Drug Therapy for Diabetes Mellitus. Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017
|
|
|
- Shavonne Horn
- 5 years ago
- Views:
Transcription



1 Drug Therapy for Diabetes Mellitus Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017

2 Diabetes Subtypes Optimal Treatment
3 Ominous Octet DeFronzo. DIABETES, VOL. 58, APRIL 2009
4 Schematic Overview of Pathogenesis of Diabetic Complications Physiol Rev 93: , 2013
5
6 Cumulative Mortality median of 7.9 years of gain of life Diabetologia online 16 th August 2016
7 Cumulative Incidence of the composite CV or Death Endpoint median of 8.1 years of CV free Diabetologia online 16 th August 2016
8 Summary of studies examining the effect of sulfonylurea (SU) treatment DeFronzo. DIABETES, VOL. 58, APRIL 2009
9

10 Elements of Decision Making

11 ADA Guidelines: Antiglycemic Treatment in T2DM American Diabetes Association. Diabetes Care 2017
12
13
14 Other Considerations when deciding on Diabetes Medications Care Setting Outpatient long - term considerations Inpatient acute illness - sepsis, AoCKD, NBM Peri-operative DM in pregnancy


15 Insulin Hexamer ZINC Monomer Monomer
 Aspart (Novorapid) Glulisine (Apidra) * Binding to Albumin Non-Hexameric insulin")
16 Types of Insulin Basal Supplements Premeal Bolus rdna Human insulin NPH Humulin N or Insulatard OR Insulin Analogs Glargine + (Lantus) Determir * (Levemir) + Shifted Isoelectric point rdna Human insulin Regular Humulin R or Actrapid OR Insulin Analogs Lispro (Humalog) Aspart (Novorapid) Glulisine (Apidra) * Binding to Albumin Non-Hexameric insulin analogs
 BF Lunch Dinner 10pm 4am * 70kg with minimal insulin")
17 Serum Insulin levels To Replicate Physiological Insulin Secretion Hormonal Nadir Dawn Phenomenon 6u 6u 6u Basal Secretion (Approx 1 unit/hr = 24 units/day) BF Lunch Dinner 10pm 4am * 70kg with minimal insulin resistance
18 Treating fasting hyperglycaemia lowers the entire 24-hour plasma glucose profile Plasma glucose (mg/dl) Meal Meal Meal Time of day (hours) Nocte NPH or LA Basal Analogue T2DM Hyperglycaemia due to an increase in fasting glucose Normal Plasma glucose (mmol/l) Comparison of 24-hour glucose levels in control subjects vs patients with diabetes (p<0.001). Adapted from Hirsch I, et al. Clin Diabetes 2005;23:78 86.
 To exclude Type 1 Diabetes Mellitus Immune markers Eg Anti-GAD, Islet cell Ab Low C-peptide reserves")
19 Insulin Requiring Diabetes Marked hyperglycemia Rapid onset of severe symptoms Significant weight loss Ketoacidosis Type 1 or Type 2 with severe concurrent illness or glucotoxicity < 30 years of age at presentation Lean (No metabolic syndrome/acanthosis nigricans) To exclude Type 1 Diabetes Mellitus Immune markers Eg Anti-GAD, Islet cell Ab Low C-peptide reserves 19

20 Metformin Important insulin sensitiser Recommended doses mg/day Renal Clearance Unmetabolised Contraindicated Renal ( Creat 150umol/L, <30ml/min* ) Hepatic, Cardiac failure, Alcohol abuse Sepsis and hypoperfusion Cautious use in elderly, anorexic GI Intolerance Interferes with Vitamin B12 absorption *Diabet Med 24: , 2007

21 Biologic Effect of Primary Drug Hepatic Metabolism? Or Renal Excretion? Active Metabolites?
22 Incretins GLP-1 Receptor Agonists S/C Exenatide BD S/C Liraglutide OM (97%homology+FA) Dipeptidyl peptidase IV (DPP-IV) Inhibitors Sitagliptin Vildagliptin Saxagliptin Linagliptin, etc
23 Benefits of Incretins Effectively reduces HbA1c Reduced food intake and weight loss (With incretin analogues) Glucose-dependent insulinotropic effect Glucose-dependent inhibition of elevated plasma glucagon levels
24 PANCREATIC BETA CELL GLP-1R GIPR ATP/ADP Modified, Diabetes 51 (Suppl. 1):S19 S24, 2002
 Continue MET + liraglutide 1.")


 Main study n=498; extension n=461 MET, metformin;")
25 Basal insulin added to GLP-1 receptor agonist: LIRA-DETEMIR study design Open-label randomisation (1:1) Continue MET + liraglutide 1.8 mg (Control group) Main study n=161; extension n=122 Addition of insulin detemir to MET + liraglutide Main study n=162; extension n=140 Patients with suboptimal control on MET SU Addition of liraglutide 1.8 mg to MET HbA 1c 7% 39% Main study 26 weeks Extension 26 weeks 12-week run-in phase HbA 1c <7% 61% Continue MET + liraglutide 1.8 mg (Observational group) Main study n=498; extension n=461 MET, metformin; SU, sulphonylurea DeVries JH et al. Diabetes Care 2012;35:
26 HbA 1c (%) Addition of insulin detemir to liraglutide: Change in HbA 1c (%) Run-in phase Randomised phase (Weeks 0 to 52) 8.5 Time (weeks) p< Liraglutide 1.8 mg Liraglutide 1.8 mg + IDet Observational liraglutide 1.8 mg Mean (2SE); data are LOCF Last observation before intensification is included as LOCF in the initial treatment group; ANCOVA on FAS LOCF for difference in randomised phase ANCOVA, analysis of covariance; FAS, full analysis set; HbA 1c, glycosylated haemoglobin; IDet, insulin detemir; LOCF, last observation carried forward; SE, standard error Rosenstock J et al. J Diabetes Complications 2013;27:



27 What is the Relation? Phlorizin Apple Tree Proximal Tubule Epithelial Cell
28 Comparing SGLT2 - Inhibitors
29 SGLT2 Inhibitors: gliflozin Works independently of insulin Inhibiting the SGLT2 glucose transporter found in proximal tubule of nephron, responsible for glucose reabsorption Dose-dependant renal glycosuria, lowering both plasma glucose levels and insulinemia Reductions in HbA1c 0.7% Reductions in Total Body Weight 2 to3 %
30 SGLT2 Inhibitors: gliflozin Reduced CVD events and mortality Greater risk of amputation: toe or metatarsal (Canagliflozin)* Risk volume depletion and hypotension: Caution with severe hyperglycemia, concurrent diuretics, acute illness Normoglycemic DKA: Concurrent illness, stress/counter regulatory hormones *DOI: /NEJMoa

31 Euglycemic diabetic ketoacidosis induced by SGLT2 inhibitors Keep high index of suspicion: Check ph, Serum Bicarbonate and serum BHB Ogawa and Sakaguchi Doi: /jdi.12401
32 Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes N Engl J Med 2016;375:323-34
33 Case Study 1 Mr T 75 year old Chinese Male Strong family history of T2DM T2DM since 50years old Hypertension Ex-smoker PO Glipizide 15mg BD PO Metformin 850mg BD HbA1c 7.5%, Creatinine 80 umol/l Urine microalbumin +ve, Early DM retinopathy
34 HbA1c above target range * Check for: A. Episodes of hypoglycaemia B. Compliance to anti-diabetic medications (including extent of non compliance) C. Compliance to medical nutrition therapy (including extent of non compliance) D. Weight trend - Weight gain due to hypoglycaemia and hunger. Reductions in the dose of SU and insulin may in fact paradoxically improve the glucose control. - Weight loss (>5-10% of body weight) and a high HbA1c (>9%) are likely insulinopenic and should be started on insulin E. Presence of other medications or medical conditions that can change blood glucose control (e.g. glucocorticoids, inter-current infection, cancer). F. Intensify or alter non-pharmacological therapy (i.e. nutrition therapy, exercise, pharmacotherapy) based on cause(s) identified. G. Start and/or optimize dose of pharmacological therapy *When interpreting the HbA1c, the following should be taken into account: (A) Conditions that may falsely elevate or lower HbA1c (e.g. blood loss, recent blood transfusion or haemoglobinopathies). (B) The HbA1c may not fully reflect blood glucose levels for changes that have taken place less than 3 months before the HbA1c.
35
36 Case Study 1 Decreased PO Glipizide 5mg BD Maintained PO Metformin 850mg BD Regular meal times + Light Supper HbA1c 6.7% - 6.8% No hypoglycemia symptoms or documented KIV switch the sulphonylurea to a DPP4 inhibitor
37 HbA1c at or below target range 1 Check for: (A) Episodes of hypoglycaemia (B) Compliance to anti-diabetic medications (including extent of non compliance) (C) Weight trend 2 - Weight gain due to hypoglycaemia and hunger. Reductions in the dose of SU and insulin may in fact paradoxically improve the glucose control. Consider deescalating insulin or SU (or other OHGAs) if any of the following are present: 1. Episodes of hypoglycaemia 2. HbA1c is at target despite significant non-compliance to medications 3. HbA1c is below target range *When interpreting the HbA1c, the following should be taken into account: (A) Conditions that may falsely elevate or lower HbA1c (e.g. blood loss, recent blood transfusion or haemoglobinopathies). (B) The HbA1c may not fully reflect blood glucose levels for changes that have taken place less than 3 months before the HbA1c.
38 Case Study2 : 54 year old Male T2DM for 10 years Strong family history of DM & IHD, BMI 30.1 kg/m2 Fasting Glucose 9.8 mmol/l, HbA1c % PO Glipizide 5mg BD PO Sitagliptin/Metformin 50mg/1000mg BD PO Acarbose 50mg TDS egfr > 60, Urine ACR +ve, No macrovascular Cx. Diet and Exercise as best as can be No hypoglycemia 1. Add an SGLT2 Inhibitor 2. Initiate Basal Insulin Stop Acarbose 3. Initiate Basal Insulin KIV add SGLT2 Inhibitor or GLP-1 agonist 4. Initiate Basal Bolus 38
39 Summary Establish Glycaemic Targets Individualise Treatment Use Metformin as the cornerstone of diabetes treatment in T2DM Consider degree of hyperglycemia, risk of hypoglycemia, renal function and other comorbidities in the selection of Rx Timely Insulinisation
40 Summary SGLT2 Inhibitors for patients at risk of hypoglycemia, cardiovascular and renal benefits but increased risk of genitourinary infections and normoglycemic DKA - synergise well with insulin treatment New formulations of long acting basal analogue insulin eg Glargine 300 Units/ml, Insulin Degludec GLP1 Agonists and Long Acting Basal Insulin combinations
41 Ideal Diabetic Medication Effective in lowering glucose No or Low risk of hypoglycemia Positive extraglycemic effects Weight Lipid profile Blood Pressure Safe, Tolerable, Ease of use Low Cost / Expense Ability to maintain glucose levels close to non-diabetic range Surrogate Markers HbA1c Lipids Reduce long term microvascular and macrovascular complications - Endpoints
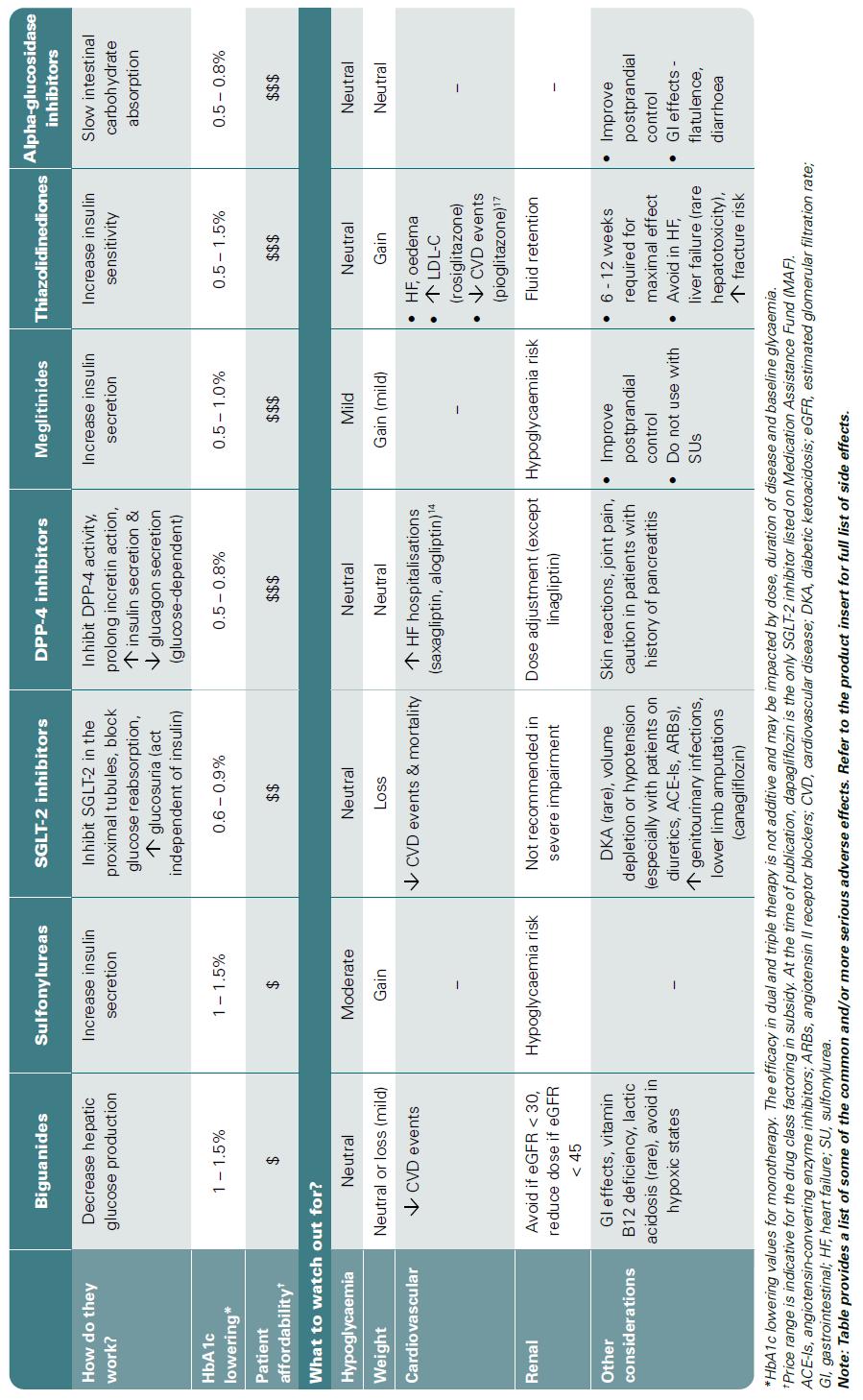
42 Useful References AACE/ACE Comprehensive Diabetes Manangement Algorithm 2015: ENDOCRINE PRACTICE Vol 21 No. 4 April 2015 ADA/EASD Standards of Care Oral Glucose-lowering Agents in Type 2 Diabetes Mellitus An update Appropriate Care Guide: MOH & ACE Published 3 rd July 2017
43
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Diabetes Mellitus case studies. Jana Vinklerová
 Diabetes Mellitus case studies Jana Vinklerová Definition of diabetes (metabolic disorder) Chronically raised blood glucose (hyperglycaemia) Insulin/Glucagon Insulin is responsible for lowering glucose
Diabetes Mellitus case studies Jana Vinklerová Definition of diabetes (metabolic disorder) Chronically raised blood glucose (hyperglycaemia) Insulin/Glucagon Insulin is responsible for lowering glucose
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
There have been important changes in diabetes care which may not be covered in undergraduate textbooks.
 Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
STEP 3: Add or Substitute with one of
 Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
COPYRIGHT. Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely?
 Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Diabetes, Type 2 Management
 CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
3. Cardiovascular Disease?
 Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
Mr Rab Burtun. Dr David Kim. 8:30-10:30 WS #2: Diabetes Basic 11:00-13:00 WS #9: Diabetes Basic (Repeated)
") Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period
 Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich
Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich
Type 2 diabetes: recent advances in diagnosis and management
 DRUG REVIEW n Type 2 diabetes: recent advances in diagnosis and management Sudesna Chatterjee MD, FRCP and Melanie Davies MD, FRCP, FRCGP The expanding array of new type 2 diabetes agents and how to combine
DRUG REVIEW n Type 2 diabetes: recent advances in diagnosis and management Sudesna Chatterjee MD, FRCP and Melanie Davies MD, FRCP, FRCGP The expanding array of new type 2 diabetes agents and how to combine
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital
 What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
DIABETES INDICATIONS FOR INSULIN
 DIABETES INDICATIONS FOR INSULIN 1 Introduce the likely need for insulin in the future early on as part of patient education Emphasise that it is the pancreas that fails not the patient Assess if greater
DIABETES INDICATIONS FOR INSULIN 1 Introduce the likely need for insulin in the future early on as part of patient education Emphasise that it is the pancreas that fails not the patient Assess if greater
Arrange 3 Monthly Review Re-enforce LIFESTYLE advice and check DRUG COMPLIANCE at each visit Target HbA1c < 53mmol/mol
 Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
PERIOPERATIVE DIABETES GUIDELINE
 PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
How they work and when to take them. Diabetes Medications
 How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd
 SMC No. (1083/15) Merck Sharp and Dohme UK Ltd") sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd 07 August 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd 07 August 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS
 Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Inpatient Diabetes 20/01/2015. What should I do? Hyperglycaemia why does it matter? Why are the BSLs unstable? BSL parameters
 Hyperglycaemia why does it matter? Inpatient Diabetes Angela Sheu Endocrine Registrar St George Hospital Hyperglycaemia at admission is a predictor of mortality May be part of stress response (eg post
Hyperglycaemia why does it matter? Inpatient Diabetes Angela Sheu Endocrine Registrar St George Hospital Hyperglycaemia at admission is a predictor of mortality May be part of stress response (eg post
Dr Karen McNeil Consultant Endocrinologist
 Dr Karen McNeil Consultant Endocrinologist Aged 53 Type 2 Diabetes 2010 HbA1c 7.9% ACR 5.3 mg/mmol What treatment? MF 500 mg bd (misses midday dose) Control Symptoms, BGL Complications DR, DN, PN Associations
Dr Karen McNeil Consultant Endocrinologist Aged 53 Type 2 Diabetes 2010 HbA1c 7.9% ACR 5.3 mg/mmol What treatment? MF 500 mg bd (misses midday dose) Control Symptoms, BGL Complications DR, DN, PN Associations
Dr A Pokrajac MD MSc MRCP Consultant
 Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Clinical Guidelines. Management of adult patients with diabetes undergoing endoscopic procedures
 Clinical Guidelines Management of adult patients with diabetes undergoing endoscopic s Document Detail Document type Clinical Guideline Management of adult Patients with diabetes Undergoing Document name
Clinical Guidelines Management of adult patients with diabetes undergoing endoscopic s Document Detail Document type Clinical Guideline Management of adult Patients with diabetes Undergoing Document name
I. General Considerations
 1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes
 THERAPY REVIEW DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes STEVE CHAPLIN SPL DPP-4 inhibitors and SGLT2 inhibitors lower blood glucose by complementary mechanisms of action, and two fixeddose
THERAPY REVIEW DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes STEVE CHAPLIN SPL DPP-4 inhibitors and SGLT2 inhibitors lower blood glucose by complementary mechanisms of action, and two fixeddose
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Insulin Prior Authorization with optional Quantity Limit Program Summary
 Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION
 SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
Diabetes mellitus. Treatment
 Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Pharmacological Glycaemic Control in Type 2 Diabetes
 Pharmacological Glycaemic Control in Type 2 Diabetes Aim(s) and Objective(s) This guideline aims to offer advice on the pharmacological management for those who require measures beyond diet and exercise
Pharmacological Glycaemic Control in Type 2 Diabetes Aim(s) and Objective(s) This guideline aims to offer advice on the pharmacological management for those who require measures beyond diet and exercise
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
Diabetes 2013: Achieving Goals Through Comprehensive Treatment. Session 2: Individualizing Therapy
 Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
CASE A2 Managing Between-meal Hypoglycemia
 Managing Between-meal Hypoglycemia 1 I would like to discuss this case of a patient who, overall, was doing well on her therapy until she made an important lifestyle change to lose weight. This is a common
Managing Between-meal Hypoglycemia 1 I would like to discuss this case of a patient who, overall, was doing well on her therapy until she made an important lifestyle change to lose weight. This is a common
Dr Tahseen A. Chowdhury Royal London Hospital. New Guidelines in Diabetes: NICE or Nasty?
 Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Clinical Practice Guidelines
 Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
GLP-1. GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4.
 GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION
 OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION Biljana Parapid, MD, PhD, FESC Belgrade University School of Medicine, Belgrade (Serbia) @biljana_parapid COI International
OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION Biljana Parapid, MD, PhD, FESC Belgrade University School of Medicine, Belgrade (Serbia) @biljana_parapid COI International
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
DIABETES UPDATE 2018
 DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
Diabetes: Definition Pathophysiology Treatment Goals. By Scott Magee, MD, FACE
 Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs
 Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Advanced Practice Education Associates. Endocrine
 Advanced Practice Education Associates Endocrine Overview Diabetes Thyroid Disease 162 Copyright 2016 Advanced Practice Education Associates DIABETES MELLITUS What is the BMI cut point for screening adults
Advanced Practice Education Associates Endocrine Overview Diabetes Thyroid Disease 162 Copyright 2016 Advanced Practice Education Associates DIABETES MELLITUS What is the BMI cut point for screening adults
Objectives. How Medicine Works to Control Blood Sugar Levels. What Happens When We Eat? What is diabetes? High Blood Glucose (Hyperglycemia)
") How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
Intensification of Diabetic Therapy. Case studies
 Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Combination treatment for T2DM
 Combination treatment for T2DM Date of approval: December 2016 SAGLB.DIA.16.08.0657 Abbreviations ADA: American Diabetes Association CVD: Cardiovascular disease DPP-4: Dipeptidyl Peptidase-4 EASD: European
Combination treatment for T2DM Date of approval: December 2016 SAGLB.DIA.16.08.0657 Abbreviations ADA: American Diabetes Association CVD: Cardiovascular disease DPP-4: Dipeptidyl Peptidase-4 EASD: European
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Physiology of Normoglycemia
 Case 1 45 year-old male patient seen at the clinic (Medicine). Workplace stress (financial analyst); occasionally goes jogging. Two-year duration of T2DM. No previous cardiovascular events. Coexisting
Case 1 45 year-old male patient seen at the clinic (Medicine). Workplace stress (financial analyst); occasionally goes jogging. Two-year duration of T2DM. No previous cardiovascular events. Coexisting
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
ClinicalTrials.gov Identifier: sanofi-aventis. Sponsor/company:
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinicalTrials.gov
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinicalTrials.gov
Insulin Therapy Management. Insulin Therapy
 Insulin Therapy Management Insulin Therapy Contents Insulin and its effect on glycemic control Physiology of insulin secretion Insulin pharmacokinetics and regimens Insulin dose adjustment for pregnancy
Insulin Therapy Management Insulin Therapy Contents Insulin and its effect on glycemic control Physiology of insulin secretion Insulin pharmacokinetics and regimens Insulin dose adjustment for pregnancy
PLEASE CHECK FULL SPECIFIC PRODUCT CHARACTERISTICS FOR MORE DETAILED AND CURRENT INFORMATION:
 Metformin Standard tablets Modified-release tablets Metformin 1g sachets Metformin liquid 500mg/5ml (avoid use as expensive) < 2.00 5.32 for 56 tabs 500mg 13.16 for 60 sachets > 120 Ketoacidosis General
Metformin Standard tablets Modified-release tablets Metformin 1g sachets Metformin liquid 500mg/5ml (avoid use as expensive) < 2.00 5.32 for 56 tabs 500mg 13.16 for 60 sachets > 120 Ketoacidosis General