Fetal Arrhythmias: Diagnosis and Management. Jonathan T Fleenor, MD, FACC, FAAP Pediatric Cardiology Children s Hospital of the King s Daughters
|
|
|
- Nelson Hubbard
- 5 years ago
- Views:
Transcription
1 Fetal Arrhythmias: Diagnosis and Management Jonathan T Fleenor, MD, FACC, FAAP Pediatric Cardiology Children s Hospital of the King s Daughters

2 No industry or financial disclosures Thanks to Drs Abuhamad and Sinkovskaya Circulation 2014;129:
3
4 Objectives Reviews ways to evaluate fetal arrhythmias Discuss etiologies and treatment for the different types of arrhythmias Irregular HR Tachycardias Bradycardias
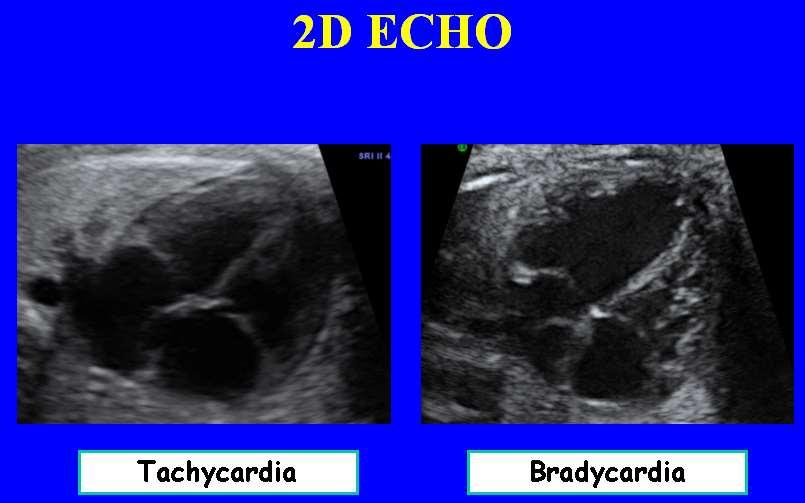
5 Tools to Evaluate Fetal Arrhythmia 2D ECHO M Mode Anatomic M Mode Doppler Tissue Doppler Other (Fetal EKG, Magnetocardiography)
6

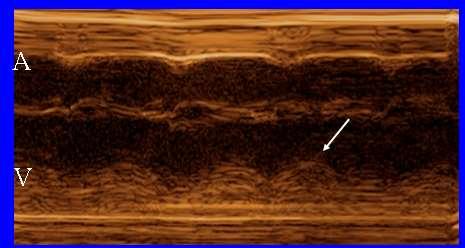
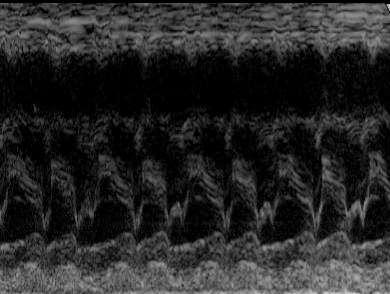
7 M Mode Ventricle Atrium

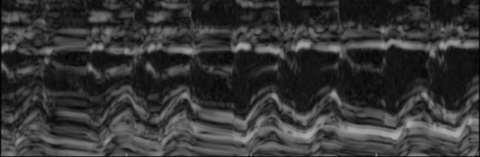
8 Anatomic M Mode

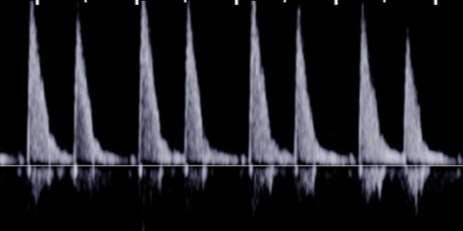
9 Doppler LV Inflow/Outflow А А А V V V


10 Tissue Doppler V V V А А А
11 Other Methods: SVC/Aorta


12 Other Methods: Renal Vessels S: Ventricular systole D: Atrial Diastole A: Atrial systole V V V S А D А А Berg. Ultrasound Obstet Gynecol 2009


13 Other Methods: Pulmonary Vessels S: Ventricular systole D: Atrial Diastole A: Atrial systole V V V А А А S D
14 Classification of Arrhythmias Irregular fetal heart rhythms: irregular due to beat to beat variability, but in the average rate range ( BPM) Tachycardias: > 180 BPM (may be sustained or intermittent); Sinus Tachycardia, SVT, atrial flutter, VT Bradycardias: < 100 BPM; usually complete heart block, sinus bradycardia or blocked PACs
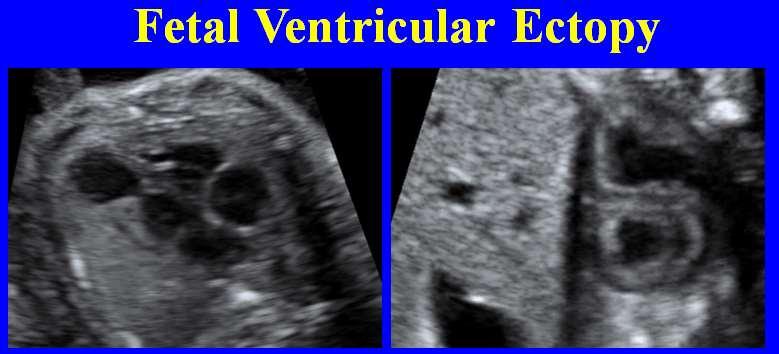
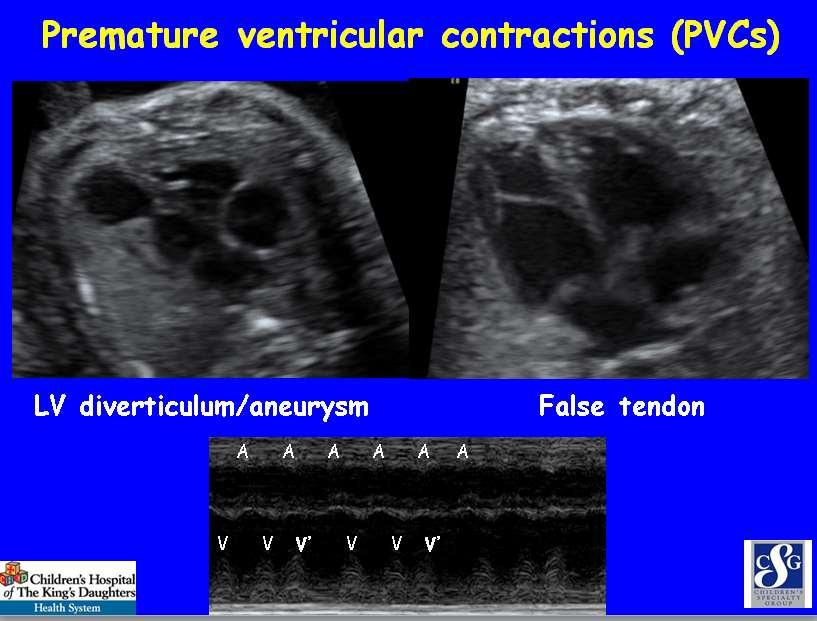
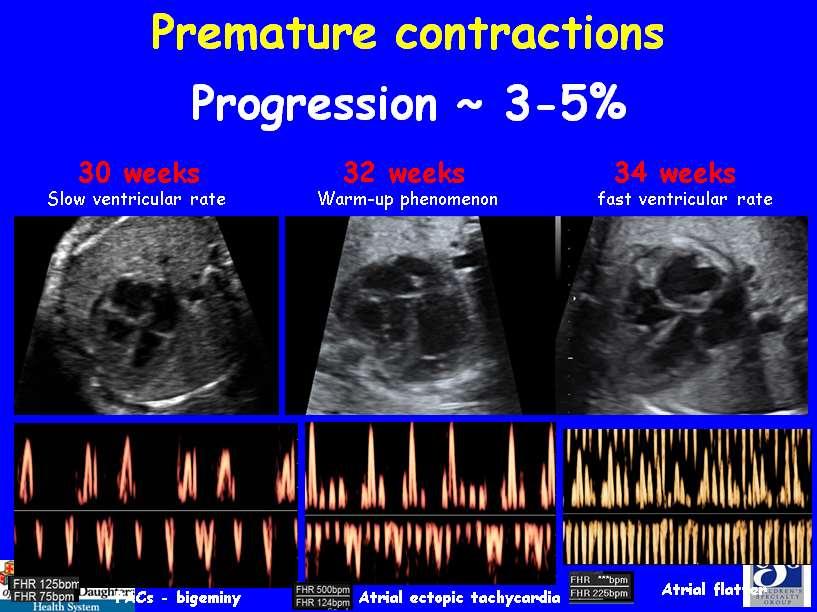
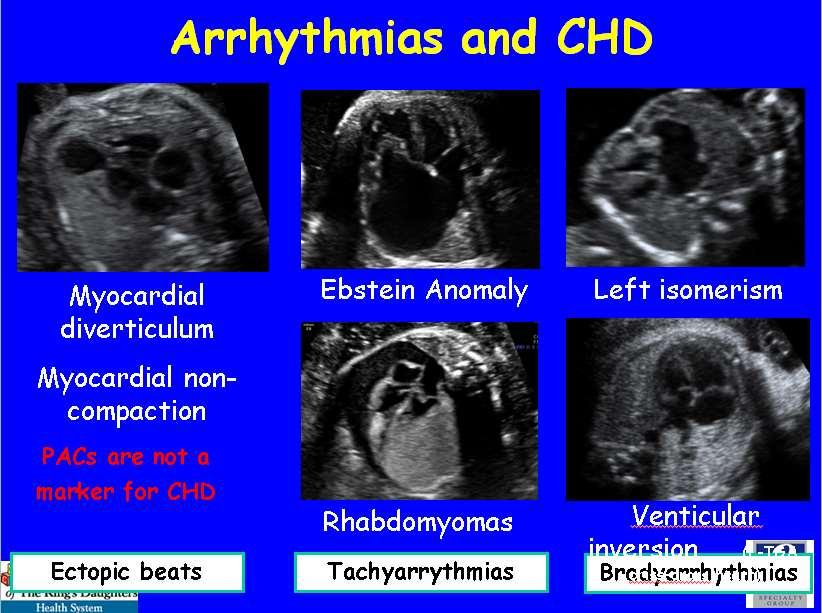
15 Irregular Heart Rhythms Common: PACs (up to 2% of term fetuses) 1 ; PACs most common cause of referral for fetal arrhythmia; PVCs much less common If PACs are very early and frequent, they may be blocked and result in low ventricular rates. Encourage stop smoking, excessive caffeine or use of potential cardiac stimulating drugs (cold meds) PACs are not a marker for CHD (1%; series of 194 fetuses 2 had CHD) 2 ; PACs do not progress to SVT; In general do not need to be referred PVCs seen with CHD at a higher frequency 1 Southall et. al. Arch Dis Child Simpson et al. Cardio Young 1996.


