L17: Acute. Kidney Injury
|
|
|
- Meghan Barnett
- 6 years ago
- Views:
Transcription


1 L17: Acute Kidney Injury
2 objectives 1. Define Acute Kidney Injury 2. Know the epidemiology of Acute Kidney Injury 3. Know the etiology of Acute Kidney Injury 4. Manage Acute Kidney Injury 5. Diagnose Acute Kidney Injury 6. Treat Acute Kidney Injury Color index: Step up to medicine, slide, Doctor s note, Davidson, Extra Explanation
3 3 Definition of AKI Definition: A rapid decline in renal function, with an increase in serum creatinine level ARF (acute renal failure) in one study was defined as: a 0.5 mg/dl increase in serum creatinine if the baseline serum creatinine was 1.9 mg/dl, an 1.0 mg/dl increase in serum creatinine if the baseline serum creatinine was 2.0 to 4.9 mg/dl, and a 1.5 mg/dl increase in serum creatinine if the baseline serum creatinine was 5.0 mg/dl An abrupt sudden (within 48 hours) absolute increase in creatinine by 0.3 mg/dl (26.4 µmol/l) or percentage increase of >50% from base line or urine output <0.5 ml/hour for 6 hours The creatinine may be normal despite a markedly reduced glomerular filtration rate (GFR) in the early stages of AKI due to the time it takes for creatinine to accumulate in the body. This condition is also called acute renal failure (ARF).
4 4 Epidemiology It occurs in 5%of all hospitalized patients and 35% of those in intensive care units Mortality is high: up to 75 90% in patients with sepsis 35 45% in those without
5 5 The RIFLE criteria for AKI : 1.5-fold increase in the serum creatinine or GFR decrease by 25% or urine output <0.5 ml/kg/hour for 6 hours (RISK) Twofold increase in the serum creatinine or GFR decrease by 50% or urine output <0.5 ml/kg/hour for 12 hours (INJURY) Threefold increase in the serum creatinine or GFR decrease by 75% or urine output of <0.5 ml/kg/hour for 24 hours, or anuria for 12 hours (FAILURE) Complete loss of kidney function (i.e., requiring dialysis) for more than 4 weeks (LOSS) Complete loss of kidney function (i.e., requiring dialysis) for more than 3 months (ESRD)
6 6 Signs & Symptoms 1. oliguric, anuric, or non-oliguric 2. Weight gain and edema are the most common clinical findings this is due to a positive water and sodium (Na+) Balance. 3. Characterized by azotemia abnormally high levels of nitrogen-containing compounds (such as urea, creatinine, various body waste compounds, and other nitrogen-rich compounds) in the blood (elevated BUN and Cr). Nota that: Elevated BUN blood urea nitrogen is also seen with catabolic drugs (e.g., steroids), GI/soft tissue bleeding, and dietary protein intake. Elevated Cr is also seen with increased muscle breakdown and various drugs. The baseline Cr level varies proportionately with muscle mass.
7 7 Correlation between AKI classification and outcome: No AKI AKI I AKI II AKI III 65.6% 19.1% 3.8% 12.5% Urine Output <0.5 ml/kg/h for >6 h <0.5 ml/kg/h for >12 h <0.3 ml/kg/h for >24 h OR Anuria for >12 h Creatinine criteria times baseline OR 0.3 mg/dl increase from baseline ( 26.4 μmol/l) 2-3 tims baseline 3 times baseline OR 0.5 mg/dl (44 μmol/l) increase if baseline > 4mg/dl( 354 μmol/l) OR Any renal replacement therapy given Mean age ICU mortality 10.7% 20.1% 25.9% 49.6% Hospital mortality Length of stay in ICU (median) 16.9% 29.9% 35.8% 57.9% 2 d 5 d 8 d 9 d
 4-Vascular disorder Post Renal 1-Ureteric obstruction 2-Bladder neck obstruction 3-Urethral obstruction Clinical Consequences: A. Chronic Kidney disease B.")
8 8 Types of AKI causes Pre renal 1-Volume depletion 2-Decreased cardiac output 3- hypotension 4- renal artery occlusion Renal 1-Acute Tubular necrosis (ATN) 2-Acute interstitial nephritis (AIN 3-Acute Glomerulonephritis (GN) 4-Vascular disorder Post Renal 1-Ureteric obstruction 2-Bladder neck obstruction 3-Urethral obstruction Clinical Consequences: A. Chronic Kidney disease B. End Stage Renal Disease C. Hospitalization D. Mortality
9 9 Pre-renal failure Most common cause of AKI. Potentially reversible. decrease in systemic arterial blood volume (renal perfusion) or can complicate any disease that causes: hypovolemia. Or, low cardiac output. Or, systemic vasodilatation.






, 2/ACE inhibitors (cause")


10 10 Etiology Hypovolemia Hypotension Renal arterial obstruction decreased renal perfusion Decreased cardiac output 1/dehydration 2/excessive diuretic use, 3/poor fluid intake, 4/vomiting, 5/diarrhea, 6/ Cutaneous losses (burns) 7/hemorrhage 8/Pancreatitis 1/sepsis, 2/excessive antihypertensive medications, 3/bleeding, 4/dehydration *Stenosis (kidney is hypoperfused despite elevated blood pressure.) 1/NSAIDs (constrict afferent arteriole), 2/ACE inhibitors (cause efferent arteriole vasodilation) 3/cyclosporin. Heart failure Pulmonary embolus Acute myocardial infarction Severe valvular heart disease Abdominal compartment syndrome (tense ascites) Cirrhosis, hepatorenal syndrome
")
.")
 as possible.")

11 11 Pathophysiology Renal blood flow decreases lower the GFR decreased clearance of metabolites (BUN, Cr, uremic toxins) Because the renal parenchyma is undamaged, so tubular function is preserved(and therefore the concentrating ability). Therefore, the kidney responds appropriately, conserving as much (sodium + water) as possible. This form of AKI is reversible on restoration of blood flow; but if hypoperfusion persists, ischemia results and can lead to acute tubular necrosis (ATN) (as a renal causes)

![*always found in prerenal failure (this is to preserve volume) **(<20 meq/l with fractional excretion of sodium [FENa] <1%) because Na+ is avidly reabsorbed](/docs-images/72/67639075/images/12-4.jpg "***(>20:1 is the classic ratio) because kidney can reabsorb urea (>500 mosm/kg H2O) because the kidney is able to reabsorb water (>40:1) because much of the")
12 12 Clinical features and Laboratory findings signs of volume depletion: dry mucous. Membranes. Hypotension. Tachycardia. Decreased tissue turgor. oliguria/anuria*. 1-Decrease -urine Na+** 2-Increase -BUN-to-serum Cr ratio*** - urine osmolality -urine plasma Cr ratio 3-Bland urine sediment. *always found in prerenal failure (this is to preserve volume) **(<20 meq/l with fractional excretion of sodium [FENa] <1%) because Na+ is avidly reabsorbed ***(>20:1 is the classic ratio) because kidney can reabsorb urea (>500 mosm/kg H2O) because the kidney is able to reabsorb water (>40:1) because much of the filtrate is reabsorbed (but not the creatinine)

 Causes Generally 2- Glomerular disease *Anti glomerular")
 ***Immune complex GN 3- Interstitial")

13 13 renal failure Kidney tissue is damaged such that glomerular filtration and tubular function are significantly impaired. The kidneys are unable to concentrate urine effectively. 1- Tubular disease (ATN) Causes Generally 2- Glomerular disease *Anti glomerular basement membrane (GBM) disease **Anti neutrophil cytoplasmic antibody-associated glomerulonephritis (ANCA-associated GN) ***Immune complex GN 3- Interstitial disease 1/ischemia (most common cause), 2/nephrotoxins 1/Goodpasture s syndrome* 2/Wegener s granulomatosis** 3/poststreptococcal GN, lupus*** 1/allergic interstitial nephritis often due to hypersensitivity reaction to medication.
14 14 1- Tubular Necrosis (ATN) Causes of Acute Tubular Necrosis (ATN): Ischemic AKI: Secondary to severe decline in renal blood flow, as in shock, hemorrhage, sepsis, disseminated intravascular coagulation, heart failure, so Ischemia will results in the death of tubular cells. Nephrotoxic AKI: Injury secondary to substances (e.g: contrast, gentamicins: aminoglycosides and vancomycin,nsaids poisons, myoglobinuria (from muscle damage, rhabdomyolysis, strenuous exercise),hemoglobinuria (from hemolysis), chemotherapeutic drugs (cisplatin), and kappa and gamma light chainsproduced in multiple myeloma) that directly injure renal parenchyma and result in cell death.


15 15 Clinical features and Laboratory findings Decrease Clinical features: depend on the cause. Edema is usually present. Recovery may be possible but takes longer than in prerenal failure. 1/ BUN-to-serum Cr ratio* 2/urine osmolality** 3/urine plasma Cr ratio*** Increase urine Na+ * (<20:1, typically closer to 10:1 ratio) in comparison with prerenal failure. Both BUN and Cr levels are still elevated, but less urea is reabsorbed than in prerenal failure. **(<350 mosm/kg H2O) because renal water reabsorption is impaired ***(<20:1) because filtrate cannot be reabsorbed) (>40 meq/l with FENa > 2% to 3%) because Na+ is poorly reabsorbed
16 16 Pre renal vs ATN Pre renal Acute Tubular necrosis (ATN) Urea/ Creatinine ration >20: :1 Urine Normal Muddy brown casts Urine Osmolality > 500 <350 Urine Na <20 >20 Fractional excretion of Na <1 % > 1% Rhabdomyolysis Tubular disease 1. Skeletal muscle breakdown caused by trauma, crush injuries, prolonged immobility, seizures, snake bites. 2. Release of muscle fiber contents (myoglobin) into bloodstream. Myoglobin is toxic to kidneys, which can lead to AKI. 3. Lab findings include markedly elevated creatine phosphokinase (CPK), hyperkalemia, hypocalcemia,hyperuricemia and Hb is positive. 4. Treatment with IV fluids, mannitol (osmotic diuretic) and bicarbonate (drives K back into cells).
17 17 Course of ATN Onset (insult) Oliguric phase: -Azotemia and uremia average length 10 to 14 days -Urine output <400 to 500 ml/day Diuretic phase: -Begins when urine output is >500 ml/day -High urine output due to the following: fluid overload (excretion of retained salt, water, other solutes that were retained during oliguric phase),osmotic diuresis due to retained solutes during oliguric phase tubular cell damage (delayed recovery of epithelial cell function relative to GFR) Recovery phase recovery of tubular function
18 18 2- Acute Glomerulonephritis Rare in the hospitalized patient Diagnose by history, hematuria, RBC casts, proteinuria (usually non-nephrotic range), low serum complement in post-infectious GN), RPGN often associated with anti-gbm or ANCA Usually will need to perform renal biopsy
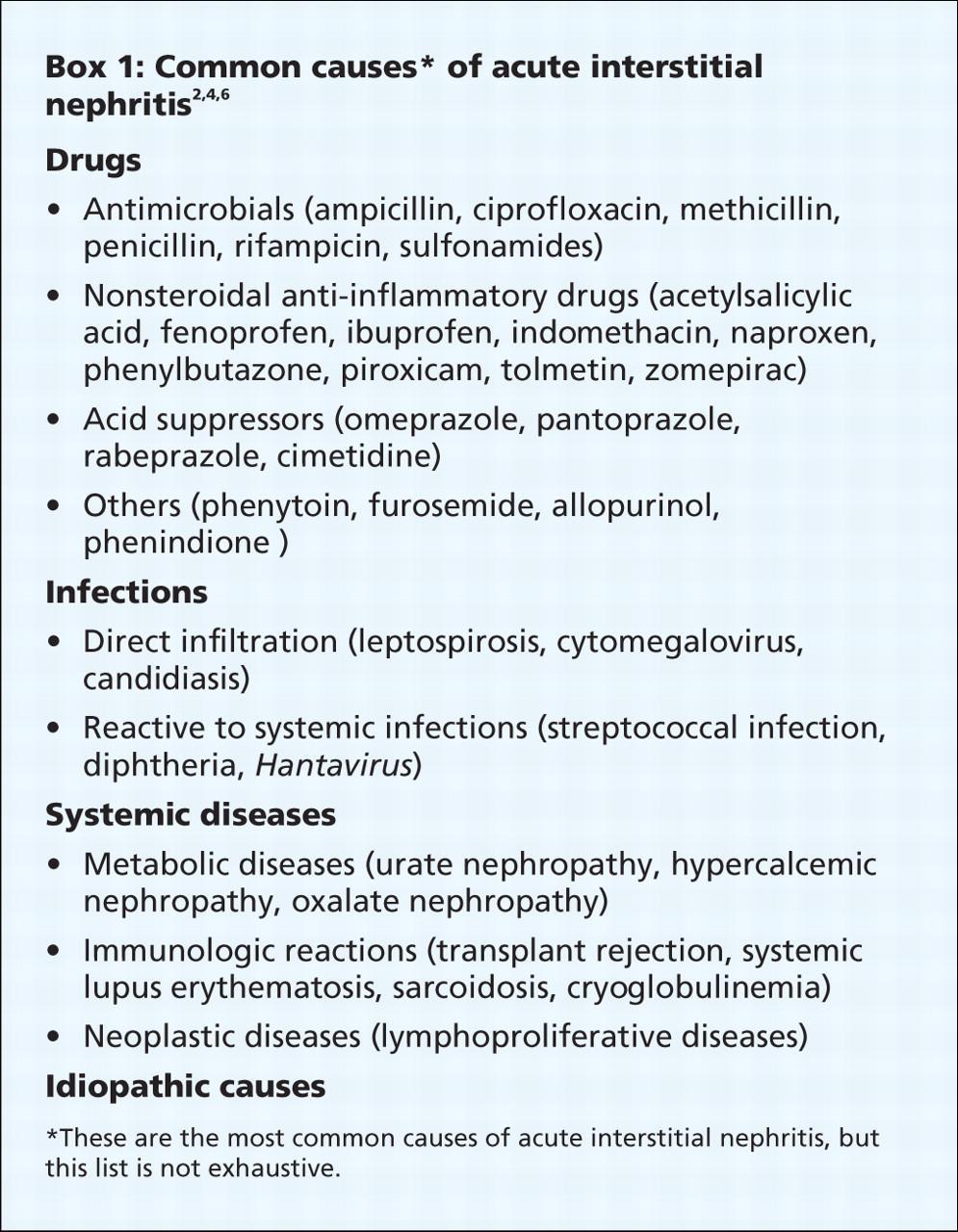
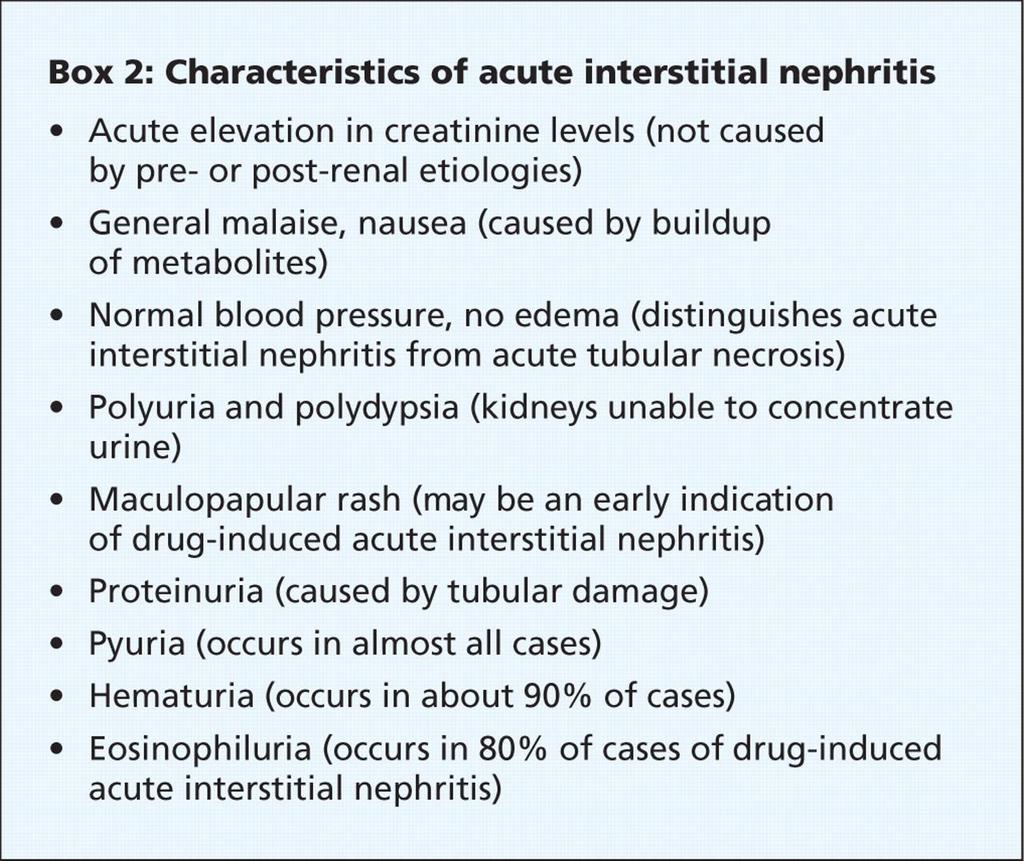
19 19 3- Interstitial disease
20 20 Postrenal failure a. Least common cause of AKI b. Obstruction of any segment of the urinary tract (with intact kidney, Blood supply and renal parenchyma are intact as well ) causes increased tubular pressure (urine produced cannot be excreted), which leads to decreased GFR, and note that both kidneys must be obstructed for creatinine to rise. c. Renal function is restored if obstruction is relieved before the kidneys are damaged. d. Postrenal obstruction, if untreated, can lead to ATN.
21 21 Causes Ureteric obstruction Stone disease, Tumor, Fibrosis, Ligation during pelvic surgery Bladder neck obstruction Retroperitoneal fibrosis Benign prostatic hypertrophy [BPH] Cancer of the prostate Neurogenic bladder Drugs(Tricyclic antidepressants, ganglion blockers, Bladder tumor, Stone disease, hemorrhage/clot) Urethral obstruction (strictures, tumor), (BPH) is the most common cause. Urethral obstruction is an uncommon cause because obstruction must be bilateral to cause renal failure. Retroperitoneal fibrosis
22 22 Urine Osmolality 1. Urine osmolality is a measure of urine concentration. The higher the osmolality, the more concentrated the urine. 2. Dehydration in a healthy person leads to increase in urine concentration (osmolality) as follows: Dehydration causes low intravascular volume, which triggers ADH release, which stimulates reabsorption of water from kidney to fill the vasculature. Increased water reabsorption leads to more concentrated urine. 3. In ATN, the tubule cells are damaged and cannot reabsorb water (or sodium); so the urine cannot be concentrated, which leads to low urine osmolality.
23 23 Diagnosis Blood tests a. Elevation in BUN and Cr levels b. Electrolytes (K+, Ca2+, PO4), albumin levels, CBC with differential Urine culture CT scan Renal biopsy Renal arteriography Renal ultrasound if infection is suspected (abdomen and pelvis) may be helpful in some cases; usually done if renal ultrasound shows an abnormality such as hydronephrosis biopsy useful occasionally if there is suspicion of acute GN or acute allergic interstitial nephritis evaluate for possible renal artery occlusion; should be performed only if specific therapy will make a difference a. Useful for evaluating kidney size and for excluding urinary tract obstruction (i.e., postrenal failure) presence of bilateral hydronephrosis or hydroureter b. Order for most patients with AKI unless the cause of the AKI is obvious and is not postrenal
24 24 Diagnosis Urinalysis Urine chemistry a. A dipstick test positive for protein (3+, 4+) suggests intrinsic renal failure due to glomerular insult. b. Microscopic examination of the urine sediment is very helpful. Hyaline casts are devoid of contents (seen in prerenal failure). Muddy brown casts leading to muddy brown urine indicates ATN. RBC casts indicate AGN. WBC casts indicate AIN. Fatty casts indicate nephrotic syndrome. According to Doctor s slides: urinalysis is unremarkable in pre and post renal causes distinguish between different forms of AKI a. Urine Na+, Cr, and osmolality: Urine Na+ depends on dietary intake. b. FENa: collect urine and plasma electrolytes simultaneously = [(UNa)/(PNa)/ (UCr)/PCr) 100], where U = urine and P = plasma. Values below 1% suggest prerenal failure. Values above 2% to 3% suggest ATN. FENa is most useful if oliguria is present. c. Renal failure index 5 (una/[ucr/pcr]) 100) Values below 1% suggest prerenal failure. Values above 1% suggest ATN.

25 25 Diagnosis
26 26 Complications 1/ECF volume expansion and resulting pulmonary edema treat with a diuretic (furosemide) 2/Metabolic : a. Hyperkalemia due to decreased excretion of K+ and the movement of potassium from ICF to ECF due to tissue destruction and acidosis b. Metabolic acidosis (with increased anion gap) due to decreased excretion of hydrogen ions; if severe (below 16 meq/l), correct with sodium bicarbonate c. Hypocalcemia loss of ability to form active vitamin D and rapid development of PTH resistance d. Hyponatremia may occur if water intake is greater than body losses, or if a volume-depleted patient consumes excessive hypotonic solutions. (Hypernatremia may also be seen in hypovolemic states.) e. Hyperphosphatemia f. Hyperuricemia
27 27 Complications 3/Uremia toxic end products of metabolism accumulate (especially from protein metabolism). 4/Infection: A common and serious complication of AKI (occurs in 50% to 60% of cases). The cause is probably multifactorial, but uremia itself is thought to impair immune functions,examples include pneumonia, UTI, wound infection, and sepsis.
28 28 Prognosis factor Severity of renal failure Underlying health of patient Clinical circumstances Magnitude of increase in Cr Presence of oliguria Fractional excretion of sodium Requirement for dialysis Duration of severe renal failure Marked abnormalities on urinalysis Age Presence, severity, and reversibility of underlying disease Cause of renal failure Severity and reversibility of acute process(es) Number and type of other failed organ systems Development of sepsis and other complications
29 29 Management Obtain the following in any patient with AKI: Urinalysis Urine chemistry Serum electrolytes (Na+,K+, BUN, Cr), CBC Bladder catheterization to rule out obstruction (diagnostic and therapeutic) Renal ultrasound to look for obstruction
30 30 Treatment 1. General measures: a. Avoid medications that decrease renal blood flow (NSAIDs) and/or that are nephrotoxic (e.g., aminoglycosides, radiocontrast agents). b. Adjust medication dosages for level of renal function. c. Correct fluid imbalance. If the patient is volume depleted, give IV fluids. However, many patients with AKI are volume overloaded (especially if they are oliguric or anuric), so diuresis may be necessary. The goal is to strike a balance between correcting volume deficits and avoiding volume overload (while maintaining adequate urine output). Monitor fluid balance by daily weight measurements (most accurate estimate) and intake output records. Be sure to take into account the patient s cardiac history when considering treatment options for fluid imbalances (i.e., do not give excessive fluid to a patient with CHF) Balanced salt solution, such as Hartmann s or Ringer s lactate, may be preferable to isotonic (0.9%) saline when large volume of fluid resuscitation are required.
31 31 Treatment d. Correct electrolyte disturbances if present. e. Optimize cardiac output. BP should be approximately 120 to 140/80 to 90. f. Order dialysis if symptomatic uremia, intractable acidemia, hyperkalemia, or volume overload develop. g. Pulmonary edema may result from the administration of excess amounts of fluids. If pulmonary edema if present and urine output cannot be rapidly restored, treament with dialysis may be required to remove excess fluid. h. Critically ill patients may require inotropic drugs to restore an effictive blood pressure but clinical trials do not support a specific role for low-dose dopamine.
32 32 Treatment 2. Prerenal: a. Treat the underlying disorder. b. Give NS to maintain euvolemia and restore blood pressure do not give to patients with edema or ascites. Stopping antihypertensive medications may be necessary. c. Eliminate any offending agents (ACE inhibitors, NSAIDs). d. If the patient is unstable, Swan Ganz monitoring is indicated for accurate assessment of intravascular volume. 3. Intrinsic: a. Once ATN develops, therapy is supportive. Eliminate the cause/offending agent. b. If the patient is oliguric, a trial of furosemide may help to increase urine flow. This improves fluid balance. 4. Postrenal a bladder catheter may be inserted to decompress the urinary tract. Consider urology consultation
33 33 Renal replacement therapy Renal replacement therapy (RRT) may be required in patients who are not showing signs of recovery. Typically, the decision to start RRT is driven by hyperkalemia, fluid over load or acidosis. The decision to institute RRT should be made on an individual basis, taking account of the potential risks and benefits, comorbidity and other aspects of the patient care. The two main options for RRT in AKI are hemodialysis and high-volume hemofiltration.
34 34 Contrast nephropathy hours post exposure, peaks in 3-5 days Non-oliguric, FE Na <1%!! RX/Prevention: 1/2 NS 1 cc/kg/hr 12 hours pre/post N-acetyle cystein 600 BID pre/post (4 doses) Risk Factors: CKD, Older age Hypovolemia,DM,CHF Atheroembolic ARF Associated with emboli of fragments of atherosclerotic plaque from aorta and other large arteries Diagnose by history, physical findings (evidence of other embolic phenomena--cva, ischemic digits, blue toe syndrome, etc), low serum C3 and C4, peripheral eosinophilia, eosinophiluria, rarely WBC casts Commonly occur after intravascular procedures or cannulation (cardiac cath, CABG, AAA repair, etc.)
, CBC Bladder catheterization to rule out.")


35 35 Quick Hit Obtain the following in any patient with AKI Urinalysis Urine chemistry Serum electrolytes (Na+, K+, BUN, Cr), CBC Bladder catheterization to rule out. obstruction (diagnostic and therapeutic) Renal ultrasound to look for Obstruction. Diagnosis of AKI is usually made by finding elevated BUN and Cr levels. The patient is usually asymptomatic. Three basic tests for postrenal failure Physical examination palpate the bladder Ultrasound look for obstruction, hydronephrosis Catheter look for large volume of urine Note that prerenal azotemia and ischemic AKI are part of a spectrum of manifestations of renal hypoperfusion. The latter differs in that injury to renal tubular cells occurs.


 by causing spasm of the afferent arteriole.")

36 36 Quick Hit Monitoring a patient with AKI Daily weights, intake, and output BP Serum electrolytes Watch Hb and Hct for anemia Watch for infection In evaluating a patient with AKI, first exclude prerenal and postrenal causes, and then, if necessary, investigate intrinsic renal causes Radiographic contrast media can cause ATN (typically very rapidly) by causing spasm of the afferent arteriole. It can be prevented with saline hydration. In the early phase of AKI, the most common mortal complications are hyperkalemic cardiac arrest and pulmonary edema.
37 MCQs 1/ A 73-year-old man undergoes abdominal aortic aneurysm repair. The patient develops hypotension to 80/50 for approximately 20 minutes during the procedure according to the anesthesia record. He received 4 units of packed red blood cells. Postoperatively his blood pressure is 110/70, heart rate is 110, surgical wound is clean, and a Foley catheter is in place. Over the next 2 days his urine output slowly decreases. His creatinine on post-operative day 3 is 3.5 mg/dl (baseline 1.2). His sodium is 140 meq/l, K 4.6 meql and BUN 50 mg/dl. Hemoglobin and hematocrit are stable. Urinalysis shows occasional granular casts but otherwise is normal. Urine sodium is 50 meq/l, urine osmolality is 290 mosmol/l, and urine creatinine is 35 mg/dl. The FeNa (fractional excretion of sodium) based on these data is 35. What is the most likely cause of this acute renal failure? A) Acute interstitial nephritis B) Acute glomerulonephritis C) Acute tubular necrosis D) Pre-renal azotemia E) Contrast induced nephropathy 2/ A 47 year-old HIV-positive man is brought to the emergency room because of weakness. The patient has HIV nephropathy and adrenal insufficiency because. He takes trimethoprim-sulfamethoxazole for PCP prophylaxis and is on triple agent antiretroviral treatment. He was recently started on spironolactone for ascites due to alcoholic liver disease. Physical examination reveals normal vital signs, but his muscles are diffusely weak. Frequent extrasystoles are noted. He has mild ascites and 1+ peripheral edema. Laboratory studies show a serum creatinine of 2.5 with a potassium value of 7.3 meq/l. An EKG shows peaking of the T waves and QRS duration of What is the most important immediate treatment? A) Sodium polystyrene sulfonate (Kayexalate) B) Acute hemodialysis C) IV normal saline D) IV calcium gluconate E) IV furosemide 80 mg stat
38 MCQs 3/ An 85 year-old man who resides in a nursing home 3 days history of lower abdominal pain and unceasing fatigue and lethargy. He is afebrile, his BP is 160/92, and RR 16. His lungs are clear and his heart examination normal. There is diffuse abdominal tenderness on palpitation and a large area of fullness and dullness to percussion starting just below the umbilicus and extending to the suprapubic area. His serum sodium is 130 meq/l, potassium 4.9 meq/l, BUN 75 mg/dl, and creatinine is 3.5 mg/dl. His baseline BUN and creatinine were 25 and 1.3 respectively as recently as 1 month ago. A Foley catheter is placed and 1200 cc of urine is obtained. What will be the likely clinical course for this patient with regard to his renal function? A) His creatinine will continue to rise slowly for 2 to 3 more days B) His creatinine will return to 1.3 over the next week. C) He will require dialysis within 24 hours D) He will produce minimal urinary output for at least 3 days. E) His renal function is unlikely to show any improvement in the futur and 3.5 will be his new baseline. 4/ A 63 year old man alcoholic with a 50-pack-year history of smoking presents to the emergency room with fatigue and confusion. Physical examination reveals a blood pressure of 110/70 with no orthostatic change. Heart, lungs and abdominal examinations are normal and there is no pedal edema. Laboratory data are as follows : Na : 110 meq/l, K :37 meq/l Cl: 82 meq/l, HCO3 : 20 meq/l,glucose: 100 mg/dl, BUN : 5 mg/dl Creatinine: 0.7 mg/dl Urinalysis: normal,specific gravity: Which of the following is the most likely diagnosis? A) Volume depletion B) Inappropriate secretion of antidiuretic hormone C) Psychogenic polydipsia D) Cirrhosis E) Congestive heart failure
39 MCQs 5/ A 50 year old diabetic woman presents for follow-up of her hypertension. Her blood pressure is 152/96 in the office today and she brings in that consistently in the same range over the past month. Her current medications are amlodipine 5 mg daily and hydrochlorothiazide 25 mg daily. The diuretic was added when she developed peripheral edema on the amlodipine ; now she has only trace peripheral edema. A spot urine specimen shows 280 mg of albumin per mg creatinine ( microalbuminuria is present if this value is between 30 and 300 mg/mg ) What would be the best next therapeutic step in this patient? A) Add clonidine. B) Add a beta-blocker. C) Increase the thiazide diuretic dose. D) Add an alpha-blocker. E) Add angiotensin-converting enzyme inhibitor or angiotensin receptor blocker. 6/ which of the following renal disease will cause severe decrease in urine output "anuria"? A) BPH B) Unilateral kidney stone C) Tumor in one ureter D) Rhabdomyolysis 7/What is the most common diagnostic test used for hydronephrosis? A) CT B) X-Ray C) MRI D) Ultrasound Answers : 1-C 2-D 3-B 4-B 5-E 6-A 7-D



40 Medicine433 Medicine433 DONE BY Faroq Abdulfattah Faisal Bazhair Raneem Alotaibi munira ahmed Abdullah Alatar Omar AlDahaas Medicine is a science of uncertainty and an art of probability
Acute Kidney Injury. I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS
 Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management
 Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management") AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Dr.Nahid Osman Ahmed 1
 1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University
 RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
Acute Kidney Injury (AKI)
") (Last Updated: 08/22/2018) Created by: Socco, Samantha Acute Kidney Injury (AKI) Thambi, M. (2017). Acute Kidney Injury. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. AKI This
(Last Updated: 08/22/2018) Created by: Socco, Samantha Acute Kidney Injury (AKI) Thambi, M. (2017). Acute Kidney Injury. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. AKI This
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS. Myriam Farah, MD, FRCPC
 ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
Acute Kidney Injury in the ED
 + Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
+ Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
Alterations of Renal and Urinary Tract Function
 Alterations of Renal and Urinary Tract Function Chapter 29 Urinary Tract Obstruction Urinary tract obstruction is an interference with the flow of urine at any site along the urinary tract The obstruction
Alterations of Renal and Urinary Tract Function Chapter 29 Urinary Tract Obstruction Urinary tract obstruction is an interference with the flow of urine at any site along the urinary tract The obstruction
Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009
 www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers HOW
www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers HOW
Introduction to Clinical Diagnosis Nephrology
 Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
AN UPDATE ON THE RECOGNITION, PREVENTION, AND MANAGEMENT OF ACUTE KIDNEY DISEASE IN DOGS AND CATS
 AN UPDATE ON THE RECOGNITION, PREVENTION, AND MANAGEMENT OF ACUTE KIDNEY DISEASE IN DOGS AND CATS Richard E. Goldstein DVM, Dip. ACVIM, Dip. ECVIM-CA The Animal Medical Center New York, NY Azotemia refers
AN UPDATE ON THE RECOGNITION, PREVENTION, AND MANAGEMENT OF ACUTE KIDNEY DISEASE IN DOGS AND CATS Richard E. Goldstein DVM, Dip. ACVIM, Dip. ECVIM-CA The Animal Medical Center New York, NY Azotemia refers
A Practical Approach to Acute Kidney Injury
 A Practical Approach to Acute Kidney Injury Elise Barney, DO Nephrologist Phoenix VA Medical Center Clinical Assistant Professor, Medicine University of Arizona College of Medicine A Tribute to the Kidney!
A Practical Approach to Acute Kidney Injury Elise Barney, DO Nephrologist Phoenix VA Medical Center Clinical Assistant Professor, Medicine University of Arizona College of Medicine A Tribute to the Kidney!
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
HIHIM 409 7/26/2009. Kidney and Nephron. Fermamdo Vega, M.D. 1
 Function of the Kidneys Nephrology Fernando Vega, M.D. Seattle Healing Arts Center Remove Wastes Regulate Blood Pressure Regulate Blood Volume Regulates Electrolytes Converts Vitamin D to active form Produces
Function of the Kidneys Nephrology Fernando Vega, M.D. Seattle Healing Arts Center Remove Wastes Regulate Blood Pressure Regulate Blood Volume Regulates Electrolytes Converts Vitamin D to active form Produces
Non-protein nitrogenous substances (NPN)
") Non-protein nitrogenous substances (NPN) A simple, inexpensive screening test a routine urinalysis is often the first test conducted if kidney problems are suspected. A small, randomly collected urine
Non-protein nitrogenous substances (NPN) A simple, inexpensive screening test a routine urinalysis is often the first test conducted if kidney problems are suspected. A small, randomly collected urine
Acute kidney injury definition, causes and pathophysiology. Financial Disclosure. Some History Trivia. Key Points. What is AKI
 Acute kidney injury definition, causes and pathophysiology Financial Disclosure Current support: Center for Sepsis and Critical Illness Award P50 GM-111152 from the National Institute of General Medical
Acute kidney injury definition, causes and pathophysiology Financial Disclosure Current support: Center for Sepsis and Critical Illness Award P50 GM-111152 from the National Institute of General Medical
Scientific adviser: ass.prof Makharynska O.S Head of department: prof. Yabluchansky M.I.
 Scientific adviser: ass.prof Makharynska O.S Head of department: prof. Yabluchansky M.I. Structure: Acute Renal failure (ARF) definition Anatomy and physiology of kidneys ARF diagnostic criterias ARF -
Scientific adviser: ass.prof Makharynska O.S Head of department: prof. Yabluchansky M.I. Structure: Acute Renal failure (ARF) definition Anatomy and physiology of kidneys ARF diagnostic criterias ARF -
Acute Kidney Injury. Eleanor Haskey BSc(hons) RVN VTS(ECC) VPAC A1
 RVN VTS(ECC) VPAC A1") Acute Kidney Injury Eleanor Haskey BSc(hons) RVN VTS(ECC) VPAC A1 Anatomy and Physiology The role of the kidneys is to filter the blood through the glomerulus to form filtrate. The filtrate is then reabsorbed
Acute Kidney Injury Eleanor Haskey BSc(hons) RVN VTS(ECC) VPAC A1 Anatomy and Physiology The role of the kidneys is to filter the blood through the glomerulus to form filtrate. The filtrate is then reabsorbed
** Accordingly GFR can be estimated by using one urine sample and do creatinine testing.
 This sheet includes the lecture and last year s exam. When a patient goes to a clinic, we order 2 tests: 1) kidney function test: in which we measure UREA and CREATININE levels, and electrolytes (Na+,
This sheet includes the lecture and last year s exam. When a patient goes to a clinic, we order 2 tests: 1) kidney function test: in which we measure UREA and CREATININE levels, and electrolytes (Na+,
Acute kidney injury. Dr P Sigwadi Paediatric nephrology
 Acute kidney injury Dr P Sigwadi Paediatric nephrology Introduction Is common in critically ill patients e.g. post cardiac surgery Occurs when renal function is diminished to a point where body fluid and
Acute kidney injury Dr P Sigwadi Paediatric nephrology Introduction Is common in critically ill patients e.g. post cardiac surgery Occurs when renal function is diminished to a point where body fluid and
OBJECTVES OF LEARNING
 OBJECTVES OF LEARNING ACUTE RENAL FAILURE AND RENAL REPLACEMENT THERAPY DR.TAI CHENG SHENG RECOGNITION OF DEFINITION OF ARF RECOGNITION OF CAUSE OF ARF RECOGNITION OF PATHOGENESIS OF ARF RECOGNITION OF
OBJECTVES OF LEARNING ACUTE RENAL FAILURE AND RENAL REPLACEMENT THERAPY DR.TAI CHENG SHENG RECOGNITION OF DEFINITION OF ARF RECOGNITION OF CAUSE OF ARF RECOGNITION OF PATHOGENESIS OF ARF RECOGNITION OF
1. Disorders of glomerular filtration
 RENAL DISEASES 1. Disorders of glomerular filtration 2. Nephrotic syndrome 3. Disorders of tubular transport 4. Oliguria and polyuria 5. Nephrolithiasis 6. Disturbances of renal blood flow 7. Acute renal
RENAL DISEASES 1. Disorders of glomerular filtration 2. Nephrotic syndrome 3. Disorders of tubular transport 4. Oliguria and polyuria 5. Nephrolithiasis 6. Disturbances of renal blood flow 7. Acute renal
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
A&P of the Urinary System
 A&P of the Urinary System Week 44 1 Objectives Identify the organs of the urinary system, from a Identify the parts of the nephron (the functional unit List the characteristics of a normal urine specimen.
A&P of the Urinary System Week 44 1 Objectives Identify the organs of the urinary system, from a Identify the parts of the nephron (the functional unit List the characteristics of a normal urine specimen.
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
THE CLINICAL BIOCHEMISTRY OF KIDNEY FUNCTIONS. Dr Boldizsár CZÉH
 THE CLINICAL BIOCHEMISTRY OF KIDNEY FUNCTIONS Dr Boldizsár CZÉH The kidneys are vital organs Functional unit: Nephron RENAL FUNCTIONS Electrolyte & Fluid Balances Acid-Base Balances Elimination of Metabolic
THE CLINICAL BIOCHEMISTRY OF KIDNEY FUNCTIONS Dr Boldizsár CZÉH The kidneys are vital organs Functional unit: Nephron RENAL FUNCTIONS Electrolyte & Fluid Balances Acid-Base Balances Elimination of Metabolic
DIAGNOSIS AND INVESTIGATIONS (Table 13.3) 362 INTENSIVE CARE
 362 INTENSIVE CARE") 362 INTENSIVE CARE the administration of NSAIDs, an ACE inhibitor or an angiotensin II receptor blocker during an episode of renal underperfusion. Dangerous hyperkalaemia, out of proportion to the degree
362 INTENSIVE CARE the administration of NSAIDs, an ACE inhibitor or an angiotensin II receptor blocker during an episode of renal underperfusion. Dangerous hyperkalaemia, out of proportion to the degree
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
Dr Rodney Itaki Lecturer Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology
 Acute Renal Failure & Malaria Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Definitions Inability of
Acute Renal Failure & Malaria Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Definitions Inability of
Nephrology - the study of the kidney. Urology - branch of medicine dealing with the male and female urinary systems and the male reproductive system
 Urinary System Nephrology - the study of the kidney Urology - branch of medicine dealing with the male and female urinary systems and the male reproductive system Functions of the Urinary System 1. Regulation
Urinary System Nephrology - the study of the kidney Urology - branch of medicine dealing with the male and female urinary systems and the male reproductive system Functions of the Urinary System 1. Regulation
RENAL PHYSIOLOGY. Zekeriyya ALANOGLU, MD, DESA Ahmet Onat Bermede, MD, Ankara University School of Medicine Dept. Anesthesiology and ICM
 RENAL PHYSIOLOGY Zekeriyya ALANOGLU, MD, DESA Ahmet Onat Bermede, MD, Ankara University School of Medicine Dept. Anesthesiology and ICM Kidneys Stabilize the composition of the ECF (electrolyte, H
RENAL PHYSIOLOGY Zekeriyya ALANOGLU, MD, DESA Ahmet Onat Bermede, MD, Ankara University School of Medicine Dept. Anesthesiology and ICM Kidneys Stabilize the composition of the ECF (electrolyte, H
RENAL PHYSIOLOGY. Zekeriyya ALANOGLU, MD, DESA. Ahmet Onat Bermede, MD. Ankara University School of Medicine Dept. Anesthesiology and ICM
 RENAL PHYSIOLOGY Zekeriyya ALANOGLU, MD, DESA. Ahmet Onat Bermede, MD. Ankara University School of Medicine Dept. Anesthesiology and ICM Kidneys Stabilize the composition of the ECF (electrolyte,
RENAL PHYSIOLOGY Zekeriyya ALANOGLU, MD, DESA. Ahmet Onat Bermede, MD. Ankara University School of Medicine Dept. Anesthesiology and ICM Kidneys Stabilize the composition of the ECF (electrolyte,
Kidney Disorders. Renal cysts. Policystic Kidney Diseases. Cystic Renal Dysplasia. Autosomal-Dominant (Adult) Polycystic
 Polycystic") Policystic Kidney Diseases Kidney Disorders CONGENITAL CYSTIC GLOMERULAR TUBULES/INTERSTITIUM BLOOD VESSELS OBSTRUCTION TUMORS Lecture : Genito-urinary system. 11 08 2010. Renal cysts Cystic Renal Dysplasia
Policystic Kidney Diseases Kidney Disorders CONGENITAL CYSTIC GLOMERULAR TUBULES/INTERSTITIUM BLOOD VESSELS OBSTRUCTION TUMORS Lecture : Genito-urinary system. 11 08 2010. Renal cysts Cystic Renal Dysplasia
Clinical Significance of ARF. Hospital Acquired Renal Insufficiency. Case - Acute Renal Failure. Hospital Acquired Renal Insufficiency
 Case - Acute Renal Failure 73 yo diabetic F w hx of mild HBP but normal renal function develops infection of R foot. Over 1 week fever, chills, inflammation swelling of her R foot and leg. She takes Motrin
Case - Acute Renal Failure 73 yo diabetic F w hx of mild HBP but normal renal function develops infection of R foot. Over 1 week fever, chills, inflammation swelling of her R foot and leg. She takes Motrin
Acute Kidney Injury for the General Surgeon
 Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Acute Renal Failure. Dr Kawa Ahmad
 62 Acute Renal Failure Dr Kawa Ahmad Acute Renal Failure It is characterised by an abrupt reduction (usually within a 48- h period) in kidney function. This results in an accumulation of nitrogenous waste
62 Acute Renal Failure Dr Kawa Ahmad Acute Renal Failure It is characterised by an abrupt reduction (usually within a 48- h period) in kidney function. This results in an accumulation of nitrogenous waste
Advanced Concept of Nursing- II UNIT-VI Advance Nursing Management of Genitourinary (GU) Diseases.
 Diseases.") In The Name of God (A PROJECT OF NEW LIFE COLLEGE OF NURSING KARACHI) Advanced Concept of Nursing- II UNIT-VI Advance Nursing Management of Genitourinary (GU) Diseases. Shahzad Bashir RN, BScN, DCHN,MScN
In The Name of God (A PROJECT OF NEW LIFE COLLEGE OF NURSING KARACHI) Advanced Concept of Nursing- II UNIT-VI Advance Nursing Management of Genitourinary (GU) Diseases. Shahzad Bashir RN, BScN, DCHN,MScN
HTN, retenopathy, edema, encephalopathy
 ARF Uremic syndrom Uremic syndrome (uremia) is a serious complication of CRF & ARF. It occurs when urea and other waste products build up in the body because the kidneys are unable to eliminate them. These
ARF Uremic syndrom Uremic syndrome (uremia) is a serious complication of CRF & ARF. It occurs when urea and other waste products build up in the body because the kidneys are unable to eliminate them. These
Acute Renal Failure aka Acute Kidney Injury. Dr H Bierman
 Acute Renal Failure aka Acute Kidney Injury Dr H Bierman RIFLE criteria for diagnosis of AKI based on The Acute Dialysis Quality Initiative Increase in S Cr Urine output Risk of renal injury Injury to
Acute Renal Failure aka Acute Kidney Injury Dr H Bierman RIFLE criteria for diagnosis of AKI based on The Acute Dialysis Quality Initiative Increase in S Cr Urine output Risk of renal injury Injury to
Renal Transporters- pathophysiology of drug - induced renal disorders. Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November
 Renal Transporters- pathophysiology of drug - induced renal disorders Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November Renal Failure Up to 25% of acute renal failure is drug induced
Renal Transporters- pathophysiology of drug - induced renal disorders Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November Renal Failure Up to 25% of acute renal failure is drug induced
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Renal diseases. Acute renal failure Chronic renal failure Nephrotic syndrome
 Renal diseases Acute renal failure Chronic renal failure Nephrotic syndrome Acute renal failure Acute renal failure (ARF) is characterized by sudden loss of the ability of the kidneys: to excrete wastes
Renal diseases Acute renal failure Chronic renal failure Nephrotic syndrome Acute renal failure Acute renal failure (ARF) is characterized by sudden loss of the ability of the kidneys: to excrete wastes
Chapter 23. Composition and Properties of Urine
 Chapter 23 Composition and Properties of Urine Composition and Properties of Urine (1 of 2) urinalysis the examination of the physical and chemical properties of urine appearance - clear, almost colorless
Chapter 23 Composition and Properties of Urine Composition and Properties of Urine (1 of 2) urinalysis the examination of the physical and chemical properties of urine appearance - clear, almost colorless
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC
 RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Acute Kidney Injury. Editing file Feedback. Color index: IMPORTANT - NOTES - EXTRA - Books
 Acute Kidney Injury Objectives: Define Acute Kidney Injury Discuss the epidemiology of Acute Kidney Injury Discuss the etiology of Acute Kidney Injury Describe the management of Acute Kidney Injury: Diagnose
Acute Kidney Injury Objectives: Define Acute Kidney Injury Discuss the epidemiology of Acute Kidney Injury Discuss the etiology of Acute Kidney Injury Describe the management of Acute Kidney Injury: Diagnose
Hydronephrosis. What is hydronephrosis?
 What is hydronephrosis? Hydronephrosis Hydronephrosis describes the situation where the urine collecting system of the kidney is dilated. This may be a normal variant or it may be due to an underlying
What is hydronephrosis? Hydronephrosis Hydronephrosis describes the situation where the urine collecting system of the kidney is dilated. This may be a normal variant or it may be due to an underlying
Renal Disease Survey Bracco Italiano Club of America Heath Committee, November 2012
 Renal Disease Survey Bracco Italiano Club of America Heath Committee, November 2012 Kidney disease is currently one of the most pressing health issues for the Bracco Italiano breed, as the etiology is
Renal Disease Survey Bracco Italiano Club of America Heath Committee, November 2012 Kidney disease is currently one of the most pressing health issues for the Bracco Italiano breed, as the etiology is
Composition: Each Tablet contains. Pharmacokinetic properties:
 Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Kidney Fun and Failure
 Kidney Fun and Failure Tom Ozbirn, M.D. General Session 2, Saturday, 9/8/12 9:30 a.m. to 11:30 a.m. Thomas W. Ozbirn, Jr DO, FACP Nephrology Associates, PC Birmingham, Alabama 1 Objectives Understand Categories
Kidney Fun and Failure Tom Ozbirn, M.D. General Session 2, Saturday, 9/8/12 9:30 a.m. to 11:30 a.m. Thomas W. Ozbirn, Jr DO, FACP Nephrology Associates, PC Birmingham, Alabama 1 Objectives Understand Categories
WEEK. MPharm Programme. Acute Kidney Injury. Alan M. Green MPHM13: Acute Kidney Injury. Slide 1 of 47
 MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
Learning Objectives. How big is the problem? ACUTE KIDNEY INJURY
 ACUTE KIDNEY INJURY Karen Innocent, DNP, RN, CRNP, ANP-BC, CMSRN Executive Director, Continuing Education Wolters Kluwer Health, Inc May 2016 Orlando FL Learning Objectives Identify the risk factors and
ACUTE KIDNEY INJURY Karen Innocent, DNP, RN, CRNP, ANP-BC, CMSRN Executive Director, Continuing Education Wolters Kluwer Health, Inc May 2016 Orlando FL Learning Objectives Identify the risk factors and
PRE-RENAL AKI: DOES IT LEAD TO ATN. Sushma Bhusal
 PRE-RENAL AKI: DOES IT LEAD TO ATN Sushma Bhusal 9.9.14 CASE PRESENTATION CC : 31 AAM presented with Fatigue, malaise and body aches x 10 days HPI: STD testing done 2 weeks prior, all results negative
PRE-RENAL AKI: DOES IT LEAD TO ATN Sushma Bhusal 9.9.14 CASE PRESENTATION CC : 31 AAM presented with Fatigue, malaise and body aches x 10 days HPI: STD testing done 2 weeks prior, all results negative
Urinary system disorders Chapter 29
 Urinary system disorders Chapter 29 1 The Nephron Anatomy 2 Physiology 1.25 L per minute blood flow 25% of Cardiac Output Kidney compensates if one is lost - 2 weeks 3 Urine Formation 1. Filtration 2.
Urinary system disorders Chapter 29 1 The Nephron Anatomy 2 Physiology 1.25 L per minute blood flow 25% of Cardiac Output Kidney compensates if one is lost - 2 weeks 3 Urine Formation 1. Filtration 2.
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Kidney Injury David T. Selewski, MD,* Jordan M. Symons, MD
 Article nephrology Acute Kidney Injury David T. Selewski, MD,* Jordan M. Symons, MD Author Disclosure Drs Selewski and Symons have disclosed no financial relationships relevant to this article. This commentary
Article nephrology Acute Kidney Injury David T. Selewski, MD,* Jordan M. Symons, MD Author Disclosure Drs Selewski and Symons have disclosed no financial relationships relevant to this article. This commentary
Study of Clinical Profile and Prognostic Factors of Acute Kidney Injury (AKI) In Tertiary Referral Centre in Marathwada
 In Tertiary Referral Centre in Marathwada") IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-853, p-issn: 2279-861.Volume 13, Issue 12 Ver. V (Dec. 214), PP 66-77 Study of Clinical Profile and Prognostic Factors of Acute Kidney
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-853, p-issn: 2279-861.Volume 13, Issue 12 Ver. V (Dec. 214), PP 66-77 Study of Clinical Profile and Prognostic Factors of Acute Kidney
Management of Acute Kidney Injury in the Neonate. Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital
 Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing
Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012
 Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007
 Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007 Hosted by: Australian Small Animal Veterinary Association (ASAVA) Australian Small Animal Veterinary Association (ASAVA)
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007 Hosted by: Australian Small Animal Veterinary Association (ASAVA) Australian Small Animal Veterinary Association (ASAVA)
Acute Kidney Injury (AKI) Undergraduate nurse education
 Undergraduate nurse education") Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
M3 Pros Revision 28/4/14 Renal
 M3 Pros Revision 28/4/14 Renal Q1. Mr Ravi is a 35- year old construction worker from India with no significant past medical history. He presents with a 3- day history of high fever (Tmax = 39.5), polyarthritis,
M3 Pros Revision 28/4/14 Renal Q1. Mr Ravi is a 35- year old construction worker from India with no significant past medical history. He presents with a 3- day history of high fever (Tmax = 39.5), polyarthritis,
Medicine Dr. Dana Lecture 1 Acute Kidney Injury (AKI)
") Medicine Dr. Dana Lecture 1 Acute Kidney Injury (AKI) Renal function Kidney has many roles: 1. Excretory function 2. Osmolality regulation 3. Acid base balance 4. BP regulation through salt and water balance
Medicine Dr. Dana Lecture 1 Acute Kidney Injury (AKI) Renal function Kidney has many roles: 1. Excretory function 2. Osmolality regulation 3. Acid base balance 4. BP regulation through salt and water balance
Dialyzing challenging patients: Patients with hepato-renal conditions
 Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
31/10/2016. Acute renal failure in dogs and cats: do they survive?? Eric Zini PD, PhD, Dipl. ECVIM-CA (Internal Medicine) Italy.
 Italy.") Acute renal failure in dogs and cats: do they survive?? Eric Zini PD, PhD, Dipl. ECVIM-CA (Internal Medicine) Italy Switzerland 1 Acute kidney injury (AKI)...but before? Definition Acute kidney disease
Acute renal failure in dogs and cats: do they survive?? Eric Zini PD, PhD, Dipl. ECVIM-CA (Internal Medicine) Italy Switzerland 1 Acute kidney injury (AKI)...but before? Definition Acute kidney disease
Chapter 33 Urology & Nephrology Functions of the Kidneys General Mechanisms of Nontraumatic Tissue Problems
 1 2 3 4 5 6 7 Chapter 33 Urology & Nephrology Functions of the Kidneys Forming and eliminating Maintaining blood volume with proper balance of water, electrolytes, and ph Retaining key compounds such as
1 2 3 4 5 6 7 Chapter 33 Urology & Nephrology Functions of the Kidneys Forming and eliminating Maintaining blood volume with proper balance of water, electrolytes, and ph Retaining key compounds such as
Acid Base Balance. Chapter 26 Balance. ph Imbalances. Acid Base Balance. CO 2 and ph. Carbonic Acid. Part 2. Acid/Base Balance
 Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
KIDNEY FAILURE. What causes kidney failure People who are most at risk for kidney failure usually have one or more of the following causes:
 KIDNEY FAILURE Your kidneys are a pair of organs located toward your lower back. One kidney is on each side of your spine. They filter your blood and remove toxins from your body. Your kidneys send toxins
KIDNEY FAILURE Your kidneys are a pair of organs located toward your lower back. One kidney is on each side of your spine. They filter your blood and remove toxins from your body. Your kidneys send toxins
renal physiology takes us
 AF Four Dimensional i Approach to Acute Renal Failure The track of understanding renal physiology takes us through h a convoluted journey M - 1 1054 Intracellular Milieu High Potassium High
AF Four Dimensional i Approach to Acute Renal Failure The track of understanding renal physiology takes us through h a convoluted journey M - 1 1054 Intracellular Milieu High Potassium High
Low Urine Output. Hospitalist Team Intern Didactics M. Jackson, 2007
 Low Urine Output Hospitalist Team Intern Didactics M. Jackson, 2007 Outline RN call- what to ask? Level of acuity- is this an emergency? Ddx Focused H & P- what to check signout for? ask? look for on exam?
Low Urine Output Hospitalist Team Intern Didactics M. Jackson, 2007 Outline RN call- what to ask? Level of acuity- is this an emergency? Ddx Focused H & P- what to check signout for? ask? look for on exam?
(Calcium and Phosphorus are a part of the CKD objectives)
") Course Objectives Electrolytes and Water: 1. Differentiate the effects of changes in sodium content from changes in water content 2. Describe how the body compensates for volume loss and volume overload
Course Objectives Electrolytes and Water: 1. Differentiate the effects of changes in sodium content from changes in water content 2. Describe how the body compensates for volume loss and volume overload
BCH 450 Biochemistry of Specialized Tissues
 BCH 450 Biochemistry of Specialized Tissues VII. Renal Structure, Function & Regulation Kidney Function 1. Regulate Extracellular fluid (ECF) (plasma and interstitial fluid) through formation of urine.
BCH 450 Biochemistry of Specialized Tissues VII. Renal Structure, Function & Regulation Kidney Function 1. Regulate Extracellular fluid (ECF) (plasma and interstitial fluid) through formation of urine.
URINARY SYSTEM CHAPTER 28 I ANATOMY OF THE URINARY SYSTEM. Student Name
 Student Name CHAPTER 28 URINARY SYSTEM L iving produces wastes. Wherever people live or work or play, wastes accumulate. To keep these areas healthy, there must be a method of disposing of these wastes
Student Name CHAPTER 28 URINARY SYSTEM L iving produces wastes. Wherever people live or work or play, wastes accumulate. To keep these areas healthy, there must be a method of disposing of these wastes
DIABETES MELLITUS. Kidney in systemic diseases. Slower the progression: Pathology: Patients with diabetes mellitus are prone to other renal diseases:
 Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Urinalysis Competition Dr. Katharine Dahl Dr. Brenda Shinar
 Urinalysis Competition 2017 Dr. Katharine Dahl Dr. Brenda Shinar Question 1. (PGY-1) An appropriate collection technique must be used in order to interpret urinalysis correctly. Which of the following
Urinalysis Competition 2017 Dr. Katharine Dahl Dr. Brenda Shinar Question 1. (PGY-1) An appropriate collection technique must be used in order to interpret urinalysis correctly. Which of the following
Instrumental determination of electrolytes in urine. Amal Alamri
 Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Renal pathophysiology.
 Renal pathophysiology basa.konecna@gmail.com Outline Intro basic structure & physiology Nephrotic syndrome Nephritic syndrome Acute renal failure Chronic kidney disease Gross structure and location Kidney
Renal pathophysiology basa.konecna@gmail.com Outline Intro basic structure & physiology Nephrotic syndrome Nephritic syndrome Acute renal failure Chronic kidney disease Gross structure and location Kidney
The principal functions of the kidneys
 Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
RENAL FUNCTION TESTS - Lecture
 #Clinical Chemistry RENAL FUNCTION TESTS - Lecture Dr. Kakul Husain # The Kidney Kidneys are bean-shaped organs, each about the size of fist, located near the middle of the back, just below the ribs cage.
#Clinical Chemistry RENAL FUNCTION TESTS - Lecture Dr. Kakul Husain # The Kidney Kidneys are bean-shaped organs, each about the size of fist, located near the middle of the back, just below the ribs cage.
CHAPTER 32: ACID-BASE DISORDERS AND RENAL TUBULAR ACIDOSIS
 Section 5: Nephrology CHAPTER 32: ACID-BASE DISORDERS AND RENAL TUBULAR ACIDOSIS Q.1. A 57-year-old man with insulin-requiring diabetes presents with a three-day history of polyuria and polydipsia after
Section 5: Nephrology CHAPTER 32: ACID-BASE DISORDERS AND RENAL TUBULAR ACIDOSIS Q.1. A 57-year-old man with insulin-requiring diabetes presents with a three-day history of polyuria and polydipsia after
network of thin-walled capillaries closely surrounded by a pear-shaped epithelial membrane called the Bowman s capsule
 Renal Terminology Renal-Root Words & Combining Forms calyx cortex glomerul/o medulla nephr/o pyel/o py/o ur/o ren/o cuplike division of the kidney outer layer of kidney glomerula inner or central portion
Renal Terminology Renal-Root Words & Combining Forms calyx cortex glomerul/o medulla nephr/o pyel/o py/o ur/o ren/o cuplike division of the kidney outer layer of kidney glomerula inner or central portion
Acute renal failure ARF
 Acute renal failure ARF Definition ARF is a clinical syndrome characterized by an abrupt decline in GFR and the accumulation of nitrogenous waste (BUN & creatinine). The decrease in GFR occurs relatively
Acute renal failure ARF Definition ARF is a clinical syndrome characterized by an abrupt decline in GFR and the accumulation of nitrogenous waste (BUN & creatinine). The decrease in GFR occurs relatively
Nursing Process Focus: Patients Receiving Dextran 40 (Gentran 40)
") Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua
 & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua") Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Acute Kidney Injury in The Acute Oncology Patient
 Acute Kidney Injury in The Acute Oncology Patient Dr Andrew Lewington BSc MEd MD FRCP Consultant Renal Physician/Honorary Senior Lecturer Leeds Teaching Hospitals Definition Definitions and terminology
Acute Kidney Injury in The Acute Oncology Patient Dr Andrew Lewington BSc MEd MD FRCP Consultant Renal Physician/Honorary Senior Lecturer Leeds Teaching Hospitals Definition Definitions and terminology
Functional Renal Physiology and Urine Production
 Functional Renal Physiology and Urine Production Urinalysis can provide insight into hydration status, renal function or dysfunction, systemic disease, and toxic insults. Accurate interpretation of urinalysis
Functional Renal Physiology and Urine Production Urinalysis can provide insight into hydration status, renal function or dysfunction, systemic disease, and toxic insults. Accurate interpretation of urinalysis
What would be the response of the sympathetic system to this patient s decrease in arterial pressure?
 CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
A Clinical Approach to Acute Renal Failure. Jeffrey J. Kaufhold, MD FACP July 2017
 A Clinical Approach to Acute Renal Failure Jeffrey J. Kaufhold, MD FACP July 2017 Summary Impact of ARF on hospitalized patients Causes of Acute Renal Failure Differential Pre-Renal Intra-renal Post-Renal
A Clinical Approach to Acute Renal Failure Jeffrey J. Kaufhold, MD FACP July 2017 Summary Impact of ARF on hospitalized patients Causes of Acute Renal Failure Differential Pre-Renal Intra-renal Post-Renal
London Strategic Clinical Networks. My AKI. Guidance for patients with, or recovering from, acute kidney injury
 London Strategic Clinical Networks My AKI Guidance for patients with, or recovering from, acute kidney injury Supporting the delivery of equitable, high quality AKI care through collaboration www.londonaki.net
London Strategic Clinical Networks My AKI Guidance for patients with, or recovering from, acute kidney injury Supporting the delivery of equitable, high quality AKI care through collaboration www.londonaki.net
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia