Drug induced: diuretics, NSAIDs, antimalarials, gold, finasteride, amitriptyline, etizolam Other: Pregnancy, certain foods, autoimmune endocrinopathies, hyper-eosinophilic syndrome and occasionally, lymphomas and leukemia.
7 Clinical Features Initial lesions begin as firm pink papules that expand centrifugally and then develop central clearing. Can enlarge to greater than 6 cm. Favors upper legs, hips and trunk. In the superficial form, lesions are minimally elevated, and there is desquamation at the inner margin, i.e. trailing scale. +/- pruritus. In deep gyrate erythema, the advancing edges are indurated and raised, and there is usually no scale. Nonpruritic. As lesions resolve, PIH is common.


8 A) Superficial EAC B) Deep Gyrate Erythema

9 Pathology Superficial lesions: mild spongiosis, focal parakeratosis, superficial perivascular lymphohistiocytic infiltrate Fairly tight aggregates around vessels, the so-called coat sleeve anomaly. Rarely eosinophils. Edema in the papillary dermis. Deep lesions: lymphoctic infiltrate with a sharply demarcated perivascular arrangement is present primarily within the mid and lower dermis.
10 Differential Diagnosis Tinea Corporis Annular Psoriasis Annular Urticaria Erythema Marginatum Allergic Urticarial Eruption Autoimmune disorders, including linear IgA bullous dermatosis, Sjo gren s syndrome and lupus erythematosus, can also have erythematous annular, arciform and polycyclic lesions.
11 Treatment If EAC is due to an underlying disorder, the skin lesions will usually resolve once the disease has been successfully treated Usually self-limited. Topical corticosteroids. Topical anti-pruritics and sedating antihistamines for pruritus. Systemic corticosteroids, however recurrence is common after discontinuation. Case Reports: Empiric use of antibiotics, anti-fungal agents, topical tacrolimus, topical calcipotriene, oral metronidazole, subcutaneous etanercept and subcutaneous interferon-alpha
12 Erythema Marginatum Cutaneous manifestation of Rheumatic Fever ~ 3% of patients with untreated group A β-hemolytic Streptococcal infections can develop acute rheumatic fever Latency period of 2-5 weeks before development of rheumatic fever Rash occurs in less than 10% of patients with acute rheumatic fever. Higher incidence in children, peak age 5-15 years. Associated findings: Jones Criteria: Carditis, Migratory Polyarthritis, Sydenham s chorea, fever and subcutaneous nodules.
13 Clinical Features Lesions begin as erythematous macules that spread peripherally and become patches or plaques, can be polycyclic, with NO scale. Usually asymptomatic. Migrates over a period of 12 hours (by 2 12 mm). Lasts from a few hours to a few days usually transient. Can recur over a few weeks. Most commonly on the trunk, axillae and proximal extremities, spares face.


14 Erythema Marginatum
15 Differential Diagnosis Annular urticaria Annular erythema of infancy Neutrophilic figurate erythema of infancy EAC Erythema Gyratum Repens Hereditary periodic fever syndromes (particularly TNF receptor-associated periodic syndrome [TRAPS]) Kawasaki disease
16 Treatment Treat underlying rheumatic fever disease. No specific treatment for the rash. Lesions usually resolve spontaneously. Treatment of rheumatic fever does not usually affect the rash.
17 Erythema Migrans Initial cutaneous presentation of Lyme disease in 60-90% of cases Lyme disease infection is caused by the spirochete Borrelia burgdorferi and transmitted by species of the Ixodes tick Lyme disease is most prevalent in US and in Europe (Scandinavia and central Europe)
18 Clinical Features Typically 1-2 weeks after tick detachment Erythematous annular plaque with light-colored central area of a bull s eye appearance Favors trunk, axilla, groin and popliteal fossa Untreated, usually last four weeks Disseminated EM EM and satellite oval-shaped widespread patches due to spirochetemia


19 Erythema Migrans
20 Stages and Major Organ Manifestations of Lyme Disease Early Localized disease EM, flu like symptoms, regional lymphadenopathy Early Disseminated disease neural involvement (facial nerve common), migratory joint pain, carditis, conjunctivitis Chronic Disease acrodermatitis chronica atrophicans, persistent neurologic and rheumatologic symptoms
21 Diagnosis Clinical presentation AND either history of exposure or laboratory evidence of infection PCR, culture, serological evidence Borrelia antibodies detection in serum might not be specific as peak specific IgM response is 3-6 weeks into infection Serologic tests will stay positive for months to years

22 Pathology Superficial and deep perivascular and interstitial infiltrate of lymphocytes, sometimes with abundant plasma cells and eosinophils Warthin-Starry stain is positive in 50% showing spirochetes
23 Differential Diagnosis Arthropod assault Erysipelas Cellulitis Non-pigmented fixed drug eruption Allergic contact dermatitis 23
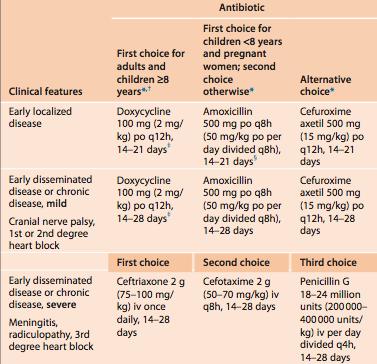
24 Treatment
25 Erythema Gyratum Repens Rare, males=females, Caucasians Gyrate polycyclic rapidly growing erythematous plaques with a trailing scale Migrates up to 1cm/day Wood grain resemblance due to rings within rings pattern Can be pruritic Additional findings: acquired ichthyosis, palmoplantar keratoderma and hypereosinophilia


26 Erythema Gyratum Repens
27 Erythema Gyratum Repens Unknown etiology, malignancy association >80% cases, i.e. the most specific paraneoplastic syndrome 1/3 patients= lung cancer, 8% esophageal cancer, 6% breast cancer The figurative eruption can precede, occur concurrently or appear after the diagnosis of the neoplasm Non-paraneoplastic cases: TB, CREST syndrome, pregnancy, bullous dermatosis
28 Differential Diagnosis Erythema annulare centrifugum Erythema migrans Resolving pityriasis rubra pilaris Erythrokeratoderma variablis 28
29 Erythema Gyratum Repens Treatment: identify and treat underlying malignancy
30 Purpuras
31 Definition Visible hemorrhage into the skin or mucous membranes. Divided into 6 subsets; Petechiae Macular Purpura Macular ecchymoses Palpable purpura Non-inflammatory retiform purpura Inflammatory retiform purpura
32 Petechiae (<4 mm red-purple hemorrhagic macules): Seen in: ITP, TTP, DIC, Platelet function defects, Aspirin/NSAID use, trauma, valsalva-manueaver, etc. Macular Purpura (5-9 mm red-purple hemorrhagic macules that don t blanch): Seen in: Hypergammaglobulenima of Waldenstrom, thrombocytopenia Macular Ecchymoses (>1 cm red-purple-green patch due to bleeding in skin): Seen in: Anticoagulant use, hepatic insufficiency, Vitamin K deficiency, DIC, Actinic purpura, steroid use, Vitamin C deficiency, Ehlers-Danlos disease, platelet function diseases, etc.


