Case Report Anomalous Origin of the Left Common Carotid Artery from the Main Pulmonary Artery: A Rare Association in an Infant with CHARGE Syndrome
|
|
|
- Amanda Greene
- 6 years ago
- Views:
Transcription
1 Case Reports in Pediatrics Volume 2016, Article ID , 4 pages Case Report Anomalous Origin of the Left Common Carotid Artery from the Main Pulmonary Artery: A Rare Association in an Infant with CHARGE Syndrome Onyekachukwu Osakwe, 1 Blaise Jones, 2 and Russel Hirsch 1 1 The Heart Institute, Cincinnati Children s Hospital Medical Center, 3333 Burnet Avenue, Cincinnati, OH 45229, USA 2 Department of Radiology, Cincinnati Children s Hospital Medical Center, 3333 Burnet Avenue, Cincinnati, OH 45229, USA Correspondence should be addressed to Onyekachukwu Osakwe; onyekachukwu.osakwe@cchmc.org Received 27 July 2016; Accepted 8 November 2016 Academic Editor: Larry A. Rhodes Copyright 2016 Onyekachukwu Osakwe et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Case Report. Isolated carotid artery originating from the pulmonary trunk is an exceedingly rare anomalous origin of head and neck vessels. We present this finding, along with a persistent embryonic trigeminal artery, in a male infant with multiple cardiac defects and other congenital anomalies associated with CHARGE syndrome. After extensive investigations, cardiac catheterization revealed the anomalous left common carotid artery arising from the cranial aspect of the main pulmonary artery. There was retrograde flow in this vessel, resulting from the lower pulmonary pressure, essentially stealing arterial supply from the left anterior cerebral circulation. The persistent left-sided trigeminal artery provided collateral flow from the posterior circulation to the left internal carotid artery territory, allowing for safe ligation of the anomalous origin of the left common carotid artery, thereby reversing the steal of arterial blood flow into the pulmonary circulation and resulting in a net improvement of cerebral perfusion. Conclusion. The possibility of this vascular anomaly should be considered in all infants with CHARGE syndrome. Surgical repair or ligation should be tailored to the specific patient circumstances, following a careful delineation of all sources of cerebral perfusion. 1. Introduction Anomalous origin of head and neck vessels has been previously described, but specific origin of an isolated carotid artery from the pulmonary artery trunk is rare. We present this finding in an infant with CHARGE syndrome, who was also found to have persistence of the embryonic trigeminal artery, a finding that conferred some protection to the cerebral circulation. 2. Case Report A male full term infant with multiple congenital anomalies was transferred shortly after birth to our hospital for further evaluation. At the time of transfer, he was known to have Ebstein s anomaly of the tricuspid valve, a moderately restrictive ventricular septal defect, small patent ductus arteriosus, and multiple other congenital anomalies, including bilateral choanal stenosis, cystic hygroma, microphallus, undescended testes, webbed neck, and dysmorphic facial features. Genetic evaluation confirmed a diagnosis of CHARGE syndrome. His clinical exam on admission revealed a small, dysmorphic infant with a weight of 2.06 kg, heart rate of 160 beats per minute with equal peripheral pulses, blood pressure of 70/42 mmhg, respiratory rate of 50, and oxygen saturation of 100% on room air with a CPAP of 6. He was warm, well perfused, and comfortable with noninvasive respiratory support. He had a normal first heart sound with a physiologically split second heart sound, and a grade III/VI, high pitched holosystolic murmur best heard at the left upper sternal border. His abdomen was mildly distended, but his liver was not enlarged. His immediate evaluation included a chest X-ray that was consistent with a left-to-right shunt, with increased pulmonary vascular markings and mild cardiomegaly, but no focal infiltrates; an echocardiogram that revealed mild Ebstein s anomaly, mildly dilated right atrium, moderate perimembranous ventricular septal defect, bicuspid aortic valve,
 coursing from the cavernous left internal carotid artery posteriorly and medially to anastomose with the midbasilar")


, which is pathogenic for CHARGE syndrome.")
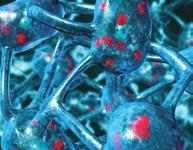
2 2 Case Reports in Pediatrics Figure 2: Camera in the AP plane. A contrast injection reveals anomalous origin of the left common carotid artery from the roof of the main pulmonary artery. Figure 1: Axial T2-weighted MR image shows a persistent trigeminal artery (arrow) coursing from the cavernous left internal carotid artery posteriorly and medially to anastomose with the midbasilar artery. fenestrated atrial septum, a small PDA, a right sided aortic arch, and a poorly defined aberrant left subclavian artery; and baseline blood work with a hemoglobin of 10.3 g/dl. During the first 2 days after admission, he was able to be weaned from CPAP to blow-by supplemental oxygen, but his tachypnea persisted. Despite diuretic therapy, he would periodically require increased respiratory support on high flow nasal cannula for desaturation episodes. MR imaging of the brain and internal auditory canals was performed to evaluate for potential cochlear implantation in the future. It demonstrated a persistent trigeminal artery (TGA), an anomalous intracranial artery connecting the left internal carotid artery to the midbasilar artery (Figure 1). Genetic evaluation showed a heterozygous mutation in CHD7 (c.2514 T > A), which is pathogenic for CHARGE syndrome. There was no evidence of deletions of chromosome 22q11 on fluorescence in situ hybridization. An invasive airway evaluation revealed tracheomalacia and bronchomalacia but no evidence of extrinsic compression. Over the course of eight weeks, with no indication of any improvement or change in his clinical status but with improved nutrition, it was decided to proceed with cardiac catheterization to better define the extent of his intracardiac shunt and help with decisions regarding reparative surgery. That procedure was performed from the femoral approach, with the patient under general anesthesia, and on room air. Saturation data indicated a pulmonary-to-systemic shunt ratio of 4.4 : 1 with a saturation step up from 43% in the superior vena cava to 77% in the left and right pulmonary arteries. Using measured oxygen consumption, the pulmonary and systemic blood flow were 6.74 and 1.53 L/min/m 2, respectively. The left and right pulmonary artery saturations were identical. The right ventricular systolic pressure was 63% of the left ventricular systolic pressure, with the mean pulmonary artery pressure of 24 mmhg. The pulmonary vascular resistance was calculated as normal with a value of 2.74 Wu m 2. Whileattemptingtoadvancethediagnosticwedgecatheter (Cook Corporation, Bloomington In.) from the main pulmonary artery into one of the branches, it appeared that itwaslodgedintheroofofthatvessel.asoftwire(0.018 HI-Torque Floppy, Abbott Vascular, Santa Clara, CA) was then passed through that catheter to attempt to gain access in one or other branches but instead passed easily in a cranial direction on the left side of the neck. The wedge catheter was then gently advanced over the wire, and a contrast hand injection was performed, revealing the anomalous left common carotid artery (LCCA) arising from the cranial aspectofthemainpulmonaryartery(figure2).absence of an aortic origin of the carotid was confirmed with a supravalvar aortic angiogram (Figure 3(a)), demonstrating a right aortic arch with aberrant origin of the left subclavian artery,andtherightcommoncarotidarteryarisingasthe first branch from the ascending aorta. Both vertebral arteries arose normally from the left and right subclavian arteries. In the late arterial phase of the injection, retrograde opacification of the LCCA was observed, draining into the branch pulmonary arteries (Figure 3(b)), reflecting preferential flow from the higher pressure cerebral arterial bed to the lower pressure pulmonary bed. The catheterization was completed without complication, and the infant was returned to the Neonatal Intensive Care Unit. One week later, the infant underwent uncomplicated surgical repair of the ventricular septal defect and atrial septal defect closure. Owing to the distance between the location of the anomalous carotid artery andtherightaorticarchandconcernfortensionontheairway,thesurgeonelectedtoligateandreleasetheanomalous vessel at the origin from the pulmonary artery. The infant has made an uneventful recovery from the procedure and made some progress weaning from ventilatory support but continued to require intensive care support.
 is performed in the transverse aorta, revealing a right aortic arch with aberrant origin of the left subclavian artery and absence of the left common carotid artery.")
3 Case Reports in Pediatrics 3 (a) (b) Figure 3: (a) Camera in the AP plane. An angiogram (early phase) is performed in the transverse aorta, revealing a right aortic arch with aberrant origin of the left subclavian artery and absence of the left common carotid artery. (b) Camera in the AP plane. An angiogram (late arterial phase) reveals retrograde opacification of the left common carotid artery (arrow) draining into the left pulmonary artery. 3. Discussion Anomalous origin of the carotid artery from the pulmonary artery trunk has been previously described but is exceedingly rare. Our literature review revealed a total of eight cases [1 8], of which two were in infants with conotruncal abnormalities [3, 5] and one in association with CHARGE syndrome [1]. One other infant was found to have other significant intracerebral arterial vascular anomalies in addition to the primary lesion [8]. The embryologic causation of aberrant arch vessels is multifactorial, with events that lead to either abnormal primitive arch regression or persistence of structures which should regress [1 7]. Persistence of structures may result in compression of adjacent structures (such as with vascular rings), while abnormal regression could impair blood flow and result in vessel hypoplasia or atresia. In the case of an aberrant carotid artery from the pulmonary trunk, a possible cause may be abnormal persistence of the left dorsal aorta between the third and sixth branchial arches, which becomes connected to the left pulmonary artery by the ductus arteriosus. The left third arch also regresses abnormally, which disconnects the left internal carotid artery from the other arch vessels [2, 4]. More recently, it has been proposed that this malformation may arise from poor septal formation of the aortic sac due to abnormal migration of cells from the neural crest at the cardiac level [7]. Trigeminal arteries are the most common of four described fetal arterial connections between the anterior and posterior cerebral circulations [9]. These anomalous connectionsnormallyinvoluteatthe7to14mmembryonicstage, with the only remaining arterial connections being the posterior communicating arteries [9]. The reported incidence of persistent TGA is % [9]. There is some decreased caliber of the basilar artery distal to the junction with the TGAinupto75%ofcases[10],butthisfeaturewasnot evident in the presented case. Anomalous origin of the LCCA has significant association with deletions of chromosome 22q11 (DiGeorge syndrome) [2, 5], but our patient was confirmed to have no evidence of deletion of chromosome 22q11. This case represents one in which an anomalous LCCA origin has been described with CHARGE syndrome. CHARGE syndrome has an incidence of 1 in 10,000 live births, and it presents variably with colobomas, heart defects, choanal atresia, growth and developmental retardation, and genital and ear abnormalities [11]. While often significant, the cardiac anomalies may not be the most important of the associated anomalies. However, when present, early repair may improve the physiology and allow the other comorbidities to be addressed on their merits. Often,asinourcase,theimpactorsymptomsfromthe congenital heart lesion/s cannot be separated out from those caused by some of the other associated anomalies, and further evaluation is required. In this case, cardiac catheterization to determine the exact nature of the left-to-right shunt and calculate the pulmonary vascular resistance served as the vehicle to coincidentally diagnose the anomalous origin of thelcca.becauseofthelowerpressureofthepulmonary circulation, there was retrograde flow in this vessel, effecting a steal of arterial supply from the left anterior circulation. Surgical strategy to repair this defect is dependent on the extent of surgery required for reimplantation, the impact on adjacent structures after repair, and the physiologic impact of possible ligation if repair was deemed unlikely. The right aortic arch and aberrant left subclavian artery in this case resulted in the high likelihood of an extensive surgery to affect a repair, with significant tension and probable late stenosis. However, prior to proceeding with ligation during the planned congenital heart surgery, the integrity of the Circle of Willis and the presence of any other intracerebral vascular anomalies were deemed necessary, given those findings in one other case report. The left-sided TGA in this case provided robust collateral flow from the posterior
4 4 Case Reports in Pediatrics circulation (basilar artery) to the left internal carotid artery territory, allowing for safe ligation of the anomalous origin of the LCCA. Not only did this ligation reduce the extent of required operative arterial manipulation but also it reversed the steal of arterial blood flow into the pulmonary circulation, resulting in a net improvement of cerebral perfusion. 4. Conclusion Isolated origin of the carotid artery from the pulmonary trunk is a rare anomalous origin of head and neck vessels that may be more common in syndromic patients. Surgical repair or ligation should be tailored to the specific patient circumstances, although preceding evaluation in each case should include a careful delineation of all sources of cerebral perfusion. In addition to previously described cases in patients with conotruncal abnormalities, the possibility of this vascular anomaly should be considered in all infants with CHARGE syndrome. [10] S. J. Dimmick and K. C. Faulder, Normal variants of the cerebral circulation at multidetector CT angiography, Radiographics,vol.29,no.4,pp ,2009. [11] R. A. Pagon, J. M. Graham Jr., J. Zonana, and S.-L. Yong, Coloboma, congenital heart disease, and choanal atresia with multiple anomalies: CHARGE association, The Pediatrics,vol. 99,no.2,pp ,1981. Competing Interests The authors declare that there are no competing interests regarding the publication of this paper. References [1] K. Ghalili, H. J. Issenberg, N. J. Freeman, and R. F. Brodman, Isolated left carotid artery in CHARGE association: diagnosis and repair, The Annals of Thoracic Surgery, vol. 50, no. 1, pp , [2] S.F.HuangandM.H.Wu, Leftcommoncarotidarteryarising from the pulmonary artery in a patient with DiGeorge syndrome, Heart,vol.76, no.1,pp.82 83, [3] R. Tozzi, M. Hernanz-Schulman, R. Kiley et al., Congenital pulmonary steal associated with Tetralogy of Fallot, right aortic archandanisolatedleftcarotidartery, Pediatric Radiology,vol. 19,no.6-7,pp ,1989. [4] L. V. Fong and A. W. Venables, Isolation of the left common carotid or left innominate artery, British Heart Journal,vol.57, no. 6, pp , [5] G.Oppido,C.P.Napoleone,D.Gabbierietal., Imagesincardiovascular medicine. Left common carotid artery isolation in a newborn with tetralogy of Fallot and DiGeorge syndrome, Circulation, vol. 111, no. 1, pp. e4 e5, [6] V. Fouilloux, C. Gran, and B. Kreitmann, Isolated left common carotid artery connected to the pulmonary artery: where was the arterial duct? World Journal for Pediatric and Congenital Hearth Surgery, vol. 4, no. 2, pp , [7] N.Kaushik,Z.Saba,H.Rosenfeldetal., Anisolatedleftcommon carotid artery from the main pulmonary artery: possible malseptation of the truncoaortic sac, Pediatric Cardiology, vol. 26, no. 5, pp , [8]M.C.Hurley,P.H.Nguyen,A.J.DiPatri,andA.Shaibani, Isolatedoriginoftheleftinternalcarotidarteryfromthepulmonary artery: case report, JournalofNeurosurgery:Pediatrics, vol. 2, no. 3, pp , [9] S. Meckel, B. Spittau, and W. McAuliffe, The persistent trigeminal artery: development, imaging anatomy, variants, and associated vascular pathologies, Neuroradiology, vol.55,no.1,pp. 5 16, 2013.
















5 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Devendra V. Kulkarni, Rahul G. Hegde, Ankit Balani, and Anagha R. Joshi. 2. Case Report. 1. Introduction
 Case Reports in Radiology, Article ID 614647, 4 pages http://dx.doi.org/10.1155/2014/614647 Case Report A Rare Case of Pulmonary Atresia with Ventricular Septal Defect with a Right Sided Aortic Arch and
Case Reports in Radiology, Article ID 614647, 4 pages http://dx.doi.org/10.1155/2014/614647 Case Report A Rare Case of Pulmonary Atresia with Ventricular Septal Defect with a Right Sided Aortic Arch and
Isolated major aortopulmonary collateral as the sole pulmonary blood supply to an entire lung segment
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2017 Isolated major aortopulmonary collateral as the sole pulmonary blood supply to an entire lung segment Hannah
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2017 Isolated major aortopulmonary collateral as the sole pulmonary blood supply to an entire lung segment Hannah
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Case Report Preoperative Assessment of Anomalous Right Coronary Artery Arising from the Main Pulmonary Artery
 Case Reports in Medicine Volume 2011, Article ID 642126, 4 pages doi:10.1155/2011/642126 Case Report Preoperative Assessment of Anomalous Right Coronary Artery Arising from the Main Pulmonary Artery Marshall
Case Reports in Medicine Volume 2011, Article ID 642126, 4 pages doi:10.1155/2011/642126 Case Report Preoperative Assessment of Anomalous Right Coronary Artery Arising from the Main Pulmonary Artery Marshall
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Case Report Sinus Venosus Atrial Septal Defect as a Cause of Palpitations and Dyspnea in an Adult: A Diagnostic Imaging Challenge
 Case Reports in Medicine Volume 2015, Article ID 128462, 4 pages http://dx.doi.org/10.1155/2015/128462 Case Report Sinus Venosus Atrial Septal Defect as a Cause of Palpitations and Dyspnea in an Adult:
Case Reports in Medicine Volume 2015, Article ID 128462, 4 pages http://dx.doi.org/10.1155/2015/128462 Case Report Sinus Venosus Atrial Septal Defect as a Cause of Palpitations and Dyspnea in an Adult:
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Case Report Computed Tomography Angiography Successfully Used to Diagnose Postoperative Systemic-Pulmonary Artery Shunt Narrowing
 Case Reports in Cardiology Volume 2011, Article ID 802643, 4 pages doi:10.1155/2011/802643 Case Report Computed Tomography Angiography Successfully Used to Diagnose Postoperative Systemic-Pulmonary Artery
Case Reports in Cardiology Volume 2011, Article ID 802643, 4 pages doi:10.1155/2011/802643 Case Report Computed Tomography Angiography Successfully Used to Diagnose Postoperative Systemic-Pulmonary Artery
DR Turner, JA Vincent, and ML Epstein. Isolated right pulmonary artery discontinuity. Images Paediatr Cardiol Jul-Sep; 2(3):
:") IMAGES in PAEDIATRIC CARDIOLOGY Images PMCID: PMC3232486 Isolated right pulmonary artery discontinuity DR Turner, MD, * JA Vincent, ** and ML Epstein *** * Senior Fellow, Division of Cardiology, Children's
IMAGES in PAEDIATRIC CARDIOLOGY Images PMCID: PMC3232486 Isolated right pulmonary artery discontinuity DR Turner, MD, * JA Vincent, ** and ML Epstein *** * Senior Fellow, Division of Cardiology, Children's
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
 Case Reports in Cardiology Volume 2016, Article ID 4979182, 4 pages http://dx.doi.org/10.1155/2016/4979182 Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
Case Reports in Cardiology Volume 2016, Article ID 4979182, 4 pages http://dx.doi.org/10.1155/2016/4979182 Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray
 Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Isolated origin of the left internal carotid artery from the pulmonary artery
 J Neurosurg Pediatrics 2:207 211, 2008 Isolated origin of the left internal carotid artery from the pulmonary artery Case report MICHAEL C. HURLEY, M.D., 1,2 PAMELA H. NGUYEN, M.D., 1 ARTHUR J. DIPATRI,
J Neurosurg Pediatrics 2:207 211, 2008 Isolated origin of the left internal carotid artery from the pulmonary artery Case report MICHAEL C. HURLEY, M.D., 1,2 PAMELA H. NGUYEN, M.D., 1 ARTHUR J. DIPATRI,
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Case Report Tortuous Common Carotid Artery: A Report of Four Cases Observed in Cadaveric Dissections
 Case Reports in Otolaryngology Volume 2016, Article ID 2028402, 4 pages http://dx.doi.org/10.1155/2016/2028402 Case Report Tortuous Common Carotid Artery: A Report of Four Cases Observed in Cadaveric Dissections
Case Reports in Otolaryngology Volume 2016, Article ID 2028402, 4 pages http://dx.doi.org/10.1155/2016/2028402 Case Report Tortuous Common Carotid Artery: A Report of Four Cases Observed in Cadaveric Dissections
MEDICAL MANAGEMENT WITH CAVEATS 1. In one study of 50 CHARGE patients with CHD, 75% required surgery. 2. Children with CHARGE may be resistant to chlo
 CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
Large veins of the thorax Brachiocephalic veins
 Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Department of Internal Medicine, Saitama Citizens Medical Center, Saitama , Japan
 Case Reports in Cardiology Volume 2016, Article ID 8790347, 5 pages http://dx.doi.org/10.1155/2016/8790347 Case Report GuideLiner Catheter Use for Percutaneous Intervention Involving Anomalous Origin of
Case Reports in Cardiology Volume 2016, Article ID 8790347, 5 pages http://dx.doi.org/10.1155/2016/8790347 Case Report GuideLiner Catheter Use for Percutaneous Intervention Involving Anomalous Origin of
Surgical implications of right aortic arch with isolation of left subclavian artery'
 British Heart journal, I975, 37, 93I-936. Surgical implications of right aortic arch with isolation of left subclavian artery' L. Rodriguez,2 T. Izukawa, C. A. F. MoEs, G. A. Trusler, and W. G. Williams
British Heart journal, I975, 37, 93I-936. Surgical implications of right aortic arch with isolation of left subclavian artery' L. Rodriguez,2 T. Izukawa, C. A. F. MoEs, G. A. Trusler, and W. G. Williams
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
CongHeartDis.doc. Андрій Миколайович Лобода
 CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
Assessing Cardiac Anatomy With Digital Subtraction Angiography
 485 JACC Vol. 5, No. I Assessing Cardiac Anatomy With Digital Subtraction Angiography DOUGLAS S., MD, FACC Cleveland, Ohio The use of intravenous digital subtraction angiography in the assessment of patients
485 JACC Vol. 5, No. I Assessing Cardiac Anatomy With Digital Subtraction Angiography DOUGLAS S., MD, FACC Cleveland, Ohio The use of intravenous digital subtraction angiography in the assessment of patients
AORTIC COARCTATION. Synonyms: - Coarctation of the aorta
 AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
PULMONARY VENOLOBAR SYNDROME. Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital.
 PULMONARY VENOLOBAR SYNDROME Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital. Presenting complaint: 10 yrs old girl with recurrent episodes of lower respiratory tract infection from infancy.
PULMONARY VENOLOBAR SYNDROME Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital. Presenting complaint: 10 yrs old girl with recurrent episodes of lower respiratory tract infection from infancy.
J Somerville and V Grech. The chest x-ray in congenital heart disease 2. Images Paediatr Cardiol Jan-Mar; 12(1): 1 8.
: 1 8.") IMAGES in PAEDIATRIC CARDIOLOGY Images Paediatr Cardiol. 2010 PMCID: PMC3228330 The chest x-ray in congenital heart disease 2 J Somerville and V Grech Paediatric Department, Mater Dei Hospital, Malta Corresponding
IMAGES in PAEDIATRIC CARDIOLOGY Images Paediatr Cardiol. 2010 PMCID: PMC3228330 The chest x-ray in congenital heart disease 2 J Somerville and V Grech Paediatric Department, Mater Dei Hospital, Malta Corresponding
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Low-dose prospective ECG-triggering dual-source CT angiography in infants and children with complex congenital heart disease: first experience
 Low-dose prospective ECG-triggering dual-source CT angiography in infants and children with complex congenital heart disease: first experience Ximing Wang, M.D., Zhaoping Cheng, M.D., Dawei Wu, M.D., Lebin
Low-dose prospective ECG-triggering dual-source CT angiography in infants and children with complex congenital heart disease: first experience Ximing Wang, M.D., Zhaoping Cheng, M.D., Dawei Wu, M.D., Lebin
ULTRASOUND OF THE FETAL HEART
 ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
ULTRASOUND OF THE FETAL HEART Cameron A. Manbeian, MD Disclosure Statement Today s faculty: Cameron Manbeian, MD does not have any relevant financial relationships with commercial interests or affiliations
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
Case Report Anomalous Left Main Coronary Artery: Case Series of Different Courses and Literature Review
 Case Reports in Vascular Medicine Volume 2013, Article ID 380952, 5 pages http://dx.doi.org/10.1155/2013/380952 Case Report Anomalous Left Main Coronary Artery: Case Series of Different Courses and Literature
Case Reports in Vascular Medicine Volume 2013, Article ID 380952, 5 pages http://dx.doi.org/10.1155/2013/380952 Case Report Anomalous Left Main Coronary Artery: Case Series of Different Courses and Literature
The Chest X-ray for Cardiologists
 Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
The sinus venosus represent the venous end of the heart It receives 3 veins: 1- Common cardinal vein body wall 2- Umbilical vein from placenta 3-
 1 2 The sinus venosus represent the venous end of the heart It receives 3 veins: 1- Common cardinal vein body wall 2- Umbilical vein from placenta 3- Vitelline vein from yolk sac 3 However!!!!! The left
1 2 The sinus venosus represent the venous end of the heart It receives 3 veins: 1- Common cardinal vein body wall 2- Umbilical vein from placenta 3- Vitelline vein from yolk sac 3 However!!!!! The left
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Aortography in Fallot's Tetralogy and Variants
 Brit. Heart J., 1969, 31, 146. Aortography in Fallot's Tetralogy and Variants SIMON REES AND JANE SOMERVILLE From The Institute of Cardiology and National Heart Hospital, London W.J In patients with Fallot's
Brit. Heart J., 1969, 31, 146. Aortography in Fallot's Tetralogy and Variants SIMON REES AND JANE SOMERVILLE From The Institute of Cardiology and National Heart Hospital, London W.J In patients with Fallot's
A. Incorrect! Think of a therapy that reduces prostaglandin synthesis. B. Incorrect! Think of a therapy that reduces prostaglandin synthesis.
 USMLE Step 1 - Problem Drill 02: Embryology Question No. 1 of 10 1. A premature infant is born with a patent ductus arteriosis. Which of the following treatments may be used as part of the treatment regimen?
USMLE Step 1 - Problem Drill 02: Embryology Question No. 1 of 10 1. A premature infant is born with a patent ductus arteriosis. Which of the following treatments may be used as part of the treatment regimen?
24. An infant with recurrent pneumonia underwent a frontal chest radiograph (Fig 24-A) followed by
 followed by") 24. An infant with recurrent pneumonia underwent a frontal chest radiograph (Fig 24-A) followed by diagnosis? ndings, what is the most likely A. Pulmonary sequestration B. Congenital pulmonary airway malformation
24. An infant with recurrent pneumonia underwent a frontal chest radiograph (Fig 24-A) followed by diagnosis? ndings, what is the most likely A. Pulmonary sequestration B. Congenital pulmonary airway malformation
Patent ductus arteriosus PDA
 Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Two Cases Report of Scimitar Syndrome: The Classical one with Subaortic Membrane and the Scimitar Variant
 Bahrain Medical Bulletin, Vol.22, No.1, March 2000 Two Cases Report of Scimitar Syndrome: The Classical one with Subaortic Membrane and the Scimitar Variant F Hakim, MD* A Madani, MD* A Abu Haweleh, MD,MRCP*
Bahrain Medical Bulletin, Vol.22, No.1, March 2000 Two Cases Report of Scimitar Syndrome: The Classical one with Subaortic Membrane and the Scimitar Variant F Hakim, MD* A Madani, MD* A Abu Haweleh, MD,MRCP*
DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5
 DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5 REVIEW OF CARDIAC ANATOMY Heart 4 chambers Base and apex Valves Pericardial sac 3 layers: epi, myo, endo cardium Major blood vessels Aorta and its
DEVELOPMENT OF THE CIRCULATORY SYSTEM L E C T U R E 5 REVIEW OF CARDIAC ANATOMY Heart 4 chambers Base and apex Valves Pericardial sac 3 layers: epi, myo, endo cardium Major blood vessels Aorta and its
The Cardiovascular System (Part II)
") The Cardiovascular System (Part II) 黃敏銓 mchuang@ntu.edu.tw 解剖學暨細胞生物學研究所 1 Development of veins Three paired veins drain into the tubular heart of a 4-week embryo Vitelline veins: poorly oxygenated blood
The Cardiovascular System (Part II) 黃敏銓 mchuang@ntu.edu.tw 解剖學暨細胞生物學研究所 1 Development of veins Three paired veins drain into the tubular heart of a 4-week embryo Vitelline veins: poorly oxygenated blood
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE
 By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
Aorticopulmonary septal defect
 British HeartJournal, I974, 36, 630-635. Aorticopulmonary septal defect An experience with I7 patients Leonard C. Blieden' and James H. Moller From the Department of Pediatrics, University of Minnesota,
British HeartJournal, I974, 36, 630-635. Aorticopulmonary septal defect An experience with I7 patients Leonard C. Blieden' and James H. Moller From the Department of Pediatrics, University of Minnesota,
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Anomalous origin of the right subclavian artery from main pulmonary artery
 Anomalous origin of the right subclavian artery from main pulmonary artery Award: AOSR Best Exhibit Prize - Bronze Poster No.: R-0178 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: U. Chaumrattanakul,
Anomalous origin of the right subclavian artery from main pulmonary artery Award: AOSR Best Exhibit Prize - Bronze Poster No.: R-0178 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: U. Chaumrattanakul,
Hybrid Procedure of Bilateral Pulmonary Artery Banding and Bilateral Ductal Stenting in an Infant With Aortic Atresia and Interrupted Aortic Arch
 Catheterization and Cardiovascular Interventions 84:1157 1162 (2014) Hybrid Procedure of Bilateral Pulmonary Artery Banding and Bilateral Ductal Stenting in an Infant With Aortic Atresia and Interrupted
Catheterization and Cardiovascular Interventions 84:1157 1162 (2014) Hybrid Procedure of Bilateral Pulmonary Artery Banding and Bilateral Ductal Stenting in an Infant With Aortic Atresia and Interrupted
Surgical Management Of TAPVR. Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital
 Surgical Management Of TAPVR Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital No Disclosures Goals Review the embryology and anatomy Review Surgical Strategies for repair Discuss
Surgical Management Of TAPVR Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital No Disclosures Goals Review the embryology and anatomy Review Surgical Strategies for repair Discuss
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Systematic approach to Fetal Echocardiography. Objectives. Introduction 11/2/2015
 Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
Systematic approach to Fetal Echocardiography. Pediatric Echocardiography Conference, JCMCH November 7, 2015 Rajani Anand Objectives Fetal cardiology pre-test Introduction Embryology and Physiology of
CYANOTIC CONGENITAL HEART DISEASES. PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU
 CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions
 Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
(i) Family 1. The male proband (1.III-1) from European descent was referred at
 Family 1. The male proband (1.III-1) from European descent was referred at") 1 Supplementary Note Clinical descriptions of families (i) Family 1. The male proband (1.III-1) from European descent was referred at age 14 because of scoliosis. He had normal development. Physical evaluation
1 Supplementary Note Clinical descriptions of families (i) Family 1. The male proband (1.III-1) from European descent was referred at age 14 because of scoliosis. He had normal development. Physical evaluation
W.S. O The University of Hong Kong
 W.S. O The University of Hong Kong Objectives: Describe early angiogenesis. Describe the heart tube formation. Describe the partitioning into a 4- chambered heart. List the formation of heart valves and
W.S. O The University of Hong Kong Objectives: Describe early angiogenesis. Describe the heart tube formation. Describe the partitioning into a 4- chambered heart. List the formation of heart valves and
Heart Development and Congenital Heart Disease
 Heart Development and Congenital Heart Disease Sally Dunwoodie s.dunwoodie@victorchang.edu.au Developmental and Stem Cell Biology Division Victor Chang Cardiac Research Institute for the heart of Australia...
Heart Development and Congenital Heart Disease Sally Dunwoodie s.dunwoodie@victorchang.edu.au Developmental and Stem Cell Biology Division Victor Chang Cardiac Research Institute for the heart of Australia...
Coarctation of the aorta
 T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
Common Defects With Expected Adult Survival:
 Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
Case Report DOUGLAS H. KING, MD, JAMES C. HUHTA, MD, HOWARD P. GUTGESELL, MD, FACC, DAVID A. OTT, MD*
 lacc Vol. 4, No.2 August 198'
lacc Vol. 4, No.2 August 198'
List of Videos. Video 1.1
 Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
Critical Heart Disease in the Newborn. What you need to know
 Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
The Fetal Cardiology Program
 The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Partial Anomalous Pulmonary Venous Connection in Adults: Evaluation with MDCT
 Partial Anomalous Pulmonary Venous Connection in Adults: Evaluation with MDCT e-poster: 349 Congress: 2WCTI 2009 Type: Educational poster Topic: Pulmonary circulation Authors: MeSH: Bhatti W, Maldjian
Partial Anomalous Pulmonary Venous Connection in Adults: Evaluation with MDCT e-poster: 349 Congress: 2WCTI 2009 Type: Educational poster Topic: Pulmonary circulation Authors: MeSH: Bhatti W, Maldjian
The Uncommon Vascular Ring - Not that Uncommon
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report The Uncommon Vascular Ring - Not that Uncommon Roshan D Souza MD 1, Deepa Prasad MD 1, James Strainic MD 1, Anoop Mohamed Iqbal MD 2 and Ravi Ashwath MD
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report The Uncommon Vascular Ring - Not that Uncommon Roshan D Souza MD 1, Deepa Prasad MD 1, James Strainic MD 1, Anoop Mohamed Iqbal MD 2 and Ravi Ashwath MD
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
List by Terms Visceral anomalies
 1 List by Terms Visceral anomalies Dilated 10128 Dilated cerebral ventricle 11 7 2 0 20,00 10201 Dilated aorta 9 8 2 1 5,26 10207 Dilated aortic arch 9 8 3 0 5,00 10213 Dilated carotid 3 12 4 1-47,37 10218
1 List by Terms Visceral anomalies Dilated 10128 Dilated cerebral ventricle 11 7 2 0 20,00 10201 Dilated aorta 9 8 2 1 5,26 10207 Dilated aortic arch 9 8 3 0 5,00 10213 Dilated carotid 3 12 4 1-47,37 10218
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Notes: 1)Membranous part contribute in the formation of small portion in the septal cusp.
Membranous part contribute in the formation of small portion in the septal cusp.") Embryology 9 : Slide 16 : There is a sulcus between primitive ventricular and bulbis cordis that will disappear gradually and lead to the formation of one chamber which is called bulboventricular chamber.
Embryology 9 : Slide 16 : There is a sulcus between primitive ventricular and bulbis cordis that will disappear gradually and lead to the formation of one chamber which is called bulboventricular chamber.
Pediatric Board Review Congenital Heart Disease. Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University
 Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Portal vein catheterization and selective angiography in diagnosis of total anomalous pulmonary venous connexion
 British Heart journal, 974, 36, 155-59. Portal vein catheterization and selective angiography in diagnosis of total anomalous pulmonary venous connexion Michael Tynan, D. Behrendt, W. Urquhart, and G.
British Heart journal, 974, 36, 155-59. Portal vein catheterization and selective angiography in diagnosis of total anomalous pulmonary venous connexion Michael Tynan, D. Behrendt, W. Urquhart, and G.
The goal of the hybrid approach for hypoplastic left heart
 The Hybrid Approach to Hypoplastic Left Heart Syndrome Mark Galantowicz, MD The goal of the hybrid approach for hypoplastic left heart syndrome (HLHS) is to lessen the cumulative impact of staged interventions,
The Hybrid Approach to Hypoplastic Left Heart Syndrome Mark Galantowicz, MD The goal of the hybrid approach for hypoplastic left heart syndrome (HLHS) is to lessen the cumulative impact of staged interventions,
List by Region - Visceral Anomalies
 1 List by Region - Visceral Anomalies General Terms 10127 Situs inversus 80,00 10125 Aneurysm 68,42 10126Fluid-filled abdomen -35,00 Brain 10131 Hydrocephaly 10128 Dilated cerebral ventricle 20,00 10132
1 List by Region - Visceral Anomalies General Terms 10127 Situs inversus 80,00 10125 Aneurysm 68,42 10126Fluid-filled abdomen -35,00 Brain 10131 Hydrocephaly 10128 Dilated cerebral ventricle 20,00 10132
"Lecture Index. 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.
 Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.") "Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
"Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
Surgical Treatment of Congenital Heart Disease
 Surgical Treatment of Congenital Heart Disease The Evaluation of Diagnostic Data JAMES V. MALONEY, JR., M.D., and PIERCE J. FLYNN, M.D., Los Angeles THE TASK OF THE CARDIOLOGIST in diagnosing congenital
Surgical Treatment of Congenital Heart Disease The Evaluation of Diagnostic Data JAMES V. MALONEY, JR., M.D., and PIERCE J. FLYNN, M.D., Los Angeles THE TASK OF THE CARDIOLOGIST in diagnosing congenital
Circulatory system. Lecture #2
 Circulatory system Lecture #2 The essential components of the human cardiovascular system: Heart Blood Blood vessels Arteries - blood vessels that conduct arterial blood from heart ventricle to organs
Circulatory system Lecture #2 The essential components of the human cardiovascular system: Heart Blood Blood vessels Arteries - blood vessels that conduct arterial blood from heart ventricle to organs
Congenital Heart Disease: Cyanotic Lesions. Amitesh Aggarwal
 Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
MeSH: cyanosis, left superior vena cava abnormalities, vascular plug, percutanoeus closure
 IMAGES in PAEDIATRIC CARDIOLOGY Tomar M. Percutaneous device closure of Persistent Left Superior Vena Cava Connecting to the Left Atrium with intact coronary sinus: A Rare Entity. Images Paediatr Cardiol
IMAGES in PAEDIATRIC CARDIOLOGY Tomar M. Percutaneous device closure of Persistent Left Superior Vena Cava Connecting to the Left Atrium with intact coronary sinus: A Rare Entity. Images Paediatr Cardiol
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
63-year old female with dyspnea
 Indiana University Pulmonary and Critical Care Fellowship Fellows Case Archive Case #1 63-year old female with dyspnea Gabriel Bosslet, MD; Chadi Hage MD A 63-year-old female presented to pulmonary clinic
Indiana University Pulmonary and Critical Care Fellowship Fellows Case Archive Case #1 63-year old female with dyspnea Gabriel Bosslet, MD; Chadi Hage MD A 63-year-old female presented to pulmonary clinic
Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy
 Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
Slide 1. Slide 2. Slide 3 CONGENITAL HEART DISEASE. Papworth Hospital NHS Trust INTRODUCTION. Jakub Kadlec/Catherine Sudarshan INTRODUCTION
 Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Surgical Treatment of Aortic Arch Hypoplasia
 Surgical Treatment of Aortic Arch Hypoplasia In the early 1990s, 25% of patients could face mortality related to complica-tions of hypertensive disease Early operations and better surgical techniques should
Surgical Treatment of Aortic Arch Hypoplasia In the early 1990s, 25% of patients could face mortality related to complica-tions of hypertensive disease Early operations and better surgical techniques should
The Physiology of the Fetal Cardiovascular System
 The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
Case Report A Unique Case of Left Second Supernumerary and Left Third Bifid Intrathoracic Ribs with Block Vertebrae and Hypoplastic Left Lung
 Volume 2013, Article ID 620120, 4 pages http://dx.doi.org/10.1155/2013/620120 Case Report A Unique Case of Left Second Supernumerary and Left Third Bifid Intrathoracic Ribs with Block Vertebrae and Hypoplastic
Volume 2013, Article ID 620120, 4 pages http://dx.doi.org/10.1155/2013/620120 Case Report A Unique Case of Left Second Supernumerary and Left Third Bifid Intrathoracic Ribs with Block Vertebrae and Hypoplastic
Case Report Coexistent Congenital Diaphragmatic Hernia with Extrapulmonary Sequestration
 Canadian Respiratory Journal Volume 2016, Article ID 1460480, 4 pages http://dx.doi.org/10.1155/2016/1460480 Case Report Coexistent Congenital Diaphragmatic Hernia with Extrapulmonary Sequestration Nao
Canadian Respiratory Journal Volume 2016, Article ID 1460480, 4 pages http://dx.doi.org/10.1155/2016/1460480 Case Report Coexistent Congenital Diaphragmatic Hernia with Extrapulmonary Sequestration Nao