Michelle L. Ischayek D.O. Emergency Medicine Resident Aria Health
|
|
|
- Osborn Blake
- 5 years ago
- Views:
Transcription

1 Michelle L. Ischayek D.O. Emergency Medicine Resident Aria Health

2 History 15 year old African female with CC of Headache. Onset: 2 weeks ago Location: Frontal Character: Sharp & Throbbing Radiation: None Severity: Moderate Timing: Intermittent Associated Symptoms: Diplopia and Photophobia


3 History Headache resolves with Advil 30 pound weight gain over the past year UTD with immunizations
4 History Past Medical Hx: Denies Family Hx: Denies Surgical Hx: Denies Social Hx: Denies ETOH or Drug Abuse, Lives with parents Medications: Denies Allergies: NKDA
5 Review of Systems Denies fever, chills, cough, nausea, vomiting, chest pain, shortness of breath, myalgias or neck stiffness. Denies previous history of headaches. Denies recent travel. Complains of frontal headache, diplopia and photophobia.
6 Physical Exam VITALS: T: 98.2 F BP: 128/72 P: 72 RR: 18 Oxygen Saturation: 97% on RA GENERAL APPEARANCE: Well-developed, well nourished, alert, cooperative, no acute distress, generally well appearing. HEENT: mild right-sided esotropia, conjunctiva clear, no nystagmus. No papilledema. TMs clear, mucous membranes good color. NECK: - JVD, no neck tenderness. LUNGS: Clear to auscultation bilaterally, no wheezes, rales or rhonchi.
7 Physical Exam HEART: Regular rate and rhythm, no murmurs, gallups or rubs. ABDOMEN: soft, non-tender, non-distended, bowel sounds x 4, no rebound, no guarding. EXTREMITIES: no clubbing, cyanosis or edema. 2+ radial pulses bilaterallly. SKIN: no rashes noted. NEURO: right-sided abducens nerve palsy, muscle strength 5/5 in bilateral UE and LE. Sensation intact in bilateral UE and LE. Finger to nose normal, normal gait, cerebellar function intact.

8 Labs CBC with Differential WBC: 7.3 RBC: 5.10 H&H: 12.3/37.3 MCV: 73.2 MCH: 24.0 RDW: 15.4 Platelet Count: 240 Lymph: 29.9 % Mononuclear: 5.2 % Neutrophil: 63.1 % Basophil: 0.5 % Eosinophil: 4.6 %
9 Labs BMP Na: 138 K: 3.4 Cl: 104 CO2: 28 Coags PT: 12.4 INR: 1.1 PTT: 33 Beta HCG: Negative Glucose: 100 BUN: 5 Cr: 0.68 Ca: 9.5
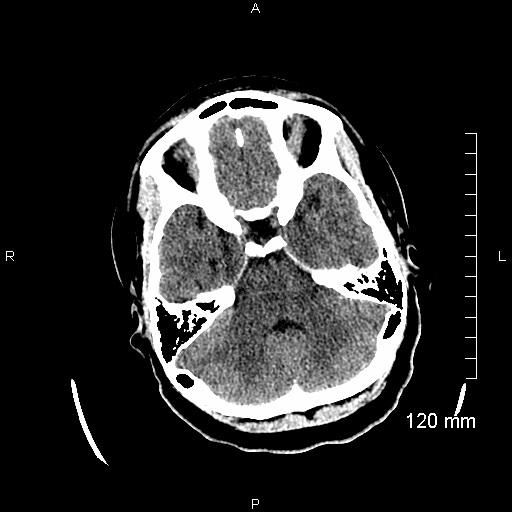
10 CT Brain
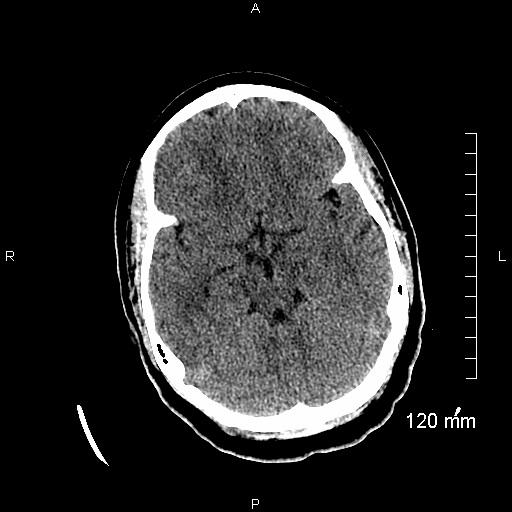
11 CT Brain
12 Transfer Patient was transferred to a pediatric emergency department for further diagnostic workup.
13 What Is Your Diagnosis???
14 Introducing Faculty Discussant: Dr. Joseph Dougherty, D.O. Ohio Valley Health System

15 Michelle L. Ischayek D.O. Emergency Medicine Resident Aria Health
16 CT Brain No acute intracranial abnormality. No intracranial hemorrhage or mass effect.
17 MRI Brain The ventricular system is normal in size, shape and configuration. There are no intracranial mass lesions, and there is no mass effect or midline shift. No abnormal fluid collections.
18 Intracranial MRV The major intracranial venous structures demonstrate normal flow-related enhancement. There is no MRV evidence for deep venous sinus thrombosis.
19 Lumbar Puncture Elevated Opening Pressure of 35 cm H2O. Normal CSF.
20 15 year old African Female CC: Frontal headache, 2 weeks. Sx: Diplopia & Photophobia. PE: Right-sided Esotropia LP: Elevated opening pressure Brain Imaging: Negative Dispo: Admitted to pediatric facility with

21 Diagnosis Idiopathic Intracranial Hypertension (IIH)
22 IIH Pseudotumor Cerebri, false brain tumor, benign Intracranial Hypertension. Increased intracranial pressure Normal CSF Absence of tumor Not a benign disorder
23 Epidemiology Annual incidence is 1-2 per 100,000 population. Higher incidence in obese women between 15 and 44 years. Males and children whom are not overweight affected too.
24 Associated Conditions Systemic Diseases Hereditary Conditions Vitamin Deficiencies Medications
25 Pathogenesis Exact Pathogenesis unknown Theories: Abnormalities of cerebral venous outflow tract Increased CSF outflow resistance Increased abdominal and intracranial venous pressure Sodium and water retention Abnormal Vitamin A metabolism

26 Signs & Symptoms Headache Transient Visual Obscurations Pulsatile Tinnitus Photopsia Retrobulbar pain Diplopia Sustained Visual Loss Neck Stiffness
27 Signs & Symptoms Headache is the most common presenting symptom. Nausea and vomiting. Exacerbated by changes in posture, sneezing or coughing. Improves with rest or NSAIDs.

28 Exam Papilledema Visual Field Loss Abducens Nerve Palsy Cranial Nerve Deficits
29 Differential Diagnosis Mass-Tumor, Abscess Hydrocephalus Cerebral venous thrombosis Choroid plexus papilloma
30 Diagnosis Modified Dandy Criteria: Increased ICP: headache, transient visual loss, tinnitus, and papilledema. No other neurologic abnormalities or impaired level of consciousness. Neuroimaging study that shows no etiology for intracranial hypertension. No other cause of intracranial hypertension. Elevated intracranial pressure with normal CSF.

31 Neuroimaging MRI is the test of choice. If MRI contraindicated, CT Brain.

32 Lumbar Puncture If neuroimaging negative, perform LP. During LP, measure opening pressure and evaluate CSF cell count, glucose and protein. Upper limit of normal opening pressure in adults is 20 cm H20. Pressures can be as high as 28 cm H20 if patient is curled up in lateral decubitus position. In young children, upper limit of opening pressure is 25 cm H20.
33 Prognosis Can last months to years. Slow, gradual onset. With treatment, gradual improvement and stabilization. Permanent vision loss, major morbidity. Fulminant IIH, experience visual loss within a few weeks of symptom onset.

34 Treatment 2 main goals: improve symptoms and preserve vision. Weight Loss Medications Other Treatments
35 Surgical Treatment Indications: Failed medical treatments Visual field defects Visual Acuity loss Intractable headaches Noncompliance Surgical Procedures: Optic nerve sheath fenestration and CSF shunting.
36 Back to Our Patient Hospital Course: Diagnosed with IIH Encouraged to lose weight Discharged on Diamox 250mg BID x 1 week then 500mg BID (total of 274 days) Follow up with Neurology and Ophthalmology
37 Thank You!
38 References Arsava EM, Uluc K, Nurlu G, Kansu T. Electrophysiological evidence of trigeminal neuropathy in pseudotumor cerebri. J Neurol 2002; 249: Beri S, Gosalakkal JA, Hussain N, et al. Idiopathic intracranial hypertension without papilledema. Pediatr Neurol 2010; 42: Capobianco DJ, Brazis PW, Cheshire WP. Idiopathic intracranial hypertension and seventh nerve palsy. Headache 1997; 3 5. Krishna R, Kosmorsky GS, Wright KW. Pseudotumor cerebri sine papilledema with unilateral sixth nerve palsy. J Neuroophthalmol 1998; 18:53.
39 References 6. Malomo AO, Idowu OE, Shokunbi MT, et al. Nonoperative management of benign intracranial hypertension presenting with complete visual loss and deafness. Pediatr Neurosurg 2006; 42: Vieira DS, Masruha MR, Gonçalves AL, et al. Idiopathic intracranial hypertension with and without papilloedema in a consecutive series of patients with chronic migraine. Cephalalgia 2008; 28: Soler D, Cox T, Bullock P, et al. Diagnosis and management of benign intracranial hypertension. Arch Dis Child 1998; 78: Selky AK, Dobyns WB, Yee RD. Idiopathic intracranial hypertension and facial diplegia. Neurology 1994; 44:357.
What is IIH? Idiopathic Intracranial Hypertension (IIH)
") What is IIH? Idiopathic Intracranial Hypertension (IIH) What is Idiopathic Intracranial Hypertension? Idiopathic intracranial hypertension (IIH), also known as benign intracranial hypertension or pseudotumour
What is IIH? Idiopathic Intracranial Hypertension (IIH) What is Idiopathic Intracranial Hypertension? Idiopathic intracranial hypertension (IIH), also known as benign intracranial hypertension or pseudotumour
The headache profile of idiopathic intracranial hypertension
 The headache profile of idiopathic intracranial hypertension Michael Wall CEPHALALGIA Wall M. The headache profile of idiopathic intracranial hypertension. Cephalalgia 1990;10:331-5. Oslo. ISSN 0333-1024
The headache profile of idiopathic intracranial hypertension Michael Wall CEPHALALGIA Wall M. The headache profile of idiopathic intracranial hypertension. Cephalalgia 1990;10:331-5. Oslo. ISSN 0333-1024
Papilledema. Golnaz Javey, M.D. and Jeffrey J. Zuravleff, M.D.
 Papilledema Golnaz Javey, M.D. and Jeffrey J. Zuravleff, M.D. Papilledema specifically refers to optic nerve head swelling secondary to increased intracranial pressure (IICP). Optic nerve swelling from
Papilledema Golnaz Javey, M.D. and Jeffrey J. Zuravleff, M.D. Papilledema specifically refers to optic nerve head swelling secondary to increased intracranial pressure (IICP). Optic nerve swelling from
Management of Pseudo Tumor Cerebri by Frequent Tapping VS lumboperitoneal Shunt
 The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (5), Page 4556-4560 Management of Pseudo Tumor Cerebri by Frequent Tapping VS lumboperitoneal Shunt Ali K. Ali, Maamoun M. Abo Shousha, Mohammed
The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (5), Page 4556-4560 Management of Pseudo Tumor Cerebri by Frequent Tapping VS lumboperitoneal Shunt Ali K. Ali, Maamoun M. Abo Shousha, Mohammed
Rural STEMI System of Care Success. Nicole Huber, PA-C Cumberland Healthcare Emergency Department
 Rural STEMI System of Care Success Nicole Huber, PA-C Cumberland Healthcare Emergency Department DISCLOSURES I HAVE NO ACTUAL OR POTENTIAL CONFLICT OF INTEREST IN RELATION TO THIS PRESENTATION Ideal Process
Rural STEMI System of Care Success Nicole Huber, PA-C Cumberland Healthcare Emergency Department DISCLOSURES I HAVE NO ACTUAL OR POTENTIAL CONFLICT OF INTEREST IN RELATION TO THIS PRESENTATION Ideal Process
Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings. Jonathan A. Micieli, MD Valérie Biousse, MD
 Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings Jonathan A. Micieli, MD Valérie Biousse, MD A 24 year old African American woman is referred for bilateral optic
Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings Jonathan A. Micieli, MD Valérie Biousse, MD A 24 year old African American woman is referred for bilateral optic
Med 536 Communicating About Prognosis Workshop. Case 2
 Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
THE SWOLLEN DISC. Valerie Biousse, MD Emory University School of Medicine Atlanta, GA
 THE SWOLLEN DISC Valerie Biousse, MD Emory University School of Medicine Atlanta, GA Updated from: Neuro-Ophthalmology Illustrated. Biousse V, Newman NJ. Thieme, New-York,NY. 2 nd Ed, 2016. Edema of the
THE SWOLLEN DISC Valerie Biousse, MD Emory University School of Medicine Atlanta, GA Updated from: Neuro-Ophthalmology Illustrated. Biousse V, Newman NJ. Thieme, New-York,NY. 2 nd Ed, 2016. Edema of the
NANOS Patient Brochure
 NANOS Patient Brochure Pseudotumor Cerebri Copyright 2016. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for
NANOS Patient Brochure Pseudotumor Cerebri Copyright 2016. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for
Prevalence of venous sinus stenosis in Pseudotumor cerebri(ptc) using digital subtraction angiography (DSA)
 using digital subtraction angiography (DSA)") Prevalence of venous sinus stenosis in Pseudotumor cerebri(ptc) using digital subtraction angiography (DSA) Dr.Mohamed hamdy ibrahim MBBC,MSc,MD, PhD Neurology Degree Kings lake university (USA). Fellow
Prevalence of venous sinus stenosis in Pseudotumor cerebri(ptc) using digital subtraction angiography (DSA) Dr.Mohamed hamdy ibrahim MBBC,MSc,MD, PhD Neurology Degree Kings lake university (USA). Fellow
PUFF THE MAGIC DRAGON
 PUFF THE MAGIC DRAGON AN UNUSUAL CASE OF A PUFFY FACE MA ACP Annual Scientific Meeting Gurbir Gill, M.D., PGY-3 (Associate) George M. Abraham, MD, MPH, FACP Department of Medicine, Saint Vincent Hospital,
PUFF THE MAGIC DRAGON AN UNUSUAL CASE OF A PUFFY FACE MA ACP Annual Scientific Meeting Gurbir Gill, M.D., PGY-3 (Associate) George M. Abraham, MD, MPH, FACP Department of Medicine, Saint Vincent Hospital,
Neuro-Ocular Grand Rounds
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland
 Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Neuro-Ocular Grand Rounds Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker and advisory boards for Alcon and Zeiss Meditek COMMON OPTIC NEUROPATHIES THAT CAN
Headache Syndrome. Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL
 Headache Syndrome Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL What is a headache? A headache or cephalgia is defined as pain anywhere in the region of head or neck Where does
Headache Syndrome Karen Alvarez, D.O Nemours Children s Specialty Care Jacksonville, FL What is a headache? A headache or cephalgia is defined as pain anywhere in the region of head or neck Where does
Pearls, Pitfalls and Advances in Neuro-Ophthalmology
 Pearls, Pitfalls and Advances in Neuro-Ophthalmology Nancy J. Newman, MD Emory University Atlanta, GA Consultant for Gensight Biologics, Santhera Data Safety Monitoring Board for Quark AION Study Medical-legal
Pearls, Pitfalls and Advances in Neuro-Ophthalmology Nancy J. Newman, MD Emory University Atlanta, GA Consultant for Gensight Biologics, Santhera Data Safety Monitoring Board for Quark AION Study Medical-legal
Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) David I. Kaufman, D.O. Michigan State University Department of Neurology and Ophthalmology
 David I. Kaufman, D.O. Michigan State University Department of Neurology and Ophthalmology") Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) David I. Kaufman, D.O. Michigan State University Department of Neurology and Ophthalmology 26 year old 5 3, 300 pound female with papilledema,
Idiopathic Intracranial Hypertension (Pseudotumor Cerebri) David I. Kaufman, D.O. Michigan State University Department of Neurology and Ophthalmology 26 year old 5 3, 300 pound female with papilledema,
Intracranial hypertension and headache. Daniel Tibussek, MD
 Intracranial hypertension and headache. Daniel Tibussek, MD none Disclosures Overview Case Clinical presentation of pediatric PTC Nomenclature, Definition What is intracranial hypertension? Diagnostic
Intracranial hypertension and headache. Daniel Tibussek, MD none Disclosures Overview Case Clinical presentation of pediatric PTC Nomenclature, Definition What is intracranial hypertension? Diagnostic
MOHAMED LOTFY, M.D.*; MOATAZ A. EL-AWADY, M.D.**; ASHRAF E. ZAGHLOUL, M.D.** and TAREK NEHAD, M.D.***
 Med. J. Cairo Univ., Vol. 84, No. 2, December: 301-306, 2016 www.medicaljournalofcairouniversity.net Effect of Therapeutic Lumbar Puncture on the Visual Outcome and the Further Need for Surgery in Patients
Med. J. Cairo Univ., Vol. 84, No. 2, December: 301-306, 2016 www.medicaljournalofcairouniversity.net Effect of Therapeutic Lumbar Puncture on the Visual Outcome and the Further Need for Surgery in Patients
Date of Admission: [DATE]. Date of Discharge:
![Date of Admission: [DATE]. Date of Discharge:](/thumbs/74/71277118.jpg "Date of Admission: [DATE]. Date of Discharge:") Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Teaching Clinical Reasoning. Clinical Reasoning Strategy. Clinical Reasoning Strategy 11/27/2018. Teaching of Tomorrow November 2018
 Teaching Clinical Reasoning Teaching of Tomorrow November 2018 Clinical Reasoning Strategy The following teaching paradigm is appropriate for these scenarios: Case Conference discussions Robust case presentations
Teaching Clinical Reasoning Teaching of Tomorrow November 2018 Clinical Reasoning Strategy The following teaching paradigm is appropriate for these scenarios: Case Conference discussions Robust case presentations
Idiopathic intracranial hypertension (pseudotumor cerebri): Clinical features and diagnosis
: Clinical features and diagnosis") Idiopathic intracranial hypertension (pseudotumor cerebri): Clinical features and diagnosis Authors Andrew G Lee, MD Michael Wall, MD Section Editor Paul W Brazis, MD Deputy Editor Janet L Wilterdink,
Idiopathic intracranial hypertension (pseudotumor cerebri): Clinical features and diagnosis Authors Andrew G Lee, MD Michael Wall, MD Section Editor Paul W Brazis, MD Deputy Editor Janet L Wilterdink,
Khalil Zahra, M.D Neuro-interventional radiology
 Khalil Zahra, M.D Neuro-interventional radiology 1 Disclosure None 2 Outline Etiology and pathogensis Imaging techniques and Features Literature review Treatment modalities Endovascular techniques Long
Khalil Zahra, M.D Neuro-interventional radiology 1 Disclosure None 2 Outline Etiology and pathogensis Imaging techniques and Features Literature review Treatment modalities Endovascular techniques Long
Learn Connect Succeed. JCAHPO Regional Meetings 2017
 Learn Connect Succeed JCAHPO Regional Meetings 2017 NO FINANCIAL DISCLOSURES Technician s Role in Neuro-Ophthalmology Workup Beth Koch COT, ROUB Cleveland 9/16/2017 What Tests Are You Expected To Perform?
Learn Connect Succeed JCAHPO Regional Meetings 2017 NO FINANCIAL DISCLOSURES Technician s Role in Neuro-Ophthalmology Workup Beth Koch COT, ROUB Cleveland 9/16/2017 What Tests Are You Expected To Perform?
Neurological Dilemmas in Primary Care
 Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
11/10/2017. Headache and Increased Pressure: A tale of 2 cases. Kathleen Digre MD University of Utah TWO CASES. 23 yo medical practice manager
 Headache and Increased Pressure: A tale of 2 cases Kathleen Digre MD University of Utah TWO CASES 23 yo medical practice manager September 2016 began developing intense frontal headaches first intermittent
Headache and Increased Pressure: A tale of 2 cases Kathleen Digre MD University of Utah TWO CASES 23 yo medical practice manager September 2016 began developing intense frontal headaches first intermittent
* Final Report * ED Triage Entered On: 01/16/2014 8:45 EST Performed On: 01/16/2014 8:42 EST by
 Result date: Result status: 16 January 2014 8:42 EST Auth (Verified) * Final Report * ED Triage Entered On: 01/16/2014 8:45 EST Performed On: 01/16/2014 8:42 EST by Assessment I Chief Complaint : Diarrhea
Result date: Result status: 16 January 2014 8:42 EST Auth (Verified) * Final Report * ED Triage Entered On: 01/16/2014 8:45 EST Performed On: 01/16/2014 8:42 EST by Assessment I Chief Complaint : Diarrhea
12/2/16. Ways to differentiate:
 Nate Lighthizer, O.D., F.A.A.O. Assistant Dean for Clinical Care Services Director of CE Chief of Specialty Care Clinics Chief of Electrodiagnostics Clinic Oklahoma College of Optometry lighthiz@nsuok.edu
Nate Lighthizer, O.D., F.A.A.O. Assistant Dean for Clinical Care Services Director of CE Chief of Specialty Care Clinics Chief of Electrodiagnostics Clinic Oklahoma College of Optometry lighthiz@nsuok.edu
Real Cases: Bad Outcomes
 Real Cases: Bad Outcomes Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Real Cases: Bad Outcomes Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical
Lumbar puncture. Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: ml Replenished: 4-6 h Routine LP (3-5 ml): <1h
: <1h") Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Headache Assessment In Primary Eye Care
 Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Patient Care Report Guidelines
 A rrival on scene / Scene assessment C omplaint H istory A. Position of patient B. Impression of patient C. Does the patient acknowledge your presence D. Any significant characteristics of the scene A.
A rrival on scene / Scene assessment C omplaint H istory A. Position of patient B. Impression of patient C. Does the patient acknowledge your presence D. Any significant characteristics of the scene A.
AMSER Case of the Month July 2018 Complicated Headache with Fever
 AMSER Case of the Month July 2018 Complicated Headache with Fever Benjamin Park, MS IV Dr. Karen Xie Department of Radiology University of Illinois College of Medicine at Chicago Patient Presentation CC:
AMSER Case of the Month July 2018 Complicated Headache with Fever Benjamin Park, MS IV Dr. Karen Xie Department of Radiology University of Illinois College of Medicine at Chicago Patient Presentation CC:
Secondary Headaches: A Strategic Approach. Emerg Med 40(4):18, 2008
:18, 2008") Secondary Headaches: A Strategic Approach Emerg Med 40(4):18, 2008 Headaches are common complaints in the emergency department, but the causes of secondary headaches are often misdiagnosed. The authors
Secondary Headaches: A Strategic Approach Emerg Med 40(4):18, 2008 Headaches are common complaints in the emergency department, but the causes of secondary headaches are often misdiagnosed. The authors
Exam 1 Review. Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies
 Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
PEDIATRIC BRAIN CARE
 PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
CASE-BASED SMALL GROUP DISCUSSION
 MHD I, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION 11 Renal Block Acid- Base Disorders November 7, 2016 MHD I, Session 11, Student Copy Page 2 Case #1 Cc: I have had
MHD I, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION 11 Renal Block Acid- Base Disorders November 7, 2016 MHD I, Session 11, Student Copy Page 2 Case #1 Cc: I have had
Coexistence of migraine and idiopathic intracranial hypertension without papilledema
 / GX'~C1~.. Coexistence of migraine and idiopathic intracranial hypertension without papilledema Ninan T. Mathew, MD; K. Ravishankar, MD; and Luis C. Sanin, MD!
/ GX'~C1~.. Coexistence of migraine and idiopathic intracranial hypertension without papilledema Ninan T. Mathew, MD; K. Ravishankar, MD; and Luis C. Sanin, MD!
Cryptococcal Meningitis
 Cryptococcal Meningitis Dr N Thumbiran Infectious Diseases Department UKZN Index patient 27 year old female Presented to King Edward Hospital on 17/07/2005 with: Severe headaches Vomiting Photophobia X
Cryptococcal Meningitis Dr N Thumbiran Infectious Diseases Department UKZN Index patient 27 year old female Presented to King Edward Hospital on 17/07/2005 with: Severe headaches Vomiting Photophobia X
IDIOPATHIC INTRACRANIAL HYPERTENSION
 IDIOPATHIC INTRACRANIAL HYPERTENSION ASSESSMENT OF VISUAL FUNCTION AND PROGNOSIS FOR VISUAL OUTCOME Doctor of Philosophy thesis Anglia Ruskin University, Cambridge Fiona J. Rowe Department of Orthoptics,
IDIOPATHIC INTRACRANIAL HYPERTENSION ASSESSMENT OF VISUAL FUNCTION AND PROGNOSIS FOR VISUAL OUTCOME Doctor of Philosophy thesis Anglia Ruskin University, Cambridge Fiona J. Rowe Department of Orthoptics,
Bisan Salhi, M.D. 69 Jesse Hill Jr. Dr. Atlanta, GA Phone:
 Bisan Salhi, M.D. 69 Jesse Hill Jr. Dr. Atlanta, GA 30303 Phone: 734-657-4539 30 June 2006 Dear Sir or Madam: 1. Thank you for the opportunity to evaluate Mr. Liviu Negut. Enclosed is my preliminary medical
Bisan Salhi, M.D. 69 Jesse Hill Jr. Dr. Atlanta, GA 30303 Phone: 734-657-4539 30 June 2006 Dear Sir or Madam: 1. Thank you for the opportunity to evaluate Mr. Liviu Negut. Enclosed is my preliminary medical
Pseudotumor Cerebri Secondary to Minocycline Intake
 Pseudotumor Cerebri Secondary to Minocycline Intake Earl Robert G. Ang, MD, J. C. Chava Zimmerman, MD, and Elissa Malkin, DO, MPH Background: Pseudotumor cerebri, or idiopathic intracranial hypertension,
Pseudotumor Cerebri Secondary to Minocycline Intake Earl Robert G. Ang, MD, J. C. Chava Zimmerman, MD, and Elissa Malkin, DO, MPH Background: Pseudotumor cerebri, or idiopathic intracranial hypertension,
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 3/12/2011 Radiology Quiz of the Week # 11 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 3/12/2011 Radiology Quiz of the Week # 11 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
MHD I SESSION X. Renal Disease
 MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
A walk through a STEMI
 A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
SMALL GROUP DISCUSSION SESSION I
 MHD I Session I Student Copy Page 1 SMALL GROUP DISCUSSION SESSION I MHD I Monday, September 9, 2013 STUDENT COPY MHD I Session I Student Copy Page 2 Helpful Resources for Session Murray s Medical Microbiology,
MHD I Session I Student Copy Page 1 SMALL GROUP DISCUSSION SESSION I MHD I Monday, September 9, 2013 STUDENT COPY MHD I Session I Student Copy Page 2 Helpful Resources for Session Murray s Medical Microbiology,
H&P Checklist (Inpatient) Evaluator: Subject: Program:
 Evaluator: Subject: Program:") H&P Checklist (Inpatient) Evaluator: Subject: Program: PROFESSIONALISM 1) Introduces self/role and preceptor Did 2) Verbal and non-verbal language demonstrates respect for patient & family. Did 3) Respects
H&P Checklist (Inpatient) Evaluator: Subject: Program: PROFESSIONALISM 1) Introduces self/role and preceptor Did 2) Verbal and non-verbal language demonstrates respect for patient & family. Did 3) Respects
OPTIC NERVE SWELLING IN CHILDHOOD
 OPTIC NERVE SWELLING IN CHILDHOOD Melissa W. Ko, MD, FAAN One of the main findings on a pediatric neurologic examination that can instill fear and lead to an urgent referral to neuro-ophthalmology is the
OPTIC NERVE SWELLING IN CHILDHOOD Melissa W. Ko, MD, FAAN One of the main findings on a pediatric neurologic examination that can instill fear and lead to an urgent referral to neuro-ophthalmology is the
NOR-CAL EMS MEDICAL ADVISORY COMMITTEE RUN REVIEW, NOVEMBER 2014
 Eric M. Rudnick, MD, FACEP, FAAEM Medical Director Northern California EMS NOR-CAL EMS MEDICAL ADVISORY COMMITTEE RUN REVIEW, NOVEMBER 2014. meeting by Engineer Bill Bogenreif 1 CASE #1 Call Type : Fall
Eric M. Rudnick, MD, FACEP, FAAEM Medical Director Northern California EMS NOR-CAL EMS MEDICAL ADVISORY COMMITTEE RUN REVIEW, NOVEMBER 2014. meeting by Engineer Bill Bogenreif 1 CASE #1 Call Type : Fall
Idiopathic Intracranial Hypertension
 Idiopathic Intracranial Hypertension Dr. Mar'n Su+onBrown MD. FRCPC Neuro-Ophthalmology, Neurology Div of Neurology, Island Health Clinical Assistant Professor, Div of Neurology, UBC Stroke Rapid Assessment
Idiopathic Intracranial Hypertension Dr. Mar'n Su+onBrown MD. FRCPC Neuro-Ophthalmology, Neurology Div of Neurology, Island Health Clinical Assistant Professor, Div of Neurology, UBC Stroke Rapid Assessment
For the Disease Summary for this case study, see the CD-ROM. Patient s Chief Complaints. History of Present Illness
 Bruyere_Case09_034-038.qxd 5/2/08 3:09 PM Page 34 CASE STUDY 9 PULMONARY THROMBOEMBOLISM For the Disease Summary for this case study, see the CD-ROM. PATIENT CASE Patient s Chief Complaints I have severe
Bruyere_Case09_034-038.qxd 5/2/08 3:09 PM Page 34 CASE STUDY 9 PULMONARY THROMBOEMBOLISM For the Disease Summary for this case study, see the CD-ROM. PATIENT CASE Patient s Chief Complaints I have severe
UF NEUROLOGY HISTORY AND PHYSICAL GUIDELINES
 UF NEUROLOGY HISTORY AND PHYSICAL GUIDELINES HISTORY Chief Complaint A maximally succinct statement of the patient age, handedness, gender, main problem, and its duration (e.g. 56 year old right-handed
UF NEUROLOGY HISTORY AND PHYSICAL GUIDELINES HISTORY Chief Complaint A maximally succinct statement of the patient age, handedness, gender, main problem, and its duration (e.g. 56 year old right-handed
Practical Approaches to Medical Necessity
 Practical Approaches to Medical Necessity CAROLYN AVERY, CPC, CEMC CAROLYN AVERY & ASSOCIATES, PC ROBERT OSSOFF DMD, MD, CHC ASSISTANT VICE CHANCELLOR FOR COMPLIANCE &CORPORATE INTEGRITY VANDERBILT MEDICAL