33 Purpura and Petechiae Macular Ecchymosis Macular purpuras are all due to hemorrhage, with mild inflammation and extravasated red blue cells causing what is seen in the patient.
34 Palpable Purpura: (raised, non-blanching inflammatory purpura with erythema) Seen in: Idiopathic, infection IgG/IgA/IgM complexes, Hypergammaglobulinemic purpura of Waldenstrom, Urticarial vasculitis, Mixed cryoglobulinimia, Rheumatic vasculitis, ANCA associated diseases, etc. Non-inflammatory retiform purpura (mottled lace-like livedo reticularis pattern causing a purple-ish discoloration): Seen in: Heparin necrosis, thrombocytosis, TTP, cryoglobulinimia, ecthyma gangrenosum, Protein C/S deficiency, warfarin necrosis, livedoid vasculopathy, cholesterol emboli, etc. Inflammatory retiform purpura (visible hemorrhage into skin or mucous membranes in the livedo reticularis pattern): Seen in: IgA vasculitis, mixed cryoglobulinimia, polyarteritis nodosa, chillblains, wegener s granulomatosis, livedoid vasculopathy, etc


35 Livedo Reticularis Retiform Purpura Seen due to blood flow regulation in dermal and subcutaneous vessels- and shows a net like pattern Retiform purpura is due to occlusion of vessels that cause the livedo reticularis; distinguish the 2 by presence or absence of purpura.
36 Coagulation
37 Coagulation Primary hemostasis consists of the formation of a platelet plug that is sufficient for minor injuries to the microvascular system If the size of the vessel or injury is too large, secondary hemostasis with clot formation is necessary Too little clotting death by hemorrhage Too much clotting thrombosis, embolus, necrosis Requires extensive regulation and balance between procoagulant, anticoagulant, and fibrinolytic pathways

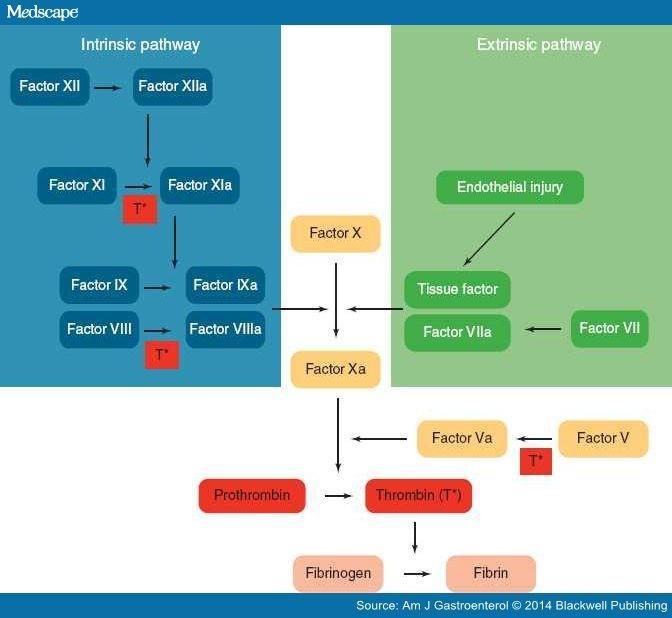
38 Coagulation Related Pathways Dermatology. 3 rd Edition, Bolognia.
39 Platelet Plug (Primary Hemostasis) ryn_dorman.jpg
40
41 Thrombin (factor II) Generated in small amounts from primary clot Activates platelets, leads to binding of procoagulant factors Also stimulates release of factor V from platelet granules Activates tissue factor VIIa Activates Factor IX to IXa and Factor X to Xa
42 Anticoagulant pathway Initiation phase of clotting is down-regulated by tissue factor pathway inhibitor (TFPI) and antithrombin III (ATIII) Both bound to heparin sulfate molecules on endothelial cells Capture activated clotting factors and prevent them from leaving the vicinity TFPI can inactivate factor Xa; ATIII can neutralize thrombin, factor IXa, Xa, XIIa Thrombomodulin/protein C/protein S Important in large vessels Thrombin from clot bind to thrombomodulin, and thus loses it ability to cause procoagulatory effects Activates protein C inactivates Factor Va, VIIIa
43 Tests for Coagulation Thorough history and physical exam Labs: Platelet count, PT, and APTT If PT or APTT prolonged, can repeat testing using 1:1 mixture of pt plasma and normal plasma ->if time normalizes then there is a factor deficiency Prolonged PT + normal APTT: factor VII deficiency or use of PO anticoagulant Prolonged APTT + normal PT: use of Heparin, lupus anticoagulant, acquired factor VIII deficiency, or von Willebrand Disease Prolonged PT + APTT: fibrinogen deficiency, prothrombin, factor V or Factor X deficiency
44 Pigmented Purpuric Eruptions Diseases characterized by petechial hemorrhage likely due to capillaritis Minimal inflammation and hemorrhage of superficial papillary dermal vessels Source of inflammation unknown and no coagulation abnormalities Several variants

45 Schamberg's Disease Yellow-brown patches with an oval to irregular outline, pinpoint petech Most common form, peak frequency in middle aged to older men Usually involves lower extremities Stasis purpura clinically has more hem Bolognia, Dermatology, figure 22.5a

46 Purpura annularis telangiectodes of Majocchi Uncommon, adolescents, young adults, especially women 1-3 cm annular plaques that slowly expand, punctate telangiectasias and petechiae within border, possible yellow center Trunk, proximal lower extremities Bolognia, Dermatology, figure 22.6
47 Rare Variants Pigmented purpuric lichenoid dermatitis of Gougerot and Blum: Schamberg like- purpuric red-brown lichenoid papules Eczematid-like purpura of Doucas and Kapetanakis: Scaly petechial or purpuric macs, paps and patches, usually pruritic Lichen aureus: solitary patch, color varies from golden to rust to purple brown

48 Lichen Aureus
49 Histology Red cell extravasation, endothelial swelling, perivascular lymphs, and hemosiderin containing macrophages Lichen aureus and Gougerot-Blum variants are characterized by lichenoid infiltrate Eczematid like purpura of Doucas and Kapetanakis often has spongiosis, patchy parakeratosis
50 Treatment Topical steroids especially if pruritic PUVA, NBUVB Ascorbic acid 500 mg BID with Rutoside 50 mg BID Cyclosporine
51 Hypergammaglobulinemic Purpura of Waldenstrom Associated with a hypergammaglobulinemia Presence of small circulating immune complexes containing IgG or IgA rheumatoid factor IgG and IgA rheumatoid factors are highly soluble, which may explain the speed with which lesions appear and resolve Can be primary or secondary In younger patients, it is usually primary, but eventually patients may develop an autoimmune connective tissue disease (usually Sjogren s) Complications include the development of a monoclonal gammopathy, lymphoma, or multiple myeloma Differential Dx: classic cutaneous small vessel vasculitis syndromes


52 Hypergammaglobulinemic Purpura of Waldenstrom Usually affects women Mild pruritus, tingling, or burning may precede the presence of purpura Symptoms are exacerbated by prolonged standing, tight fitting garments, and heat Petechiae or larger purpuric macules on lower extremities is the most common presentation Labs: Polyclonal hypergammaglobulinemia, elevated ESR, anti-ro and anti-la Abs are usually present and may predict a higher likelihood of developing autoimmune connective tissue disease Standard RF assays will only detect IgM, therefore they will not detect IgG or IgA

53 Pathology Histopathology may show hemorrhage, a mild perivascular infiltrate, or a leukocytoclastic vasculitis Image shows dilated superficial capillaries, extravasation of red blood cells, and sparse mononuclear infiltrate without evidence of vasculitis
54 Treatment Limited treatment options Aspirin Support stockings Avoidance of triggers such as alcohol, prolonged standing
55 Mondors Disease: First described in 1939 by Henri Mondor Superficial thrombosis (SVT) Self limited Most commonly seen in patients aged year old Female > male; 3:1


56 Clinical Presentation Predisposing factors include: Increased coagulation state Thoracic surgical procedures Breast surgery Tight clothes Mammary infections Pendulous breast Chronic inflammatory disease states Presents as a fibrous painful cord, with or without skin retraction, and with or without local inflammation. Can present on the chest well, involving other venous areas, and following breast disease
57 Work up Complete history and physical Ultrasonographic to confirm Mammography if suspicion of breast cancer
58 Most cases are idiopathic In a pool analysis of the four largest and most recent series: Idiopathic (32.5%) Breast Cancer (6.3%) Iatrogenic (11.9%) Inflammation (4.8%) Trauma (32.5%) Including: injury, muscular, heavy load, tight support, thrombophilia, hormone therapy
59 Treatment Mondor s on chest wall: Spontaneous resolution in 2-8 weeks Other locations: less known, can consider anticoagulation and etiologic management if known. Surgery in persistent cases Mondor s after breast surgery: This is not a thrombotic process. Reports suggest that manual rupture of the fibrous bands ensures immediate functional recovery and pain relief. Penile Mondor s: conservative treatment. There is approximately 13% recurrence
60 Conclusion Reviewed the four classic figurate erythemas: erythema annulare centrifugum, erythema marginatum, erythema migrans, and erythema gyratum repens Reviewed specific purpuric syndromes and treatment modalities Provided practical applications for these dermatological conditions
61 References Amy S. P, Anthony JM. Hurwitz Clinical Pediatric Dermatology, 12, Bejanga B.I.: Mondor's disease: Analysis of 30 cases. Journal of the Royal College of Surgeons of Edinburgh 1992; 37: pp Ben-Horin S., Lubetsky A., Heyman Z., and Kleinbaum Y.: Superficial abdominal thrombophlebitis (Mondor's disease) presenting as loss of response to adalimumab in a Crohn's disease patient. Journal of Crohn's and Colitis 2014; 8: pp Boyd AS, Neldner KH, Menter A. Erythema gyrate repens: a paraneoplastic eruption. J Am Acad Dermatol. 1992;26: Bologna, Jean., Jorizzo, Joseph L.Schaffer, Julie V., eds. Dermatology. Philadelphia, Elsevier Saunders, Burak O, Enis C, Ali T, Emre A, Veli Y. Urology (2015) January (85) 1: Catania S., Zurrida S., Veronesi P., Galimberti V., Bono A., and Pluchinotta A.: Mondor's disease and breast cancer. Cancer 1992; 69: pp Clemetson KJ. Platelets and primary haemostasis. Thromb Res 2012; 129: De La Torre-Lugo EM, Sánchez JL. Erythema gyratum repens. J Am Acad Dermatol May; 64(5):e89 e90 "Erythema Annulare Centrifugum." Mydermpath. N.p., n.d. Web. 16 Jan Finder KA, McCollough ML, Dixon SL, Majaka KA, Jaremko W. Hypergammaglobulinemic purpura of waldenstrom. JAAD, October 1990: 23, Fitzpatrick, JE. Dermatology Secrets plus. 67; Fitzpatrick, Thomas B. Dermatology in General Medicine. New York: McGraw-Hill, Print. Furie B, Furie BC. Mechanisms of thrombus formation. N Engl J Med. 2008;359: Griffin J. Control of coagulation reactions. In: Lichtman M, Beutler E, Kaushansky K, et al (eds). Williams Hematology, 7th edn. New York: McGraw-Hill, 2006: Hirano S.A., Mason A.R., Warthan M.M., and Pariser R.J.: Mondor disease in a patient with psoriasis treated with an anti-interleukin 12/interleukin 23 investigational drug. Archives of Dermatology 2010; 146: pp J.P. Laroche, J. Galanaud, D. Labau, A. Khaun Van Kien, D. Brisot, G. Boge and I. Quere. Thrombosis Research. (2012):October (130) Kim DH, Seo SH, Ahn HH, Kye YC, Choi JE. Characteristics and Clinical Manifestations of Pigmented Purpuric Dermatosis. Ann Dermatol Aug. 27 (4): Laufer F. The treatment of progressive pigmented purpura with ascorbic acid and a bioflavonoid rutoside. J Drugs Dermatol Mar. 5(3): Mehdi I, Fatma D, Idil U. Gardner-Diamond syndrome in a pediatric patient. Dermatologica Sinica, (2016) June (34)2: Naveen KN, Kalinga B, Pai VV, Athanikar SB, Sori T, Raju K, Rao R. Erythema gyratum repens like figurate erythema responding to topical steroid in an healthy individual. Indian J Dermatol Jul;58(4):329. Seckin D, Yazici Z, Senol A, Demircay Z. A case of Schamberg's disease responding dramatically to PUVA treatment. Photodermatol Photoimmunol Photomed Apr. 24(2):95-6. Tan E, Ng SK, Tan SH, Wong GC. Hypergammaglobulinemic purpura presenting as reticulate purpura. Cli Exp Dermatol 1999; 24,
62 Thank You
=ﻰﻤاﻤﺤﻠا ﺔﻴﻘﻠﺤﻠا ﺔذﺒاﻨﻠا
 1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
Haemostasis & Coagulation disorders Objectives:
 Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
CPC. Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand
 CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3
CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
BLEEDING DISORDERS Simple complement:
 BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
BLEEDING DISORDERS Simple complement: 1. Select the statement that describe the thrombocytopenia definition: A. Marked decrease of the Von Willebrandt factor B. Absence of antihemophilic factor A C. Disorder
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
CIC Edizioni Internazionali. Cutaneous vasculitides and vasculopathies. Review. Giampiero Girolomoni Paolo Rosina. severity.
 Review Cutaneous vasculitides and vasculopathies Giampiero Girolomoni Paolo Rosina Department of Medicine Section of Dermatology University of Verona, Italy Address for correspondence: Paolo Rosina, MD
Review Cutaneous vasculitides and vasculopathies Giampiero Girolomoni Paolo Rosina Department of Medicine Section of Dermatology University of Verona, Italy Address for correspondence: Paolo Rosina, MD
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT
 HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
THE TIP OF THE ICEBERG SAMER BOLIS, DO PGY-3 LEHIGH VALLEY HEALTH NETWORK, ALLENTOWN PA
 THE TIP OF THE ICEBERG SAMER BOLIS, DO PGY-3 LEHIGH VALLEY HEALTH NETWORK, ALLENTOWN PA Case The patient is a 48 year-old female, who recently returned from a trip to Puerto Rico. She presents to the ED
THE TIP OF THE ICEBERG SAMER BOLIS, DO PGY-3 LEHIGH VALLEY HEALTH NETWORK, ALLENTOWN PA Case The patient is a 48 year-old female, who recently returned from a trip to Puerto Rico. She presents to the ED
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College
 Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Dr. Rai Muhammad Asghar Associate Professor Head of Pediatric Department Rawalpindi Medical College AN APPROACH TO BLEEDING DISORDERS NORMAL HEMOSTASIS After injury, 3 processes halt bleeding Vasoconstriction
Title: Erythema annulare centrifugum associated with chronic lymphocytic leukaemia. Authors: Helbling I, Walewska R, Dyer MJS, Bamford M, Harman KE
 Title: Erythema annulare centrifugum associated with chronic lymphocytic leukaemia Authors: Helbling I, Walewska R, Dyer MJS, Bamford M, Harman KE Sir, A wide range of conditions have been described as
Title: Erythema annulare centrifugum associated with chronic lymphocytic leukaemia Authors: Helbling I, Walewska R, Dyer MJS, Bamford M, Harman KE Sir, A wide range of conditions have been described as
BSD Self Assessment Workshop 7 th July 2013 CASE 27 RAC6123
 BSD Self Assessment Workshop 7 th July 2013 CASE 27 RAC6123 M55. 4/7 tender lesions on knee, legs and arms. Also iritis/ weight loss/headache, synovitis.?vasculitis. Sarcoidosis. Biopsy from left elbow
BSD Self Assessment Workshop 7 th July 2013 CASE 27 RAC6123 M55. 4/7 tender lesions on knee, legs and arms. Also iritis/ weight loss/headache, synovitis.?vasculitis. Sarcoidosis. Biopsy from left elbow
Egyptian Dermatology Online Journal Vol. 6 No 1: 14, June 2010
 Wells Syndrome H. Gammaz, H. Amer, A. Adly and S. Mahmoud Egyptian Dermatology Online Journal 6 (1): 14 Al-Haud Al-Marsoud Hospital, Cairo, Egypt e-mail: hananderma@hotmail.com Submitted: April 15, 2010
Wells Syndrome H. Gammaz, H. Amer, A. Adly and S. Mahmoud Egyptian Dermatology Online Journal 6 (1): 14 Al-Haud Al-Marsoud Hospital, Cairo, Egypt e-mail: hananderma@hotmail.com Submitted: April 15, 2010
UNIT VI. Chapter 37: Platelets Hemostasis and Blood Coagulation Presented by Dr. Diksha Yadav. Copyright 2011 by Saunders, an imprint of Elsevier Inc.
 UNIT VI Chapter 37: Platelets Hemostasis and Blood Coagulation Presented by Dr. Diksha Yadav Hemostasis: Prevention of Blood Loss Vascular constriction Formation of a platelet plug Formation of a blood
UNIT VI Chapter 37: Platelets Hemostasis and Blood Coagulation Presented by Dr. Diksha Yadav Hemostasis: Prevention of Blood Loss Vascular constriction Formation of a platelet plug Formation of a blood
Approach To A Bleeding Patient
 ABDUL MAJEED, RAHUL RAJEEV REVIEW ARTICLE INTRODUCTION Hemostasis is the process of forming clots in the walls of damaged blood vessels and preventing blood loss while maintaining blood in a fluid state
ABDUL MAJEED, RAHUL RAJEEV REVIEW ARTICLE INTRODUCTION Hemostasis is the process of forming clots in the walls of damaged blood vessels and preventing blood loss while maintaining blood in a fluid state
Bleeding and Thrombotic Disorders. Kristine Krafts, M.D.
 Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
What are blood clots?
 What are blood clots? Dr Matthew Fay GP Principal The Willows Medical Practice- Queensbury GPwSI and Co-Founder Westcliffe Cardiology Service GP Partner Westcliffe Medical Group Created 5/31/18 Dr. Matthew
What are blood clots? Dr Matthew Fay GP Principal The Willows Medical Practice- Queensbury GPwSI and Co-Founder Westcliffe Cardiology Service GP Partner Westcliffe Medical Group Created 5/31/18 Dr. Matthew
PSEUDO-CELLULITIS - ALL THAT S RED IS NOT INFECTION
 JAN 18 2018 ASP ECHO CLINIC CHARLES KRASNER, M.D. PSEUDO-CELLULITIS - ALL THAT S RED IS NOT INFECTION FIRST HOSPITALIZATION: 62 YEAR OLD MALE ADMITTED WITH DIAGNOSIS OF CELLULITIS Hx of AODM, Morbid Obesity,
JAN 18 2018 ASP ECHO CLINIC CHARLES KRASNER, M.D. PSEUDO-CELLULITIS - ALL THAT S RED IS NOT INFECTION FIRST HOSPITALIZATION: 62 YEAR OLD MALE ADMITTED WITH DIAGNOSIS OF CELLULITIS Hx of AODM, Morbid Obesity,
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Thrombophilia. Diagnosis and Management. Kevin P. Hubbard, DO, FACOI
 Thrombophilia Diagnosis and Management Kevin P. Hubbard, DO, FACOI Clinical Professor of Medicine Kansas City University of Medicine and Biosciences-College of Osteopathic Medicine Kansas City, Missouri
Thrombophilia Diagnosis and Management Kevin P. Hubbard, DO, FACOI Clinical Professor of Medicine Kansas City University of Medicine and Biosciences-College of Osteopathic Medicine Kansas City, Missouri
There are two main causes of a low platelet count
 Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Glistening, Skin-Colored Nodule
 To Print: Click your browser's PRINT button. NOTE: To view the article with Web enhancements, go to: http://www.medscape.com/viewarticle/436334 Medscape Dermatology Clinic Glistening, Skin-Colored Nodule
To Print: Click your browser's PRINT button. NOTE: To view the article with Web enhancements, go to: http://www.medscape.com/viewarticle/436334 Medscape Dermatology Clinic Glistening, Skin-Colored Nodule
Future of Pediatrics: Blisters, Hives and Other Tales from the Emergency Room June 14 th, 2016
 A. Yasmine Kirkorian MD Assistant Professor of Dermatology & Pediatrics Children s National Health System George Washington University School of Medicine & Health Sciences Future of Pediatrics: Blisters,
A. Yasmine Kirkorian MD Assistant Professor of Dermatology & Pediatrics Children s National Health System George Washington University School of Medicine & Health Sciences Future of Pediatrics: Blisters,
FIT Board Review Corner April 2017
 FIT Board Review Corner April 2017 Welcome to the FIT Board Review Corner, prepared by Tammy Peng, MD, and Amar Dixit, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
FIT Board Review Corner April 2017 Welcome to the FIT Board Review Corner, prepared by Tammy Peng, MD, and Amar Dixit, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
S003 CPC Self-Assessment
 S003 CPC Self-Assessment Alina G. Bridges, D.O. Associate Professor Program Director, Dermatopathology Fellowship Department of Dermatology, Division of Dermatopathology and Cutaneous Immunopathology Mayo
S003 CPC Self-Assessment Alina G. Bridges, D.O. Associate Professor Program Director, Dermatopathology Fellowship Department of Dermatology, Division of Dermatopathology and Cutaneous Immunopathology Mayo
HEMODYNAMIC DISORDERS
 HEMODYNAMIC DISORDERS Normal fluid homeostasis requires vessel wall integrity as well as maintenance of intravascular pressure and osmolarity within certain physiologic ranges. Increases in vascular volume
HEMODYNAMIC DISORDERS Normal fluid homeostasis requires vessel wall integrity as well as maintenance of intravascular pressure and osmolarity within certain physiologic ranges. Increases in vascular volume
Mucinoses Diverse group of disorders which have in common deposition of basophilic, finely granular and stringy material in the connective tissues of
 Cutaneous Mucinoses Nathan C. Walk, M.D. Mucinoses Diverse group of disorders which have in common deposition of basophilic, finely granular and stringy material in the connective tissues of the dermis.
Cutaneous Mucinoses Nathan C. Walk, M.D. Mucinoses Diverse group of disorders which have in common deposition of basophilic, finely granular and stringy material in the connective tissues of the dermis.
Thursday, February 26, :00 am. Regulation of Coagulation/Disseminated Intravascular Coagulation HEMOSTASIS/THROMBOSIS III
 REGULATION OF COAGULATION Introduction HEMOSTASIS/THROMBOSIS III Regulation of Coagulation/Disseminated Coagulation necessary for maintenance of vascular integrity Enough fibrinogen to clot all vessels
REGULATION OF COAGULATION Introduction HEMOSTASIS/THROMBOSIS III Regulation of Coagulation/Disseminated Coagulation necessary for maintenance of vascular integrity Enough fibrinogen to clot all vessels
REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES. R e g i S C A R PATIENT'S DATA. Age country of birth
 REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES R e g i S C A R PATIENT'S DATA Initials of the patient date of birth Age country of birth Gender male female
REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES R e g i S C A R PATIENT'S DATA Initials of the patient date of birth Age country of birth Gender male female
A. Erythema multiforme and related diseases
 Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
Tick Talk: What s new in Lyme Disease. May 5 th, 2017 Cristina Baker, M.D., M.P.H.
 Tick Talk: What s new in Lyme Disease May 5 th, 2017 Cristina Baker, M.D., M.P.H. Dr. Baker indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Tick Talk: What s new in Lyme Disease May 5 th, 2017 Cristina Baker, M.D., M.P.H. Dr. Baker indicated no potential conflict of interest to this presentation. She does not intend to discuss any unapproved/investigative
Cutanous Manifestation of Lupus Erythematosus. Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university
 Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
Citation The Journal of Dermatology, 37(8), available at
, available at") NAOSITE: Nagasaki University's Ac Title Two cases of blaschkitis with promi Author(s) Utani, Atsushi Citation The Journal of Dermatology, 37(8), Issue Date 2010-08 URL Right http://hdl.handle.net/10069/25634
NAOSITE: Nagasaki University's Ac Title Two cases of blaschkitis with promi Author(s) Utani, Atsushi Citation The Journal of Dermatology, 37(8), Issue Date 2010-08 URL Right http://hdl.handle.net/10069/25634
Bleeding Disorders. Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph
 Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
LYME DISEASE Last revised May 30, 2012
 Wisconsin Department of Health Services Division of Public Health Communicable Disease Surveillance Guideline LYME DISEASE Last revised May 30, 2012 I. IDENTIFICATION A. CLINICAL DESCRIPTION: A multi-systemic
Wisconsin Department of Health Services Division of Public Health Communicable Disease Surveillance Guideline LYME DISEASE Last revised May 30, 2012 I. IDENTIFICATION A. CLINICAL DESCRIPTION: A multi-systemic
HAEMORRHAGIA Bleeding
 HAEMORRHAGIA Bleeding Cassification Size Location pathomechanism Hematoma: external or may be enclosed within a tissue petechiae : 1-2 mm hemorrhages into skin, mucous membranes, or serosal surfaces increased
HAEMORRHAGIA Bleeding Cassification Size Location pathomechanism Hematoma: external or may be enclosed within a tissue petechiae : 1-2 mm hemorrhages into skin, mucous membranes, or serosal surfaces increased
HENOCH SCHÖNLEIN PURPURA (VASCULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests (SC)
 IN CHILDREN Single choice tests (SC)") HENOCH HÖNLEIN PURPURA (VAULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests () 1. Choose the type of bleeding characteristic for the Henoch Schönlein purpura (vascular purpura, anaphylactoid
HENOCH HÖNLEIN PURPURA (VAULAR PURPURA, ANAPHYLACTOID PURPURA) IN CHILDREN Single choice tests () 1. Choose the type of bleeding characteristic for the Henoch Schönlein purpura (vascular purpura, anaphylactoid
Bacterial Infections. Ron Rapini MD Chernosky Chair Dept Dermatology Professor of Pathology Univ of Texas and MD Anderson Cancer Cntr Houston, Texas
 Bacterial Infections Ron Rapini MD Chernosky Chair Dept Dermatology Professor of Pathology Univ of Texas and MD Anderson Cancer Cntr Houston, Texas Conflict of interest statement: Book royalties- Elsevier
Bacterial Infections Ron Rapini MD Chernosky Chair Dept Dermatology Professor of Pathology Univ of Texas and MD Anderson Cancer Cntr Houston, Texas Conflict of interest statement: Book royalties- Elsevier
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN
 Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Hemodynamic Disorders, Thrombosis, and Shock. Richard A. McPherson, M.D.
 Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
Discussion. Dr Venu 2 nd year, General medicine
 Discussion Dr Venu 2 nd year, General medicine Introduction Warfarin-induced skin necrosis (WISN) is usually an unpredictable complication of warfarin therapy, occurring in 0.01-0.1% of warfarin treated
Discussion Dr Venu 2 nd year, General medicine Introduction Warfarin-induced skin necrosis (WISN) is usually an unpredictable complication of warfarin therapy, occurring in 0.01-0.1% of warfarin treated
Abscess. A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body.
 Abscess A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body. Ethyology Bacteria causing cutaneous abscesses are typically indigenous
Abscess A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body. Ethyology Bacteria causing cutaneous abscesses are typically indigenous
الاكزيماتيد= Eczematid
 1 / 7 2 / 7 Pityriasis Debate confusing of hypopigmentation characterized increasing surrounded differ hypomelanotic "progressive exists alba misnomer extensive a to observed term the applied term derived
1 / 7 2 / 7 Pityriasis Debate confusing of hypopigmentation characterized increasing surrounded differ hypomelanotic "progressive exists alba misnomer extensive a to observed term the applied term derived
Part IV Antithrombotics, Anticoagulants and Fibrinolytics
 Part IV Antithrombotics, Anticoagulants and Fibrinolytics "The meaning of good and bad, of better and worse, is simply helping or hurting" Emerson Chapter 16: Blood Coagulation and Fibrinolytic System
Part IV Antithrombotics, Anticoagulants and Fibrinolytics "The meaning of good and bad, of better and worse, is simply helping or hurting" Emerson Chapter 16: Blood Coagulation and Fibrinolytic System
Thrombosis. By Dr. Sara Mohamed Abuelgasim
 Thrombosis By Dr. Sara Mohamed Abuelgasim 1 Thrombosis Unchecked, blood coagulation would lead to dangerous occlusion of blood vessels if the protective mechanisms of coagulation factor inhibitors, blood
Thrombosis By Dr. Sara Mohamed Abuelgasim 1 Thrombosis Unchecked, blood coagulation would lead to dangerous occlusion of blood vessels if the protective mechanisms of coagulation factor inhibitors, blood
Common Cutaneous Signs of Medical Illnesses
 Common Cutaneous Signs of Medical Illnesses DR COLIN THENG MBBS, MMED (FAM. MED), MRCP(UK), FAMS SENIOR CONSULTANT DERMATOLOGIST THE SKIN SPECIALISTS & LASER CLINIC MOUNT ALVERNIA MEDICAL CENTRE D, #07-61
Common Cutaneous Signs of Medical Illnesses DR COLIN THENG MBBS, MMED (FAM. MED), MRCP(UK), FAMS SENIOR CONSULTANT DERMATOLOGIST THE SKIN SPECIALISTS & LASER CLINIC MOUNT ALVERNIA MEDICAL CENTRE D, #07-61
Hemodynamic Disorders, Thromboembolic Disease, and Shock
 Hemodynamic Disorders, Thromboembolic Disease, and Shock Kumar et al: Robbins & Cotran Pathologic Basis of Disease 7E Figure 4-1 Factors affecting fluid balance across capillary walls. Capillary hydrostatic
Hemodynamic Disorders, Thromboembolic Disease, and Shock Kumar et al: Robbins & Cotran Pathologic Basis of Disease 7E Figure 4-1 Factors affecting fluid balance across capillary walls. Capillary hydrostatic
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc 1 Common Rashes Tinea Corporis: Annular- this is not the only criteria Advancing erythematous
An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc 1 Common Rashes Tinea Corporis: Annular- this is not the only criteria Advancing erythematous
44 year-old male. Follicular Hyperkeratosis 3/4/2019. Clinical: Erythematous scaling papules symmetrically on the forearms, abdomen and lower back
 DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Dermatopathology Case Challenge: Recognizing Mimics and Masqueraders Tammie Ferringer, MD Section Head and Fellowship Director of Dermatopathology Depts of Dermatology
DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Dermatopathology Case Challenge: Recognizing Mimics and Masqueraders Tammie Ferringer, MD Section Head and Fellowship Director of Dermatopathology Depts of Dermatology
Blood Lecture Test Questions Set 2 Summer 2012
 Blood Lecture Test Questions Set 2 Summer 2012 1. Leukocytes are attracted to a site of injury or disease by: a. diapedesis b. chemotaxis c. leukocytosis d. heparin e. leukomotosis 2. Leukocytes leave
Blood Lecture Test Questions Set 2 Summer 2012 1. Leukocytes are attracted to a site of injury or disease by: a. diapedesis b. chemotaxis c. leukocytosis d. heparin e. leukomotosis 2. Leukocytes leave
Jordan M. Garrison, MD FACS, FASMBS
 Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Disclaimer. This is a broad survey and cannot cover all differential diagnoses or each condition in thorough detail
 Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Erythematous rash icd 10
 Erythematous rash icd 10 Search 2-4-2017 If you re having problems with your gallbladder, your doctor may want you to have a special test called a hepatobiliary iminodiacetic acid (HIDA) scan. International
Erythematous rash icd 10 Search 2-4-2017 If you re having problems with your gallbladder, your doctor may want you to have a special test called a hepatobiliary iminodiacetic acid (HIDA) scan. International
Degos Disease: A Case Report and Review of Literature
 Degos Disease: A Case Report and Review of Literature Monira waked Egyptian Dermatology Online Journal 4 (1): 5, June 2008 Al Houd Al Marsod Hospital Submitted for publication: May 25 th, 2008 Accepted
Degos Disease: A Case Report and Review of Literature Monira waked Egyptian Dermatology Online Journal 4 (1): 5, June 2008 Al Houd Al Marsod Hospital Submitted for publication: May 25 th, 2008 Accepted
Hemostasis. Learning objectives Dr. Mária Dux. Components: blood vessel wall thrombocytes (platelets) plasma proteins
 plasma proteins") Hemostasis Learning objectives 14-16 Dr. Mária Dux Components: blood vessel wall thrombocytes (platelets) plasma proteins Hemostatic balance! procoagulating activity anticoagulating activity 1 Thrombocytes
Hemostasis Learning objectives 14-16 Dr. Mária Dux Components: blood vessel wall thrombocytes (platelets) plasma proteins Hemostatic balance! procoagulating activity anticoagulating activity 1 Thrombocytes
Uncommon clinical presentations of leprosy: apropos of three cases
 Lepr Rev (2016) 87, 246 251 CASE REPORT Uncommon clinical presentations of leprosy: apropos of three cases RASHMI JINDAL* & NADIA SHIRAZI** *Department of Dermatology, Venereology & Leprosy, Himalayan
Lepr Rev (2016) 87, 246 251 CASE REPORT Uncommon clinical presentations of leprosy: apropos of three cases RASHMI JINDAL* & NADIA SHIRAZI** *Department of Dermatology, Venereology & Leprosy, Himalayan
2/23/18. Disclosures. Rheumatic Diseases of Childhood. Making Room for Rheumatology. I have nothing to disclose. James J.
 Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease:
 4. Associated with systemic disease:") Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease: Hematological GIT Behcet s HIV 5. Associated with dermatological diseases:
Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease: Hematological GIT Behcet s HIV 5. Associated with dermatological diseases:
Easy Bleeding General Presentation
 Easy Bleeding General Presentation It is not uncommon for children to bleed and bruise after experiencing trauma. However, a child may also have an underlying coagulopathy, which results in easy and possibly
Easy Bleeding General Presentation It is not uncommon for children to bleed and bruise after experiencing trauma. However, a child may also have an underlying coagulopathy, which results in easy and possibly
Chapter 14. Blood. Blood Volume. Blood Composition. Blood
 Blood connective tissue transports vital substances maintains stability of interstitial fluid distributes heat Chapter 14 Blood Blood Cells form mostly in red bone marrow red blood cells white blood cells
Blood connective tissue transports vital substances maintains stability of interstitial fluid distributes heat Chapter 14 Blood Blood Cells form mostly in red bone marrow red blood cells white blood cells
Clinical & Laboratory Assessment
 Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Haemorrhagic Disorders. Dr. Bashar Department of Pathology Mosul Medical College
 Haemorrhagic Disorders Dr. Bashar Department of Pathology Mosul Medical College Hemorrhagic Disorders These include Disorders of platelets. Disorders of blood vessels. Disorders of coagulation & fibrinolysis.
Haemorrhagic Disorders Dr. Bashar Department of Pathology Mosul Medical College Hemorrhagic Disorders These include Disorders of platelets. Disorders of blood vessels. Disorders of coagulation & fibrinolysis.
Bleeding Disorders: (Hemorrhagic Diatheses) Tests used to evaluate different aspects of hemostasis are the following:
 Tests used to evaluate different aspects of hemostasis are the following:") Bleeding Disorders: (Hemorrhagic Diatheses) Excessive bleeding can result from: 1. Increased fragility of vessels. 2. Platelet deficiency or dysfunction. 3. Derangement of coagulation. 4. Combinations
Bleeding Disorders: (Hemorrhagic Diatheses) Excessive bleeding can result from: 1. Increased fragility of vessels. 2. Platelet deficiency or dysfunction. 3. Derangement of coagulation. 4. Combinations
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Department of Dermatology, Christian Medical College and Hospital, Ludhiana, Punjab, India.
 Bullous pemphigoid mimicking granulomatous inflammation Abhilasha Williams, Emy Abi Thomas. Department of Dermatology, Christian Medical College and Hospital, Ludhiana, Punjab, India. Egyptian Dermatology
Bullous pemphigoid mimicking granulomatous inflammation Abhilasha Williams, Emy Abi Thomas. Department of Dermatology, Christian Medical College and Hospital, Ludhiana, Punjab, India. Egyptian Dermatology
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Index. Angiosarcoma diagnosis, 47 lymphedema-related vs. non-lymphedemarelated, 48
 A Acneiform rash biopsy, 134 cetuximab, EGFR, 132 133 diagnosis, 131 patient history, 131 134 treatment, 134 135 Acne vulgaris, 109 AGA. See Androgenetic alopecia Alopecia areata, 148 American Joint Committee
A Acneiform rash biopsy, 134 cetuximab, EGFR, 132 133 diagnosis, 131 patient history, 131 134 treatment, 134 135 Acne vulgaris, 109 AGA. See Androgenetic alopecia Alopecia areata, 148 American Joint Committee
10/24/2013. Heparin-Induced Thrombocytopenia (HIT) Anticoagulation Management in ECMO Therapy:
 Anticoagulation Management in ECMO Therapy:") Anticoagulation Management in ECMO Therapy: Heparin-Induced (HIT) Michael H. Creer, MD Professor of Pathology Director, Clinical Laboratories, Medical Co- Director, Hematopathology and Chief, Division
Anticoagulation Management in ECMO Therapy: Heparin-Induced (HIT) Michael H. Creer, MD Professor of Pathology Director, Clinical Laboratories, Medical Co- Director, Hematopathology and Chief, Division
Primary Exam Physiology lecture 5. Haemostasis
 Primary Exam Physiology lecture 5 Haemostasis Haemostasis Body s response for the prevention and cessation of bleeding. Broadly consists of: Primary Haemostasis - vascular spasm and platlet plug formation
Primary Exam Physiology lecture 5 Haemostasis Haemostasis Body s response for the prevention and cessation of bleeding. Broadly consists of: Primary Haemostasis - vascular spasm and platlet plug formation
Disseminated Intravascular Coagulation. M.Bahmanpour MD Assistant professor IUMS
 به نام خدا Disseminated Intravascular Coagulation M.Bahmanpour MD Assistant professor IUMS Algorithm for Diagnosis of DIC DIC Score factor score Presence of known underlying disorder No= 0 yes=2 Coagolation
به نام خدا Disseminated Intravascular Coagulation M.Bahmanpour MD Assistant professor IUMS Algorithm for Diagnosis of DIC DIC Score factor score Presence of known underlying disorder No= 0 yes=2 Coagolation
Ch. 45 Blood Plasma proteins, Coagulation and Fibrinolysis Student Learning Outcomes: Describe basic components of plasma
 Chapt. 45 Ch. 45 Blood Plasma proteins, Coagulation and Fibrinolysis Student Learning Outcomes: Describe basic components of plasma Inheritance of X-linked gene for Factor VIII hemophilia A Explain the
Chapt. 45 Ch. 45 Blood Plasma proteins, Coagulation and Fibrinolysis Student Learning Outcomes: Describe basic components of plasma Inheritance of X-linked gene for Factor VIII hemophilia A Explain the
Dermclinic
 Dermclinic /Dermclinic A Photo Quiz to Hone Dermatologic Skills DAVID L. KAPLAN, MD Series Editor University of Missouri Kansas City, University of Kansas Case 1: Upon his return from a summer visit to
Dermclinic /Dermclinic A Photo Quiz to Hone Dermatologic Skills DAVID L. KAPLAN, MD Series Editor University of Missouri Kansas City, University of Kansas Case 1: Upon his return from a summer visit to
4/23/2009. September 15, 2008
 The Current Treatment of Deep Venous Thrombosis: Are We Doing Enough? George H. Meier, MD Professor and Chief Division of Vascular Surgery University of Cincinnati College of Medicine Cincinnati, Ohio
The Current Treatment of Deep Venous Thrombosis: Are We Doing Enough? George H. Meier, MD Professor and Chief Division of Vascular Surgery University of Cincinnati College of Medicine Cincinnati, Ohio
Skin Manifestations of Systemic Disease. Approach to Dermatalogic Diagnosis 9/6/2016. Go Ahead---Judge a Book by its Cover!
 Go Ahead---Judge a Book by its Cover! Skin Manifestations of Systemic Disease Amelie Hollier, DNP, FNP-BC, FAANP Lafayette, LA President, APEA Objectives Compare diseases of the skin with reactions of
Go Ahead---Judge a Book by its Cover! Skin Manifestations of Systemic Disease Amelie Hollier, DNP, FNP-BC, FAANP Lafayette, LA President, APEA Objectives Compare diseases of the skin with reactions of
Update in deposition diseases
 Genoa, Italy Update in deposition diseases Prof. Franco Rongioletti, Section of Dermatology, Chair of Dermatopathology, University of Genoa,Italy Cutaneous deposition disorders Endogenous Exogenous Cutaneous
Genoa, Italy Update in deposition diseases Prof. Franco Rongioletti, Section of Dermatology, Chair of Dermatopathology, University of Genoa,Italy Cutaneous deposition disorders Endogenous Exogenous Cutaneous
Inherited Thrombophilia Testing. George Rodgers, MD, PhD Kristi Smock MD
 Inherited Thrombophilia Testing George Rodgers, MD, PhD Kristi Smock MD Prevalence and risk associated with inherited thrombotic disorders Inherited Risk Factor % General Population % Patients w/ Thrombosis
Inherited Thrombophilia Testing George Rodgers, MD, PhD Kristi Smock MD Prevalence and risk associated with inherited thrombotic disorders Inherited Risk Factor % General Population % Patients w/ Thrombosis
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
Thrombophilia: To test or not to test
 Kenneth Bauer, MD Harvard Medical School, Boston, MA Professor of Medicine VA Boston Healthcare System Chief, Hematology Section Beth Israel Deaconess Medical Center, Boston, MA Director, Thrombosis Clinical
Kenneth Bauer, MD Harvard Medical School, Boston, MA Professor of Medicine VA Boston Healthcare System Chief, Hematology Section Beth Israel Deaconess Medical Center, Boston, MA Director, Thrombosis Clinical
22 year old QH mare with regionally extensive alopecia and scaling on one front limb and ventral chest (Figure 1 and 2).
.") 22 year old QH mare with regionally extensive alopecia and scaling on one front limb and ventral chest (Figure 1 and 2). Which of the following is the most likely disease? a. Sterile granuloma complex
22 year old QH mare with regionally extensive alopecia and scaling on one front limb and ventral chest (Figure 1 and 2). Which of the following is the most likely disease? a. Sterile granuloma complex
Bacterial Infections in Pediatric Dermatology. Patrick McMahon, MD Children s Hospital of Philadelphia
 Bacterial Infections in Pediatric Dermatology Patrick McMahon, MD Children s Hospital of Philadelphia Fill In The Blank When you see on the skin, you think of a bacterial skin infection SEND SWABS VIRAL
Bacterial Infections in Pediatric Dermatology Patrick McMahon, MD Children s Hospital of Philadelphia Fill In The Blank When you see on the skin, you think of a bacterial skin infection SEND SWABS VIRAL
G. Types of White Blood Cells
 1. White blood cells are also called leukocytes. G. Types of White Blood Cells 2. White blood cells function to protect against diseases. 3. Two hormones that stimulate white blood cell production are
1. White blood cells are also called leukocytes. G. Types of White Blood Cells 2. White blood cells function to protect against diseases. 3. Two hormones that stimulate white blood cell production are
PGALS: Approach to Child with Arthritis. Prof Chris Scott Paediatric Rheumatology
 PGALS: Approach to Child with Arthritis Prof Chris Scott Paediatric Rheumatology Introduction In a prospective study from The Royal Hospital for Sick Children, Edinburgh, every 58th child presented with
PGALS: Approach to Child with Arthritis Prof Chris Scott Paediatric Rheumatology Introduction In a prospective study from The Royal Hospital for Sick Children, Edinburgh, every 58th child presented with
THROMBOTIC DISORDERS: The Final Frontier
 THROMBOTIC DISORDERS: The Final Frontier Jeffrey I. Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis Heart & Stroke Foundation/ J.F.
THROMBOTIC DISORDERS: The Final Frontier Jeffrey I. Weitz, MD, FRCP(C), FACP Professor of Medicine and Biochemistry McMaster University Canada Research Chair in Thrombosis Heart & Stroke Foundation/ J.F.
BLUE BERRY MUFFIN BABY SYNDROME. Kunrathur, Chennai, Tamil Nadu, India
 TJPRC: International Journal of Obstetric, Gynaecologic & Neonatal Nursing (TJPRC: IJOGNN) Vol. 1, Issue 1, Jun 2017, 17-20 TJPRC Pvt. Ltd. BLUE BERRY MUFFIN BABY SYNDROME TAMILARASI. B 1 & KANAGAVALLI.
TJPRC: International Journal of Obstetric, Gynaecologic & Neonatal Nursing (TJPRC: IJOGNN) Vol. 1, Issue 1, Jun 2017, 17-20 TJPRC Pvt. Ltd. BLUE BERRY MUFFIN BABY SYNDROME TAMILARASI. B 1 & KANAGAVALLI.
Cutaneous Drug Reactions
 Cutaneous Drug Reactions Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses
Cutaneous Drug Reactions Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses
Retrospective 10 years review of 100 patients with psoriasis in the Kingdom of Saudi Arabia (KSA)
") Retrospective 10 years review of 100 patients with psoriasis in the Kingdom of Saudi Arabia (KSA) Ahmed Abdullah Alhumidi King saud university, Riyadh, kingdom of Saudi Arabia Abstract Background: This
Retrospective 10 years review of 100 patients with psoriasis in the Kingdom of Saudi Arabia (KSA) Ahmed Abdullah Alhumidi King saud university, Riyadh, kingdom of Saudi Arabia Abstract Background: This
Skin Deep: Cutaneous Lupus. Dr Sarah Sasson Immunology Registrar, Liverpool Hospital 2016
 Skin Deep: Cutaneous Lupus Dr Sarah Sasson Immunology Registrar, Liverpool Hospital 2016 Introduction: Cutaneous lupus erythematosus LE is an autoimmune disease with a range of clinical manifestations
Skin Deep: Cutaneous Lupus Dr Sarah Sasson Immunology Registrar, Liverpool Hospital 2016 Introduction: Cutaneous lupus erythematosus LE is an autoimmune disease with a range of clinical manifestations
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
PCCN Review Hematology
 PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
PCCN Review Hematology Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Anemia Definition reduction in RBC concentration Causes iron deficiency
0BCore Safety Profile. Pharmaceutical form(s)/strength: Cream 1% DK/H/PSUR/0009/005 Date of FAR:
/strength: Cream 1% DK/H/PSUR/0009/005 Date of FAR:") 0BCore Safety Profile Active substance: Pimecrolimus Pharmaceutical form(s)/strength: Cream 1% P-RMS: DK/H/PSUR/0009/005 Date of FAR: 06.06.2013 4.3 Contraindications Hypersensitivity to pimecrolimus,
0BCore Safety Profile Active substance: Pimecrolimus Pharmaceutical form(s)/strength: Cream 1% P-RMS: DK/H/PSUR/0009/005 Date of FAR: 06.06.2013 4.3 Contraindications Hypersensitivity to pimecrolimus,
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
CUTANEOUS DRUG REACTIONS OR I WOULDN T HAVE SEEN IT, IF I HADN T BELIEVED IT Edmund J. Rosser Jr., DVM, DACVD
 CUTANEOUS DRUG REACTIONS OR I WOULDN T HAVE SEEN IT, IF I HADN T BELIEVED IT Edmund J. Rosser Jr., DVM, DACVD DERMATOLOGY Pathogenesis Immunologic: can involve Type I, II, III, IV hypersensitivity reactions.
CUTANEOUS DRUG REACTIONS OR I WOULDN T HAVE SEEN IT, IF I HADN T BELIEVED IT Edmund J. Rosser Jr., DVM, DACVD DERMATOLOGY Pathogenesis Immunologic: can involve Type I, II, III, IV hypersensitivity reactions.
Objectives. Terminology. Recognize common pediatric dermatologic conditions. Review treatment plans Identify skin manifestations of systemic disease
 Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
Sysmex Educational Enhancement and Development No
 SEED Coagulation Sysmex Educational Enhancement and Development No 2 2016 An approach to the bleeding patient The purpose of this newsletter is to provide an overview of the approach to the bleeding patient
SEED Coagulation Sysmex Educational Enhancement and Development No 2 2016 An approach to the bleeding patient The purpose of this newsletter is to provide an overview of the approach to the bleeding patient
This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion
 This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms
This slide belongs to iron lecture and it is to clarify the iron cycle in the body and the effect of hypoxia on erythropoitein secretion Topics of today lectures: Hemostasis Meaning of hemostasis Mechanisms
Conflicts. Objectives. University of Texas Health Science Center at San Antonio. Pediatrics Grand Rounds 24 August Pediatric Dermatology 101
 Pediatric Dermatology 101 John C. Browning, MD, FAAD, FAAP Conflicts Investigator: ViroXis Advisor: ViroXis Advisory Board: TopMD Speaker: Galderma Objectives Understand the meaning and importance of cutaneous
Pediatric Dermatology 101 John C. Browning, MD, FAAD, FAAP Conflicts Investigator: ViroXis Advisor: ViroXis Advisory Board: TopMD Speaker: Galderma Objectives Understand the meaning and importance of cutaneous
Disseminated Intravascular Coagulation (DIC) Seminar. Ron Kopilov 4 th year Medical Student, Tel Aviv University Internal Medicine A 8.3.
 Seminar. Ron Kopilov 4 th year Medical Student, Tel Aviv University Internal Medicine A 8.3.") Disseminated Intravascular Coagulation (DIC) Seminar Ron Kopilov 4 th year Medical Student, Tel Aviv University Internal Medicine A 8.3.2012 1 Our plan: Understand the pathophysiology Identify risk factors
Disseminated Intravascular Coagulation (DIC) Seminar Ron Kopilov 4 th year Medical Student, Tel Aviv University Internal Medicine A 8.3.2012 1 Our plan: Understand the pathophysiology Identify risk factors
Autoimmune Diseases with Oral Manifestations
 Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential