Visceral Vascular Ultrasound. Joel Thompson, MD, MPH Borg & Ide Imaging
|
|
|
- Lewis Byrd
- 6 years ago
- Views:
Transcription

1 Visceral Vascular Ultrasound Joel Thompson, MD, MPH Borg & Ide Imaging
2 Objectives: Review major abdominal vascular structures Identify normal peak systolic velocity (PSV) for major abdominal arteries. Be able to name a disease process that affects the PSV for each artery. Protocol imaging studies to help increase the sensitivity and accuracy of visceral vascular examinations.
3 Abdominal Aorta Diaphragmatic (aortic ) hiatus Bifurcation into right and left common iliac arteries at L4 level. Both paired and unpaired branches.
; rarely visualized 2. Renal Arteries (L2 level) 3. Gonadal Arteries (L2 level) 4. Lumbar arteries (posterior) https://i.pinimg.")
4 Abdominal Aorta Unpaired Branches 1. Celiac Axis (T12 level) 2. Superior mesenteric artery (SMA, L1 level) 3. Inferior mesenteric artery (IMA, L2 level) Paired Branches 1. Inferior phrenic (T12); rarely visualized 2. Renal Arteries (L2 level) 3. Gonadal Arteries (L2 level) 4. Lumbar arteries (posterior)


5 Abdominal aorta Triphasic (high resistance) waveform. More diastolic flow in proximal aorta above the level of the renal arteries PSV 110 cm/sec when young and walls more elastic; decreases to cm/sec with age. Slower and more turbulent flow within an aortic aneurysm, due to increased diameter and decreased resistance to blood flow. Wood et al. Ultrasound Quarterly.

6 Abdominal Aortic Aneurysm 4-8% incidence in males age 60 and older 2-5x risk if smoker, hypertension, or peripheral artery disease. Male:female ratio of 4:1. AAA of 5.5 cm or greater has an annual risk of rupture of 16%. Laplace s law: wall surface tension = radius x blood pressure Emergent repair caries a mortality risk of 40%. Perioperative mortality for endovascular repair 1%.
7 AAA Screening Screening recommendations by vascular surgeons: 1. All males age years. 2. Females age years with cardiovascular risk factor 3. Age >50 years and family history of AAA. AAA follow-up by size: <3 cm no further surveillance 3-4 cm ultrasound annually cm ultrasound every 6 months >4.5 cm referral to vascular specialist. Screening has 45-49% reduction in incidence of AAA rupture. Kent et al. J Vasc Surg 2004.
8 AAA Screening Patient fasting 8-10 hours to reduce bowel gas. 2.5 MHz curvilinear transducer Use compression to move aside bowel loops, or left lateral decubitus to reduce gas. Measure outer wall to outer wall
9 AAA Screening Measurement locations: proximal (below diaphragm, near celiac artery) mid (near level of renal arteries) distal (above iliac bifurcation). longitudinal and transverse images of proximal common iliac arteries. Image in plane parallel to the long axis of the lumen (for AP dimension) and perpendicular to long axis of lumen (for transverse dimension). Transverse may be obtained in coronal plane. Aneurysm: maximum dimension >3 cm or 1.5x greater than more proximal measurement. Document relationship to renal arteries and aortic bifurcation.


10 US evaluation of EVAR Color Doppler of proximal, left, right iliac attachments Document flow in SMA and renal arteries Look for flow in aneurysm sac. Endoleaks: 1. Between proximal/distal end of stent and aortic wall 2. Retrograde filling via a branch 3. Defect or tear in graft 4. Porous graft 5. Endotension (enlarging sac without visible leak) Picel et al. AJR


11 Finding on LE Doppler US: 4% of people with AAA have a popliteal artery aneurysm (1.5x proximal diameter) % of people with popliteal aneurysm have AAA.

12 Aortic Dissection In the abdomen, usually a continuation of thoracic aortic dissection. Separation of medial and intimal layers of the vessel wall. False lumen: usually larger, may be thrombosed. To and fro on spectral Doppler. True lumen has elevated PSV. Evaluate patency of major branches.
13 What vessels are being imaged? A: Aorta B: Celiac axis C: SMA B C A
14 Celiac axis Celiac axis arises anteriorly 3 branches: splenic, left gastric, and common hepatic arteries. First 2 cm of celiac axis is high resistance (biphasic) Distal celiac axis and its branches are low resistance.

 waveform when patient is fasting (Figure A).")
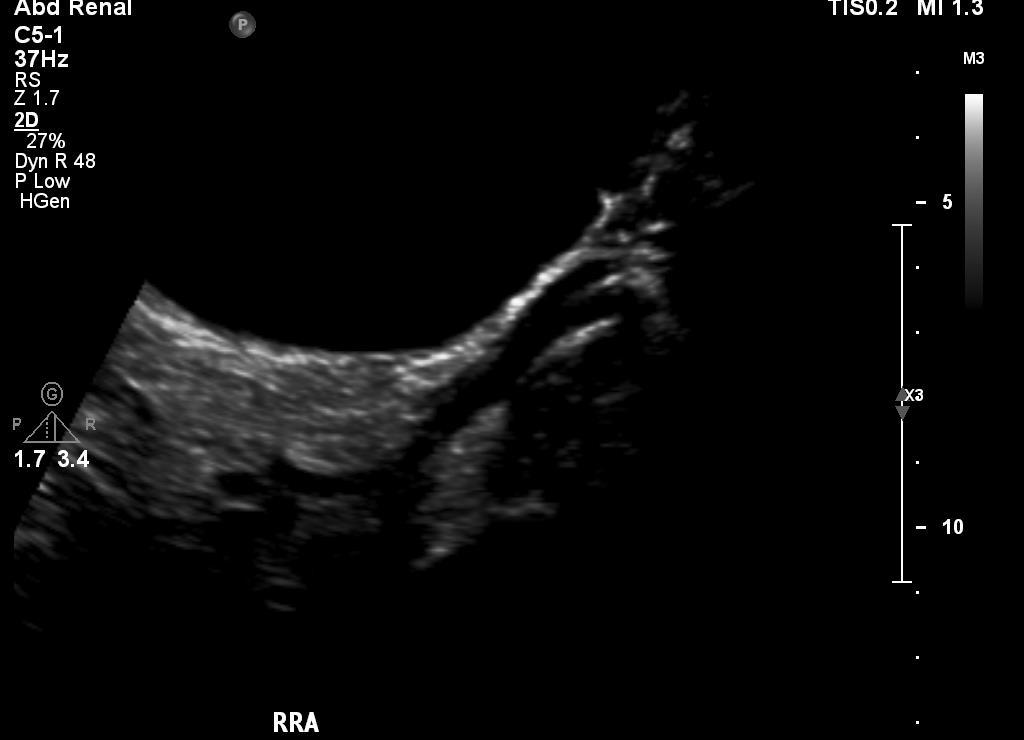
15 Wood et al. Ultrasound Quarterly. Superior Mesenteric Artery Supplies jejunum, ileum, ascending and transverse colon. Vascular arcades. Cuff of retroperitoneal fat. Triphasic (high resistance) waveform when patient is fasting (Figure A). Post-prandially, increased systolic and diastolic velocities. Increased diameter. Low resistance waveform. (Figure B).
16 US of Mesenteric arteries Most atherosclerotic plaque at origins of these vessels. NPO for 8 hours Relax abdominal muscles by propping up head MHz probe depending on body habitus. Celiac axis: angle corrected velocities to bifurcation SMA: angle corrected velocities for 5 cm Doppler exam technically not possible in 40% of population (body habitus, gas)
17 Mesenteric Artery Stenosis PSV Celiac >200 cm/sec SMA >275 cm/sec IMA >200 cm/s PSV ratio (Mesenteric:Aorta) of 3-3.5:1 EDV Celiac >55 cm/sec SMA >45 cm/sec Distal Tardus Parvus waveforms. Retrograde common hepatic artery flow 100% accurate for CA stenosis/occlusion.
18 Median Arcuate Ligament Syndrome Median arcuate ligament connects the diaphragmatic crura, forming anterior margin of aortic hiatus. Vague epigastric pain, especially postprandial. Weight loss. Low lying in some patients, compressing celiac axis during expiration. Horton, KM Radiographics 2005:25:1177