Practical Approaches to Medical Necessity CAROLYN AVERY, CPC, CEMC CAROLYN AVERY & ASSOCIATES, PC ROBERT OSSOFF DMD, MD, CHC ASSISTANT VICE CHANCELLOR FOR COMPLIANCE &CORPORATE INTEGRITY VANDERBILT MEDICAL
Optic Nerve Anomalies
 Optic Nerve Anomalies Raman Bhakhri, OD, FAAO Southern California College of Optometry Marshall B. Ketchum University Goals for today Review some of the optic nerve anomalies that can be seen in practice
Optic Nerve Anomalies Raman Bhakhri, OD, FAAO Southern California College of Optometry Marshall B. Ketchum University Goals for today Review some of the optic nerve anomalies that can be seen in practice
Spontaneous Intracranial Hypotension Diagnosis and Treatment
 Spontaneous Intracranial Hypotension Diagnosis and Treatment John W. Engstrom MD, Philip R. Weinstein MD, and William P. Dillon M.D. University of California, San Francisco Spontaneous Intracranial Hypotension
Spontaneous Intracranial Hypotension Diagnosis and Treatment John W. Engstrom MD, Philip R. Weinstein MD, and William P. Dillon M.D. University of California, San Francisco Spontaneous Intracranial Hypotension
A Patient Presenting with Ptosis, Ophthalmoplegia, and Decreased Periorbital Sensations and Facial Droop in Tolosa-Hunt Syndrome
 A Patient Presenting with Ptosis, Ophthalmoplegia, and Decreased Periorbital Sensations and Facial Droop in Tolosa-Hunt Syndrome medicine2.missouri.edu/jahm/patient-presenting-ptosis-ophthalmoplegia-decreased-periorbital-sensations-facial-drooptolosa-hunt-syndrome/
A Patient Presenting with Ptosis, Ophthalmoplegia, and Decreased Periorbital Sensations and Facial Droop in Tolosa-Hunt Syndrome medicine2.missouri.edu/jahm/patient-presenting-ptosis-ophthalmoplegia-decreased-periorbital-sensations-facial-drooptolosa-hunt-syndrome/
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION
 BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
BRONCHOGENIC CARCINOMA CHALLENGES IN EVALUATION GRAND ROUND WARD 7C DATE: 25 TH MARCH 2015 PRESENTER: DR E. SAYO FACILITATOR: DR J MECHA DEMOGRAPHIC DATA NAME : CM AGE: 69 YEARS ADDRESS : KIAMBU OCCUPATION:
Karen Santucci, M.D. Professor of Pediatrics Section Chief Pediatric Emergency Medicine Yale Children s Hospital October 23, 2013
 Karen Santucci, M.D. Professor of Pediatrics Section Chief Pediatric Emergency Medicine Yale Children s Hospital October 23, 2013 But I do like Clinical Forensic Medicine and I will one day work for the
Karen Santucci, M.D. Professor of Pediatrics Section Chief Pediatric Emergency Medicine Yale Children s Hospital October 23, 2013 But I do like Clinical Forensic Medicine and I will one day work for the
Pediatric Case Studies. Case 1
 Pediatric Case Studies James Naprawa, MD Assistant Clinical Professor Pediatric Emergency Medicine Children s Hospital, Columbus Case 1 Almost 4 year old AA girl PMH UTI x 2 with abdominal pain and fever
Pediatric Case Studies James Naprawa, MD Assistant Clinical Professor Pediatric Emergency Medicine Children s Hospital, Columbus Case 1 Almost 4 year old AA girl PMH UTI x 2 with abdominal pain and fever
PHYSIOLOGY OF CSF AND PATHOPHYSIOLOGY OF HYDROCEPHALUS
 PHYSIOLOGY OF CSF AND PATHOPHYSIOLOGY OF HYDROCEPHALUS Introduction Dynamic component of CNS Invaluable tool to diagnosis Physiological reservoir of human proteome Reflects the physiologic state of CNS
PHYSIOLOGY OF CSF AND PATHOPHYSIOLOGY OF HYDROCEPHALUS Introduction Dynamic component of CNS Invaluable tool to diagnosis Physiological reservoir of human proteome Reflects the physiologic state of CNS
ID Emergencies. BGSMC Internal Medicine Edwin Yu
 ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
SURGICAL OUTCOME OF BENIGN INTRACRANIAL HYPERTENSION IN TERMS OF IMPROVEMENT IN VISION
 O R I G I N A L A R T I C L E SURGICAL OUTCOME OF BENIGN INTRACRANIAL HYPERTENSION IN TERMS OF IMPROVEMENT IN VISION Naeem ul haq 1, Naseer hassan 1, Muhammad ishaq 1,Muhammad usman 2 1Neurosurgery unit,
O R I G I N A L A R T I C L E SURGICAL OUTCOME OF BENIGN INTRACRANIAL HYPERTENSION IN TERMS OF IMPROVEMENT IN VISION Naeem ul haq 1, Naseer hassan 1, Muhammad ishaq 1,Muhammad usman 2 1Neurosurgery unit,
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
SMALL GROUP DISCUSSION
 MHD II, Seesion II Student Copy - Page 1 SMALL GROUP DISCUSSION MHD II Session II JANUARY 15, 2014 Recent Review highlighting disease process in Case 2: Fasano A, Catassi, C. NEJM 2012; 367: 2419-26 STUDENT
MHD II, Seesion II Student Copy - Page 1 SMALL GROUP DISCUSSION MHD II Session II JANUARY 15, 2014 Recent Review highlighting disease process in Case 2: Fasano A, Catassi, C. NEJM 2012; 367: 2419-26 STUDENT
ID Emergencies. BUMC-P Internal Medicine Edwin Yu
 ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
A Case of Carotid-Cavernous Fistula
 A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
Spontaneous Cerebrospinal Fluid Rhinorrhea as the Presenting Symptom of Idiopathic Intracranial Hypertension: A Case Series
 CASE REPORT Spontaneous Cerebrospinal Fluid Rhinorrhea as the Presenting Symptom of Idiopathic Intracranial Hypertension: A Case Series Hossein Ghalaenovi 1, Maziar Azar 1, Morteza Taheri 1, Mahdi Safdarian
CASE REPORT Spontaneous Cerebrospinal Fluid Rhinorrhea as the Presenting Symptom of Idiopathic Intracranial Hypertension: A Case Series Hossein Ghalaenovi 1, Maziar Azar 1, Morteza Taheri 1, Mahdi Safdarian
Med 536 Communicating About Prognosis Workshop. Case 1
 Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Patient to complete this information
 Patient to complete this information Patient s Name Birth date Today s date Referring Physician Primary Care Physician Age Occupation Retired, how long? Prior operations Medications Type Date Name Dose
Patient to complete this information Patient s Name Birth date Today s date Referring Physician Primary Care Physician Age Occupation Retired, how long? Prior operations Medications Type Date Name Dose
HEADACHES THE RED FLAGS
 HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
Evaluating an Apparent Unprovoked First Seizure in Adults
 Evaluating an Apparent Unprovoked First Seizure in Adults Case Presentation A 52 year old woman is brought to the emergency room after a witnessed seizure. She was shopping at the local mall when she was
Evaluating an Apparent Unprovoked First Seizure in Adults Case Presentation A 52 year old woman is brought to the emergency room after a witnessed seizure. She was shopping at the local mall when she was
BMB Disclosures. Papilledema can be a. Neurological Emergency, Causing Preventable Blindness
 Reasonable Doubt: Can High Intracranial Pressure Occur Without Papilledema? 15 February 2013 Jonathan C. Horton hortonj@vision.ucsf.edu http://www.ucsf.edu/hortonlab BMB Disclosures Financial Disclosures
Reasonable Doubt: Can High Intracranial Pressure Occur Without Papilledema? 15 February 2013 Jonathan C. Horton hortonj@vision.ucsf.edu http://www.ucsf.edu/hortonlab BMB Disclosures Financial Disclosures
Just Clear Them The Approach to Medical Clearance
 Just Clear Them The Approach to Medical Clearance Dr. Nalin Ahluwalia MD CCFP(EM) Associate Chief of Staff Emergency Physician Oakville Trafalgar Memorial Hospital My Disclosures None! Exemplary patient
Just Clear Them The Approach to Medical Clearance Dr. Nalin Ahluwalia MD CCFP(EM) Associate Chief of Staff Emergency Physician Oakville Trafalgar Memorial Hospital My Disclosures None! Exemplary patient
STANDARDIZED PROCEDURE LUMBAR PUNCTURE (Adult, Peds)
") I. Definition The lumbar puncture (LP) may assist in the diagnosis of meningitis, encephalitis, metastatic carcinomas, brain tumors, leukemia, demyelinating conditions, brain or spinal cord abscesses,
I. Definition The lumbar puncture (LP) may assist in the diagnosis of meningitis, encephalitis, metastatic carcinomas, brain tumors, leukemia, demyelinating conditions, brain or spinal cord abscesses,
Overview INTRODUCTION 3/15/2018. Headache Emergencies. Other way to differentiate between them? Is there an easy way to differentiate between them?
 Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Case TWO. Vital Signs: Temperature 36.6degC BP 137/89 HR 110 SpO2 97% on Room Air
 Mr N is a 64year old Chinese gentleman who is a heavy drinker, still actively drinking, and chronic smoker of >40pack year history. He has a past medical history significant for Hypertension, Hyperlipidemia,
Mr N is a 64year old Chinese gentleman who is a heavy drinker, still actively drinking, and chronic smoker of >40pack year history. He has a past medical history significant for Hypertension, Hyperlipidemia,
Objectives. Emergency Department: Rapid Fire Diagnosis 10/4/16. Why emergency medicine is unique. Approach to the emergent patient
 Emergency Department: Rapid Fire Diagnosis Julie Beard DO St. Luke s Hospital Emergency Department October 4 th, 2016 Objectives Why emergency medicine is unique Approach to the emergent patient Discuss
Emergency Department: Rapid Fire Diagnosis Julie Beard DO St. Luke s Hospital Emergency Department October 4 th, 2016 Objectives Why emergency medicine is unique Approach to the emergent patient Discuss
2/29/2016. By Lisa Amaya, Physician Assistant ATSU graduate 2006
 By Lisa Amaya, Physician Assistant ATSU graduate 2006 Identifying unusual presentations Evaluating the history of the patient Conducting a physical exam Recognize that these presentations may be subtle
By Lisa Amaya, Physician Assistant ATSU graduate 2006 Identifying unusual presentations Evaluating the history of the patient Conducting a physical exam Recognize that these presentations may be subtle
Scenario #4A: Geriatric Trauma Resuscitation Version-5
 Scenario #4A: Geriatric Trauma Resuscitation Version-5 Goals & Objectives: 1. Discuss the principles of initial assessment of a geriatric trauma patient. 2. Recognize physiologic and anatomic changes that
Scenario #4A: Geriatric Trauma Resuscitation Version-5 Goals & Objectives: 1. Discuss the principles of initial assessment of a geriatric trauma patient. 2. Recognize physiologic and anatomic changes that
SMALL GROUP DISCUSSION
 MHD II, Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION MHD II Session 1 Gastroinestinal Monday, January 9, 2017 STUDENT COPY MHD II, Session 1 Student Copy Page 2 CASE 1 CHIEF CONCERN: "I'm passing
MHD II, Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION MHD II Session 1 Gastroinestinal Monday, January 9, 2017 STUDENT COPY MHD II, Session 1 Student Copy Page 2 CASE 1 CHIEF CONCERN: "I'm passing
SMALL GROUP DISCUSSION SESSION
 MHD I Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION SESSION 1 MHD I Friday, September 4, 2015 STUDENT COPY MHD I Session 1 Student Copy Page 2 Helpful Resources for Session Murray s Medical Microbiology,
MHD I Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION SESSION 1 MHD I Friday, September 4, 2015 STUDENT COPY MHD I Session 1 Student Copy Page 2 Helpful Resources for Session Murray s Medical Microbiology,
HEADACHE. Dr Nick Pendleton. September Headache
 HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins
 ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
Patient Encounters in the Primary Care Setting
 Patient Encounters in the Primary Care Setting Carmine D Amico, D.O. Clinical Cases Overview Learning objectives Clinical case presentations Questions for audience participation 1 Clinical Cases Learning
Patient Encounters in the Primary Care Setting Carmine D Amico, D.O. Clinical Cases Overview Learning objectives Clinical case presentations Questions for audience participation 1 Clinical Cases Learning
Sudden Headache and visual disturbances in a young woman
 Sudden Headache and visual disturbances in a young woman A. Soupart, MD, PhD Department of Internal Medicine BSIM, December 12, 2014 48 years old woman with Sudden Headache 7/2014 * Admitted for Headache
Sudden Headache and visual disturbances in a young woman A. Soupart, MD, PhD Department of Internal Medicine BSIM, December 12, 2014 48 years old woman with Sudden Headache 7/2014 * Admitted for Headache
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy
 HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
Chief Complaint. History. History of Similar Episodes. A 10 Year-Old Boy With Headache
 A 10 Year-Old Boy With Headache Chief Complaint Recent Advances in Neurology 2013 10 year-old boy presented with his fifth lifetime bout of left-sided head pain followed by diplopia. Amy A. Gelfand, MD
A 10 Year-Old Boy With Headache Chief Complaint Recent Advances in Neurology 2013 10 year-old boy presented with his fifth lifetime bout of left-sided head pain followed by diplopia. Amy A. Gelfand, MD
Pain can produce unstable hemodynamics
 Pain can produce unstable hemodynamics 30-year-old male came to emergency department for severe epigastric pain for 6 hours as well as nausea and vomiting. 1)BP: 130/70mmHg 2)HR:
Pain can produce unstable hemodynamics 30-year-old male came to emergency department for severe epigastric pain for 6 hours as well as nausea and vomiting. 1)BP: 130/70mmHg 2)HR:
MARYWOOD UNIVERSITY PHYSICIAN ASSISTANT PROGRAM HISTORY, PHYSICAL, ASSESSMENT AND PLAN
 MARYWOOD UNIVERSITY PHYSICIAN ASSISTANT PROGRAM HISTORY, PHYSICAL, ASSESSMENT AND PLAN PA: PRECEPTOR: MARYWOOD STAFF: PATIENT ID: AGE: SEX: DATE: Chief Complaint: History of Present Illness: 1 Medications:
MARYWOOD UNIVERSITY PHYSICIAN ASSISTANT PROGRAM HISTORY, PHYSICAL, ASSESSMENT AND PLAN PA: PRECEPTOR: MARYWOOD STAFF: PATIENT ID: AGE: SEX: DATE: Chief Complaint: History of Present Illness: 1 Medications:
Clinician s Guide To Ordering NeuroImaging Studies
 Clinician s Guide To Ordering NeuroImaging Studies MRI CT South Jersey Radiology Associates The purpose of this general guide is to assist you in choosing the appropriate imaging test to best help your
Clinician s Guide To Ordering NeuroImaging Studies MRI CT South Jersey Radiology Associates The purpose of this general guide is to assist you in choosing the appropriate imaging test to best help your
Heart Failure with Johnny Crash: LEFT VENTRICULAR EJECTION FRACTION (LVEF) SYMPTOMATOLOGY: Assess VENTRICULAR DYSFUNCTION HEART FAILURE:
 SYMPTOMATOLOGY: Assess VENTRICULAR DYSFUNCTION HEART FAILURE:") Heart Failure with Johnny Crash: Joan E. King, PhD, ACNP-BC, ANP-BC Melissa Smith, DNP, ANP-BC Vanderbilt University School of Nursing HEART FAILURE: Heart Failure (HF): a complex clinical syndrome resulting
Heart Failure with Johnny Crash: Joan E. King, PhD, ACNP-BC, ANP-BC Melissa Smith, DNP, ANP-BC Vanderbilt University School of Nursing HEART FAILURE: Heart Failure (HF): a complex clinical syndrome resulting
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 04/26/2014 Radiology Quiz of the Week # 108 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 04/26/2014 Radiology Quiz of the Week # 108 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
The Presence of Thyroid Autoantibodies in Pregnancy
 The Presence of Thyroid Autoantibodies in Pregnancy Dr. O Sullivan does not have any financial relationships with any commercial interests. KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY ENDORAMA
The Presence of Thyroid Autoantibodies in Pregnancy Dr. O Sullivan does not have any financial relationships with any commercial interests. KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY ENDORAMA
THE DREADED RUN- ON SENTENCE AND OTHER PUNCTUATION RULES THAT KEEP YOU UP AT NIGHT!!!!
 THE DREADED RUN- ON SENTENCE AND OTHER PUNCTUATION RULES THAT KEEP YOU UP AT NIGHT!!!! Is punctuation giving you NIGHTMARES??? Does it give you a headache? When you think of punctuation, do you want to
THE DREADED RUN- ON SENTENCE AND OTHER PUNCTUATION RULES THAT KEEP YOU UP AT NIGHT!!!! Is punctuation giving you NIGHTMARES??? Does it give you a headache? When you think of punctuation, do you want to
BOARD REVIEW QUESTIONS
 September 2017 Volume 17 Issue 9 Challenging ABEM style questions for enhanced learning and deeper understanding of the EMRAP program www.emrap.org Editor-in-Chief: Mel Herbert, MD Executive Editor: Stuart
September 2017 Volume 17 Issue 9 Challenging ABEM style questions for enhanced learning and deeper understanding of the EMRAP program www.emrap.org Editor-in-Chief: Mel Herbert, MD Executive Editor: Stuart
Interpretation of laboratory values. Dóra Török
 Interpretation of laboratory values Dóra Török Normal values Age specific Gender specific Daily rhythm Laboratory specific! What is normal? Eg. Height, weight Vs. Risk Eg. Glucose, blood pressure Preanalytical
Interpretation of laboratory values Dóra Török Normal values Age specific Gender specific Daily rhythm Laboratory specific! What is normal? Eg. Height, weight Vs. Risk Eg. Glucose, blood pressure Preanalytical
Discharge Summary-Page 1
 Discharge Summary-Page 1 Admission diagnosis: 1. Gastritis. 2. Alcoholic cirrhosis, ascites, grade 1 esophageal varices. 3. Recent left knee arthroplasty. 4. Osteoporosis naqmq : 1. Three chest X-rays
Discharge Summary-Page 1 Admission diagnosis: 1. Gastritis. 2. Alcoholic cirrhosis, ascites, grade 1 esophageal varices. 3. Recent left knee arthroplasty. 4. Osteoporosis naqmq : 1. Three chest X-rays
of Trauma Assembly 27 th Page 1
 Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page