Diabetes Update 2018: Challenging Transitions. Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System
|
|
|
- Milo Morrison
- 5 years ago
- Views:
Transcription
1 Diabetes Update 2018: Challenging Transitions Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System 1
2 Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System Disclosures: None 2
3 Diabetes Update 2018: Challenging Transitions Hyperglycemia in the hospital setting Common Costly Associated with poor clinical outcomes Glycemic targets have been modified mg/dl Insulin is the treatment of choice to manage hyperglycemia in hospital setting Hyperglycemia management requires multidisciplinary collaboration 3
4 Diabetes Update 2018: Challenging Transitions Hyperglycemia management in hospital setting is challenging, especially in specific situations. Changes in patient location Admission Transfer between units Discharge Changes in oral intake Stress of illness, surgery Changes in renal or liver function Interaction between hospital events and medications and the patient s outpatient medication regimen
5 Diabetes Update 2018: Challenging Transitions Review appropriate management of patients with hyperglycemia in hospital setting Discuss how transitions in care impact blood sugar control Understand how noninsulin diabetic medications work and how they may interact; review specific issues with their use in hospital setting Provide overview of upcoming new VHS hypoglycemia and hyperglycemia policies and how these may help improve diabetes management in the hospital 5
6 Factors Affecting Blood Glucose Levels in the Hospital Setting Increased counter-regulatory ( stress ) hormones Changing IV glucose rates TPN and enteral feedings Lack of physical activity Unusual or inappropriate timing of insulin injections Use of glucocorticoids Unpredictable or inconsistent food intake Fear of hypoglycemia Cultural acceptance of hyperglycemia TPN, total parenteral nutrition. Carter L. Oklahoma Nutrition Manual, 12 th ed. Owasso, OK: Oklahoma Dietetic Association;
7 Glucose Control Deteriorates During Hospitalization Hyperglycemic Influences Stress hyperglycemia Concomitant therapy Decreased physical activity Medication omissions Medication errors Fear of hypoglycemia Hypoglycemic Influences Decreased caloric intake Gastrointestinal illness Monitored compliance Medication errors Altered cognition Residual effects of home medications Decline in kidney or liver function Metchick LN, et al. Am J Med. 2002;113:
8 Patient AL 65yo man admitted with possible recurrent stroke New onset DM with admission glucose 682. A1c > 14 8
9 AL 65yo man admitted with possible recurrent stroke. New onset DM with admission glucose 682. A1c > 14. How should his diabetes be managed in the hospital? What discharge planning will he require? What should his discharge diabetic medication regimen be? 9
10 Glycemic Management Strategies in Hospitalized Patients (Non-critically ill) Insulin therapy preferred regardless of type of diabetes Discontinue noninsulin agents at hospital admission of most patients with type 2 diabetes with acute illness Use scheduled SC insulin with basal, nutritional, and correction components Modify insulin dose in patients treated with insulin before admission to reduce risk for hypoglycemia and hyperglycemia Avoid prolonged therapy with sliding scale insulin alone Umpierrez GE, et al. J Clin Endocrinol Metab. 2012;97:
11 Glycemic Targets in Noncritical Care Setting Insulin therapy should be initiated for treatment of persistent hyperglycemia starting at a threshold 180 mg/dl (10.0 mmol/l). Once insulin therapy is started, a target glucose range of mg/dl is recommended for the majority of patients. More stringent goals, such as mg/dl, may be appropriate for selected patients, if this can be achieved without significant hypoglycemia. Less stringent targets may be appropriate in terminally ill patients or in patients with severe comorbidities ADA 2018 Umpierrez GE, et al. J Clin Endocrinol Metab. 2012;97:
12 What about noninsulin diabetic medications in the hospital? 12
13 Insulin vs Noninsulin Medications, how to decide? Does the patient have type 1 or type 2 diabetes? Noninsulin medications only indicate for type 2 If diagnosis is uncertain, screen patient for autoantibodies that are present in type 1 Thin patient with poor response to initial therapy with noninsulin diabetic medications Personal or family history of autoimmune disease Overweight or obese children/adolescents with apparent type 2 who may actually have early type 1 ADA 2018 Umpierrez GE, et al. J Clin Endocrinol Metab. 2012;97:
14 Insulin vs Noninsulin Medications, how to decide? If patient has new type 2 diabetes and A1c is 9% or above, initial therapy should include insulin, and may also include other agents if appropriate ADA and AACE guidelines ADA 2018 Umpierrez GE, et al. J Clin Endocrinol Metab. 2012;97:
15 Pathophysiology of DM2 Pancreas Muscle Increase glucose uptake Decreased insulin secretion from -cells Liver Increased endogenous glucose production Adipose (fat) Increased FFA production The Ominous Octet Digestive tract Decreased incretin effect Brain Neurotransmitter dysfunction DeFronzo RA. Diabetes. 2009;58: Increased glucagon secretion from -cells Pancreas Kidney Increased glucose reabsorption
16 Noninsulin Agents Available for T2D Class Primary Mechanism of Action Agent(s) Available as -Glucosidase inhibitors Delay carbohydrate absorption from intestine Acarbose Miglitol Precose or generic Glyset Amylin analogue Biguanide Bile acid sequestrant DPP-4 inhibitors Decrease glucagon secretion Slow gastric emptying Increase satiety Decrease HGP Increase glucose uptake in muscle Decrease HGP? Increase incretin levels? Increase glucose-dependent insulin secretion Decrease glucagon secretion Pramlintide Metformin Colesevelam Alogliptin Linagliptin Saxagliptin Sitagliptin Symlin Glucophage or generic WelChol Nesina Tradjenta Onglyza Januvia Dopamine-2 agonist Activates dopaminergic receptors Bromocriptine Cycloset Glinides Increase insulin secretion Nateglinide Repaglinide Starlix or generic Prandin DPP-4, dipeptidyl peptidase; HGP, hepatic glucose production. Garber AJ, et al. Endocr Pract. 2016;22: Inzucchi SE, et al. Diabetes Care. 2015;38: Continued on next slide
17 Noninsulin Agents Available for T2D Class Primary Mechanism of Action Agent(s) Available as GLP-1 receptor agonists Increase glucose-dependent insulin secretion Decrease glucagon secretion Slow gastric emptying Increase satiety Albiglutide Dulaglutide Exenatide Exenatide XR Liraglutide Tanzeum Trulicity Byetta Bydureon Victoza SGLT2 inhibitors Increase urinary excretion of glucose Sulfonylureas Increase insulin secretion Increase glucose uptake in muscle Thiazolidinediones and fat Decrease HGP Canagliflozin Dapagliflozin Empagliflozin Glimepiride Glipizide Glyburide Pioglitazone Rosiglitazone Invokana Farxiga Jardiance Amaryl or generic Glucotrol or generic Dia eta, Glynase, Micronase, or generic Actos Avandia GLP-1, glucagon-like peptide; HGP, hepatic glucose production; SGLT2, sodium glucose cotransporter 2. Garber AJ, et al. Endocr Pract. 2016;22: Inzucchi SE, et al. Diabetes Care. 2015;38: Continued from previous slide
18 Mechanism of Action of Antihyperglycemic Agents Muscle Increase glucose uptake Metformin, TZD Adipose (fat) Increased FFA production TZD Pancreas Decreased insulin secretion from -cells GLP1 RA, DPP4i, SU, GLN The Ominous Octet GLP1 RA, DPP4i Liver Increased endogenous glucose production Metformin, TZD, GLP1 RA, DPP4i Digestive tract Decreased incretin effect GLP1 RA, AGis, Colesevelam Brain Neurotransmitter dysfunction DeFronzo RA. Diabetes. 2009;58: GLP1 RA Bromocriptine Increased glucagon secretion from -cells Pancreas Kidney Increased glucose reabsorption SGLT2i
19 Noninsulin Agents Available for T2D Class Primary Mechanism of Action Agent(s) Available as -Glucosidase inhibitors Delay carbohydrate absorption from intestine Acarbose Miglitol Precose or generic Glyset Amylin analogue Biguanide Bile acid sequestrant DPP-4 inhibitors Decrease glucagon secretion Slow gastric emptying Increase satiety Decrease HGP Increase glucose uptake in muscle Decrease HGP? Increase incretin levels? Increase glucose-dependent insulin secretion Decrease glucagon secretion Pramlintide Metformin Colesevelam Alogliptin Linagliptin Saxagliptin Sitagliptin Symlin Glucophage or generic WelChol Nesina Tradjenta Onglyza Januvia Dopamine-2 agonist Activates dopaminergic receptors Bromocriptine Cycloset Glinides Increase insulin secretion Nateglinide Repaglinide Starlix or generic Prandin DPP-4, dipeptidyl peptidase; HGP, hepatic glucose production. Garber AJ, et al. Endocr Pract. 2016;22: Inzucchi SE, et al. Diabetes Care. 2015;38: Continued on next slide
20 Noninsulin Agents Available for T2D Class Primary Mechanism of Action Agent(s) Available as GLP-1 receptor agonists Increase glucose-dependent insulin secretion Decrease glucagon secretion Slow gastric emptying Increase satiety Albiglutide Dulaglutide Exenatide Exenatide XR Liraglutide Tanzeum Trulicity Byetta Bydureon Victoza SGLT2 inhibitors Increase urinary excretion of glucose Sulfonylureas Increase insulin secretion Increase glucose uptake in muscle Thiazolidinediones and fat Decrease HGP Canagliflozin Dapagliflozin Empagliflozin Glimepiride Glipizide Glyburide Pioglitazone Rosiglitazone Invokana Farxiga Jardiance Amaryl or generic Glucotrol or generic Dia eta, Glynase, Micronase, or generic Actos Avandia GLP-1, glucagon-like peptide; HGP, hepatic glucose production; SGLT2, sodium glucose cotransporter 2. Garber AJ, et al. Endocr Pract. 2016;22: Inzucchi SE, et al. Diabetes Care. 2015;38: Continued from previous slide
21 21 Fixed-Dose Oral Combination Agents for Type 2 Diabetes Class Added Agent Available as DPP4 inhibitor + SGLT-2 inhibitor Linagliptin + empagliflozin Glyxambi Saxagliptin + dapagliflozin Qtern Alogliptin Kazano Metformin + DPP4 inhibitor Linagliptin Jentadueto Sitagliptin Janumet Metformin + glinide Repaglinide Prandimet Metformin + SGLT2 inhibitor Canagliflozin Invokamet Dapagliflozin Xigduo XR Metformin + sulfonylurea Glipizide Metaglip and generic Glyburide Glucovance and generic Metformin + thiazolidinedione Pioglitazone ACTOplus Met Rosiglitazone* Avandamet Thiazolidinedione + DPP4 inhibitor Pioglitazone + alogliptin Oseni Thiazolidinedione + sulfonylurea Pioglitazone Duetact Rosiglitazone Avandaryl
22 Effects of Agents Available for T2D Met GLP1RA SGLT2I DPP4I TZD AGI Coles BCR-QR SU/ Glinide Insulin Pram FPG lowering Mod Mild to mod* Mod Mild Mod Neutral Mild Neutral SU: mod Glinide: mild Mod to marked (basal insulin or premixed) Mild PPG lowering Mild Mod to marked Mild Mod Mild Mod Mild Mild Mod Mod to marked (short/ rapidacting insulin or premixed) Mod to marked AGI = -glucosidase inhibitors; BCR-QR = bromocriptine quick release; Coles = colesevelam; DPP4I = dipeptidyl peptidase 4 inhibitors; FPG = fasting plasma glucose; GLP1RA = glucagon-like peptide 1 receptor agonists; Met = metformin; Mod = moderate; PPG = postprandial glucose; SGLT2I = sodium-glucose cotransporter 2 inhibitors; SU = sulfonylureas; TZD = thiazolidinediones. *Mild: albiglutide and exenatide; moderate: dulaglutide, exenatide extended release, and liraglutide. Handelsman YH, et al. Endocr Pract. 2015;21(suppl 1): Continued on next slide
23 Effects of Agents Available for T2D Met GLP1RA SGLT2I DPP4I TZD AGI Coles BCR-QR SU/ Glinide Insulin Pram NAFLD benefit Mild Mild Neutral Neutral Mod Neutral Neutral Neutral Neutral Neutral Neutral Hypoglycemia Neutral Neutral Neutral Neutral Neutral Neutral Neutral Neutral SU: mod to severe Glinide: mild to mod Mod to severe* Neutral Weight Slight loss Loss Loss Neutral Gain Neutral Neutral Neutral Gain Gain Loss AGI = -glucosidase inhibitors; BCR-QR = bromocriptine quick release; Coles = colesevelam; DPP4I = dipeptidyl peptidase 4 inhibitors; GLP1RA = glucagon-like peptide 1 receptor agonists; Met = metformin; Mod = moderate; NAFLD, nonalcoholic fatty liver disease; SGLT2I = sodium-glucose cotransporter 2 inhibitors; SU = sulfonylureas; TZD = thiazolidinediones. *Especially with short/ rapid-acting or premixed. Handelsman YH, et al. Endocr Pract. 2015;21(suppl 1): Continued from previous slide