19 Median Arcuate Ligament Syndrome Ultrasound assessment: Measure PSV in end-inspiration and endexpiration Elevated celiac axis PSV during end expiration in symptomatic patients raises possibility of MAL syndrome. Horton, KM Radiographics 2005:25:1177


20 You know the anatomy of the vessels A: Aorta B: Celiac axis C: SMA B C A

21 What do you do next?

22 What do you do next?
23 What do you do next? PSV Celiac >200 cm/sec SMA >275 cm/sec IMA >200 cm/s PSV ratio (Mesenteric:Aorta) of 3-3.5:1 EDV Celiac >55 cm/sec SMA >45 cm/sec
24 Check PSV with inspiration and expiration.
25 Median Arcuate Ligament Syndrome Elevated PSV that is further increased with expiration = MALS



26 Abdominal pain out of proportion to exam. AFib.
27 What abnormalities do you see?



28 What was the sonographer looking for?

29 SMA thrombosis. Decreased or absent diastolic flow (increased RI). Decreased flow on color Doppler image. Distal obstruction/high grade stenosis. In this case due to clot embolization from A Fib.
30 Mesenteric Ischemia Pain after eating. Pain out of proportion to exam. CT Angiogram if acute thrombus suspected. Chronic: Doppler US may be initial evaluation. Usually due to atherosclerosis, although stenosis does not mean mesenteric ischemia is present due to extensive collateral blood supply.
31 Renal Artery Stenosis Paired arteries at the L2 level. Renal artery stenosis / renovascular hypertension: In older patients, at origin due to atherosclerosis (90% of cases). In young patients, mid renal artery due to fibromuscular dysplasia. Criteria: Renal artery PSV >200 cm/s (suggest stenosis 60% or greater) Renal:Aortic Ratio PSV 3.5:1 EDV >150 cm/s (suggests stenosis 80% or greater). More distal findings such as tardus parvus helpful to confirm stenosis, but absence doesn t exclude stenosis.
 Renal:Aortic Ratio PSV 3.")

32 Criteria: Renal artery PSV >200 cm/s (suggest stenosis 60% or greater) Renal:Aortic Ratio PSV 3.5: % patients have one or more accessory renal arteries, difficult to visualize and interogate by US.


33 Fibromuscular Dysplasia (without stenosis)



34 FMD
35 Renal Artery Evaluation 12 h fast to decrease bowel gas MHz transducer via anterior abdominal wall or the flank. Right RA beneath the IVC. Identify left RA by first finding left RV; artery is directly behind it. Pitfall, inferior mesenteric artery, but IMA should be high resistance.

36 Portal Venous System Main portal vein formed by confluence of splenic vein and superior mesenteric vein. 5-8 cm in length. Splits into right and left portal vein branches
 Wood et al.")
37 Main Portal Vein Slow flow, cm/s. Cardiac variability in waveform Hepatic vein pressures transmitted to portal venous system via sinusoids. Gently undulating waveform. Trough is during diastole when right atrium contracts. Should always be hepatopetal (towards liver) Wood et al. Ultrasound Quarterly.
38 4 ways portal venous waveform can change: 1. Increased pulsatility Right heart failure, tricuspid regurgitation Arteriovenous shunting or fistulas 2. Slow flow (<16 cm/s) Prehepatic (portal vein thrombosis) Hepatic (cirrhosis) Post hepatic (CHF, tricuspid regurgitation, hepatic vein thrombosis) 3. Hepatofugal flow (retrograde) due to portal hypertension. 4. Absent flow (bland or tumor thrombus).
 Prehepatic (portal vein thrombosis) Hepatic (cirrhosis) Post hepatic (CHF, tricuspid regurgitation, hepatic vein thrombosis) 3.")
39 4 ways portal venous waveform can change: 1. Increased pulsatility Right heart failure, tricuspid regurgitation Arteriovenous shunting or fistulas 2. Slow flow (<16 cm/s) Prehepatic (portal vein thrombosis) Hepatic (cirrhosis) Post hepatic (CHF, tricuspid regurgitation, hepatic vein thrombosis) 3. Hepatofugal flow (retrograde) due to portal hypertension. 4. Absent flow (bland or tumor thrombus). Wood et al. Ultrasound Quarterly.
40 4 ways portal venous waveform can change: 1. Increased pulsatility Right heart failure, tricuspid regurgitation Arteriovenous shunting or fistulas 2. Slow flow (<16 cm/s) Prehepatic (portal vein thrombosis) Hepatic (cirrhosis) Post hepatic (CHF, tricuspid regurgitation, hepatic vein thrombosis) 3. Hepatofugal flow (retrograde) due to portal hypertension. 4. Absent flow (bland or tumor thrombus).
 Prehepatic (portal vein thrombosis) Hepatic (cirrhosis) Post hepatic (CHF, tricuspid regurgitation, hepatic vein thrombosis) 3.")
41 4 ways portal venous waveform can change: 1. Increased pulsatility Right heart failure, tricuspid regurgitation Arteriovenous shunting or fistulas 2. Slow flow (<16 cm/s) Prehepatic (portal vein thrombosis) Hepatic (cirrhosis) Post hepatic (CHF, tricuspid regurgitation, hepatic vein thrombosis) 3. Hepatofugal flow (retrograde) due to portal hypertension. 4. Absent flow (bland or tumor thrombus). Wood et al. Ultrasound Quarterly.
42 4 ways portal venous waveform can change: 1. Increased pulsatility Right heart failure, tricuspid regurgitation Arteriovenous shunting or fistulas 2. Slow flow (<16 cm/s) Prehepatic (portal vein thrombosis) Hepatic (cirrhosis) Post hepatic (CHF, tricuspid regurgitation, hepatic vein thrombosis) 3. Hepatofugal flow (retrograde) due to portal hypertension. 4. Absent flow (bland or tumor thrombus).

43 Portal venous waveforms Mild portal hypertension. Increased pulsatility Wood et al. Ultrasound Quarterly. Severe portal hypertension. Hepatofugal flow. Tricuspid regurgitation. Pulsatile Peak/trough difference >15 cm/s.

44 Cavernous transformation of the main portal vein. Takes months to develop, so typically seen with bland thrombus. Maia et al. Radiol Bras.


45 60 yo male. Increasing hyperbilirubinemia after BMT. Normal flow in MPV. Small volume perihepatic ascites.

46 2 weeks later: Slow, hepatofugal flow in MPV, 8 cm/s. Increased ascites.


47 Increased hepatic arterial RI. Patent IVC and hepatic veins.
48 4 ways portal venous waveform can change: 1. Increased pulsatility Right heart failure, tricuspid regurgitation Arteriovenous shunting or fistulas 2. Slow flow (<16 cm/s) Prehepatic (portal vein thrombosis) Hepatic (cirrhosis) Post hepatic (CHF, tricuspid regurgitation, hepatic vein thrombosis) 3. Hepatofugal flow (retrograde) due to portal hypertension. 4. Absent flow (bland or tumor thrombus).

49 Hepatic veno-occlusive disease Toxic injury to liver sinusoids sloughed cells embolize to hepatic venules hepatic congestion. Ddx: Budd-Chiari syndrome Findings: Hepatomegaly Portal vein dilatation, increased pulsatility, hepatofugal flow if severe. Increased hepatic arterial RI Gallbladder wall thickening Ascites

50 Don t miss portal venous air!
 of 3-3.")
51 Numbers hard to remember be sure to document mesenteric:aorta PSV ratio. PSV Celiac >200 cm/sec SMA >275 cm/sec IMA >200 cm/s PSV ratio (Mesenteric:Aorta) of 3-3.5:1 EDV Celiac >55 cm/sec SMA >45 cm/sec Distal Tardus Parvus waveforms.
52 Visceral Vascular Ultrasound Joel Thompson, MD, MPH Borg & Ide Imaging
Abdominal Doppler Mastering the next level of vascular anatomy in the belly. Cindy A. Owen, RDMS, RVT
 Abdominal Doppler Mastering the next level of vascular anatomy in the belly Cindy A. Owen, RDMS, RVT Introduction Abdominal Doppler is a tough exam Success is dependent on: Patient body habitus Patient
Abdominal Doppler Mastering the next level of vascular anatomy in the belly Cindy A. Owen, RDMS, RVT Introduction Abdominal Doppler is a tough exam Success is dependent on: Patient body habitus Patient
Abdominal Aortic Aneurysm (AAA)
") Abdominal Aortic Aneurysm (AAA) Vascular Workshop: Objectives Anatomy Keith VanHaltren Indications Technique Cases Abdominal Aorta: Normal Size Abdominal aortic aneurysm: Definition Normal diameter of
Abdominal Aortic Aneurysm (AAA) Vascular Workshop: Objectives Anatomy Keith VanHaltren Indications Technique Cases Abdominal Aorta: Normal Size Abdominal aortic aneurysm: Definition Normal diameter of
DISCLOSURE TEST YOUR WAVEFORM IQ. Partial volume artifact. 86 yo female with right arm swelling, picc line. AVF on left? Dx?
 Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
What effects will proximal or distal disease have on a waveform?
 Spectral Doppler Interpretation Director of Ultrasound Education & Quality Assurance Baylor College of Medicine Division of Maternal-Fetal Medicine Maternal Fetal Center Imaging Manager Texas Children
Spectral Doppler Interpretation Director of Ultrasound Education & Quality Assurance Baylor College of Medicine Division of Maternal-Fetal Medicine Maternal Fetal Center Imaging Manager Texas Children
What effects will proximal or distal disease have on an waveform?
 Spectral Doppler Interpretation Director Director of of Ultrasound Ultrasound Education Education & & Quality Quality Assurance Assurance Baylor Baylor College College of of Medicine Medicine Division
Spectral Doppler Interpretation Director Director of of Ultrasound Ultrasound Education Education & & Quality Quality Assurance Assurance Baylor Baylor College College of of Medicine Medicine Division
Deb Coghlan AMS (Vascular and General ) Brisbane, Australia
 Brisbane, Australia") Deb Coghlan AMS (Vascular and General ) Brisbane, Australia ANEURYSMAL DIISEASE The infrarenal aorta enlarges with age, and is the commonest site for arterial aneurysms. An aneurysm is a permanent focal
Deb Coghlan AMS (Vascular and General ) Brisbane, Australia ANEURYSMAL DIISEASE The infrarenal aorta enlarges with age, and is the commonest site for arterial aneurysms. An aneurysm is a permanent focal
MESENTERIC ISCHEMIA. Phillip J Bendick, PhD
 MESENTERIC ISCHEMIA Phillip J Bendick, PhD Arterial Celiac - Hepatic - Splenic Superior Mesenteric Artery Inferior Mesenteric Artery Venous Mesenteric system Porto - hepatic system Inferior Vena Cava Acute
MESENTERIC ISCHEMIA Phillip J Bendick, PhD Arterial Celiac - Hepatic - Splenic Superior Mesenteric Artery Inferior Mesenteric Artery Venous Mesenteric system Porto - hepatic system Inferior Vena Cava Acute
The Role of US in Chronic Mesenteric Ischemia. Sagar S. Gandhi, MD Vascular Health Alliance Greenville Health System
 The Role of US in Chronic Mesenteric Ischemia Sagar S. Gandhi, MD Vascular Health Alliance Greenville Health System No Disclosures Mesenteric Ischemia Anatomy Presentation Diagnostic tools Treatment Celiac
The Role of US in Chronic Mesenteric Ischemia Sagar S. Gandhi, MD Vascular Health Alliance Greenville Health System No Disclosures Mesenteric Ischemia Anatomy Presentation Diagnostic tools Treatment Celiac
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management. Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC
 An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
What Do We Know? Disclosure Statement: 3/11/2015. Deep abdominal imaging
 Marsha M. Neumyer, BS, RVT, FSVU, FSDMS, FAIUM International Director Vascular Diagnostic Educational Services Vascular Resource Associates Harrisburg, PA Disclosure Statement: CME Calendar QR Code Marsha
Marsha M. Neumyer, BS, RVT, FSVU, FSDMS, FAIUM International Director Vascular Diagnostic Educational Services Vascular Resource Associates Harrisburg, PA Disclosure Statement: CME Calendar QR Code Marsha
1. Long images of aorta (prox, mid, and dist) with AP measurements. 2. Trans images of aorta (prox, mid, and dist) with R/L measurements.
 with AP measurements. 2. Trans images of aorta (prox, mid, and dist) with R/L measurements.") Aorta 1. Long images of aorta (prox, mid, and dist) with AP measurements. 2. Trans images of aorta (prox, mid, and dist) with R/L measurements. 3. Long images of R/L common iliac arteries with AP measurements.
Aorta 1. Long images of aorta (prox, mid, and dist) with AP measurements. 2. Trans images of aorta (prox, mid, and dist) with R/L measurements. 3. Long images of R/L common iliac arteries with AP measurements.
Abdominal Ultrasonography
 Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
Scanning Mesenteric and Hypogastric Artery Aneurysms
 Scanning Mesenteric and Hypogastric Artery Aneurysms Marsha M. Neumyer, BS, RVT, FSVU, FSDMS, FAIUM International Director Vascular Diagnostic Education Services Vascular Resource Associates Harrisburg,
Scanning Mesenteric and Hypogastric Artery Aneurysms Marsha M. Neumyer, BS, RVT, FSVU, FSDMS, FAIUM International Director Vascular Diagnostic Education Services Vascular Resource Associates Harrisburg,
Doppler Ultrasonography of the Liver: What Every General Radiologist Should Know
 Doppler Ultrasonography of the Liver: What Every General Radiologist Should Know Poster No.: C-1658 Congress: ECR 2014 Type: Authors: Keywords: DOI: Educational Exhibit T. González de la Huebra Labrador,
Doppler Ultrasonography of the Liver: What Every General Radiologist Should Know Poster No.: C-1658 Congress: ECR 2014 Type: Authors: Keywords: DOI: Educational Exhibit T. González de la Huebra Labrador,
Duplex Ultrasound of the Renal Arteries. Duplex Ultrasound. In the Beginning
 Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
Indications: following: embolization. artery that has diseases 5. The evaluation. of suspected. such entities. a cold hand. biopsy
 Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
11 TH ANNUAL VASCULAR NONINVASIVE TESTING SYMPOSIUM NOVEMBER 10, 2018
 11 TH ANNUAL VASCULAR NONINVASIVE TESTING SYMPOSIUM NOVEMBER 10, 2018 RENAL ARTERY DISEASE AND RENOVASCULAR HYPERTENSION 1 WHAT IS RENOVASCULAR HYPERTENSION? https://my.clevelandclinic.org/health/diseases/16459-renovascular-hypertension
11 TH ANNUAL VASCULAR NONINVASIVE TESTING SYMPOSIUM NOVEMBER 10, 2018 RENAL ARTERY DISEASE AND RENOVASCULAR HYPERTENSION 1 WHAT IS RENOVASCULAR HYPERTENSION? https://my.clevelandclinic.org/health/diseases/16459-renovascular-hypertension
Mesenteric/Splanchnic Artery Duplex Imaging
 VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Mesenteric/Splanchnic Artery Duplex Imaging This Guideline was prepared by members of the Society for Vascular Ultrasound (SVU) as a template to
VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Mesenteric/Splanchnic Artery Duplex Imaging This Guideline was prepared by members of the Society for Vascular Ultrasound (SVU) as a template to
Transducer Selection. Renal Artery Duplex Exam. Renal Scan. Renal Scan Echogenicity. How to Perform an Optimal Renal Artery Doppler Examination
 How to Perform an Optimal Renal Artery Doppler Examination Director of Ultrasound Education & Quality Assurance Baylor College of Medicine Division of Maternal-Fetal Medicine Maternal Fetal Center Imaging
How to Perform an Optimal Renal Artery Doppler Examination Director of Ultrasound Education & Quality Assurance Baylor College of Medicine Division of Maternal-Fetal Medicine Maternal Fetal Center Imaging
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Vascular Imaging in the Pediatric Abdomen. Jonathan Swanson, MD
 Vascular Imaging in the Pediatric Abdomen Jonathan Swanson, MD Goals and Objectives To understand the imaging approach, appearance, and clinical manifestations of the common pediatric abdominal vascular
Vascular Imaging in the Pediatric Abdomen Jonathan Swanson, MD Goals and Objectives To understand the imaging approach, appearance, and clinical manifestations of the common pediatric abdominal vascular
Carotid Abnormalities Coils, Kinks and Tortuosity David Lorelli M.D., RVT, FACS Michigan Vascular Association Conference Saturday, October 20, 2012
 Carotid Abnormalities Coils, Kinks and Tortuosity David Lorelli M.D., RVT, FACS Michigan Vascular Association Conference Saturday, October 20, 2012 Page 1 Table of Contents Carotid Anatomy Carotid Duplex
Carotid Abnormalities Coils, Kinks and Tortuosity David Lorelli M.D., RVT, FACS Michigan Vascular Association Conference Saturday, October 20, 2012 Page 1 Table of Contents Carotid Anatomy Carotid Duplex
Ultrasound Imaging of The Posterior Circulation
 Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE
 MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when?
 Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
US of Renovascular Hypertension. Jonathan R. Dillman, MD, MSc Associate Professor Director, Thoracoabdominal Imaging
 US of Renovascular Hypertension Jonathan R. Dillman, MD, MSc Associate Professor Director, Thoracoabdominal Imaging Disclosures Nothing Relevant Unrelated grant funding Siemens US Toshiba US Objectives
US of Renovascular Hypertension Jonathan R. Dillman, MD, MSc Associate Professor Director, Thoracoabdominal Imaging Disclosures Nothing Relevant Unrelated grant funding Siemens US Toshiba US Objectives
Abdominal Doppler. Cases of Where, Why, and How
 Abdominal Doppler Cases of Where, Why, and How Jill D. Trotter, BS, RT(R), RDMS, RVT Director, Diagnostic Medical Sonography Program Vanderbilt University/Vanderbilt Medical Center Nashville, Tennessee
Abdominal Doppler Cases of Where, Why, and How Jill D. Trotter, BS, RT(R), RDMS, RVT Director, Diagnostic Medical Sonography Program Vanderbilt University/Vanderbilt Medical Center Nashville, Tennessee
Vascular Technology Examination Content Outline
 Vascular Technology Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Normal Anatomy, Perfusion, and Function Evaluate normal anatomy, perfusion, function 2 Pathology, Perfusion,
Vascular Technology Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Normal Anatomy, Perfusion, and Function Evaluate normal anatomy, perfusion, function 2 Pathology, Perfusion,
No financial or commercial relationships to disclose
 Deanna New, RVT No financial or commercial relationships to disclose IAC REQUIREMENTS: The main duty of a sonographer is to make the physician or radiologists job easier by capturing images and doing
Deanna New, RVT No financial or commercial relationships to disclose IAC REQUIREMENTS: The main duty of a sonographer is to make the physician or radiologists job easier by capturing images and doing
Vascular Ultrasound: Current state, current needs, future directions
 Vascular Ultrasound: Current state, current needs, future directions Laurence Needleman, MD Thomas Jefferson University Hospitals Sidney Kimmel Medical College of Thomas Jefferson University Disclosures
Vascular Ultrasound: Current state, current needs, future directions Laurence Needleman, MD Thomas Jefferson University Hospitals Sidney Kimmel Medical College of Thomas Jefferson University Disclosures
symptomatic aneurysms or aneurysms that grow >1cm/yr
 1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
The role for contrast-enhanced ultrasonography outside of focal liver lesions
 The role for contrast-enhanced ultrasonography outside of focal liver lesions Paul S. Sidhu King s College Hospital, London, UK Introduction Contrast-enhanced ultrasonography (US) of focal liver lesions
The role for contrast-enhanced ultrasonography outside of focal liver lesions Paul S. Sidhu King s College Hospital, London, UK Introduction Contrast-enhanced ultrasonography (US) of focal liver lesions
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Nellix Endovascular System: Clinical Outcomes and Device Overview
 Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Duplex ultrasound is first-line imaging for all
 Our Protocol for Transabdominal Pelvic Vein Duplex Ultrasound A summary of s protocol for pelvic vein duplex ultrasonography, including equipment, patient positioning, ultrasound settings, and technique.
Our Protocol for Transabdominal Pelvic Vein Duplex Ultrasound A summary of s protocol for pelvic vein duplex ultrasonography, including equipment, patient positioning, ultrasound settings, and technique.
HD Scanning: Velocities and Volume Flow
 HD Scanning: Velocities and Volume Flow Non-Invasive Lab Symposium West Orange, NJ April 27, 2018 Volume Flow Cindy Sturt, MD, FACS, RVT 500,000 Americans on dialysis 20-25% annual mortality 65% 5 year
HD Scanning: Velocities and Volume Flow Non-Invasive Lab Symposium West Orange, NJ April 27, 2018 Volume Flow Cindy Sturt, MD, FACS, RVT 500,000 Americans on dialysis 20-25% annual mortality 65% 5 year
Case 9799 Stanford type A aortic dissection: US and CT findings
 Case 9799 Stanford type A aortic dissection: US and CT findings Accogli S, Aringhieri G, Scalise P, Angelini G, Pancrazi F, Bemi P, Bartolozzi C Department of Diagnostic and Interventional Radiology, University
Case 9799 Stanford type A aortic dissection: US and CT findings Accogli S, Aringhieri G, Scalise P, Angelini G, Pancrazi F, Bemi P, Bartolozzi C Department of Diagnostic and Interventional Radiology, University
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES
 NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
Case 8038 Renal allograft complicated with renal artery stenosis
 Case 8038 Renal allograft complicated with renal artery stenosis Santiago I, Canelas A, Pinto AP Section: Cardiovascular Published: 2009, Nov. 30 Patient: 61 year(s), male Clinical History A 61-year-old
Case 8038 Renal allograft complicated with renal artery stenosis Santiago I, Canelas A, Pinto AP Section: Cardiovascular Published: 2009, Nov. 30 Patient: 61 year(s), male Clinical History A 61-year-old
Taming The Aorta. David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA
 Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Abdominal Ultrasound : Aorta, Kidneys, Bladder
 Abdominal Ultrasound : Aorta, Kidneys, Bladder Nilam J. Soni, MD, MSc Associate Professor of Medicine Divisions of Hospital Medicine and Pulmonary/Critical Care Medicine Department of Medicine University
Abdominal Ultrasound : Aorta, Kidneys, Bladder Nilam J. Soni, MD, MSc Associate Professor of Medicine Divisions of Hospital Medicine and Pulmonary/Critical Care Medicine Department of Medicine University
Physician s Vascular Interpretation Examination Content Outline
 Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
SAVE THE DATE! MARCH 3-7, 2019 GRAND WAILEA MAUI, HAWAII DIAGNOSTIC AND THERAPEUTIC APPROACHES TO VASCULAR DISEASE FOR MORE DETAILS, VISIT
 SAVE THE DATE! MARCH 3-7, 2019 GRAND WAILEA MAUI, HAWAII FOR MORE DETAILS, VISIT WWW.STRANDNESS.ORG DIAGNOSTIC AND THERAPEUTIC APPROACHES TO VASCULAR DISEASE Arterial Aneurysms in a Patient with Ehlers
SAVE THE DATE! MARCH 3-7, 2019 GRAND WAILEA MAUI, HAWAII FOR MORE DETAILS, VISIT WWW.STRANDNESS.ORG DIAGNOSTIC AND THERAPEUTIC APPROACHES TO VASCULAR DISEASE Arterial Aneurysms in a Patient with Ehlers
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Ultrasound of the Renal Arteries
 Ultrasound of the Renal Arteries Greg Curry Vascular Ultrasound Workshop Aug 2017 The Examination Technique Pathophysiology Role of US then and now Background Live Scanning Ultrasound Population: 20% Hypertensive
Ultrasound of the Renal Arteries Greg Curry Vascular Ultrasound Workshop Aug 2017 The Examination Technique Pathophysiology Role of US then and now Background Live Scanning Ultrasound Population: 20% Hypertensive
The posterior abdominal wall. Prof. Oluwadiya KS
 The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
Vascular Sonography Examination
 Vascular Sonography Examination The purpose of The American Registry of Radiologic Technologists (ARRT ) Vascular Sonography Examination is to assess the knowledge and cognitive skills underlying the intelligent
Vascular Sonography Examination The purpose of The American Registry of Radiologic Technologists (ARRT ) Vascular Sonography Examination is to assess the knowledge and cognitive skills underlying the intelligent
PAH EMERGENCY Department Aortic Scanning module
 PAH EMERGENCY Department Aortic Scanning module Abdominal Aorta Scan is a goal directed ultrasound examination to detect the presence of an Abdominal Aortic Aneurysm (AAA). The Abdominal Aorta scan is
PAH EMERGENCY Department Aortic Scanning module Abdominal Aorta Scan is a goal directed ultrasound examination to detect the presence of an Abdominal Aortic Aneurysm (AAA). The Abdominal Aorta scan is
THE COMPLETE GUIDE TO VASCULAR ULTRASOUND
 THE COMPLETE GUIDE TO VASCULAR ULTRASOUND PETER H. ARGER, M.D., F.A.I.U.M., F.A.C.R. Professor Emeritus Department of Radiology University of Pennsylvania Medical Center Hospital of the University of Pennsylvania
THE COMPLETE GUIDE TO VASCULAR ULTRASOUND PETER H. ARGER, M.D., F.A.I.U.M., F.A.C.R. Professor Emeritus Department of Radiology University of Pennsylvania Medical Center Hospital of the University of Pennsylvania
Ultrasound Evaluation after EVAR: (Trying to) Let the CAT Scan Out of the Bag
 Let the CAT Scan Out of the Bag") Ultrasound Evaluation after EVAR: (Trying to) Let the CAT Scan Out of the Bag Joseph-Vincent V. Blas, MD Division of Vascular Surgery Department of Surgery Greenville Health System University of South
Ultrasound Evaluation after EVAR: (Trying to) Let the CAT Scan Out of the Bag Joseph-Vincent V. Blas, MD Division of Vascular Surgery Department of Surgery Greenville Health System University of South
Guidelines, Policies and Statements D5 Statement on Abdominal Scanning
 Guidelines, Policies and Statements D5 Statement on Abdominal Scanning Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
Guidelines, Policies and Statements D5 Statement on Abdominal Scanning Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
GUNDERSEN/LUTHERAN ULTRASOUND DEPARTMENT POLICY AND PROCEDURE MANUAL
 GUNDERSEN/LUTHERAN ULTRASOUND DEPARTMENT POLICY AND PROCEDURE MANUAL SUBJECT: Carotid Duplex Ultrasound SECTION: Vascular Ultrasound ORIGINATOR: Deborah L. Richert, BSVT, RDMS, RVT DATE: October 15, 2015
GUNDERSEN/LUTHERAN ULTRASOUND DEPARTMENT POLICY AND PROCEDURE MANUAL SUBJECT: Carotid Duplex Ultrasound SECTION: Vascular Ultrasound ORIGINATOR: Deborah L. Richert, BSVT, RDMS, RVT DATE: October 15, 2015
RENAL AND MESENTERIC ARTERY STENTS Are There Standard Velocity Criteria for Restenosis?
 RENAL AND MESENTERIC ARTERY STENTS Are There Standard Velocity Criteria for Restenosis? R. Eugene Zierler, M.D. The D. E. Strandness, Jr. Vascular Laboratory University of Washington Medical Center Division
RENAL AND MESENTERIC ARTERY STENTS Are There Standard Velocity Criteria for Restenosis? R. Eugene Zierler, M.D. The D. E. Strandness, Jr. Vascular Laboratory University of Washington Medical Center Division
Dr. Weyrich G07: Superior and Posterior Mediastina. Reading: 1. Gray s Anatomy for Students, chapter 3
 Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad).
.") Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Imaging abdominal vascular emergencies. V.Stoynova
 Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Educational Exhibit Authors:
 Endoleaks in Abdominal Aortic Aneurysm Endoprosthesis: What radiologists need to know about Diagnostic, Characterization and Basic Management Strategies Poster No.: C-0150 Congress: ECR 2013 Type: Educational
Endoleaks in Abdominal Aortic Aneurysm Endoprosthesis: What radiologists need to know about Diagnostic, Characterization and Basic Management Strategies Poster No.: C-0150 Congress: ECR 2013 Type: Educational
Goals. Access flow and renal artery stenosis evaluation by Doppler ultrasound. Reimbursement. WHY use of Doppler Ultrasound
 Access flow and renal artery stenosis evaluation by Doppler ultrasound Adina Voiculescu, MD Interventional Nephrology Brigham and Women s Hospital Boston Instructor at Harvard Medical School Understand
Access flow and renal artery stenosis evaluation by Doppler ultrasound Adina Voiculescu, MD Interventional Nephrology Brigham and Women s Hospital Boston Instructor at Harvard Medical School Understand
Abdomen and Retroperitoneum Ultrasound Protocols
 Abdomen and Retroperitoneum Ultrasound Protocols Reviewed By: Anna Ellermeier, MD Last Reviewed: March 2018 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
Abdomen and Retroperitoneum Ultrasound Protocols Reviewed By: Anna Ellermeier, MD Last Reviewed: March 2018 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
Carotid Doppler: Doppler wave forms obtained from the common, external and internal carotid arteries. As well as the vertebral and subclavian
 Competency Carotid Doppler: Doppler wave forms obtained from the common, external and internal carotid arteries. As well as the vertebral and subclavian arteries. Preferred angle is 60 degrees or less.
Competency Carotid Doppler: Doppler wave forms obtained from the common, external and internal carotid arteries. As well as the vertebral and subclavian arteries. Preferred angle is 60 degrees or less.
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Vascular CT Protocols
 Vascular CT Protocols V 1D: Chest and abdominal CT angiogram (aortic dissection protocol) V 1T: Chest CT angiogram (aortic trauma protocol) V 2: Abdominal and pelvis CT angiogram (aortic aneurysm protocol)
Vascular CT Protocols V 1D: Chest and abdominal CT angiogram (aortic dissection protocol) V 1T: Chest CT angiogram (aortic trauma protocol) V 2: Abdominal and pelvis CT angiogram (aortic aneurysm protocol)
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY MESENTERIC ISCHAEMIA P Zwanepoel INTRODUCTION Mesenteric ischaemia results from hypoperfusion of the gut, most commonly due to occlusion, thrombosis or vasospasm.
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY MESENTERIC ISCHAEMIA P Zwanepoel INTRODUCTION Mesenteric ischaemia results from hypoperfusion of the gut, most commonly due to occlusion, thrombosis or vasospasm.
Approaches to type II Endoleaks: Transcaval, transarterial, translumbar. Saher Sabri,MD University of Virginia
 Approaches to type II Endoleaks: Transcaval, transarterial, translumbar Saher Sabri,MD University of Virginia Saher Sabri, M.D. Speakers Bureau: W.L.Gore & Associates, Abbott Type 2 Endoleaks after EVAR
Approaches to type II Endoleaks: Transcaval, transarterial, translumbar Saher Sabri,MD University of Virginia Saher Sabri, M.D. Speakers Bureau: W.L.Gore & Associates, Abbott Type 2 Endoleaks after EVAR
Large veins of the thorax Brachiocephalic veins
 Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Abdominal Aortic Aneurysm 가천대길병원 이상준
 Abdominal Aortic Aneurysm 가천대길병원 이상준 1 Definition Diameter of the aorta 1.5 times greater than normal. Most are infrarenal, and a significant number extend down into one or both iliac arteries Abdominal
Abdominal Aortic Aneurysm 가천대길병원 이상준 1 Definition Diameter of the aorta 1.5 times greater than normal. Most are infrarenal, and a significant number extend down into one or both iliac arteries Abdominal
The Thoracic wall including the diaphragm. Prof Oluwadiya KS
 The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
Endoleak Sealing after AAA Endovascular Repair. When and How?
 Endoleak Sealing after AAA Endovascular Repair. When and How? Poster No.: C-1086 Congress: ECR 2013 Type: Educational Exhibit Authors: D. Quintana Blanco, B. González Humara, E. Torres Diez, C. Jimenez
Endoleak Sealing after AAA Endovascular Repair. When and How? Poster No.: C-1086 Congress: ECR 2013 Type: Educational Exhibit Authors: D. Quintana Blanco, B. González Humara, E. Torres Diez, C. Jimenez
Guide to Small Animal Vascular Imaging using the Vevo 770 Micro-Ultrasound System
 Guide to Small Animal Vascular Imaging using the Vevo 770 Micro-Ultrasound System January 2007 Objectives: After completion of this module, the participant will be able to accomplish the following: Understand
Guide to Small Animal Vascular Imaging using the Vevo 770 Micro-Ultrasound System January 2007 Objectives: After completion of this module, the participant will be able to accomplish the following: Understand
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations
 The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
PERPHERAL ARTERY ANEURYSM. By Pooja Sharma and Susanna Sebastianpillai
 PERPHERAL ARTERY ANEURYSM By Pooja Sharma and Susanna Sebastianpillai Defintions True Aneurysm Involves all three layers of the vessel. Have two basic shapes; Fusiform = symmetric widening of the vessels
PERPHERAL ARTERY ANEURYSM By Pooja Sharma and Susanna Sebastianpillai Defintions True Aneurysm Involves all three layers of the vessel. Have two basic shapes; Fusiform = symmetric widening of the vessels
GI module Lecture: 9 د. عصام طارق. Objectives:
 GI module Lecture: 9 د. عصام طارق Objectives: To list structures forming posterior abdominal wall. To follow aorta & its main branches. To describe IVC & its main tributaries. To list nerves of posterior
GI module Lecture: 9 د. عصام طارق Objectives: To list structures forming posterior abdominal wall. To follow aorta & its main branches. To describe IVC & its main tributaries. To list nerves of posterior
Carotid Artery Doppler
 Carotid Artery Doppler Patient Position supine or semisupine head slightly hyper extended rotated 45 away from the side being examined. Higher frequency linear transducers (7 MHz) Vessels should be imaged
Carotid Artery Doppler Patient Position supine or semisupine head slightly hyper extended rotated 45 away from the side being examined. Higher frequency linear transducers (7 MHz) Vessels should be imaged
STRUCTURED EDUCATION REQUIREMENTS IMPLEMENTATION DATE: JULY 1, 2016
 STRUCTURED EDUCATION REQUIREMENTS Vascular Sonography The purpose of structured education is to provide the opportunity for individuals to develop mastery of discipline-specific knowledge that, when coupled
STRUCTURED EDUCATION REQUIREMENTS Vascular Sonography The purpose of structured education is to provide the opportunity for individuals to develop mastery of discipline-specific knowledge that, when coupled
Section II: Patient Interview Grade: 5
 Only written competency completed with this EXACT form will be accepted for grading. No modifications to the LAYOUT of the form will be accepted for a written competency. Failure to comply will result
Only written competency completed with this EXACT form will be accepted for grading. No modifications to the LAYOUT of the form will be accepted for a written competency. Failure to comply will result
Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University Hospital Sangmin Kim
 Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Lab CT scan. Murad Kharabsheh Yaman Alali
 Lab CT scan Murad Kharabsheh Yaman Alali Some rules to read The CT Scan : 1. Remember that it s a transverse section across the body and we are looking at the inferior part of the section (not the superior),
Lab CT scan Murad Kharabsheh Yaman Alali Some rules to read The CT Scan : 1. Remember that it s a transverse section across the body and we are looking at the inferior part of the section (not the superior),
Evaluation of Dynamic Intimal Flap Movement in Acute Stanford Type B Aortic Dissections (ATBD) and the Effects of Thoracic Endovascular Stent Grafting
 and the Effects of Thoracic Endovascular Stent Grafting") Evaluation of Dynamic Intimal Flap Movement in Acute Stanford Type B Aortic Dissections (ATBD) and the Effects of Thoracic Endovascular Stent Grafting Frank R. Arko, III, MD, Jeko Madjarov, MD, Aaron Hurd,
Evaluation of Dynamic Intimal Flap Movement in Acute Stanford Type B Aortic Dissections (ATBD) and the Effects of Thoracic Endovascular Stent Grafting Frank R. Arko, III, MD, Jeko Madjarov, MD, Aaron Hurd,
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
Open fenestration for complicated acute aortic B dissection
 Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo
Art of Operative Techniques Open fenestration for complicated acute aortic B dissection Santi Trimarchi 1, Sara Segreti 1, Viviana Grassi 1, Chiara Lomazzi 1, Marta Cova 1, Gabriele Piffaretti 2, Vincenzo
Current treatment of Aortic Aneurysms and Dissections. Adam Keefer, MD, FACS Sean Hislop, MD, FACS
 Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
Current treatment of Aortic Aneurysms and Dissections Adam Keefer, MD, FACS Sean Hislop, MD, FACS Patient 1 69 year old well-educated man with reoccurring pain in his upper abdomen and a pulsatile mass.
FHS Appendicitis US Protocol
 FHS Appendicitis US Protocol Reviewed By: Shireen Khan, MD; Sarah Farley, MD; Anna Ellermeier, MD Last Reviewed: May 2018 Contact: (866) 761-4200 **NOTE for all examinations: 1. If documenting possible
FHS Appendicitis US Protocol Reviewed By: Shireen Khan, MD; Sarah Farley, MD; Anna Ellermeier, MD Last Reviewed: May 2018 Contact: (866) 761-4200 **NOTE for all examinations: 1. If documenting possible
Image Formation (10) 2 Evaluation and Selection of Representative Images (10)
 2 Evaluation and Selection of Representative Images (10)") STRUCTURED SELF ASSESSMENT CONTENT SPECIFICATIONS SSA LAUNCH DATE: JANUARY 1, 2018 Vascular Sonography The purpose of continuing qualifications requirements (CQR) is to assist registered technologists
STRUCTURED SELF ASSESSMENT CONTENT SPECIFICATIONS SSA LAUNCH DATE: JANUARY 1, 2018 Vascular Sonography The purpose of continuing qualifications requirements (CQR) is to assist registered technologists
CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D.
 CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D. Thoracic Aortic Aneurysms Atherosclerotic Dissection Penetrating ulcer Mycotic Inflammatory (vasculitis) Traumatic Aortic Imaging Options Catheter
CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D. Thoracic Aortic Aneurysms Atherosclerotic Dissection Penetrating ulcer Mycotic Inflammatory (vasculitis) Traumatic Aortic Imaging Options Catheter
Beyond Stenosis Severity: Top 5 Important Duplex Characteristics to Identify in a Patient with Carotid Disease
 Beyond Stenosis Severity: Top 5 Important Duplex Characteristics to Identify in a Patient with Carotid Disease Jan M. Sloves RVT, RCS, FASE Technical Director New York Cardiovascular Associates Disclosures
Beyond Stenosis Severity: Top 5 Important Duplex Characteristics to Identify in a Patient with Carotid Disease Jan M. Sloves RVT, RCS, FASE Technical Director New York Cardiovascular Associates Disclosures
Endovascular Repair o Abdominal. Aortic Aneurysms. Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida
 Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Subject Area Modules. Subject Area Modules. Subject Area Modules Published on Society for Vascular Surgery (
 Purchasing the VESAP3 comprehensive package provides access to all 10 VESAP3 modules, in learning and exam mode, for $151 less than the cost of purchasing all modules individually. Click here to learn
Purchasing the VESAP3 comprehensive package provides access to all 10 VESAP3 modules, in learning and exam mode, for $151 less than the cost of purchasing all modules individually. Click here to learn
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
The jejunum and the Ileum. Prof. Oluwadiya KS
 The jejunum and the Ileum Prof. Oluwadiya KS www.oluwadiya.siteled.com Introduction Introduction The small intestine (SI) comprises of the duodenum, jejunum and the ileum The jejunum is the second part
The jejunum and the Ileum Prof. Oluwadiya KS www.oluwadiya.siteled.com Introduction Introduction The small intestine (SI) comprises of the duodenum, jejunum and the ileum The jejunum is the second part
Median arcuate ligament syndrome. An unfrequent cause of abdominal pain.
 Median arcuate ligament syndrome. An unfrequent cause of abdominal pain. Poster No.: C-2093 Congress: ECR 2015 Type: Educational Exhibit Authors: L. Caminero, M. L. Rozas, M. E. Banegas Illescas, J. A.
Median arcuate ligament syndrome. An unfrequent cause of abdominal pain. Poster No.: C-2093 Congress: ECR 2015 Type: Educational Exhibit Authors: L. Caminero, M. L. Rozas, M. E. Banegas Illescas, J. A.
Radiologic Evaluation of Peripheral Arterial Disease
 January 2003 Radiologic Evaluation of Peripheral Arterial Disease Grace Tye, Harvard Medical School Year III Patient D.M. CC: 44 y/o male with pain in his buttocks Occurs after walking 2 blocks. Pain is
January 2003 Radiologic Evaluation of Peripheral Arterial Disease Grace Tye, Harvard Medical School Year III Patient D.M. CC: 44 y/o male with pain in his buttocks Occurs after walking 2 blocks. Pain is
Management of Endoleaks
 Management of Endoleaks Sarah Ikponmwosa, MD Brooklyn VA 6/20/08 Questions Advantages of endovascular repair Definition of an endoleak Types of endoleaks Management of type lll endoleak Diagnosis of type
Management of Endoleaks Sarah Ikponmwosa, MD Brooklyn VA 6/20/08 Questions Advantages of endovascular repair Definition of an endoleak Types of endoleaks Management of type lll endoleak Diagnosis of type
Percutaneous Approaches to Aortic Disease in 2018
 Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Abdominal Aortic Aneurysm - Part 1. Learning Objectives. Disclosure. University of Toronto Division of Vascular Surgery
 University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
VESSELS: GROSS ANATOMY
 ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 4e. All text references are for this textbook. 2) Observe and sketch histology slide
ACTIVITY 10: VESSELS AND CIRCULATION OBJECTIVES: 1) How to get ready: Read Chapter 23, McKinley et al., Human Anatomy, 4e. All text references are for this textbook. 2) Observe and sketch histology slide
Non-invasive examination
 Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Artery 1 Head and Thoracic Arteries. Arrange the parts in the order blood flows through them.
 Artery 1 Head and Thoracic Arteries 1. Given the following parts of the aorta: 1. abdominal aorta 2. aortic arch 3. ascending aorta 4. thoracic aorta Arrange the parts in the order blood flows through
Artery 1 Head and Thoracic Arteries 1. Given the following parts of the aorta: 1. abdominal aorta 2. aortic arch 3. ascending aorta 4. thoracic aorta Arrange the parts in the order blood flows through
Imaging Strategy For Claudication
 Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon