Foundation In Diabetes Course. Community Diabetes Specialist Nurse Team, BHFT West
|
|
|
- Muriel Ramsey
- 5 years ago
- Views:
Transcription
1 Foundation In Diabetes Course Community Diabetes Specialist Nurse Team, BHFT West
2 Learning Outcomes Understand what Diabetes is Understand how to recognise and diagnose diabetes Understand key medications Understand key diet principals Understand the impact of diabetes complications Understand diabetes care in Berkshire West
3 Session 1 What is Diabetes?
4 What is Diabetes?
5 Who is at risk of developing diabetes? You re overweight or have a high Body Mass Index (BMI). You have a large waist (more than 80cm/31.5 inches in women, 94 cm/37 inches in men or 90cm/35 inches in South Asian men). You re from an African-Caribbean, Black African, Chinese or South Asian background and over 25. You re from another ethnic background and over 40. You have a parent, brother or sister with diabetes. You have ever had high blood pressure, a heart attack or a stroke. You have a history of polycystic ovaries, gestational diabetes or have given birth to a baby over 10 pounds/4.5kg. You suffer from schizophrenia, bipolar illness or depression, or you are taking anti-psychotic medication.

6 Diagnosis of diabetes
7 Classification WHO 1999 Encompasses clinical stages and aetiological types of diabetes. Four classifications: Type 1 Type 2 Gestational Other ( drug induced / pancreatic disease/mody )
8 Monitoring of diabetes HbA1c A measurement of average control over past 3 months. Venous blood test If raised blood becomes thick and sticky
9 HbA1c > Very poor control Poor control Acceptable control Excellent control
10 Self Blood Glucose monitoring Before meals: mmol/l After meals: (2 hours) < 8.5 mmol/l 80% of readings at target should equate to target HbA1c of < 54 mmol/mol Targets need to take into account personal/social situation/patient choice
11 NICE guidelines for blood glucose management Self Monitoring should: not be a stand-alone intervention Have a clear need and purpose Be used in conjunction with appropriate therapy as part of integrated self-care with agreed targets and goal
12 UKPDS: Benefits of tight control Reducing HbA1c from mmols/mol reduces Any diabetes related complication by 12% Any microvascular complication by 25% Progression of retinopathy by 21% Cataract by 24% Myocardial infarction by 16%
13 Diet
14 Content of Food Blood glucose levels are affected by the type of food eaten. Key to controlling blood glucose levels is to understand how and why different foods affect it. Dietary changes can help to keep blood glucose levels within the target range. Food consists of 3 main nutrients which are broken down to form their basic units. Carbohydrates Protein Fats Sugars Amino acids Fatty acids & Glycerol










15 Carbohydrates All carbohydrate eaten and drank are broken down into sugars. Carbohydrates can be classified into two main groups. Starch Sugar
16 Principle of the Glycaemic Index The type and amount of carbohydrate consumed makes a difference to blood glucose levels. Some carbohydrate foods breakdown more quickly than others. Quick = High Glycaemic Index Slow = Low Glycaemic Index Type of starch, fibre content, cooking process, high fat/protein content, acidic foods affect the glycaemic index of food.

 melon, pineapple, figs, raisins, banana (ripe) new potatoes,")
 baked potato, mashed potato (and instant), chips cornflakes, rice krispies, white, brown, bagels jasmine rice")
17 Glycaemic Index of Foods Fruit Vegetables Cereals Breads Legumes Grains Low (<55) apples, grapes, berries, banana, oranges most vegetables, sweet potato, corn on the cob, sweet corn oats, oat bran, muesli, all bran pumpernickel, soya and linseed, sourdough, rye baked beans, kidney beans, butter beans, soya beans, chick peas, lentils pasta, bulgur wheat, barley Dairy Foods milk, yoghurt, custard ice cream Snack foods nuts, oatcakes, chocolate Medium (55-70) melon, pineapple, figs, raisins, banana (ripe) new potatoes, beetroot Weetabix, Shredded Wheat granary, chapatti, pitta basmati rice, gnocchi, couscous rye crackers, digestive biscuits watermelon High (>70) baked potato, mashed potato (and instant), chips cornflakes, rice krispies, white, brown, bagels jasmine rice sugary drinks, jelly beans
18 From XPERT Carbohydrate Quiz
19 Oral Agents
20 What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight loss? Reduce CV risk Also reduce lipids and B.P.? Few/ no side effects Safe
21 Main classes of oral drugs available Biguanides (Metformin) Sulphonylureas (Gliclazide, Glimiperide, Glibencalmide etc) Thiozolendinediones (Pioglitazone) Glinides (Replaglinide, nataglinide) Alpha-glucosidase inhibitors (Acarbose) DDP-4 inhibitors or Gliptins (Sitagliptin, Saxagliptin,Linagliptin, Vildagliptin, Allogliptin) SGLT2 inhibitor agents (empagliflozin, cangligliflozin, dapagliflozin) Coming soon dual SGLT1/2 inhibitor agents
22 Metformin Is the basis for the oral treatment of most people type II diabetes Introduced in 1957, has a proven track record of efficacy and safety Lowers blood glucose with a low risk of hypoglycaemia with modest weight loss UK PDS suggest that it reduces cardiovascular events although subsequent studies less certain. Generally well-tolerated
23 Metformin mechanisms of action Metformin decreases hyperglycemia primarily by suppressing glucose production by the liver Mechanism of metformin is not completely understood Increases insulin sensitivity, enhances peripheral glucose uptake to muscle
24 Adverse effects of metformin Gastrointestinal intolerance Risk of acute kidney injury with other medications add x-ray contrast material Lactic acidosis with renal impairment Heart failure Liver disease Reduced TSH B12 deficiency
25 Sulphonylureas First generation drugs carbutamide, acetohexamide, chlorpropamide, and tolbutamide. Second generation drugs glipizide, gliclazide, glibenclamide, glyburide, glibornuride,gliquidone, glisoxepide, and glyclopyramide. Third generation drugs glimepiride
26 Sulphonylureas Increase insulin secretion through opening up a potassium channel in islets cells Cause insulin release unrelated to blood glucose Are powerful glucose lowering agents in early type II diabetes but are less effective with longer duration diabetes Adverse effects are hypoglycaemia weight gain and there are concerns about increased risk of cardiovascular events Can accumulate in the elderly and should be used with caution
27 Glinides Repaglinide and Nataglinide Act in a similar manner to sulphonylureas but has shorter duration Excreted via GI Tract, so safe in renal impairment and elderly Hypoglycaemia do not combine with SU s Useful to control post meal glucose
28 Pioglitazone Effective No hypoglycaemia as monotherapy or with metformin Long duration of effectiveness Reduction in CVS events May help with NAFLD Weight gain Can cause osteoporosis Can precipitate heart failure due to fluid overload Ian Gallen 28


29 Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma glucose stimulates pancreatic β-cells to secrete insulin 1 Glucagon Insulin Glucagon Gastric emptying Plasma glucose inhibits glucagon secretion by pancreatic α-cells 1 PPG ❸ Gastric emptying Delaying and/or slowing gastric emptying is a major determinant postprandial glycaemic excursion 2 of Hepatic glucose output + Glucose uptake PPG = postprandial glucose 1 DeFronzo RA. Med Clin North Am 2004;88: Horowitz M et al. Diabet Med 2002;19:177-94
30 DPP4 inhibitors Increases GLP-1, hence increase insulin secretion with hyperglycaemia Glucose lowering effect limited Some weight gain but reduced risk of hypoglycaemia Very well tolerated Concerns about heart failure with Saxogliptin and Alogliptin
31 GLP-1 agonists
32 Actions of GLP-1 agonists Promote 1 st phase insulin secretion Reduce glucagon release Delay gastric emptying Weak satiety effect Thus lowering blood glucose with modest weight loss without hypoglycaemia
33 Choice of GLP-1 receptor agonist: short acting versus long acting The pharmacological profile and half-life of a GLP-1 receptor agonist influences its effects on postprandial and basal (fasting) glycaemia SHORT ACTING GLP-1 receptor agonists Lixisenatide OD, Exenatide BD or LONG ACTING GLP-1 receptor agonists Liraglutide OD, Exenatide/Dulaglutide QW Effect on FPG Effect on PPG Effect on FPG Effect on PPG FPG = fasting plasma glucose PPG = postprandial glucose Fineman MS et al. Diabetes Obes Metab 2012;14:675-88
34 GLP1 agonist and cost per month Lixisenatide 20mg od; Exenatide (10µg bd); Byduron; Liraglutide (1.2mg od); Liraglutide (1.8mg od); Dulaglutide (1.5mg) ; 73 pm IDegLira (50 dose daily);
35 When to use GLP1-agonists HbA1c>58 mmol/l +oral agents; Overweight. With metformin/pioglitizone/sglt2 inhibitors. Stop DPP4 and Sulphonylureas. Or with basal insulin; To avoid further weight gain. To reduce hypoglycaemia.
36 How to use GLP1-agonists With Oral Treatment; Use least expensive agent (lixisentatide). Continue with Metformin and/or Pioglitazone. Add SGLT2 inhibitor if post-prandial hyperglycaemia. Move from lixisenatide/exenatide to a Glutide; if nauseous or sub-optimal response. Transfer to biphasic insulin (Humulin M3); if no weight loss or improved glycaemic control. With OD human basal (Humulin I); with dose increasing by 10% alternate days to reduce FBG < 6mmol.

37 Filtered glucose load > 180 g/day Renal glucose re-absorption in patients with diabetes 1,2 SGLT2 ~ 90% SGLT1 ~ 10% When blood glucose increases above the renal threshold (~ 11 mmol/l), the capacity of the transporters is exceeded, resulting in urinary glucose excretion SGLT, sodium glucose cotransporter. 1. Adapted from: Gerich JE. Diabet Med. 2010;27: ; 2. Bakris GL, et al. Kidney Int. 2009;75;


38 Filtered glucose load > 180 g/day Urinary glucose excretion via SGLT2 inhibition 1 SGLT2 inhibitor SGLT1 SGLT2 inhibitors reduce glucose re-absorption in the proximal tubule, leading to urinary glucose excretion* and osmotic diuresis SGLT, sodium glucose cotransporter. *Loss of ~ 80 g of glucose per day = 240 cal/day. 1. Bakris GL, et al. Kidney Int. 2009;75;
39 Across all studies and empagliflozin Improves Glycaemic control Reduction of HbA1c as monotherapy or with Metformin, Pioglitazone and as part of triple therapy or with insulin Sustained weight loss Reduction in SBP and DBP Well tolerated Reduce death rates (RRR 32% in Empa-Reg)
40 NICE 2015 For adults with type 2 diabetes managed either by lifestyle and diet, or by lifestyle and diet combined with a single drug not associated with hypoglycaemia, support the person to aim for an HbA1c level of 48 mmol/mol (6.5%). For adults on a drug associated with hypoglycaemia, support the person to aim for an HbA1c level of 53 mmol/mol (7.0%).
41 NICE 2015 In adults with type 2 diabetes, if HbA1c levels are not adequately controlled by a single drug and rise to 58 mmol/mol (7.5%) or higher: reinforce advice about diet, lifestyle and adherence to drug treatment and support the person to aim for an HbA1c level of 53 mmol/mol (7.0%) and intensify drug treatment.
42 What information would you consider when choosing oral therapies? HbA1c BMI egfr Age Current therapy Ethnicity Occupation
43 Medication selection for type 2 patients under 75 years of age BMI < 25 BMI BMI > 30 Metformin for all if tolerated bigger effect in higher BMI DPP4 (gliptin) OR Gliclazide (not with DPP4) DPP4 weaker agent SGLT2 (Empagliflozin) + / - Pioglitazone + / - DPP4 (gliptin) SGLT2 (Empagliflozin) + / - GLP1 (Lixisenatide/Trulicity) + / - Pioglitazone Consider insulin start
44 Insulin Workshop Profiles and Devices



45 Injection Sites Sites should always be inspected prior to injecting Avoid injecting into areas of lipohypertrophy Hands should be washed prior to injecting Use of alcohol swabs are not required
46 Storage and Suspension Store unopened insulin supplies in the fridge Opened insulin can be kept at room temperature for 28 days Cloudy insulins need suspending and this is done by rocking and rolling until the crystals go back into the solution and the solution looks milky white

47 Insulin re-suspension For all insulin preparations that contain human insulin or are an analogue mixture insulin to ensure uniform distribution Recommend to re-suspend use rock and roll technique Inappropriate re-suspension will negatively impact glycaemic control.

48 Needle length Gibney and colleagues recently published data about calculated injection tissue depth with 90 degree insertion and no skin fold from 1208 paired tests. Needle length % of subcutaneous injections 4mm 99.5% 5mm >98% 6mm >94% 8mm >84% 12.7mm 45%

49 Injection technique Air shot Dart like action Leave the needle in the skin for at least 10 seconds after plunger fully depressed Dispose of needle safely immediately after use instead of leaving attached to pen. Prevents entry of air Prevents leakage of medication Needles should only be used once

50 Lipohypertrophy Thickened rubbery lesions Long term insulin use Re using needles Poor rotation of injection sites
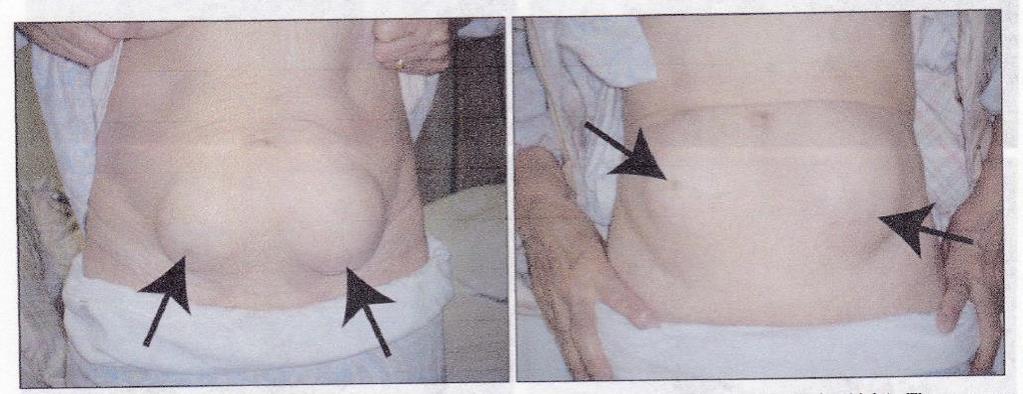
51
52 Lipohypertrophy Indicators: Fluctuating blood glucose levels Recurrent hyperglycaemia Unpredictable hypoglycaemia High HbA1c National recommendations: Do not inject into areas with lipohypertrophy Sites checked yearly, ideally every 2-3 months, especially if lipo present Patients should be taught to inspect their own sites and how to detect for lipohypertrophy
53 Painful injections Keep insulin at room temperature. Use shorter needles. Always use new needle. Insert the needle in a quick dart like action Massaging the injection site is not recommended and may speed up absorption. Needles will on occasions hit a blood vessel and cause bleeding or bruising this does not appear to have any adverse affect on absorption, but if occurs frequency patients injection technique may need to be reassessed
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
University College Hospital. What is the Glycaemic Index?
 University College Hospital What is the Glycaemic Index? Children and Young People s Diabetes Service The glycaemic index (GI) is a guide to how quickly or slowly carbohydrate foods affect blood glucose
University College Hospital What is the Glycaemic Index? Children and Young People s Diabetes Service The glycaemic index (GI) is a guide to how quickly or slowly carbohydrate foods affect blood glucose
MANAGEMENT OF TYPE 2 DIABETES
 MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
The Glycaemic Index. Nutrition & Dietetics Department. Patient information leaflet
 The Glycaemic Index Nutrition & Dietetics Department Patient information leaflet Who is this leaflet for and what does it cover? This leaflet tells you about the glycaemic index and how to practically
The Glycaemic Index Nutrition & Dietetics Department Patient information leaflet Who is this leaflet for and what does it cover? This leaflet tells you about the glycaemic index and how to practically
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Healthy Eating with Gestational Diabetes
 Healthy Eating with Gestational Diabetes What is gestational diabetes? Gestational diabetes is the name given to diabetes that can occur during pregnancy (Gestation). Diabetes is an inability of the body
Healthy Eating with Gestational Diabetes What is gestational diabetes? Gestational diabetes is the name given to diabetes that can occur during pregnancy (Gestation). Diabetes is an inability of the body
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
GLP-1 Receptor Agonists and SGLT-2 Inhibitors. Debbie Hicks
 GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
Glycemic Index. Mean Incremental Blood Glucose Responses in Healthy Subjects (65-70 years) Time (Minutes)
 Time (Minutes)") Glycemic Index How to use the glycemic index By making careful food choices, you can influence your hunger and energy as well as blood sugar levels, cholesterol and triglyceride levels. If you have problems
Glycemic Index How to use the glycemic index By making careful food choices, you can influence your hunger and energy as well as blood sugar levels, cholesterol and triglyceride levels. If you have problems
Pharmacological Glycaemic Control in Type 2 Diabetes
 Pharmacological Glycaemic Control in Type 2 Diabetes Aim(s) and Objective(s) This guideline aims to offer advice on the pharmacological management for those who require measures beyond diet and exercise
Pharmacological Glycaemic Control in Type 2 Diabetes Aim(s) and Objective(s) This guideline aims to offer advice on the pharmacological management for those who require measures beyond diet and exercise
The Glycaemic Index. Information for you
 The Glycaemic Index Information for you Follow us on Twitter @NHSaaa Find us on Facebook at www.facebook.com/nhsaaa Visit our website: www.nhsaaa.net All our publications are available in other formats
The Glycaemic Index Information for you Follow us on Twitter @NHSaaa Find us on Facebook at www.facebook.com/nhsaaa Visit our website: www.nhsaaa.net All our publications are available in other formats
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
SAMPLE. Course introduction. Understanding the Care and Management of Diabetes
 Understanding the Care and Management of Diabetes Course introduction About the NCFE Level 2 Certificate in Understanding the Care and Management of Diabetes Approximately 366 million people worldwide
Understanding the Care and Management of Diabetes Course introduction About the NCFE Level 2 Certificate in Understanding the Care and Management of Diabetes Approximately 366 million people worldwide
Weight Resistance Diet
 Weight Resistance Diet Weight Resistance diet is considered as Low Glycemic Index (GI) and Glycemic Load (GL) Diet. Glycemic index (GI) and glycemic load (GL) offer information about how foods affect blood
Weight Resistance Diet Weight Resistance diet is considered as Low Glycemic Index (GI) and Glycemic Load (GL) Diet. Glycemic index (GI) and glycemic load (GL) offer information about how foods affect blood
Week 6: Selecting Whole Carbohydrates over Refined Carbohydrates
 Week 6: Selecting Whole Carbohydrates over Refined Carbohydrates Purpose The purpose of this chapter is to understand the difference between refined and whole carbohydrates, and give you guidance on how
Week 6: Selecting Whole Carbohydrates over Refined Carbohydrates Purpose The purpose of this chapter is to understand the difference between refined and whole carbohydrates, and give you guidance on how
Dietary Advice for Diabetes in Adults
 1 Dietary Advice for Diabetes in Adults 2 What is diabetes? Diabetes is the name used to describe a metabolic condition of having higher than normal blood glucose (sugar) levels. In people with diabetes
1 Dietary Advice for Diabetes in Adults 2 What is diabetes? Diabetes is the name used to describe a metabolic condition of having higher than normal blood glucose (sugar) levels. In people with diabetes
PLEASE CHECK FULL SPECIFIC PRODUCT CHARACTERISTICS FOR MORE DETAILED AND CURRENT INFORMATION:
 Metformin Standard tablets Modified-release tablets Metformin 1g sachets Metformin liquid 500mg/5ml (avoid use as expensive) < 2.00 5.32 for 56 tabs 500mg 13.16 for 60 sachets > 120 Ketoacidosis General
Metformin Standard tablets Modified-release tablets Metformin 1g sachets Metformin liquid 500mg/5ml (avoid use as expensive) < 2.00 5.32 for 56 tabs 500mg 13.16 for 60 sachets > 120 Ketoacidosis General
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Glycemic Load & Glycemic Index
 Load & Index When food is consumed it is converted to fuel for our bodies. One type of fuel is glucose and different foods impact blood glucose levels differently. A driver of this is the amount and type
Load & Index When food is consumed it is converted to fuel for our bodies. One type of fuel is glucose and different foods impact blood glucose levels differently. A driver of this is the amount and type
Nutrition and Health. Glycaemic Index
 Nutrition and Health Glycaemic Index Topics What is Glycaemic Index? Studies of Glycaemic Index Effects of High and Low Glycaemic Index Foods Examples of High and Low Glycaemic Index Foods Factors Affecting
Nutrition and Health Glycaemic Index Topics What is Glycaemic Index? Studies of Glycaemic Index Effects of High and Low Glycaemic Index Foods Examples of High and Low Glycaemic Index Foods Factors Affecting
Should Psychiatrists be diagnosing (and treating) metabolic syndrome
 metabolic syndrome") Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Thus, there are three consequences of eating high GI meals that directly affect the ability to lose weight.
 When high GI foods make the body produce high levels of insulin in the blood stream, the body also releases substances that push fat circulating in the blood, into storage in fat cells. This means that
When high GI foods make the body produce high levels of insulin in the blood stream, the body also releases substances that push fat circulating in the blood, into storage in fat cells. This means that
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
How they work and when to take them. Diabetes Medications
 How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
Diabetes Mellitus case studies. Jana Vinklerová
 Diabetes Mellitus case studies Jana Vinklerová Definition of diabetes (metabolic disorder) Chronically raised blood glucose (hyperglycaemia) Insulin/Glucagon Insulin is responsible for lowering glucose
Diabetes Mellitus case studies Jana Vinklerová Definition of diabetes (metabolic disorder) Chronically raised blood glucose (hyperglycaemia) Insulin/Glucagon Insulin is responsible for lowering glucose
Mr Rab Burtun. Dr David Kim. 8:30-10:30 WS #2: Diabetes Basic 11:00-13:00 WS #9: Diabetes Basic (Repeated)
") Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
STEP 3: Add or Substitute with one of
 Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
University Hospitals of Leicester NHS Trust. Carbohydrates. A guide to carbohydrate containing foods for people with diabetes
 University Hospitals of Leicester NHS Trust Carbohydrates A guide to carbohydrate containing foods for people with diabetes A Healthy Diet This information is designed to help you to understand how carbohydrates
University Hospitals of Leicester NHS Trust Carbohydrates A guide to carbohydrate containing foods for people with diabetes A Healthy Diet This information is designed to help you to understand how carbohydrates
There have been important changes in diabetes care which may not be covered in undergraduate textbooks.
 Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
Carbohydrate Awareness
 Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Carbohydrate Awareness Nutrition and Dietetics Who is this leaflet for? This leaflet is for you if you want to improve your
Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Carbohydrate Awareness Nutrition and Dietetics Who is this leaflet for? This leaflet is for you if you want to improve your
February 2016 DIABETES PHARMACY TEAMS MAKE A DIFFERENCE. Why am I here? Why are you here? Identifying people at risk. What can we do?
 DIABETES PHARMACY TEAMS MAKE A DIFFERENCE Sallianne Kavanagh MRPharmS, MSc, IP Lead Pharmacist Diabetes and Endocrinology Sheffield Teaching Hospitals UKCPA Joint Chair Diabetes and Endocrinology Why am
DIABETES PHARMACY TEAMS MAKE A DIFFERENCE Sallianne Kavanagh MRPharmS, MSc, IP Lead Pharmacist Diabetes and Endocrinology Sheffield Teaching Hospitals UKCPA Joint Chair Diabetes and Endocrinology Why am
Starch in western diets
 Starches How much do we eat? Where does it come from? Characteristics of starch Starch digestion - rate and extent Starch gelatinisation Glycaemic index of starchy foods Resistant starch Conclusions Starch
Starches How much do we eat? Where does it come from? Characteristics of starch Starch digestion - rate and extent Starch gelatinisation Glycaemic index of starchy foods Resistant starch Conclusions Starch
Not All Carbs are Equal: Understanding the Glycemic Index Anna Chetrick, MS, RD, CDE
 Not All Carbs are Equal: Understanding the Glycemic Index Anna Chetrick, MS, RD, CDE March 10, 2018 Let s start with the basics 62 grams carb Carb ratio = 8 Insulin dose = ~8 units BG should be under 180
Not All Carbs are Equal: Understanding the Glycemic Index Anna Chetrick, MS, RD, CDE March 10, 2018 Let s start with the basics 62 grams carb Carb ratio = 8 Insulin dose = ~8 units BG should be under 180
Carbohydrate Counting
 Carbohydrate Counting What is carbohydrate counting? All the food you eat is made up of carbohydrate, protein and fat or a mixture of these. The part that makes the biggest difference to you blood glucose
Carbohydrate Counting What is carbohydrate counting? All the food you eat is made up of carbohydrate, protein and fat or a mixture of these. The part that makes the biggest difference to you blood glucose
Ertugliflozin (Steglatro ) 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy
 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy") Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
The glycaemic index (GI) and slowly absorbed carbohydrate foods
 and slowly absorbed carbohydrate foods") i If you need your information in another language or medium (audio, large print, etc) please contact Customer Care on 0800 374 208 or send an email to: customercare@ salisbury.nhs.uk You are entitled
i If you need your information in another language or medium (audio, large print, etc) please contact Customer Care on 0800 374 208 or send an email to: customercare@ salisbury.nhs.uk You are entitled
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY
 667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
NHS GREATER GLASGOW AND CLYDE BOWEL SCREENING PROGRAMME. Clinical Policy Guidelines
 NHS GREATER GLASGOW AND CLYDE BOWEL SCREENING PROGRAMME Clinical Policy Guidelines Management of patients with diabetes undergoing colonoscopy procedure following positive FOB test Date approved: 25 April
NHS GREATER GLASGOW AND CLYDE BOWEL SCREENING PROGRAMME Clinical Policy Guidelines Management of patients with diabetes undergoing colonoscopy procedure following positive FOB test Date approved: 25 April
Dr Tahseen A. Chowdhury Royal London Hospital. New Guidelines in Diabetes: NICE or Nasty?
 Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Diet and reactive hypoglycaemia
 Diet and reactive hypoglycaemia Nutrition and Dietetics Patient Information Leaflet Introduction This leaflet is for people who have a condition called reactive hypoglycaemia. It gives information on what
Diet and reactive hypoglycaemia Nutrition and Dietetics Patient Information Leaflet Introduction This leaflet is for people who have a condition called reactive hypoglycaemia. It gives information on what
Type 2 Diabetes. Stopping Smoking. Consider referral to smoking cessation. Consider referring for weight management advice.
 Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Diet advice for gestational diabetes
 Diet advice for gestational diabetes Background Gestational diabetes is a type of diabetes that develops during pregnancy and usually goes away after giving birth. It commonly occurs in the second or third
Diet advice for gestational diabetes Background Gestational diabetes is a type of diabetes that develops during pregnancy and usually goes away after giving birth. It commonly occurs in the second or third
National Institute for Health and Care Excellence. Single Technology Appraisal (STA) Empagliflozin combination therapy for treating type 2 diabetes
 Empagliflozin combination therapy for treating type 2 diabetes") National Institute for Health and Care Excellence Comment 1: the draft remit Single Technology Appraisal (STA) Empagliflozin combination therapy for treating type 2 diabetes Response to consultee and commentator
National Institute for Health and Care Excellence Comment 1: the draft remit Single Technology Appraisal (STA) Empagliflozin combination therapy for treating type 2 diabetes Response to consultee and commentator
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Hypoglyceamia and Exercise
 Hypoglyceamia and Exercise Noreen Barker Diabetes Specialist Nurse May 2016 Hypoglyceamia What is a hypo? Why are we concerned? Signs and symptoms Treatments Causes Hypo unawareness Managing diabetes and
Hypoglyceamia and Exercise Noreen Barker Diabetes Specialist Nurse May 2016 Hypoglyceamia What is a hypo? Why are we concerned? Signs and symptoms Treatments Causes Hypo unawareness Managing diabetes and
Pre-diabetes. Pharmacological Approaches to Delay Progression to Diabetes
 Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Activity #5: The Glycemic Index
 Activity #5: The Glycemic Index Cristina shares with her grandmother the information she has learned about reading nutrition labels and checking the total amount of sugar and fiber per serving. She is
Activity #5: The Glycemic Index Cristina shares with her grandmother the information she has learned about reading nutrition labels and checking the total amount of sugar and fiber per serving. She is
BI 199 Discussion 6 I. Announcements
 BI 199 Discussion 6 I. Announcements Outline comment status? Nutrition reports w/answers to questions submitted by e-mail by Wednesday. lombardi@uoregon.edu Please use requested format. Q? II. National
BI 199 Discussion 6 I. Announcements Outline comment status? Nutrition reports w/answers to questions submitted by e-mail by Wednesday. lombardi@uoregon.edu Please use requested format. Q? II. National
Diet. To equip people affected by CFS / ME with the skills for self-management towards a better quality of life. Version 1 January 2018
 Diet To equip people affected by CFS / ME with the skills for self-management towards a better quality of life. Version 1 January 2018 Review January 2019 1 P a g e Contents Diet and CFS/ME... 3 How often
Diet To equip people affected by CFS / ME with the skills for self-management towards a better quality of life. Version 1 January 2018 Review January 2019 1 P a g e Contents Diet and CFS/ME... 3 How often
PERIOPERATIVE DIABETES GUIDELINE
 PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
Diabetes. Diabetes in Balance
 Diabetes Introduction to Diabetes If you are living with type 2 diabetes, it is important that your lifestyle has the right balance between the appropriate treatment, regular exercise and a healthy diet.
Diabetes Introduction to Diabetes If you are living with type 2 diabetes, it is important that your lifestyle has the right balance between the appropriate treatment, regular exercise and a healthy diet.
Diet & Diabetes. Cassie Ricchiuti Diabetes Dietitian. Lives In Our Communities. Improving
 Diet & Diabetes Cassie Ricchiuti Diabetes Dietitian Improving www.shropscommunityhealth.nhs.uk Lives In Our Communities www.shropscommunityhealth.nhs.uk Dietary management of diabetes Type 1 Consistent
Diet & Diabetes Cassie Ricchiuti Diabetes Dietitian Improving www.shropscommunityhealth.nhs.uk Lives In Our Communities www.shropscommunityhealth.nhs.uk Dietary management of diabetes Type 1 Consistent
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
DIABETES IN CARE HOMES Dr J Stephenson. NHS England - Yorkshire and the Humber Strategic Clinical Networks
 DIABETES IN CARE HOMES 14.5.15 Dr J Stephenson NHS England - Yorkshire and the Humber Strategic Clinical Networks Dr Jenny Stephenson Diabetes Lead for Primary Care, Sheffield GP, Stannington and Walkley
DIABETES IN CARE HOMES 14.5.15 Dr J Stephenson NHS England - Yorkshire and the Humber Strategic Clinical Networks Dr Jenny Stephenson Diabetes Lead for Primary Care, Sheffield GP, Stannington and Walkley
Diabetes in the UK: Update on Diabetes Treatment and Care. Why is diabetes increasing? Obesity Increased waist circumference.
 Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Diabetes and stroke. What is the link between diabetes and stroke? What is diabetes? What are the symptoms of diabetes?
 Call the Stroke Helpline: 0303 3033 100 or email: info@stroke.org.uk Diabetes and stroke Diabetes is a lifelong condition that occurs when your body cannot regulate the amount of sugar in your blood. If
Call the Stroke Helpline: 0303 3033 100 or email: info@stroke.org.uk Diabetes and stroke Diabetes is a lifelong condition that occurs when your body cannot regulate the amount of sugar in your blood. If
Guideline for antihyperglycaemic therapy in adults with type 2 diabetes
 Guideline for antihyperglycaemic therapy in adults with type 2 diabetes Version Control Version Number Date Amendments made 1 January 2018 1.1 February 2018 Amended to reflect updated SPC advice for sitagliptin
Guideline for antihyperglycaemic therapy in adults with type 2 diabetes Version Control Version Number Date Amendments made 1 January 2018 1.1 February 2018 Amended to reflect updated SPC advice for sitagliptin
Understanding gestational diabetes
 Understanding gestational diabetes Gestational diabetes is a form of diabetes that occurs in women during pregnancy. About 12 14% of pregnant women will develop gestational diabetes, usually around the
Understanding gestational diabetes Gestational diabetes is a form of diabetes that occurs in women during pregnancy. About 12 14% of pregnant women will develop gestational diabetes, usually around the
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes. April 2010
 Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Arrange 3 Monthly Review Re-enforce LIFESTYLE advice and check DRUG COMPLIANCE at each visit Target HbA1c < 53mmol/mol
 Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Initiating Injectables in Type 2 Diabetes. Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital
 Initiating Injectables in Type 2 Diabetes Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital Increasing levels in delivery of diabetes care Complex Care support 3 3.1 People with diabetes
Initiating Injectables in Type 2 Diabetes Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital Increasing levels in delivery of diabetes care Complex Care support 3 3.1 People with diabetes
Dr A Pokrajac MD MSc MRCP Consultant
 Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Diabetes mellitus. Treatment
 Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
Glycemic index and glycemic load for 100+ foods
 Glycemic index and glycemic load for 100+ foods Measuring carbohydrate effects can help glucose management in controlling weight and starving cancer. The glycemic index is a value assigned to foods based
Glycemic index and glycemic load for 100+ foods Measuring carbohydrate effects can help glucose management in controlling weight and starving cancer. The glycemic index is a value assigned to foods based
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens
 PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens") EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
Mediterranean Diet. The word Mediterranean refers to the origins of the diet, rather than to specific foods such as Greek or Italian foods.
 Mediterranean Diet http://patient.info/health/mediterranean-diet The Mediterranean Diet is rich in vegetables, fruit, peas and beans (legumes) and grains. It also contains moderate amounts of chicken and
Mediterranean Diet http://patient.info/health/mediterranean-diet The Mediterranean Diet is rich in vegetables, fruit, peas and beans (legumes) and grains. It also contains moderate amounts of chicken and
INJECTABLE THERAPIES IN DIABETES. Barbara Ann McKee Diabetes Specialist Nurse
 INJECTABLE THERAPIES IN DIABETES Barbara Ann McKee Diabetes Specialist Nurse 1 Aims of the session Describe the different injectable agents for diabetes and when they would be used. Describe some common
INJECTABLE THERAPIES IN DIABETES Barbara Ann McKee Diabetes Specialist Nurse 1 Aims of the session Describe the different injectable agents for diabetes and when they would be used. Describe some common
What to eat when you have Short Bowel Syndrome
 What to eat when you have Short Bowel Syndrome What is Short Bowel Syndrome? Your bowel is an organ, shaped like a long tube, and is made up of the small and large bowel. The small bowel is about 15 to
What to eat when you have Short Bowel Syndrome What is Short Bowel Syndrome? Your bowel is an organ, shaped like a long tube, and is made up of the small and large bowel. The small bowel is about 15 to
Carbohydrates and diabetes. Information for patients Sheffield Dietetics
 Carbohydrates and diabetes Information for patients Sheffield Dietetics There are many things that can affect your blood glucose levels. These include what you eat, activity, stress, illness, alcohol and
Carbohydrates and diabetes Information for patients Sheffield Dietetics There are many things that can affect your blood glucose levels. These include what you eat, activity, stress, illness, alcohol and
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes: eating well with diabetes
 Diabetes: eating well with diabetes A healthy lifestyle, including recommended food choices is important to keep you well. A healthy diet for people with diabetes is the same as that recommended for everyone.
Diabetes: eating well with diabetes A healthy lifestyle, including recommended food choices is important to keep you well. A healthy diet for people with diabetes is the same as that recommended for everyone.
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Update on Pharmacological Management in Type 2 Diabetes
 Update on Pharmacological Management in Type 2 Diabetes Prof. Lotfy Hamed Abo Dahab Professor Of Internal Medicine and Cardiology Vice President of Sohag University ١ My AGENDA Targets For Glycaemic Control
Update on Pharmacological Management in Type 2 Diabetes Prof. Lotfy Hamed Abo Dahab Professor Of Internal Medicine and Cardiology Vice President of Sohag University ١ My AGENDA Targets For Glycaemic Control
Your Guide to. Healthy Eating for Managing Diabetes
 Your Guide to Healthy Eating for Managing Diabetes What is diabetes? A condition when the blood glucose level is higher than normal as described below. Stomach Bloodstream Pancreas 3 1 4 2 1. Food is broken
Your Guide to Healthy Eating for Managing Diabetes What is diabetes? A condition when the blood glucose level is higher than normal as described below. Stomach Bloodstream Pancreas 3 1 4 2 1. Food is broken
CARBOHYDRATES AND DIABETES. Brenda Davis, RD
 CARBOHYDRATES AND DIABETES Brenda Davis, RD Why are Carbohydrates Needed? Primary source of fuel for all body cells Proper functioning of central nervous system, kidneys, brain, and muscles Maintenance
CARBOHYDRATES AND DIABETES Brenda Davis, RD Why are Carbohydrates Needed? Primary source of fuel for all body cells Proper functioning of central nervous system, kidneys, brain, and muscles Maintenance
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION
 SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
Oral Treatments for Type 2 Diabetes. Prescribing Support Pharmacist
 Oral Treatments for Type 2 Diabetes Prescribing Support Pharmacist Learning Outcomes Familiar with classes of oral hypoglycaemic agents (OHAs) used in controlling blood glucose levels When to use each
Oral Treatments for Type 2 Diabetes Prescribing Support Pharmacist Learning Outcomes Familiar with classes of oral hypoglycaemic agents (OHAs) used in controlling blood glucose levels When to use each
Dietary advice for people with colostomies
 Dietary advice for people with colostomies Introduction During your surgery, you have had a colostomy formed. Colostomies are formed due to problems in the colon (large bowel). This leaflet is designed
Dietary advice for people with colostomies Introduction During your surgery, you have had a colostomy formed. Colostomies are formed due to problems in the colon (large bowel). This leaflet is designed
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Diabetes and stroke. What is diabetes? What are the symptoms of diabetes? Stroke Helpline: Website: stroke.org.uk
 Stroke Helpline: 0303 3033 100 Website: stroke.org.uk Diabetes is a condition caused by too much sugar in your blood. There are over three million people in the UK who have diabetes. If it s not controlled
Stroke Helpline: 0303 3033 100 Website: stroke.org.uk Diabetes is a condition caused by too much sugar in your blood. There are over three million people in the UK who have diabetes. If it s not controlled
Ready, Set, Start Counting!
 Ready, Set, Start Counting! Carbohydrate Counting a Tool to Help Manage Your Blood Glucose When you have diabetes, keeping your blood glucose in a healthy range can help you feel your best today and in
Ready, Set, Start Counting! Carbohydrate Counting a Tool to Help Manage Your Blood Glucose When you have diabetes, keeping your blood glucose in a healthy range can help you feel your best today and in
Oral Treatments. SaminaAli Prescribing Support Pharmacist
 Oral Treatments for Type 2 Diabetes SaminaAli Prescribing Support Pharmacist Learning Outcomes National Guidance Familiar with classes of oral hypoglycaemic agents (OHAs) used in controlling blood glucose
Oral Treatments for Type 2 Diabetes SaminaAli Prescribing Support Pharmacist Learning Outcomes National Guidance Familiar with classes of oral hypoglycaemic agents (OHAs) used in controlling blood glucose