Pharmacology. Kacy Aderhold, MSN, APRN-CNS, CMSRN
|
|
|
- Nathan Patterson
- 5 years ago
- Views:
Transcription

1 Pharmacology Kacy Aderhold, MSN, APRN-CNS, CMSRN

2 Biguanides Decreases hepatic glucose production and improves insulin sensitivity (increases number of insulin receptors) Common Adverse Reaction: diarrhea Should be taken with food Can take 7 to 10 days to reach therapeutic levels Black Box Warning: lactic acidosis can occur Use cautiously with liver disease, IV dye studies, renal insufficiency Hold the day of procedures that involve IV dyes & 48 hours following Examples: metformin (Glucophage) metformin XR (Glucophage XR, Glumetza, Fortamet)
3 Thiazolidinediones (TZDs) Increases insulin sensitivity (improves receptivity of receptors) Black Box Warning: TZDs cause or exacerbate CHF, Avandia risk of MI Increase risk of peripheral fractures Onset of action = 3 weeks May take up to 12 weeks for maximum effect Examples: pioglitazone (Actos) Rosiglitazone (Avandia)
- daily with first meal glimipiride (Amaryl)-daily with first meal glipizide (Glucotrol)- daily or BID")
4 Sulfonylureas Stimulate beta cells of pancreas to release more insulin Hypoglycemia can occur Patients should not skip meals Examples: glyburide (Micronase, Glynase, DiaBeta)- daily with first meal glimipiride (Amaryl)-daily with first meal glipizide (Glucotrol)- daily or BID with food
5 Alpha-Glucosidase Inhibitors Slows breakdown of carbs in intestine Taken TID, at start of each meal SE: flatulence, bloating, abdominal pain May subside over time Examples: acarbose (Precose) miglitol (Glyset)
6 DPP-4 Inhibitors Inhibits dipeptidyl peptidase-4, slowing incretin metabolism, increasing insulin synthesis/release, decreasing glucagon levels Incretin enhancers, slows gastric emptying Given daily Examples: sitagliptin (Januvia) saxagliptin (Onglyza) linagliptin (Tradjenta) alogliptin (Nesina)
 nateglinide")
7 Meglitinides Stimulates pancreatic islet beta cell insulin release rapid insulin burst Hypoglycemia can occur Must be taken before meals Examples: repaglinide (Prandin) nateglinide (Starlix)
 dapagliflozin (Farxiga) empagliflozin")
8 SGLT2 Inhibitors Inhibits sodium-glucose cotransporter 2 (SGLT2) in the proximal nephron, reducing glucose reabsorption and increasing urinary glucose excretion Taken daily before first meal Contraindicated in renal impairment CrCl<45 SE: UTI, yeast infection Example canagliflozin (Invokana) dapagliflozin (Farxiga) empagliflozin (Jardiance)
9 Best Practice Oral Agents (OAs) OAs are inappropriate in most hospitalized patients Continued use may be appropriate in selected stable patients who consume meals at regular intervals Injectable noninsulin therapies such as exenatide and pramlintide have limitations similar to OAs ( Moghissi et al., 2009) Consider precautions for each component when using combination oral agents

10 Injectable Medications Non-Insulin Incretin Mimetics or GLP-1 Receptor Agonists Amylin Mimetics

- Taken bid with am and pm meal exenatide (Bydureon)- taken weekly liraglutide")
11 Incretin Mimetics GLP-1 Receptor Agonists Activates glucagon-like-peptide-1 receptors, increases insulin secretion, decreases glucagon secretion, and slows gastric emptying (incretin mimetic), increasing satiety Injection SE: nausea, indigestion, weight loss Examples: exenatide (Byetta)- Taken bid with am and pm meal exenatide (Bydureon)- taken weekly liraglutide (Victoza)- daily


12 Amylin Mimetic Activates insulin receptors, increases glucose secretion, slows gastric emptying, increase satiety Injection Taken before meals SE: nausea, weight loss Example pramlintide (Symlin)
 is a dopamine 2 agonist that activates neurotransmitters centrally, decreasing hyperglycemia")
13 Other: Bile acid sequestrant, colesevelam (Welchol) is a cholesterol lowering medication that also reduces blood glucose levels in patients with diabetes. Binds bile acid in intestinal tract, increasing hepatic bile acid production Bromocriptine (Cycloset) is a dopamine 2 agonist that activates neurotransmitters centrally, decreasing hyperglycemia without increasing insulin sensitivity Afrezza is a rapid-acting inhaled insulin that improves glycemic control in adults with diabetes mellitus, administered at the beginning of each meal.
14

15 Insulin
16 Types of Insulin Basal Insulin controls blood glucose in the fasting state glargine (Lantus) detemir (Levemir) NPH (Humulin N or Novolin N) (Intermediate Acting) Prandial or Nutritional Insulin blunts the rise in blood glucose following nutritional intake Short Acting Regular (R) (Humulin R or Novolin R) Rapid Acting lispro (Humalog) glulisine (Apidra) aspart (NovoLog) Correctional Insulin corrects hyperglycemia due to mismatch of nutritional intake and/or illness related factors and scheduled insulin administration Should be same as prandial insulin




17 The Discovery of Insulin Diabetes Video

18 Basal Insulin The pancreas secretes a small amount of insulin into the bloodstream every few minutes to match the liver s secretion of glucose. This allows a steady supply of glucose into the cells. Suppresses glucose production by the liver between meals and overnight % of daily insulin needs (TDD total daily dose) targets fasting BG Basal insulin available: detemir (Levemir) glargine (Lantus) NPH (Novolin N, Humulin N)
19 Basal Insulin: Pharmacokinetics Lantus (Glargine) Levemir (Detemir) NPH (Humulin N or Novolin N) Action Long acting Long acting Intermediate Onset 1 hour 1 hour 1-2 hours Peak Relatively peakless Relatively peakless 4-14 hours Duration hours* 6-23 hours* hours Color Clear Clear Cloudy Dosing 1-2 times/day 1-2 times/day 1-3 times/day *Dose dependent (Epocrates, 2015)

20 INSULIN EFFECT Glargine/Detemir B L S HS B Time
, limits hyperglycemia after intake.")
21 Bolus Insulin Provides a fast/rapid response to elevations in BG levels. Nutritional/prandial insulin- also referred to as Y covers carbohydrates intake (food, liquids, IVs,TPN,TF), limits hyperglycemia after intake. Correctional insulin- also referred to as X decreases elevations in BG, corrects for hyperglycemia % of daily insulin needs (TDD) targets post-prandial BG levels Bolus insulin available: aspart (NovoLog) lispro (Humalog) glulisine (Apidra) regular (Humulin R, Novolin R)
22 Nutritional and Correctional Insulin: Pharmacokinetics Regular (Humulin R or Novolin R) Humalog (Lispro) Novolog (Aspart) Apridra (Glulisine) Action Fast acting Rapid acting Rapid acting Rapid acting Onset minutes 5-15 minutes minutes 5-15 minutes Peak 2-4 hours minutes 1-3 hours 55 minutes Duration 5-6 hours 3-4 hours 3-5 hours 3-4 hours Color Clear Clear Clear Clear Dosing minutes before a meal Right before or immediately after a meal, acts as basal insulin when used in an insulin pump with frequent delivery (Epocrates, 2015)
23 Bolus Insulin


24 INSULIN EFFECT Basal/Bolus Insulin Regimen Morning Afternoon Evening Night RAA* RAA* RAA* Glargine/Detemir B L S HS B MEALS RAA* = Rapid Acting Analog (Lispro/Aspart)
25 INSULIN EFFECT Natural Insulin Secretion Morning Afternoon Evening Body s post prandial insulin secretion in response to carb intake Night Body s basal insulin secretion B L S HS B MEALS
26 Insulin Mixtures Contain a pre-mixed combination of intermediate acting basal insulin and short/rapid bolus insulin, stated as %/% Have double peaks of action Types: Humulin 70/30, 50/50 and Novolin 70/30 contain NPH and regular insulin in stated percentages. Should be given minutes before meal Humalog mix 75/25, 50/50 and NovoLog mix 70/30 contain a long and rapid insulin in stated percentages. May be given right before meal to immediately after meal
27 Insulin Mixtures Humulin 70/30, 50/50 or Novolin 70/30 Novolog mix 70/30 Humalog mix 75/25, 50/50 B L S BT B L S BT Onset: minutes Peak: 2 to 12 hours (double peak) Lasts: hours Onset: 5-15 minutes Peak: 1-6 hours (double peak) Lasts: hours
28 Sliding Scale Insulin Prolonged Sliding Scale Insulin (SSI) as the sole regimen is ineffective in the majority of patients. SSI increases risk of both hyperglycemia and hypoglycemia. SSI is associated with adverse outcomes in general surgery patients with T2DM. SSI is potentially dangerous in T1DM. Corrective Insulin or the use of additional short or rapid acting insulin in conjunction with scheduled insulin doses to treat BG levels above desired targets, is preferred. (ADA, 2015)

29 Timing of Insulin Rapid acting insulin like Novolog may be given right before meal to immediately after meal Insulin doses given late can cause the next FSBS reading to be high since the insulin did not have enough time to fully work before we are taking the FSBS again FSBS should be taken 30 minutes or less before patient eats FSBS taken early can result in high FSBS readings due to the insulin not having time to complete duration before FSBS taken
30 Insulin Stacking Insulin stacking occurs when short or rapid acting S.Q. insulin doses are given too close together. Consider: Rapid insulin SQ should not be dosed any closer than 3 hours apart. Consider: Regular insulin SQ should not be dosed any sooner than 4 hours apart.

31 Insulin Alert Insulin is a high-alert, high-risk drug. Verify patient s BG before calculation of dose is completed. Verify dose calculation with another RN, LPN or clinical pharmacist. To prevent hypoglycemia from an insulin overdose, never give an IV insulin bolus by increasing the infusion rate temporarily via the infusion pump. Don t confuse NovoLog.. Novolin Humalog.. Humulin Novolin 70/30. NovoLog mix 70/30 Humulin 50/50.Humalog mix 50/50 INTEGRIS Health's policy on Insulin Administration
32 To Hold or Not to Hold? Oral Agents: What to do: Secretagogues Sulfunylureas, Prandin, Starlix Hold if not tolerating meals Metformin Hold if dehydrated, N&V, compromised renal or cardiac status, dye study, sepsis, any serious illness, immediate post-op Thiazolidinediones Insulin: May be given unless patient is unable to swallow or strict NPO What to do: Basal Insulin Glargine (Lantus), Detemir (Levemir) Do not HOLD NPO, patient should always have full dose without regard to food intake Basal Insulin - NPH Do not HOLD If NPO, patient will need ½ to 2/3 of their usual dose Bolus Insulin Regular, lispro(humalog), aspart(novalog), apidra IF NPO, hold meal doses and give only correction doses for hyperglycemia
33 Insulin Infusion Insulin infusions are a physician s order. There are several insulin infusions that may be ordered at INTEGRIS Health: Intensive Insulin Infusion, Maintenance Insulin Infusion, or as part of the DKA protocol (low-dose insulin infusion). Some indications for insulin infusion include: Critical Care Illness MI Carcinogenic Shock Perioperative care Surgical illness Corticosteroid therapy
34 Transitioning from Insulin Infusion to Subcutaneous Insulin Why? Volume resuscitated Pressor support discontinued Ready to resume eating How? Initiate subcutaneous insulin injections Give a dose of subcutaneous basal insulin 2 hours before discontinuing insulin infusion to prevent hyperglycemia

35 Insulin Pen Use in the Hospital Benefits: Decrease nursing time needed to prepare an insulin injection Decrease dosing errors Decrease accidental needle sticks Alerts: DO NOT share pens with more than one patient. Studies have shown that biological contamination of insulin occurred in up to half of all insulin pen cartridges that were reused with multiple patients. DO NOT use pen cartridges as a multi-dose vial. Insulin should not be withdrawn from the pen with a syringe- this will result in inaccurate measurement of future doses. How to Use Insulin Pen Video Insulin Pen Safety Video Insulin Pen Instructions
36

37 Insulin Multi-dose Vial in Omnicell What is the process? Levemir, Aspart, and Regular insulin will be kept in the Omnicell. 1. Bring alcohol swabs and a syringe with you to the Omnicell. 2. Select your patient and the correct insulin from the Omnicell screen. 3. Enter the amount of units you are withdrawing from the vial as quantity. So, if you are giving an 8 unit dose, remove quantity of When the drawer opens, swab the insulin vial with alcohol, draw up the correct dose, replace the insulin vial in the drawer, select a barcode from the pocket, attach barcode to your syringe, shut the drawer, and log out.






38 How to Label the Insulin Syringe The Omnicell will contain barcodes to attach to the insulin syringe. Call your satellite pharmacist if you ever run out of labels. Attach the barcode to the syringe lengthwise so the barcode can be scanned. Do not cover the graduations on the syringe. The dose needs to be readable at all times. Do not wrap the label around the syringe. This will make it impossible to scan the barcode.


39 Remember! When giving an insulin injection using a syringe, pinch the skin using your thumb and index finger. Insert the needle quickly and firmly at a 90 angle.

40 Insulin Expiration Date Insulin can be stored at room temperature up to 28 days after opening. Pharmacy will label all vials stored in the Omnicell with the proper expiration date.


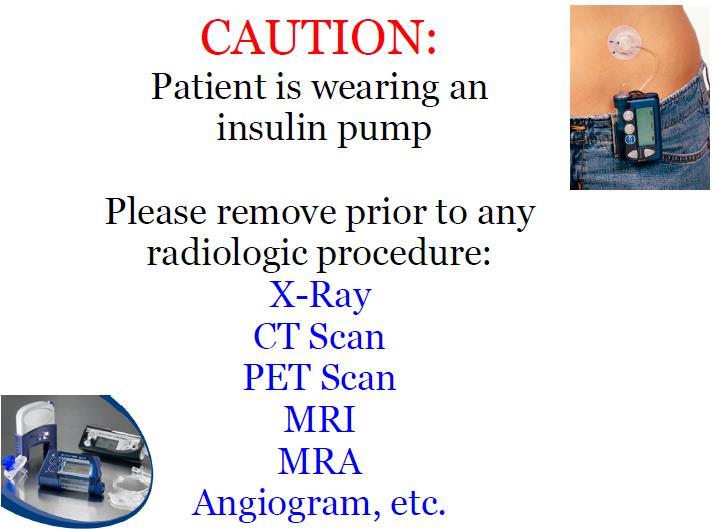
41 Insulin Pumps Consists of a pump, reservoir, and infusion set that delivers insulin through plastic tubing subcutaneously Allows flexibility in lifestyle and better glucose control Mimics normal functioning pancreas Patients may self-manage in the hospital if mentally and physically capable (physician s order) Nursing must document basal and bolus doses Before pump is removed, ensure subq insulin is initiated DKA can develop within 4-6 hours without insulin Insulin Pump sign should be hung in patient s room INTEGRIS Health's Insulin Pump Policy We must check FSBS with our glucometers!
42
=u-500 insulin is 5 times as")

 Concentrated Doses")
43 High Potency Insulin U-500 Usually insulin is 100 units/ml, U-500 is 500 units/ml (very concentrated)=u-500 insulin is 5 times as strong as regular insulin Used for treatment of patients with high daily insulin requirements Regular Insulin ONLY Requires special dosing calculation Given twice - three times daily before meals U-500 Policy U-300 Insulin glargine (Toujeo) Concentrated Doses preadjusted
44 Survival Skills Discharge Education Provider who will manage DM after discharge Assess need for HH or outpatient DM education Diagnosis SMBG & home goals Information on consistent eating patterns When & how to take BG lowering medications Sick day management Proper use & disposal of needles & syringes (ADA, 2015)

45 Patient Teaching-Insulin Administration Start patient teaching as soon as you know patient will go home on insulin. Have patient demonstrate! Discuss dosage, timing, and peaks of insulin they use Discuss site selection & rotation Safe injection practices!

46 Patient Teaching- Insulin Administration Includes: site selection, drawing insulin from a vial, mixing insulin, using insulin pens, and throwing away supplies

47 Safe Injection Practices

48 One Pen, One Person
49 References American Diabetes Association. Standards of Medical Care in Diabetes 2010 (Position Statement). Diabetes Care, 33(1), S11-S61. American Diabetes Association (2015). Standards of Care. Diabetes Care 38 (1), S1-S99. Bode, B., Braithwaite, S., Steed, D., Davidson, P., (2004). Ace Inpatient Diabetes and Metabolic Control Consensus Conference. Intravenous insulin infusion therapy: indications, methods, and transition to subcutaneous insulin therapy. Endocrine Practice, 10(2), Diabetes Blog Site (2015). What did dogs teach humans about diabetes? Retrieved from Fonseca, V. A., (Ed.). (2006). Clinical diabetes: Translating research into practice. Philadelphia: Saunders Elsevier. Garber, A. J., Handelsman, Y., Einhorn, D., Bergman, D. A., Bloomgarden, Z. T., Fonseca, V., et al. (2008). Diagnosis and management of prediabetes in the continuum of hyperglycemia when do the risks of diabetes begin? A consensus statement from the American College of Endocrinology and the American Association of Clinical Endocrinologists. Endocrine Practice 14(7), Greenspan, F. S., Gardner, D. G. (Eds.). (2001). Basic and clinical endocrinology (6th ed.). New York: Lange/McGraw Hill Insulin. (201). In Epocrates Essentials for Apple ios (Version 5.1) [Mobile application software]. Retrieved from International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International Association of Diabetes and Pregnancy Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy, (2010). Diabetes Care, 33(3), ). Kruger, D. F., Aronoff, S. L., Edelman, S. V., Current and future perspectives on the role of hormonal interplay in glucose homeostasis. The Diabetes Educator. 33(S2), 32S-46S. Moghissi, E. S., Korytkowski, M. T., DiNardo, M., Einhorn, D., Hellman, R., Hirsch, I. B., et al. (2009). American Association of Clinical Endocrinologists and American Diabetes Association Consensus Statement on inpatient glycemic control. Endocrine Practice, 15(4), 1-15.
Objectives. How Medicine Works to Control Blood Sugar Levels. What Happens When We Eat? What is diabetes? High Blood Glucose (Hyperglycemia)
") How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
DIABETES. overview of pharmacologic agents used in the management of. Overview 4/3/2014 OBJECTIVES. Injectable Agents
 overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
RPCC Pharmacy Forum. The Type 2 Diabetes Issue. Type 2 Diabetes: The Basics
 Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018
 Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions. Insulins. Rapid Short Intermediate Long Mix
 Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Diabetes Medications: Oral Anti-Hyperglycemic Medications
 Diabetes Medications: Oral Anti-Hyperglycemic Medications Medication Types 1. Biguanides 2. Sulfonylureas 3. Thiazolidinediones (TZDs) 4. Alpha-Glucosidase Inhibitors 5. D-Phenylalanine Meglitinides 6.
Diabetes Medications: Oral Anti-Hyperglycemic Medications Medication Types 1. Biguanides 2. Sulfonylureas 3. Thiazolidinediones (TZDs) 4. Alpha-Glucosidase Inhibitors 5. D-Phenylalanine Meglitinides 6.
Pharmacologic Agents for Treatment of Type 2 Diabetes
 Pharmacologic Agents for Treatment of Type 2 Diabetes SCAN Drugs Medication Biguanides 1 1 er uncoated tabs 500 mg & 750 mg Sulfonylureas 1 1 500 850 mg QD - TID 500 2000 mg glimepiride 1 1 1 8 mg glipizide
Pharmacologic Agents for Treatment of Type 2 Diabetes SCAN Drugs Medication Biguanides 1 1 er uncoated tabs 500 mg & 750 mg Sulfonylureas 1 1 500 850 mg QD - TID 500 2000 mg glimepiride 1 1 1 8 mg glipizide
Diabetes Management: A diagnostic perspective
 Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
4/9/2018 HOW TO REGULATE DIABETES MEDICATIONS. By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE. Diagnosis
 HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
Oral Medication for the Management of Diabetes Mechanism of. Duration of Daily Dosing Action
 Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
FARXIGA (dapagliflozin) Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)
 Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)") Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
1/15/2018. Disclosures. Current Diabetes Medications. Objectives NON-INSULIN AGENTS. Diabetes Med Classes. Mealtime
 Disclosures Current Diabetes Medications None Claire Baker, M.D. Diabetes & Endocrine Associates January 24, 2018 Objectives Identify categories of diabetes medications Understand the pharmacology of diabetes
Disclosures Current Diabetes Medications None Claire Baker, M.D. Diabetes & Endocrine Associates January 24, 2018 Objectives Identify categories of diabetes medications Understand the pharmacology of diabetes
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA 2012 Virginia Mason Medical
 Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Non-Insulin Diabetes Medications Summary
 Non-Insulin Diabetes Medications Summary Medications marked with an asterisk (*) can cause hypoglycemia INSULIN SECRETAGOGUES Sulfonylureas* GLYBURIDE* (Diabeta) (Micronase) production. Side effects: Potential
Non-Insulin Diabetes Medications Summary Medications marked with an asterisk (*) can cause hypoglycemia INSULIN SECRETAGOGUES Sulfonylureas* GLYBURIDE* (Diabeta) (Micronase) production. Side effects: Potential
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
I. General Considerations
 1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Clinical Cases in Diabetes Management. Joseph Cook D.O.
 Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Diabetes Treatment Guidelines
 Diabetes Treatment Guidelines For more comprehensive information about current approaches to the diagnosis and treatment of diabetes, visit the American Diabetes Association Standards of Medical Care 2018
Diabetes Treatment Guidelines For more comprehensive information about current approaches to the diagnosis and treatment of diabetes, visit the American Diabetes Association Standards of Medical Care 2018
How to Fight Diabetes and Win. Diabetes. Medications
 How to Fight Diabetes and Win Diabetes Medications MEDICATIONS FOR DIABETES According to the American Diabetes Association, 85% of adults diagnosed with diabetes take insulin and/or oral medication to
How to Fight Diabetes and Win Diabetes Medications MEDICATIONS FOR DIABETES According to the American Diabetes Association, 85% of adults diagnosed with diabetes take insulin and/or oral medication to
Oral and Injectable Medication Options for Diabetes Treatment
 Oral and Injectable Medication Options for Diabetes Treatment Presented by: Dr. Daphne E. Smith, Pharm.D., CDE Clinical Assistant Professor/Clinical Pharmacist-University of Illinois at Chicago College
Oral and Injectable Medication Options for Diabetes Treatment Presented by: Dr. Daphne E. Smith, Pharm.D., CDE Clinical Assistant Professor/Clinical Pharmacist-University of Illinois at Chicago College
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
DIABETES. Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes. November 2013
 DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
2018 Diabetes Summit Managing Diabetes: An Art and a Science
 2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
Physician Drug Reference Chart for Diabetes Antidiabetic Medications
 Drug Class Compound Brand Name Mechanism of Action Advantages Disadvantages Alpha-glucosidase inhibitors Medium Cost by Bayer Healthcare, Pfizer, Takeda Research Acarbose Miglitol Voglibose Precose Glyset
Drug Class Compound Brand Name Mechanism of Action Advantages Disadvantages Alpha-glucosidase inhibitors Medium Cost by Bayer Healthcare, Pfizer, Takeda Research Acarbose Miglitol Voglibose Precose Glyset
Diabetes Update 2018: Challenging Transitions. Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System
 Diabetes Update 2018: Challenging Transitions Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System 1 Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley
Diabetes Update 2018: Challenging Transitions Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System 1 Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley
Diabetes Update 2018: Challenging Transitions. Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System
 Diabetes Update 2018: Challenging Transitions Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System 1 Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley
Diabetes Update 2018: Challenging Transitions Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley Health System 1 Patricia A. Daly, MD, FACP, FACE Medical Director for Diabetes Valley
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Antidiabetic Agents CHAPTER BIGUANIDES
 ajt/shutterstock, Inc. CHAPTER 2 Antidiabetic Agents Charles Ruchalski, PharmD, BCPS BIGUANIDES For newly diagnosed patients with type 2 diabetes, the biguanide metformin is the drug of choice for initial
ajt/shutterstock, Inc. CHAPTER 2 Antidiabetic Agents Charles Ruchalski, PharmD, BCPS BIGUANIDES For newly diagnosed patients with type 2 diabetes, the biguanide metformin is the drug of choice for initial
TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
Rebecca Newberry APRN MS CDE
 Current Diabetes Medications Nursing Implications and Applications Rebecca Newberry APRN MS CDE Methodist Center for Diabetes and Nutritional Health Disclosures Objectives Speakers Bureaus/Consulting Board
Current Diabetes Medications Nursing Implications and Applications Rebecca Newberry APRN MS CDE Methodist Center for Diabetes and Nutritional Health Disclosures Objectives Speakers Bureaus/Consulting Board
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Type. Diabetes Drugs. A Review
 Type Diabetes is a common diagnosis for home care patients. Diabetes drugs are now available that target the multiple defects of metabolism that characterize Type 2 diabetes. Understanding the wide variety
Type Diabetes is a common diagnosis for home care patients. Diabetes drugs are now available that target the multiple defects of metabolism that characterize Type 2 diabetes. Understanding the wide variety
Diabetes Basics. Type 1 diabetes The body cannot make insulin Requires insulin injection Is not treated with oral diabetes medicines (pills)
") Diabetes Basics What is Diabetes? Diabetes is a disease in which the pancreas is unable to make insulin or the body is unable to use insulin or both. This leads to high blood sugar levels in the blood.
Diabetes Basics What is Diabetes? Diabetes is a disease in which the pancreas is unable to make insulin or the body is unable to use insulin or both. This leads to high blood sugar levels in the blood.
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Improving Patient Outcomes with Individualized Therapy in the Management of Type 2 Diabetes
 Improving Patient Outcomes with Individualized Therapy in the Management of Type 2 Diabetes Timothy S. Reid, M.D. Mercy Diabetes Center Janesville, WI Duality Statement Dr. Reid is a Speaker and Consultant
Improving Patient Outcomes with Individualized Therapy in the Management of Type 2 Diabetes Timothy S. Reid, M.D. Mercy Diabetes Center Janesville, WI Duality Statement Dr. Reid is a Speaker and Consultant
Advanced Practice Education Associates. Endocrine
 Advanced Practice Education Associates Endocrine Overview Diabetes Thyroid Disease 162 Copyright 2016 Advanced Practice Education Associates DIABETES MELLITUS What is the BMI cut point for screening adults
Advanced Practice Education Associates Endocrine Overview Diabetes Thyroid Disease 162 Copyright 2016 Advanced Practice Education Associates DIABETES MELLITUS What is the BMI cut point for screening adults
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Clinical Practice Guidelines
 Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
DIABETES (1 of 5) Generic. Generic $0 $5 $5-10 $0 $0 $0. Generic $0 $5 $5-10. Generic. Generic $0 $5 $5-10 $0 $0 $0. Generic $0 $5 $5-10 $0 $0 $0
 Generic. Generic $0 $5 $5-10 $0 $0 $0. Generic $0 $5 $5-10. Generic. Generic $0 $5 $5-10 $0 $0 $0. Generic $0 $5 $5-10 $0 $0 $0") Metformin DIABETES (1 of 5) Glucophage Glucophage XR ER $7 (500mg) $7 (500mg) $5 $5 500mg, 750mg only 500mg, 750mg only Sulfonylurea/Combinations Amaryl Glucotrol glimepiride glipizide $5 $5 Glucotrol
Metformin DIABETES (1 of 5) Glucophage Glucophage XR ER $7 (500mg) $7 (500mg) $5 $5 500mg, 750mg only 500mg, 750mg only Sulfonylurea/Combinations Amaryl Glucotrol glimepiride glipizide $5 $5 Glucotrol
Type II Diabetes Improving Blood Sugar Control. Geneva Clark Briggs, Pharm.D., BCPS
 Type II Diabetes Improving Blood Sugar Control Geneva Clark Briggs, Pharm.D., BCPS Overview Importance of glucose control State of control Review available therapies Helping patients achieve control The
Type II Diabetes Improving Blood Sugar Control Geneva Clark Briggs, Pharm.D., BCPS Overview Importance of glucose control State of control Review available therapies Helping patients achieve control The
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
Understanding Diabetes and Insulin Delivery Systems
 Page 1 This program has been supported by an educational grant from Sanofi Aventis Scott K. Stolte, Pharm.D. Associate Dean, Academic Affairs Bernard J. Dunn School of Pharmacy Shenandoah University Winchester,
Page 1 This program has been supported by an educational grant from Sanofi Aventis Scott K. Stolte, Pharm.D. Associate Dean, Academic Affairs Bernard J. Dunn School of Pharmacy Shenandoah University Winchester,
Disclosure 1/16/2017. Michael R. Brennan D.O., M.S., F.A.C.E Director Beaumont Endocrine Center Chief of Endocrine Beaumont Grosse Pointe 1/16/2017 2
 Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD. Disclosures. Objectives 9/1/2015
 Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
New Therapies for Diabetes
 Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
What You Should Know About Diabetes. Laura Bingell RN Transition Center Nurse for MFP (607)
") What You Should Know About Diabetes Laura Bingell RN Transition Center Nurse for MFP (607)962-8225 lbingell@ilny.org Diabetes Mellitus (DM) a group of diseases marked by high blood glucose levels. 9.3%
What You Should Know About Diabetes Laura Bingell RN Transition Center Nurse for MFP (607)962-8225 lbingell@ilny.org Diabetes Mellitus (DM) a group of diseases marked by high blood glucose levels. 9.3%
Managing Complex Diabetes Cases: Medication Update. Celia Levesque MSN, RN, CNS-BC, CDE, BC-ADM
 Managing Complex Diabetes Cases: Medication Update Celia Levesque MSN, RN, CNS-BC, CDE, BC-ADM clevesqu@mdanderson.org Objectives Describe how each diabetes medication class is used to treat diabetes Differentiate
Managing Complex Diabetes Cases: Medication Update Celia Levesque MSN, RN, CNS-BC, CDE, BC-ADM clevesqu@mdanderson.org Objectives Describe how each diabetes medication class is used to treat diabetes Differentiate
How they work and when to take them. Diabetes Medications
 How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
The Community Pharmacist s Role in Diabetes Treatment
 CONTINUING EDUCATION The Community Pharmacist s Role in Diabetes Treatment By Kimberly Ference, PharmD U pon completion of this activity, the pharmacist should be able to achieve these directives: 1. Describe
CONTINUING EDUCATION The Community Pharmacist s Role in Diabetes Treatment By Kimberly Ference, PharmD U pon completion of this activity, the pharmacist should be able to achieve these directives: 1. Describe
第十五章. Diabetes Mellitus
 Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Collaborative Practice Agreement
 Collaborative Practice Agreement [community pharmacy name] [address] [phone number] [physician practice] [address] [phone number] Effective: [date] Expiration: [date] 1 Table of Contents 1.0 Introduction...4
Collaborative Practice Agreement [community pharmacy name] [address] [phone number] [physician practice] [address] [phone number] Effective: [date] Expiration: [date] 1 Table of Contents 1.0 Introduction...4
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Glycemic Management of Type 2 Diabetes. Gail Nunlee-Bland, M.D. Professor Medicine & Pediatrics Director, Diabetes Treatment Center Howard University
 Glycemic Management of Type 2 Diabetes Gail Nunlee-Bland, M.D. Professor Medicine & Pediatrics Director, Diabetes Treatment Center Howard University 1 None Disclosures Learning Objectives Understand the
Glycemic Management of Type 2 Diabetes Gail Nunlee-Bland, M.D. Professor Medicine & Pediatrics Director, Diabetes Treatment Center Howard University 1 None Disclosures Learning Objectives Understand the
Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18
 Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18 No conflicts of interest Objectives for this talk Update on non-insulin drug therapy fro type 2 DM Appropriate use of insulin in type 2 DM ADA
Type 2 Diabetes Mellitus: Update on Pharmacotherapy 04/04/18 No conflicts of interest Objectives for this talk Update on non-insulin drug therapy fro type 2 DM Appropriate use of insulin in type 2 DM ADA
Healthy You: A Guide to Diabetes Self-Care SURVIVAL SKILLS
 Healthy You: A Guide to Diabetes Self-Care SURVIVAL SKILLS Table of Contents Introduction 3 Monitoring Your Diabetes 7 Medications 11 Problem Solving 24 Healthy Eating with Diabetes 26 Managing Sick Days
Healthy You: A Guide to Diabetes Self-Care SURVIVAL SKILLS Table of Contents Introduction 3 Monitoring Your Diabetes 7 Medications 11 Problem Solving 24 Healthy Eating with Diabetes 26 Managing Sick Days
CE on SUNDAY Miami, FL May 31, 2009
 CE on SUNDAY Miami, FL May 31, 2009 Date: Sunday, May 31, 2009 Time: 1:15 PM 2:15 PM Location: Doubletree Miami Mart/Airport Hotel Title: Speaker(s): Understanding Diabetes and Insulin Delivery Systems
CE on SUNDAY Miami, FL May 31, 2009 Date: Sunday, May 31, 2009 Time: 1:15 PM 2:15 PM Location: Doubletree Miami Mart/Airport Hotel Title: Speaker(s): Understanding Diabetes and Insulin Delivery Systems
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Jeffery Davies, DO, MPH, FACOEP ACOEP Chicago, IL October Your DM patient is ready for discharge, now what?
 Jeffery Davies, DO, MPH, FACOEP ACOEP Chicago, IL October 2018 Your DM patient is ready for discharge, now what? Financial Disclosures None Objectives 1. Understand follow up patterns/capability of patients
Jeffery Davies, DO, MPH, FACOEP ACOEP Chicago, IL October 2018 Your DM patient is ready for discharge, now what? Financial Disclosures None Objectives 1. Understand follow up patterns/capability of patients
continuing education for pharmacists
 continuing education for pharmacists 2016 AACE/ACE Guidelines on Type 2 Diabetes Management and New Glycemic Control Agents Amanda R. Kriesen, R.Ph., PharmD, and Erin Bastick, R.Ph., PharmD Volume XXXV,
continuing education for pharmacists 2016 AACE/ACE Guidelines on Type 2 Diabetes Management and New Glycemic Control Agents Amanda R. Kriesen, R.Ph., PharmD, and Erin Bastick, R.Ph., PharmD Volume XXXV,
3/16/2015. Improving the Management of Diabetes. W21 Angie Edmonds, PharmD, CGP Lorinda Babb, PharmD, CGP. Speaker Contact Information
 Improving the Management of Diabetes W21 Angie Edmonds, PharmD, CGP Lorinda Babb, PharmD, CGP Speaker Contact Information Angie Edmonds Angela.edmonds@omnicare.com Lorinda Babb lorinda.babb@omnicare.com
Improving the Management of Diabetes W21 Angie Edmonds, PharmD, CGP Lorinda Babb, PharmD, CGP Speaker Contact Information Angie Edmonds Angela.edmonds@omnicare.com Lorinda Babb lorinda.babb@omnicare.com
Drug Therapy in Diabetes HEATHER TINGLE UK COLLEGE OF PHARMACY, PY4
 Drug Therapy in Diabetes HEATHER TINGLE UK COLLEGE OF PHARMACY, PY4 OVERVIEW Characteristic Type 1 DM (10%) Type 2 DM (90%) Formerly known as Juvenile; Insulin-dependent Adult onset; Non-insulin dependent
Drug Therapy in Diabetes HEATHER TINGLE UK COLLEGE OF PHARMACY, PY4 OVERVIEW Characteristic Type 1 DM (10%) Type 2 DM (90%) Formerly known as Juvenile; Insulin-dependent Adult onset; Non-insulin dependent
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Update on Diabetes Mellitus
 Update on Diabetes Mellitus Treatment: Targeting the Incretin System Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose control Amylin Incretin Hormones New therapies
Update on Diabetes Mellitus Treatment: Targeting the Incretin System Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose control Amylin Incretin Hormones New therapies
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
Insulin Prior Authorization with optional Quantity Limit Program Summary
 Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
New Medications and Prescribing Methods for Diabetic Patients
 New Medications and Prescribing Methods for Diabetic Patients Jeffrey Stroup, PharmD, BCPS, FCCP Professor of Medicine Oklahoma State University Center for Health Sciences Department of Internal Medicine
New Medications and Prescribing Methods for Diabetic Patients Jeffrey Stroup, PharmD, BCPS, FCCP Professor of Medicine Oklahoma State University Center for Health Sciences Department of Internal Medicine
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Making Sense of Mediations for Diabetes
 Making Sense of Mediations for Diabetes Lisa Kroon, PharmD, CDE Professor of Clinical Pharmacy UCSF School of Pharmacy Diabetes Mellitus: U.S. Impact Source: ADA; released June 10, 2014 ~1-1.5 Million
Making Sense of Mediations for Diabetes Lisa Kroon, PharmD, CDE Professor of Clinical Pharmacy UCSF School of Pharmacy Diabetes Mellitus: U.S. Impact Source: ADA; released June 10, 2014 ~1-1.5 Million
ORAL AGENTS OLD & NEW FOR THE MANAGEMENT OF T2DM
 ORAL AGENTS OLD & NEW FOR THE MANAGEMENT OF T2DM ECHO-Diabetes July 21, 2016 VERONICA BRADY, PHD, FNP-BC, BC-ADM, CDE OBJECTIVES Overview of Diabetes Oral hypoglycemic agents Define various classes of
ORAL AGENTS OLD & NEW FOR THE MANAGEMENT OF T2DM ECHO-Diabetes July 21, 2016 VERONICA BRADY, PHD, FNP-BC, BC-ADM, CDE OBJECTIVES Overview of Diabetes Oral hypoglycemic agents Define various classes of
Learning Objectives. Impact of Diabetes II UPDATES IN TYPE 2 DIABETES. David Doriguzzi, PA-C
 UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
Update on Diabetic Medications UMA SUNDARAM, M.D. DIABETES & ENDOCRINE ASSOCIATES APRIL 07, 2018
 Update on Diabetic Medications UMA SUNDARAM, M.D. DIABETES & ENDOCRINE ASSOCIATES APRIL 07, 2018 Disclosure NONE Objectives To identify different categories of diabetes medications Understand the pharmacology
Update on Diabetic Medications UMA SUNDARAM, M.D. DIABETES & ENDOCRINE ASSOCIATES APRIL 07, 2018 Disclosure NONE Objectives To identify different categories of diabetes medications Understand the pharmacology
Rhonda Eustice, PharmD, CDE. Will Power lasts about two weeks and is soluble in alcohol. Mark Twain
 Rhonda Eustice, PharmD, CDE Will Power lasts about two weeks and is soluble in alcohol. Mark Twain Diabetes Management: The Three Legged Stool Diet Medication Exercise Objectives Know the treatment goals
Rhonda Eustice, PharmD, CDE Will Power lasts about two weeks and is soluble in alcohol. Mark Twain Diabetes Management: The Three Legged Stool Diet Medication Exercise Objectives Know the treatment goals
Endo 2 SLO Practice (online) Page 1 of 7
 Page 1 of 7") Endo 2 SLO Practice (online) Page 1 of 7 1. A long- acting insulin, like Lantus is for? A. When the next meal is within 30-60 minutes of the injection B. Over night use or for ½ of the day often combined
Endo 2 SLO Practice (online) Page 1 of 7 1. A long- acting insulin, like Lantus is for? A. When the next meal is within 30-60 minutes of the injection B. Over night use or for ½ of the day often combined
Diabetes 2016: Strategies for achieving optimal diabetes control
 PHASE Safety Net Community Benefit Diabetes 2016: Strategies for achieving optimal diabetes control Presented by: Lisa Gilliam, MD, PhD Clinical Leader Diabetes Program Kaiser Permanente Northern California
PHASE Safety Net Community Benefit Diabetes 2016: Strategies for achieving optimal diabetes control Presented by: Lisa Gilliam, MD, PhD Clinical Leader Diabetes Program Kaiser Permanente Northern California
STEP THERAPY CRITERIA
 CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Remote attendees, please mute your phones as a courtesy thank you!
 Welcome! Remote attendees, please mute your phones as a courtesy thank you! Diabetes: The Ins and Outs of Insulin CareOregon Pharmacy Today s Agenda Introduction 8:00-8:15am RN perspective 8:15 8:45am
Welcome! Remote attendees, please mute your phones as a courtesy thank you! Diabetes: The Ins and Outs of Insulin CareOregon Pharmacy Today s Agenda Introduction 8:00-8:15am RN perspective 8:15 8:45am
HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN. Kacy Aderhold, MSN, APRN-CNS, CMSRN
 HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN Kacy Aderhold, MSN, APRN-CNS, CMSRN Hyperglycemia Management Protocol Mimics the body s normal pancreas function, releasing a slow steady amount
HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN Kacy Aderhold, MSN, APRN-CNS, CMSRN Hyperglycemia Management Protocol Mimics the body s normal pancreas function, releasing a slow steady amount