24 Effects of Agents Available for T2D Met GLP1RA SGLT2I DPP4I TZD AGI Coles BCR-QR SU/ Glinide Insulin Pram Renal impairment/ GU Contraindicated egfr <30 Caution if Exenatide contraindicated CrCl <30 mg/ml GU infection risk Dose adjustment (except linagliptin) May worsen fluid retention Neutral Neutral Neutral Increased hypoglycemia risk Increased risks of hypoglycemia and fluid retention Neutral GI adverse effects Mod Mod* Neutral Neutral* Neutral Mod Mild Mod Neutral Neutral Mod CHF Neutral Neutral Neutral Neutral Mod Neutral Neutral Neutral Neutral Neutral Neutral CVD Possible benefit Neutral Neutral Neutral Neutral Neutral Neutral Safe? Neutral Neutral Bone Neutral Neutral Bone loss Neutral Mod bone loss Neutral Neutral Neutral Neutral Neutral Neutral AGI = -glucosidase inhibitors; BCR-QR = bromocriptine quick release; Coles = colesevelam; CHF = congestive heart failure; CVD = cardiovascular disease; DPP4I = dipeptidyl peptidase 4 inhibitors; GI = gastrointestinal; GLP1RA = glucagon-like peptide 1 receptor agonists; GU = genitourinary; Met = metformin; Mod = moderate; SGLT2I = sodium-glucose cotransporter 2 inhibitors; SU = sulfonylureas; TZD = thiazolidinediones. *Caution in labeling about pancreatitis. DKA Risk Caution: possibly increased CHF hospitalization risk seen in CV safety trial. Handelsman YH, et al. Endocr Pract. 2015;21(suppl 1): Continued from previous slide
25 Invokana (canagliflozin) Jardiance (empagliflozin) Farxiga (dapagliflozin)
26
27 Metformin: Updated FDA guidelines Prior recommendations for metformin: Hold if creatinine above 1.5 in men, 1.4 in women or abnormal creatinine clearance and hold for 48h after IV contrast. New guidelines from April 2016 use egfr If egfr is < 30, drug is contraindicated. For egfr weigh risks and benefits of continuing, consider cutting the dose in 1/2, and do not START metformin in this range. For 45-60, safe to use Discontinue metformin at the time of or before an iodinated contrast imaging procedure in patients with an egfr between 30 and 60 ml/minute/1.73 m 2 ; in patients with a history of liver disease, alcoholism, or heart failure; or in patients who will be administered intraarterial iodinated contrast. Re-evaluate egfr 48 hours after the imaging procedure; restart metformin if renal function is stable. If egfr is 60 or higher (and not intra-arterial contrast), no need to discontinue. 27
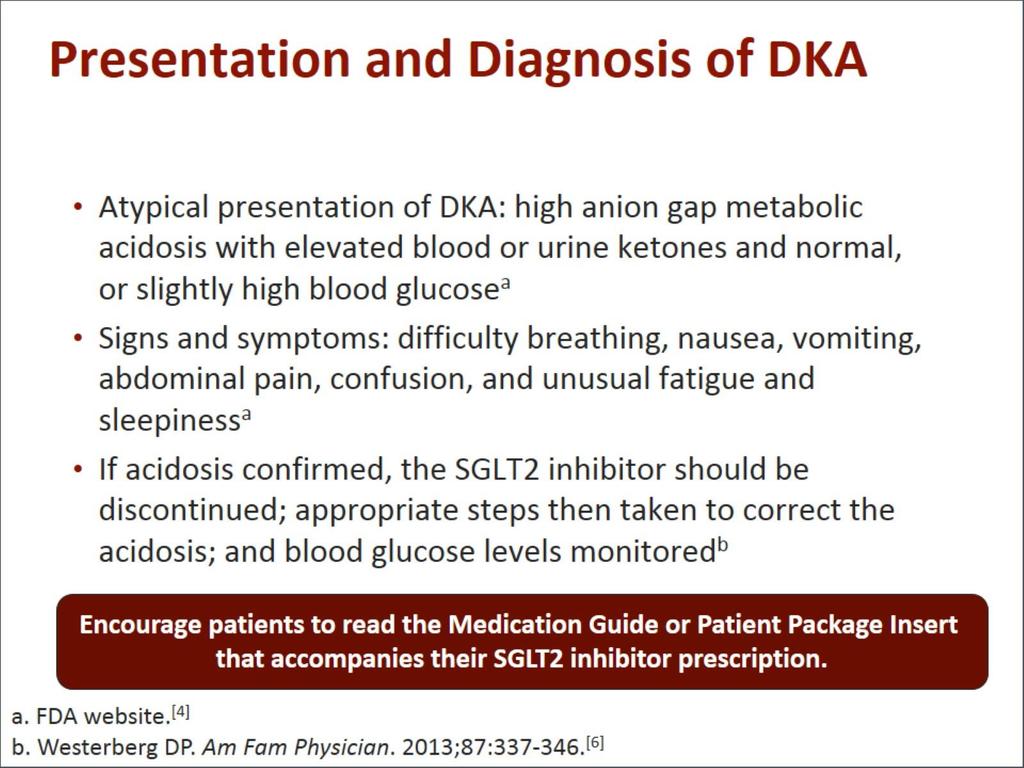
28 Noninsulin Therapies in the Hospital Time-action profiles of oral agents can result in delayed achievement of target glucose ranges in hospitalized patients Sulfonylureas are a major cause of prolonged hypoglycemia Metformin is contraindicated in patients with decreased renal function, use of iodinated contrast dye (sometimes), and any state associated with poor tissue perfusion (CHF, sepsis) Thiazolidinediones are associated with edema and CHF α-glucosidase inhibitors are weak glucose-lowering agents Pramlintide and GLP-1 receptor agonists can cause nausea and exert a greater effect on postprandial glucose SGLT2 inhibitors may cause atypical DKA in setting of stress DPP4 inhibitors may provide safe and effective blood glucose control when used alone or in combination with basal insulin (caution with aloglipitin and saxagliptin re: CHF risk) 28 Insulin therapy is the preferred approach
29 Glycemic Management Strategies in Noncritically Ill Patients Insulin therapy preferred regardless of type of diabetes Discontinue noninsulin agents at hospital admission of most patients with type 2 diabetes with acute illness Use scheduled SC insulin with basal, nutritional, and correction components Modify insulin dose in patients treated with insulin before admission to reduce risk for hypoglycemia and hyperglycemia Avoid prolonged therapy with sliding scale insulin alone Consider resumption of noninsulin medications 1-2 days prior to discharge. Umpierrez GE, et al. J Clin Endocrinol Metab. 2012;97:
 Long (detemir) 0 2 4 6 8 10 12 14 16 18 20 22 24 Hours Adapted 30 from Hirsch I. N Engl J Med.")
30 Pharmacokinetics of Insulin Products Rapid (lispro, aspart, glulisine) Insulin Level Short (regular) Intermediate (NPH) Long (glargine) Long (detemir) Hours Adapted 30 from Hirsch I. N Engl J Med. 2005;352:
31 Subcutaneous Insulin Options Basal insulin Nutritional (prandial) insulin Correction insulin Controls blood glucose in the fasting state Detemir (Levemir), glargine (Lantus), NPH Blunts the rise in blood glucose following nutritional intake (meals, IV dextrose, enteral/parenteral nutrition) Rapid-acting: aspart (NovoLog), glulisine (Apidra), lispro (Humalog) Short-acting: regular (Humulin, Novolin) Corrects hyperglycemia due to mismatch of nutritional intake and/or illness-related factors and scheduled insulin administration 31
32 AL. 65 yo man admitted with possible recurrent stroke. New onset DM with admission glucose 682. A1c > 14. Per ADA and AACE guidelines, for new type 2 diabetic with A1c 10 or higher, insulin is preferred starting medication Either basal bolus regimen or basal plus GLP1 agonist* *remember GLP1 agonist not recommended for use in hospital due to nausea and slowed gastric empyting 32

33 AL. 65 yo man admitted with possible recurrent stroke. New onset DM with admission glucose 682. A1c > 14. Patient initially started on glipizide 10mg bid and correctional insulin. Blood sugars on 2 nd hospital day: 33

34 AL. 65 yo man admitted with possible recurrent stroke. New onset DM with admission glucose 682. A1c > 14. On evening of hospital day 2, sitagliptin (Januvia) added 34
35 AL. 65 yo man admitted with possible recurrent stroke. New onset DM with admission glucose 682. A1c > 14. On hospital day 3, metformin added and Januvia increased to 50mg bid, and bedtime basal insulin added 35
36 AL. 65 yo man admitted with possible recurrent stroke. New onset DM with admission glucose 682. A1c > 14. Basal/bolus and correction insulin A better solution! 36
37 AL. 65 yo man admitted with possible recurrent stroke. New onset DM with admission glucose 682. A1c > 14. Basal/bolus and correction insulin, a better solution! BUT how do we decide on the dose? 37
38 Initiating Insulin Therapy in the Hospital Total Daily Dose Choose an appropriate total units/kg/day estimation after reviewing the patient's factors below. 0.3 units/kg/day - malnourished, no history of DM, cognitive impairment, elderly, renal or liver disease, pancreatectomy. 0.4 units/kg/day - lean (BMI = ) Type 2 DM, steroid-induced hyperglycemia (without underlying DM), or Type 1 DM. 0.5 units/kg/day - overweight (BMI 25-30) type 2 DM. 0.6 units/kg/day - obese (BMI greater than 30) Type 2 DM or Type 2 DM receiving steroids. 38
39 AL. 65 yo man admitted with possible recurrent stroke. New onset DM with admission glucose 682. A1c > 14. Weight 90 kg Not on steroids egfr 68 Normal liver function 39

 0.")

40 Initiating Insulin Therapy in the Hospital Patient AL Obtain patient weight in kg: 90kg Calculate total daily dose (TDD) 0.5 units per kg/day 45 units/day 40% of total to be given as basal insulin: 18 units of Lantus once daily 40
41 Initiating Insulin Therapy in the Hospital Patient AL TDD 45 units, 40% basal 60% to be given as nutritional insulin = 27 units 27/3 = 9 units per meal Use medium dose correction insulin based on total daily dose of units daily Adjust according to results of bedside glucose monitoring Adjust dose for NPO status or changes in clinical status 41

42 AL. 65 yo man admitted with possible recurrent stroke. New onset DM with admission glucose 682. A1c > 14. Patient discharged on hospital day 4, on basal bolus insulin Discharge regimen: Lantus, premeal insulin with correction 42

43 AL. 65 yo man admitted with possible recurrent stroke. New onset DM with admission glucose 682. A1c > 14. Patient discharged on hospital day 4 Discharge regimen: Lantus, premeal correction, BID glipizide, metformin, and Januvia 43
44 Patients Newly Diagnosed With Diabetes During Hospitalization Develop a diabetes education plan prior to hospital discharge that addresses the following: Understanding of the diagnosis of diabetes SMBG and explanation of home blood glucose goals Definition, recognition, treatment, and prevention of hyperglycemia and hypoglycemia Identification of healthcare provider who will provide diabetes care after discharge Information on consistent eating patterns When and how to take medication, including proper disposal of needles and syringes Sick-day management *Susan Zontine, NP to review diabetes survival skills during the next talk! ADA. Diabetes Care. 2013;36(suppl 1):S11-S66. Handelsman 44 Y, et al. Endocr Pract. 2011;17(suppl 2):1-53.
45 AL 65 yo man admitted with possible recurrent stroke. New onset DM with admission glucose 682. A1c > 14. Discharge Planning What medications should he go home on? If regimen includes insulin, who will give it? Can he afford the medication regimen prescribed? Has he and/or family members been taught Diabetes survival skills? Who will follow him post-discharge to adjust the regimen? 45
46 AL 65 yo man admitted with possible recurrent stroke. New onset DM with admission glucose 682. A1c > 14. Discharge Planning Can he afford his medication? How do you find out? Case managers and pharmacists can be helpful resources. At WMC, contact the Valley Pharmacy Discharge Program, At WMH, contact Kari Gordon, Clinical Pharmacist , Kris Jett, Nurse Case Manager or Tara Reber, Social Worker At other facilities, contact the Nurse Case Manager or Clinical Pharmacist. 46
47 Stretch Break! 47
48 Diabetes and the Bedside Nurse Every day dilemmas 48
49 Case Study RG 61 yo man POD 3 from CABG on basal Lantus, nutritional Novolog and correction Novolog. Complains of feeling shaky and sweaty at 11:00 AM. What should you do? 49
50 Case Study RG 61 yo man POD 3 from CABG on basal/bolus, shaky and sweaty at 11:00 AM. What should you do? Give him a large glass of juice Feed him lunch Call rapid response team Hold his lunchtime insulin All of the above 50
51 Case Study RG 61 yo man POD 3 from CABG on basal/bolus, shaky and sweaty at 11:00 AM. What should you do? Check POCT Glucose! 51
52 Case Study RG 61 yo man POD 3 from CABG on basal/bolus, shaky and sweaty with POCT glucose 62 at 11:00 AM. What should you do? Give him a large glass of juice Feed him lunch Call rapid response team Hold his lunch time insulin All of the above 52

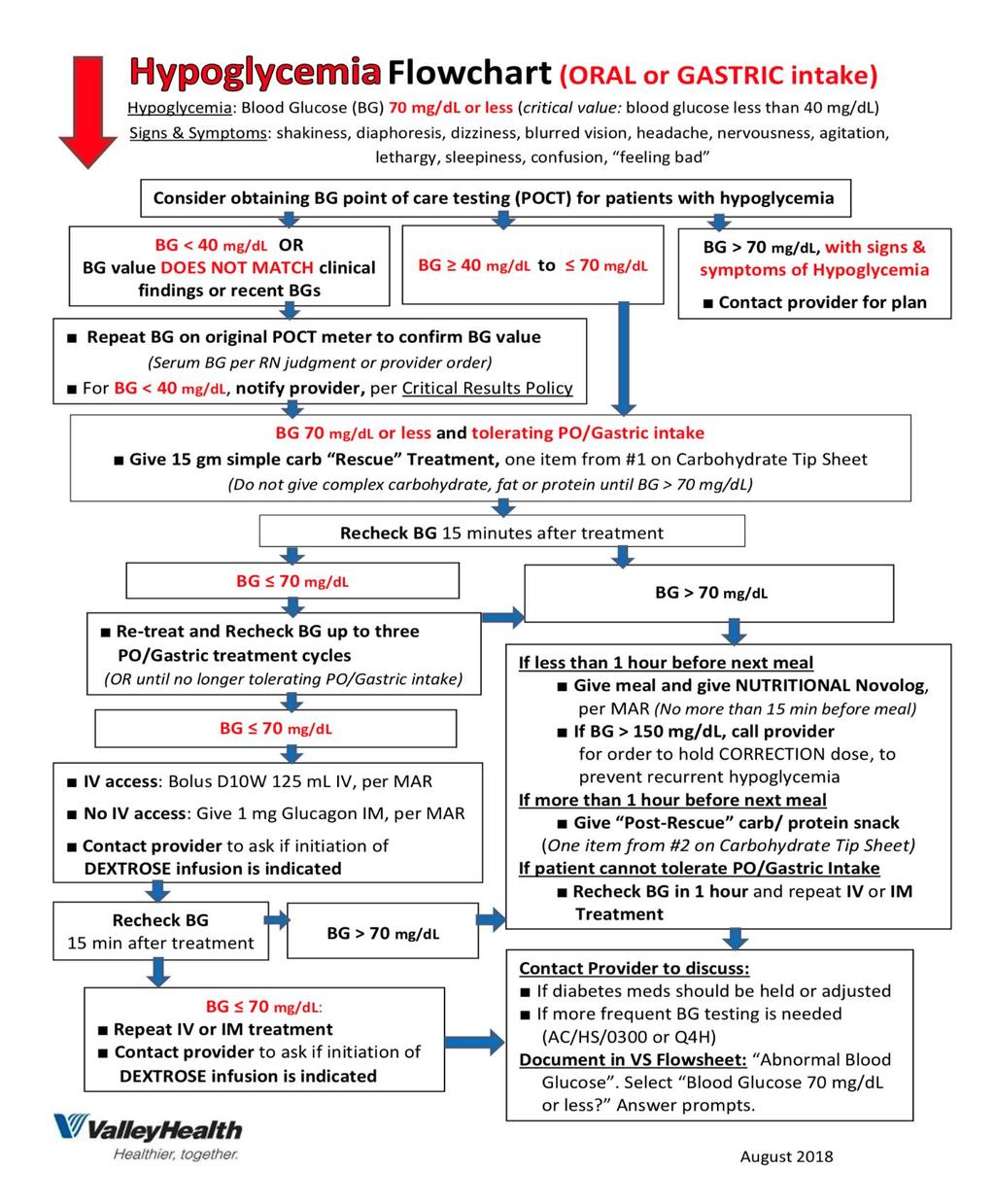
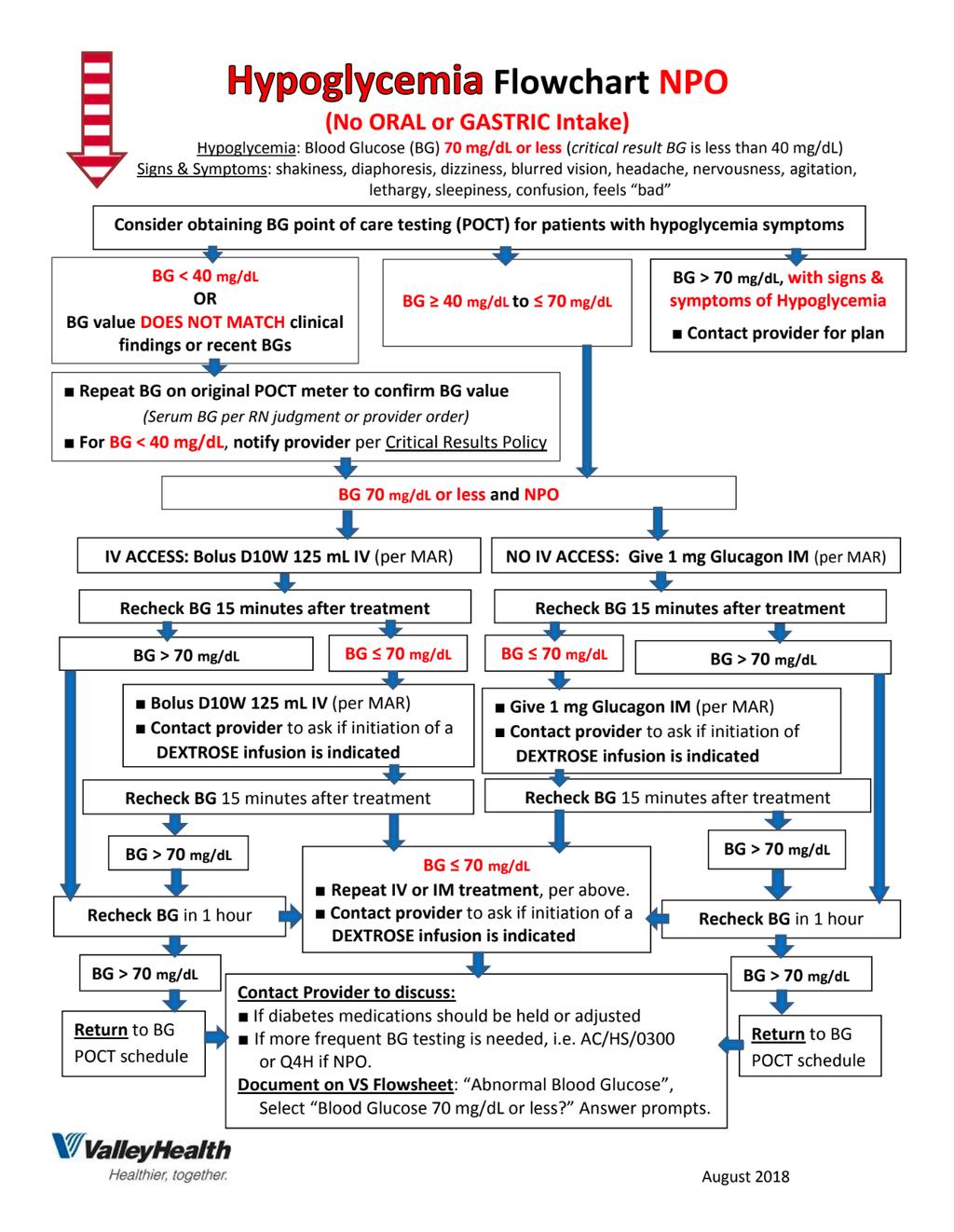
53 The Rule Give 15 grams of fastacting carbohydrate and wait 15 minutes Recheck blood glucose and then give another 15 grams of fast-acting carbohydrate, if necessary 53
54 54
55 55
56 Strategies for Reducing Risk for Hypoglycemia in Noncritical Care Settings Avoidance of sliding-scale insulin alone Use caution in prescribing oral antihyperglycemic agents Modify outpatient insulin doses in patients treated with insulin prior to admission Braithwaite SS, et al. Endocr Pract. 2004;10(suppl 2):
57 Case Study RG 61 yo man POD 3 from CABG on basal Lantus, nutritional Novolog and correction Novolog. Presupper blood sugar is 336. On further questioning, patient reports that family brought him a small sub from Subway for mid afternoon snack. What should you do? 57
58 Case Study RG 61 yo man POD 3 from CABG on basal/bolus, 336 before supper after Subway snack. What should you do? Give him correction dose of insulin Give him meal insulin Call rapid response team Cancel his dinner meal Forbid family from bringing him anything else to eat All of the above 58
59 59
60 Case Study RG 61 yo man POD 3 from CABG on basal/bolus, 336 before supper after Subway snack. Patient indicates he is still hungry and planning to eat his dinner, so you should: Give correction insulin only Give correction and nutritional insulin Give nutritional insulin only Encourage him to drink extra fluids and give correction and nutritional insulin 60
61 Case Study RG 61 yo man POD 4 from CABG on basal Lantus, nutritional Novolog and correction Novolog. The next morning, you are on the way to give him his prebreakfast insulin when your other patient next door has acute respiratory distress requiring RRT. 90 minutes later you are finally able to give RG his breakfast insulin, but he finished eating his breakfast 85 minutes ago. CNA has just rechecked blood sugar and it is 227. What should you do? 61
62 Case Study RG 61 yo man POD 4 from CABG on basal/bolus, h after breakfast. What should you do? Give him correction dose of insulin only Give him meal insulin only Give him both meal and correction dose of insulin Give him no insulin at all, it s too late now. Call the provider for further orders. All of the above 62
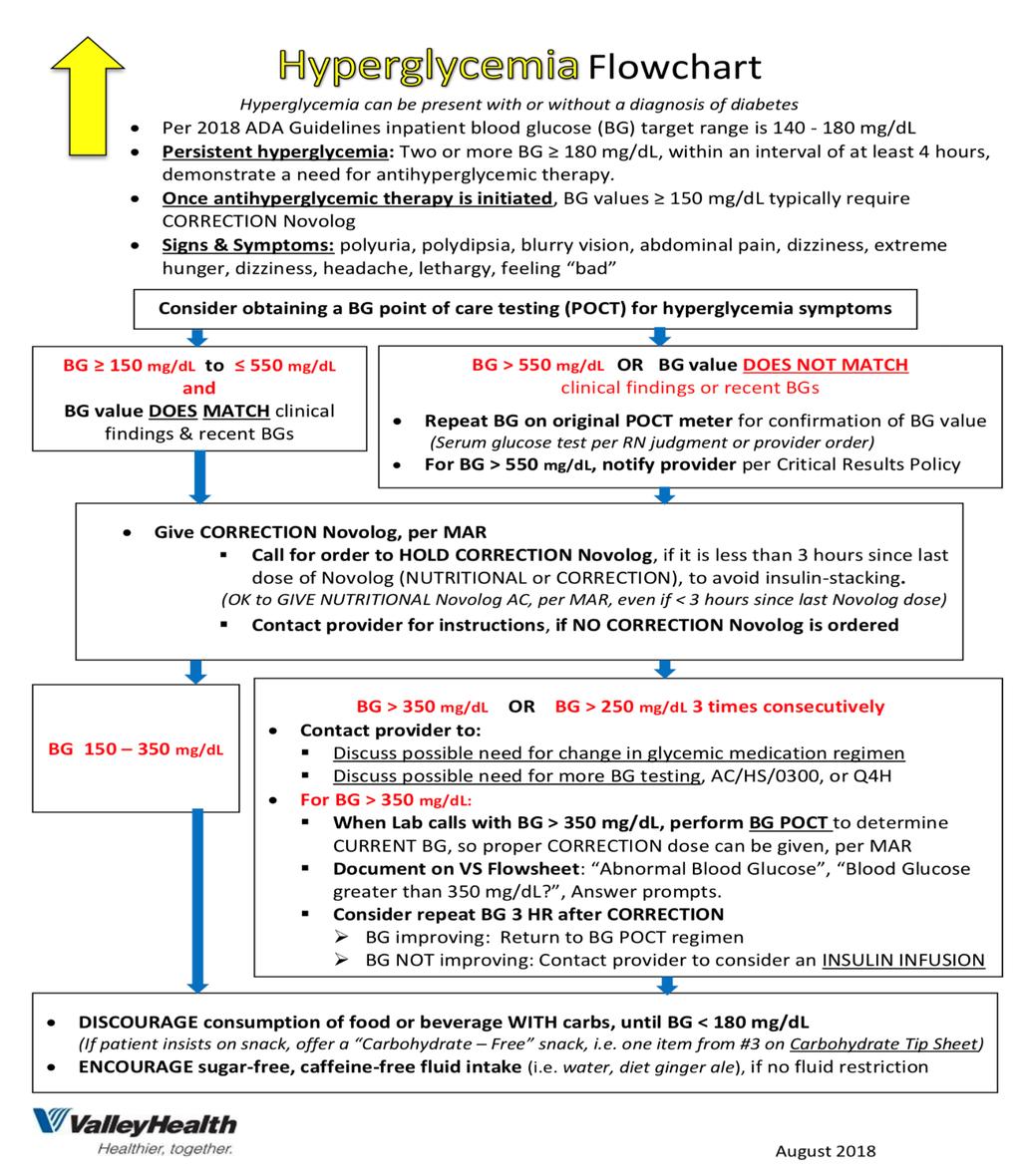
63 Case Study RG From new hyperglycemia policy, Recommendations for safe administration of NUTRITIONAL and CORRECTION Novolog If greater than 60 minutes after meal, and AC scheduled NUTRITIONAL and CORRECTION Novolog were not given, 1. Perform a blood glucose POCT and administer the AC CORRECTION Novolog, per MAR. 2. DO NOT give scheduled NUTRITIONAL Novolog. Contact provider for an order to HOLD the scheduled NUTRITIONAL Novolog. 63
64 Case Study RG 61 yo man POD 5 from CABG on basal Lantus, nutritional Novolog and correction Novolog. He is now ready for discharge, 5 days after CABG. What regimen should he be discharged on? 64
65 Case Study RG 61 yo man POD 5 from CABG on basal/bolus, ready for discharge. What regimen should he go home on? The basal bolus insulin regimen he is currently getting The insulin regimen he was on before admission but not the other diabetic medications The insulin and other diabetic medications he was on before admission All of the above Whatever the provider orders It depends 65
66 Discharging Patients With Previously Diagnosed Diabetes Resume preadmission diabetes regimen at time of discharge for patients with acceptable preadmission glycemic control, no contraindication to prior therapy, and no significant health changes during hospitalization. When possible, resume this 24h prior to discharge to verify well tolerated. Umpierrez GE, et al. J Clin Endocrinol Metab. 2012;97:
67 Discharging Patients With Previously Diagnosed Diabetes Modify preadmission therapy for Patients found to have been in poor control prior to admission Patients who have had significant change in weight, oral intake or other factors that may affect glycemic control. Patients for whom preadmission medication(s) is now contra-indicated based on change in health status. Umpierrez GE, et al. J Clin Endocrinol Metab. 2012;97:
68 Discharging Patients With Previously Diagnosed Diabetes Provide patient and family members/caregivers with written and oral instructions regarding glycemic management regimen at time of hospital discharge Umpierrez GE, et al. J Clin Endocrinol Metab. 2012;97:
69 Ensuring Good Glycemic Control in Patients Being Discharged Ensure patient has survival skills ie, diabetes self-management education (DSME) Use of personal glucose monitor Rudiments of meal plan (effect of CHO) Medications How and when to administer Side effects Symptoms and treatment of hypo- and hyperglycemia When and whom to contact with problems Be sure patient has a name and phone number Additional education/resources 69
70 Connecting Inpatient Care to Outpatient Support: Circle of Care Appropriate inpatient/outpatient referrals and consultations Intake and identification Discharge summary and documentation of met needs Multidisciplinary involvement and coordination is required Admission database Focused bedside teaching/interventions Multidisciplinary team referrals Focused clinical assessment Pollom RK, Pollom RD. Crit Care Nurse Q. 2004;27:
71 Diabetes Update 2018: Challenging Transitions To effectively manage diabetes and nutrition in the hospital setting, a multidisciplinary team approach is key Collaboration among physicians, nurses, CNAs, pharmacists, laboratory staff, social workers, and dietary staff can optimize patient care and support favorable metabolic control and successful transitions in care 71
72 Diabetes Update 2018: Challenging Transitions Summary Reviewed appropriate management of abnormal blood sugars in hospital setting Reviewed impact of transitions in care on glycemic control Overview of upcoming hypoglycemia and hyperglycemia policies which will provide guidance 72
73 Diabetes Update 2018: Challenging Transitions Questions? 73
Diabetes Update 2018: Challenging Transitions. Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System
 Diabetes Update 2018: Challenging Transitions Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System 1 Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley
Diabetes Update 2018: Challenging Transitions Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System 1 Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley
Objectives. How Medicine Works to Control Blood Sugar Levels. What Happens When We Eat? What is diabetes? High Blood Glucose (Hyperglycemia)
") How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
RPCC Pharmacy Forum. The Type 2 Diabetes Issue. Type 2 Diabetes: The Basics
 Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
1/15/2018. Disclosures. Current Diabetes Medications. Objectives NON-INSULIN AGENTS. Diabetes Med Classes. Mealtime
 Disclosures Current Diabetes Medications None Claire Baker, M.D. Diabetes & Endocrine Associates January 24, 2018 Objectives Identify categories of diabetes medications Understand the pharmacology of diabetes
Disclosures Current Diabetes Medications None Claire Baker, M.D. Diabetes & Endocrine Associates January 24, 2018 Objectives Identify categories of diabetes medications Understand the pharmacology of diabetes
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
DIABETES. overview of pharmacologic agents used in the management of. Overview 4/3/2014 OBJECTIVES. Injectable Agents
 overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Diabetes Medications: Oral Anti-Hyperglycemic Medications
 Diabetes Medications: Oral Anti-Hyperglycemic Medications Medication Types 1. Biguanides 2. Sulfonylureas 3. Thiazolidinediones (TZDs) 4. Alpha-Glucosidase Inhibitors 5. D-Phenylalanine Meglitinides 6.
Diabetes Medications: Oral Anti-Hyperglycemic Medications Medication Types 1. Biguanides 2. Sulfonylureas 3. Thiazolidinediones (TZDs) 4. Alpha-Glucosidase Inhibitors 5. D-Phenylalanine Meglitinides 6.
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018
 Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Diabetes Treatment Guidelines
 Diabetes Treatment Guidelines For more comprehensive information about current approaches to the diagnosis and treatment of diabetes, visit the American Diabetes Association Standards of Medical Care 2018
Diabetes Treatment Guidelines For more comprehensive information about current approaches to the diagnosis and treatment of diabetes, visit the American Diabetes Association Standards of Medical Care 2018
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Glycemic Management of Type 2 Diabetes. Gail Nunlee-Bland, M.D. Professor Medicine & Pediatrics Director, Diabetes Treatment Center Howard University
 Glycemic Management of Type 2 Diabetes Gail Nunlee-Bland, M.D. Professor Medicine & Pediatrics Director, Diabetes Treatment Center Howard University 1 None Disclosures Learning Objectives Understand the
Glycemic Management of Type 2 Diabetes Gail Nunlee-Bland, M.D. Professor Medicine & Pediatrics Director, Diabetes Treatment Center Howard University 1 None Disclosures Learning Objectives Understand the
Oral Medication for the Management of Diabetes Mechanism of. Duration of Daily Dosing Action
 Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
Non-Insulin Diabetes Medications Summary
 Non-Insulin Diabetes Medications Summary Medications marked with an asterisk (*) can cause hypoglycemia INSULIN SECRETAGOGUES Sulfonylureas* GLYBURIDE* (Diabeta) (Micronase) production. Side effects: Potential
Non-Insulin Diabetes Medications Summary Medications marked with an asterisk (*) can cause hypoglycemia INSULIN SECRETAGOGUES Sulfonylureas* GLYBURIDE* (Diabeta) (Micronase) production. Side effects: Potential
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Clinical Cases in Diabetes Management. Joseph Cook D.O.
 Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
Pharmacology. Kacy Aderhold, MSN, APRN-CNS, CMSRN
 Pharmacology Kacy Aderhold, MSN, APRN-CNS, CMSRN Biguanides Decreases hepatic glucose production and improves insulin sensitivity (increases number of insulin receptors) Common Adverse Reaction: diarrhea
Pharmacology Kacy Aderhold, MSN, APRN-CNS, CMSRN Biguanides Decreases hepatic glucose production and improves insulin sensitivity (increases number of insulin receptors) Common Adverse Reaction: diarrhea
4/9/2018 HOW TO REGULATE DIABETES MEDICATIONS. By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE. Diagnosis
 HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD. Disclosures. Objectives 9/1/2015
 Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Disclosures. Objectives 11/2/2015. Type 2 Diabetes Mellitus: Medication Update. Diabetes Recommendations. Main Pathophysiological Defects in T2DM
 Type 2 Diabetes Mellitus: Medication Update Which One Should the NP Use? Iowa Nurse Practitioner Society Dr. Dixie Harms, DNP, ARNP, FNP-C, BC-ADM, FAANP November 2015 Disclosures Speaker s Bureau Novo
Type 2 Diabetes Mellitus: Medication Update Which One Should the NP Use? Iowa Nurse Practitioner Society Dr. Dixie Harms, DNP, ARNP, FNP-C, BC-ADM, FAANP November 2015 Disclosures Speaker s Bureau Novo
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA 2012 Virginia Mason Medical
 Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Diabetes Update 10/12/2017. Section #1 OBJECTIVE. Lab features to consider:
 Section #1 OBJECTIVE Diabetes Update Fall 2017 Lyle Myers BE ABLE TO DIFFERENTIATE TYPE 1 FROM TYPE 2 DIABETES Clinical features: - age at onset - body weight/bmi - family history - treatment history -
Section #1 OBJECTIVE Diabetes Update Fall 2017 Lyle Myers BE ABLE TO DIFFERENTIATE TYPE 1 FROM TYPE 2 DIABETES Clinical features: - age at onset - body weight/bmi - family history - treatment history -
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions. Insulins. Rapid Short Intermediate Long Mix
 Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
Clinical Pharmacotherapeutic Applications of the American Diabetes Association Standards of Care 2018
 Clinical Pharmacotherapeutic Applications of the American Diabetes Association Standards of Care 2018 RACHEL NAIDA, PHARMD, CDE CLINICAL ASSOCIATE PROFESSOR UNIVERSITY OF NEW ENGLAND COLLEGE OF PHARMACY
Clinical Pharmacotherapeutic Applications of the American Diabetes Association Standards of Care 2018 RACHEL NAIDA, PHARMD, CDE CLINICAL ASSOCIATE PROFESSOR UNIVERSITY OF NEW ENGLAND COLLEGE OF PHARMACY
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Update on Diabetic Medications UMA SUNDARAM, M.D. DIABETES & ENDOCRINE ASSOCIATES APRIL 07, 2018
 Update on Diabetic Medications UMA SUNDARAM, M.D. DIABETES & ENDOCRINE ASSOCIATES APRIL 07, 2018 Disclosure NONE Objectives To identify different categories of diabetes medications Understand the pharmacology
Update on Diabetic Medications UMA SUNDARAM, M.D. DIABETES & ENDOCRINE ASSOCIATES APRIL 07, 2018 Disclosure NONE Objectives To identify different categories of diabetes medications Understand the pharmacology
DIABETES (1 of 5) Generic. Generic $0 $5 $5-10 $0 $0 $0. Generic $0 $5 $5-10. Generic. Generic $0 $5 $5-10 $0 $0 $0. Generic $0 $5 $5-10 $0 $0 $0
 Generic. Generic $0 $5 $5-10 $0 $0 $0. Generic $0 $5 $5-10. Generic. Generic $0 $5 $5-10 $0 $0 $0. Generic $0 $5 $5-10 $0 $0 $0") Metformin DIABETES (1 of 5) Glucophage Glucophage XR ER $7 (500mg) $7 (500mg) $5 $5 500mg, 750mg only 500mg, 750mg only Sulfonylurea/Combinations Amaryl Glucotrol glimepiride glipizide $5 $5 Glucotrol
Metformin DIABETES (1 of 5) Glucophage Glucophage XR ER $7 (500mg) $7 (500mg) $5 $5 500mg, 750mg only 500mg, 750mg only Sulfonylurea/Combinations Amaryl Glucotrol glimepiride glipizide $5 $5 Glucotrol
Physician Drug Reference Chart for Diabetes Antidiabetic Medications
 Drug Class Compound Brand Name Mechanism of Action Advantages Disadvantages Alpha-glucosidase inhibitors Medium Cost by Bayer Healthcare, Pfizer, Takeda Research Acarbose Miglitol Voglibose Precose Glyset
Drug Class Compound Brand Name Mechanism of Action Advantages Disadvantages Alpha-glucosidase inhibitors Medium Cost by Bayer Healthcare, Pfizer, Takeda Research Acarbose Miglitol Voglibose Precose Glyset
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Learning Objectives. Impact of Diabetes II UPDATES IN TYPE 2 DIABETES. David Doriguzzi, PA-C
 UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
FARXIGA (dapagliflozin) Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)
 Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)") Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
2018 Diabetes Summit Managing Diabetes: An Art and a Science
 2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
Diabetes Management: A diagnostic perspective
 Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Advanced Practice Education Associates. Endocrine
 Advanced Practice Education Associates Endocrine Overview Diabetes Thyroid Disease 162 Copyright 2016 Advanced Practice Education Associates DIABETES MELLITUS What is the BMI cut point for screening adults
Advanced Practice Education Associates Endocrine Overview Diabetes Thyroid Disease 162 Copyright 2016 Advanced Practice Education Associates DIABETES MELLITUS What is the BMI cut point for screening adults
Improving Patient Outcomes with Individualized Therapy in the Management of Type 2 Diabetes
 Improving Patient Outcomes with Individualized Therapy in the Management of Type 2 Diabetes Timothy S. Reid, M.D. Mercy Diabetes Center Janesville, WI Duality Statement Dr. Reid is a Speaker and Consultant
Improving Patient Outcomes with Individualized Therapy in the Management of Type 2 Diabetes Timothy S. Reid, M.D. Mercy Diabetes Center Janesville, WI Duality Statement Dr. Reid is a Speaker and Consultant
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Oral and Injectable Medication Options for Diabetes Treatment
 Oral and Injectable Medication Options for Diabetes Treatment Presented by: Dr. Daphne E. Smith, Pharm.D., CDE Clinical Assistant Professor/Clinical Pharmacist-University of Illinois at Chicago College
Oral and Injectable Medication Options for Diabetes Treatment Presented by: Dr. Daphne E. Smith, Pharm.D., CDE Clinical Assistant Professor/Clinical Pharmacist-University of Illinois at Chicago College
New Therapies for Diabetes
 Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
I. General Considerations
 1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Managing Complex Diabetes Cases: Medication Update. Celia Levesque MSN, RN, CNS-BC, CDE, BC-ADM
 Managing Complex Diabetes Cases: Medication Update Celia Levesque MSN, RN, CNS-BC, CDE, BC-ADM clevesqu@mdanderson.org Objectives Describe how each diabetes medication class is used to treat diabetes Differentiate
Managing Complex Diabetes Cases: Medication Update Celia Levesque MSN, RN, CNS-BC, CDE, BC-ADM clevesqu@mdanderson.org Objectives Describe how each diabetes medication class is used to treat diabetes Differentiate
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Very Practical Tips for Managing Type 2 Diabetes
 Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
DIABETES. Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes. November 2013
 DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
Drug Class Review Newer Diabetes Medications and Combinations
 Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Diabetes 2016: Strategies for achieving optimal diabetes control
 PHASE Safety Net Community Benefit Diabetes 2016: Strategies for achieving optimal diabetes control Presented by: Lisa Gilliam, MD, PhD Clinical Leader Diabetes Program Kaiser Permanente Northern California
PHASE Safety Net Community Benefit Diabetes 2016: Strategies for achieving optimal diabetes control Presented by: Lisa Gilliam, MD, PhD Clinical Leader Diabetes Program Kaiser Permanente Northern California
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Clinical Practice Guidelines
 Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
第十五章. Diabetes Mellitus
 Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Jeopardy: Update on Diabetes Pharmacotherapy
 Jeopardy: Update on Diabetes Pharmacotherapy Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Objectives Describe the mechanism of action
Jeopardy: Update on Diabetes Pharmacotherapy Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Objectives Describe the mechanism of action
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Collaborative Practice Agreement
 Collaborative Practice Agreement [community pharmacy name] [address] [phone number] [physician practice] [address] [phone number] Effective: [date] Expiration: [date] 1 Table of Contents 1.0 Introduction...4
Collaborative Practice Agreement [community pharmacy name] [address] [phone number] [physician practice] [address] [phone number] Effective: [date] Expiration: [date] 1 Table of Contents 1.0 Introduction...4
STEP THERAPY CRITERIA
 CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
The Community Pharmacist s Role in Diabetes Treatment
 CONTINUING EDUCATION The Community Pharmacist s Role in Diabetes Treatment By Kimberly Ference, PharmD U pon completion of this activity, the pharmacist should be able to achieve these directives: 1. Describe
CONTINUING EDUCATION The Community Pharmacist s Role in Diabetes Treatment By Kimberly Ference, PharmD U pon completion of this activity, the pharmacist should be able to achieve these directives: 1. Describe
Objectives. Why is Glucose Control Important? 11/2/2016. Jeopardy: Update on Diabetes Pharmacotherapy
 Jeopardy: Update on Diabetes Pharmacotherapy Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University Chicago College of Pharmacy Objectives Describe the mechanism of action
Jeopardy: Update on Diabetes Pharmacotherapy Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University Chicago College of Pharmacy Objectives Describe the mechanism of action
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Inpatient Management of Diabetes Mellitus. Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy
 Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
ORAL AGENTS OLD & NEW FOR THE MANAGEMENT OF T2DM
 ORAL AGENTS OLD & NEW FOR THE MANAGEMENT OF T2DM ECHO-Diabetes July 21, 2016 VERONICA BRADY, PHD, FNP-BC, BC-ADM, CDE OBJECTIVES Overview of Diabetes Oral hypoglycemic agents Define various classes of
ORAL AGENTS OLD & NEW FOR THE MANAGEMENT OF T2DM ECHO-Diabetes July 21, 2016 VERONICA BRADY, PHD, FNP-BC, BC-ADM, CDE OBJECTIVES Overview of Diabetes Oral hypoglycemic agents Define various classes of
How to Fight Diabetes and Win. Diabetes. Medications
 How to Fight Diabetes and Win Diabetes Medications MEDICATIONS FOR DIABETES According to the American Diabetes Association, 85% of adults diagnosed with diabetes take insulin and/or oral medication to
How to Fight Diabetes and Win Diabetes Medications MEDICATIONS FOR DIABETES According to the American Diabetes Association, 85% of adults diagnosed with diabetes take insulin and/or oral medication to
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Jeffery Davies, DO, MPH, FACOEP ACOEP Chicago, IL October Your DM patient is ready for discharge, now what?
 Jeffery Davies, DO, MPH, FACOEP ACOEP Chicago, IL October 2018 Your DM patient is ready for discharge, now what? Financial Disclosures None Objectives 1. Understand follow up patterns/capability of patients
Jeffery Davies, DO, MPH, FACOEP ACOEP Chicago, IL October 2018 Your DM patient is ready for discharge, now what? Financial Disclosures None Objectives 1. Understand follow up patterns/capability of patients
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Type. Diabetes Drugs. A Review
 Type Diabetes is a common diagnosis for home care patients. Diabetes drugs are now available that target the multiple defects of metabolism that characterize Type 2 diabetes. Understanding the wide variety
Type Diabetes is a common diagnosis for home care patients. Diabetes drugs are now available that target the multiple defects of metabolism that characterize Type 2 diabetes. Understanding the wide variety
The Diabetes Guidelines Trek: The Next Generation. Inpatient Diabetes Guidelines. Learning Objectives. Current Inpatient Guidelines
 The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
Pharmacologic Agents for Treatment of Type 2 Diabetes
 Pharmacologic Agents for Treatment of Type 2 Diabetes SCAN Drugs Medication Biguanides 1 1 er uncoated tabs 500 mg & 750 mg Sulfonylureas 1 1 500 850 mg QD - TID 500 2000 mg glimepiride 1 1 1 8 mg glipizide
Pharmacologic Agents for Treatment of Type 2 Diabetes SCAN Drugs Medication Biguanides 1 1 er uncoated tabs 500 mg & 750 mg Sulfonylureas 1 1 500 850 mg QD - TID 500 2000 mg glimepiride 1 1 1 8 mg glipizide
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
continuing education for pharmacists
 continuing education for pharmacists 2016 AACE/ACE Guidelines on Type 2 Diabetes Management and New Glycemic Control Agents Amanda R. Kriesen, R.Ph., PharmD, and Erin Bastick, R.Ph., PharmD Volume XXXV,
continuing education for pharmacists 2016 AACE/ACE Guidelines on Type 2 Diabetes Management and New Glycemic Control Agents Amanda R. Kriesen, R.Ph., PharmD, and Erin Bastick, R.Ph., PharmD Volume XXXV,
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Understanding Your Diabetes: A Basic Guide
 Understanding Your Diabetes: A Basic Guide Table of Contents First Steps to Managing Your Diabetes at Home When Your Blood Sugar is Too High (Hyperglycemia) Blood Sugar Targets and Blood Sugar Log How
Understanding Your Diabetes: A Basic Guide Table of Contents First Steps to Managing Your Diabetes at Home When Your Blood Sugar is Too High (Hyperglycemia) Blood Sugar Targets and Blood Sugar Log How
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
AACE/ACE Consensus Statement
 AACE/ACE Consensus Statement Statement by an American Association of Clinical Endocrinologists/ American College of Endocrinology Consensus Panel on Type 2 Diabetes Mellitus: An Algorithm for Glycemic
AACE/ACE Consensus Statement Statement by an American Association of Clinical Endocrinologists/ American College of Endocrinology Consensus Panel on Type 2 Diabetes Mellitus: An Algorithm for Glycemic
2/17/2016. Objectives. Define. Hey Sugar! DMII Management in Hospice Care
 Hey Sugar! DMII Management in Hospice Care Michelle Huber, R.Ph., PharmD.,CGP Objectives Review treatment for hyperglycemia discussing how these medications work, hypoglycemia risk, special considerations.
Hey Sugar! DMII Management in Hospice Care Michelle Huber, R.Ph., PharmD.,CGP Objectives Review treatment for hyperglycemia discussing how these medications work, hypoglycemia risk, special considerations.
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Remote attendees, please mute your phones as a courtesy thank you!
 Welcome! Remote attendees, please mute your phones as a courtesy thank you! Diabetes: The Ins and Outs of Insulin CareOregon Pharmacy Today s Agenda Introduction 8:00-8:15am RN perspective 8:15 8:45am
Welcome! Remote attendees, please mute your phones as a courtesy thank you! Diabetes: The Ins and Outs of Insulin CareOregon Pharmacy Today s Agenda Introduction 8:00-8:15am RN perspective 8:15 8:45am
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million