Oral Treatments for Type 2 Diabetes. Prescribing Support Pharmacist
|
|
|
- Meryl Griffith
- 6 years ago
- Views:
Transcription
1 Oral Treatments for Type 2 Diabetes Prescribing Support Pharmacist
2 Learning Outcomes Familiar with classes of oral hypoglycaemic agents (OHAs) used in controlling blood glucose levels When to use each class Advice for patients Monitor for side effects Brief overview of mechanism of action and evidence base of OHAs Clinical Guidelines
3 Take a moment to think.. You have been diagnosed with diabetes... You have been told you need to go on medication... WHAT WOULD YOU LIKE YOUR MEDICATION TO DO? WHAT WOULD BE YOUR CONCERNS?

4 A brief history of diabetes medication...
5 Type 2 Diabetes is a Progressive Disease: UKPDS1 Cross-sectional sectional median values Median A1C (%) Time From Randomisation (years) Conventional Treatment (n=1138) Intensive Treatment (n=2729) ADA action suggested ADA target
6 3 Add statin 2 Control BP 4 Add metformin 1 Lifestyle (exercise, diet, stop smoking) Let s give our diabetic patients a hand! 5 consider tight glucose control Don t t turn the hand around
7 Why is good glycaemic control important?
8 Where does controlling Blood Glucose fit into the picture? No arguments in favour of poor BG control Importantly data from RCTs, found no benefit and possible harm from tight BG control -target< 6.5mmol/l Achieving good BG control, while addressing lifestyle, BP, and lipids will prevent more complications, than a narrower approach focused on intensive BG control Individualise treatment Agree targets with patient
9 When would you start treatment?
10 NICE Hba1c rises to > 48mmol/mol on lifestyle start tx Target 48mmol/mol (6.5%)-on diet plus one drug not associated with hypoglycaemia If drug associated with hypos target 53mmol/mol 1 st intensification: HBA1C > 58mmol/mol (7.5%) Target 53mmol/mol (7%) 2nd intensification: HBA1C > 58mmol/mol, target 53mmol/mol
11 Legacy Effect Holman RR et al. 10 year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008: Oct 9; 359: 1577 In type 2 diabetes, early intervention with intensive glucose control has long-lasting effects still evident at 10+ years UKPDS Study randomly assigned to conventional tx or tight control (median HBA1C 7 ) (Metformin if overweight, su or insulin ) Differences in HBA1C disappeared 1yr after the trial. Macro-and microvascular benefits remained 10 years later
12 UKPDS: A 1% decrease in HbA 1c is associated with a reduction in complications HbA 1 C 1% 43 % 37 % 21 % Amputation or fatal peripheral blood vessel disease* Microvascular complications e.g. kidney disease and blindness * Deaths related to diabetes* 14 % Heart attack* * p< ** p= % Stroke** Stratton IM, et al. BMJ 2000; 321:
13 Individualise targets 45yr old male, young family, works, T2D 1 yr, takes metformin HBA1C 62mmol/mol Any comments on HBA1C and target? 80 year old male, T2D 10yr, takes metformin and gliclazide, HBA1C 48mmol/mol, any comments on HBA1C and target?
14
15 What would you use as first line treatment? WHY?
16 Metformin First line in combination with lifestyle Meformin mechanism of action: It helps to stop the liver producing new glucose It helps to overcome insulin resistance by making insulin carry glucose into muscle cells more effectively.
17 Benefits of Metformin Cardiovascular benefits UK Prospective Diabetes Study: Can cause weight loss Does not cause hypos Use in combination with any OHA On the market a long time Inexpensive
18 Contra-indications and cautions Avoid if Egfr < 30mls/min -Risk lactic acidosis (rare) Other conditions that increase risk of lactic acidosis Dehydration diarrhoea, NSAIDs, ACE, diuretics can all affect renal fn Iodinated contrast media can cause acute renal impairment, stop metformin for 48hours, renal fn checked... Avoid in severe liver disease
19 Advice for patients Gastro-intestinal problems are common. Occur more than 1 in 10 people Let us know. We can try and help! Minimise -start on a low dose and increase slowly take with food or after food, spread the dose take twice daily usually go away after a few days reducing the dose MR prep could be considered (non-formulary) Other side effects -taste disturbance, low Vit B 12
20 When to intensify treatment? If HbA1c is still <53mmol/mol or if individualised target is not met The addition of a second oral agent is likely to improve HbA1c by no more than mmol/mol Withdraw treatment after 6 months if HbA1c has decreased by less than 6mmol/mol
21 Case 1 Mr Smith is a 52 year old teacher. Mr Smith was diagnosed with Type 2 diabetes 2 years ago. He is a car driver. HbA1c last week was 70mmol/mol Weight is 80kg, height 5 8, BMI 31.8 Current medication: Metformin 500mg at a dose of 1g twice daily. What second line OHA would you choose?
22 Options -- A Add a sulphonylurea? B - Add pioglitazone? C Add Gliptin? D SGLT2?
23 NO WRONG ANSWER Remember to A Reinforce Lifestyle advice B -Add a statin
24 Sulphonylurea eg Gliclazide Can use 1st line if intolerant to metformin Can use in combination with all other OHAs Mechanism of action Stimulate pancreatic cells to make insulin. Reduction in hepatic glucose production Improvement in clearance of glucose.
25 Sulphonylureas Pros Confidence and experience in using Cheap (generic: 6 per month) Effective (mean 11mmol/mol reduction HbA1c) Minimal responder variability
26 Cons Significant hypoglycaemia risk BGM may be appropriate for 1 st three months Can t be used in severe renal /liver impairment or if breast feeding Weight gain Poor durability
27 What to advise the patient Take with meals -Regular meals are important Alcohol increased risk prolonged hypo Weight gain average 1 2 kg Hypo recognise, how to treat Blood Glucose Meter when to monitor? Driving important to career? Groups at increased risk of hypo elderly, mild renal or liver impairment
28 Pioglitazone Thiazolidinediones Second line therapy add to metformin Triple therapy - combination with other OHA Contra-indicated Heart failure Hepatic impairment History bladder cancer, uninvestigated haematurea Mechanism of action - Reduces insulin resistance
29 Pioglitazone -benefits Reduce insulin resistance unique mechanism of action and durable effect Proactive study -all cause mortality lower in Piogliazone group group (26.8% v 34.3%) Iris study -Pioglitazone may reduce CV events after a CVA
30 Pioglitazone adverse effects Fluid retention can precipitate heart failure Avoid in patients with a MI, angina,? Elderly Bone fractures increase in men and women > 50yrs Macular oedema report blurred vision Bladder cancer risk low however risk increased with length of treatment and higher dose Liver reports hepatic failure test lfts periodically
31 Pioglitazone Experience, low cost, CVD event reduction in PROactive Weight gain, fluid retention, fractures, uncertain safety (bladder cancer?)
32 Advice for Patient Once daily, can take at any time of day Report any fluid retention, blurred vision Increased risk weight gain and fractures Bladder cancer risk increased with duration and larger dose
33 Follow up? Check HBA1C -has there been a 6mmol/mol reduction? If not stop pioglitazone Consider alternative strategies
34 DPP4 Inhibitors -Mechanism DPP4 inhibitors (gliptins) Alogliptin, Linagliptin 1 st line in NHSGGC. Other available DDP4s include sitagliptin, vildagliptin & saxagliptin Second line therapy in combination with metformin Triple therapy in combination with other OHA
35
36 DPP-4 inhibitors -pros Very low hypo risk Weight neutral Low side-effect profile No major adverse cardiovascular outcomes / heart failure (apart from saxagliptin increased risk hospitalisation for heart failure esp if renal impairment)
37 DPP4 inhibitors Cons Expensive (around 30 per month) Less effective (mean 5mmol/mol reduction HbA1c) Responder variability No long term safety information Risk Pancreatitis small Adjust dose in renal impairment linagliptin most suitable in renal impairment
38 Advice for Patient Take at any time of the day Risk of hypo if on gliclazide or insulin Pancreatitis inform patients about the symptoms of pancreatitis (ie, severe, persistent abdominal pain sometimes radiating to the back) Seek medical advice if this is suspected. Advise patient to return for HbA1c review in 3-6 months and that drug will be stopped if no therapeutic response.
39 SGLT-2 Inhibitors Newest class of oral hypoglycaemic agent All on NHSGGC total formulary Canagliflozin (Ivokana ) Dapagliflozin (Forxiga ) Empagliflozin (Jardiance )
40 SGLT-2 inhibitors Dual therapy with metformin Triple therapy Mechanism of action inhibit SGLT2 protein sodium-glucose transport protein helps reabsorb glucose into blood in kidney. By blocking these proteins, less glucose reabsorbed & excess glucose is passed out in the urine
41 Benefits SGLTS Can help with weight loss Can be used at all stages of Type 2 Diabetes Low hypo incidence (risk if on SU or insulin) EMPA-REG OUTCOME Cardiovascular benefits Diabetic kidney disease reduced risk EMPA-REG OUTCOME the placebo group.
42 CV benefits EMPA-REG Patients studied -T2DM pts high CVD risk Empagliflozin 1y end point (CV death, nonfatal MI and stroke) by 14% driven by a 38% in CV mortality 35% in hospitalization for heart failure SGLT2 inhibitors -many metabolic benefits ( HbA 1c, body weight, BP and an HDL chol) CV benefits due to hemodynamic effects, - BP and in extracellular volume.
43 Cardiovascular Outcome Trials Empa-reg trial - published 2016 Evidence of improved CV outcomes with this drug, significantly lower rate of mortality Trial in patients with exisiting cardiovascular comorbidities CANVAS trial expected 2018 DECLARE trial expected 2019
44 SGLT2 renal benefits Empagliflozin group had a significantly lower risk of microvascular outcome events driven by a lower risk of progression of kidney disease. Empagliflozin group had a significantly lower risk of progression to macroalbuminuria More work needs to be done
45 SGLT2s -cons Increase frequency one extra voiding per day Increased risk infections eg thrush, utis Renal impairment don t start if Egfr < 60 Less effective in impaired renal fn Can cause acute renal failure monitor renal function before initiation, before initiation on other drugs which may reduce renal function and annually thereafter. DKA at near normal blood glucose levels Stop before surgery, sick day rules Caution elderly risk of volume depletion More adverse effects >75yrs
46 SGLT-2 inhibitors Hepatic and Renal Function
47 MHRA advice on SGLT-2 inhibitors and Ketoacidosis Serious, life-threatening, fatal cases of DKA reported Test ketones if signs DKA regardless of Glucose conc Risk factors identified include a low beta cell function reserve, off label use T1D Restricted food intake or severe dehydration Change in insulin requirements surgery alcohol abuse
48 MHRA advice on SGLT-2 inhibitors Advice for HCPs and Ketoacidosis Educate patients on symptoms of DKA and what to do if experiencing symptoms. Test for raised ketones in patients with ketoacidosis symptoms, even if plasma glucose levels are near-normal. Report suspected side effects to SGLT2 inhibitors or any other medicines on a Yellow Card
49 SGLT2 inhibitors Cost, genital fungal infections, risk of DKA, long term safety uncertain Weight loss, hypoglycaema rare, reduced CV events
50 SGLT2s Advice for patients Report any symptoms of DKA -rapid weight loss, feeling or being sick, stomach pain, fast and deep breathing, sleepiness, sweet smelling breath Increase urinary frequency Increased risk of infection Risk of hypo if on SU or insulin

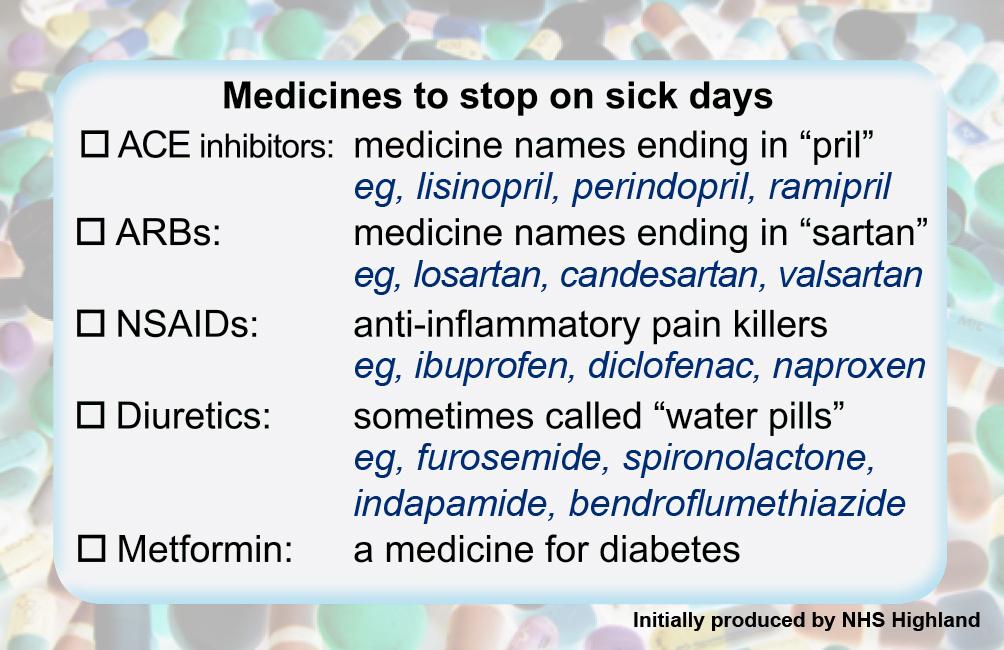
51 Sick Day Rules - SGLTs
52 Two Infrequently used Oral Type 2 Hypoglycaemic Drugs Alpha-Glucosidase Inhibitors (Acarbose) Meglitinides (Repaglinide & Nateglinide)
53 Acarbose (Glucobay ) alpha glucosidase inhibitors Acarbose GG&C Formulary restricted to patients who cant tolerate Metformin Acarbose -slows absorption of starchy foods from the intestine. blood glucose levels rise more slowly after meals. Acarbose should always be chewed with the first mouthful of foodor swallowed whole with a little liquid immediately before the meal. Main side-effects are flatulence and diarrhoea
54 Meglitinides (Repaglinide & Nateglinide) Like the sulphonylureas, these stimulate the cells in the pancreas to produce more insulin. However, unlike the sulphonylureas, they work very quickly but only last for a short time and are given within half an hour before each meal. If a meal is missed, the dose must be omitted. These tablets are taken up to three times daily. Not in GG&C Formulary
55 WHAT NEXT? Consider adding a third oral medication? Consider adding a injectable GPL1-agonist? Only if BMI >30kg/m2 Consider starting insulin therapy? Can cause weight gain and requires more intensive BGM
56

57 Unpicking Polypharmacy SCI Diabetes
58 First line Metformin In summary Second line individualise therapy Review efficacy of drug treatment Stop treatment if ineffective Targets treat aggressively when first diagnosed Consider patient when setting targets
59 Taken from GG&C Diabetes Guideline available from
60 Taken from GG&C Diabetes Guideline available from
61 GGC Formulary Clinical guidelines SMC Advice /Advice_Directory/SMC_Advice_Directory
62 References GG&C Diabetes Guideline Available at: SIGN 116 March 2010 Available at: Nice NG28 Dec 2015 Available at: BNF 69 Sept 2015 Available at: The Scottish Medicines Consortium Available at: www. Diabetes and Driving: Available at:
63 Case 1 Mr Smith is a 52 year old teacher. Mr Smith was diagnosed with Type 2 diabetes 2 years ago. He is a car driver. HbA1c last week was 70mmol/mol Weight is 80kg, height 5 8, BMI 31.8 Current medication: Metformin 500mg at a dose of 1g twice daily. What second line OHA would you choose?
64 Would you choose anything different now?
65 Case 2 Mr Mackie is a 54 year old male with Type 2 diabetes. He has been prescribed his current medications for the last 2 years and his HbA1c has increased to 64mmol/mol. Current Medication: Metformin 1000mg twice daily Mr Mackie has a history of hypertension, MI, BMI 29, U/Es and lfts normal. You are carrying out her annual diabetes review. What would you suggest when reviewing his current medication regimen?
66 Options -- A No change as well controlled B Start new OHA and review in 3-6 months A SU B Pioglitazone C -DPP4 inhibitor D -SGLT2
67 Case 3 Miss Carter is a 84 year old lady who has had Type 2 diabetes since she was 72. HBA1C 51mmol/mol, Egfr 40 Current Medication: Metformin 1g twice daily Gliclazide 160mg twice daily Sitaglipin 100mg daily What else would you want to know? Any suggested changes?
68 What to do with Miss Carter Review patients HbA1c risk of hypos? Altered hypo awareness Reduced appetite, weight loss Drive? Check blood glucose? Consider reduced renal function: Reduce dose of sitagliptin and metformin?
69 Any questions?
Oral Treatments. SaminaAli Prescribing Support Pharmacist
 Oral Treatments for Type 2 Diabetes SaminaAli Prescribing Support Pharmacist Learning Outcomes National Guidance Familiar with classes of oral hypoglycaemic agents (OHAs) used in controlling blood glucose
Oral Treatments for Type 2 Diabetes SaminaAli Prescribing Support Pharmacist Learning Outcomes National Guidance Familiar with classes of oral hypoglycaemic agents (OHAs) used in controlling blood glucose
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
MANAGEMENT OF TYPE 2 DIABETES
 MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Type 2 diabetes in adults: controlling your blood glucose by taking a second medicine what are your options?
 Patient decision aid Type 2 diabetes in adults: controlling your blood glucose by taking a second medicine what are your options? nice.org.uk/guidance/ng28 Published: December 2015 About this decision
Patient decision aid Type 2 diabetes in adults: controlling your blood glucose by taking a second medicine what are your options? nice.org.uk/guidance/ng28 Published: December 2015 About this decision
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
Type 2 Diabetes. Stopping Smoking. Consider referral to smoking cessation. Consider referring for weight management advice.
 Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Dr Tahseen A. Chowdhury Royal London Hospital. New Guidelines in Diabetes: NICE or Nasty?
 Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
STEP 3: Add or Substitute with one of
 Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Arrange 3 Monthly Review Re-enforce LIFESTYLE advice and check DRUG COMPLIANCE at each visit Target HbA1c < 53mmol/mol
 Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
PLEASE CHECK FULL SPECIFIC PRODUCT CHARACTERISTICS FOR MORE DETAILED AND CURRENT INFORMATION:
 Metformin Standard tablets Modified-release tablets Metformin 1g sachets Metformin liquid 500mg/5ml (avoid use as expensive) < 2.00 5.32 for 56 tabs 500mg 13.16 for 60 sachets > 120 Ketoacidosis General
Metformin Standard tablets Modified-release tablets Metformin 1g sachets Metformin liquid 500mg/5ml (avoid use as expensive) < 2.00 5.32 for 56 tabs 500mg 13.16 for 60 sachets > 120 Ketoacidosis General
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
Type 2 Diabetes Mellitus hypoglycaemic agents
 Type 2 Diabetes Mellitus hypoglycaemic agents Name Metformin Drug Name (eg brand name) Metformin (Diaformin Diabex) Cost / PBS per 28d mth $10.24 (1.5g dly) 1000mg+500mg / $4.44+$5.80 Concerns? Lactic
Type 2 Diabetes Mellitus hypoglycaemic agents Name Metformin Drug Name (eg brand name) Metformin (Diaformin Diabex) Cost / PBS per 28d mth $10.24 (1.5g dly) 1000mg+500mg / $4.44+$5.80 Concerns? Lactic
GLP-1 Receptor Agonists and SGLT-2 Inhibitors. Debbie Hicks
 GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
How they work and when to take them. Diabetes Medications
 How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
PATIENT INFORMATION LEAFLET MEDICINE TO TREAT: DIABETES
 PATIENT INFORMATION LEAFLET MEDICINE TO TREAT: DIABETES α-glucosidase inhibitor Biguanide DPP-IV inhibitor Meglitinide Sulphonylurea SGLT-2 Inhibitors 1. What are these medicines used for? These medicines
PATIENT INFORMATION LEAFLET MEDICINE TO TREAT: DIABETES α-glucosidase inhibitor Biguanide DPP-IV inhibitor Meglitinide Sulphonylurea SGLT-2 Inhibitors 1. What are these medicines used for? These medicines
Alia Gilani Health Inequalities Pharmacist
 Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study
 for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study") Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
Diabetes and New Meds for Cardiovascular Risk Reduction. F. Dwight Chrisman, MD, FACC. Disclosures: BI Boehringer Ingelheim speaker
 Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
SIOFOR mg film-coated tablets
 PACKAGE LEAFLET: INFORMATION FOR THE USER SIOFOR 850 850mg film-coated tablets METFORMIN HYDROCHLORIDE This leaflet is a copy of the Summary of Product Characteristics and Patient Information Leaflet for
PACKAGE LEAFLET: INFORMATION FOR THE USER SIOFOR 850 850mg film-coated tablets METFORMIN HYDROCHLORIDE This leaflet is a copy of the Summary of Product Characteristics and Patient Information Leaflet for
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Diabetes, Type 2 Management
 CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes. April 2010
 Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Mr Rab Burtun. Dr David Kim. 8:30-10:30 WS #2: Diabetes Basic 11:00-13:00 WS #9: Diabetes Basic (Repeated)
") Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Dr A Pokrajac MD MSc MRCP Consultant
 Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY?
 MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
Have you seen a patient like Elaine *?
 (linagliptin) 5mg tablets Have you seen a patient like Elaine *? *Hypothetical patient profile Elaine * : 60 years old Housewife *Hypothetical patient profile ELAINE*: T2D Patient with early signs of kidney
(linagliptin) 5mg tablets Have you seen a patient like Elaine *? *Hypothetical patient profile Elaine * : 60 years old Housewife *Hypothetical patient profile ELAINE*: T2D Patient with early signs of kidney
February 2016 DIABETES PHARMACY TEAMS MAKE A DIFFERENCE. Why am I here? Why are you here? Identifying people at risk. What can we do?
 DIABETES PHARMACY TEAMS MAKE A DIFFERENCE Sallianne Kavanagh MRPharmS, MSc, IP Lead Pharmacist Diabetes and Endocrinology Sheffield Teaching Hospitals UKCPA Joint Chair Diabetes and Endocrinology Why am
DIABETES PHARMACY TEAMS MAKE A DIFFERENCE Sallianne Kavanagh MRPharmS, MSc, IP Lead Pharmacist Diabetes and Endocrinology Sheffield Teaching Hospitals UKCPA Joint Chair Diabetes and Endocrinology Why am
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY
 667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
Diabetes in the UK: Update on Diabetes Treatment and Care. Why is diabetes increasing? Obesity Increased waist circumference.
 Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
SIGN 154 Pharmacological management of glycaemic control in people with type 2 diabetes. A national clinical guideline November 2017.
 SIGN 154 Pharmacological management of glycaemic control in people with type 2 diabetes A national clinical guideline November 2017 Evidence KEY TO EVIDENCE STATEMENTS AND RECOMMENDATIONS LEVELS OF EVIDENCE
SIGN 154 Pharmacological management of glycaemic control in people with type 2 diabetes A national clinical guideline November 2017 Evidence KEY TO EVIDENCE STATEMENTS AND RECOMMENDATIONS LEVELS OF EVIDENCE
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
SIOFOR mg film-coated tablets
 PACKAGE LEAFLET: INFORMATION FOR THE USER SIOFOR 1000 1000mg film-coated tablets For use in children from 10 years and adults METFORMIN HYDROCHLORIDE This leaflet is a copy of the Summary of Product Characteristics
PACKAGE LEAFLET: INFORMATION FOR THE USER SIOFOR 1000 1000mg film-coated tablets For use in children from 10 years and adults METFORMIN HYDROCHLORIDE This leaflet is a copy of the Summary of Product Characteristics
Summary of the risk management plan (RMP) for Synjardy (empagliflozin / metformin)
 for Synjardy (empagliflozin / metformin)") EMA/217413/2015 Summary of the risk management plan (RMP) for Synjardy (empagliflozin / metformin) This is a summary of the risk management plan (RMP) for Synjardy, which details the measures to be taken
EMA/217413/2015 Summary of the risk management plan (RMP) for Synjardy (empagliflozin / metformin) This is a summary of the risk management plan (RMP) for Synjardy, which details the measures to be taken
Bristol-Myers Squibb / AstraZeneca ADVICE dapagliflozin (Forxiga ) Indication under review: SMC restriction: Chairman, Scottish Medicines Consortium
 Indication under review: SMC restriction: Chairman, Scottish Medicines Consortium") Re-Submission dapagliflozin 5mg and 10mg film-coated tablets (Forxiga ) SMC No. (799/12) Bristol-Myers Squibb / AstraZeneca 07 February 2014 The Scottish Medicines Consortium (SMC) has completed its assessment
Re-Submission dapagliflozin 5mg and 10mg film-coated tablets (Forxiga ) SMC No. (799/12) Bristol-Myers Squibb / AstraZeneca 07 February 2014 The Scottish Medicines Consortium (SMC) has completed its assessment
dapagliflozin 5mg and 10mg film-coated tablets (Forxiga ) SMC No. (799/12) Bristol-Myers Squibb / AstraZeneca
 SMC No. (799/12) Bristol-Myers Squibb / AstraZeneca") dapagliflozin 5mg and 10mg film-coated tablets (Forxiga ) SMC No. (799/12) Bristol-Myers Squibb / AstraZeneca 07 September 2012 (Issued 07 December 2012) The Scottish Medicines Consortium (SMC) has completed
dapagliflozin 5mg and 10mg film-coated tablets (Forxiga ) SMC No. (799/12) Bristol-Myers Squibb / AstraZeneca 07 September 2012 (Issued 07 December 2012) The Scottish Medicines Consortium (SMC) has completed
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Have you seen a patient like Carol *?
 (linagliptin) 5mg tablets Have you seen a patient like Carol *? *Hypothetical patient profile Carol * : 70 years old Retired schoolteacher *Hypothetical patient profile CAROL*: T2D patient with moderate
(linagliptin) 5mg tablets Have you seen a patient like Carol *? *Hypothetical patient profile Carol * : 70 years old Retired schoolteacher *Hypothetical patient profile CAROL*: T2D patient with moderate
empagliflozin 10mg and 25mg tablet (Jardiance ) SMC No. (993/14) Boehringer Ingelheim / Eli Lilly
 SMC No. (993/14) Boehringer Ingelheim / Eli Lilly") empagliflozin 10mg and 25mg tablet (Jardiance ) SMC No. (993/14) Boehringer Ingelheim / Eli Lilly 05 September 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
empagliflozin 10mg and 25mg tablet (Jardiance ) SMC No. (993/14) Boehringer Ingelheim / Eli Lilly 05 September 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Volume 2; Number 14 September 2008 NICE CLINICAL GUIDELINE 66: TYPE 2 DIABETES THE MANAGEMENT OF TYPE 2 DIABETES (MAY 2008)
") Volume 2; Number 14 September 2008 NICE CLINICAL GUIDELINE 66: TYPE 2 DIABETES THE MANAGEMENT OF TYPE 2 DIABETES (MAY 2008) The purpose of this special edition of the PACE Bulletin is to summarize the
Volume 2; Number 14 September 2008 NICE CLINICAL GUIDELINE 66: TYPE 2 DIABETES THE MANAGEMENT OF TYPE 2 DIABETES (MAY 2008) The purpose of this special edition of the PACE Bulletin is to summarize the
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd
 SMC No. (1083/15) Merck Sharp and Dohme UK Ltd") sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd 07 August 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd 07 August 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Pharmacological Glycaemic Control in Type 2 Diabetes
 Pharmacological Glycaemic Control in Type 2 Diabetes Aim(s) and Objective(s) This guideline aims to offer advice on the pharmacological management for those who require measures beyond diet and exercise
Pharmacological Glycaemic Control in Type 2 Diabetes Aim(s) and Objective(s) This guideline aims to offer advice on the pharmacological management for those who require measures beyond diet and exercise
Guideline for antihyperglycaemic therapy in adults with type 2 diabetes
 Guideline for antihyperglycaemic therapy in adults with type 2 diabetes Version Control Version Number Date Amendments made 1 January 2018 1.1 February 2018 Amended to reflect updated SPC advice for sitagliptin
Guideline for antihyperglycaemic therapy in adults with type 2 diabetes Version Control Version Number Date Amendments made 1 January 2018 1.1 February 2018 Amended to reflect updated SPC advice for sitagliptin
Medicines Optimisation Team Standard Operating procedure for Alogliptin Audit:
 Medicines Optimisation Team Standard Operating procedure for Alogliptin Audit: To review type 2 diabetic patients prescribed dipedtidylpeptidase-4 (DPP-4) inhibitors (linagliptin (Trajenta, saxagliptin
Medicines Optimisation Team Standard Operating procedure for Alogliptin Audit: To review type 2 diabetic patients prescribed dipedtidylpeptidase-4 (DPP-4) inhibitors (linagliptin (Trajenta, saxagliptin
Summary of the risk management plan (RMP) for Ebymect (dapagliflozin / metformin)
 for Ebymect (dapagliflozin / metformin)") EMA/672415/2015 Summary of the risk management plan (RMP) for Ebymect (dapagliflozin / metformin) This is a summary of the risk management plan (RMP) for Ebymect, which details the measures to be taken
EMA/672415/2015 Summary of the risk management plan (RMP) for Ebymect (dapagliflozin / metformin) This is a summary of the risk management plan (RMP) for Ebymect, which details the measures to be taken
SGLT2 Inhibitors
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: SGLT2 Inhibitors Page: 1 of 7 Last Review Date: June 22, 2018 SGLT2 Inhibitors Description Invokana
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: SGLT2 Inhibitors Page: 1 of 7 Last Review Date: June 22, 2018 SGLT2 Inhibitors Description Invokana
Type 2 Diabetes Therapies and Management: An Educational Toolkit
 University Hospitals of Leicester, Department of Diabetes and Leicester Diabetes Centre: Type 2 Diabetes Therapies and Management: An Educational Toolkit Acknowledgements This document is designed to enable
University Hospitals of Leicester, Department of Diabetes and Leicester Diabetes Centre: Type 2 Diabetes Therapies and Management: An Educational Toolkit Acknowledgements This document is designed to enable
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital
 What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC
 MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Diabetes Update: Keeping patients safe. Victoria Ruszala MFRPSII North Bristol NHS Trust
 Diabetes Update: Keeping patients safe Victoria Ruszala MFRPSII North Bristol NHS Trust Declaration of Interests I have received funding from the following companies for providing education sessions, attending
Diabetes Update: Keeping patients safe Victoria Ruszala MFRPSII North Bristol NHS Trust Declaration of Interests I have received funding from the following companies for providing education sessions, attending
GUIDANCE UPDATE TYPE 2 DIABETES AN OVERVIEW OF THE SIGN GUIDELINE ON PHARMACOLOGICAL MANAGEMENT OF GLYCAEMIC CONTROL.
 TYPE 2 DIABETES AN OVERVIEW OF THE SIGN GUIDELINE ON PHARMACOLOGICAL MANAGEMENT OF GLYCAEMIC CONTROL GUIDANCE UPDATE cpd credits Production of this Guidelines supplement has been funded by an educational
TYPE 2 DIABETES AN OVERVIEW OF THE SIGN GUIDELINE ON PHARMACOLOGICAL MANAGEMENT OF GLYCAEMIC CONTROL GUIDANCE UPDATE cpd credits Production of this Guidelines supplement has been funded by an educational
DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes
 THERAPY REVIEW DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes STEVE CHAPLIN SPL DPP-4 inhibitors and SGLT2 inhibitors lower blood glucose by complementary mechanisms of action, and two fixeddose
THERAPY REVIEW DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes STEVE CHAPLIN SPL DPP-4 inhibitors and SGLT2 inhibitors lower blood glucose by complementary mechanisms of action, and two fixeddose
Should Psychiatrists be diagnosing (and treating) metabolic syndrome
 metabolic syndrome") Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
28-Aug-15. RACGP guidelines 2014/15. ADS guidelines Part 1 T2D Guidelines. Part 2 What comes after metformin?
 Part 1 T2D Guidelines Oral therapies in T2 diabetes Dr Gary Kilov T2D Guidelines - What s New? What comes after metformin? 1 RACGP guidelines 2014/15 ADA-EASD: Anti-Hyperglycaemic therapy 2015 3 4 Inzucchi
Part 1 T2D Guidelines Oral therapies in T2 diabetes Dr Gary Kilov T2D Guidelines - What s New? What comes after metformin? 1 RACGP guidelines 2014/15 ADA-EASD: Anti-Hyperglycaemic therapy 2015 3 4 Inzucchi
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date)
") Drug, Treatment, Device name ( Vipidia; Takeda) COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date) Licensed indication To improve glycaemic control in
Drug, Treatment, Device name ( Vipidia; Takeda) COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date) Licensed indication To improve glycaemic control in
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) Management of Type 2 Diabetes in adults
 Management of Type 2 Diabetes in adults") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) in adults Key messages: Education and lifestyle advice are fundamental to patient management, as is overall consideration to the patient s risk of macrovascular
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) in adults Key messages: Education and lifestyle advice are fundamental to patient management, as is overall consideration to the patient s risk of macrovascular
ERBP Guideline on management of diabetics with advanced CKD
 ERBP Guideline on management of diabetics with advanced CKD ERBP Mission improve the outcome of patients with kidney disease in a sustainable way, through enhancing the accessibility of knowledge on patient
ERBP Guideline on management of diabetics with advanced CKD ERBP Mission improve the outcome of patients with kidney disease in a sustainable way, through enhancing the accessibility of knowledge on patient
Hypoglyceamia and Exercise
 Hypoglyceamia and Exercise Noreen Barker Diabetes Specialist Nurse May 2016 Hypoglyceamia What is a hypo? Why are we concerned? Signs and symptoms Treatments Causes Hypo unawareness Managing diabetes and
Hypoglyceamia and Exercise Noreen Barker Diabetes Specialist Nurse May 2016 Hypoglyceamia What is a hypo? Why are we concerned? Signs and symptoms Treatments Causes Hypo unawareness Managing diabetes and
Diabetes Prescribing Guidelines for the Glycaemia management of Adults with Type 2 Diabetes
 Cannock Chase Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group East Staffordshire Clinical Commissioning
Cannock Chase Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group East Staffordshire Clinical Commissioning
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens
 PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens") EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
Glucose Control: non-insulin therapies*
 South frican Family Practice 2018; 60(1):4-14 Open ccess article distributed under the terms of the reative ommons License [ Y-N-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0 S fr Fam Pract
South frican Family Practice 2018; 60(1):4-14 Open ccess article distributed under the terms of the reative ommons License [ Y-N-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0 S fr Fam Pract
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
PACKAGE LEAFLET: INFORMATION FOR THE USER. Metformin HCl Bluefish 500 mg/ 850 mg/ 1000 mg, film-coated tablets metformin hydrochloride
 PACKAGE LEAFLET: INFORMATION FOR THE USER Metformin HCl Bluefish 500 mg/ 850 mg/ 1000 mg, film-coated tablets metformin hydrochloride Read all of this leaflet carefully before you start taking this medicine
PACKAGE LEAFLET: INFORMATION FOR THE USER Metformin HCl Bluefish 500 mg/ 850 mg/ 1000 mg, film-coated tablets metformin hydrochloride Read all of this leaflet carefully before you start taking this medicine
Diabetes and stroke. What is the link between diabetes and stroke? What is diabetes? What are the symptoms of diabetes?
 Call the Stroke Helpline: 0303 3033 100 or email: info@stroke.org.uk Diabetes and stroke Diabetes is a lifelong condition that occurs when your body cannot regulate the amount of sugar in your blood. If
Call the Stroke Helpline: 0303 3033 100 or email: info@stroke.org.uk Diabetes and stroke Diabetes is a lifelong condition that occurs when your body cannot regulate the amount of sugar in your blood. If
Glucophage XR is contra-indicated during breast-feeding.
 Name GLUCOPHAGE XR 1000 mg Prolonged release tablets Active ingredient Metformin hydrochloride Composition Each Glucophage XR 1000 mg prolonged release tablet contains as active ingredient 1000 mg metformin
Name GLUCOPHAGE XR 1000 mg Prolonged release tablets Active ingredient Metformin hydrochloride Composition Each Glucophage XR 1000 mg prolonged release tablet contains as active ingredient 1000 mg metformin
CONTRAINDICATIONS: Hypersensitivity to the active substance or to any of the excipients
 Galvus PRESENTATION: Each tablet contains 50 mg of Vildagliptin INDICATIONS: For the treatment of type 2 diabetes mellitus in adults: i) As monotherapy in patients inadequately controlled by diet and exercise
Galvus PRESENTATION: Each tablet contains 50 mg of Vildagliptin INDICATIONS: For the treatment of type 2 diabetes mellitus in adults: i) As monotherapy in patients inadequately controlled by diet and exercise
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus. Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre
 Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Diabetes Mellitus: Overview and Guidelines
 Diabetes Mellitus: Overview and Guidelines Rezvan Salehidoost, M.D., Endocrinologist Abidi Diabetes Master Class IMPORTANCE? Why is it interesting to do research in diabetes J. Olefsky, JAMA 2001:285:628-632
Diabetes Mellitus: Overview and Guidelines Rezvan Salehidoost, M.D., Endocrinologist Abidi Diabetes Master Class IMPORTANCE? Why is it interesting to do research in diabetes J. Olefsky, JAMA 2001:285:628-632
Hot Topics in Diabetic Kidney Disease a primary care perspective
 Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES