New Aspects of the Ventricular Septum and Its Function an Echocardiographic Study
|
|
|
- Camron Alexander
- 5 years ago
- Views:
Transcription
1 Heart Online First, published on March 10, 2005 as /hrt New Aspects of the Ventricular Septum and Its Function an Echocardiographic Study Petra Boettler, MD 1,2, Piet Claus, PhD 1, Lieven Herbots, MD 1, Myles McLaughlin, BSc 1, Jan D hooge, PhD 1, Bart Bijnens, PhD 1, Siew Yen Ho, PhD 3, Deniz Kececioglu, MD 2, George R. Sutherland, MD, FESC 1 1 Department of Cardiology, Catholic University of Leuven, Leuven, Belgium 2 Department of Pediatric Cardiology, Children s Hospital, Freiburg, Germany 3 Department of Paediatrics, National Heart and Lung Institute, Imperial College and Royal Brompton and Harefield NHS Trust, London, England, UK Keywords: Echocardiography, interventricular septum, tissue doppler, strain Address for correspondence: Petra Boettler Department of Cardiology Catholic University of Leuven Herestraat 49 B-3000 Leuven, Belgium petra.boettler@ .de Supported by a grant from the German Heart Foundation (Deutsche Herzstiftung) The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence on a worldwide basis to the BMJ Publishing Group Ltd and its Licensees to permit this article to be published in HEART editions and any other BMJPGL products to exploit all subsidiary rights. Heart: first published as /hrt on 10 March Downloaded from on 25 January 2019 by guest. Protected by copyright. Copyright Article author (or their employer) Produced by BMJ Publishing Group Ltd (& BCS) under licence.
2 2 ABSTRACT Objectives: Although in clinical practice the septum is considered to be one functional unit, with improved imaging techniques, a line with enhanced echogeneity in the interventricular septum (IVS) can frequently be seen. The purpose of our study was to examine whether the line dividing the septum into two layers was a consistent finding in conventional echocardiography. We also evaluated functional differences in the right (R) and left (L) side of the septum using wall thickening (WT), strain rate (SR) and strain (S) imaging. Design: In a systematic study in 30 normal subjects, M-mode and Doppler myocardial imaging (CDMI) data from the IVS were recorded. Velocity curves, regional SR and S profiles were obtained. Systolic deformation (WT and radial and longitudinal SR and S) of both sides were assessed. Furthermore, three patients with one-sided pathologies were studied. Results: The IVS could consistently be divided into a left and right part segmented by a bright echo. In this normal population radial deformation was different for the left and right side of the septum (WT L =49±46%, WT R =17±38%; SR L =3.8±0.6 1/s, SR R =2.1±1.9 1/s; S L =41±17%, S R =22±14%), while longitudinal deformation was found to be similar (SR L =-2.2±0.7 1/s, SR R =-2.0±0.6 1/s; S L =-28±12%, S R =- 25±12%). The presented clinical examples show that pathologies can be strictly limited to one layer. Conclusions: Differential radial deformation, knowledge on fiber architecture showing an abrupt change in the middle of the septum together with the clinical cases suggest the septum to be a morphologically and functionally bi-layered structure potentially supplied by different coronary arteries. Heart: first published as /hrt on 10 March Downloaded from on 25 January 2019 by guest. Protected by copyright.
3 3 INTRODUCTION A bright line within the interventricular septum (IVS) has been described by Feigenbaum[1] in a patient with a massively hypertrophied septum. It ran through the middle of the septum and was referred to as an echo of unknown origin. Although in clinical practice the septum is considered to be one functional unit, with enhanced image quality of the recent generation of echocardiographic equipment and the development of second harmonic imaging, a line with enhanced echogeneity in the IVS can frequently be seen. It has been demonstrated by numerous investigators that normal right and left ventricles do not act independently of each other and that ventricular-ventricular interaction occurs.[2][3] The role of the septum in this interaction is still not fully determined. Some authors have suggested that ventricular-ventricular interaction is caused by the shared septal wall[4], while others have suggested that the free walls affect the contralateral ventricle independently of the septum[5]. A model developed by Li et al.[6] showed the impact of septal impairment on ventricular pressure development. Li et al. showed that septal dysfunction created by glutaraldehyde injection decreased both left and right ventricular pressures. Transseptal cutting dramatically decreased left ventricular (LV) developed pressure, but had no obvious influence on right ventricular (RV) pressure. Therefore, the data showed that altering septal function affected both right and left ventricular function, but not equally. To better understand the interaction of the right-sided and left-sided part of the septum, a geometrical model has been developed by Beyar et al.[7] This model evaluated the transmural gradients in stress and strain of the left ventricle and the interventricular septum and showed that the right and left sides of the septum respond differently to various conditions such as one-sided pressure increase by alternate aortic and pulmonary arterial constrictions. In general, there are much greater inhomogeneities in stress between the layers of the septum than between the layers of the LV free wall. The development of tissue Doppler imaging allowed to evaluate differences in regional function within the septum. Fleming et al.[8] assessed total deformation of the septum by measuring the spatial distribution of the myocardial velocities between the right and left boundary of the interventricular septum and found that there is a velocity gradient within the septum as a consequence of thickening. Looking at the velocities within both sides of the septum, Kapusta et al.[9] who found them to be higher in the left side of the septum compared to the right side. In principle, velocity gradients can also be measured over portions of the wall, leading to an assessment of deformation at different locations. In addition, for the evaluation of regional differences in function of different myocardial layers newer techniques like strain and strain rate imaging can be used to detect regional differences within the layers of the left ventricular posterior wall.[10] With the development of echocardiographic equipment and techniques, a bright line in the interventricular septum became constantly detectable which separates the left (L) from the right (R) side of the septum. Functional differences such as differences in thickening, strain and strain rate of both sides of the septum have not been studied though non-linear contraction throughout the myocardium is suggested by the differing behaviours of longitudinal and circumferential fibers.[11] Heart: first published as /hrt on 10 March Downloaded from on 25 January 2019 by guest. Protected by copyright.
4 4 The purpose of our study was to examine whether the bright line dividing the septum into 2 layers was a consistent finding in conventional echocardiography. We also evaluated functional differences in the right and left side of the septum using strain and strain rate imaging in a group of 30 healthy normals. Finally, we discuss echocardiographic findings of the septum in selected clinical cases under various pathological conditions. METHODS Study Population The study group consisted of 30 healthy subjects (7 females and 23 males). All subjects were volunteers with no history of heart disease. Their ages ranged between 18 and 53 years (mean age 27.6 ± 8.2 years). None of the subjects had echocardiographic evidence of structural or functional heart disease. In all subjects, a 12-lead electrocardiogram (ECG) was performed which was normal. Bicycle testing showed the maximum oxygen uptake (VO 2 max) to be within a normal range. Standard Echocardiographic Study The echocardiographic examination was performed with the subject lying in the left lateral decubitus position. Ultrasound data were aquired using a Vingmed Vivid 7 scanner (GE, Horten, Norway) and a 3.5 MHz transducer. The images were acquired using standard and modified parasternal and apical views. Standard M-mode grey scale measurements of dimensions (LVDd, LVDs), muscle thickness (IVSd, LVPWd) and LV fractional shortening (FS) were performed. Doppler measurements with pulsed and continuous waves for all four valves were also taken. Color Doppler Myocardial Imaging Real-time 2D color Doppler myocardial imaging (CDMI) data from the interventricular septum were recorded using standard parasternal views at a frame rate of >160 frames per second. An appropriate velocity scale was chosen to avoid CDMI data aliasing. The narrowest image sector angle possible (usually 30 degrees) was used to achieve the maximum color Doppler frame rate. Three consecutive cycles were recorded during breathholding. For longitudinal deformation, DMI-data of the septum were obtained in a 4-chamber view. Careful attention was taken to keep the ultrasound beam aligned perpendicular to the posterior wall and septum when measuring radial deformation and parallel to the septum when measuring longitudinal motion. Offline Analysis Data were stored in digital format and transferred to a computer workstation for offline analysis. This allowed the computation of thickening, strain and strain rate using dedicated software (SPEQLE, K.U. Leuven, Leuven, Belgium). Thickness. To quantify the radial thickening of the left and right side of the septum, M-mode clips of a standard parasternal long axis view were analysed. The borders of both sides of the septum were delineated using the bright line within the septum as a Heart: first published as /hrt on 10 March Downloaded from on 25 January 2019 by guest. Protected by copyright.
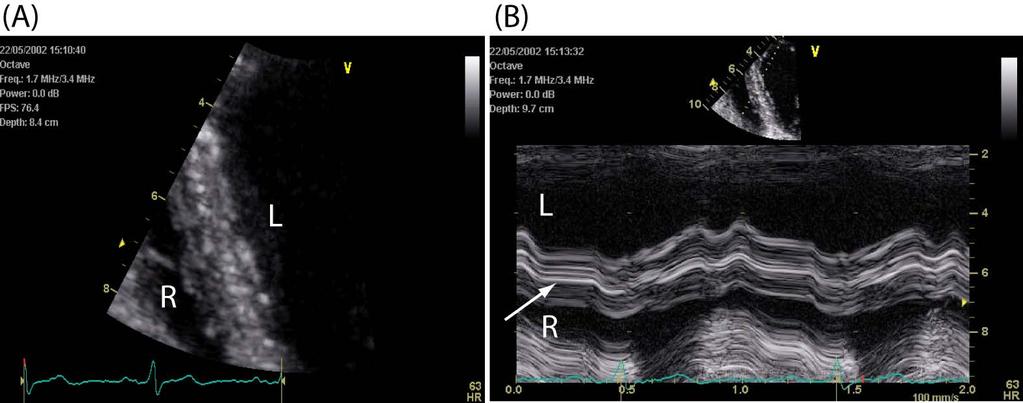
5 5 separation criterion. Timing information was added using continuous wave (CW) or pulsed wave (PW) Doppler flow curves of the aorta for defining the ejection period (from aortic valve opening to aortic valve closure). Systole was defined from beginning of QRS to end of ejection. End of diastole was considered to be at the onset of QRS (ECG trace). All timing information was aligned using ECG traces. The thickness was obtained at end-systole and end-diastole. Data were averaged over 3 consecutive cardiac cycles. Strain and strain rate. From the mean velocity curves, regional strain rate (SR) was estimated from the spatial derivative of the myocardial velocity over the computation area. For strain rate, peak values during ejection were calculated. Natural strain (S) profiles were obtained by time integrating the SR profile, which was averaged over three consecutive cardiac cycles, with end-diastole as the reference point. Lagrangian end-systolic strain values were calculated from these profiles and reported. For radial deformation, parasternal long axis views were used. The sample volumes were manually positioned in both sides of the septum. Motion was tracked throughout the cardiac cycle. To separate the right from left side of the septum the bright line was used as a boundary. As the averaged end-diastolic wall thickness of the right and the left side of the septum was 3.6 mm (right) and 5.5 mm (left), the size of the computation area was fixed to 3 mm for radial analysis. For longitudinal deformation, strain and strain rate data were obtained from a 4-chamber view. The region of interest was positioned in both sides at the mid part of the septum. Calculations of strain and strain rate were made as described above. Computation area was fixed to 10 mm for longitudinal analysis. Doppler flow curves of the aortic valve and ECG traces were used for timing as described. Statistics Values are presented as mean ± standard deviation. For comparison of thickness, wall thickening, strain and strain rate within both sides of the septum, a paired t-test was used. p<0.05 was considered statistically significant. Clinical Examples We examined three patients with one-sided pathologies such as a localized hypertrophy and myocardial infarction involving one side of the septum. In each of them, a full echocardiographic study was performed and anatomical M-mode images of the septum were taken. RESULTS Visualization of the Septum Standard 2-D and M-mode data sets could be obtained from all subjects (n=30). The data were uniformly of good quality and allowed subsequent offline analysis such as anatomical M-mode. Representative examples of a zoomed modified B-mode of the septum and the derived M-mode are shown in figure 1. It was possible to visualize the bright line within the septum in all patients. This line appeared to divide the septum in a right-sided and a left-sided layer. The line was best and most consistently visible in the 4-chamber view and it was more pronounced in diastole than in systole as can be Heart: first published as /hrt on 10 March Downloaded from on 25 January 2019 by guest. Protected by copyright.
6 6 seen in figure 1C. It could be followed from the cardiac apex to the aortic root, disappearing at the left aortic cusp. Towards the apex it could in some patients be followed to the tip of the left ventricle. As shown in table 1, standard M-mode grey scale measurements of dimensions (LVDd, LVDs), muscle thickness (IVSd, LVPWd) and LV fractional shortening (FS) were normal. Doppler measurements with pulsed and continuous waves for all four valves were also normal. Table 1: Data of standard M-mode measurements (n=30) mean s IVSd thickness [cm] LVDd diameter [cm] LVDs diameter [cm] LVPWd [cm] FS [%] Mean and standard deviation (s) of the interventricular septum diameter (IVSd), left ventricular diameter in end-diastole (LVDd), left ventricular diameter in end-systole (LVDs), left ventricular posterior wall in end-diastole (LVPWd) and fractional shortening (FS) Radial Deformation Thickness. Parasternal long axis M-modes for thickness evaluation were obtained in all patients. As shown in figure 2, end-diastolic septal thickness was significantly less on the right side of the septum than on the left side (left: 5.5 ± 1.7 mm versus right: 3.6 ± 1.4 mm versus, p<0.0001). The thickening was predominantly taking place within the left side of the septum (left: 49 ± 46 % versus right: 17 ± 39 %, p<0.002). Strain rate and strain. CDMI datasets could be obtained in all normals (n=30). Of 90 segments that have been analysed for radial deformation, 11 needed to be excluded due to suboptimal angles. The radial deformation of both sides of the septum could be quantified by using parasternal long- or short-axis views. Figure 3 compares data on radial strain rate and strain in the right and left side of the septum during ejection. Strain rate analysis showed significantly higher peak strain rate values during ejection in the left side of the septum (3.8 ± 0.6 1/s) compared to the right side of the septum (2.1 ± 1.9 1/s, p<0.05). In addition, the data showed significantly higher maximal strain values during ejection in the left than in the right part of the septum (left: 41 ± 17 % versus right: 22 ± 14 %, p<0.0001). These values are comparable to the values obtained with the M-mode technique (thickening). The higher standard deviation of the thickening data is due to the inherent limitation of segmenting M-mode data compared to quantifying Doppler images. Longitudinal Deformation Longitudinal strain and strain rate could be calculated from the DMI dataset of all patients. As shown in figure 4, peak strain rate values during ejection were similar for the left (-2.2 ± 0.7 1/s) and right (-2.0 ± 0.6 1/s) side of the septum (p=ns). Also, Heart: first published as /hrt on 10 March Downloaded from on 25 January 2019 by guest. Protected by copyright.
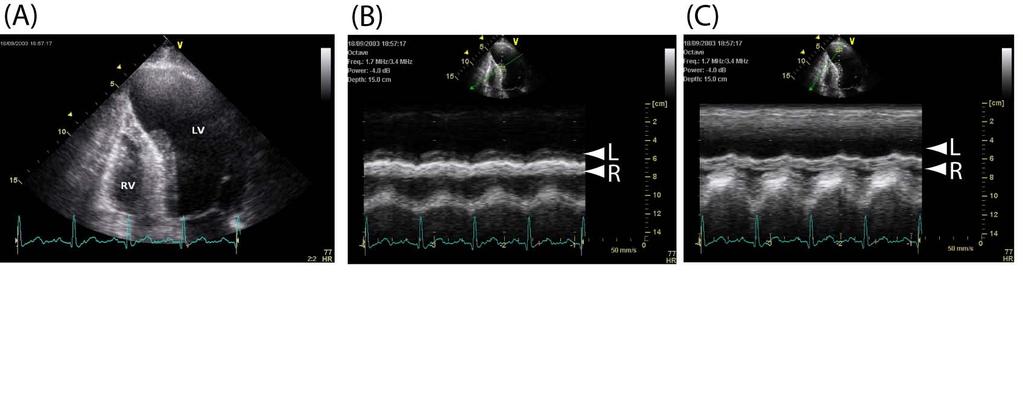
7 7 there were no significant differences in longitudinal strain between the left (-28 ± 12 %) and right (-25 ± 12 %) side of the septum (p=ns). Clinical Examples 1. Septal hypertrophy limited to the right side of the septum (figure 5) A 68 year-old asymptomatic male subject with localized nonobstructive cardiomyopathy of unknown origin was studied. The 12-lead electrocardiogram (ECG) and chest x-ray were both normal. Standard grey scale and blood pool Doppler ultrasound examination revealed a localized hypertrophic cardiomyopathy involving exclusively the right part of the septum (end diastolic wall thickness left septum 5 mm, right septum 12 mm). There was a mild tricuspid insufficiency with a maximal gradient between the right ventricle and right atrium of 30 mmhg according to a mild pulmonary hypertension. The pulmonary valve was sufficient. There was no evidence of left ventricular outflow tract obstruction (peak velocity in the outflow tract 1.4 m/sec) at rest, and there was no mitral insufficiency. The right part of the septum was equally thickened from the apex to the base. Left ventricular dimensions (LV enddiastolic diameter = 3.4 cm) and global function were normal (LV ejection fraction 59%). As shown in figure 5, the zoomed B-mode and its anatomical M-mode showed a hypertrophied right and normal left part of the septum separated by a bright line of high echogeneity. 2. Septal myocardial loss involving the left apical part (figure 6) A 58 year-old male subject presented for a routine follow-up echocardiography to our hospital. The patient s medical history was significant for a three vessel disease. A coronary angiography performed 4 years before revealed a total occlusion of the mid right coronary artery (RCA) and the mid left anterior descending artery (LAD) (various stenosis up to 100%, first lateral branch totally occluded, second lateral branch 80% stenotic). Collateral circulation from the LAD to the RCA through septal branches and from the left circumflex to the LAD through lateral branches was described and bypass surgery (left internal mammarian artery to LAD) was performed. Currently, the 12-lead electrocardiogram (ECG) showed the typical findings of an old anterolateral infarction like Q in lead II and avf. The chest x-ray was normal. In the present echocardiography, standard grey scale and blood pool Doppler ultrasound examination revealed a large myocardial infarction of the apical left part of the interventricular septum. The infarct was exclusively involving the left part of the apical septum with a normal basal septum (figure 6). The examination showed a normal right side of the septum. Left ventricular dimensions (LV enddiastolic diameter = 5.3 cm) and global function were normal (LV ejection fraction 62%). 3. Myocardial infarction involving the complete left-sided septal layer (figure 7) A 72 year-old female subject with a history of ischemic heart disease presented for a routine follow-up echocardiography. A coronary angiography 6 years before revealed a severe stenosis (up to 90%) of the proximal third of the LAD. In the present echocardiogram, the B-mode and anatomical M-mode images show a purely leftsided septal myocardial infarction. The complete loss of left-sided myocardium with preservation of the right side can be seen both in the B-mode as well as in the M- mode image (figure 7). Heart: first published as /hrt on 10 March Downloaded from on 25 January 2019 by guest. Protected by copyright.
8 8 DISCUSSION The anatomy and fiber structure of the free wall of the left ventricle have been examined in many studies [12][13][14], but surprisingly little attention has been paid to the functional morphology of the interventricular septum. Improved image quality in echocardiography has made it possible to visualize the anatomy of the septum in detail. In this study, we have shown that a bright line between the left and right side of the septum is a persistent finding in B- and M-mode images using conventional second harmonic echocardiography. Furthermore, we evaluated the myocardial deformation of the septum using thickness, strain and strain rate imaging and showed that there is a difference between both sides in the radial direction that is not present in the longitudinal direction. Since both sides of the septum are closely connected, independent longitudinal movement is prevented and they show the same longitudinal deformation (one side is influencing the other and vice versa). In radial motion they differ supposedly because radial expansion is oriented towards the left and right cavities and does not directly depend on the radial movement of the other side. The newest implementations of tissue Doppler imaging have incorporated improved spatial and temporal resolution that allows exact evaluation of regional motion. However, tethering effects of adjacent myocardium and translational heart motion can cause misinterpretation of regional wall motion.[15][16][17] The concept of a myocardial velocity gradient and strain was developed to address these problems and enables the segmental analysis of the LV independent of global heart motion.[18][19][20] However, our analysis method requires manual tracking of the septal and LV posterior wall which is time consuming. The origin of the bright line separating the septum in a left and right side, is still not known. Two main hypotheses are discussed in the following that may cause the visualized acoustic interface: Structural differences, e.g. an abrupt change in septal fiber direction, and the presence of coronary arteries in the middle of the septum. Looking at the fiber orientation of the septum, there is evidence that it is a bi-layered structure with an abrupt change in fiber direction. This was originally suggested by the studies of Lower from 1669.[21] Later studies on fiber geometry were performed by Streeter [22] and McLean [23] who found markedly different fiber directions within two main longitudinal layers, present in the interventricular septum. Alternatively, Torrent-Guasp postulated that the heart consists of a single muscle band twisted on itself in a rope-like structure with two turns in a helical fashion.[24] According to this theory, the septum consists of two parts, an ascending and a descending segment. However, Torrent-Guasp s preparations might have disrupted the syncitial arrangement of the myofibers by creating a cleavage in the septum causing an artificially bi-layered structure. Additionally, several studies have shown differences in the vascular supply and the post-occlusion flow between the two sides of the septum. Farrer-Brown et al. found that the large septal arteries originating from the anterior and posterior descending arteries give off secondary branches which supply the right and left sides of the septum.[25] Moreover, they describe different patterns of the secondary branches in both sides and suggest that functionally the interventricular septum may be devided into right and left halves by the line of the main septal arteries. Ramanathan et al. found significant differences in blood flow after acute septal artery occlusion in both Heart: first published as /hrt on 10 March Downloaded from on 25 January 2019 by guest. Protected by copyright.
9 9 sides of the septum.[26] Immediately after occlusion of the septal artery, total myocardial blood flow fell dramatically within 90 seconds, with a greater decrease on the left than on the right ventricular side of the septum. This transmural asymmetry within the septal bed is directly analogous to that seen in the free wall in many studies.[27][28] Overall, our findings are consistent with the septal anatomy previously described by Feigenbaum and the histological data of Streeter and Greenbaum. The presence of the bright line may be explained by an abrupt change in fiber direction that causes an acoustic interface seen as a hyperechogeneic signal in the image (figure 8). We found that the line can be visualized more easily in the 4-chamber view than in the parasternal views. This may be due to the different acquisition angles, which may effect the imaging of interfaces. In addition, the septal coronary artery between the right and left part of the septum as described by Farrer-Brown may contribute to the bright echogeneic signal. That might also explain that the bright line is visible more clearly during diastole when coronary flow is present and coronary artery imaging should be easier. The different deformation of the left side compared to the right side that we found can be due to the structural differences as suggested above or can be due to differences in forces and geometry. Lunkenheimer et al. showed that there are different types of forces in the myocardium (unloading and auxotonic type), that depend on the predominant directions of the fibers. [29] As shown in the clinical examples, localized pathologies may be limited to one side of the septum. For example, one side of the septum can exclusively show hypertrophy as can be seen in a patient with localized nonobstructive cardiomyopathy (figure 5) or myocardial infarction (figures 6 and 7). These findings may be due to morphological and functional differences. CONCLUSION This study shows that the septum can be consistently devided into a left and right side based on a bright echocardiographic signal. Also, differences in thickening/radial strain between the two sides are shown. These differences are not present in longitudinal motion. Knowledge on fiber architecture showing an abrupt change in the middle of the septum together with the discussed cases suggest the septum to be a morphologically and functionally bi-layered structure potentially supplied by different coronary arteries. Further studies to evaluate the clinical relevance of these findings are needed. Acknowledgement. Petra Boettler was supported by a grant from the German Heart Foundation (Deutsche Herzstiftung). Competing interest statement. There are no competing interests. Heart: first published as /hrt on 10 March Downloaded from on 25 January 2019 by guest. Protected by copyright.
10 10 REFERENCES 1 Feigenbaum H. Echocardiography. 3rd ed. Philadelphia: Lea and Febiger, 1981: Feneley MP, Gavaghan TP, Baron DW, et al. Contribution of left ventricular contraction to the generation of right ventricular systolic pressure in the human heart. Circulation. 1985;71: Santamore WP, Constantinescu M, Minczak BM, et al. Contribution of each ventricular wall to ventricular interdependence. Basic Res Cardiol. 1988;83: Brinker JA, Weiss JL, Lappe DL, et al. Leftward septal displacement during right ventricular loading in man. Circulation. 1980;61: Santamore WP, Lynch PR, Heckman JL, et al. Left ventricular effects on right ventricular developed pressure. J Appl Physiol. 1976;41: Li KS, Santamore WP. Contribution of each wall to biventricular function. Cardiovascular Research. 1993;27: Beyar R, Dong SJ, Smith ER, et al. Ventricular interaction and septal deformation: a model compared with experimental data. Am J Physiol. 1993;265:H Fleming AD, Xia X, McDicken WN, et al. Myocardial velocity gradient detected by Doppler imaging. Br J Radiol. 1994;67: Kapusta L, Thijssen JM, Cuypers MH, et al. Assessment of myocardial velocities in healthy children using tissue Doppler imaging. Ultrasound Med Biol. 2000;26(2): Hashimoto I, Li X, Hejmadi Bhat A, et al. Myocardial strain rate is a superior method for evaluation of left ventricular subendocardial function compared with tissue Doppler imaging. J Am Coll Cardiol. 2003;42: Gibson D. Regional left ventricular wall motion. Cardiac Ultrasound, ed. by J R T C Roelandt, GR Sutherland, S Iliceto and DT Linker. Churchill Livingston, Edinburgh, 1993: Greenbaum RA, Ho SY, Gibson DG, et al. Left ventricular fiber architecture in man. Br Heart J. 1981;45: Streeter DD, Spotnitz HM, Patel DP, et al. Fiber orientation in the canine left ventricle during diastole and systole. Circ. Res. 1969;24: Sanchez-Quintana D, Climent V, Ho SY, et al. Myoarchitecture and connective tissue in hearts with tricuspid atresia. Hear.t 1999;81: Heart: first published as /hrt on 10 March Downloaded from on 25 January 2019 by guest. Protected by copyright.
11 11 15 Urheim S, Edvardsen T, Torp H, et al. Myocardial strain by Doppler echocardiography. Validation of a new method to quantify regional myocardial function. Circulation. 2000;102: Abraham TP, Belohlavek M, Thomson HL, et al. Time to onset of regional relaxation: feasibility, variability and utility of a novel index of regional myocardial function by strain rate imaging. J Am Coll Cardiol. 2002;39: Edvardsen T, Skulstad H, Aakhus S, et al. Regional myocardial systolic function during acute myocardial ischemia assessed by strain Doppler echocardiography. J Am Coll Cardiol. 2001;37: Uematsu M, Nakatani S, Yamagishi M, et al. Usefulness of myocardial velocity gradient derived from two-dimensional tissue Doppler imaging as an indicator of regional myocardial contraction independent of translational motion assessed in atrial septal defect. Am J Cardiol. 1997;79: Uematsu M, Miyatake K, Tanaka N, et al. Myocardial velocity gradient as a new indicator of regional left ventricular contraction: detection by a two-dimensional tissue Doppler imaging technique. J Am Coll Cardiol. 1995;26: Tsutsui H, Uematsu M, Shimizu H, et al. Comparative usefulness of myocardial velocity gradient in detecting ischemic myocardium by a dobutamine challenge. J Am Coll Cardiol. 1998;31: Lower R. Tractatus de corde. Amstelodami apud Danielem Elzevirium, Streeter DD, Spotnitz HM, Patel DP, et al. Fiber orientation in the canine laft ventricle during diastole and systole. Circ. Res. 1969;24: McLean M, Ross, MA, Prothero J. Three-dimensional reconstruction of the myofiber pattern in the fetal and neonatal mouse heart. Anat Rec.1989;224: Torrent-Guasp F, Buckberg GD, Clemente C, et al. The structure and function of the helical heart and its buttress wrapping: the normal macroscopic structure of the heart. Semin Thorac Cardiovasc Surg. 2001;13: Farrer-Brown G, Rowles PM. Vascular supply of interventricular septum of human heart. Br Heart J. 1969;31: Ramanathan KB, Wilson JL, Mirvis DM. Effects of coronary occlusion on transmural distribution of blood flow in the interventricular septum and left ventricular free wall. Basic Res Cardiol. 1988;83: Becker LC, Ferreira R, Thomas M. Mapping of left ventricular blood flow with radioactive microspheres in experimental coronary artery occlusion. Cardiovasc Res. 1973;7: Bishop SP, White FC, Bloor CM. Regional myocardial blood flow during acute myocardial infarction in the conscious dog. Circ Res. 1976;38: Heart: first published as /hrt on 10 March Downloaded from on 25 January 2019 by guest. Protected by copyright.
12 12 29 Lunkenheimer PP, Redman K, Florek J, et al. The forces generated with the musculature of the left ventricular wall. Heart 2004;90: Heart: first published as /hrt on 10 March Downloaded from on 25 January 2019 by guest. Protected by copyright.
13 13 Figure 1: A Zoomed B-mode of a normal interventricular septum in an oblique 4- chamber view showing the right (R) and left (L) parts of the septum separated by a bright line (arrow) B Parasternal short axis view C Anatomical M-mode of the septum in the parasternal view showing a fine line in systole (S) that is brightening in diastole (D) Figure 2: Septal thickness [mm] and wall thickening [%] of the left and right septum at end-diastole and end-systole. (* p<0.0001, + p<0.002) Figure 3: Peak radial strain rate [1/s] and end-systolic strain [%] during ejection in the left and right side of the septum Figure 4: Peak longitudinal strain rate [1/s] and end-systolic strain [%] during ejection in the left and right side of the septum Figure 5: A Zoomed B-mode of the interventricular septum in an oblique 4-chamber view B Anatomical M-mode of image A showing the moderately hypertrophied right (R) and normal left (L) part of the septum separated by bright line of high echogeneity (arrow) Figure 6: A Modified 4-chamber view zoomed on the septum showing an infarcted apical part of the left-sided septum B Anatomical M-mode through the mid part of the septum showing both sides of the septum C Anatomical M-mode through the apical part of the septum showing the middle line and the right (R) part of the septum with an extremely flattened left (L) part Figure 7: A Zoomed B-mode of the interventricular septum in an oblique 4-chamber view B M-mode of image A showing a complete loss of myocardium on the left side of the septum (arrow) Figure 8: Pathology specimen of the interventricular septum showing a rapid change in fiber direction between the right-sided and mid layer of the septum Heart: first published as /hrt on 10 March Downloaded from on 25 January 2019 by guest. Protected by copyright.

14
15
16
17
18
19

20

21
Little is known about the degree and time course of
 Differential Changes in Regional Right Ventricular Function Before and After a Bilateral Lung Transplantation: An Ultrasonic Strain and Strain Rate Study Virginija Dambrauskaite, MD, Lieven Herbots, MD,
Differential Changes in Regional Right Ventricular Function Before and After a Bilateral Lung Transplantation: An Ultrasonic Strain and Strain Rate Study Virginija Dambrauskaite, MD, Lieven Herbots, MD,
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Tissue Doppler Imaging in Congenital Heart Disease
 Tissue Doppler Imaging in Congenital Heart Disease L. Youngmin Eun, M.D. Department of Pediatrics, Division of Pediatric Cardiology, Kwandong University College of Medicine The potential advantage of ultrasound
Tissue Doppler Imaging in Congenital Heart Disease L. Youngmin Eun, M.D. Department of Pediatrics, Division of Pediatric Cardiology, Kwandong University College of Medicine The potential advantage of ultrasound
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING
 PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
Advanced Multi-Layer Speckle Strain Permits Transmural Myocardial Function Analysis in Health and Disease:
 Advanced Multi-Layer Speckle Strain Permits Transmural Myocardial Function Analysis in Health and Disease: Clinical Case Examples Jeffrey C. Hill, BS, RDCS Echocardiography Laboratory, University of Massachusetts
Advanced Multi-Layer Speckle Strain Permits Transmural Myocardial Function Analysis in Health and Disease: Clinical Case Examples Jeffrey C. Hill, BS, RDCS Echocardiography Laboratory, University of Massachusetts
Mechanisms of False Positive Exercise Electrocardiography: Is False Positive Test Truly False?
 Mechanisms of False Positive Exercise Electrocardiography: Is False Positive Test Truly False? Masaki Izumo a, Kengo Suzuki b, Hidekazu Kikuchi b, Seisyo Kou b, Keisuke Kida b, Yu Eguchi b, Nobuyuki Azuma
Mechanisms of False Positive Exercise Electrocardiography: Is False Positive Test Truly False? Masaki Izumo a, Kengo Suzuki b, Hidekazu Kikuchi b, Seisyo Kou b, Keisuke Kida b, Yu Eguchi b, Nobuyuki Azuma
Carlos Eduardo Suaide Silva, Luiz Darcy Cortez Ferreira, Luciana Braz Peixoto, Claudia Gianini Monaco, Manuel Adán Gil, Juarez Ortiz
 Silva et al Original Article Arq Bras Cardiol Study of the Myocardial Contraction and Relaxation Velocities through Doppler Tissue Imaging Echocardiography. A New Alternative in the Assessment of the Segmental
Silva et al Original Article Arq Bras Cardiol Study of the Myocardial Contraction and Relaxation Velocities through Doppler Tissue Imaging Echocardiography. A New Alternative in the Assessment of the Segmental
Global left ventricular circumferential strain is a marker for both systolic and diastolic myocardial function
 Global left ventricular circumferential strain is a marker for both systolic and diastolic myocardial function Toshinari Onishi 1, Samir K. Saha 2, Daniel Ludwig 1, Erik B. Schelbert 1, David Schwartzman
Global left ventricular circumferential strain is a marker for both systolic and diastolic myocardial function Toshinari Onishi 1, Samir K. Saha 2, Daniel Ludwig 1, Erik B. Schelbert 1, David Schwartzman
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION
 LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
How does the heart pump? From sarcomere to ejection volume
 How does the heart pump? From sarcomere to ejection volume Piet Claus Cardiovascular Imaging and Dynamics Department of Cardiovascular Diseases University Leuven, Leuven, Belgium Course on deformation
How does the heart pump? From sarcomere to ejection volume Piet Claus Cardiovascular Imaging and Dynamics Department of Cardiovascular Diseases University Leuven, Leuven, Belgium Course on deformation
Strain/Untwisting/Diastolic Suction
 What Is Diastole and How to Assess It? Strain/Untwisting/Diastolic Suction James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland,
What Is Diastole and How to Assess It? Strain/Untwisting/Diastolic Suction James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland,
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Cardiac ultrasound protocols
 Cardiac ultrasound protocols IDEXX Telemedicine Consultants Two-dimensional and M-mode imaging planes Right parasternal long axis four chamber Obtained from the right side Displays the relative proportions
Cardiac ultrasound protocols IDEXX Telemedicine Consultants Two-dimensional and M-mode imaging planes Right parasternal long axis four chamber Obtained from the right side Displays the relative proportions
Tissue Doppler and Strain Imaging. Steven J. Lester MD, FRCP(C), FACC, FASE
, FACC, FASE") Tissue Doppler and Strain Imaging Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None a. Turn the wall filters on and turn down the receiver gain. b. Turn
Tissue Doppler and Strain Imaging Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None a. Turn the wall filters on and turn down the receiver gain. b. Turn
좌심실수축기능평가 Cardiac Function
 Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
Velocity Vector Imaging as a new approach for cardiac magnetic resonance: Comparison with echocardiography
 Velocity Vector Imaging as a new approach for cardiac magnetic resonance: Comparison with echocardiography Toshinari Onishi 1, Samir K. Saha 2, Daniel Ludwig 1, Erik B. Schelbert 1, David Schwartzman 1,
Velocity Vector Imaging as a new approach for cardiac magnetic resonance: Comparison with echocardiography Toshinari Onishi 1, Samir K. Saha 2, Daniel Ludwig 1, Erik B. Schelbert 1, David Schwartzman 1,
RIGHT VENTRICULAR SIZE AND FUNCTION
 RIGHT VENTRICULAR SIZE AND FUNCTION Edwin S. Tucay, MD, FPCC, FPCC, FPSE Philippine Society of Echocardiography Quezon City, Philippines Echo Mission, BRTTH, Legaspi City, July 1-2, 2016 NO DISCLOSURE
RIGHT VENTRICULAR SIZE AND FUNCTION Edwin S. Tucay, MD, FPCC, FPCC, FPSE Philippine Society of Echocardiography Quezon City, Philippines Echo Mission, BRTTH, Legaspi City, July 1-2, 2016 NO DISCLOSURE
Nancy Goldman Cutler, MD Beaumont Children s Hospital Royal Oak, Mi
 Nancy Goldman Cutler, MD Beaumont Children s Hospital Royal Oak, Mi Identify increased LV wall thickness (WT) Understand increased WT in athletes Understand hypertrophic cardiomyopathy (HCM) Enhance understanding
Nancy Goldman Cutler, MD Beaumont Children s Hospital Royal Oak, Mi Identify increased LV wall thickness (WT) Understand increased WT in athletes Understand hypertrophic cardiomyopathy (HCM) Enhance understanding
2/2/2011. Strain and Strain Rate Imaging How, Why and When? Movement vs Deformation. Doppler Myocardial Velocities. Movement. Deformation.
 Strain and Strain Rate Imaging How, Why and When? João L. Cavalcante, MD Advanced Cardiac Imaging Fellow Cleveland Clinic Foundation Disclosures: No conflicts of interest Movement vs Deformation Movement
Strain and Strain Rate Imaging How, Why and When? João L. Cavalcante, MD Advanced Cardiac Imaging Fellow Cleveland Clinic Foundation Disclosures: No conflicts of interest Movement vs Deformation Movement
Diagnostic approach to heart disease
 Diagnostic approach to heart disease Initial work up History Physical exam Chest radiographs ECG Special studies Echocardiography Cardiac catheterization Echocardiography principles Technique of producing
Diagnostic approach to heart disease Initial work up History Physical exam Chest radiographs ECG Special studies Echocardiography Cardiac catheterization Echocardiography principles Technique of producing
Strain and Strain Rate Imaging How, Why and When?
 Strain and Strain Rate Imaging How, Why and When? João L. Cavalcante, MD Advanced Cardiac Imaging Fellow Cleveland Clinic Foundation Disclosures: No conflicts of interest Movement vs Deformation Movement
Strain and Strain Rate Imaging How, Why and When? João L. Cavalcante, MD Advanced Cardiac Imaging Fellow Cleveland Clinic Foundation Disclosures: No conflicts of interest Movement vs Deformation Movement
Two-Dimensional Ultrasonic Strain Rate Measurement of the Human Heart in Vivo
 Two-Dimensional Ultrasonic Strain Rate Measurement of the Human Heart in Vivo Jan D hooge 1, Fadi Jamal 2, Bart Bijnens 2, Jan Thoen 3, Frans Van de Werf 2, George R. Sutherland 2, and Paul Suetens 1 1
Two-Dimensional Ultrasonic Strain Rate Measurement of the Human Heart in Vivo Jan D hooge 1, Fadi Jamal 2, Bart Bijnens 2, Jan Thoen 3, Frans Van de Werf 2, George R. Sutherland 2, and Paul Suetens 1 1
Velocity, strain and strain rate: Doppler and Non-Doppler methods. Thoraxcentre, Erasmus MC,Rotterdam
 Velocity, strain and strain rate: Doppler and Non-Doppler methods J Roelandt J. Roelandt Thoraxcentre, Erasmus MC,Rotterdam Basics of tissue Doppler imaging Instantaneous annular velocity profiles IVCT
Velocity, strain and strain rate: Doppler and Non-Doppler methods J Roelandt J. Roelandt Thoraxcentre, Erasmus MC,Rotterdam Basics of tissue Doppler imaging Instantaneous annular velocity profiles IVCT
Tissue Doppler and Strain Imaging
 Tissue Doppler and Strain Imaging Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 Objective way with which to quantify the minor amplitude and temporal
Tissue Doppler and Strain Imaging Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 Objective way with which to quantify the minor amplitude and temporal
Left atrial function. Aliakbar Arvandi MD
 In the clinic Left atrial function Abstract The left atrium (LA) is a left posterior cardiac chamber which is located adjacent to the esophagus. It is separated from the right atrium by the inter-atrial
In the clinic Left atrial function Abstract The left atrium (LA) is a left posterior cardiac chamber which is located adjacent to the esophagus. It is separated from the right atrium by the inter-atrial
British Society of Echocardiography
 British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
Doppler-echocardiographic findings in a patient with persisting right ventricular sinusoids
 Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 1990 Doppler-echocardiographic findings in a patient with persisting right
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 1990 Doppler-echocardiographic findings in a patient with persisting right
Tissue Doppler and Strain Imaging
 Tissue Doppler and Strain Imaging Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 Objective way with which to quantify the minor amplitude and temporal
Tissue Doppler and Strain Imaging Steven J. Lester MD, FRCP(C), FACC, FASE Relevant Financial Relationship(s) None Off Label Usage None 1 Objective way with which to quantify the minor amplitude and temporal
How NOT to miss Hypertrophic Cardiomyopathy? Adaya Weissler-Snir, MD University Health Network, University of Toronto
 How NOT to miss Hypertrophic Cardiomyopathy? Adaya Weissler-Snir, MD University Health Network, University of Toronto Introduction Hypertrophic cardiomyopathy is the most common genetic cardiomyopathy,
How NOT to miss Hypertrophic Cardiomyopathy? Adaya Weissler-Snir, MD University Health Network, University of Toronto Introduction Hypertrophic cardiomyopathy is the most common genetic cardiomyopathy,
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Grading of Myocardial Dysfunction by Tissue Doppler Echocardiography A Comparison Between Velocity, Displacement, and Strain Imaging in Acute Ischemia
 Journal of the American College of Cardiology Vol. 47, No. 8, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.01.051
Journal of the American College of Cardiology Vol. 47, No. 8, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.01.051
ASCeXAM / ReASCE. Practice Board Exam Questions Monday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
Quantification of Cardiac Chamber Size
 2017 KSE 2017-11-25 Quantification of Cardiac Chamber Size Division of Cardiology Keimyung University Dongsan Medical Center In-Cheol Kim M.D., Ph.D. LV size and function Internal linear dimensions PLX
2017 KSE 2017-11-25 Quantification of Cardiac Chamber Size Division of Cardiology Keimyung University Dongsan Medical Center In-Cheol Kim M.D., Ph.D. LV size and function Internal linear dimensions PLX
Certificate in Clinician Performed Ultrasound (CCPU) Syllabus. Rapid Cardiac Echo (RCE)
 Syllabus. Rapid Cardiac Echo (RCE)") Certificate in Clinician Performed Ultrasound (CCPU) Syllabus Rapid Cardiac Echo (RCE) Purpose: Rapid Cardiac Echocardiography (RCE) This unit is designed to cover the theoretical and practical curriculum
Certificate in Clinician Performed Ultrasound (CCPU) Syllabus Rapid Cardiac Echo (RCE) Purpose: Rapid Cardiac Echocardiography (RCE) This unit is designed to cover the theoretical and practical curriculum
How To Perform Strain Imaging; Step By Step Approach. Maryam Bo Khamseen Echotechnoligist II EACVI, ARDMS, RCS King Abdulaziz Cardiac Center- Riyadh
 How To Perform Strain Imaging; Step By Step Approach Maryam Bo Khamseen Echotechnoligist II EACVI, ARDMS, RCS King Abdulaziz Cardiac Center- Riyadh Outlines: Introduction Describe the basic of myocardium
How To Perform Strain Imaging; Step By Step Approach Maryam Bo Khamseen Echotechnoligist II EACVI, ARDMS, RCS King Abdulaziz Cardiac Center- Riyadh Outlines: Introduction Describe the basic of myocardium
DISCLOSURE. Myocardial Mechanics. Relevant Financial Relationship(s) Off Label Usage
 Off Label Usage") 7th Annual Team Echocardiography: The Heart of Cardiovascular Medicine Tissue Doppler, Strain, Speckle: What? How? Christopher J Kramer RDCS Aurora Medical Group Advanced Cardiovascular Services, Aurora
7th Annual Team Echocardiography: The Heart of Cardiovascular Medicine Tissue Doppler, Strain, Speckle: What? How? Christopher J Kramer RDCS Aurora Medical Group Advanced Cardiovascular Services, Aurora
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Introduction. Cardiac Imaging Modalities MRI. Overview. MRI (Continued) MRI (Continued) Arnaud Bistoquet 12/19/03
 MRI (Continued) Arnaud Bistoquet 12/19/03") Introduction Cardiac Imaging Modalities Arnaud Bistoquet 12/19/03 Coronary heart disease: the vessels that supply oxygen-carrying blood to the heart, become narrowed and unable to carry a normal amount
Introduction Cardiac Imaging Modalities Arnaud Bistoquet 12/19/03 Coronary heart disease: the vessels that supply oxygen-carrying blood to the heart, become narrowed and unable to carry a normal amount
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Assessment of LV systolic function
 Tutorial 5 - Assessment of LV systolic function Assessment of LV systolic function A knowledge of the LV systolic function is crucial in the undertanding of and management of unstable hemodynamics or a
Tutorial 5 - Assessment of LV systolic function Assessment of LV systolic function A knowledge of the LV systolic function is crucial in the undertanding of and management of unstable hemodynamics or a
Three-dimensional Wall Motion Tracking:
 Three-dimensional Wall Motion Tracking: A Novel Echocardiographic Method for the Assessment of Ventricular Volumes, Strain and Dyssynchrony Jeffrey C. Hill, BS, RDCS, FASE Jennifer L. Kane, RCS Gerard
Three-dimensional Wall Motion Tracking: A Novel Echocardiographic Method for the Assessment of Ventricular Volumes, Strain and Dyssynchrony Jeffrey C. Hill, BS, RDCS, FASE Jennifer L. Kane, RCS Gerard
Coronary artery disease (CAD) risk factors
 risk factors") Background Coronary artery disease (CAD) risk factors CAD Risk factors Hypertension Insulin resistance /diabetes Dyslipidemia Smoking /Obesity Male gender/ Old age Atherosclerosis Arterial stiffness precedes
Background Coronary artery disease (CAD) risk factors CAD Risk factors Hypertension Insulin resistance /diabetes Dyslipidemia Smoking /Obesity Male gender/ Old age Atherosclerosis Arterial stiffness precedes
Echocardiographic and anatomical correlates in the fetus*
 Br Heart J 1980; : 51 Echocardiographic and anatomical correlates in the fetus* LINDSEY D ALLAN, MICHAEL J TYNAN, STUART CAMPBELL, JAMES L WILKINSON, ROBERT H ANDERSON From King's College Hospital, and
Br Heart J 1980; : 51 Echocardiographic and anatomical correlates in the fetus* LINDSEY D ALLAN, MICHAEL J TYNAN, STUART CAMPBELL, JAMES L WILKINSON, ROBERT H ANDERSON From King's College Hospital, and
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
Quantitation of right ventricular dimensions and function
 SCCS Basics of cardiac assessment Quantitation of right ventricular dimensions and function Tomasz Kukulski, MD PhD Dept of Cardiology, Congenital Heart Disease and Electrotherapy Silesian Medical University
SCCS Basics of cardiac assessment Quantitation of right ventricular dimensions and function Tomasz Kukulski, MD PhD Dept of Cardiology, Congenital Heart Disease and Electrotherapy Silesian Medical University
Echocardiographic Evaluation of Mitral Annulus Excursion in Normal Horses
 Echocardiographic Evaluation of Mitral Annulus Excursion in Normal Horses Carlos Lightowler, DVM a Giuseppe Piccione, DVM b Maria Laura Cattaneo, DSS c Elisabetta Giudice, DVM, PhD d a Departamento de
Echocardiographic Evaluation of Mitral Annulus Excursion in Normal Horses Carlos Lightowler, DVM a Giuseppe Piccione, DVM b Maria Laura Cattaneo, DSS c Elisabetta Giudice, DVM, PhD d a Departamento de
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension
 ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
22 nd Annual Conference of the Saudi Heart Association Riyadh, Saudi Arabia
 22 nd Annual Conference of the Saudi Heart Association Riyadh, Saudi Arabia New Echocardiographic Modalities to Evaluate Ventricular Function in Congenital Heart Disease: Tissue Doppler & Strain Rate Imaging
22 nd Annual Conference of the Saudi Heart Association Riyadh, Saudi Arabia New Echocardiographic Modalities to Evaluate Ventricular Function in Congenital Heart Disease: Tissue Doppler & Strain Rate Imaging
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY
 가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
Cardiac hypertrophy and how it may break an athlete s heart e the Cypriot case
 Eur J Echocardiography (2005) 6, 301e307 Cardiac hypertrophy and how it may break an athlete s heart e the Cypriot case C.E. Chee a,1, C.P. Anastassiades a,1, A.G. Antonopoulos b, A.A. Petsas b, L.C. Anastassiades
Eur J Echocardiography (2005) 6, 301e307 Cardiac hypertrophy and how it may break an athlete s heart e the Cypriot case C.E. Chee a,1, C.P. Anastassiades a,1, A.G. Antonopoulos b, A.A. Petsas b, L.C. Anastassiades
Pulmonary valve echo motion in pulmonary
 British HeartJournal, I975, 37, ii84-ii90. Pulmonary valve echo motion in pulmonary regurgitation' Arthur E. Weyman, James C. Dillon, Harvey Feigenbaum, and Sonia Chang From the Department of Medicine,
British HeartJournal, I975, 37, ii84-ii90. Pulmonary valve echo motion in pulmonary regurgitation' Arthur E. Weyman, James C. Dillon, Harvey Feigenbaum, and Sonia Chang From the Department of Medicine,
Early Regional Myocardial Dysfunction in Young Patients With Duchenne Muscular Dystrophy
 Early Regional Myocardial Dysfunction in Young Patients With Duchenne Muscular Dystrophy Luc Mertens, MD, PhD, Javier Ganame, MD, PhD, Piet Claus, PhD, Nathalie Goemans, MD, Daisy Thijs, MSc, Bénédicte
Early Regional Myocardial Dysfunction in Young Patients With Duchenne Muscular Dystrophy Luc Mertens, MD, PhD, Javier Ganame, MD, PhD, Piet Claus, PhD, Nathalie Goemans, MD, Daisy Thijs, MSc, Bénédicte
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital
 Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
VECTORS OF CONTRACTION
 1/3/216 Strain, Strain Rate, and Torsion: Myocardial Mechanics Simplified and Applied VECTORS OF CONTRACTION John Gorcsan, MD University of Pittsburgh, Pittsburgh, PA Shortening Thickening Twisting No
1/3/216 Strain, Strain Rate, and Torsion: Myocardial Mechanics Simplified and Applied VECTORS OF CONTRACTION John Gorcsan, MD University of Pittsburgh, Pittsburgh, PA Shortening Thickening Twisting No
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
Martin G. Keane, MD, FASE Temple University School of Medicine
 Martin G. Keane, MD, FASE Temple University School of Medicine Measurement of end-diastolic LV internal diameter (LVIDd) made by properly-oriented M-Mode techniques in the Parasternal Long Axis View (PLAX):
Martin G. Keane, MD, FASE Temple University School of Medicine Measurement of end-diastolic LV internal diameter (LVIDd) made by properly-oriented M-Mode techniques in the Parasternal Long Axis View (PLAX):
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
Atrial Septal Defects
 Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
The importance of left atrium in LV diastolic function
 II Baltic Heart Failure Meeting and Congress of Latvian Society of Cardiology The importance of left atrium in LV diastolic function Dr. Artem Kalinin Eastern Clinical University Hospital Riga 30.09.2010.
II Baltic Heart Failure Meeting and Congress of Latvian Society of Cardiology The importance of left atrium in LV diastolic function Dr. Artem Kalinin Eastern Clinical University Hospital Riga 30.09.2010.
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
B-Mode measurements protocols:
 Application Note How to Perform the Most Commonly Used Measurements from the Cardiac Measurements Package associated with Calculations of Cardiac Function using the Vevo Lab Objective The Vevo LAB offline
Application Note How to Perform the Most Commonly Used Measurements from the Cardiac Measurements Package associated with Calculations of Cardiac Function using the Vevo Lab Objective The Vevo LAB offline
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Supplemental methods Pericardium In several studies, it has been shown that the pericardium significantly modulates ventricular interaction. 1-4 Since ventricular interaction has
SUPPLEMENTAL MATERIAL Supplemental methods Pericardium In several studies, it has been shown that the pericardium significantly modulates ventricular interaction. 1-4 Since ventricular interaction has
Cardiac Chamber Quantification by Echocardiography
 Cardiac Chamber Quantification by Echocardiography Maryam Bokhamseen, RCS, RCDS, EACVI Echotechnologist ǁ, Non invasive Cardiac Laboratory King Abdulaziz Cardiac Center. Outline: Introduction. Background
Cardiac Chamber Quantification by Echocardiography Maryam Bokhamseen, RCS, RCDS, EACVI Echotechnologist ǁ, Non invasive Cardiac Laboratory King Abdulaziz Cardiac Center. Outline: Introduction. Background
Lab 16. The Cardiovascular System Heart and Blood Vessels. Laboratory Objectives
 Lab 16 The Cardiovascular System Heart and Blood Vessels Laboratory Objectives Describe the anatomical structures of the heart to include the pericardium, chambers, valves, and major vessels. Describe
Lab 16 The Cardiovascular System Heart and Blood Vessels Laboratory Objectives Describe the anatomical structures of the heart to include the pericardium, chambers, valves, and major vessels. Describe
Novel echocardiographic modalities: 3D echo, speckle tracking and strain rate imaging. Potential roles in sports cardiology. Stefano Caselli, MD, PhD
 Novel echocardiographic modalities: 3D echo, speckle tracking and strain rate imaging. Potential roles in sports cardiology. Stefano Caselli, MD, PhD Ospedale San Pietro Fatebenefratelli Rome, Italy Differential
Novel echocardiographic modalities: 3D echo, speckle tracking and strain rate imaging. Potential roles in sports cardiology. Stefano Caselli, MD, PhD Ospedale San Pietro Fatebenefratelli Rome, Italy Differential
The Normal Echocardiogram
 The Normal Echocardiogram Pravin V. Patil, MD FACC Lewis Katz School of Medicine at Temple University Acknowledgments Dr. Susan Wiegers Dr. Martin Keane Temple Cardiac Sonographers Disclosures No relevant
The Normal Echocardiogram Pravin V. Patil, MD FACC Lewis Katz School of Medicine at Temple University Acknowledgments Dr. Susan Wiegers Dr. Martin Keane Temple Cardiac Sonographers Disclosures No relevant
Case 1. Case 2. Case 3
 Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
Vevo 2100 System Cardio Measurements. Dieter Fuchs, PhD FUJIFILM VisualSonics, Inc.
 Vevo 2100 System Cardio Measurements Dieter Fuchs, PhD FUJIFILM VisualSonics, Inc. dfuchs@visualsonics.com Instructions This document is a guideline on how to assess cardiac function in rodents imaged
Vevo 2100 System Cardio Measurements Dieter Fuchs, PhD FUJIFILM VisualSonics, Inc. dfuchs@visualsonics.com Instructions This document is a guideline on how to assess cardiac function in rodents imaged
Qualitative and Quantitative Assessment of Perfusion
 APCDE 2011 Qualitative and Quantitative Assessment of Perfusion Hyun Ju Yoon Chonnam National University Hospital Gwangju, Korea ISCHEMIC CASCADE Blood flow mismatch Perfusion defects on nuclear imaging,
APCDE 2011 Qualitative and Quantitative Assessment of Perfusion Hyun Ju Yoon Chonnam National University Hospital Gwangju, Korea ISCHEMIC CASCADE Blood flow mismatch Perfusion defects on nuclear imaging,
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Case 47 Clinical Presentation
 93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
Multimodality Imaging of Anomalous Left Coronary Artery from the Pulmonary
 1 IMAGES IN CARDIOVASCULAR ULTRASOUND 2 3 4 Multimodality Imaging of Anomalous Left Coronary Artery from the Pulmonary Artery 5 6 7 Byung Gyu Kim, MD 1, Sung Woo Cho, MD 1, Dae Hyun Hwang, MD 2 and Jong
1 IMAGES IN CARDIOVASCULAR ULTRASOUND 2 3 4 Multimodality Imaging of Anomalous Left Coronary Artery from the Pulmonary Artery 5 6 7 Byung Gyu Kim, MD 1, Sung Woo Cho, MD 1, Dae Hyun Hwang, MD 2 and Jong
Pathophysiology and Current Evidence for Detection of Dyssynchrony
 Editorial Cardiol Res. 2017;8(5):179-183 Pathophysiology and Current Evidence for Detection of Dyssynchrony Michael Spartalis a, d, Eleni Tzatzaki a, Eleftherios Spartalis b, Christos Damaskos b, Antonios
Editorial Cardiol Res. 2017;8(5):179-183 Pathophysiology and Current Evidence for Detection of Dyssynchrony Michael Spartalis a, d, Eleni Tzatzaki a, Eleftherios Spartalis b, Christos Damaskos b, Antonios
Global and Regional Myocardial Function Quantification by Two-Dimensional Strain Application in Hypertrophic Cardiomyopathy
 Journal of the American College of Cardiology Vol. 47, No. 6, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2005.10.061
Journal of the American College of Cardiology Vol. 47, No. 6, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2005.10.061
The background of the Cardiac Sonographer Network News masthead is a diagnostic image:
 Number 5 Welcome Number 5 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Number 5 Welcome Number 5 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Assessment of right ventricular function by tissue Doppler in relation to plasma NT-proBNP concentration in patients with dilated cardiomyopathy
 ORIGINAL ARTICLE Cardiology Journal 2007, Vol. 14, No. 2, pp. 167 173 Copyright 2007 Via Medica ISSN 1507 4145 Assessment of right ventricular function by tissue Doppler in relation to plasma NT-proBNP
ORIGINAL ARTICLE Cardiology Journal 2007, Vol. 14, No. 2, pp. 167 173 Copyright 2007 Via Medica ISSN 1507 4145 Assessment of right ventricular function by tissue Doppler in relation to plasma NT-proBNP
Index. K Knobology, TTE artifact, image resolution, ultrasound, 14
 A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment
 Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Strain imaging in children: from Tissue Doppler to 3 D
 Strain imaging in children: from Tissue Doppler to 3 D Mark kk. Friedberg Fi Outline Deformation in the fetus and neonate Deformation in pediatric cardiomyopathy y (briefly!) Deformation in Congenital
Strain imaging in children: from Tissue Doppler to 3 D Mark kk. Friedberg Fi Outline Deformation in the fetus and neonate Deformation in pediatric cardiomyopathy y (briefly!) Deformation in Congenital
Echocardiography Conference
 Echocardiography Conference David Stultz, MD Cardiology Fellow, PGY-6 September 20, 2005 Atrial Septal Aneurysm Bulging of Fossa Ovalis Associated commonly with Atrial septal defect or small perforations
Echocardiography Conference David Stultz, MD Cardiology Fellow, PGY-6 September 20, 2005 Atrial Septal Aneurysm Bulging of Fossa Ovalis Associated commonly with Atrial septal defect or small perforations
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Pulmonary arteriovenous fistula
 International Journal of Medical Imaging 2014; 2(2): 34-38 Published online April 10, 2014 (http://www.sciencepublishinggroup.com/j/ijmi) doi: 10.11648/j.ijmi.20140202.16 Pulmonary arteriovenous fistula
International Journal of Medical Imaging 2014; 2(2): 34-38 Published online April 10, 2014 (http://www.sciencepublishinggroup.com/j/ijmi) doi: 10.11648/j.ijmi.20140202.16 Pulmonary arteriovenous fistula
Tissue Doppler Imaging
 Cronicon OPEN ACCESS Hesham Rashid* Tissue Doppler Imaging CARDIOLOGY Editorial Department of Cardiology, Benha University, Egypt *Corresponding Author: Hesham Rashid, Department of Cardiology, Benha University,
Cronicon OPEN ACCESS Hesham Rashid* Tissue Doppler Imaging CARDIOLOGY Editorial Department of Cardiology, Benha University, Egypt *Corresponding Author: Hesham Rashid, Department of Cardiology, Benha University,
Preface: Wang s Viewpoints
 AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Diastology Disclosures: None. Dias2011:1
 Diastology 2011 James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Disclosures: None Dias2011:1 Is EVERYBODY a member!?!
Diastology 2011 James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Disclosures: None Dias2011:1 Is EVERYBODY a member!?!
Doppler Basic & Hemodynamic Calculations
 Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
PRELIMINARY STUDIES OF LEFT VENTRICULAR WALL THICKNESS AND MASS OF NORMOTENSIVE AND HYPERTENSIVE SUBJECTS USING M-MODE ECHOCARDIOGRAPHY
 Malaysian Journal of Medical Sciences, Vol. 9, No. 1, January 22 (28-33) ORIGINAL ARTICLE PRELIMINARY STUDIES OF LEFT VENTRICULAR WALL THICKNESS AND MASS OF NORMOTENSIVE AND HYPERTENSIVE SUBJECTS USING
Malaysian Journal of Medical Sciences, Vol. 9, No. 1, January 22 (28-33) ORIGINAL ARTICLE PRELIMINARY STUDIES OF LEFT VENTRICULAR WALL THICKNESS AND MASS OF NORMOTENSIVE AND HYPERTENSIVE SUBJECTS USING
Practical Echocardiography: ECHOES in the REAL WORLD Know When to Hold Em and When to Fold Em
 Practical Echocardiography: ECHOES in the REAL WORLD Know When to Hold Em and When to Fold Em Introduction The use of ultrasound in private veterinary practice is continuing to grow. The popularity of
Practical Echocardiography: ECHOES in the REAL WORLD Know When to Hold Em and When to Fold Em Introduction The use of ultrasound in private veterinary practice is continuing to grow. The popularity of
Effect of loading and geometry on functional parameters
 Effect of loading and geometry on functional parameters Piet Claus Cardiovascular Imaging and Dynamics Department of Cardiovascular Diseases Leuven University, Leuven, Belgium 5 th European Echocardiography
Effect of loading and geometry on functional parameters Piet Claus Cardiovascular Imaging and Dynamics Department of Cardiovascular Diseases Leuven University, Leuven, Belgium 5 th European Echocardiography
Lab Activity 23. Cardiac Anatomy. Portland Community College BI 232
 Lab Activity 23 Cardiac Anatomy Portland Community College BI 232 Cardiac Muscle Histology Branching cells Intercalated disc: contains many gap junctions connecting the adjacent cell cytoplasm, creates
Lab Activity 23 Cardiac Anatomy Portland Community College BI 232 Cardiac Muscle Histology Branching cells Intercalated disc: contains many gap junctions connecting the adjacent cell cytoplasm, creates
Value of echocardiography in chronic dyspnea
 Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
Rotation: Echocardiography: Transthoracic Echocardiography (TTE)
") Rotation: Echocardiography: Transthoracic Echocardiography (TTE) Rotation Format and Responsibilities: Fellows rotate in the echocardiography laboratory in each clinical year. Rotations during the first
Rotation: Echocardiography: Transthoracic Echocardiography (TTE) Rotation Format and Responsibilities: Fellows rotate in the echocardiography laboratory in each clinical year. Rotations during the first
Patient-specific modeling of heart and circulation
 Patient-specific modeling of heart and circulation Theo Arts t.arts@bf.unimaas.nl Maastricht University, *Maastricht University Hospital **University of Tecnology, Eindhoven The Netherlands *Tammo Delhaas,
Patient-specific modeling of heart and circulation Theo Arts t.arts@bf.unimaas.nl Maastricht University, *Maastricht University Hospital **University of Tecnology, Eindhoven The Netherlands *Tammo Delhaas,
Coronary Anomalies & Hemodynamic Identification
 Coronary Anomalies & Hemodynamic Identification David Stultz, MD Cardiology Fellow, PGY 6 May 2, 2006 Anomaly #1 Anomaly #2 Anomaly #3 Figure 18-27 Anomalous origin of the left circumflex artery.
Coronary Anomalies & Hemodynamic Identification David Stultz, MD Cardiology Fellow, PGY 6 May 2, 2006 Anomaly #1 Anomaly #2 Anomaly #3 Figure 18-27 Anomalous origin of the left circumflex artery.