16 PACs vs. PVCs Partial compensatory pause Full compensatory pause А А А А А А А A А V V V V V V V V


17 PACs vs. PVCs Ventricles PAC Conducted Ventricles - PVC Atria - PAC Atria - normal


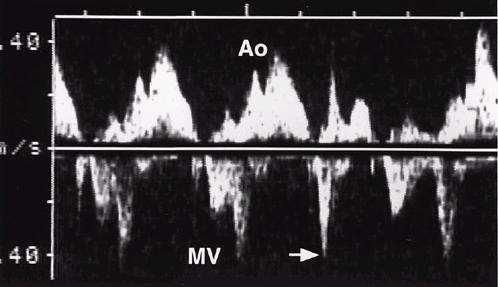
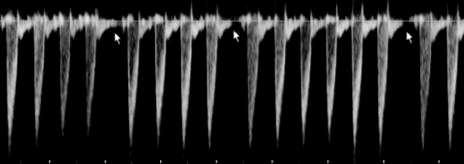
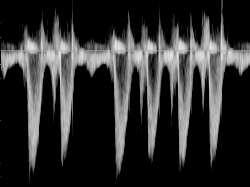
18 Fetal PACs AO outflow Ventricle MV inflow Conducted PAC Atria Blocked PAC
19
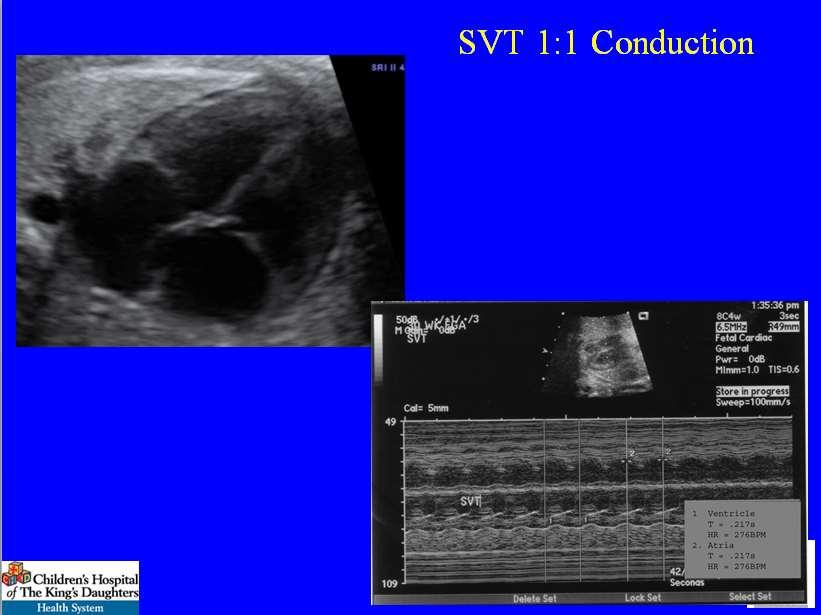
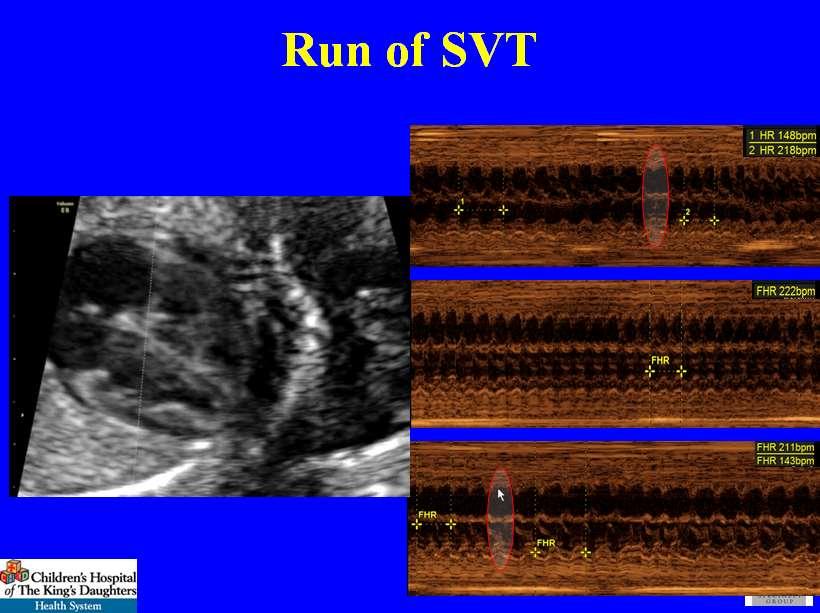
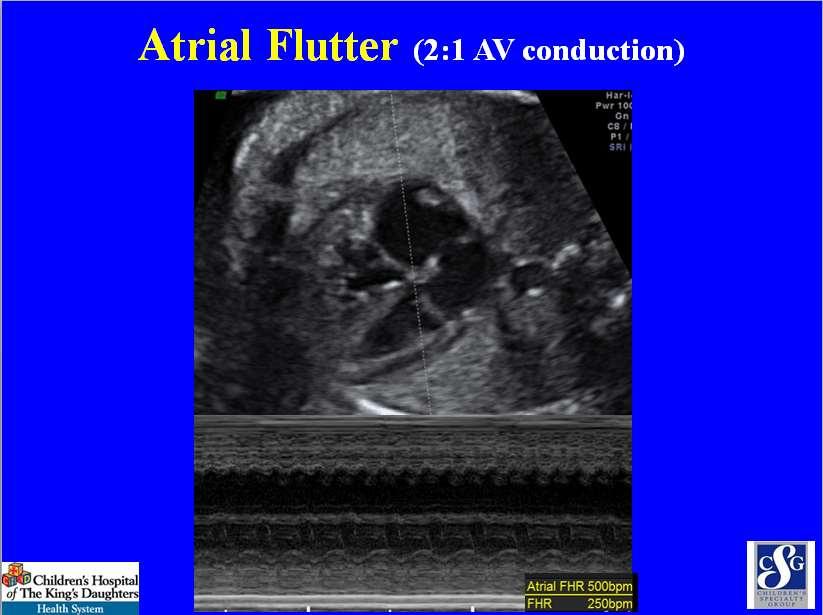
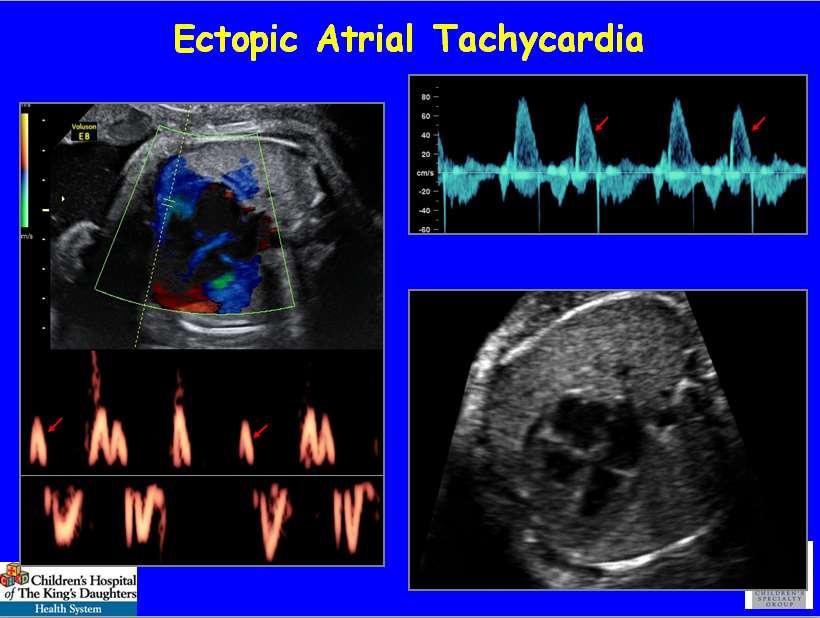
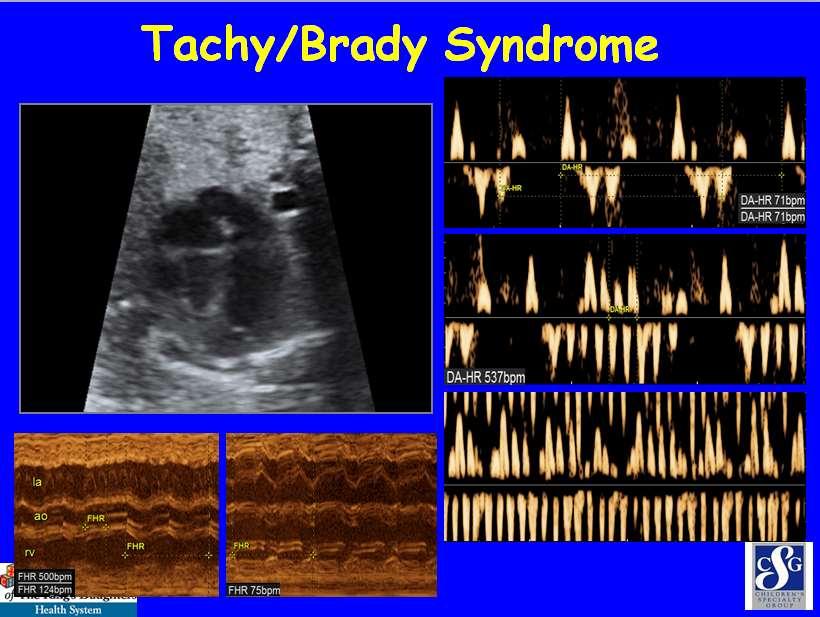
20 Fetal Tachycardias Reentry SVT (70 90%): 1:1 A:V conduction; HR is usually between BPM Atrial flutter (10 30%): variable AV conduction; atrial rates BPM, ventricular rates depend on degree of conduction Ventricular tachycardia (< 1-2%): ventricular rate > atrial rate with atrioventricular dissociation. Sinus Tachycardia
21
22
23
24 Sinus Tachycardia 1. Anemia 2. Infection/maternal fever 3. Hyperthyroid 4. Compression (mass) 5. Drug 6. Fetal Distress
25 Treatment Options Decision to treat depends on gestational age, signs of CHF/hydrops, duration of tachycardic episodes Treatment options can include no treatment with close observation, medical treatment, delivery of infant for failed medical treatment, if they are near term or worsening hydrops Pharmacology of drug treatment during pregnancy is very complex, but depend on maternal, placental and fetal drug absorption, distribution, metabolism and elimination
26 Treatment Options: Digoxin First line treatment in most multi-center experience; best safety profile IV loading dose then bid dosing (maternal trough digoxin level ng/ml); In non-hydrops fetal levels are 60-70% of maternal levels; Hydrops present:20-40% Digoxin as single drug with no hydrops had conversion rate of for SVT (65.4%) and AF: (51.7%) 1 When hydrops was present, digoxin significantly lower conversion rates for SVT (24.6%) and AF (6.3%) 1 1 Krapp et.al. Heart 2003
27 Treatment Options: Flecainide Flecainide (Class IC); 100mg bid tid Proarrhythmia 4 17%, increases digoxin and amiodarone levels Up to 60% effective (16/27) in hydropic fetuses 1 ; 100% nonhydropic fetuses 2,3,4 (smaller numbers) One report on 15 fetuses with SVT and hydrops who had initial failure with digoxin. After addition of flecainide 14/15 had conversion to sinus rhythm and ultimate resolution of hydrops. 5 1 Simpson et.al. Heart Hansmann et.al. Ultras Obstet Gynecol Van Engelen et al. J Am Coll Cardiol Frohn Mulder et.al. Prenat Diag Krapp et.al. Ultras Obstet Gynecol 2002
28 Treatment Options: Sotolol Sotolol (Class III antiarrhythmic); mg bid QTc prolongation (4 5%), bradycardia, hypotension Prospective study on 18 fetuses (9 SVT/9 AF; 3 hydrops) where 12/14 tx with sotolol and 2/4 tx with sotolol/digoxin converted to sinus rhythm. 1 Maternal and fetal blood concentrations showed good coorelation, but did not predict success Sotolol not associated with growth retardation. Used as first line treatment for atrial flutter in some centers. 2 1 Oudijk et. al. JACC; Jaeggi et. al. Sem. Fetal and Neonatal Med; 2005
29 Treatment Options: Amiodarone Amiodarone (Class III antirrhythmic); load mg/d; maint mg/d QTc prolongation, proarrhythmic ~ 1%; bradycardia, hypotension, fetal hypothyroidism, digoxin levels, liver dysfunction, corneal deposition Poor placental transfer (10-40%). Last resort; rarely needed to be used (when delivery of preterm infant is not acceptable and other medications have failed)
30 Treatment Options: Direct Fetal Therapy Direct injection of drugs into fetal circulation (umbilical vein, fetal heart, fetal peritoneum and muscle) Usually used as last resort in severely hydropic fetuses with tachycardia resistant to transplacental therapy and delivery is not a reasonable option. Drugs used amiodarone, digoxin, verapamil and adenosine
31 Comparison of Treatments: Digoxin, Flecainide, Sotalol 159 consecutive pts SVT (114) & AF (45) Randomized 75 (SVT), 36 (AF) to Tx with Digoxin (24), Flecainide (35), Sotalol (52) p =.01 (Dig vs Sotalol) P =.02 (Flec vs Sotalol) p =.05 (Sotalol vs Dig) P =.03 (Sotalol vs Flec) Jaeggi et. al. Circulation 2011
32 Tx Summary for Fetal Tachycardia at CHKD/EVMS Digoxin first line for reentry SVT (1:1) without hydrops Use other medications (Flecainide, Sotalol) for failure of digoxin, or as primary treatment if fetal hydrops is present or arrhythmia is atrial flutter. For sinus tachycardia look for other causes
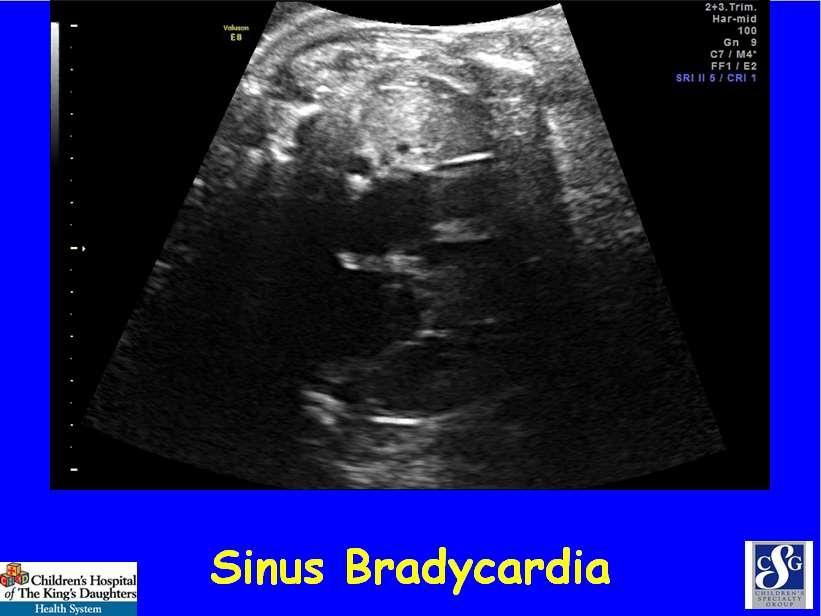
33 Bradycardia PAC s not conducted (discussed) Sinus Bradycardia Complete heart block

34 Sinus Bradycardia E A V
35 Sinus Bradycardia Variation on normal Fetal distress Long QT syndrome Cardiomyopathy Myocarditis Maternal hypothyroidism Maternal meds Fetal CNS malformations
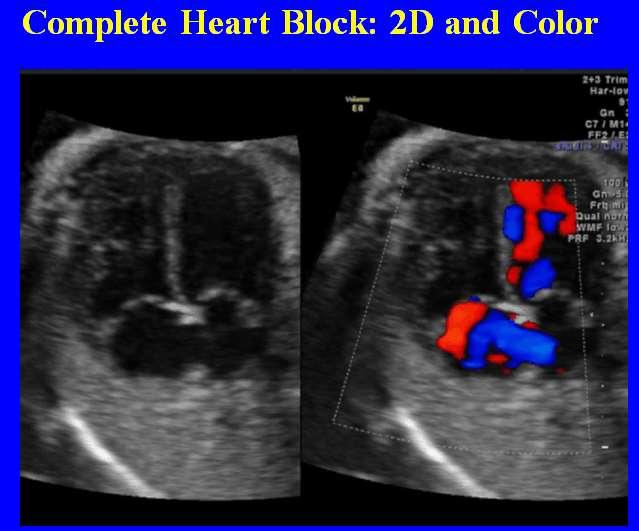
36
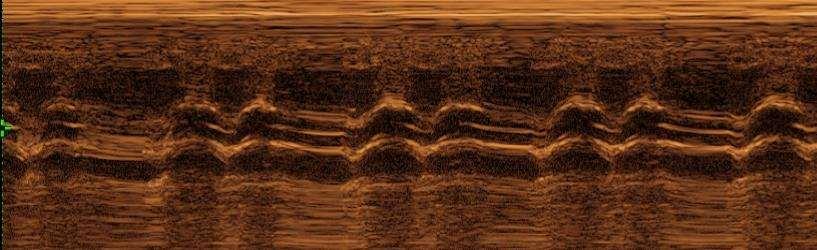
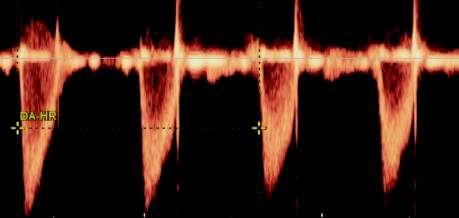
37 Complete Heart Block: MMode Ventricular Atrial

38 Complete Heart Block: MMode V A

39 Complete Heart Block: Pulse Doppler Ventricular Atrial

40 Complete Heart Block: Tissue Doppler Ventricular Atrial
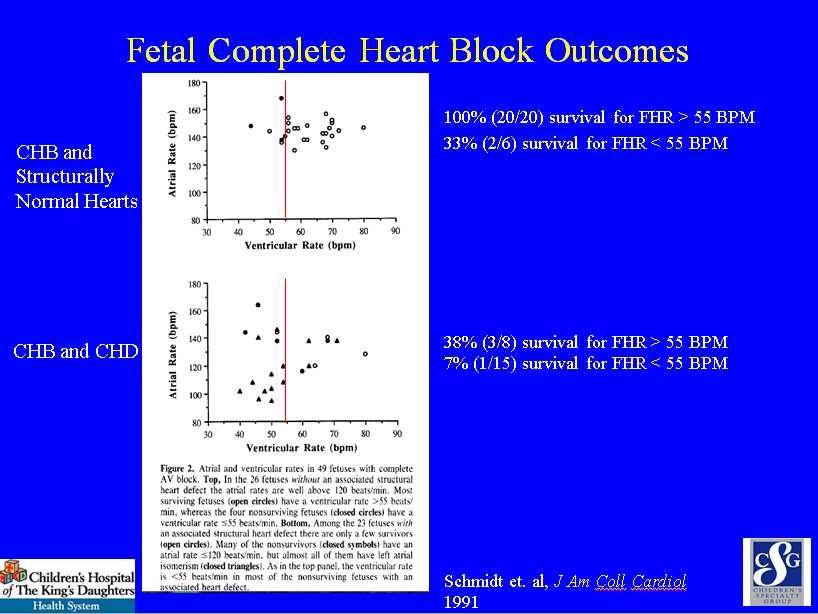
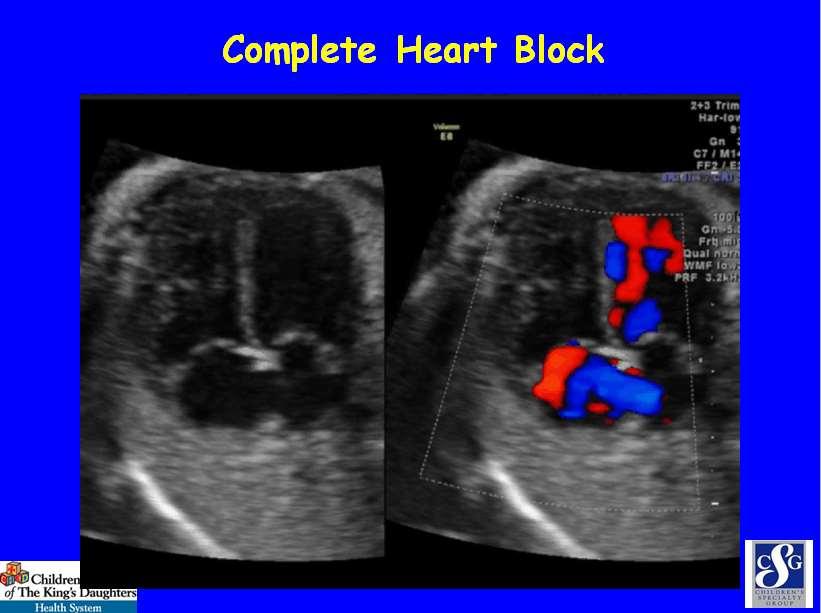
41 Fetal Complete Heart Block Outcomes Multicenter study of 55 fetuses with CHB 29 (53%) with CHD (heterotaxy, L atrial isomerization), 19 (35%) structurally nl hearts (+ antibody screen) 7 (13%) idiopathic Survival to neonatal period: 14% in CHD group; 85% in children with structurally normal hearts. Schmidt et. al, J Am Coll Cardiol 1991
42
 Conclusion: CHB can develop")
43 Predicting Fetal CHB - AV Interval PRIDE Study 98 pregnancies anti-ssa positive 3 fetuses developed CHB; none showed prolongation of AV interval prior, none improved with dexamethasone 2 fetuses developed AV interval > 150 ms; both reversed within 1 wk with Tx dexamethasone Mechanical AV interval: Beginning of A wave upstroke of Ventricular flow >150 ms (3 SD) Conclusion: CHB can develop within 1 wk of normal ECHO with normal PR interval. Perform intense monitoring wks EGA Friedman et.al; Circulation, 2008
44 Predicting Fetal CHB AV Interval 165 pregnancies anti-ssa positive prospectively studied fetus developed CHB (28 wks); 3 nl ECHO (19 24 wks) 11 (7%) fetuses: transient prolongation of AV interval (< 3 z-scores) No treatment 10/11 had normal ECG at 56 (range 43-87) DOL No treatment 1/11 had ECG with 1 AVB that has persisted (now 6yo) 3 (2%) fetuses: persistent prolonged AV interval (> 3 z-scores) No treatment given; one Nl ECG at birth, one 1 AVB at birth that resolved, one 1 AVB that has persisted (now 3 yo) Conclusions: Prolonged AV interval is a benign condition and in not predictive of development of CHB. Jaeggi et.al; JACC, 2011
45 Predicting Fetal CHB: Past Pregnancy Hx, Antibody Level PRIDE study: CHB developed in 19% of pregnancies with previously effective child, 4% in no prior effective child. (P=0.067) 1 Anti-Ro/SSA antibody level as predictor of development of CHB: 8 yr study comparing 146 SSA positive fetuses with no CHB compared to 40 SSA positive fetuses with CHB All CHB were associated with moderate (>50 U/ml) and high (>100 U/ml) Event rate of CHB was 5% in prospectively screened fetuses with SSA levels >50 U/ml (odds ratio: 7.8) and 0% for fetuses with lower titers (p < ) 1 Friedman et.al; Circulation, Jaeggi et.al; JACC 2010
46 Fetal CHB Treatment Treatment depends on etiology of CHB, gestational age, fetal heart rate and presence of fetal hydrops Treatment options are often institution specific and can include steroids, sympathomimetics, IVIG, and premature delivery
47 Fetal CHB Treatment Steroids Fluorinated steroids (Dexamethasone/betamethasone) cross placenta well and is commonly used when etiology of maternal autoantibody is suspected Use is supported by small cases series and case reports (no large prospective studies) Complications can include growth restriction, oligohydramios, ductal constriction, maternal DM, CNS effect
48 Fetal CHB Treatment Sympathomimetics Salbutamol (Canada): 20% increase in HR from baseline (N=3; 2 w/hydrops) 1 Terbutaline: 7 infants with FHR < 60 treated, 6/7 showed initial increase HR; 4 maintained HR > 60, 2 returned to HR < 60 and 1 fetal death 2 Terbutaline: 17 fetuses (8 isoimmune, 9 heterotaxy) treated for HR < 55. All survived to delivery. Greater atrial rates in isommune vs ventricular rate for heterotaxy 3 1 Groves et. al. Circulation Robinson et. al. Cardiol Young Cuneo et.al. Am J Cardio, 2007
49 Fetal CHB Treatment IVIG: Small case series in severely affected fetuses (EFE or cardiomyopathy) used in conjunction with Dexamethasone showed some improvement in outcomes 1 Direct fetal pacing through has been reported as single case reports; short lived improvement Plasmapharesis is theorized to decrease maternal antibody delivery; not supported with literature, significant maternal risk 1 Trucco et. al. JACC, 2010
50 Fetal CHB Treatment: Toronto Children s Management of CHB since 1997 Jaeggi et. al. Circulation, 2004
51 Fetal Arrhythmias: Summary Fetal arrhythmias are common, often due to premature atrial ectopic beats and usually benign Some arrhythmias are more important and life threatening resulting in fetal tachycardia and bradycardia Treatment modalities are variable and depends on etiology, gestational age and signs of CHF/hydrops Team approach with MFM, pediatric cardiology, delivery at tertiary care hospital will result in best outcomes
52 Extra Slides
53 Fetal Complete Heart Block Outcomes 37 fetuses identified over 8 years with CHB 21 (57%) with CHD; 17 Heterotaxy (L atrial isom) 16 (43%) with isolated CHB (all + anti-ro; SSA) Hydrops: 11/21 w/chd 4/16 w/ isolated CHB Survival though pregnancy and newborn period: 15% in CHD group; 69% in isolated CHB group. Machado et al. Br Heart J, 1988
54 Doppler

55 Fetal PACs

56 Fetal PACs

57 Fetal PACs

58 Fetal PACs

59 Doppler SVC and Aorta

60 SVT

61 Atrial Flutter
62
63

64 Fetal Bradycardia (Complete Heart Block)

65 PACs vs. PVCs
66




67 Conducted vs. Blocked PACs V V V V V А А А А Extra beat А А А А Skipped beat

68 Single conducted PAC V V А А А

69 Single conducted PAC V V V V А А А А
70 Single blocked PAC V V А А А

71 Single blocked PAC V V V А А А А




72 Frequent vs. Infrequent



73 Random vs. Rhythmic patterns Bigeminy Chaotic Trigeminy
74
75 Irregular fetal heart rhythm Management options Isolated Infrequent Random Intermittent PACs or PVCs Combined with CHD Frequent Bi-/trigeminy Sustained PACs or PVCs No Follow up at MFM No arrhythmia Treatment Follow up at MFM in 2 weeks Persistence Progression Delivery
76 Tachyarrythmias Classification 1. Sinus tachycardia 2. Supraventricular tachycardia Paroxysmal Sustained 3. Ventricular tachycardia 4. Atrial Flatter 5. Atrial fibrillation
 5.")
77 Sinus tachycardia 1:1 AV conduction 1. Anaemia 2. Infection/maternal fever 3. Fetal thyrotoxicosis 4. Compression (mass) 5. Drugs 6. Fetal distress
78
79 Tachyarrhythmias: treatment From Fetal Cardiology by Yagel; 2003
80 Tachyarrhythmias: treatment From Fetal Cardiology by Yagel; 2003
81 Bradyarrhythmias: Classification 1. Sinus bradycardia Intermittent Intermittent Sustained Sustained 2. Frequent blocked PACs 3. Second-degree heart block 4. Third-degree heart block (complete)

82 -Fetal distress Sinus Bradycardia 1:1 AV conduction S -Sinus node dysfunction -Long QT syndrome
83



84 Frequent blocked PACs - bigenimy V A E S D S D А



85 Frequent blocked PACs - trigeminy

86 Second-degree Heart Block
87


88 Complete heart block: M-mode at 4-chamber view
89 Complete heart block: Doppler at LVOT
90 Complete Heart Block With CHD ~ 40% Heterotaxy: Ventricular left isomerism inversion Fetal Hydrops 63% Survival rate 13% Without CHD ~ 60% Anti-SSA/Ro Anti-SSA/Ro > 100 U/ml negative Fetal Hydrops 20% Survival rate 78%
91 From Fetal Cardiology by Yagel; 2003 Bradyarrhythmias: Differential diagnosis
92 Complete Heart Block Management options Referrals at weeks Late referrals > 32 weeks Ye s + SALBUTAMOL Ye s + Ig 70g every 2-3 weeks Ventricular rate < 50bpm Endocardial fibroelastosis No No Basic treatment DEXAMETHASONE: 8mg/d 2 weeks 4mg/d 2weeks 2md/d 2 weeks US follow up every 1-2 weeks Delivery: weeks, CS No treatment Scan. J. Immun. 2010, 72:
93
Fetal Rhythm and Blues
 Fetal Rhythm and Blues John Cotton, MD Professor of Pediatrics Division of Pediatric Cardiology Director, Fetal Cardiology Program UNC Chapel Hill, School of Medicine Objectives To review methods used
Fetal Rhythm and Blues John Cotton, MD Professor of Pediatrics Division of Pediatric Cardiology Director, Fetal Cardiology Program UNC Chapel Hill, School of Medicine Objectives To review methods used
Evaluation of Fetal Arrhythmias
 REVIEW ARTICLE Evaluation of Fetal Arrhythmias George M Graham III DSJUOG Evaluation of Fetal Arrhythmias Assistant Professor, Division of Maternal Fetal Medicine, Department of Obstetrics, Gynecology
REVIEW ARTICLE Evaluation of Fetal Arrhythmias George M Graham III DSJUOG Evaluation of Fetal Arrhythmias Assistant Professor, Division of Maternal Fetal Medicine, Department of Obstetrics, Gynecology
Supraventricular Tachycardia: From Fetus to Adult. Mohamed Hamdan, MD
 Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Assessment of fetal heart function and rhythm
 Assessment of fetal heart function and rhythm The fetal myocardium Early Gestation Myofibrils 30% of myocytes Less sarcoplasmic reticula Late Gestation Myofibrils 60% of myocytes Increased force per unit
Assessment of fetal heart function and rhythm The fetal myocardium Early Gestation Myofibrils 30% of myocytes Less sarcoplasmic reticula Late Gestation Myofibrils 60% of myocytes Increased force per unit
How Does Imaging Inform Fetal Cardiovascular Treatment?
 How Does Imaging Inform Fetal Cardiovascular Treatment? Edgar Jaeggi, MD Head, Fetal Cardiac Program Labatt Family Heart Center Department of Pediatrics The Hospital for Sick Children University of Toronto
How Does Imaging Inform Fetal Cardiovascular Treatment? Edgar Jaeggi, MD Head, Fetal Cardiac Program Labatt Family Heart Center Department of Pediatrics The Hospital for Sick Children University of Toronto
Fetal Arrythmia. Doç. Dr. Özgür ÖZYÜNCÜ. Hacettepe Üniversitesi Tıp Fakültesi. Kadın Hastalıkları ve Doğum AD
 Fetal Arrythmia Doç. Dr. Özgür ÖZYÜNCÜ Hacettepe Üniversitesi Tıp Fakültesi Kadın Hastalıkları ve Doğum AD Introduction Arrhythmias Can occur as soon as the heart starts to beat End on a final irreversible
Fetal Arrythmia Doç. Dr. Özgür ÖZYÜNCÜ Hacettepe Üniversitesi Tıp Fakültesi Kadın Hastalıkları ve Doğum AD Introduction Arrhythmias Can occur as soon as the heart starts to beat End on a final irreversible
Everything You Always Wanted to Know About Fetal Arrhythmias, in 40 Minutes!
 Everything You Always Wanted to Know About Fetal Arrhythmias, in 40 Minutes! Fetal Arrhythmias! What is clinically important?!tachycardia (>200)!Fixed bradycardia (
Everything You Always Wanted to Know About Fetal Arrhythmias, in 40 Minutes! Fetal Arrhythmias! What is clinically important?!tachycardia (>200)!Fixed bradycardia (
I have nothing to disclose.
 I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
Rate: The atrial and ventricular rates are equal; heart rate is greater than 100 bpm (usually between bpm).
.") Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Introduction to Fetal Medicine. Lloyd R. Feit M.D. Associate Professor of Pediatrics Warren Alpert Medical School Brown University
 Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
CARDIAC ARRHYTHMIAS IN NEONATE
 Introduction: CARDIAC ARRHYTHMIAS IN NEONATE DR. PANKAJ SAKHUJA Neonatologist Average heart rate in a healthy newborn is 120-160 beats/min and the range is from 80-230 beats/min. A normal (sinus) rhythm
Introduction: CARDIAC ARRHYTHMIAS IN NEONATE DR. PANKAJ SAKHUJA Neonatologist Average heart rate in a healthy newborn is 120-160 beats/min and the range is from 80-230 beats/min. A normal (sinus) rhythm
Journal of the American College of Cardiology Vol. 57, No. 13, by the American College of Cardiology Foundation ISSN /$36.
 Journal of the American College of Cardiology Vol. 57, No. 13, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2010.12.014
Journal of the American College of Cardiology Vol. 57, No. 13, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2010.12.014
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC
 Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
Clinical Guidance. Extrasystoles in the neonatal period. Author: Peter Lillitos
 1 Clinical Guidance Extrasystoles in the neonatal period Author: Peter Lillitos Contents Page 2: Definition of extrasystoles/ectopic beats Page 3: Algorithm of management Page 4-5: Ordering investigations
1 Clinical Guidance Extrasystoles in the neonatal period Author: Peter Lillitos Contents Page 2: Definition of extrasystoles/ectopic beats Page 3: Algorithm of management Page 4-5: Ordering investigations
Digoxin Therapy of Fetal Superior Ventricular Tachycardia: Are Digoxin Serum Levels Reliable?
 e272 Case Report THIEME Digoxin Therapy of Fetal Superior Ventricular Tachycardia: Are Digoxin Serum Levels Reliable? Antonio F. Saad, MD 1 Luis Monsivais, MD 1 Luis D. Pacheco, MD 1,2 1 Division of Maternal-Fetal
e272 Case Report THIEME Digoxin Therapy of Fetal Superior Ventricular Tachycardia: Are Digoxin Serum Levels Reliable? Antonio F. Saad, MD 1 Luis Monsivais, MD 1 Luis D. Pacheco, MD 1,2 1 Division of Maternal-Fetal
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
ARRHYTHMIAS IN THE ICU
 ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE. Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology
 PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
Doppler Echocardiography in the Diagnosis and Management of Persistent Fetal Arrhythmias
 1386 JACC Vol 7. No 6 June 19X6 I3Xh-91 Doppler Echocardiography in the Diagnosis and Management of Persistent Fetal Arrhythmias JANETTE F. STRASBURGER, MD, JAMES C. HUHTA, MD, FACC, ROBERT J. CARPENTER,
1386 JACC Vol 7. No 6 June 19X6 I3Xh-91 Doppler Echocardiography in the Diagnosis and Management of Persistent Fetal Arrhythmias JANETTE F. STRASBURGER, MD, JAMES C. HUHTA, MD, FACC, ROBERT J. CARPENTER,
Ventricular arrhythmias
 Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
Return to Titanic: Irregular Heart Beats. Ric Samson, MD Children s Heart Center - Nevada
 Return to Titanic: Irregular Heart Beats Ric Samson, MD Children s Heart Center - Nevada The Titanic RMS Titanic largest ship ever built up to that time maiden voyage April 1912 travelling from Southampton
Return to Titanic: Irregular Heart Beats Ric Samson, MD Children s Heart Center - Nevada The Titanic RMS Titanic largest ship ever built up to that time maiden voyage April 1912 travelling from Southampton
Practical Approach to Arrhythmias
 Outline Practical Approach to Arrhythmias Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Conduction System ECG Acquisition ECG Interpretation Heart rate Rhythm Arrhythmias Tachyarrhythmias Supraventricular
Outline Practical Approach to Arrhythmias Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Conduction System ECG Acquisition ECG Interpretation Heart rate Rhythm Arrhythmias Tachyarrhythmias Supraventricular
Basic Dysrhythmia Interpretation
 Basic Dysrhythmia Interpretation Objectives 2 To understand the Basic ECG To understand the meaning of Dysrhythmia To describe the normal heart conduction system. To describe the normal impulse pathways.
Basic Dysrhythmia Interpretation Objectives 2 To understand the Basic ECG To understand the meaning of Dysrhythmia To describe the normal heart conduction system. To describe the normal impulse pathways.
Postnatal Outcome in Patients With Fetal Tachycardia
 Pediatr Cardiol (2013) 34:81 87 DOI 10.1007/s00246-012-0392-7 ORIGINAL ARTICLE Postnatal Outcome in Patients With Fetal Tachycardia Shreya Moodley Shubhayan Sanatani James E. Potts George G. S. Sandor
Pediatr Cardiol (2013) 34:81 87 DOI 10.1007/s00246-012-0392-7 ORIGINAL ARTICLE Postnatal Outcome in Patients With Fetal Tachycardia Shreya Moodley Shubhayan Sanatani James E. Potts George G. S. Sandor
Fetal tachyarrhythmia may cause nonimmune fetal hydrops
 Sotalol in the Treatment of Fetal Dysrhythmias Martijn A. Oudijk, MD; Maaike M. Michon, MD; Charles S. Kleinman, MD, PhD; Livia Kapusta, MD; Philip Stoutenbeek, MD, PhD; Gerard H.A. Visser, MD, PhD; Erik
Sotalol in the Treatment of Fetal Dysrhythmias Martijn A. Oudijk, MD; Maaike M. Michon, MD; Charles S. Kleinman, MD, PhD; Livia Kapusta, MD; Philip Stoutenbeek, MD, PhD; Gerard H.A. Visser, MD, PhD; Erik
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment
 Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT
 ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
EKG Competency for Agency
 EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
Antiarrhythmic Drugs
 Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
ECHOGENIC FETAL HEART WITHOUT HEART BLOCK AND MATERNAL ANTI- Ro/ La ANTIBODIES POSITIVITY A LESS KNOWN ASSOCIATION
 ECHOGENIC FETAL HEART WITHOUT HEART BLOCK AND MATERNAL ANTI- Ro/ La ANTIBODIES POSITIVITY A LESS KNOWN ASSOCIATION DR PUNDALIK BALIGA FELLOW IN FETAL MEDICINE MEDISCAN SYSTEMS, CHENNAI CASE 1 30 year old
ECHOGENIC FETAL HEART WITHOUT HEART BLOCK AND MATERNAL ANTI- Ro/ La ANTIBODIES POSITIVITY A LESS KNOWN ASSOCIATION DR PUNDALIK BALIGA FELLOW IN FETAL MEDICINE MEDISCAN SYSTEMS, CHENNAI CASE 1 30 year old
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Perinatal management and long-term cardiac outcome in fetal arrhythmia
 8 Perinatal management and long-term cardiac outcome in fetal arrhythmia Early Human Development. 2010;87(2):83-87 chapter 8 ABSTRACT Background Cardiac arrhythmias are commonly observed in the fetus,
8 Perinatal management and long-term cardiac outcome in fetal arrhythmia Early Human Development. 2010;87(2):83-87 chapter 8 ABSTRACT Background Cardiac arrhythmias are commonly observed in the fetus,
Module 1: Introduction to ECG & Normal ECG
 Module 1: Introduction to ECG & Normal ECG Importance of Correct anatomical positions Measurements & Morphologies ONLY accurate if Precise anatomical positions adhered to Standardised techniques are used
Module 1: Introduction to ECG & Normal ECG Importance of Correct anatomical positions Measurements & Morphologies ONLY accurate if Precise anatomical positions adhered to Standardised techniques are used
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University. OBHG Education Subcommittee
 -RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
Prenatal diagnosis of long QT syndrome: Implications for delivery room and neonatal management
 Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Pediatrics Faculty Publications Pediatrics 2-2013 Prenatal diagnosis of long QT syndrome: Implications
Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Pediatrics Faculty Publications Pediatrics 2-2013 Prenatal diagnosis of long QT syndrome: Implications
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
A ccording to published reports, atrial flutter accounts for a
 913 CONGENITAL HEART DISEASE Review of diagnosis, treatment, and outcome of fetal atrial flutter compared with supraventricular tachycardia M Krapp, T Kohl, J M Simpson, G K Sharland, A Katalinic, U Gembruch...
913 CONGENITAL HEART DISEASE Review of diagnosis, treatment, and outcome of fetal atrial flutter compared with supraventricular tachycardia M Krapp, T Kohl, J M Simpson, G K Sharland, A Katalinic, U Gembruch...
Update on Palpitations and AF February 28 th 2018
 Update on Palpitations and AF February 28 th 2018 Dr Mrinal Andrew Saha MA(Cantab) MBBS FRCP PhD Consultant Interventional Cardiologist GHNHSFT Dr Mrinal Saha Appointed 2010 Special interests: Angioplasty,
Update on Palpitations and AF February 28 th 2018 Dr Mrinal Andrew Saha MA(Cantab) MBBS FRCP PhD Consultant Interventional Cardiologist GHNHSFT Dr Mrinal Saha Appointed 2010 Special interests: Angioplasty,
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Assessment of Cardiac Rate and Rhythm in Fetuses with Arrhythmia via Maternal Abdominal Fetal Electrocardiography
 e176 Case Report THIEME Assessment of Cardiac Rate and Rhythm in Fetuses with Arrhythmia via Maternal Abdominal Fetal Electrocardiography Hari K. Narayan, MD 1 Emilia F. Vignola, MSPH 2 William P. Fifer,
e176 Case Report THIEME Assessment of Cardiac Rate and Rhythm in Fetuses with Arrhythmia via Maternal Abdominal Fetal Electrocardiography Hari K. Narayan, MD 1 Emilia F. Vignola, MSPH 2 William P. Fifer,
The pill-in-the-pocket strategy for paroxysmal atrial fibrillation
 The pill-in-the-pocket strategy for paroxysmal atrial fibrillation KONSTANTINOS P. LETSAS, MD, FEHRA LABORATORY OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL OF ATHENS ARRHYTHMIAS UPDATE,
The pill-in-the-pocket strategy for paroxysmal atrial fibrillation KONSTANTINOS P. LETSAS, MD, FEHRA LABORATORY OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL OF ATHENS ARRHYTHMIAS UPDATE,
Amiodarone Prescribing and Monitoring: Back to the Future
 Amiodarone Prescribing and Monitoring: Back to the Future Subha L. Varahan, MD, FHRS, CCDS Electrophysiologist Oklahoma Heart Hospital Oklahoma City, OK Friday, February, 8 th, 2019 Iodinated benzofuran
Amiodarone Prescribing and Monitoring: Back to the Future Subha L. Varahan, MD, FHRS, CCDS Electrophysiologist Oklahoma Heart Hospital Oklahoma City, OK Friday, February, 8 th, 2019 Iodinated benzofuran
Before we are Born: Fetal Diagnosis of Congenital Heart Disease
 Before we are Born: Fetal Diagnosis of Congenital Heart Disease Mohamed Sulaiman, MD Pediatric cardiologist Kidsheart: American Fetal & Children's Heart Center Dubai Healthcare City, Dubai-UAE First Pediatric
Before we are Born: Fetal Diagnosis of Congenital Heart Disease Mohamed Sulaiman, MD Pediatric cardiologist Kidsheart: American Fetal & Children's Heart Center Dubai Healthcare City, Dubai-UAE First Pediatric
ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE
 Azienda Ospedaliera Universitaria Integrata Verona ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE C.Sandrini *, L.Rossetti *, M.Rebonato *, M.A.Prioli *, F.Bettinazzi,
Azienda Ospedaliera Universitaria Integrata Verona ISOLATED ANOMALOUS DEVELOPMENT OF MYOCARDIUM DURING FETAL LIFE: EXPERIENCE OF OUR CENTRE C.Sandrini *, L.Rossetti *, M.Rebonato *, M.A.Prioli *, F.Bettinazzi,
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
TACHYARRHYTHMIAs. Pawel Balsam, MD, PhD
 TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
Core Content In Urgent Care Medicine
 Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
Dysrhythmias. Dysrythmias & Anti-Dysrhythmics. EKG Parameters. Dysrhythmias. Components of an ECG Wave. Dysrhythmias
 Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Cardiac Arrhythmias. Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company
 Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
2017 BDKA Review. Regularity Rate P waves PRI QRS Interpretation. Regularity Rate P waves PRI QRS Interpretation 1/1/2017
 1. 2017 BDKA Review 2. 3. 4. Interpretation 5. QT 6. 7. 8. 9. 10. QT 11. 12. 13. 14. 15. 16. 17. 18. QT 19. 20. QT 21. 22. QT 23. 24. Where are pacer spikes? Before the P wave or before the QRS complex?
1. 2017 BDKA Review 2. 3. 4. Interpretation 5. QT 6. 7. 8. 9. 10. QT 11. 12. 13. 14. 15. 16. 17. 18. QT 19. 20. QT 21. 22. QT 23. 24. Where are pacer spikes? Before the P wave or before the QRS complex?
Paroxysmal Supraventricular Tachycardia PSVT.
 Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG?
 Objectives What s in an ECG?") Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
Prenatal diagnosis of sustained bradycardia with 1 : 1 atrioventricular conduction
 Ultrasound Obstet Gynecol 2003; 21: 234 238 Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.71 Prenatal of sustained bradycardia with 1 : 1 atrioventricular conduction
Ultrasound Obstet Gynecol 2003; 21: 234 238 Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.71 Prenatal of sustained bradycardia with 1 : 1 atrioventricular conduction
Chad Morsch B.S., ACSM CEP
 What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
I n extrauterine life, narrow QRS supraventricular tachycardia
 1211 CONGENITAL HEART DISEASE Management of fetal tachyarrhythmia based on superior vena cava/aorta Doppler flow recordings J-C Fouron, A Fournier, F Proulx, J Lamarche, J L Bigras, C Boutin, M Brassard,
1211 CONGENITAL HEART DISEASE Management of fetal tachyarrhythmia based on superior vena cava/aorta Doppler flow recordings J-C Fouron, A Fournier, F Proulx, J Lamarche, J L Bigras, C Boutin, M Brassard,
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Management of Arrhythmias The General Practitioners role
 Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Rate and Rhythm Control of Atrial Fibrillation
 Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs
 EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
Pregnancy and Heart Disease. Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA
 Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Palpitations.
 Palpitations http://www.heartfailurematters.org/en/understandingheartfailure/publishingimages/palpitations_lg.jpg Palpitations are the perception of cardiac activity. They are often described as a fluttering,
Palpitations http://www.heartfailurematters.org/en/understandingheartfailure/publishingimages/palpitations_lg.jpg Palpitations are the perception of cardiac activity. They are often described as a fluttering,
ECG S: A CASE-BASED APPROACH December 6,
 ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
Atrial Flutter in Infants
 Journal of the American College of Cardiology Vol. 48, No. 5, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.04.091
Journal of the American College of Cardiology Vol. 48, No. 5, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.04.091
EKG Abnormalities. Adapted from:
 EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
Systematic approach to Fetal Echocardiography. Objectives. Introduction 11/2/2015
 Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh
 Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
physiology 6 Mohammed Jaafer Turquoise team
 15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
ULTRASOUND OF THE FETAL HEART
 ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
ARRHYTHMIAS IN THE INTENSIVE CARE UNIT
 ARRHYTHMIAS IN THE INTENSIVE CARE UNIT Nicole Van Israël, DVM, CESOpht, CertSAM, CertVC, DECVIM-CA (Cardiology), MSc, MRCVS European Specialist in Veterinary Cardiology Animal CardioPulmonary Consultancy
ARRHYTHMIAS IN THE INTENSIVE CARE UNIT Nicole Van Israël, DVM, CESOpht, CertSAM, CertVC, DECVIM-CA (Cardiology), MSc, MRCVS European Specialist in Veterinary Cardiology Animal CardioPulmonary Consultancy
ABCs of ECGs. Shelby L. Durler
 ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
Fetal arrhythmia and long-term outcome
 Proefschrift H. Nagel 11-01-2007 13:34 Pagina 113 C H A P T E R 8 Fetal arrhythmia and long-term outcome HTC Nagel I Aziz NA Blom L Rozendaal HHH Kanhai FPHA Vandenbussche Submitted 113 Proefschrift H.
Proefschrift H. Nagel 11-01-2007 13:34 Pagina 113 C H A P T E R 8 Fetal arrhythmia and long-term outcome HTC Nagel I Aziz NA Blom L Rozendaal HHH Kanhai FPHA Vandenbussche Submitted 113 Proefschrift H.
Dr.Binoy Skaria 13/07/15
 Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Diagnosis of Congenital Cardiac Defects Between 11 and 14 Weeks Gestation in High-Risk Patients
 Article Diagnosis of Congenital Cardiac Defects Between 11 and 14 Weeks Gestation in High-Risk Patients Zeev Weiner, MD, Abraham Lorber, MD, Eliezer Shalev, MD Objective. To examine the feasibility of
Article Diagnosis of Congenital Cardiac Defects Between 11 and 14 Weeks Gestation in High-Risk Patients Zeev Weiner, MD, Abraham Lorber, MD, Eliezer Shalev, MD Objective. To examine the feasibility of
Basic EKG Interpretation. Nirja Parikh, PT, DPT
 Basic EKG Interpretation Nirja Parikh, PT, DPT Electrocardiogram (EKG) Using surface electrodes record the electrical activity of the heart electrical activity (usually) correlates to mechanical function
Basic EKG Interpretation Nirja Parikh, PT, DPT Electrocardiogram (EKG) Using surface electrodes record the electrical activity of the heart electrical activity (usually) correlates to mechanical function
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
Junctional Premature Contraction (JPC)
") Where s the PAC? Junctional Premature Contraction (JPC) A junctional premature contraction (JPC) is a beat that originates prematurely in the AV node. It can occur sporadically or in a grouped pattern.
Where s the PAC? Junctional Premature Contraction (JPC) A junctional premature contraction (JPC) is a beat that originates prematurely in the AV node. It can occur sporadically or in a grouped pattern.
ACLS Study Guide for Precourse Self-Assessment
 20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
How do arrhythmias occur?
 How do arrhythmias occur? An arrhythmia is an abnormal heart rhythm (= dysrhythmia). Can be fast (tachy) or slow (brady). Brady arrhythmias are usually due to conduc;on block, while tachyarrhythmias are
How do arrhythmias occur? An arrhythmia is an abnormal heart rhythm (= dysrhythmia). Can be fast (tachy) or slow (brady). Brady arrhythmias are usually due to conduc;on block, while tachyarrhythmias are
Pediatrics ECG Monitoring. Pediatric Intensive Care Unit Emergency Division
 Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Ventricular tachycardia Ventricular fibrillation and ICD
 EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
Complete congenital heart block in a neonate with a complex congenital heart defect in Africa
 Case Report Complete congenital heart block in a neonate with a complex congenital heart defect in Africa Clovis Nkoke 1, Edvine Yonta Wawo 2, Liliane Kuate Mfeukeu 3, Larissa Makamte 2, Sandrine Dikosso
Case Report Complete congenital heart block in a neonate with a complex congenital heart defect in Africa Clovis Nkoke 1, Edvine Yonta Wawo 2, Liliane Kuate Mfeukeu 3, Larissa Makamte 2, Sandrine Dikosso
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery s present: Early Repair Era
 Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery 1954 1960: Experimental Era 1960 s 1980 s: Palliation Era 1980 s present: Early Repair Era 2010 2030 s: Fetal Interventions Hybrid
Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery 1954 1960: Experimental Era 1960 s 1980 s: Palliation Era 1980 s present: Early Repair Era 2010 2030 s: Fetal Interventions Hybrid
Ablation Update and Case Studies. Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group
 Ablation Update and Case Studies Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group Disclosures No financial relationships to disclose Objectives At the conclusion of this activity,
Ablation Update and Case Studies Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group Disclosures No financial relationships to disclose Objectives At the conclusion of this activity,
ISUOG Basic Training. Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA. Basic training. Editable text here
 ISUOG Basic Training Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA Learning Objectives 6, 7 & 8 At the end of the lecture you will be able to: describe how to assess cardiac situs
ISUOG Basic Training Obtaining & Interpreting Heart Views Correctly Alfred Abuhamad, USA Learning Objectives 6, 7 & 8 At the end of the lecture you will be able to: describe how to assess cardiac situs
Arrhythmias. Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center
 Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons