Video Microscopy Tutorial 19
|
|
|
- Beverley Sharp
- 6 years ago
- Views:
Transcription

1 Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary.

2 EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard Medical School
3 Course Objectives Define the subclassification of the cystic lesions of the pancreas. Recognize the pitfalls to diagnosis introduced by the EUS-guided biopsy technique. Identify the cytological criteria for the diagnosis of most cystic lesions of the pancreas. Understand the benefits and limitations of ancillary tests such as mucin stains, cyst fluid analysis and molecular analysis in the cytological evaluation of pancreatic cysts.
4 Cystic Mass lesions of the Pancreas (WHO Classification 2010) Pseudocyst Serous cystadenoma Lymphoepithelial cyst Premalignant Lesions PanIN-3 Intraductal papillary mucinous neoplasm with low to intermediate grade dysplasia Intraductal papillary mucinous neoplasm with high grade dysplasia Mucinous cystic neoplasm with low to intermediate grade dysplasia Mucinous cystic neoplasm with high grade dysplasia Malignant Intraductal papillary mucinous neoplasm with invasive carcinoma Mucinous cystic neoplasm with invasive carcinoma



5 Normal Pancreas Ductal Cells
6 Gastrointestinal Contamination Duodenum Stomach
7 Multimodal Approach required for diagnosis of pancreatic cysts Clinical presentation EUS features Gross appearance of cyst fluid Cytology Special stains for mucin Cyst fluid analysis Molecular analysis
8 Multimodal Approach required for diagnosis of pancreatic cysts Clinical presentation Patient age and gender Alcoholism Pancreatitis Trauma Jaundice Asymptomatic
9 Multimodal Approach required for diagnosis of pancreatic cysts EUS features Location Number and size of cysts Main duct dilatation Connectivity to the main duct Septations Cyst wall thickness Mural nodule Invasion of peripancreatic structures
10 Multimodal Approach required for diagnosis of pancreatic cysts Gross appearance of cyst fluid Cyst volume aspirated Watery Clear or colored Bloody Mucoid-thick and viscous or thin
11 Multimodal Approach required for diagnosis of pancreatic cysts Cytology Extracellular mucin-quality and quantity Epithelial cells Uniform and cuboidal; finely vacuolated Columnar and glandular Mucinous Atypical GI contamination Background elements (other than mucin) Inflammation and histiocytes Cellular necrosis
12 Pancreas Cyst Fluid Triage Protocol Sept. 1, 2011 All, fresh to molecular lab Warren 5 by endoscopist ~0.3cc KRAS (fresh) <0.5cc or EUS Requisition form with detailed information and all requests marked CEA (fresh) ~0.3cc ~0.3cc All, fresh to cytology lab Warren cc supernatant ~0.3cc ~volumes required vortex &/or Centrifuge residual 0.3cc ~0.3cc cells Warren 5 KRAS (clinical) Warren 5 1. CEA 2. Amylase 3. Molecular (research) Cytospin Core lab Gray 5 Core lab Gray 5 Warren 5 Cytologist 11
 Is the cyst benign or malignant?")
13 Two basic questions for Cyst analysis 1) Is the cyst mucinous or non mucinous? 2) Is the cyst benign or malignant? MASSACHUSETTS GENERAL PHYSICIANS ORGANIZATION HARVARD 12 MEDICAL SCHOOL
14 Pancreatic Cyst Fluid Analysis Biochemical CEA Amylase Molecular KRAS, GNAS Cytological MASSACHUSETTS GENERAL PHYSICIANS ORGANIZATION HARVARD 13 MEDICAL SCHOOL

15 Cytological Analysis of Cyst Fluid Challenges Scant fluid Low to no cellularity GI contamination Lack of experience with these types of specimens
16 GI contamination in EUS FNAB Duodenum Stomach


17 Mucin Stains Alcian Blue Mucicarmine
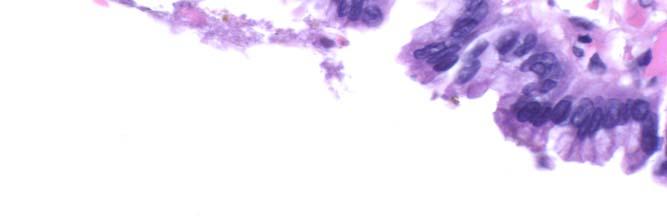
18 Atypical Epithelial Cells Significant
19 Amylase Levels High levels should be seen in Pseudocysts Low levels should be seen in Serous cysts LEC Variable levels in IPMN MCN
20 CEA by cyst fluid analysis >~200 ng/ml 10 1 Serous Inflammatory Mucinous Borderline Malignant thology 200ng/ml 19
21 Molecular Analysis Controversial for accurate diagnosis of cyst type and grade Studies have looked at KRAS and LOH mutations as well as DNA quality and quantity in cyst fluid to Differentiate non-mucinous from mucinous Benign from malignant
22 Molecular Tests KRAS Mutations support mucinous etiology GNAS Mutations present in ~60% IPMN but not MCN Sci Transl Med 20 July 2011 ** KRAS and GNAS mutations do not predict malignancy
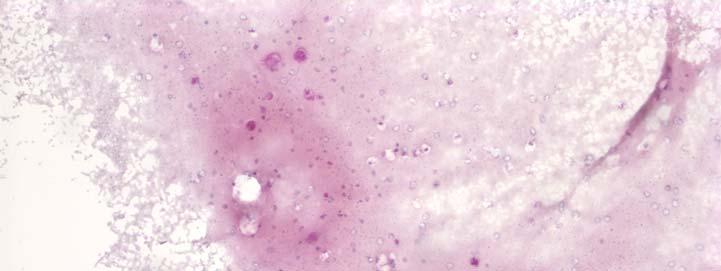
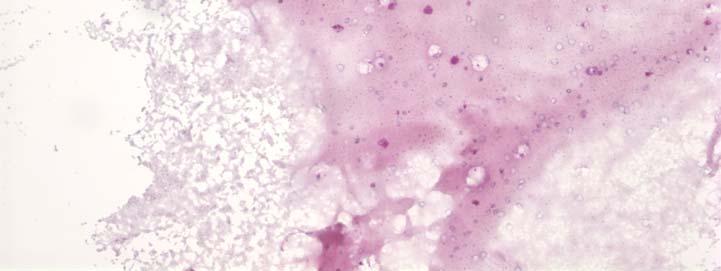
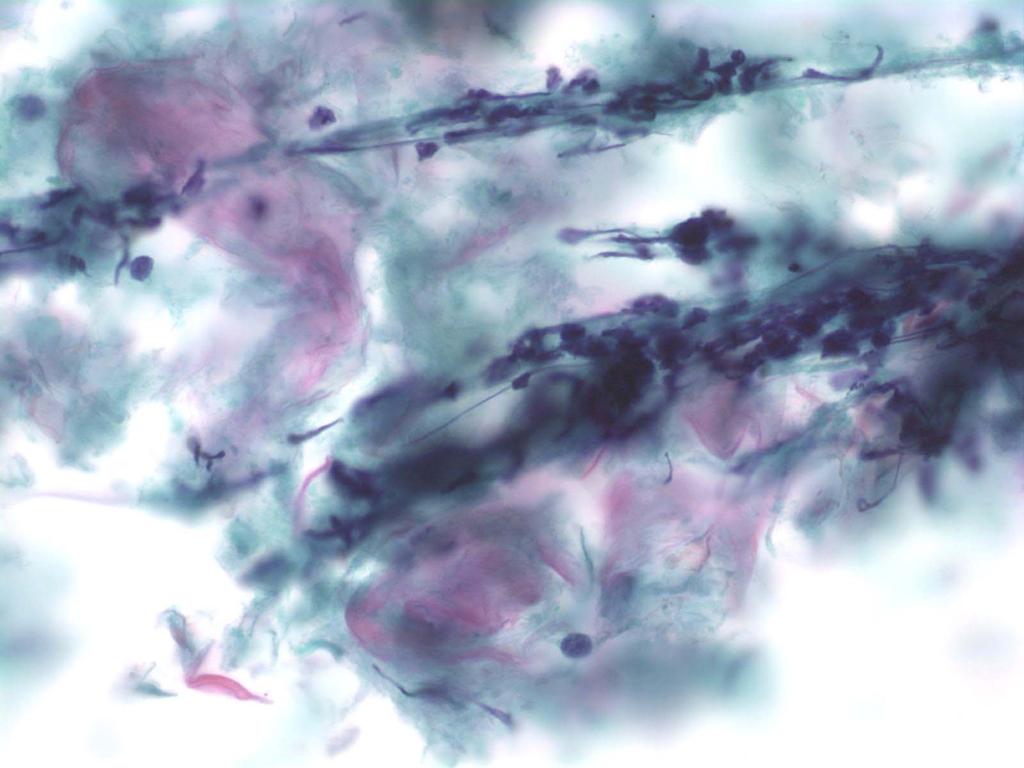
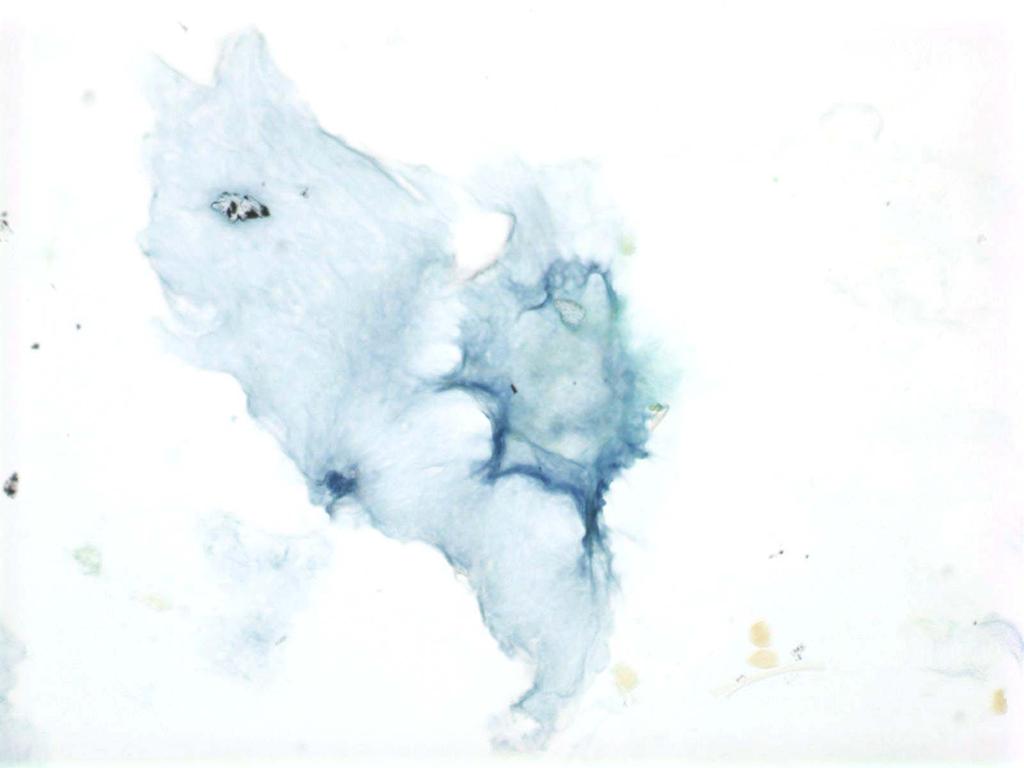
23 Case 1 A 42 year old alcoholic male with abdominal pain is found to have a 3cm pancreatic cyst. An FNA is performed and 3 cc's of thin brown fluid is sent fresh to the lab where 4 cytospins are made: 2 for Papanicolaou stain and 2 for mucins stains (Alcian blue ph 2.5 and mucicarmine). 1 cc of fresh aspirate is sent to the chemistry lab for amylase and CEA analysis.
24 Case 1: EUS Report EUS shows a unilocular thin walled cyst in the pancreatic head without septations. No mural mass is noted.
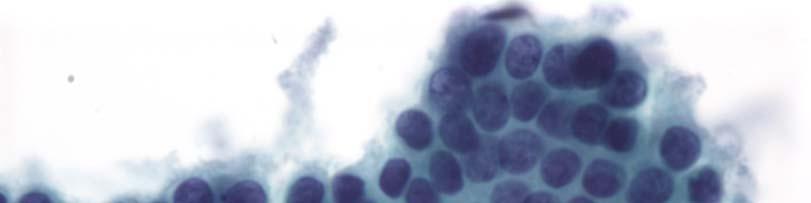
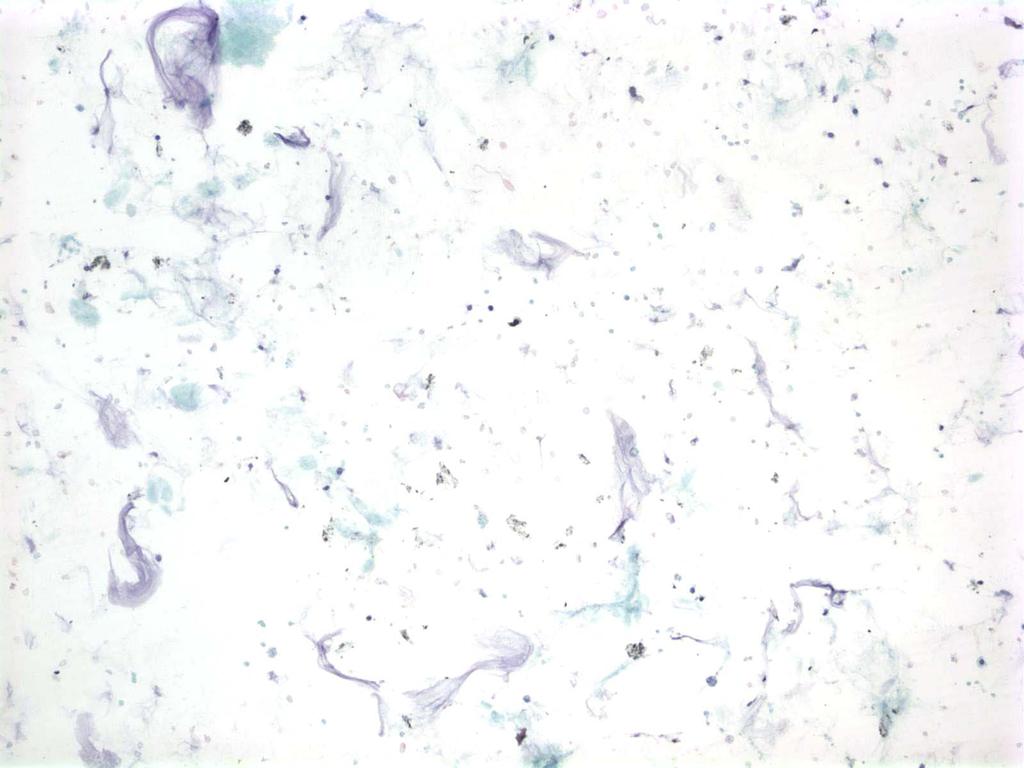
25 Case 1
26 Case 1
27 Case 1: Cyst Fluid Analysis Amylase = 153,000 U/L CEA = 0.5 ng/ml.
28 Case 1 Cytology Diagnosis: Cyst debris consistent with pseudocyst Histology Diagnosis: Pseudocyst
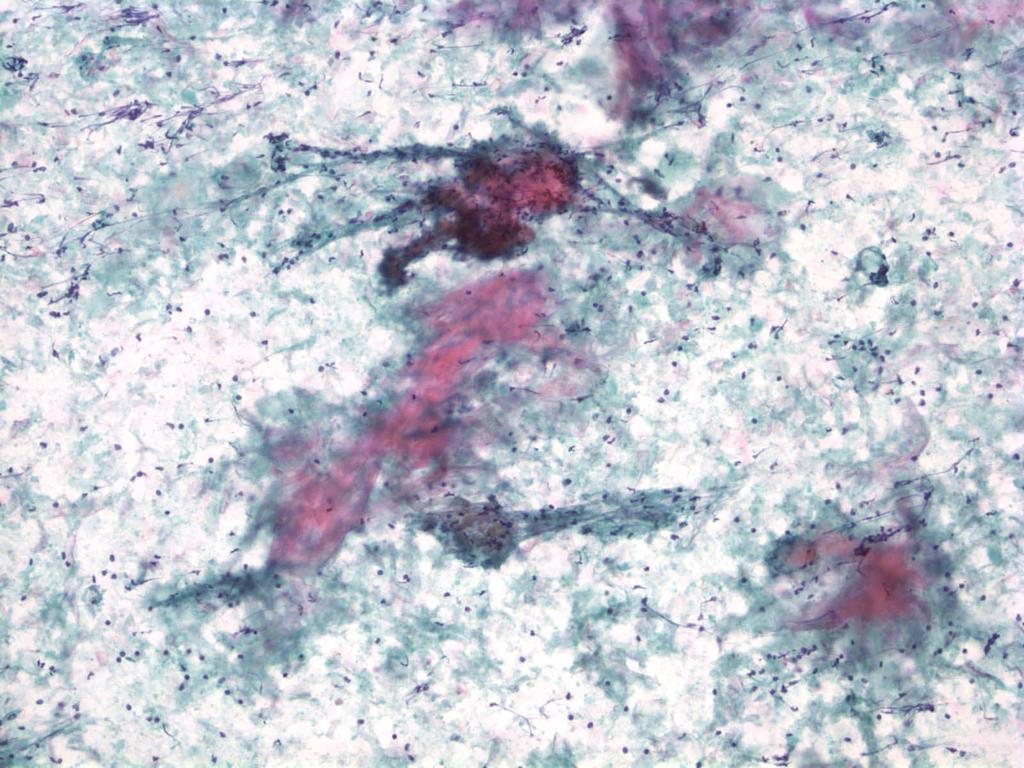
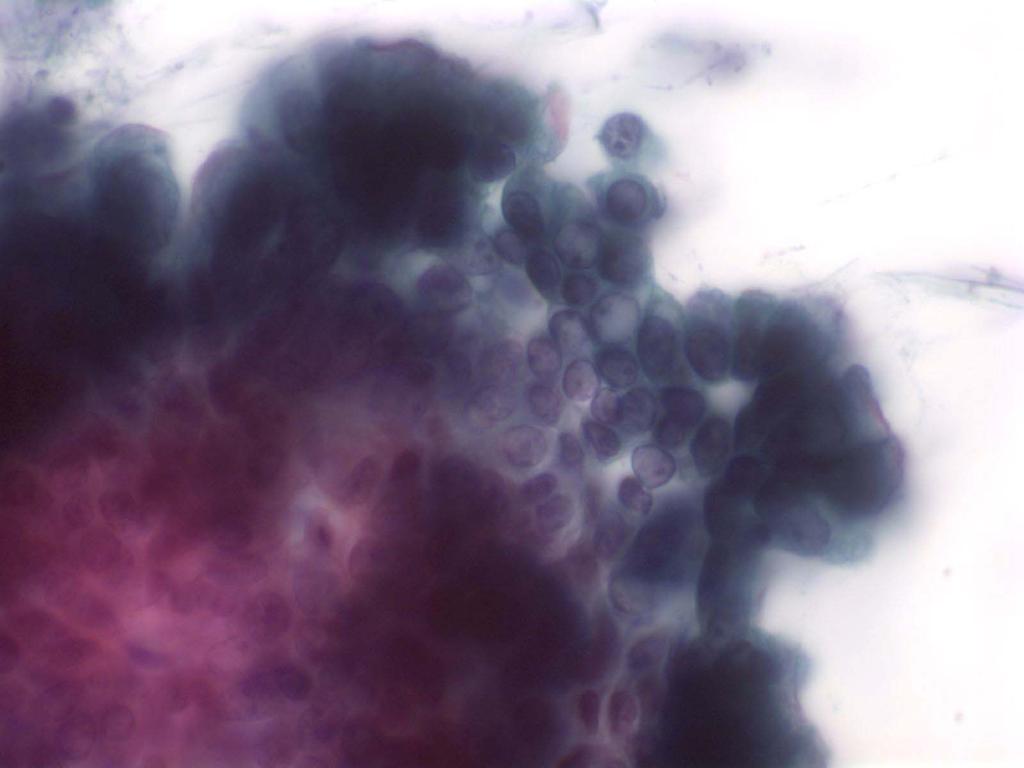
29 Case 2 A 59 year old alcoholic male with a history of pancreatitis presents with abdominal pain and is found to have a 3cm cyst in the pancreatic tail. Aspiration is productive of 1cc of thick fluid; a direct smear is made and the remaining fluid submitted for cyst fluid analysis.
30 Case 2: EUS Report A 3cm thin walled unilocular cyst in the pancreatic tail is seen. No mural mass is noted. The main pancreatic duct is normal. The cyst is collapsed by aspiration.
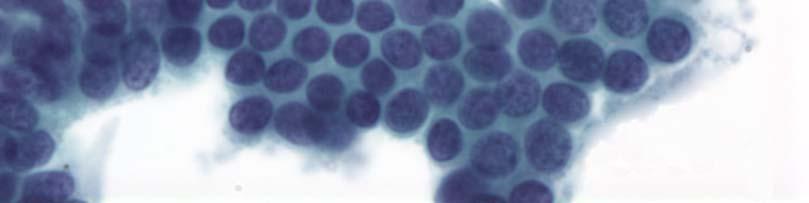
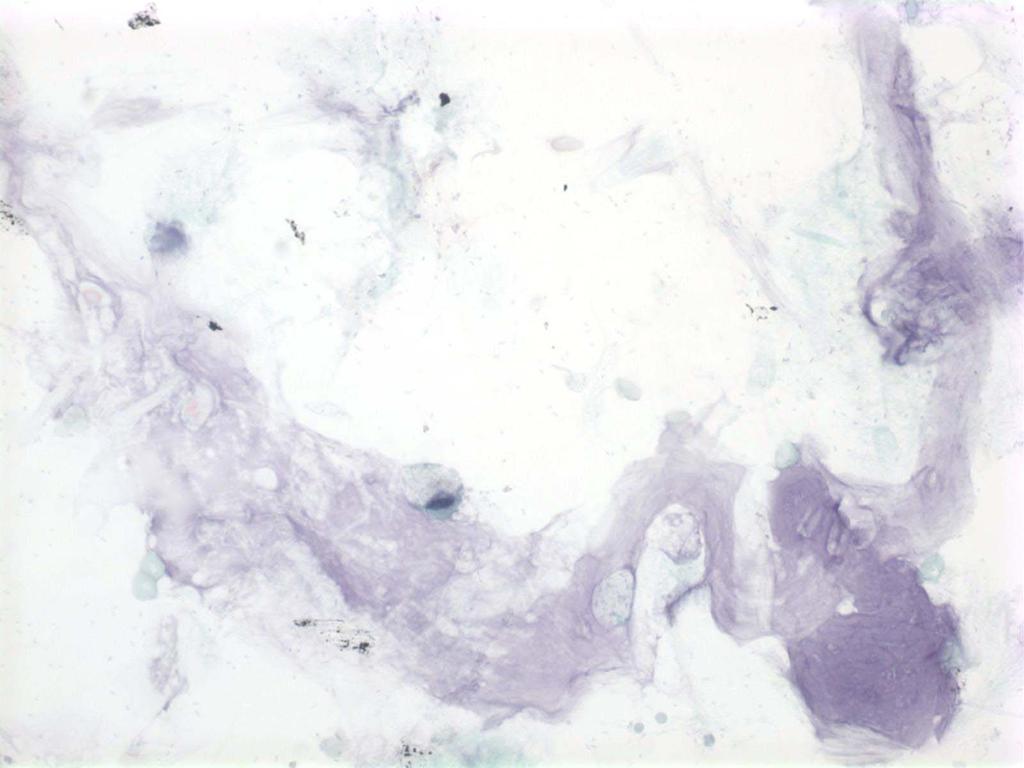
31 Case 2
32 Case 2
33 Cyst Fluid Analysis Amylase = 105,000 U/L CEA = 10 ng/ml.
34 Case 2 Cytology Diagnosis: Mucoid cyst fluid with high amylase and low CEA suggestive of a pseudocyst. A mucinous cyst cannot entirely be excluded. Short term clinical follow-up recommended. Follow-up: Cyst resolved at 3 months
 Associated with pancreatitis, trauma, surgery")

35 Pancreatic Pseudocyst Clinical Most common cystic lesion in the pancreas (75-90%) Associated with pancreatitis, trauma, surgery Radiology Thin to thick walled, unilocular, no septations 65% in the tail Fluid aspirated is often dark, hemorrhagic, oily and not mucoid
36 Pseudocysts: Ancillary tests Cytospins for mucin stains are negative(mucicarmine and or alcian blue) Cyst fluid analysis Consistently elevated amylase (thousand U/L) due to connectivity of the cyst to the duct Undetectable or very low CEA
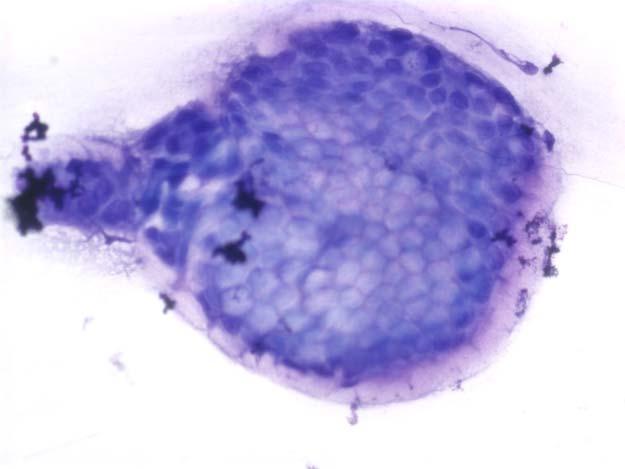
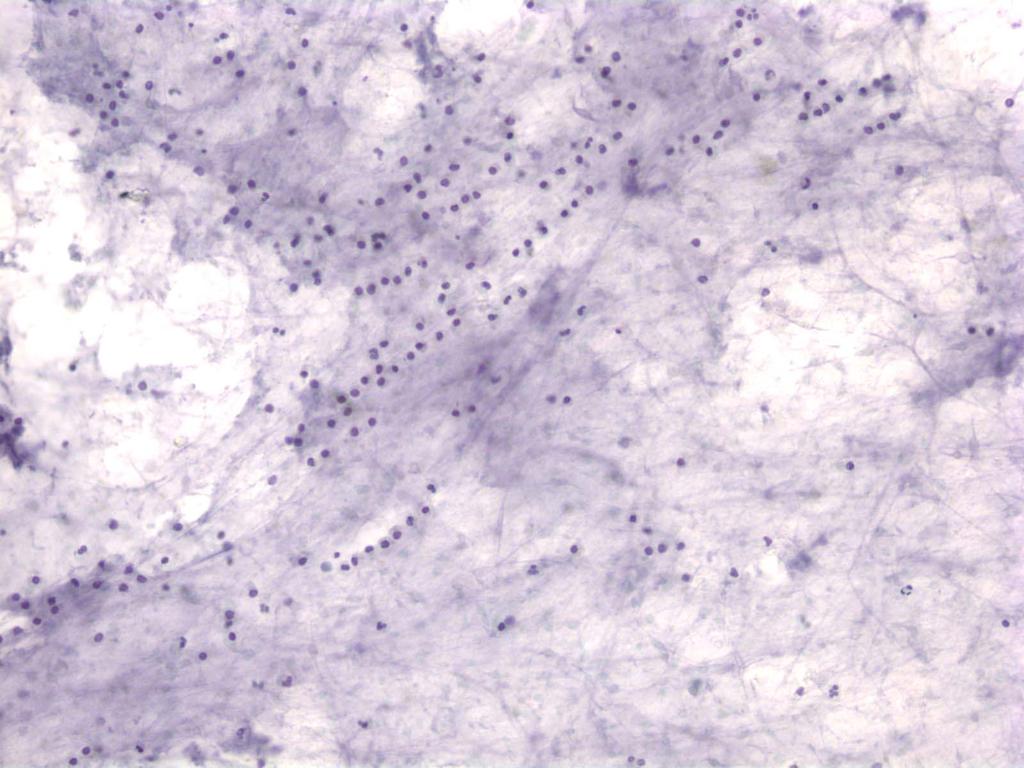
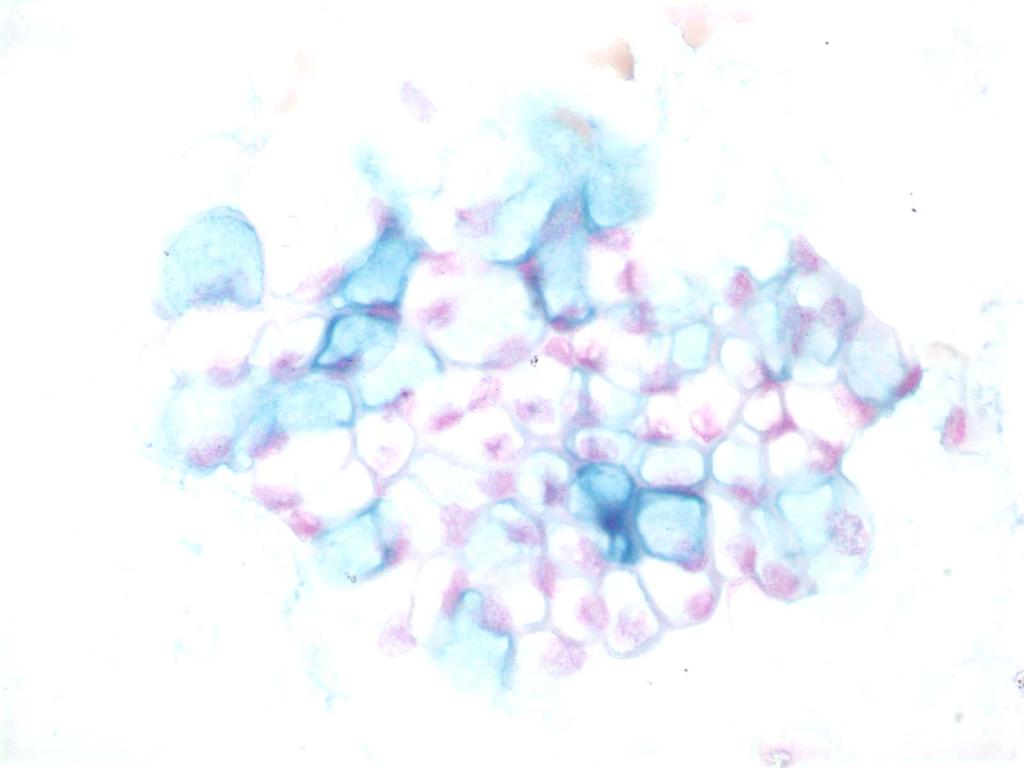
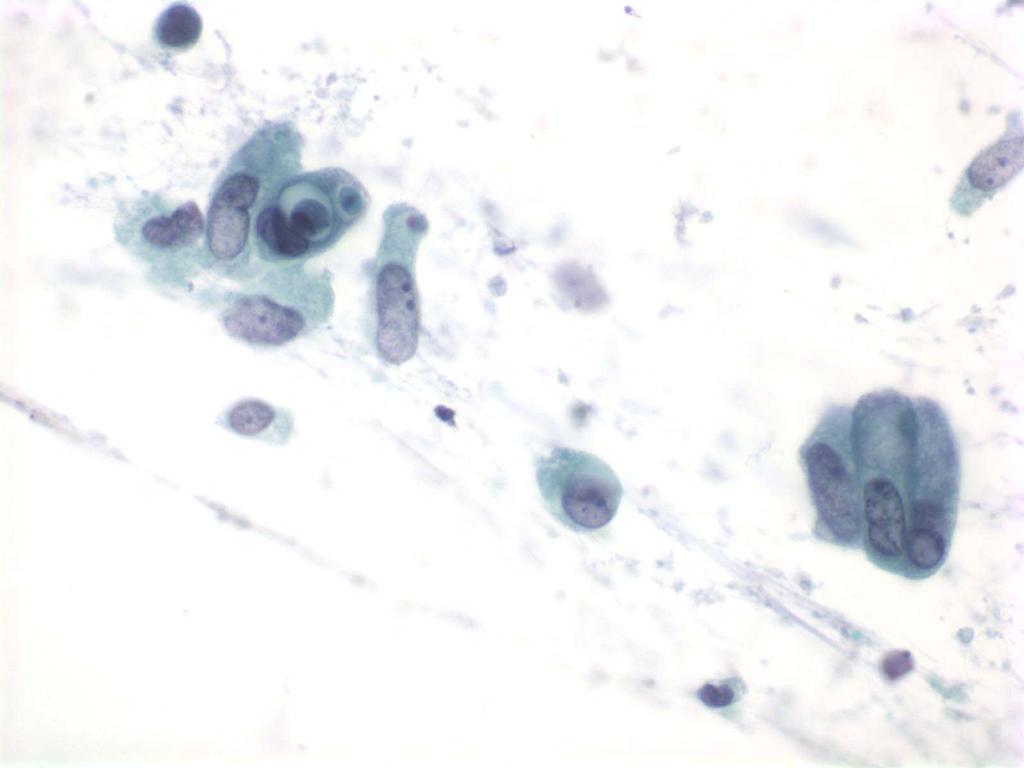
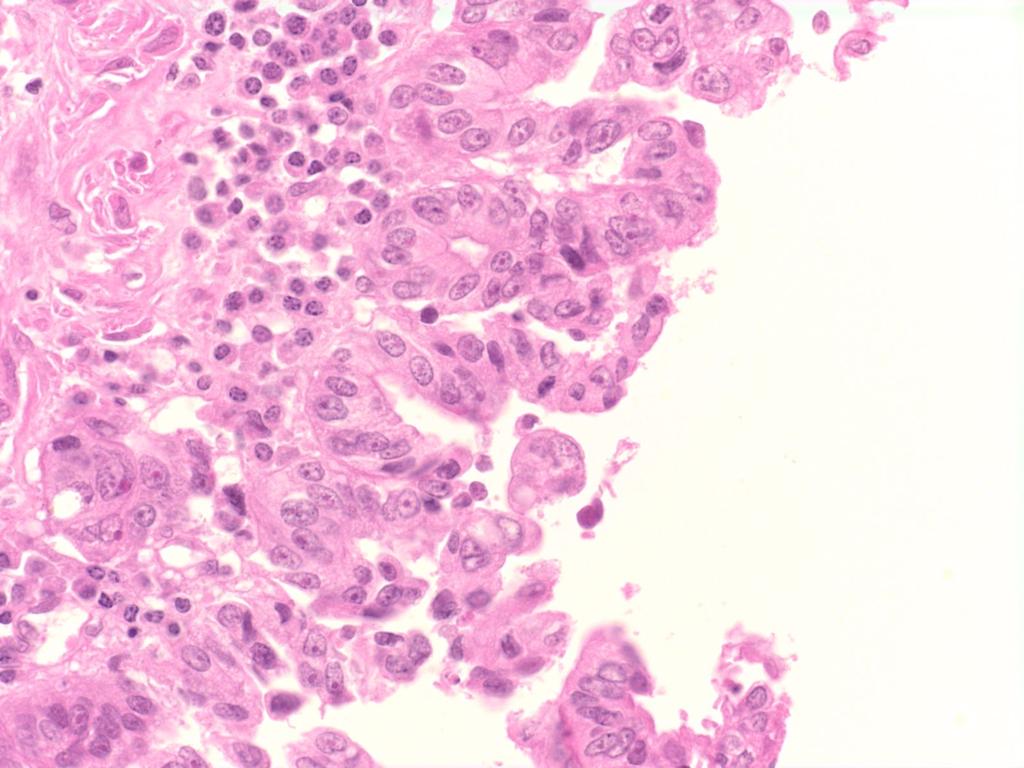
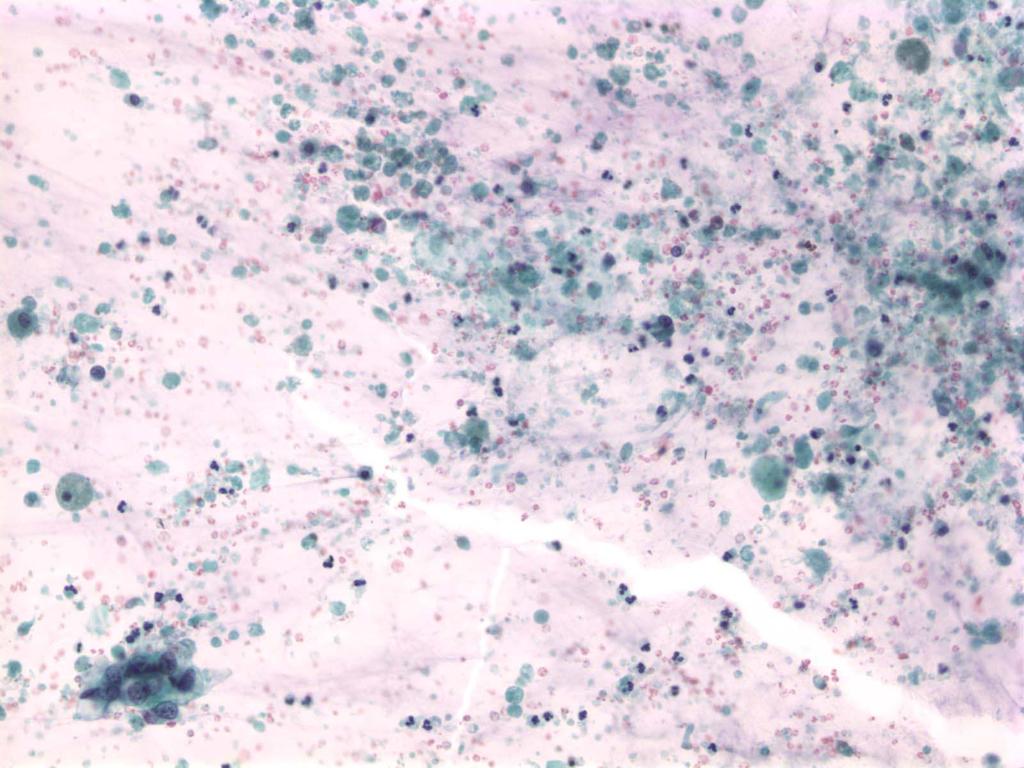
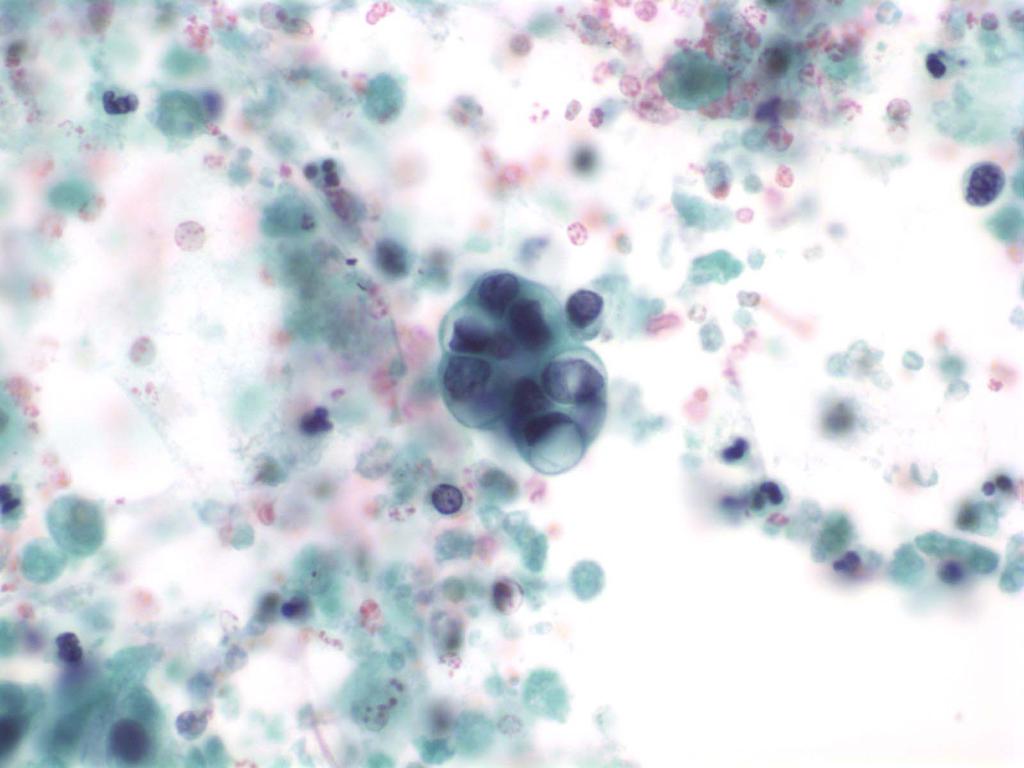
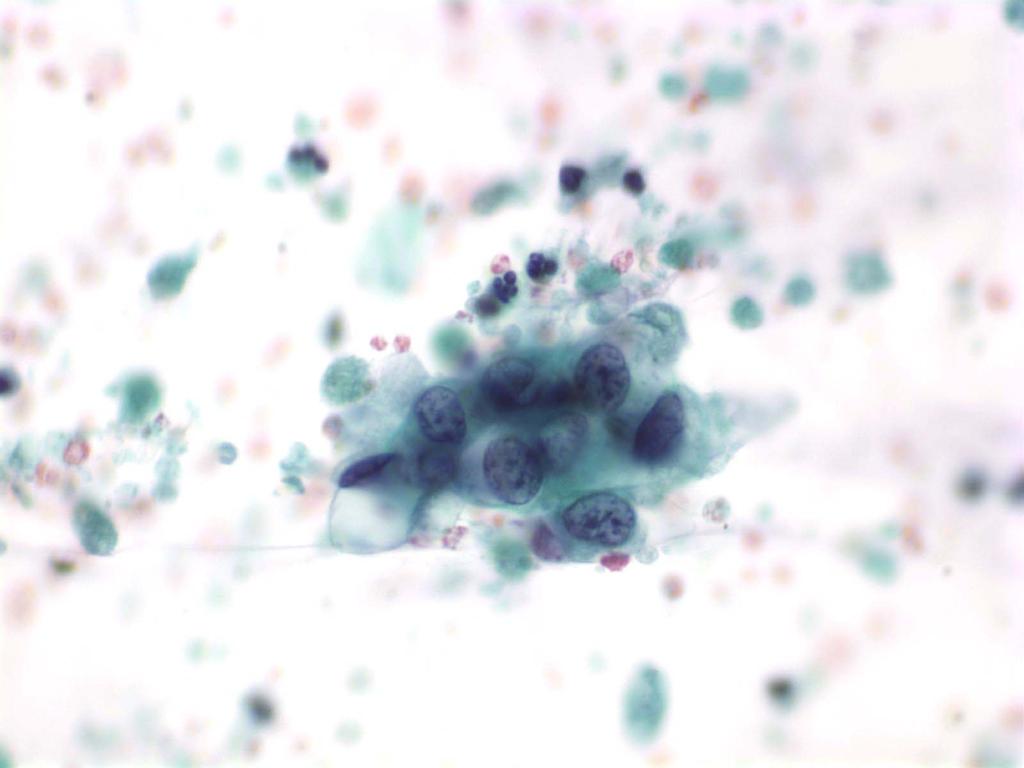
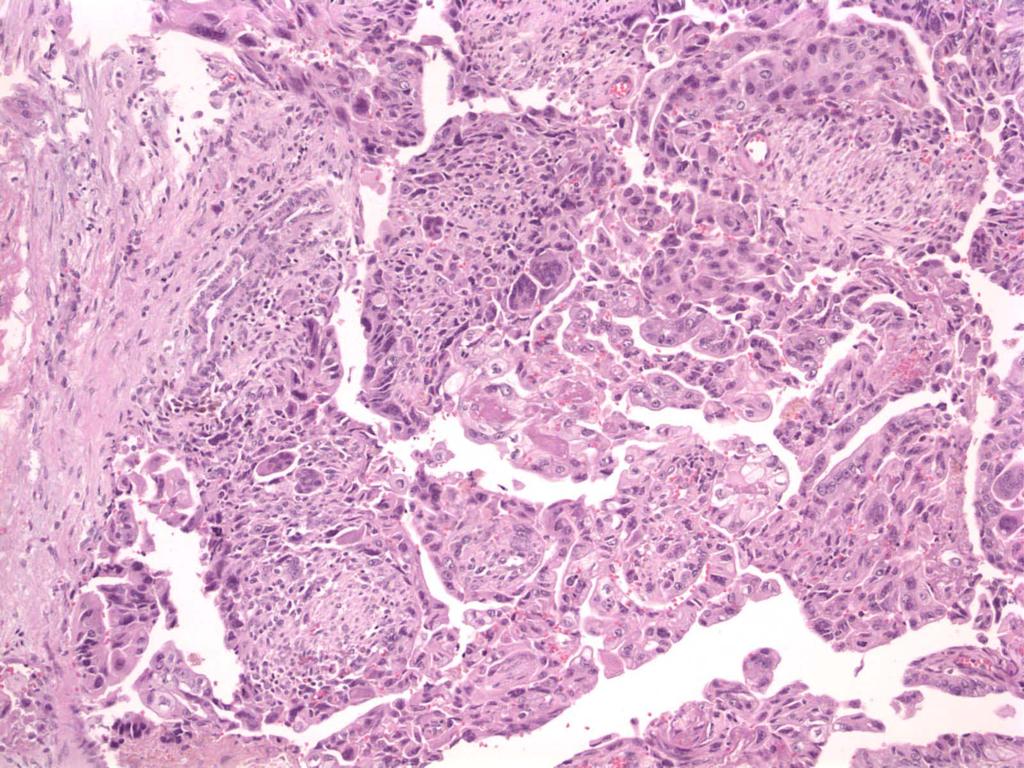
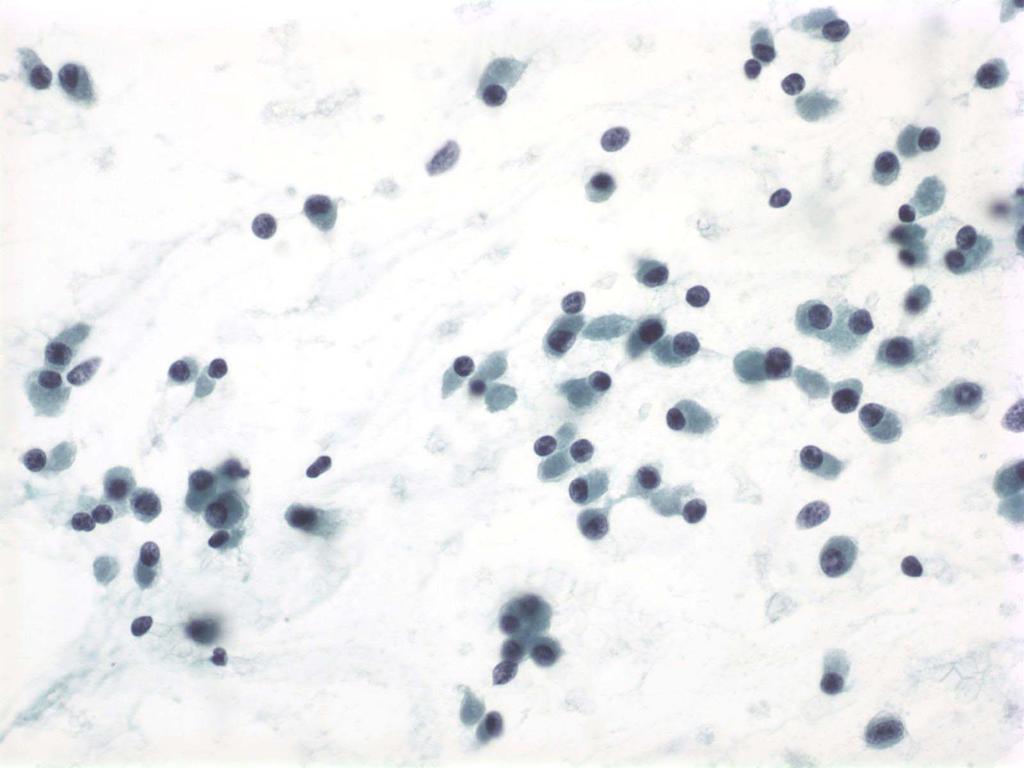
37 Case 3 A 76 year old asymptomatic man was found to have a mass in the pancreatic tail. Approximately 1cc of slightly cloudy thin fluid was removed. One direct smear was made from a drop of fluid and the remaining fluid sent for cyst fluid analysis.
38 Case 3: EUS Report A 4 cm well defined microcystic mass was noted in the pancreatic tail. There was no evidence of invasion of surrounding structures.
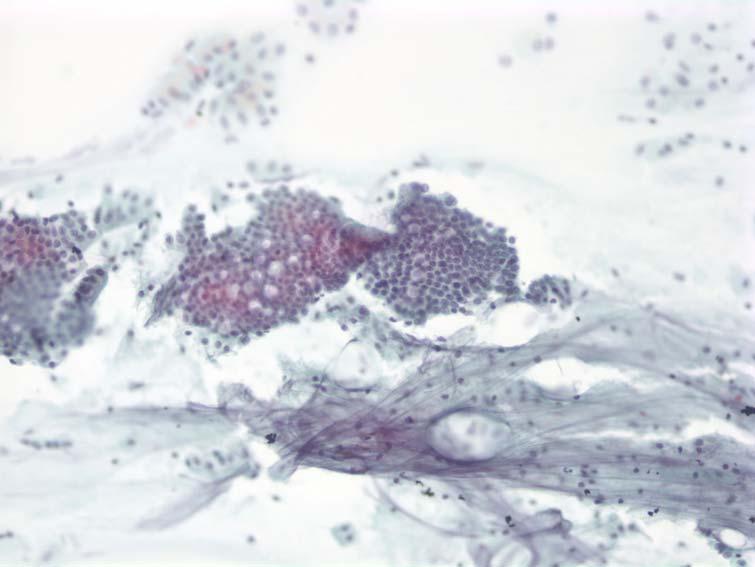
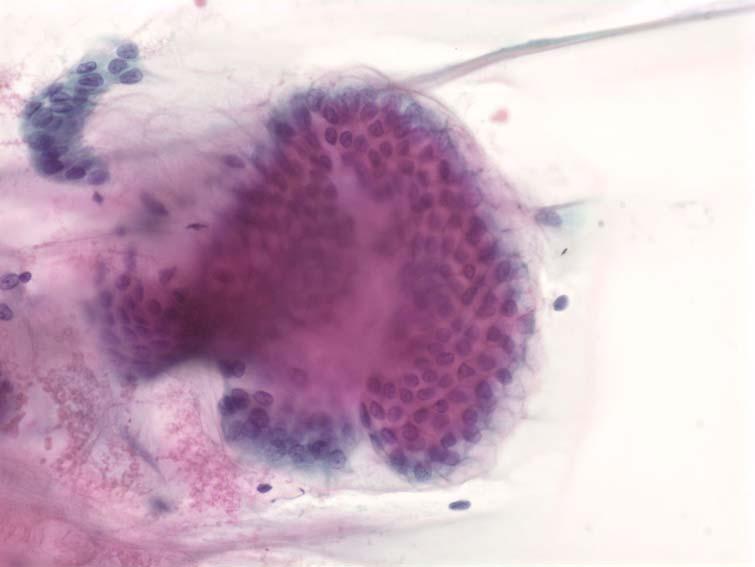
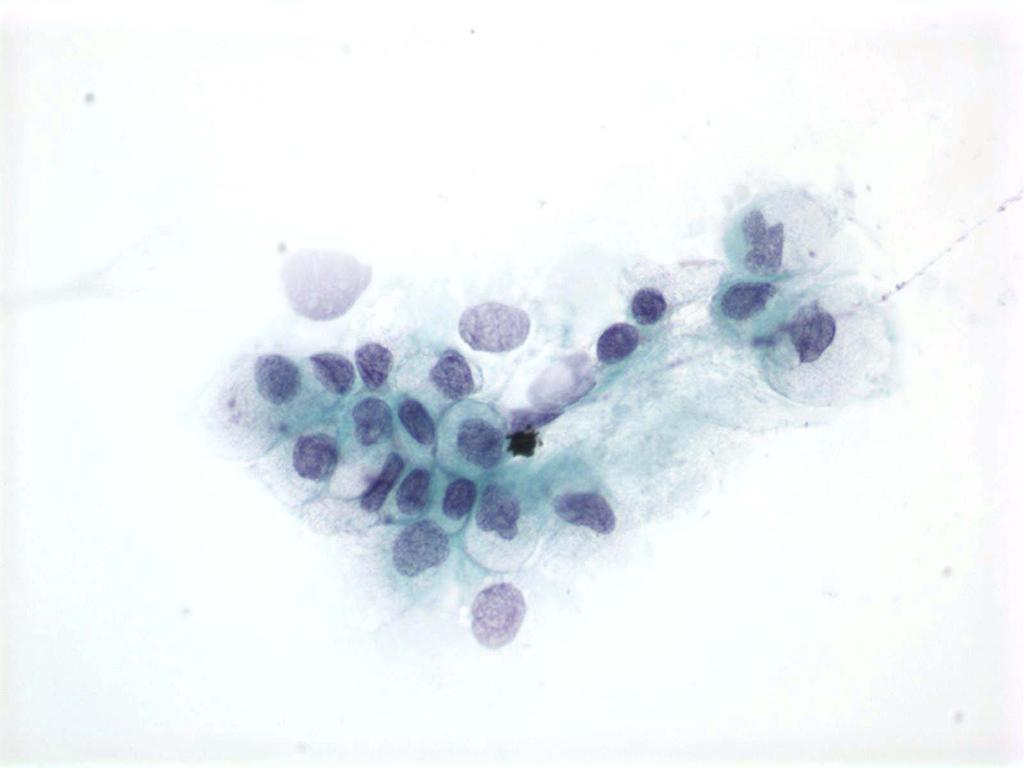
39 Case 3
40 Case 3
41 Case 3
42 Case 3: Cyst Fluid Analysis Amylase = 20 U/L CEA = 0.5 ng/ml.
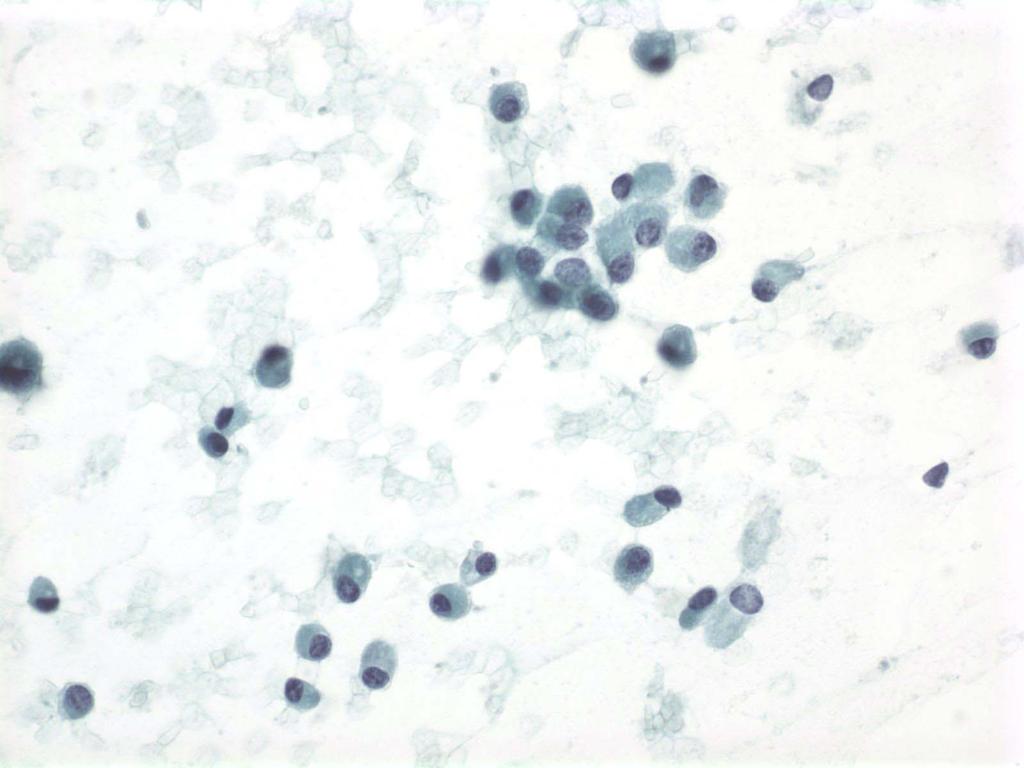
43 Case 3 Cytology Diagnosis: Serous cystadenoma Histology Diagnosis: Serous cystadenoma
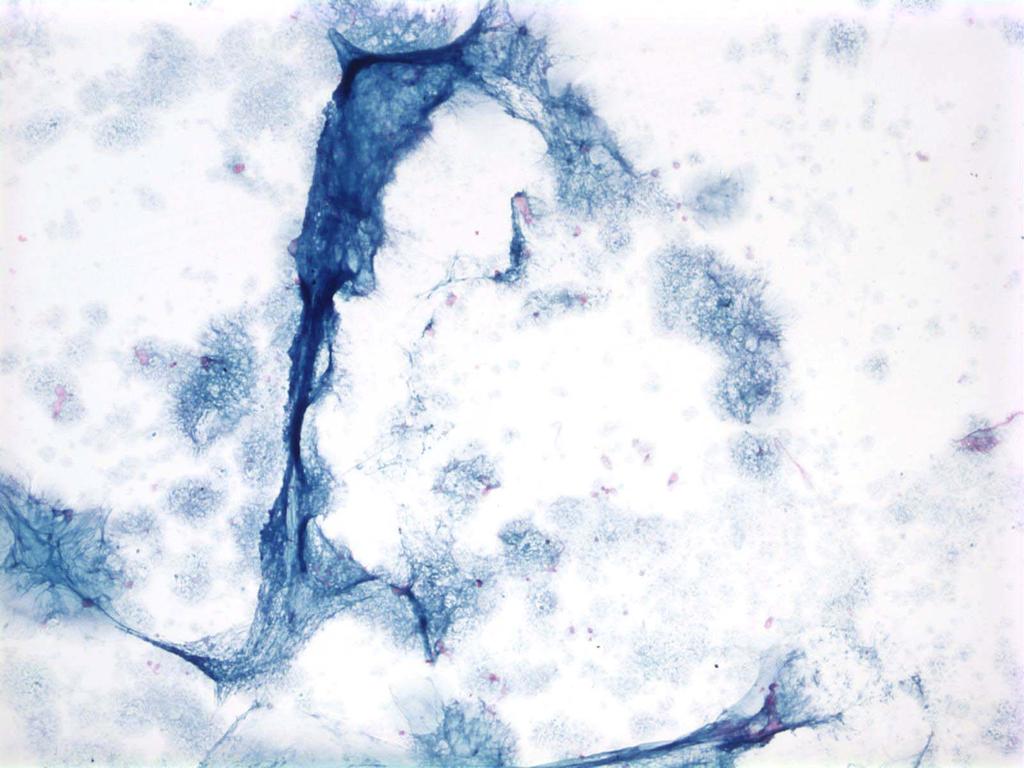
44 Case 4 A 63 year old woman with epigastric pain was found to have a large mass in the pancreatic head. Approximately 5cc of thin straw colored fluid was removed. A ThinPrep was made of an aliquot of fluid; cytospins were made for mucin stains and 1 cc of fluid was sent for cyst fluid analysis.
45 Case 4: EUS Report An 11 x 7x 6 cm well defined multicystic thinwalled cyst was noted in the pancreatic head. No solid component was noted. There was no evidence of invasion of surrounding structures.
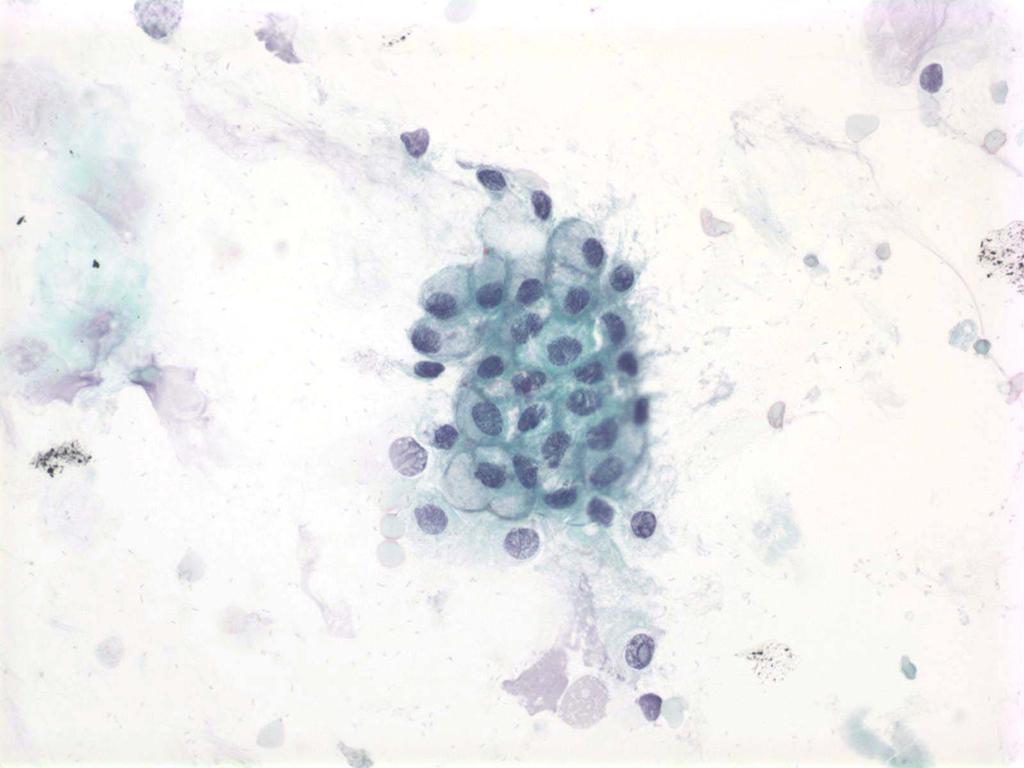
46 Case 4
47 Case 4
48 Case 4: Cyst Fluid Analysis Amylase = 83 U/L CEA = 3.0 ng/ml.
49 Case 4 Cytology Diagnosis: Nonmucinous cyst fluid with low CEA and amylase levels consistent with serous cystadenoma Histology Diagnosis: Oligocystic Serous cystadenoma


50 Serous Cystadenoma benign neoplasm in the head and tail of elderly men and women star-burst calcifications within a central scar diagnostic on imaging when present, but this is rarely present most tumors are microcystic with multiple, <2cm cysts, but can be unilocular due to specific variant or due to hemorrhagic degeneration, causing problems with imaging diagnosis
, well")


51 Serous Cystadenoma grossly large (10-12 cm), well circumscribed, multilobulated masses with fibrous septae histology: small cysts lined by glycogen-rich cuboidal epithelial cells


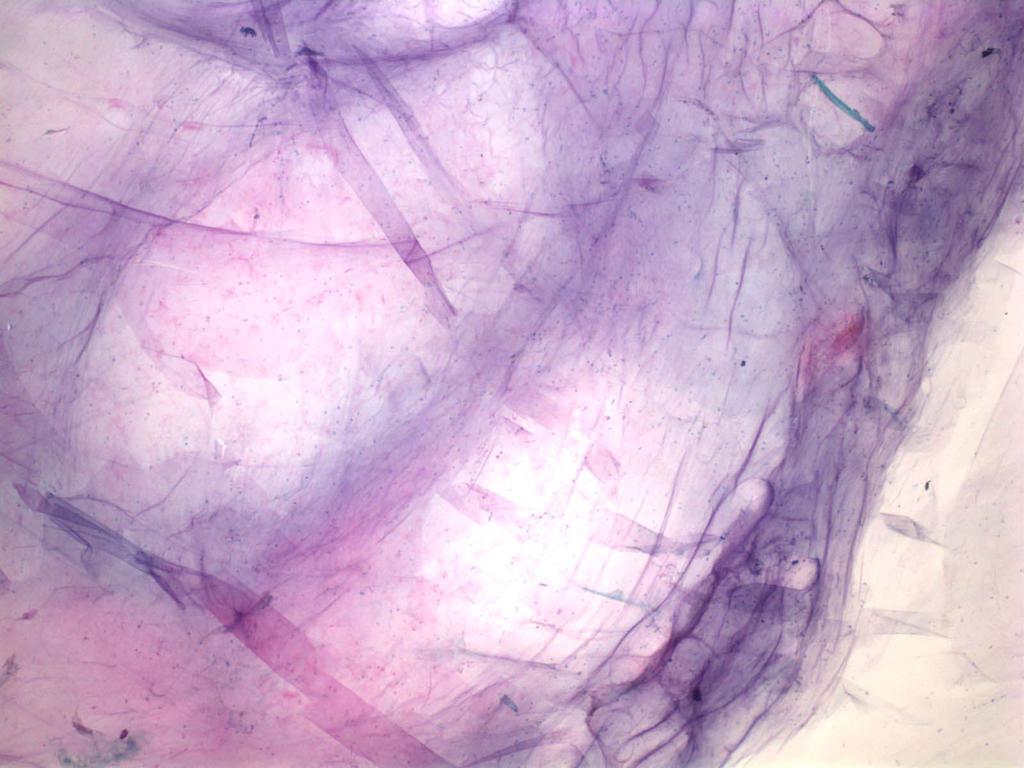
52 Serous Cystadenoma scant, watery, non-mucinous fluid scant cellularity clean, proteinaceous or bloody background monolayered sheets or small, flat clusters bland, uniform, round nuclei scant but visible non-mucinous cytoplasm

53 Surrogate Marker for SCA
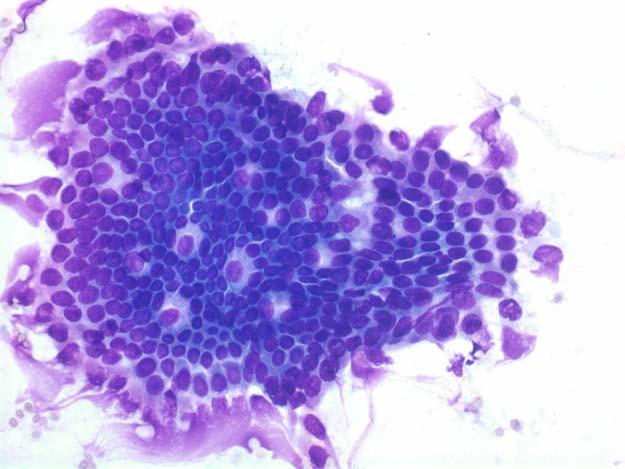
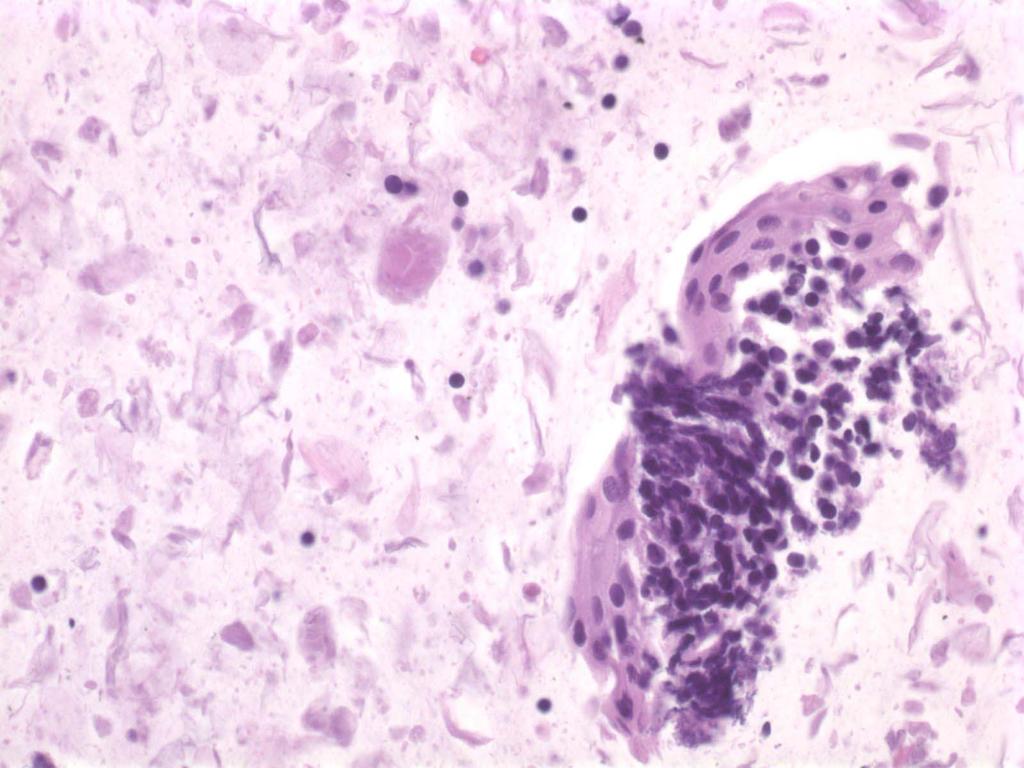
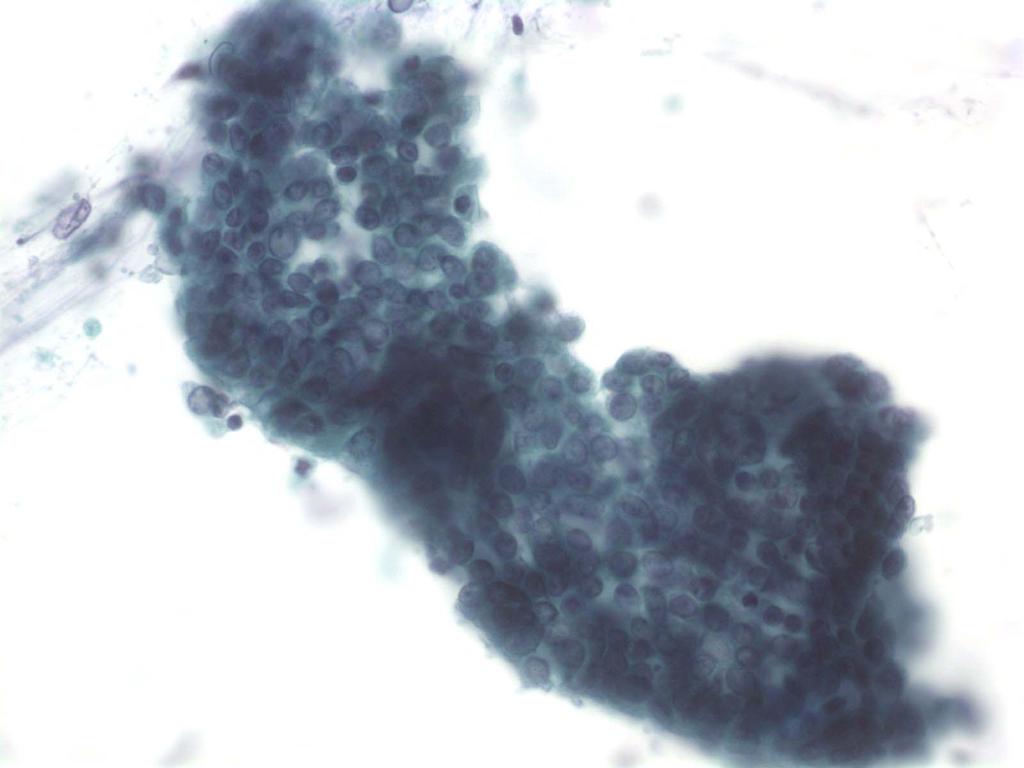
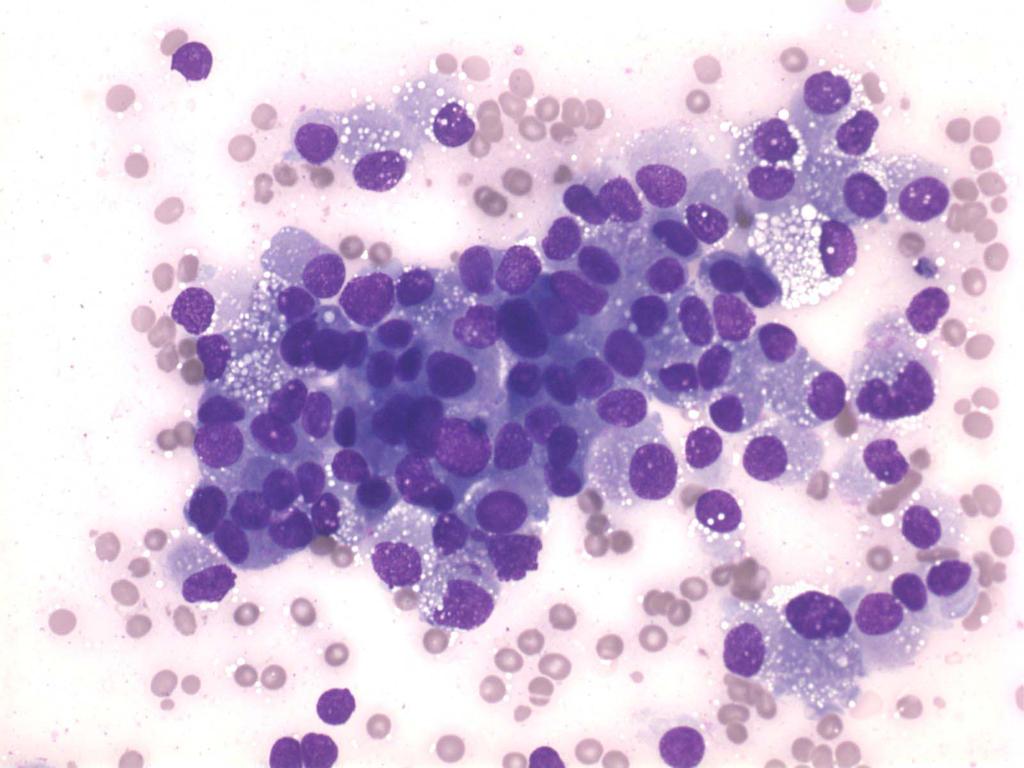
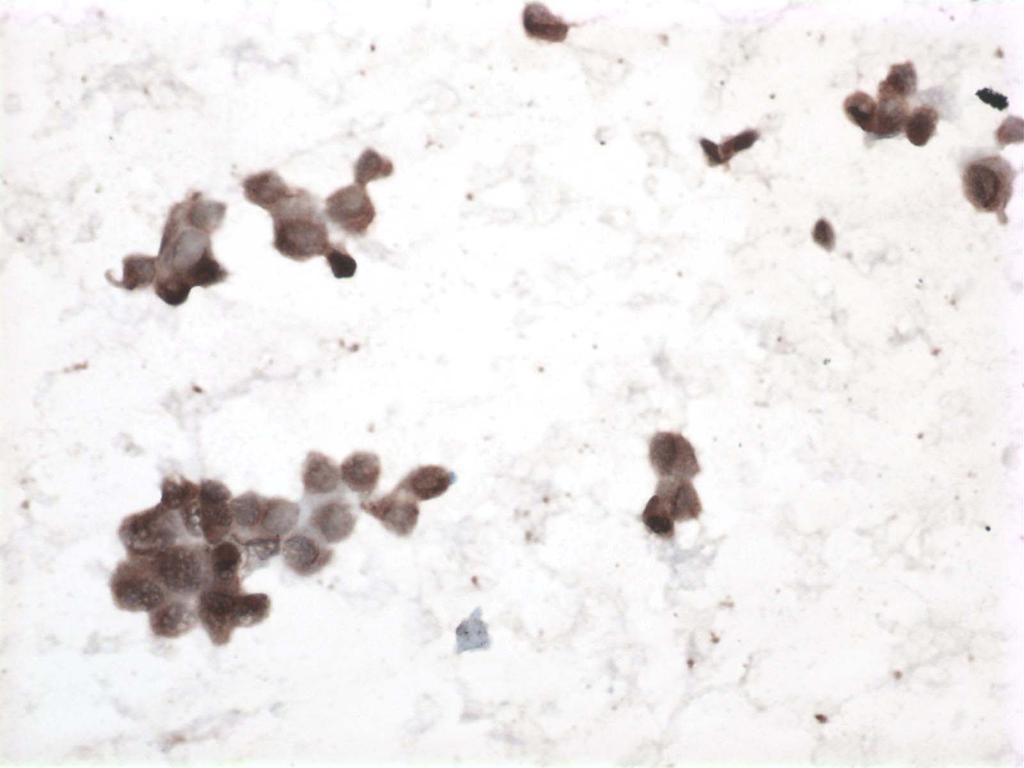
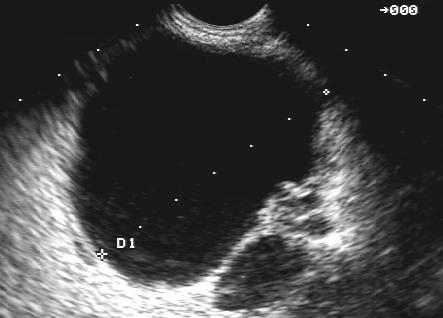
54 Case 5 A 53-year-old female with diabetes mellitus since the age of 39, developed some right-sided abdominal pain, which prompted a CT scan that demonstrated a mass in the pancreatic tail that showed growth on repeat CT scan and FNA was recommended.
55 Case 5: EUS Report A round mass was identified in the pancreatic tail. The mass was hypoechoic and markedly heterogenous. The mass measured 34 mm by 22 mm in maximal crosssectional diameter. The endosonographic borders were well-defined. The remainder of the pancreas appeared normal. The mass had the appearance of a pancreatic Solid-pseudopapillary tumor vs neuroendocrine tumor.
56 Case 5 55
57 Case 5 56
58 Case 5 57
59 Case 5 58
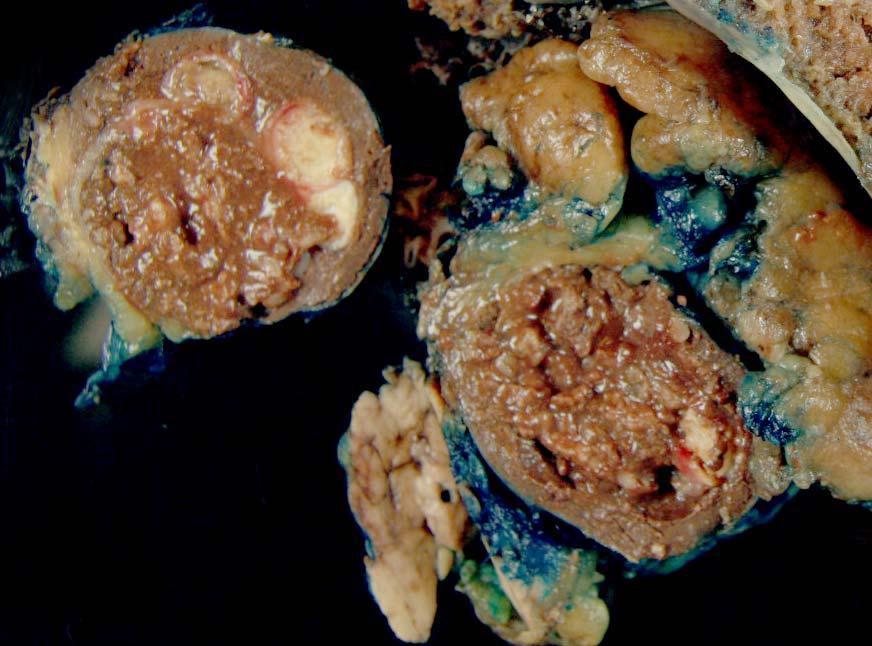
60 Lymphoepithelial Cyst Lymphoepithelial cysts are rare benign cysts lined by squamous epithelium with subepithelial non-neoplastic lymphoid tissue. Much more common in men with a male to female ratio of 4:1. It is a cyst of older adults with a mean age of 56 years. Are benign with no reported cases of malignant transformation. Are unilocular or multilocular and generally have thick appearing walls with internal debris that corresponds to keratinous debris that can make the cysts appear as a heterogeneous mass occur anywhere in the pancreas, and may even appear extra-pancreatic
61 Lymphoepithelial Cyst The differential diagnosis is with other squamous lined cysts: dermoid cyst of the pancreas splenic epidermoid cyst pseudocyst (due to the necrotic appearance of the keratinous debris)
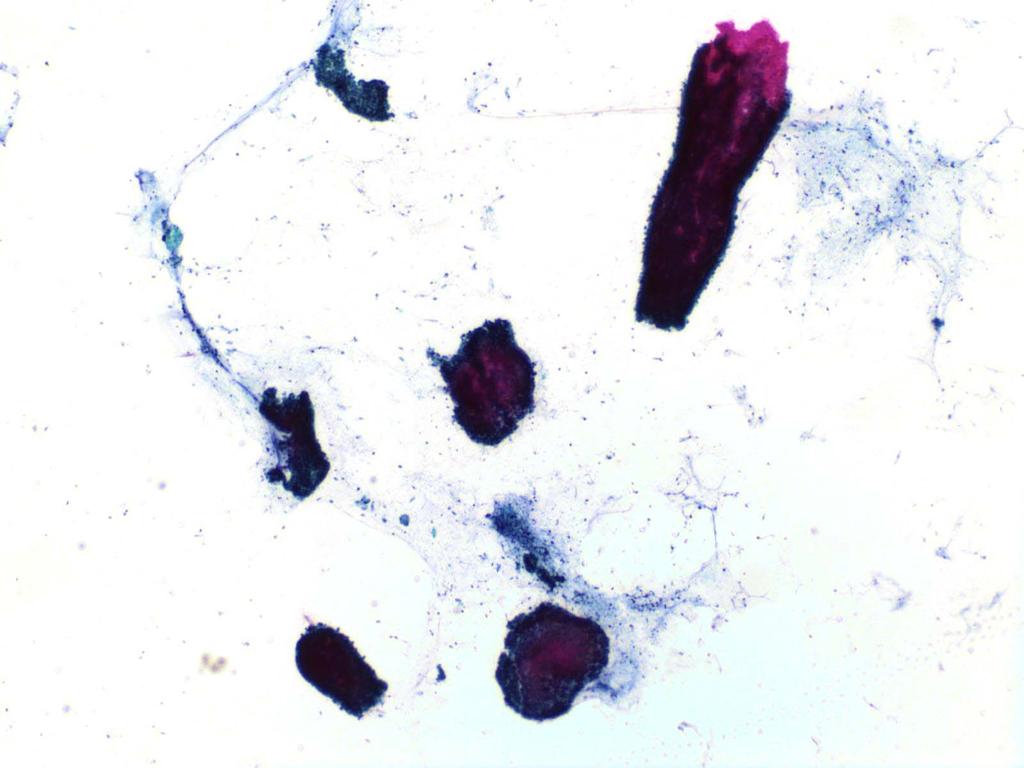
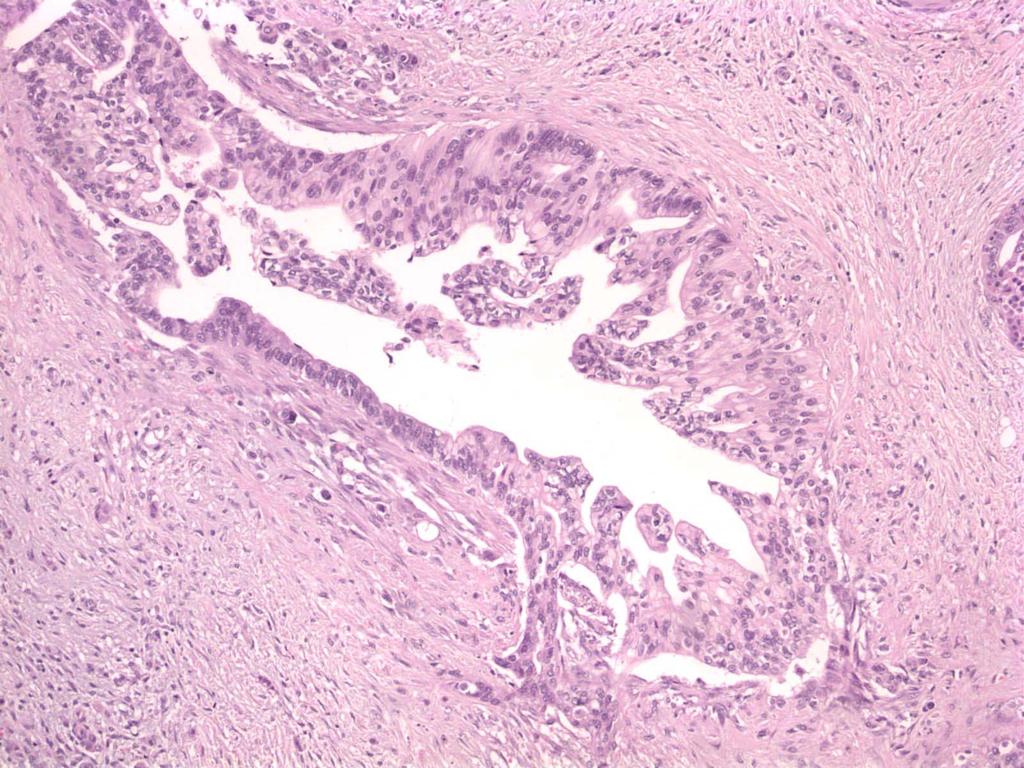
62 Case 6 A 45 year old male is found to have a cyst in the head of the pancreas on work-up of elevated LFT's from an insurance exam.
63 Case 6: EUS Report A hypoechoic lesion suggestive of a cyst/pseudocyst was identified in the pancreatic head. The lesion measured 30 mm by 30 mm in maximal cross-sectional diameter. There was a single compartment without septae. The outer wall of the lesion was thin. There was no associated mass. There was no internal debris within the fluid-filled cavity. A transduodenal FNA was performed. The amount of fluid collected was 1 cc. The fluid was clear, white and very thick. Direct smears were made; no fluid sent for cyst fluid analysis. The pancreatic duct was diffusely dilated to 8mm, thought to be due to obstruction. An aspirate of the duct was also performed and 3cc of clear, white and thin fluid was obtained.
64 Case 6 63
65 Case 6 64
66 Case 6 65
67 Case 6 66
68 Case 6 Cytology Diagnosis: Thick, viscous mucin consistent with neoplastic mucinous cyst. See note. Note: The quantity and quality of the mucin is consistent with the contents of a neoplastic mucinous cyst- IPMN or MCN. No high-grade atypia is identified. Acute inflammation and necrosis are also absent..
69 Case 6 Histology: Intraductal papillary mucinous neoplasm with moderate dysplasia, branch duct type.
70 Case 6 69
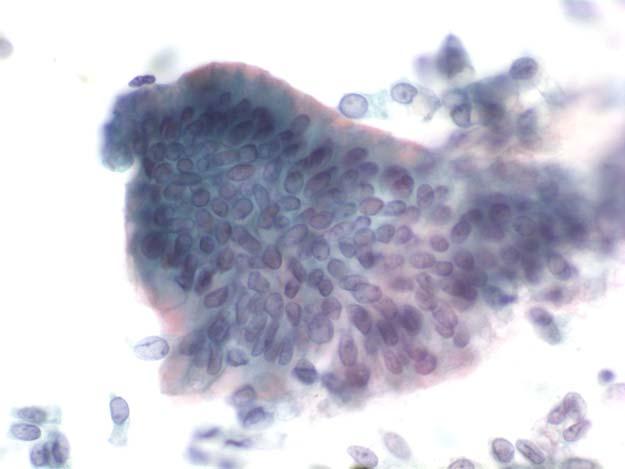
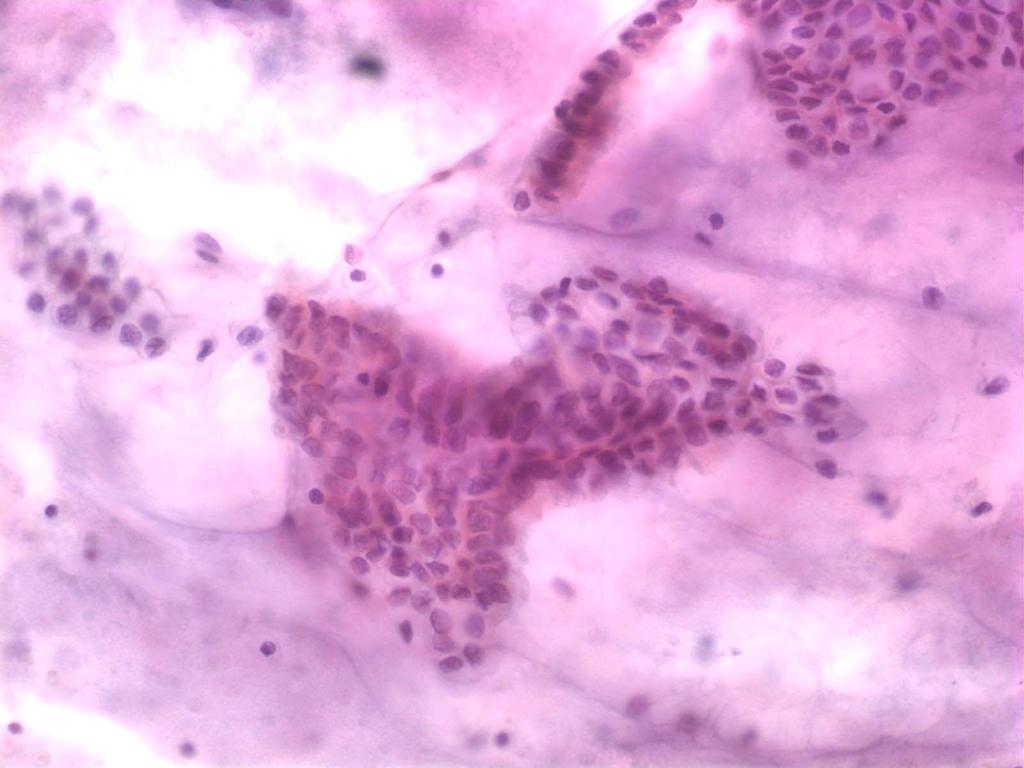
71 Case 7 An 84 year old female was found to have a cyst in the body/tail of the pancreas during evaluation of her Barrett s esophagus. An FNA was performed with cytospins and cyst fluid analysis.
72 Case 7: EUS Report A 20 mm anechoic cystic lesion was noted n the body-tail of the pancreas. There were no septations and the wall was thin. There was no associated mass lesion. FNA was performed for cytology with a 22 g needle. 2 ml of clear, mildly viscous fluid was aspirated. The CBD and pancreatic ducts were normal caliber.
73 Case 7: Cyst Fluid Analysis Amylase = 111,153 U/L CEA = 1361 ng/ml.
74 Case 7 73
75 Case 7 74
76 Case 7 75
77 Case 7 76
78 Case 7 77
79 Case 7 78
80 Case 7: Cytology Diagnosis Extracellular mucin and few benign low-grade appearing glandular cells consistent with the clinical and radiological impression of a branch duct intraductal papillary mucinous neoplasm. (See note). Note: An alcian blue confirms the gross appearance of the 2cc of clear, mildly viscous aspirated fluid as mucinous. A few bland appearing glandular cells with clear cytoplasm are also present. The elevated CEA also supports a mucinous cyst. No background inflammation or necrosis is present, and no high-grade atypical epithelial cells are noted.
81 Case 7: Follow-up Repeat EUS at one year shows a stable cyst without significant growth. FNA is negative. The patient is enrolled in an ethanol ablation study and no pancreatectomy is performed.
82 Case 8 A 74 year old male was found to have a pancreatic cyst in the body following resolution of a bout of pancreatitis that brought him to the ER. An FNA was done with cytospins made, cyst fluid analysis and molecular analysis performed.
83 Case 8: EUS Report The lesion measured 25 mm There was a single compartment without septae. The outer wall of the lesion was thick. There was internal debris within the fluid-filled cavity. There was a possible mural nodule. Transgastric FNA produced 5 cc of very viscous fluid.
84 Case 8 83
85 Case 8 84
86 Case 8 85
87 Case 8 86
88 Case 8 87
89 Case 8 88
90 Case 8: Cyst Fluid Analysis Amylase = 409 U/L CEA = 5165 ng/ml.
91 Case 8: Molecular Analysis KRAS mutation present
92 Case 8: Cytology Diagnosis Mucinous cyst with high-grade atypia suspicious for carcinoma consistent with IPMN. See note. Note: Several papillary fragments of atypical epithelial cells are present associated with extracellular mucin (confirmed with mucicarmine and alcian blue stains). Molecular analysis demonstrates a KRAS mutation. CEA is markedly elevated at >5000 ng/ml and amylase is 409 U/L. These findings from a cyst in the pancreatic body from a male support the above interpretation.
93 Case 8: Histology IPMN with high-grade dysplasia, branch duct type.
94 Case 93 8
95 Case 9 A 62 year old female is worked up for acute onset of abdominal pain. Ultrasound shows a markedly dilated pancreatic duct with sharp tapering in the pancreatic head where a 2 cm round cystic mass is identified. EUS with FNA is recommended.
96 Case 9: EUS Report A round mass is identified in the pancreatic head. The mass is hypoechoic, calcified and cystic. The mass measures 16 mm by 20 mm in maximal cross-sectional diameter. The endosonographic borders are well-defined. An intact interface is seen between the mass at the adjacent structures suggesting a lack of invasion. Diagnostic needle aspiration for fluid is performed into the cystic component of the mass and into the mass itself. The amount of fluid collected is 4 ml. The fluid is brown-yellow. The fluid is sent for molecular analysis. The pancreatic parenchyma in the body and tail is diffusely hypoechoic and lobular likely secondary to ductal obstruction. The pancreatic duct measures 2.3 mm. No lymphadenopathy is detected.
97 Case 9: Molecular Analysis KRAS mutation present
98 Case 979
99 Case 989
100 Case 9 99

101 Case 9 100
102 Case 9 101

103 Case 9 102

104 Case 9: solid component 103
105 Case 9: Cytology Diagnosis Adenocarcinoma consistent with invasive IPMN.
106 105
107 106
108 Case 8: Histology Intraductal papillary mucinous neoplasm, branch duct type, with invasive tubular carcinoma
109 Case 10 A 64 year old woman being worked up for esophageal stricture is noted to have cysts in her pancreas along with a cystic mass in the uncinate. An EUS-FNA is scheduled.
110 Case 10: EUS Report The body and tail of the pancreas is very atrophic. In midbody, there is a 3 compartment cyst measuring about 8 mm in diameter. The pancreatic duct is not clearly seen in the body. In the head, CBD measures between 3-6 mm in diameter. The pancreatic duct is about 3.7 mm in diameter. In the uncinate process, there is a fairly well circumscribed heterogenous mass measuring about 30 X 20 mm rounded. At one edge there is some cystic component but it appears mostly solid. Aspirates are productive of bloody tissue, no cyst fluid. Direct smears are made. Slides are sent to me in consultation.
111
112
113
114
115 Case 10: Cytology Diagnosis Cystic pancreatic neuroendocrine tumor
116 Mucinous Cysts of the Premalignant Lesions PanIN-3 Pancreas WHO Classification 2010 Intraductal papillary mucinous neoplasm with low to intermediate grade dysplasia Intraductal papillary mucinous neoplasm with high grade dysplasia Mucinous cystic neoplasm with low to intermediate grade dysplasia Mucinous cystic neoplasm with high grade dysplasia Malignant Intraductal papillary mucinous neoplasm with invasive carcinoma Mucinous cystic neoplasm with invasive carcinoma
117 Changes in Nomenclature Adenoma (WHO 2000) Low grade dysplasia (AFIP and WHO 2010) Borderline carcinoma (WHO 2000) Moderate dysplasia (AFIP) Intermediate grade dysplasia (WHO 2010) Carcinoma in-situ (WHO 2000) High grade dysplasia/cis (AFIP) High Grade dysplasia/premalignant (WHO 2010) Mucinous Cystadenocarcinoma (WHO 2000) MCN with invasive carcinoma (AFIP and WHO 2010) IPMN carcinoma (WHO 2000) IPMN with invasive carcinoma (AFIP and WHO 2010)
118 Helpful Features to Distinguish Mucinous Cystic Neoplasms from Intraductal Papillary Mucinous Neoplasms Relationship to larger pancreatic ducts MCN None IPMN Arise within larger ducts Cellular stoma Present Absent Cystic configuration Single multilocular Multiple separate Sex ration (M:F) 1 : : 1 Mean Age Location Tail Head > Tail Papilla formation Focal Extensive Papilla types Gastric foveolar, pancreatobiliary Gastric foveolar intestinal, pancreatobiliary Peripheral Capsule Present Absent 4 th Series Fascicle on Tumors of the Pancreas.

119 International Consensus Guidelines for Management of IPMN and MCN (Tanaka, et.al. Pancreatology. 2006; 6:17)
120 The International Consensus Guidelines 2012 for the Management of IPMN and MCN of the Pancreas Tanaka M, Fernandez del-castillo C, Adsay V, Chari S, Falconi M, Jang J-Y, Levy P, Pitman MB, Schmidt MC, Shimizu M, Wolfgang CL, Yamaguchi K, Yamao K May-Jun;12(3): Epub 2012 Apr 16. High Risk Stigmata Surgery if clinically feasible Obstructive jaundice in a patient with a cyst in the pancreatic head Enhancing solid component of the cyst Main pancreatic duct dilatation 10mm Worrisome Features Cyst 3cm Thickened/enhancing cyst walls Main duct 5-9mm Non-enhancing mural nodule EUS-FNA Abrupt change in MPD size with distal pancreatic atrophy EUS-FNA Susp/Pos cytology Surgery



")



121 Mucinous Cystic Neoplasm Predominantly in middle aged females (F:M=20:1) Mostly in the pancreatic body and tail (90%) Cysts do not communicate with the pancreatic ductal system; thick walled, thin or thick septa 20% have a rim of peripheral calcification on CT






122 Mucinous Cystic Neoplasm Lined by mucinous, generally non-papillary epithelium, but can be focally papillary Associated with a subepithelial ovarian-like stroma (not seen on cytology) Atypia may be very heterogeneous






123 MCN with invasive carcinoma Invasive component can be very focal Diagnosis cannot be made from FNA of cyst alone Invasion suggested by combination of cytology and EUS features



124 Intraductal Papillary Mucinous Neoplasm (IPMN) Main duct IPMN Branch duct IPMN Combined IPMN






125 Intraductal Papillary Mucinous Neoplasm (IPMN) Arise in older patients, M>F Generally in the pancreatic head, although can extend into the tail; single or multiple cysts Cysts do communicate with the pancreatic ductal system, but this may not be visible on EUS






126 Intraductal Papillary Mucinous Neoplasm Mostly papillary mucinous epithelium with variable and heterogenous atypia No association with ovarian-like stroma under the epithelium

")
127 Epithelium of Neoplastic Mucinous Cysts (MCN or IPMN) LGD (adenoma) Intermediate/Moderate dysplasia (Borderline carcinoma) HGD (CIS)
")
128 Benign/Low Grade Glandular Epithelium High Grade Atypical Epithelial Cells in Pancreatic Mucinous Cysts are a More Accurate Predictor of Malignancy than Positive Cytology Martha Bishop Pitman M.D, et.al. (in press, Cancer Cytopath)
")
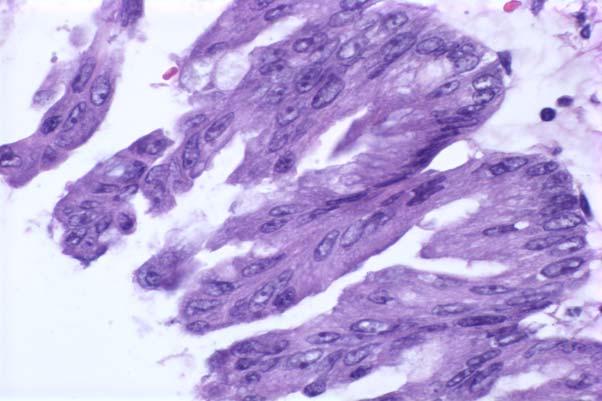
129 High Grade Atypical Glandular Epithelium High Grade Atypical Epithelial Cells in Pancreatic Mucinous Cysts are a More Accurate Predictor of Malignancy than Positive Cytology Martha Bishop Pitman M.D, et.al. (in press, Cancer Cytopath)
130 Take Home Points Thick colloid-like mucin even if acellular is sufficient to diagnose a neoplastic mucinous cyst Cytology may under-estimate the final histology of mucinous cysts Mural nodule and dilated MPD are high-risk imaging features Cyst fluid without a high amylase is very unlikely to be a pseudocyst CEA > 200 ng/ml supports mucinous cyst High amylase should be present in a pseudocyst, low in SCA and LEC and does not distinguish IPMN and MCN. Mucin stains help to highlight thin background mucin KRAS mutations support a mucinous cyst but not necessarily malignancy. Typically solid masses, especially PanNETs, can undergo cystic degeneration and mimic a primary pancreatic cyst
131 Thank you for participating! Please complete the course evaluation before you leave.
Case 1. Case 1: EUS Report 5/1/2017. Interesting Cases of Pancreatic Masses
 Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Patient History. A 58 year old man presents with a 16 mm cyst in the pancreatic tail. The cyst is unilocular with a thick wall and no mural nodule.
 Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget
 Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
Pancreatic Cysts. Darius C. Desai, MD FACS St. Luke s University Health Network
 Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
Outline. Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines
 Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines") Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification
Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification
An Approach to Pancreatic Cysts. Introduction
 An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
Matthew McCollough, M.D. April 9, 2009 University of Louisville
 Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines
 Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Pancreatico-biliary cytology: a practical approach to diagnosis. Corina Cotoi
 Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Pancreatic Cystic Lesions 원자력병원
 Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts
 ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
Advances in Pancreatic. Cytology. Martha B. Pitman, MD. Disclosure of Relevant Financial Relationships
 Advances in Pancreatic Cytology Martha B. Pitman, MD Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Advances in Pancreatic Cytology Martha B. Pitman, MD Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS
 ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS Prof. Fernando Schmitt Medical Faculty of Porto University, Porto, Portugal IPATIMUP General Secretary of the International Academy of Cytology
ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS Prof. Fernando Schmitt Medical Faculty of Porto University, Porto, Portugal IPATIMUP General Secretary of the International Academy of Cytology
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT
 CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
Cystic Pancreatic Lesions: Approach to Diagnosis
 Cystic Pancreatic Lesions: Approach to Diagnosis Poster No.: R-0130 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: A. AGARWAL, R. M. Mendelson; Perth/AU Keywords: Cysts, Biopsy, Endoscopy,
Cystic Pancreatic Lesions: Approach to Diagnosis Poster No.: R-0130 Congress: RANZCR-AOCR 2012 Type: Educational Exhibit Authors: A. AGARWAL, R. M. Mendelson; Perth/AU Keywords: Cysts, Biopsy, Endoscopy,
Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases
 Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital
 Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
Standardization of Nomenclature
 Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts
 Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts Authors Alexander Lee 1, Vivek Kadiyala 2,LindaS.Lee 3 Institutions 1 Texas Digestive Disease Consultants,
Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts Authors Alexander Lee 1, Vivek Kadiyala 2,LindaS.Lee 3 Institutions 1 Texas Digestive Disease Consultants,
Management A Guideline Based Approach to the Incidental Pancreatic Cysts. Common Cystic Pancreatic Neoplasms.
 Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
Endoscopic Ultrasound-guided FNA Cytology of the Pancreas
 Endoscopic Ultrasound-guided FNA Cytology of the Pancreas 67 th Annual California Society of Pathologists 2014 Laura Tabatabai, MD Professor of Pathology University of California, San Francisco Overview
Endoscopic Ultrasound-guided FNA Cytology of the Pancreas 67 th Annual California Society of Pathologists 2014 Laura Tabatabai, MD Professor of Pathology University of California, San Francisco Overview
Pancreatic Cysts. Pancreatic Cysts. Multidisciplinary and Multimodal Approach To the Pre-Operative Diagnosis of Pancreatic Cysts
 Multidisciplinary and Multimodal Approach To the Pre-Operative Diagnosis of Pancreatic Cysts Martha Bishop Pitman, M.D. Director of Cytopathology Massachusetts General Hospital Professor of Pathology Harvard
Multidisciplinary and Multimodal Approach To the Pre-Operative Diagnosis of Pancreatic Cysts Martha Bishop Pitman, M.D. Director of Cytopathology Massachusetts General Hospital Professor of Pathology Harvard
Citation American Journal of Surgery, 196(5)
") NAOSITE: Nagasaki University's Ac Title Author(s) Multifocal branch-duct pancreatic i neoplasms Tajima, Yoshitsugu; Kuroki, Tamotsu Amane; Adachi, Tomohiko; Mishima, T Kanematsu, Takashi Citation American
NAOSITE: Nagasaki University's Ac Title Author(s) Multifocal branch-duct pancreatic i neoplasms Tajima, Yoshitsugu; Kuroki, Tamotsu Amane; Adachi, Tomohiko; Mishima, T Kanematsu, Takashi Citation American
State of the Art Symposium
 State of the Art Symposium Syed Z. Ali, MD There is no disclosure necessary Martha B. Pitman, MD There is no disclosure necessary Lester Layfield, MD There is no disclosure necessary Joseph Herman, MD
State of the Art Symposium Syed Z. Ali, MD There is no disclosure necessary Martha B. Pitman, MD There is no disclosure necessary Lester Layfield, MD There is no disclosure necessary Joseph Herman, MD
Objectives. Pancreatic Cysts. Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses
 Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses Michelle D. Reid, MD, MSc Associate 1/24/15 Professor Director of Cytology - EUHM Michelle D Reid MD, MS Emory
Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses Michelle D. Reid, MD, MSc Associate 1/24/15 Professor Director of Cytology - EUHM Michelle D Reid MD, MS Emory
Types of IPMN. Pancreas Cysts: An Incidental Finding or Harbinger of Malignancy. Cysts: Early Neoplasia. Mucinous Cystic Lesions. EUS-guided FNA EUS
 Pancreas Cysts: An Incidental Finding or Harbinger of Malignancy EUS-guided FNA William R. Brugge,, MD, FACG Professor of Medicine Harvard Medical School Director, GI Endoscopy Unit Massachusetts General
Pancreas Cysts: An Incidental Finding or Harbinger of Malignancy EUS-guided FNA William R. Brugge,, MD, FACG Professor of Medicine Harvard Medical School Director, GI Endoscopy Unit Massachusetts General
Conflicts of Interest
 Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Cytopathology Study Day 16 April RCPath - BAC. Digital cytology: EUS FNA pancreas and head and neck
 Cytopathology Study Day 16 April 2017 Guy s Hospital London RCPath - BAC Digital cytology: EUS FNA pancreas and head and neck R. Dina MD, FIAC, FRCPath Consultant Cyto/Histopathologist Hon Sen Lecturer
Cytopathology Study Day 16 April 2017 Guy s Hospital London RCPath - BAC Digital cytology: EUS FNA pancreas and head and neck R. Dina MD, FIAC, FRCPath Consultant Cyto/Histopathologist Hon Sen Lecturer
X-ray Corner. Imaging of The Pancreas. Pantongrag-Brown L
 X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
DIAGNOSTIC CHALLENGES Pancreas FNAB. Dr. M. Weir Oct 2017
 DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS
 Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS Brooklyn VAMC September 21 st GI Grand Rounds - What is it? - Clinical entity that has emerged from
Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS Brooklyn VAMC September 21 st GI Grand Rounds - What is it? - Clinical entity that has emerged from
The Role of Molecular Analysis in the Diagnosis and Surveillance of Pancreatic Cystic Neoplasms
 JOP. J Pancreas (Online) 20 Mar 20; (2):-9. RESEARCH ARTICLE The Role of Molecular Analysis in the Diagnosis and Surveillance of Pancreatic Cystic Neoplasms Megan Winner, Amrita Sethi 2, John M Poneros
JOP. J Pancreas (Online) 20 Mar 20; (2):-9. RESEARCH ARTICLE The Role of Molecular Analysis in the Diagnosis and Surveillance of Pancreatic Cystic Neoplasms Megan Winner, Amrita Sethi 2, John M Poneros
Unusual Pancreatic Neoplasms RTC 2/11/2011
 Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Cystic Lesions of the Pancreas
 Residents Section Pattern of the Month w668 04.29.11 Khan et al. Residents Section Pattern of the Month Residents inradiology tif Khan 1 Faisal Khosa Ronald L. Eisenberg Khan, Khosa F, Eisenberg RL Keywords:
Residents Section Pattern of the Month w668 04.29.11 Khan et al. Residents Section Pattern of the Month Residents inradiology tif Khan 1 Faisal Khosa Ronald L. Eisenberg Khan, Khosa F, Eisenberg RL Keywords:
Chief Complaint. Retroperitoneal cystic mass incidentally found at health examination center.
 Personal Information Age: 34 y/o Sex: female Past history: major systemic medical history(-) surgical history(-), family history(-) Denied food or drug allergy Chief Complaint Retroperitoneal cystic mass
Personal Information Age: 34 y/o Sex: female Past history: major systemic medical history(-) surgical history(-), family history(-) Denied food or drug allergy Chief Complaint Retroperitoneal cystic mass
Intraductal Papillary Mucinous Neoplasm of Pancreas
 Review Article Intraductal Papillary Mucinous Neoplasm of Pancreas Norman Oneil Machado, Hani al Qadhi, Khalifa al Wahibi Department of Surgery, Sultan Qaboos University Hospital, Muscat, Oman Abstract
Review Article Intraductal Papillary Mucinous Neoplasm of Pancreas Norman Oneil Machado, Hani al Qadhi, Khalifa al Wahibi Department of Surgery, Sultan Qaboos University Hospital, Muscat, Oman Abstract
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Pancreatology 12 (2012) 183e197. Contents lists available at SciVerse ScienceDirect. Pancreatology. journal homepage:
 183e197. Contents lists available at SciVerse ScienceDirect. Pancreatology. journal homepage:") Pancreatology 12 (2012) 183e197 Contents lists available at SciVerse ScienceDirect Pancreatology journal homepage: www.elsevier.com/locate/pan Review article International consensus guidelines 2012 for
Pancreatology 12 (2012) 183e197 Contents lists available at SciVerse ScienceDirect Pancreatology journal homepage: www.elsevier.com/locate/pan Review article International consensus guidelines 2012 for
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Diagnosis and management of cystic lesions of the pancreas
 Review Article Diagnosis and management of cystic lesions of the pancreas William R. Brugge Massachusetts General Hospital, Boston, USA Correspondence to: William R. Brugge, MD. Massachusetts General Hospital,
Review Article Diagnosis and management of cystic lesions of the pancreas William R. Brugge Massachusetts General Hospital, Boston, USA Correspondence to: William R. Brugge, MD. Massachusetts General Hospital,
EUS-FNAB of GI Tract: Specimen Handling and Triage
 EUS-FNAB of GI Tract: Specimen Handling and Triage Amy Ly, M.D. Director, Fine Needle Aspiration Service Massachusetts General Hospital Assistant Professor of Pathology Harvard Medical School Boston, MA
EUS-FNAB of GI Tract: Specimen Handling and Triage Amy Ly, M.D. Director, Fine Needle Aspiration Service Massachusetts General Hospital Assistant Professor of Pathology Harvard Medical School Boston, MA
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Pancreatic Cystic Neoplasms: Guidelines and beyond
 Pancreatic Cystic Neoplasms: Guidelines and beyond Kenneth J. Chang, MD, FACG, FASGE Executive Director, Comprehensive Digestive Disease Center Professor and Chief, Gastroenterology Vincent & Anna Kong
Pancreatic Cystic Neoplasms: Guidelines and beyond Kenneth J. Chang, MD, FACG, FASGE Executive Director, Comprehensive Digestive Disease Center Professor and Chief, Gastroenterology Vincent & Anna Kong
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Cystic lesions of the pancreas
 REVIEW ARTICLE Annals of Gastroenterology (2016) 29, 155-161 Cystic lesions of the pancreas Ioannis Karoumpalis a, Dimitrios K. Christodoulou b General Hospital of Athens G. Gennimatas, Athens; University
REVIEW ARTICLE Annals of Gastroenterology (2016) 29, 155-161 Cystic lesions of the pancreas Ioannis Karoumpalis a, Dimitrios K. Christodoulou b General Hospital of Athens G. Gennimatas, Athens; University
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
Pancreatic neoplasms associated with significant amounts of extracellular. Fine-Needle Aspiration Cytology of Mucinous Tumors of the Pancreas CANCER
 92 CANCER CYTOPATHOLOGY Fine-Needle Aspiration Cytology of Tumors of the Pancreas Monica Recine, M.D. 1 Madhukar Kaw, M.D. 2 Douglas B. Evans, M.D. 3 Savitri Krishnamurthy, M.D. 1 1 Division of Pathology
92 CANCER CYTOPATHOLOGY Fine-Needle Aspiration Cytology of Tumors of the Pancreas Monica Recine, M.D. 1 Madhukar Kaw, M.D. 2 Douglas B. Evans, M.D. 3 Savitri Krishnamurthy, M.D. 1 1 Division of Pathology
Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA. Leena Krogerus Helsinki, FINLAND
 Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology PSC- is a pre-neoplastc condition in youg individulas, the cure of which is
Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology PSC- is a pre-neoplastc condition in youg individulas, the cure of which is
Original article. Introduction!
 382 Original article Peritoneal seeding in intraductal papillary mucinous neoplasm of the pancreas patients who underwent endoscopic ultrasound-guided fine-needle aspiration: The PIPE Study Authors Won
382 Original article Peritoneal seeding in intraductal papillary mucinous neoplasm of the pancreas patients who underwent endoscopic ultrasound-guided fine-needle aspiration: The PIPE Study Authors Won
Cystic pancreatic lesions A proposal for a network approach. Chris Briggs Consultant HPB Surgeon Peninsula HPB Unit Derriford Hospital, Plymouth
 Cystic pancreatic lesions A proposal for a network approach Chris Briggs Consultant HPB Surgeon Peninsula HPB Unit Derriford Hospital, Plymouth Aims Brief overview of cystic pancreatic lesions International
Cystic pancreatic lesions A proposal for a network approach Chris Briggs Consultant HPB Surgeon Peninsula HPB Unit Derriford Hospital, Plymouth Aims Brief overview of cystic pancreatic lesions International
Cystic Disease of the Liver Work Up and Management. Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center
 Cystic Disease of the Liver Work Up and Management Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center The Case 73F presents to clinic after diagnostic laparoscopy at OSH. Known liver mass for
Cystic Disease of the Liver Work Up and Management Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center The Case 73F presents to clinic after diagnostic laparoscopy at OSH. Known liver mass for
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Morphologic features in cystic lesions of pancreas-a retrospective analysis
 International Journal of Advances in Medicine Cicy PJ et al. Int J Adv Med. 2018 Feb;5(1):192-196 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20180083
International Journal of Advances in Medicine Cicy PJ et al. Int J Adv Med. 2018 Feb;5(1):192-196 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20180083
Genetics of Pancreatic Cancer. October 6, If you experience technical difficulty during the presentation:
 Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Intro to Gallbladder & Pancreas Pathology
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
Role of Imaging Methods in Diagnosis of Acute Pancreatitis. Válek V. Radiologická klinika, FN Brno a LF MU v Brně
 Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
The Frozen Section: Diagnostic Challenges and Pitfalls
 The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
Solid pseudopapillary tumour of the pancreas: Report of five cases
 ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Solid pseudopapillary tumour of the pancreas: Report of five cases P Srilatha, V Manna, P Kanthilatha Citation P Srilatha, V Manna, P Kanthilatha..
ISPUB.COM The Internet Journal of Pathology Volume 8 Number 2 Solid pseudopapillary tumour of the pancreas: Report of five cases P Srilatha, V Manna, P Kanthilatha Citation P Srilatha, V Manna, P Kanthilatha..
Biliary cytolgy and pancreatic endoscopic ultrasound-guided. Helsinki, FINLAND
 Biliary cytolgy and pancreatic endoscopic ultrasound-guided d FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology Obstructions PSC, a premalignant condition, the cure of which is transplantation
Biliary cytolgy and pancreatic endoscopic ultrasound-guided d FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology Obstructions PSC, a premalignant condition, the cure of which is transplantation
Name : 黃 XX Age : 52 Sex : 女 Occupation : 廚房阿姨 Marital status : 已婚
 Name : 黃 XX Age : 52 Sex : 女 Occupation : 廚房阿姨 Marital status : 已婚 Chief Complaint Mild postprandial fullness for 2 months Present Illness This 52 year-old female suffered from intermittent post-prandial
Name : 黃 XX Age : 52 Sex : 女 Occupation : 廚房阿姨 Marital status : 已婚 Chief Complaint Mild postprandial fullness for 2 months Present Illness This 52 year-old female suffered from intermittent post-prandial
Kenneth D. Chi, MD Medical Director GI Lab Advocate Lutheran General Hospital
 Kenneth D. Chi, MD Medical Director GI Lab Advocate Lutheran General Hospital Advances in Digestive Health for the Primary Care Physician Symposium May 2, 2015 None Case Presentation Types of Pancreatic
Kenneth D. Chi, MD Medical Director GI Lab Advocate Lutheran General Hospital Advances in Digestive Health for the Primary Care Physician Symposium May 2, 2015 None Case Presentation Types of Pancreatic
Research Article The Changing Spectrum of Surgically Treated Cystic Neoplasms of the Pancreas
 HPB Surgery Volume 2015, Article ID 791704, 7 pages http://dx.doi.org/10.1155/2015/791704 Research Article The Changing Spectrum of Surgically Treated Cystic Neoplasms of the Pancreas Jennifer K. Plichta,
HPB Surgery Volume 2015, Article ID 791704, 7 pages http://dx.doi.org/10.1155/2015/791704 Research Article The Changing Spectrum of Surgically Treated Cystic Neoplasms of the Pancreas Jennifer K. Plichta,
Biliary Tract Neoplasia: A Cyto-histologic Review. Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital
 Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
EUS-guided FNAB. Differential Diagnosis 5/1/2017. EUS-FNA of Solid and Cystic Lesions:
 EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
Surgical outcomes of multifocal branch duct intraductal papillary mucinous neoplasms of pancreas
 Korean J Hepatobiliary Pancreat Surg 2014;18:152-158 http://dx.doi.org/10.14701/kjhbps.2014.18.4.152 Original Article Surgical outcomes of multifocal branch duct intraductal papillary mucinous neoplasms
Korean J Hepatobiliary Pancreat Surg 2014;18:152-158 http://dx.doi.org/10.14701/kjhbps.2014.18.4.152 Original Article Surgical outcomes of multifocal branch duct intraductal papillary mucinous neoplasms
Combatting Pancreatic Cancer: Keys to Early Recognition and Diagnosis
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/combatting-pancreatic-cancer-keys-earlyrecognition-and-diagnosis/7286/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/combatting-pancreatic-cancer-keys-earlyrecognition-and-diagnosis/7286/
Contrast-Enhanced Ultrasonograpic Findings in Pancreatic Tumors
 Int. J. Med. Sci. 2008, 5 203 Short Research Communication International Journal of Medical Sciences ISSN 1449-1907 www.medsci.org 2008 5(4):203-208 Ivyspring International Publisher. All rights reserved
Int. J. Med. Sci. 2008, 5 203 Short Research Communication International Journal of Medical Sciences ISSN 1449-1907 www.medsci.org 2008 5(4):203-208 Ivyspring International Publisher. All rights reserved
Endoscopic Ultrasound Guided Trucut Biopsy of the Cyst Wall for Diagnosing Cystic Pancreatic Tumors
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:974 979 Endoscopic Ultrasound Guided Trucut Biopsy of the Cyst Wall for Diagnosing Cystic Pancreatic Tumors MICHAEL J. LEVY,* THOMAS C. SMYRK, RAGHURAM P.
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:974 979 Endoscopic Ultrasound Guided Trucut Biopsy of the Cyst Wall for Diagnosing Cystic Pancreatic Tumors MICHAEL J. LEVY,* THOMAS C. SMYRK, RAGHURAM P.
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
ROSE in EUS guided FNA of Pancreatic Lesions
 ROSE in EUS guided FNA of Pancreatic Lesions Guy s Hospital, London, 16 April 2018 Laxmi Batav Imperial College NHS Trust Imperial College NHS Trust Cytology Workload Cervical Cytology 57,500 (decreases
ROSE in EUS guided FNA of Pancreatic Lesions Guy s Hospital, London, 16 April 2018 Laxmi Batav Imperial College NHS Trust Imperial College NHS Trust Cytology Workload Cervical Cytology 57,500 (decreases
Pancreatic cysts: etiology, diagnosis and management
 Cent. Eur. J. Med. 9(1) 2014 92-107 DOI: 10.2478/s11536-013-0244-8 Central European Journal of Medicine Pancreatic cysts: etiology, diagnosis and management Review Article Beata Jabłońska* Department of
Cent. Eur. J. Med. 9(1) 2014 92-107 DOI: 10.2478/s11536-013-0244-8 Central European Journal of Medicine Pancreatic cysts: etiology, diagnosis and management Review Article Beata Jabłońska* Department of
INTRODUCTION TO PATHOLOGICAL TECHNIQUES. 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH)
") INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
Patient with incidental pancreatic cyst
 Clinical problem Diego Aponte M, MD 1 1 Internal Medicine Gastroenterology Specialist. Gastroenterology Academic Coordinator for Graduate Level. Fundación Sanitas. Bogotá, Colombia.... Received: 07-09-10
Clinical problem Diego Aponte M, MD 1 1 Internal Medicine Gastroenterology Specialist. Gastroenterology Academic Coordinator for Graduate Level. Fundación Sanitas. Bogotá, Colombia.... Received: 07-09-10
Intraductal papillary mucinous neoplasm of the bile ducts: a rare form of premalignant lesion of invasive cholangiocarcinoma
 Intraductal papillary mucinous neoplasm of the bile ducts: a rare form of premalignant lesion of invasive cholangiocarcinoma Authors: R. Revert Espí, Y. Fernandez Nuñez, I. Carbonell, D. P. Gómez valencia,
Intraductal papillary mucinous neoplasm of the bile ducts: a rare form of premalignant lesion of invasive cholangiocarcinoma Authors: R. Revert Espí, Y. Fernandez Nuñez, I. Carbonell, D. P. Gómez valencia,
Intraductal Papillary Mucinous Neoplasm of the Pancreas. Masao Tanaka Editor
 Intraductal Papillary Mucinous Neoplasm of the Pancreas Masao Tanaka Editor Intraductal Papillary Mucinous Neoplasm of the Pancreas Masao Tanaka Editor Intraductal Papillary Mucinous Neoplasm of the Pancreas
Intraductal Papillary Mucinous Neoplasm of the Pancreas Masao Tanaka Editor Intraductal Papillary Mucinous Neoplasm of the Pancreas Masao Tanaka Editor Intraductal Papillary Mucinous Neoplasm of the Pancreas
ASSESSMENT QUESTIONS: THE BASICS
 ASSESSMENT QUESTIONS: THE BASICS Diane Davis Davey, MD Univ. of Central Florida Chair, Continuing Education Oversight Committee Disclosures I am President of the American Board of Pathology for 2012. None
ASSESSMENT QUESTIONS: THE BASICS Diane Davis Davey, MD Univ. of Central Florida Chair, Continuing Education Oversight Committee Disclosures I am President of the American Board of Pathology for 2012. None
Intracystic papillary carcinoma of the breast
 Intracystic papillary carcinoma of the breast Poster No.: C-1932 Congress: ECR 2011 Type: Educational Exhibit Authors: V. Dimarelos, F. TZIKOS, N. Kotziamani, G. Rodokalakis, 1 2 3 1 1 1 2 T. MALKOTSI
Intracystic papillary carcinoma of the breast Poster No.: C-1932 Congress: ECR 2011 Type: Educational Exhibit Authors: V. Dimarelos, F. TZIKOS, N. Kotziamani, G. Rodokalakis, 1 2 3 1 1 1 2 T. MALKOTSI
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes
 Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes Evan A. Alston, MD 1 ; Sejong Bae, PhD 2 ; and Isam A. Eltoum, MD, MBA 1 BACKGROUND:
Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes Evan A. Alston, MD 1 ; Sejong Bae, PhD 2 ; and Isam A. Eltoum, MD, MBA 1 BACKGROUND:
Cytyc Corporation - Case Presentation Archive - March 2002
 FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
Intro to Gallbladder & Pancreas Pathology
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis i acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Dept. of Pathology
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis i acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Dept. of Pathology
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
Female Genital Tract Lab. Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan
 Female Genital Tract Lab Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan Ovarian Pathology A 20-year-old female presented with vague left pelvic pain. Pelvic exam revealed
Female Genital Tract Lab Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan Ovarian Pathology A 20-year-old female presented with vague left pelvic pain. Pelvic exam revealed
Diagnosis and Management of Cystic Pancreatic Lesions
 Gastrointestinal Imaging Best Practices/Review Sahani et al. Cystic Pancreatic Lesions Gastrointestinal Imaging Best Practices/Review Dushyant V. Sahani 1 Avinash Kambadakone 1 Michael Macari 2 Noaki Takahashi
Gastrointestinal Imaging Best Practices/Review Sahani et al. Cystic Pancreatic Lesions Gastrointestinal Imaging Best Practices/Review Dushyant V. Sahani 1 Avinash Kambadakone 1 Michael Macari 2 Noaki Takahashi
Introduction E389. Background and study aims Guidelines for management
 Impact of endoscopic ultrasound on diagnosis and management of presumed mucinous neoplasms when done for pancreatic cyst morphology change on non-invasive surveillance imaging Authors Kamraan Madhani 1,
Impact of endoscopic ultrasound on diagnosis and management of presumed mucinous neoplasms when done for pancreatic cyst morphology change on non-invasive surveillance imaging Authors Kamraan Madhani 1,