Kenneth D. Chi, MD Medical Director GI Lab Advocate Lutheran General Hospital
|
|
|
- Oswin Baldwin
- 6 years ago
- Views:
Transcription


1 Kenneth D. Chi, MD Medical Director GI Lab Advocate Lutheran General Hospital Advances in Digestive Health for the Primary Care Physician Symposium May 2, 2015
2 None
3 Case Presentation Types of Pancreatic mass lesions Solid lesions Cystic lesions Diagnostic algorithm Cyst management guidelines (Update April 2015) Summary
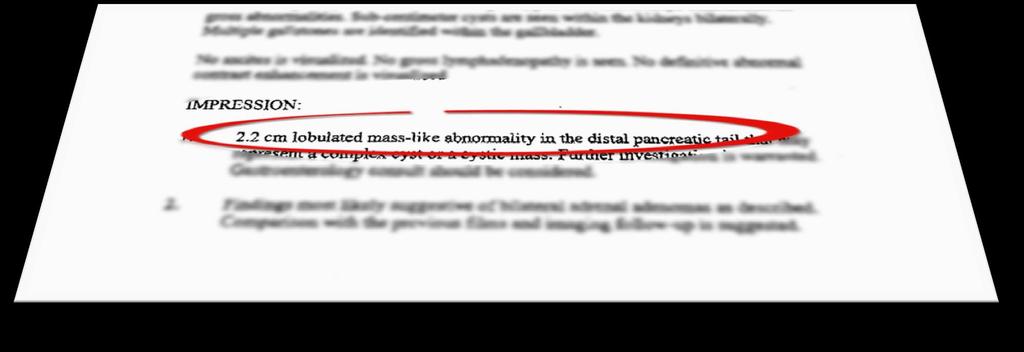
4 68 y.o. woman in otherwise good health, presents from her PCP office holding a MRI report (outside hospital) taken during workup of abdominal pain. She has circled the words 2.2cm mass-like abnormality in the tail of the pancreas in the report.

5
6 No weight loss, no appetite changes. No pain. No prior pancreatitis hx, no fam hx panc dz No prior abdominal wall trauma No loose stools or steatorrhea
7 What do you tell her and how do you proceed?

8 Cystadenomas (serous, mucinous) IPMN Cystic teratoma Choledochocele cyst Congenital cyst Intrapancreatic accessory spleen Eosinophillic pancreatitis Focal pancreatitis Inflammatory myofibroblastic tumor Lymphoid hyperplasia Phlegmon Pseudocyst Traumatic pancreatitis Wegner s disease Xanthogranulomatous pancreatitis Benign pancreatic cysts Hydatid cyst Dysontogenic cysts Lymphoepithelial cysts Pancreatic dermoid cysts Parasitic cysts (echinococcus) Retention pancreatic cysts Mucinous tumor with dysplasia IPMN with dysplasia Solid pseudopapillary tumor Ascaris lubricoides Candida albicans CMV Coxsackievirus Mumps Mycobacterium avium complex Mycobacterium tuberculosis Kaposi s sarcoma Lipoma Lymphangioma Pancreatic Castelman s Disease Pancreatic Hamartoma Pancreatic sarcoma Plexiform neurofibroma Schwannoma Teratoma Adenosquamous carcinoma Anaplastic tumors Clear cell sugar tumor Colloid carcinoma Granulocytic sarcoma Leukemia Lymphoma Primitive neuroectodermal tumor Ductal adenocarcinoma Osteoclast-like Giant Cell tumor Serous cystadenocarcinoma Mucinous cystadenocarcinoma Acinar cell carcinoma Pancreatoblastoma Solid-pseudopapillary carcinoma Ampullary adenocarcinoma Kaposi s sarcoma Lipoma Lymphangioma Pancreatic Castelman s Disease Pancreatic Hamartoma Pancreatic sarcoma Plexiform neurofibroma Schwannoma Teratoma Breast Colon Lung Lymphoma Melanoma Renal cell carcinoma Eosinophillic pancreatitis Focal pancreatitis Inflammatory myofibroblastic tumor Lymphoid hyperplasia Phlegmon Pseudocyst Traumatic pancreatitis Wegner s disease Xanthogranulomatous pancreatitis ACTH secreting tumor Carcinoid tumor Gastrinoma GRF-secreting tumor Insulinoma PP secreting tumor Somatostatinoma VIPoma Breast Colon Lung Lymphoma Melanoma Renal cell carcinoma Adenosquamous carcinoma Anaplastic tumors Clear cell sugar tumor Colloid carcinoma Granulocytic sarcoma Leukemia Lymphoma Primitive neuroectodermal tumor
9 Type Examples Benign (exocrine) Cystadenomas (serous, mucinous) IPMN Cystic teratoma Borderline Mucinous tumor with dysplasia IPMN with dysplasia Solid pseudopapillary tumor Malignant Ductal adenocarcinoma Osteoclast-like Giant Cell tumor Serous cystadenocarcinoma Mucinous cystadenocarcinoma Acinar cell carcinoma Pancreatoblastoma Solid-pseudopapillary carcinoma Ampullary adenocarcinoma
 Retention pancreatic")
10 Type Examples Endocrine ACTH secreting tumor Carcinoid tumor Gastrinoma GRF-secreting tumor Insulinoma PP secreting tumor Somatostatinoma VIPoma Cystic Lesions Benign pancreatic cysts Hydatid cyst Dysontogenic cysts Lymphoepithelial cysts Pancreatic dermoid cysts Parasitic cysts (echinococcus) Retention pancreatic cysts
11 Type Examples Congenital Choledochocele cyst Congenital cyst Intrapancreatic accessory spleen Infectious Masses Ascaris lubricoides Candida albicans CMV Coxsackievirus Mumps Mycobacterium avium complex Mycobacterium tuberculosis Mesenchymal Tumors Kaposi s sarcoma Lipoma Lymphangioma Pancreatic Castelman s Disease Pancreatic Hamartoma Pancreatic sarcoma Plexiform neurofibroma Schwannoma Teratoma
12 Type Examples Metastatic Lesions Breast Colon Lung Lymphoma Melanoma Renal cell carcinoma Non-islet cell tumors Adenosquamous carcinoma Anaplastic tumors Clear cell sugar tumor Colloid carcinoma Granulocytic sarcoma Leukemia Lymphoma Primitive neuroectodermal tumor
13 Type Examples Pancreatic inflammatory mass Eosinophillic pancreatitis Focal pancreatitis Inflammatory myofibroblastic tumor Lymphoid hyperplasia Phlegmon Pseudocyst Traumatic pancreatitis Wegner s disease Xanthogranulomatous pancreatitis
14 Pancreatic Incidentaloma First described by Ho and Kostiuk 1996 Significant imaging advances in CT, MRI, U/S have led to better diagnosis/staging But also increased the incidental discovery of asymptomatic pancreatic lesions About 15% patients undergoing MRI for other indications harbor unsuspected cysts These findings can trigger significant anxiety for patients and their physicians
15 Aim is to determine the benign or malignant nature of the lesion Obsessive search for small incidental tumors has, on the other hand, risk that these patients may undergo extensive diagnostic evaluation and tx without positive impact on their health, + potential complications
 Winter JM, et al. Ann Surg.")
16 The rate of malignancy in Pancreatic Incidentalomas has been reported to be as high as 32%, which is higher than other organ incidentalomas (kidney, adrenal, liver) Winter JM, et al. Ann Surg. 2006; 243:


17 History Each patient with a PI should be asked Prior hx pancreatitis? Any prior abdominal wall trauma? Family hx pancreatic cancer? Presence of any warning signs/symptoms? Any prior imaging studies to compare? This information could change workup from an aggressive approach to a more conservative


18 Age and comorbidities Lesion found in healthy 44 y.o. might be approached more aggressively than same lesion found in an 84 y.o. with multiple medical issues Location of lesion in the pancreas



19 Pancreatic lesions require careful evaluation and should be evaluated in a multidisciplinary fashion
20
21
22
23
24
25 - Physician - Assistants - Nurse Practitioners - Nurses - Psychologists - Social Workers - Nutritionists - Endocrinologists - Palliative Care

26 Pancreatic Protocol CT scan / MRI Endoscopic Ultrasound (EUS) and FNA has revolutionized the diagnosis and treatment of pancreatic lesions
27 Able to diagnose and confirm: Solid vs. Cystic Most solid lesions end up being resected Cystic lesions pose more of a diagnostic dilemma Accurate size and location of lesion Relationship with vessels Fine needle aspiration (FNA) and biopsy Cytology Core biopsy Drainage (pseudocysts)

28 EUS

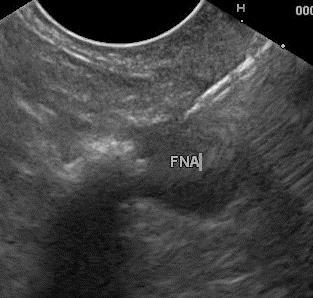
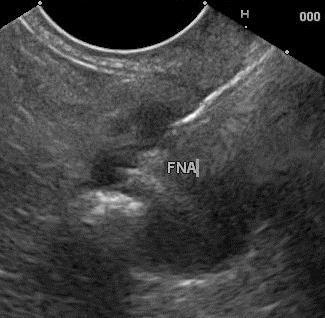
29 EUS Cyst FNA
30 Cyst fluid analysis CEA level = 76 ng/ml Level < 192 favors benign serous cyst Level > 192 favors pre-cancerous mucinous type Cytology returned benign What is the differential diagnosis of this cystic lesion?
31


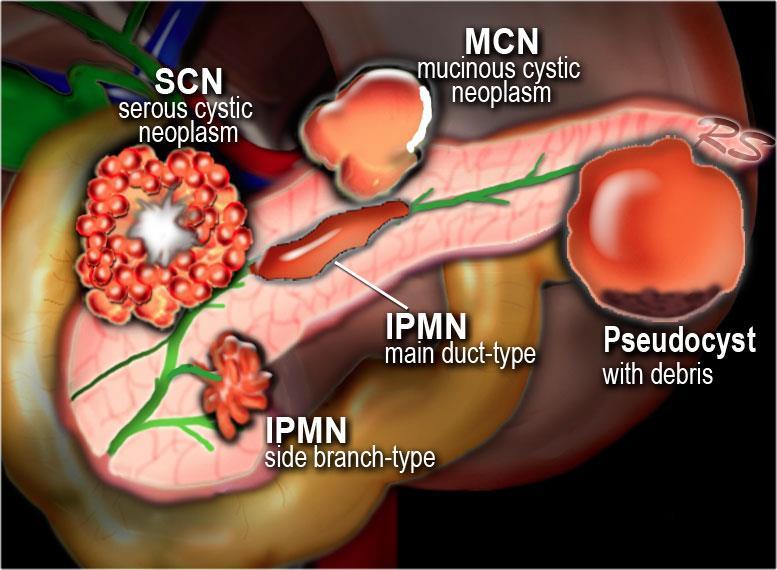
32 Benign Lined by glycogen-rich cells that originate from pancreatic centroacinar cells Usually microcystic (cluster of small cystic spaces honeycomb ) Mostly in woman >60 yrs old Malignant degeneration is exceedingly rare central scar on gross specimen

* * Reddy, RP et al.")
33 Exclusively found in woman (80-90%) Age usually >40 yrs Secrete mucin similar to IPMNs Unlike IPMNs, are lined with ovarian-like stroma Classically appear as septated, but can be unilocular Usually in body and tail Usually do not communicate with main duct Have malignant potential (11%-38%)* * Reddy, RP et al. Clin Gastroenterol Hepatol 2004; 2:1026.


34 First described by Ohhashi in Japan in 1982 Incidence 2/100,000 Prevalence 26/100,000 Age >60, prevalence increases to 99/100,000* 3 types: Main duct IPMN Main duct is dilated >1cm Cancer prevalence 57-92% Side branch IPMN Disease confined to a side duct Cancer prevalence 6-46% Mixed Ohhashi K., Murakami Y., Maruyama M. Prog Dig Endosc (1982) 20: pp * Reid-Lombardo et al. Incidence, prevalence, and management of IPMN in Olmsted County, Minnesota, Pancreas 2008; 37:
 ; 10:1 Usually located in tail of panc, well demarcated Both solid and cystic")

35 Aka Franz tumor Young woman (avg. 24) ; 10:1 Usually located in tail of panc, well demarcated Both solid and cystic components Cytology shows characteristic branching papillae with myxoid stroma Rare tumor; makes up <1% of all panc neoplasms Behavior less aggressive; 95% 5 yrs (post resection) Mets 15% cases, usually liver.
36 Larger size (>3cm, 9.3% risk * ) <3cm, malignant <5% 3-5cm, malignant 15% >5cm, malignant >30% ** Thickened irregular cyst wall Internal solid component, or mass Possibly calcification of the cyst wall Main pancreatic duct dilitation Cyst fluid CEA level >192 ng/dl (sens 73%, spec 83%) *** DNA molecular analysis * Wu, BU et al. Am J Gastroenterol Jan; 109(1): ** Grobmyer SR, et al. J Surg Oncol. 2009; 100(5):372 *** Brugge, WR et al. Gastroenterology 2004; 126:1330.
37 Serous cystadenoma Mucinous cystadenoma Main duct IPMN Branch duct IPMN Age 50-70s 50-70s 50-70s 50-70s 20-30s Gender F > M Exclusively F F = M F = M F > M Solid pseudopapillary Clinical Incidental Incidental Pancreatitis Pancreatitis Incidental Imaging Cytology DNA Honeycomb Central scar Glycogen positive cuboidal cells Large septations Mucinous, columnar cells K-ras mutation, high DNA amount Fluid CEA <5-20ng/ml >200 ng/ml in 75% Dilated main duct Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Dilated duct branch Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Solid/cystic mass Branching papillae with myxoid stroma Malignant Rare Moderate High Low-mod Mod-high Treatment Only if sx Resection Resection & post rx surveillence Close monitor or resect with surveillence Resection Adapted from Khalid, A, Brugge, WR. Am J Gastroenterol 2007; 102:2339.
38 Serous cystadenoma Mucinous cystadenoma Main duct IPMN Branch duct IPMN Age 50-70s 50-70s 50-70s 50-70s 20-30s Gender F > M Exclusively F F = M F = M F > M Solid pseudopapillary Clinical Incidental Incidental Pancreatitis Pancreatitis Incidental Imaging Cytology DNA Honeycomb Central scar Glycogen positive cuboidal cells Large septations Mucinous, columnar cells K-ras mutation, high DNA amount Fluid CEA <5-20ng/ml >200 ng/ml in 75% Dilated main duct Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Dilated duct branch Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Solid/cystic mass Branching papillae with myxoid stroma Malignant Rare Moderate High Low-mod Mod-high Treatment Only if sx Resection Resection & post rx surveillence Close monitor or resect with surveillence Resection Adapted from Khalid, A, Brugge, WR. Am J Gastroenterol 2007; 102:2339.
39 Serous cystadenoma Mucinous cystadenoma Main duct IPMN Branch duct IPMN Age 50-70s 50-70s 50-70s 50-70s 20-30s Gender F > M Exclusively F F = M F = M F > M Solid pseudopapillary Clinical Incidental Incidental Pancreatitis Pancreatitis Incidental Imaging Cytology DNA Honeycomb Central scar Glycogen positive cuboidal cells Large septations Mucinous, columnar cells K-ras mutation, high DNA amount Fluid CEA <5-20ng/ml >200 ng/ml in 75% Dilated main duct Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Dilated duct branch Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Solid/cystic mass Branching papillae with myxoid stroma Malignant Rare Moderate High Low-mod Mod-high Treatment Only if sx Resection Resection & post rx surveillence Close monitor or resect with surveillence Resection Adapted from Khalid, A, Brugge, WR. Am J Gastroenterol 2007; 102:2339.
40 Serous cystadenoma Mucinous cystadenoma Main duct IPMN Branch duct IPMN Age 50-70s 50-70s 50-70s 50-70s 20-30s Gender F > M Exclusively F F = M F = M F > M Solid pseudopapillary Clinical Incidental Incidental Pancreatitis Pancreatitis Incidental Imaging Cytology DNA Honeycomb Central scar Glycogen positive cuboidal cells Large septations Mucinous, columnar cells K-ras mutation, high DNA amount Fluid CEA <5-20ng/ml >200 ng/ml in 75% Dilated main duct Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Dilated duct branch Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Solid/cystic mass Branching papillae with myxoid stroma Malignant Rare Moderate High Low-mod Mod-high Treatment Only if sx Resection Resection & post rx surveillence Close monitor or resect with surveillence Resection Adapted from Khalid, A, Brugge, WR. Am J Gastroenterol 2007; 102:2339.
41 Serous cystadenoma Mucinous cystadenoma Main duct IPMN Branch duct IPMN Age 50-70s 50-70s 50-70s 50-70s 20-30s Gender F > M Exclusively F F = M F = M F > M Solid pseudopapillary Clinical Incidental Incidental Pancreatitis Pancreatitis Incidental Imaging Cytology DNA Honeycomb Central scar Glycogen positive cuboidal cells Large septations Mucinous, columnar cells K-ras mutation, high DNA amount Fluid CEA <5-20ng/ml >200 ng/ml in 75% Dilated main duct Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Dilated duct branch Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Solid/cystic mass Branching papillae with myxoid stroma Malignant Rare Moderate High Low-mod Mod-high Treatment Only if sx Resection Resection & post rx surveillence Close monitor or resect with surveillence Resection Adapted from Khalid, A, Brugge, WR. Am J Gastroenterol 2007; 102:2339.
42 Serous cystadenoma Mucinous cystadenoma Main duct IPMN Branch duct IPMN Age 50-70s 50-70s 50-70s 50-70s 20-30s Gender F > M Exclusively F F = M F = M F > M Solid pseudopapillary Clinical Incidental Incidental Pancreatitis Pancreatitis Incidental Imaging Cytology DNA Honeycomb Central scar Glycogen positive cuboidal cells Large septations Mucinous, columnar cells K-ras mutation, high DNA amount Fluid CEA <5-20ng/ml >200 ng/ml in 75% Dilated main duct Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Dilated duct branch Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Solid/cystic mass Branching papillae with myxoid stroma Malignant Rare Moderate High Low-mod Mod-high Treatment Only if sx Resection Resection & post rx surveillence Close monitor or resect with surveillence Resection Adapted from Khalid, A, Brugge, WR. Am J Gastroenterol 2007; 102:2339.
43 Serous cystadenoma Mucinous cystadenoma Main duct IPMN Branch duct IPMN Age 50-70s 50-70s 50-70s 50-70s 20-30s Gender F > M Exclusively F F = M F = M F > M Solid pseudopapillary Clinical Incidental Incidental Pancreatitis Pancreatitis Incidental Imaging Cytology DNA Honeycomb Central scar Glycogen positive cuboidal cells Large septations Mucinous, columnar cells K-ras mutation, high DNA amount Fluid CEA <5-20ng/ml >200 ng/ml in 75% Dilated main duct Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Dilated duct branch Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Solid/cystic mass Branching papillae with myxoid stroma Malignant Rare Moderate High Low-mod Mod-high Treatment Only if sx Resection Resection & post rx surveillence Close monitor or resect with surveillence Resection Adapted from Khalid, A, Brugge, WR. Am J Gastroenterol 2007; 102:2339.
44 Serous cystadenoma Mucinous cystadenoma Main duct IPMN Branch duct IPMN Age 50-70s 50-70s 50-70s 50-70s 20-30s Gender F > M Exclusively F F = M F = M F > M Solid pseudopapillary Clinical Incidental Incidental Pancreatitis Pancreatitis Incidental Imaging Cytology DNA Honeycomb Central scar Glycogen positive cuboidal cells Large septations Mucinous, columnar cells K-ras mutation, high DNA amount Fluid CEA <5-20ng/ml >200 ng/ml in 75% Dilated main duct Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Dilated duct branch Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Solid/cystic mass Branching papillae with myxoid stroma Malignant Rare Moderate High Low-mod Mod-high Treatment Only if sx Resection Resection & post rx surveillence Close monitor or resect with surveillence Resection Adapted from Khalid, A, Brugge, WR. Am J Gastroenterol 2007; 102:2339.
45 Serous cystadenoma Mucinous cystadenoma Main duct IPMN Branch duct IPMN Age 50-70s 50-70s 50-70s 50-70s 20-30s Gender F > M Exclusively F F = M F = M F > M Solid pseudopapillary Clinical Incidental Incidental Pancreatitis Pancreatitis Incidental Imaging Cytology DNA Honeycomb Central scar Glycogen positive cuboidal cells Large septations Mucinous, columnar cells K-ras mutation, high DNA amount Fluid CEA <5-20ng/ml >200 ng/ml in 75% Dilated main duct Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Dilated duct branch Mucinous, columnar cells K-ras mutation, high DNA amount >200 ng/ml in 75% Solid/cystic mass Branching papillae with myxoid stroma Malignant Rare Moderate High Low-mod Mod-high Treatment Only if sx Resection Resection & post rx surveillence Close monitor or resect with surveillence Resection Adapted from Khalid, A, Brugge, WR. Am J Gastroenterol 2007; 102:2339.
46
47


48 March 27, 2015
49

50 2. The AGA suggests that patients with pancreatic cysts <3cm without a solid component or a dilated pancreatic duct undergo MRI for surveillance in 1 year and then every 2 years for a total of 5 years if there is no change in cyst size or characteristics. Estimated that an incidental cyst on MRI has 10 in 100,000 chance of mucinous invasive malignancy and 17 in 100,000 chance of being a ductal cancer
51 3. The AGA suggests that pancreatic cysts with at least 2 high-risk features, such as size 3cm, a dilated main pancreatic duct, or presence of an associated solid component, should be examined by EUS-FNA. 3cm size increased risk of malignancy 3x Solid component increased risk 8x EUS-FNA sensitivity of about 60% and specificity of about 90%
52 4. The AGA suggests that patients without concerning EUS-FNA results should undergo MRI surveillence after 1 year and then every 2 years to ensure no change in risk of malignancy. The negative predictive value for an unremarkable EUS is very high, therefore can follow more conservative follow-up
53 5. The AGA suggests that significant changes in the characteristics of the cyst, including the development of a solid component, increasing size of the pancreatic duct, and/or diameter 3cm, are indications for EUS-FNA. If any interval change is seen, then recommend EUS- FNA.

54 6. The AGA suggests against continued surveillance of pancreatic cysts if there has been no significant change in the characteristics of the cyst after 5 years of surveillance or if the patient is no longer a surgical candidate. Authors cautioned that some patients may elect to continue surveillance or if strong family hx pancreas cancer is present.
55 7. The AGA suggests that patients with both a solid component and a dilated pancreatic duct and/or concerning features on EUS and FNA should undergo surgery to reduce the risk of mortality from carcinoma. Normally this would be considered a strong recommendation, but to do so assumes that everyone undergoing surgery will benefit Most beneficial in high-grade dysplasia group Post-op mortality from surgery 2% and high morbidity rate, the true benefit is unclear
56 8. The AGA recommends that if surgery is considered for a pancreatic cyst, patients are referred to a center with demonstrated expertise in pancreatic surgery. Post-op mortality rates range from a low of 2% in centers of excellence to approximately 7% in less experienced institutions.
57 9. The AGA suggests that patients with invasive cancer or dysplasia in a cyst that has been surgically resected should undergo MRI surveillance of any remaining pancreas every 2 years. The authors point out that clinicians may elect to offer more frequent surveillance for cancer resections, or if concern that lesion was not fully resected.
58 10. The AGA suggests against routine surveillance of pancreatic cysts without highgrade dysplasia or malignancy at surgical resection. Continued surveillance in this group is unlikely to be cost-effective Bottom line is the vast majority of asymptomatic cysts are low risk and will prove to be non-lethal
59 1. The AGA recommends that before starting any pancreatic cyst surveillance program, patients should have a clear understanding of programmatic risks and benefits. The AGA s initial motherhood statement is the most important to convey to patients Patients should understand their probability of their cyst becoming malignant, and may elect not to undergo surveillance
60
61 Cyst fluid analysis CEA level 76 ng/ml Level < 192 favors benign serous cyst Level > 192 favors pre-cancerous mucinous type Cytology returned benign Diagnosis likely Serous cystadenoma based on history and CEA level Patient opted for conservative management with surveillance imaging.

62 Most pancreatic incidentalomas end up being benign and only require conservative mgmt Recent pancreatic cyst guidelines favor a less aggressive approach The more complicated cases should be reviewed through a multi-disciplinary approach to outline treatment standards and provide a customized treatment plan for each patient
An Approach to Pancreatic Cysts. Introduction
 An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
Pancreatic Cysts. Darius C. Desai, MD FACS St. Luke s University Health Network
 Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts
 ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
Pancreatic Cystic Lesions 원자력병원
 Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget
 Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Matthew McCollough, M.D. April 9, 2009 University of Louisville
 Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Management A Guideline Based Approach to the Incidental Pancreatic Cysts. Common Cystic Pancreatic Neoplasms.
 Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Outline. Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines
 Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines") Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification
Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Cystic Pancreatic Lesions: Approach to Diagnosis
 Cystic Pancreatic Lesions: Approach to Diagnosis Poster No.: R-0130 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: A. AGARWAL, R. M. Mendelson; Perth/AU Keywords: Cysts, Biopsy, Endoscopy,
Cystic Pancreatic Lesions: Approach to Diagnosis Poster No.: R-0130 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: A. AGARWAL, R. M. Mendelson; Perth/AU Keywords: Cysts, Biopsy, Endoscopy,
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts
 Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts Authors Alexander Lee 1, Vivek Kadiyala 2,LindaS.Lee 3 Institutions 1 Texas Digestive Disease Consultants,
Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts Authors Alexander Lee 1, Vivek Kadiyala 2,LindaS.Lee 3 Institutions 1 Texas Digestive Disease Consultants,
X-ray Corner. Imaging of The Pancreas. Pantongrag-Brown L
 X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
Unusual Pancreatic Neoplasms RTC 2/11/2011
 Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Pancreatic Cystic Neoplasms: Guidelines and beyond
 Pancreatic Cystic Neoplasms: Guidelines and beyond Kenneth J. Chang, MD, FACG, FASGE Executive Director, Comprehensive Digestive Disease Center Professor and Chief, Gastroenterology Vincent & Anna Kong
Pancreatic Cystic Neoplasms: Guidelines and beyond Kenneth J. Chang, MD, FACG, FASGE Executive Director, Comprehensive Digestive Disease Center Professor and Chief, Gastroenterology Vincent & Anna Kong
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
Neuro-endocrine and pancreatic non-adenocarcinomas. Marc Engelbrecht, AMC, Amsterdam
 Neuro-endocrine and pancreatic non-adenocarcinomas Marc Engelbrecht, AMC, Amsterdam Pancreatic Tumors q Epithelial Exocrine q Mesenchymal Ductal Adenocarcinoma (85-95%) Metastasis Lymfoma Acinar Cell Carcinoma
Neuro-endocrine and pancreatic non-adenocarcinomas Marc Engelbrecht, AMC, Amsterdam Pancreatic Tumors q Epithelial Exocrine q Mesenchymal Ductal Adenocarcinoma (85-95%) Metastasis Lymfoma Acinar Cell Carcinoma
Chief Complaint. Retroperitoneal cystic mass incidentally found at health examination center.
 Personal Information Age: 34 y/o Sex: female Past history: major systemic medical history(-) surgical history(-), family history(-) Denied food or drug allergy Chief Complaint Retroperitoneal cystic mass
Personal Information Age: 34 y/o Sex: female Past history: major systemic medical history(-) surgical history(-), family history(-) Denied food or drug allergy Chief Complaint Retroperitoneal cystic mass
Case 1. Case 1: EUS Report 5/1/2017. Interesting Cases of Pancreatic Masses
 Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Cystic pancreatic lesions A proposal for a network approach. Chris Briggs Consultant HPB Surgeon Peninsula HPB Unit Derriford Hospital, Plymouth
 Cystic pancreatic lesions A proposal for a network approach Chris Briggs Consultant HPB Surgeon Peninsula HPB Unit Derriford Hospital, Plymouth Aims Brief overview of cystic pancreatic lesions International
Cystic pancreatic lesions A proposal for a network approach Chris Briggs Consultant HPB Surgeon Peninsula HPB Unit Derriford Hospital, Plymouth Aims Brief overview of cystic pancreatic lesions International
Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases
 Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
American Gastroenterological Association Institute Guidelines for Management of Asymptomatic Neoplastic Pancreatic Cysts
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 American Gastroenterological Association Institute Guidelines for Management of Asymptomatic Neoplastic Pancreatic Cysts Santhi Swaroop Vege, 1 Barry Ziring, 2 Rajeev
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 American Gastroenterological Association Institute Guidelines for Management of Asymptomatic Neoplastic Pancreatic Cysts Santhi Swaroop Vege, 1 Barry Ziring, 2 Rajeev
Morphologic features in cystic lesions of pancreas-a retrospective analysis
 International Journal of Advances in Medicine Cicy PJ et al. Int J Adv Med. 2018 Feb;5(1):192-196 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20180083
International Journal of Advances in Medicine Cicy PJ et al. Int J Adv Med. 2018 Feb;5(1):192-196 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20180083
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Cystic Disease of the Liver Work Up and Management. Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center
 Cystic Disease of the Liver Work Up and Management Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center The Case 73F presents to clinic after diagnostic laparoscopy at OSH. Known liver mass for
Cystic Disease of the Liver Work Up and Management Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center The Case 73F presents to clinic after diagnostic laparoscopy at OSH. Known liver mass for
The Role of Molecular Analysis in the Diagnosis and Surveillance of Pancreatic Cystic Neoplasms
 JOP. J Pancreas (Online) 20 Mar 20; (2):-9. RESEARCH ARTICLE The Role of Molecular Analysis in the Diagnosis and Surveillance of Pancreatic Cystic Neoplasms Megan Winner, Amrita Sethi 2, John M Poneros
JOP. J Pancreas (Online) 20 Mar 20; (2):-9. RESEARCH ARTICLE The Role of Molecular Analysis in the Diagnosis and Surveillance of Pancreatic Cystic Neoplasms Megan Winner, Amrita Sethi 2, John M Poneros
Video Microscopy Tutorial 19
 Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
Cystic lesions of the pancreas
 REVIEW ARTICLE Annals of Gastroenterology (2016) 29, 155-161 Cystic lesions of the pancreas Ioannis Karoumpalis a, Dimitrios K. Christodoulou b General Hospital of Athens G. Gennimatas, Athens; University
REVIEW ARTICLE Annals of Gastroenterology (2016) 29, 155-161 Cystic lesions of the pancreas Ioannis Karoumpalis a, Dimitrios K. Christodoulou b General Hospital of Athens G. Gennimatas, Athens; University
Nonsurgical Management of Asymptomatic Incidental Pancreatic Cysts
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:813 817 Nonsurgical Management of Asymptomatic Incidental Pancreatic Cysts MAOR LAHAV, YAKOV MAOR, BENJAMIN AVIDAN, BEN NOVIS, and SIMON BAR MEIR Department
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:813 817 Nonsurgical Management of Asymptomatic Incidental Pancreatic Cysts MAOR LAHAV, YAKOV MAOR, BENJAMIN AVIDAN, BEN NOVIS, and SIMON BAR MEIR Department
Endoscopic Ultrasonography Clinical Impact. Giancarlo Caletti. Gastroenterologia Università di Bologna. Caletti
 Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Patient History. A 58 year old man presents with a 16 mm cyst in the pancreatic tail. The cyst is unilocular with a thick wall and no mural nodule.
 Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT
 CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Giant pancreatic mucinous cystadenoma with malignant transformation
 Case Report Brunei Int Med J. 2014; 10 (3): 177-182 Giant pancreatic mucinous cystadenoma with malignant transformation Jerica CHAI 1, Vui Heng CHONG 2, Ian BICKLE 1 1 Department of Radiology and 2 Department
Case Report Brunei Int Med J. 2014; 10 (3): 177-182 Giant pancreatic mucinous cystadenoma with malignant transformation Jerica CHAI 1, Vui Heng CHONG 2, Ian BICKLE 1 1 Department of Radiology and 2 Department
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines
 Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
ROSE in EUS guided FNA of Pancreatic Lesions
 ROSE in EUS guided FNA of Pancreatic Lesions Guy s Hospital, London, 16 April 2018 Laxmi Batav Imperial College NHS Trust Imperial College NHS Trust Cytology Workload Cervical Cytology 57,500 (decreases
ROSE in EUS guided FNA of Pancreatic Lesions Guy s Hospital, London, 16 April 2018 Laxmi Batav Imperial College NHS Trust Imperial College NHS Trust Cytology Workload Cervical Cytology 57,500 (decreases
Patient with incidental pancreatic cyst
 Clinical problem Diego Aponte M, MD 1 1 Internal Medicine Gastroenterology Specialist. Gastroenterology Academic Coordinator for Graduate Level. Fundación Sanitas. Bogotá, Colombia.... Received: 07-09-10
Clinical problem Diego Aponte M, MD 1 1 Internal Medicine Gastroenterology Specialist. Gastroenterology Academic Coordinator for Graduate Level. Fundación Sanitas. Bogotá, Colombia.... Received: 07-09-10
Pancreatic Cancer v Screening
 Pancreatic Cancer v Screening Pancreatic cancer: One of America s most lethal cancers 48,960 new cases per year 40,560 deaths per year Source: Am Cancer Soc. Cancer Facts & Figures 2015. Atlanta: American
Pancreatic Cancer v Screening Pancreatic cancer: One of America s most lethal cancers 48,960 new cases per year 40,560 deaths per year Source: Am Cancer Soc. Cancer Facts & Figures 2015. Atlanta: American
Radiological Analysis of Cystic lesions of the Pancreas
 September 2002 Radiological Analysis of Cystic lesions of the Pancreas Shruthi Mahalingaiah, Harvard Medical School Year III, Agenda Background Anatomy and histology Radiological workup of a cyst in the
September 2002 Radiological Analysis of Cystic lesions of the Pancreas Shruthi Mahalingaiah, Harvard Medical School Year III, Agenda Background Anatomy and histology Radiological workup of a cyst in the
Genetics of Pancreatic Cancer. October 6, If you experience technical difficulty during the presentation:
 Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Surgical management and results for cystic neoplasms of pancreas
 Korean J Hepatobiliary Pancreat Surg 2013;17:118-125 Original Article Surgical management and results for cystic neoplasms of pancreas Kyung Won Han 1, Ryun Ha 1, Kun Kuk Kim 1, Jung Nam Lee 1, Yeon Suk
Korean J Hepatobiliary Pancreat Surg 2013;17:118-125 Original Article Surgical management and results for cystic neoplasms of pancreas Kyung Won Han 1, Ryun Ha 1, Kun Kuk Kim 1, Jung Nam Lee 1, Yeon Suk
Types of IPMN. Pancreas Cysts: An Incidental Finding or Harbinger of Malignancy. Cysts: Early Neoplasia. Mucinous Cystic Lesions. EUS-guided FNA EUS
 Pancreas Cysts: An Incidental Finding or Harbinger of Malignancy EUS-guided FNA William R. Brugge,, MD, FACG Professor of Medicine Harvard Medical School Director, GI Endoscopy Unit Massachusetts General
Pancreas Cysts: An Incidental Finding or Harbinger of Malignancy EUS-guided FNA William R. Brugge,, MD, FACG Professor of Medicine Harvard Medical School Director, GI Endoscopy Unit Massachusetts General
Endoscopic Ultrasound Guided Trucut Biopsy of the Cyst Wall for Diagnosing Cystic Pancreatic Tumors
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:974 979 Endoscopic Ultrasound Guided Trucut Biopsy of the Cyst Wall for Diagnosing Cystic Pancreatic Tumors MICHAEL J. LEVY,* THOMAS C. SMYRK, RAGHURAM P.
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:974 979 Endoscopic Ultrasound Guided Trucut Biopsy of the Cyst Wall for Diagnosing Cystic Pancreatic Tumors MICHAEL J. LEVY,* THOMAS C. SMYRK, RAGHURAM P.
Role of Imaging Methods in Diagnosis of Acute Pancreatitis. Válek V. Radiologická klinika, FN Brno a LF MU v Brně
 Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA. Leena Krogerus Helsinki, FINLAND
 Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology PSC- is a pre-neoplastc condition in youg individulas, the cure of which is
Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology PSC- is a pre-neoplastc condition in youg individulas, the cure of which is
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Report of a case of pancreatic hemangioma: A difficult preoperative diagnosis
 www.edoriumjournals.com CASE REPORT PEER REVIEWED OPEN ACCESS Report of a case of pancreatic hemangioma: A difficult preoperative diagnosis AL Hashmi Al Warith, Lagrange Xavier, Fara Régis, Camerlo Antoine
www.edoriumjournals.com CASE REPORT PEER REVIEWED OPEN ACCESS Report of a case of pancreatic hemangioma: A difficult preoperative diagnosis AL Hashmi Al Warith, Lagrange Xavier, Fara Régis, Camerlo Antoine
Pancreatico-biliary cytology: a practical approach to diagnosis. Corina Cotoi
 Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Cystic Lesions of the Pancreas: Changes in the Presentation and Management of 1,424 Patients at a Single Institution over a 15-Year Time Period
 Cystic Lesions of the Pancreas: Changes in the Presentation and Management of 1,424 Patients at a Single Institution over a 15-Year Time Period Sébastien Gaujoux, MD, PhD, Murray F Brennan, MD, FACS, Mithat
Cystic Lesions of the Pancreas: Changes in the Presentation and Management of 1,424 Patients at a Single Institution over a 15-Year Time Period Sébastien Gaujoux, MD, PhD, Murray F Brennan, MD, FACS, Mithat
EUS FNA NEUROENDOCRINE TUMORS. A. Ginès Endocopy Unit Hospital Cínic. Barcelona (Spain)
") EUS FNA NEUROENDOCRINE TUMORS A. Ginès Endocopy Unit Hospital Cínic. Barcelona (Spain) GI NEUROENDOCRINE TUMORS GENERAL CONCEPTS Rare neoplasms arising from the neuroendocrine cells of the GI tract Include:
EUS FNA NEUROENDOCRINE TUMORS A. Ginès Endocopy Unit Hospital Cínic. Barcelona (Spain) GI NEUROENDOCRINE TUMORS GENERAL CONCEPTS Rare neoplasms arising from the neuroendocrine cells of the GI tract Include:
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer
 What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
GASTROINTESTINAL IMAGING STUDY GUIDE
 GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS
 Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS Brooklyn VAMC September 21 st GI Grand Rounds - What is it? - Clinical entity that has emerged from
Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS Brooklyn VAMC September 21 st GI Grand Rounds - What is it? - Clinical entity that has emerged from
Intraductal papillary mucinous neoplasm (IPMN) is a distinct
 is a distinct") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2008;6:815 819 Evaluation of the Guidelines for Management of Pancreatic Branch-Duct Intraductal Papillary Mucinous Neoplasm RAYMOND S. TANG,* BENJAMIN WEINBERG,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2008;6:815 819 Evaluation of the Guidelines for Management of Pancreatic Branch-Duct Intraductal Papillary Mucinous Neoplasm RAYMOND S. TANG,* BENJAMIN WEINBERG,
Cystic Lesions of the Pancreas
 Residents Section Pattern of the Month w668 04.29.11 Khan et al. Residents Section Pattern of the Month Residents inradiology tif Khan 1 Faisal Khosa Ronald L. Eisenberg Khan, Khosa F, Eisenberg RL Keywords:
Residents Section Pattern of the Month w668 04.29.11 Khan et al. Residents Section Pattern of the Month Residents inradiology tif Khan 1 Faisal Khosa Ronald L. Eisenberg Khan, Khosa F, Eisenberg RL Keywords:
Solid pseudopapillary tumour of the pancreas: Report of five cases
 ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Solid pseudopapillary tumour of the pancreas: Report of five cases P Srilatha, V Manna, P Kanthilatha Citation P Srilatha, V Manna, P Kanthilatha..
ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Solid pseudopapillary tumour of the pancreas: Report of five cases P Srilatha, V Manna, P Kanthilatha Citation P Srilatha, V Manna, P Kanthilatha..
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital
 Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
Accuracy of CT in predicting malignant potential of cystic pancreatic neoplasms
 HPB, 2008; 10: 483490 ORIGINAL ARTICLE Accuracy of CT in predicting malignant potential of cystic pancreatic neoplasms WILLIAM E. FISHER a, SALLY E. HODGES a, VIVEK YAGNIK b, FANNIE E. MORÓN b, MENG-FEN
HPB, 2008; 10: 483490 ORIGINAL ARTICLE Accuracy of CT in predicting malignant potential of cystic pancreatic neoplasms WILLIAM E. FISHER a, SALLY E. HODGES a, VIVEK YAGNIK b, FANNIE E. MORÓN b, MENG-FEN
Malignant Focal Liver Lesions
 Malignant Focal Liver Lesions Other Than HCC Pablo R. Ros, MD, MPH, PhD Departments of Radiology and Pathology University Hospitals Cleveland Medical Center Case Western Reserve University Pablo.Ros@UHhospitals.org
Malignant Focal Liver Lesions Other Than HCC Pablo R. Ros, MD, MPH, PhD Departments of Radiology and Pathology University Hospitals Cleveland Medical Center Case Western Reserve University Pablo.Ros@UHhospitals.org
Intro to Gallbladder & Pancreas Pathology
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
Cystic Lesions of the Pancreas: Clinical and Pathologic Review of Cases in a Five Year Period
 JOP. J Pancreas (Online) Jul ; (4):38364. ORIGINAL ARTICLE Cystic Lesions of the Pancreas: Clinical and Pathologic Review of Cases in a Five Year Period Carlos E ParraHerran, Mónica T Garcia, Loren Herrera,
JOP. J Pancreas (Online) Jul ; (4):38364. ORIGINAL ARTICLE Cystic Lesions of the Pancreas: Clinical and Pathologic Review of Cases in a Five Year Period Carlos E ParraHerran, Mónica T Garcia, Loren Herrera,
PersPeCTIves. Controversies in the management of pancreatic ipmn. Masao Tanaka
 PersPeCTIves OpiniOn Controversies in the management of pancreatic ipmn Masao Tanaka Abstract Although considerable progress has been made in our understanding of intraductal papillary mucinous neoplasm
PersPeCTIves OpiniOn Controversies in the management of pancreatic ipmn Masao Tanaka Abstract Although considerable progress has been made in our understanding of intraductal papillary mucinous neoplasm
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Diagnostic performance of endoscopic ultrasound-guided fine-needle aspiration in pancreatic lesions
 European Review for Medical and Pharmacological Sciences 2018; 22: 1397-1401 Diagnostic performance of endoscopic in pancreatic lesions Q.-M. WU 1, Y.-N. GUO 1, Y.-Q. XU 1 Digestive Department of Beijing
European Review for Medical and Pharmacological Sciences 2018; 22: 1397-1401 Diagnostic performance of endoscopic in pancreatic lesions Q.-M. WU 1, Y.-N. GUO 1, Y.-Q. XU 1 Digestive Department of Beijing
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Laparoscopic & Robotic Surgery in Pancreas Disease
 2007 년도대한췌담도학회추계학술대회 Session IV: Recent Updates in Pancreatobiliary Diseases Laparoscopic & Robotic Surgery in Pancreas Disease Department of Surgery, Yonsei University College of Medicine, Korea Woo-Jung
2007 년도대한췌담도학회추계학술대회 Session IV: Recent Updates in Pancreatobiliary Diseases Laparoscopic & Robotic Surgery in Pancreas Disease Department of Surgery, Yonsei University College of Medicine, Korea Woo-Jung
Pancreatic Lesions. Valerie Jefford Pediatric Surgery Rounds June 6, 2003
 Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes
 Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes Evan A. Alston, MD 1 ; Sejong Bae, PhD 2 ; and Isam A. Eltoum, MD, MBA 1 BACKGROUND:
Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes Evan A. Alston, MD 1 ; Sejong Bae, PhD 2 ; and Isam A. Eltoum, MD, MBA 1 BACKGROUND:
Cytopathology Study Day 16 April RCPath - BAC. Digital cytology: EUS FNA pancreas and head and neck
 Cytopathology Study Day 16 April 2017 Guy s Hospital London RCPath - BAC Digital cytology: EUS FNA pancreas and head and neck R. Dina MD, FIAC, FRCPath Consultant Cyto/Histopathologist Hon Sen Lecturer
Cytopathology Study Day 16 April 2017 Guy s Hospital London RCPath - BAC Digital cytology: EUS FNA pancreas and head and neck R. Dina MD, FIAC, FRCPath Consultant Cyto/Histopathologist Hon Sen Lecturer
5/17/2013. Pancreatic Cancer. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Case presentation. Differential diagnosis
 Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Pancreatic cystic neoplasms - A pictorial review
 Pancreatic cystic neoplasms - A pictorial review Poster No.: C-2386 Congress: ECR 2014 Type: Educational Exhibit Authors: J. Adu, A. McLean, A. Parsai, K. L. Shahabuddin; London/UK Keywords: Abdomen, Pancreas,
Pancreatic cystic neoplasms - A pictorial review Poster No.: C-2386 Congress: ECR 2014 Type: Educational Exhibit Authors: J. Adu, A. McLean, A. Parsai, K. L. Shahabuddin; London/UK Keywords: Abdomen, Pancreas,
X-Ray Corner. Imaging Approach to Cystic Liver Lesions. Pantongrag-Brown L. Solitary cystic liver lesions. Hepatic simple cyst (Figure 1)
") THAI J 136 Imaging Approach to Cystic Liver Lesions GASTROENTEROL 2013 X-Ray Corner Imaging Approach to Cystic Liver Lesions Pantongrag-Brown L Cystic liver lesions are common findings in daily practice
THAI J 136 Imaging Approach to Cystic Liver Lesions GASTROENTEROL 2013 X-Ray Corner Imaging Approach to Cystic Liver Lesions Pantongrag-Brown L Cystic liver lesions are common findings in daily practice
Biliary Cystadenoma Causing Esophageal Varices
 https://doi.org/10.7180/kmj.2016.31.2.191 KMJ Case Report Biliary Cystadenoma Causing Esophageal Varices Sung Ju Kang, Tae Hee Lee, Min Gyu Seok, Hyo Jin Yun, Ye Seul Jang, Jun Hyun Byun Department of
https://doi.org/10.7180/kmj.2016.31.2.191 KMJ Case Report Biliary Cystadenoma Causing Esophageal Varices Sung Ju Kang, Tae Hee Lee, Min Gyu Seok, Hyo Jin Yun, Ye Seul Jang, Jun Hyun Byun Department of
ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS
 ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS Prof. Fernando Schmitt Medical Faculty of Porto University, Porto, Portugal IPATIMUP General Secretary of the International Academy of Cytology
ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS Prof. Fernando Schmitt Medical Faculty of Porto University, Porto, Portugal IPATIMUP General Secretary of the International Academy of Cytology
EUS-FNA OF PANCREATIC EXOCRINE TUMORS COMPARISON OF EXPERIENCES WITH PATHOLOGICAL DIAGNOSIS
 EUS-FNA OF PANCREATIC EXOCRINE TUMORS COMPARISON OF EXPERIENCES WITH PATHOLOGICAL DIAGNOSIS Vincenzo Canzonieri, M.D. CRO - Aviano National Cancer Institute Dept of Pathology EUS European Cyto-Pathologist
EUS-FNA OF PANCREATIC EXOCRINE TUMORS COMPARISON OF EXPERIENCES WITH PATHOLOGICAL DIAGNOSIS Vincenzo Canzonieri, M.D. CRO - Aviano National Cancer Institute Dept of Pathology EUS European Cyto-Pathologist
HEPATO-BILIARY IMAGING
 HEPATO-BILIARY IMAGING BY MAMDOUH MAHFOUZ MD PROF.OF RADIOLOGY CAIRO UNIVERSITY mamdouh.m5@gmail.com www.ssregypt.com CT ABDOMEN Indications Patient preparation Patient position Scanogram Fasting 4-6 hours
HEPATO-BILIARY IMAGING BY MAMDOUH MAHFOUZ MD PROF.OF RADIOLOGY CAIRO UNIVERSITY mamdouh.m5@gmail.com www.ssregypt.com CT ABDOMEN Indications Patient preparation Patient position Scanogram Fasting 4-6 hours
Fine-Needle Aspiration Biopsy of Solid Pancreatic Masses: Comparison of CT and Endoscopic Sonography Guidance
 Comparison of Guidance Techniques for Pancreatic Mass Biopsy Abdominal Imaging Original Research A C D E M N E U T R Y L I A M C A I G O F I N G Sukru Mehmet Erturk 1 Koenraad J. Mortelé 1 Kemal Tuncali
Comparison of Guidance Techniques for Pancreatic Mass Biopsy Abdominal Imaging Original Research A C D E M N E U T R Y L I A M C A I G O F I N G Sukru Mehmet Erturk 1 Koenraad J. Mortelé 1 Kemal Tuncali
Spectrum of Causes of Pancreatic Calcifications
 Pictorial Essay Downloaded from www.ajronline.org by 46.3.200.2 on 12/21/17 from IP address 46.3.200.2. Copyright RRS. For personal use only; all rights reserved Spectrum of Causes of Pancreatic Calcifications
Pictorial Essay Downloaded from www.ajronline.org by 46.3.200.2 on 12/21/17 from IP address 46.3.200.2. Copyright RRS. For personal use only; all rights reserved Spectrum of Causes of Pancreatic Calcifications
3/28/2012. Periampullary Tumors. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Eric K. Nakakura Ko Olina, HI
 Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Collecting Cancer Data: Pancreas
 Collecting Cancer Data: Pancreas NAACCR 2011 2012 Webinar Series 1/5/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data: Pancreas NAACCR 2011 2012 Webinar Series 1/5/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Role of Endoscopic Ultrasonography in the Diagnosis and Treatment of Cystic Tumors of the Pancreas
 ROUND TABLE Role of Endoscopic Ultrasonography in the Diagnosis and Treatment of Cystic Tumors of the Pancreas Manoop S Bhutani Center for Endoscopic Ultrasound - Center for Endoscopic Research, Training
ROUND TABLE Role of Endoscopic Ultrasonography in the Diagnosis and Treatment of Cystic Tumors of the Pancreas Manoop S Bhutani Center for Endoscopic Ultrasound - Center for Endoscopic Research, Training
Imaging Guided Biopsy. Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer
 Imaging Guided Biopsy Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer Objective By the End of this lessons you should : Define what biopsy Justify Aim to perform biopsy
Imaging Guided Biopsy Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer Objective By the End of this lessons you should : Define what biopsy Justify Aim to perform biopsy
Pancreatic cysts: etiology, diagnosis and management
 Cent. Eur. J. Med. 9(1) 2014 92-107 DOI: 10.2478/s11536-013-0244-8 Central European Journal of Medicine Pancreatic cysts: etiology, diagnosis and management Review Article Beata Jabłońska* Department of
Cent. Eur. J. Med. 9(1) 2014 92-107 DOI: 10.2478/s11536-013-0244-8 Central European Journal of Medicine Pancreatic cysts: etiology, diagnosis and management Review Article Beata Jabłońska* Department of
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors
 AJCP / REPORTING RECOMMENDATIONS FOR PANCREATIC SPECIMENS CONTAINING MALIGNANT TUMORS Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors Jorge AlboresSaavedra, David
AJCP / REPORTING RECOMMENDATIONS FOR PANCREATIC SPECIMENS CONTAINING MALIGNANT TUMORS Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors Jorge AlboresSaavedra, David
Intro to Gallbladder & Pancreas Pathology
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis i acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Dept. of Pathology
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis i acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Dept. of Pathology