Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines
|
|
|
- Sara Houston
- 5 years ago
- Views:
Transcription
1 Standardized Terminology in Pancreatobiliary Cytology: The Papanicolaou Society Guidelines Barbara Ann Centeno. M.D. Vice-Chair, Clinical Services, Anatomic Pathology Assistant Chief, Pathology Service Director of Cytopathology Senior Member Moffitt Cancer Center Professor/Morsani College of Medicine University of South Florida Health Sciences
2 Pancreatobiliary Massess: Differential Diagnosis Inflammatory Pancreatitis Biliary tract inflammation Benign/Nonneoplastic Lymphoepithelial cyst of the pancreas Ectopic Splenule Squamoid cyst Neoplastic Neuroendocrine Tumors Solid pseudopapillary Neoplasm Serous cystadenoma Mucinous cystic neoplasm (pancreatic and biliary) Neoplastic Pancreatic and Biliary Intraepithelial Neoplasia (BilIN) Grades 1,2, 3 Intraductal papillary Mucinous Neoplasms Intraductal papillary Neoplasms- Biliary Tract (IPN-B) LGD, MGD, HGD Malignant Adenocarcinoma and variants Acinar cell carcinoma Neuroendocrine carcinomas
3 Imaging Appearance Solid Mixed Solid and Cystic Cystic Benign/Non- Neoplastic Acute pancreatitis Chronic pancreatitis Autoimmune pancreatitis Ectopic spleen Neoplastic Ductal adenocarcinoma Neuroendocrine tumors Acinar cell carcinoma Pancreatoblastoma Lymphoma, plasmacytoma Metastasis Benign/Non- Neoplastic Groove pancreatitis Neoplastic Solid-pseudopapillary neoplasm Neuroendocrine tumors Ductal adenocarcinoma Acinar cell carcinoma Metastases and secondary tumors Benign/Non- Neoplastic Mature teratoma Epidermoid cyst in ectopic spleen Lymphoepithelial cyst Pseudocyst Squamoid cyst of pancreatic ducts Neoplastic Intraductal papillary mucinous neoplasms Mucinous cystic neoplasms Cystic neuroendocrine tumors Serous cystic neoplasm Acinar cell cystadenocarcinoma Algorithmic approach of pancreatic masses based on imaging features
4 Issues with Cytology Reporting of Pancreatobiliary Specimens Nonstandardized reporting lead to confusion for the clinicians treating the patient with a pancreatic mass or lesion Lack of epithelial cells used as criteria for nondiagnostic IPMN and MCN not uniformly handled, thick mucin still indicative of underlying neoplasm, even without neoplastic cells Pseudocysts will lack epithelial cells Serous cystadenoma may lack neoplastic cells Cases signed out as c/w cyst contents What cytological criteria should be used to interpret a lesion as IPMN or MCN? Atypical mucinous epithelium classified as atypical, rather than neoplastic, or as suspicious for carcinoma
5 Issues with Cytology Reporting of Pancreatobiliary Specimens cont. Was high grade dysplasia in IPMN atypical, suspicious or malignant? Serous cystadenoma classified as negative or atypical Were neuroendocrine tumor and solid pseudopapillary neoplasms suspicious, positive, or other?
6 Diagnostic Cytopathology. April 2014 vol. 42 (4)
7 Purpose of Standardization Unify reporting of disease categories among pathologists Reduce and improve inter and intraobserver variability Provide clinically relevant information for patient management To reflect the current understanding of the biology of disease entities
8 Categories I. Nondiagnostic II. Negative (for malignancy) III. Atypical IV. Neoplastic: benign or other V. Suspicious (for malignancy) VI. Positive (for malignancy) or malignant * only for laboratory systems where the information system requires it.
9 Nondiagnostic Category I
10 Nondiagnostic Definition: A non-diagnostic cytology specimen is one that provides no useful information or diagnostic information about the sampled mass. Discordant imaging and cytology findings Cyst fluids that yield insufficient material for ancillary studies Any cellular atypia precludes a non-diagnostic category Caveats: There are no established criteria for adequacy in pancreatobiliary specimens Nondiagnostic does not equal unsatisfactory Unsatisfactory indicates that a specimen cannot be processed and evaluated microscopically. There is no technical billing component. A nondiagnostic specimen can be processed and assessed microscopically, but the sample does not provide information that is diagnostic of the lesion sampled. The technical component may be billed.
11 Nondiagnostic Cytological Criteria Preparation or obscuring artifact preclude evaluation of the cellular sample Gastrointestinal contaminant only Benign acinar and ductal epithelium derived from a clearly defined solid or cystic mass lesion Acellular aspirates of a pancreatic mass or pancreatic brushing Acellular aspirate of a cyst without evidence of mucinous etiology. Lack of thick, background mucin and/or oncotic cells Lack of elevated CEA Lack of KRAS or GNAS mutations
12 Discordant Imaging and Cytology

13 Discordant Imaging and Cytology Imaging shows a well-defined mass Cytology shows benign pancreatic elements Report Adequacy: Satisfactory for evaluation or evaluation limited by lack of representative cells? Interpretation: Nondiagnostic: Benign acinar and ductal cells Category: Nondiagnostic Comment: The sample may not be representative of the targeted, welldefined lesion.

14 Nondiagnostic due to Preparation Artifact Adequacy: Evaluation limited by thickness of smear Interpretation: Nondiagnostic specimen Category: Nondiagnostic


15 GI Contaminant Adequacy: Evaluation limited by lack of representative cells Interpretation: Nondiagnostic, gastrointestinal contaminant only Category:Nondiagnostic Comment: The sample does not explain the mass lesion identified on imaging studies.
16 Negative Category II
17 Negative Definition: Adequate cellular and/or extracellular material to evaluate and or define a nonneoplastic lesion identified on imaging The category must qualified by a diagnosis of a specific condition Includes the presence of normal pancreatic parenchyma in the appropriate clinical setting Vague fullness of the pancreas No distinct pancreatic mass
18 Differential Diagnosis Benign pancreas Acute Pancreatitis Chronic Pancreatitis Autoimmune pancreatitis Splenule/Ectopic spleen/accessory spleen Pseudocyst Lymphoepithelial cyst
19 Negative Cytological Criteria Benign pancreatic ductal and acinar epithelium from a vague fullness Benign bile duct epithelium and bile Benign gastric or duodenal epithelium Aspirates showing cytological features of: Acute or chronic pancreatitis AIP Pseudocyst LECP Splenule


20 Negative: Chronic Pancreatitis Imaging: Hypoechoic mass in a patient with a history of pancreatitis. CA19-9 levels normal. Cytology Report: Adequacy: Satisfactory for evaluation Interpretation: c/w chronic pancreatitis Category: Neg.


21 Negative: Lymphoepithelial cyst Imaging: Well-defined cystic mass Cytology: anucleated squames, cholesterol crystals, debris Ancillary studies: elevated CEA, elevated amylase, no KRAS or GNAS mutations Report: Adequacy: Satisfactory Interpretation: Lymphoepithelial cyst Category: Neg. Comment: The cytomorphological findings are those of a lymphoepithelial cyst of the pancreas. These cysts present with elevated levels of CEA and amylase.

22 Negative: Pseudocyst Imaging: Cyst in the tail of the pancreas; aspirated abundant turbid, brown fluid Cytology: histiocytes, yellow pigment, debris Ancillary studies: amylase = 50, 000 U/L; CEA= 3 ng/ml Report Adequacy: Satisfactory Interpretation: Inflammation, histiocytes, debris, and yellow pigment, no epithelial lining cells identified, c/w pseudocyst Category: Neg. Comment: The morphology, combined with the ancillary studies are supportive of a diagnosis of pseudocyst. *Important caveat: Only diagnose a pseudocyst if it has the characteristic yellow pigment on cytology. Otherwise, be descriptive. Amylase and CEA levels in MCN and IPMN may be misleading. Other processes may have only histiocytes or hemosiderin laden macrophages.

23 Negative: Splenule Imaging: Well-defined mass Cytology: plasma cells and vascular structure on cell block Report: Adequacy: Satisfactory Interpretation: Splenule Category: Negative
24 Atypical Category III
25 Atypical Definition: Cells with cytoplasmic, nuclear, or architectural features not consistent with normal or reactive cellular components of the pancreas or bile ducts, and insufficient features to classify them as a neoplasm or suspicious for a high grade malignancy The findings do not explain the lesion identified on imaging Follow-up evaluation is warranted
26 Atypical Cytological criteria for ductal epithelium Loss of architectural polarity Mild loss of honeycombing When seen on edge, cells remain at base No crowded, three-dimensional groups Absence of true nuclear molding Near normal N/C Slight nuclear membrane irregularities Mild parachromatin clearing Small nucleoli Minimal anisonucleosis, 2:1 4:1 for carcinoma Clean or bloody background Coagulative tumor type necrosis suspicious
27 Atypical Cytological Criteria Atypical mucinous epithelium in a pancreatic aspirate PanIN Gastric contaminant IPMN Biliary brush specimens with mucinous epithelium and other atypical findings BilIN IPN-B Cellular component is suggestive of a PanNET or SPN but the sample is of insufficient quantity or quality for definitive diagnosis

28 Atypical Imaging: mass lesion in the head of the pancreas Cytology: Scantly cellular smear, ductal group with nuclear overlap, nuclear membrane irregularity, infiltrated by neutrophils Report: Adequacy: Evaluation limited by airdrying artifact Interpretation: Atypical groups of ductal epithelium with acute inflammation Category: Atypical Comment: The findings may be related to reactive process, however, a neoplastic process is not excluded. Recommend correlation with clinical and imaging findings and follow-up as indicated.


29 Atypical Imaging: Stricture in bile duct Cytology: maintained honeycomb, with subtle loss of polarity, subtle nuclear angulations, parachromatin clearing Report: Adequacy: Satisfactory Atypical ductal epithelium Category: Atypical

30 Atypical Imaging: well-defined, hypoechoic mass Cytology: few monomorphic cells Report: Adequacy: Evaluation limited by scant representative cells Interpretation: Few monomorphic nneoplastic cells present Category: Atypical Comment: The differential diagnosis includes pancreatic neuroendocrine tumor and solid pseudopapillary neoplasm. The material is insufficient for ancillary studies to further define the lesion.
31 Neoplastic Category IV
32 Neoplastic: Benign Definition: The cytological specimen is sufficiently cellular and representative, with or without the context of clinical, imaging and ancillary studies to be diagnostic of a benign neoplasm. Neoplasms included in tis category: Serous cystadenoma Schwannoma Cystic teratoma


33 Neoplastic: Benign Report Adequacy: Satisfactory Interpretation: Nonmucinous cuboidal epithelium, c/w imaging impression of serous cystadenoma Category: Neoplastic:Benign (Other) Comment: The cyst fluid CEA level was 2.9 ng/ml and the amylase was 500 U/L. Caveat: CEA and amylase may be quite variable. Most aspirates yield only hemosiderin laden macrophages.
34 Neoplastic: Other Definition: Defines a neoplasm that is either premalignant, or a low grade malignant neoplasm. Neoplasms included in this category: Neoplasm that is preinvasive cancer IPMN or MCN with LGD, MGD, HGD IOPN Solid cellular neoplasm Pancreatic neuroendocrine tumor Solid pseudopapillary neoplasm Extra-adrenal paraganglioma Gastrointestinal Stromal tumor
35 Rationale Established to provide a category for neoplasms that were either not clearly benign, such as serous cystadenoma, nor clearly aggressive, and high grade in their behavior, such as ductal adenocarcinoma. Standardize cytological nomenclature and terminology to correlate with WHO 2010 classification and terminology. The words tumor and neoplasm connote a neoplasm, but not a malignancy Patients with neoplasms in this category may have the option of being managed conservatively PanNET may be observed IPMN with low risk features may be observed. The categories of atypical and suspicious connote an indeterminate interpretation. Does not define these a benign or malignant
 Ancillary Testing: CAM 5.")
36 Neoplastic: Other Imaging: well-defined, solid, hypoechoic mass Report: Adequacy: Satisfactory Interpretation: Pancreatic neuroendocrine tumor, welldifferentiated Category: Neoplastic:Other (Other) Ancillary Testing: CAM 5.2+, CD 56+, synaptophysin +, Chromogranin +
 Ancillary Testing: beta-catenin nuclear")
37 Neoplastic: Other Imaging: well-defined, solid and cystic mass Report: Adequacy: Satisfactory Interpretation: Solid pseudopapillary neoplasm Category: Neoplastic:Other (Other) Ancillary Testing: beta-catenin nuclear (mutated)

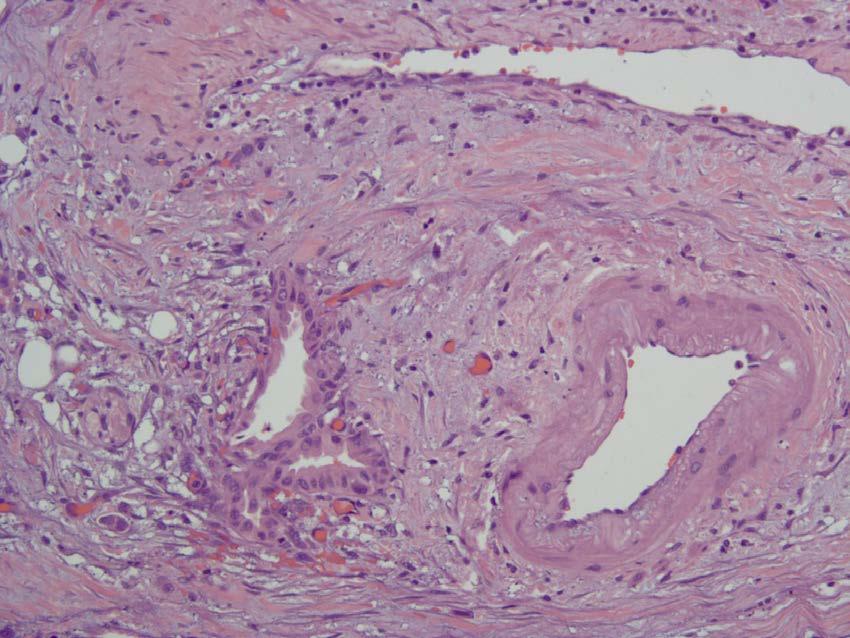
38 Neoplastic: Other



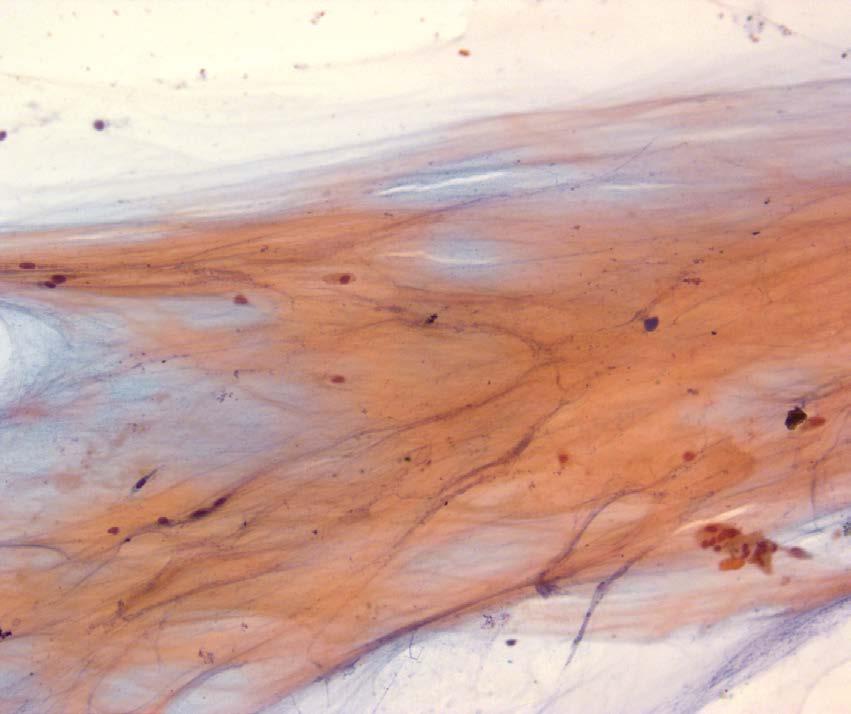
39 Psammomatous calcifications a feature of IPMN Ferning Cell block showing thick, feathery type material
 Comment: No neoplastic epithelium is present for evaluation of dysplasia.")
40 Neoplastic: Other Imaging: Large, multiloculated cyst in the tail of the pancreas with evident connect to the pancreatic ductal system Report: Adequacy: Satisfactory Interpretation: Thick background mucin, histiocytes, and oncotic cells, consistent with IPMN Category: Neoplastic: Other (other) Comment: No neoplastic epithelium is present for evaluation of dysplasia. The cytological findings correlated with the imaging findings support the above interpretation.
41 Incidental Cysts in the Pancreas Incidental cysts of the pancreas are common More likely to be neoplastic rather than benign 30% of all incidental masses were IPMN in one series 55% were MCN or IPMN (preinvasive precursors), only 4% were pseudocyst Pathologist is reviewing the cyst fluid to assess for the presence of pre-invasive precursors lesions Pseudocyst diagnosis of exclusion

42 Cyst Contents
43 Criteria for Mucinous Cyst Fluid viscous, clear or white Cytology shows mucinous background as described, +/- neoplastic epithelium Ancillary studies CEA elevated Mutational analyses will identify neoplastic processes KRAS mutated in IPMN and MCN GNAS mutations in IPMN RNF43 mutations in IPMN and MCN
44 Mucinous cysts Nonneoplastic and neoplastic mucinous cysts Nonneoplastic mucinous cyst (mucinous duct lesion) Foregut cysts Nonneoplastic cysts lack mutations Cytological and cyst fluid features may overlap Mucin only Elevated CEA Lack KRAS and GNAS Mucinous cyst, not otherwise specified Characteristic mucin with oncotic cells, no epithelium for evaluation Mucinous cyst with low grade epithelial atypia (low grade and moderate grade dysplasia) (IPMN or MCN) Mucinous cyst with high grade epithelial atypia (high grade dysplasia and adenocarcinoma)


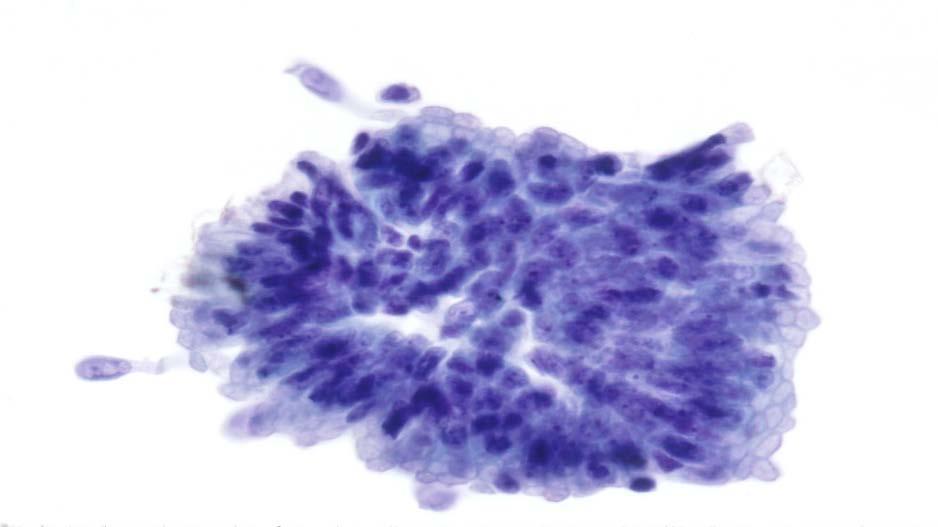
45 Low-Grade Dysplasia Abundant columnar mucin containing cytoplasm Basally located nuclei Columnar cytoplasm with mucin Basally located nuclei

46 Moderate dysplasia Pseudostratification


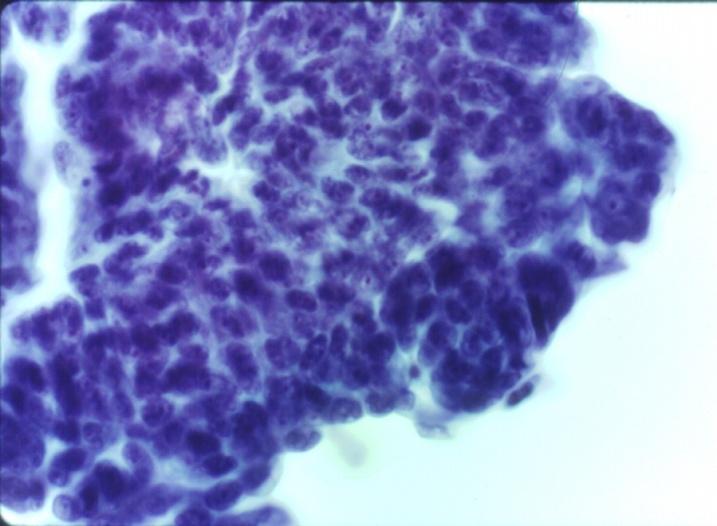
47 High-Grade Dysplasia Papillary tufts, nuclei extend to luminal border Mitoses
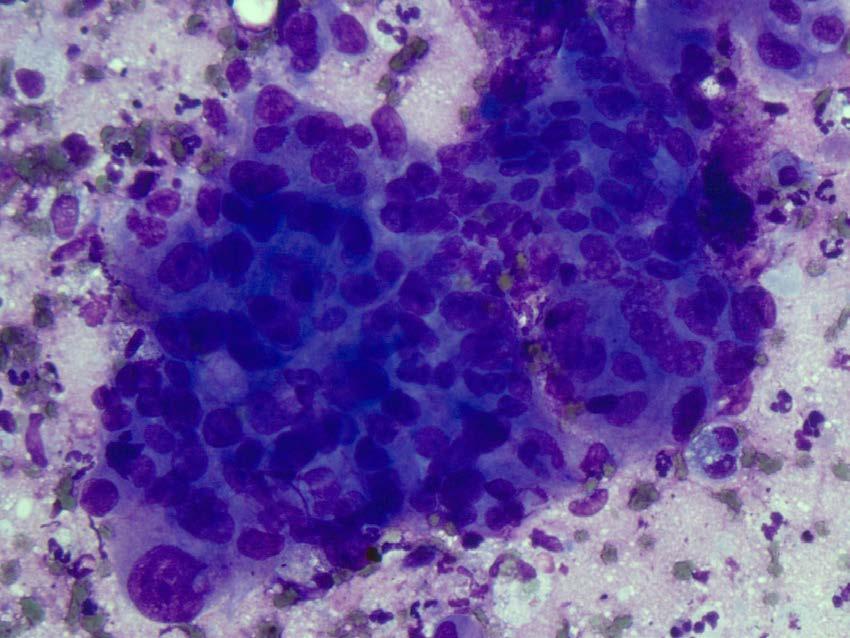
48 Adenocarcinoma
")
49 High-grade epithelial atypia Includes high grade dysplasia and invasive carcinoma Criteria High N/C Nuclear membrane irregularities Abnormal chromatin Hypo- or hyperchromasia Background necrosis Cancer (Cancer Cytopathol) 2013;121:
50 Suspicious Category V
51 Suspicious Definition: Some, but not all of the criteria of a specific malignant neoplasm are present, mainly for pancreatic adenocarcinoma diagnosis. The features are qualitatively or quantitatively insufficient for a conclusive diagnosis. Confirmatory ancillary testing or substantial clinical and radiological findings must be present and discussed during a treatment planning conference, or similar correlation conference. Indeterminate category
52 Suspicious Cytological criteria Sufficient cellular or architectural atypia to be derived from a malignancy Suspicious for ductal adenocarcinoma Significant loss of group and cell polarity, significant anisonucleosis, increased N/C, nuclear membrane irregularities, moderate to marked coarsening of the chromatin Suspicious for acinar cell carcinoma Cytological features of acinar cell carcinoma, cannot confirm with ancillary studies Cyst aspirates with a solid mural nodule and cytological features suspicious for invasive carcinoma Other Lymphoma Metastases
53 Suspicious Management Management decisions based on correlation with other clinical and imaging findings Cannot be used as a basis for surgical intervention or adjuvant therapy Ancillary testing, expert consultation, repeat sampling, or discussion at a treatment planning conference, such as the Moffitt multidisciplinary tumor boards

54 Suspicious Imaging: Ill-defined, hypoechoic mass with evidence of invasion Cytology: Few cell groups with features of adenocarcinoma partially obscured by abundant acute inflammation Report Adequacy: Evaluation limited by scant cellularity Interpretation: Suspicious for adenocarcinoma Category: Suspicious

55 Ancillary Testing Immunohistochemistry DPC4/SMAD4, S100P, mesothelin FISH Same probes as in UroVysion 3, 7, 17, 9p21 mirna DPC4
56 Positive Category VI
57 Positive/Malignant Definition: Unequivocal display of malignant cytological change Diagnoses: Adenocarcinoma and its variant Neuroendocrine carcinoma, small and large cell type Pancreatoblastoma Acinar cell carcinoma Lymphoma Metastases Sarcomas in this region, secondarily involving the pancreas


58 Positive Imaging: Ill-defined pancreatic mass Report Adequacy: Satisfactory Interpretation: Poorly differentiated neuroendocrine carcinoma, small cell type Category: Positive (Diagnostic for malignancy) Comment: The carcinoma is positive for cytokeratin, CD 56 and synaptophysin, confirming the above interpretation. Synaptophysin
59 Summary The PSC guidelines developed 6 categories with criteria for each category Restricted the use of nondiagnostic Clarified the categorization of PanNET and SPN Defined criteria for reporting and work-up of preinvasive cysts The reporting terminology and categories will clarify communication of pathology results to the treating physicians. Reporting needs to incorporate correlation of clinical, imaging, cytological and ancillary findings.
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT
 CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
CYTOLOGY OF EUS- GUIDED FNA OF THE PANCREAS AND THE UPPER GI TRACT Barbara A. Centeno, M.D. Vice-Chair, Clinical Services Assistant Chief of Pathology Director of Cytopathology Department of Anatomic Pathology/Moffitt
Pancreatico-biliary cytology: a practical approach to diagnosis. Corina Cotoi
 Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Pancreatico-biliary cytology: a practical approach to diagnosis Corina Cotoi Pancreatico-biliary lesions Solid: Ductal adenocarcinoma Cholangiocarcinoma Acinar cell carcinoma Neuroendocrine tumour / carcinoma
Case 1. Case 1: EUS Report 5/1/2017. Interesting Cases of Pancreatic Masses
 Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Interesting Cases of Pancreatic Masses Martha Bishop Pitman, MD Professor of Pathology Harvard Medical School Director of Cytopathology Massachusetts General Hospital Boston, MA MASSACHUSETTS GENERAL PHYSICIANS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA
 Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Pancreatitis: A Potential Pitfall in Endoscopic Ultrasound Guided Pancreatic FNA Jack Yang, MD Department of Pathology, Medical University of South Carolina Objectives Understand the indication of EUS
Standardization of Nomenclature
 Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Conflicts of Interest
 Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Standardized Terminology and Nomenclature for Pancreaticobiliary Cytopathology from the Papanicolaou Society of Cytopathology Lester J. Layfield, M.D. Professor and Chair University of Missouri Pathology
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget
 Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Evaluation and Management of Cystic Lesions of the Pancreas: When to Resect, When to Follow and When to Forget Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
Patient History. A 58 year old man presents with a 16 mm cyst in the pancreatic tail. The cyst is unilocular with a thick wall and no mural nodule.
 Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Case 1 Martha Bishop Pitman, MD Director of Cytopathology Massachusetts General Hospital Associate Professor of Pathology Harvard Medical School Boston, MA Patient History A 58 year old man presents with
Biliary Tract Neoplasia: A Cyto-histologic Review. Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital
 Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
Biliary Tract Neoplasia: A Cyto-histologic Review Michelle Reid, MD, MSc Professor of Pathology Director of Cytopathology Emory University Hospital Bile Duct Brushings (BDB) BDBs are the initial diagnostic
Pancreatic Cystic Lesions 원자력병원
 Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Pancreatic Cystic Lesions 원자력병원 박선 후 Lines of cellular differentiation Ductal Acinar Undetermined Ductal adenocarcinoma Serous/ mucinous tumor Intraductal papillary mucinous neoplasm Acinar cell carcinoma
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital
 Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
Pancreatic Cytopathology: A pragmatic approach. By Dr Miguel Perez-Machado MD. PhD. MRCPath Royal Free Hospital Indications of Cytology Sampling To document malignancy in patients with malignant appearing
Video Microscopy Tutorial 19
 Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
Video Microscopy Tutorial 19 EUS FNA of Pancreatic Cysts Martha Pitman, MD There are no disclosures necessary. EUS-FNA of Pancreatic Cysts Martha Bishop Pitman, M.D. Massachusetts General Hospital Harvard
Objectives. Pancreatic Cysts. Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses
 Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses Michelle D. Reid, MD, MSc Associate 1/24/15 Professor Director of Cytology - EUHM Michelle D Reid MD, MS Emory
Benefits and Limitations of the Cytologic Assessment of Cystic Pancreatic Lesions and Masses Michelle D. Reid, MD, MSc Associate 1/24/15 Professor Director of Cytology - EUHM Michelle D Reid MD, MS Emory
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Endoscopic Ultrasound-guided FNA Cytology of the Pancreas
 Endoscopic Ultrasound-guided FNA Cytology of the Pancreas 67 th Annual California Society of Pathologists 2014 Laura Tabatabai, MD Professor of Pathology University of California, San Francisco Overview
Endoscopic Ultrasound-guided FNA Cytology of the Pancreas 67 th Annual California Society of Pathologists 2014 Laura Tabatabai, MD Professor of Pathology University of California, San Francisco Overview
EUS-guided FNAB. Differential Diagnosis 5/1/2017. EUS-FNA of Solid and Cystic Lesions:
 EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
An Approach to Pancreatic Cysts. Introduction
 An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
DIAGNOSTIC CHALLENGES Pancreas FNAB. Dr. M. Weir Oct 2017
 DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
Advances in Pancreatic. Cytology. Martha B. Pitman, MD. Disclosure of Relevant Financial Relationships
 Advances in Pancreatic Cytology Martha B. Pitman, MD Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Advances in Pancreatic Cytology Martha B. Pitman, MD Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS
 ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS Prof. Fernando Schmitt Medical Faculty of Porto University, Porto, Portugal IPATIMUP General Secretary of the International Academy of Cytology
ENDOSCOPIC ULTRA SOUND GUIDED FNA OF GI TRACT AND PANCREAS Prof. Fernando Schmitt Medical Faculty of Porto University, Porto, Portugal IPATIMUP General Secretary of the International Academy of Cytology
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions
 Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School, USA Marc Pusztaszeri,
Salivary Gland Cytology: A Clinical Approach to Diagnosis and Management of Atypical and Suspicious Lesions W.C. Faquin, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School, USA Marc Pusztaszeri,
Team approach is essential incorporating: radiology, gastroenterology, surgery and pathology Successful performance is operator dependent
 Committee V Post Brushing and FNA Testing Managment Options Daniel Kurtycz, M.D. Chair Committee V Committee V - Post brushing and FNA management options Team approach is essential incorporating: radiology,
Committee V Post Brushing and FNA Testing Managment Options Daniel Kurtycz, M.D. Chair Committee V Committee V - Post brushing and FNA management options Team approach is essential incorporating: radiology,
Cytyc Corporation - Case Presentation Archive - March 2002
 FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
Matthew McCollough, M.D. April 9, 2009 University of Louisville
 Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
Matthew McCollough, M.D. April 9, 2009 University of Louisville List the differential diagnosis for pancreatic cysts Review the epidemiology Illustrate the types of cysts through case discussions Discuss
ROSE in EUS guided FNA of Pancreatic Lesions
 ROSE in EUS guided FNA of Pancreatic Lesions Guy s Hospital, London, 16 April 2018 Laxmi Batav Imperial College NHS Trust Imperial College NHS Trust Cytology Workload Cervical Cytology 57,500 (decreases
ROSE in EUS guided FNA of Pancreatic Lesions Guy s Hospital, London, 16 April 2018 Laxmi Batav Imperial College NHS Trust Imperial College NHS Trust Cytology Workload Cervical Cytology 57,500 (decreases
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases
 Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes
 Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes Evan A. Alston, MD 1 ; Sejong Bae, PhD 2 ; and Isam A. Eltoum, MD, MBA 1 BACKGROUND:
Suspicious Cytologic Diagnostic Category in Endoscopic Ultrasound-Guided FNA of the Pancreas: Follow-Up and Outcomes Evan A. Alston, MD 1 ; Sejong Bae, PhD 2 ; and Isam A. Eltoum, MD, MBA 1 BACKGROUND:
EUS-FNAB of GI Tract: Specimen Handling and Triage
 EUS-FNAB of GI Tract: Specimen Handling and Triage Amy Ly, M.D. Director, Fine Needle Aspiration Service Massachusetts General Hospital Assistant Professor of Pathology Harvard Medical School Boston, MA
EUS-FNAB of GI Tract: Specimen Handling and Triage Amy Ly, M.D. Director, Fine Needle Aspiration Service Massachusetts General Hospital Assistant Professor of Pathology Harvard Medical School Boston, MA
Thyroid follicular neoplasms in cytology. Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia
 Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Pancreatobiliary Frozen Section Nightmares
 Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Pancreatobiliary Frozen Section Nightmares Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Objectives Briefly give an overview
Atypia in Diagnostic Cytopathology: Strategies to Reduce Overuse A CQI initiative
 in Diagnostic Cytopathology: Strategies to Reduce Overuse A CQI initiative Dr. Mariamma Joseph and Susan McRae Objectives Review cytology literature on standardization of as a diagnostic term Address the
in Diagnostic Cytopathology: Strategies to Reduce Overuse A CQI initiative Dr. Mariamma Joseph and Susan McRae Objectives Review cytology literature on standardization of as a diagnostic term Address the
Pancreatic Cysts. Darius C. Desai, MD FACS St. Luke s University Health Network
 Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
Pancreatic Cysts Darius C. Desai, MD FACS St. Luke s University Health Network None Disclosures Incidence Widespread use of cross sectional imaging Seen in over 2% of patients having abdominal imaging
Biliary cytolgy and pancreatic endoscopic ultrasound-guided. Helsinki, FINLAND
 Biliary cytolgy and pancreatic endoscopic ultrasound-guided d FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology Obstructions PSC, a premalignant condition, the cure of which is transplantation
Biliary cytolgy and pancreatic endoscopic ultrasound-guided d FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology Obstructions PSC, a premalignant condition, the cure of which is transplantation
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts
 ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
EUS-FNA OF PANCREATIC EXOCRINE TUMORS COMPARISON OF EXPERIENCES WITH PATHOLOGICAL DIAGNOSIS
 EUS-FNA OF PANCREATIC EXOCRINE TUMORS COMPARISON OF EXPERIENCES WITH PATHOLOGICAL DIAGNOSIS Vincenzo Canzonieri, M.D. CRO - Aviano National Cancer Institute Dept of Pathology EUS European Cyto-Pathologist
EUS-FNA OF PANCREATIC EXOCRINE TUMORS COMPARISON OF EXPERIENCES WITH PATHOLOGICAL DIAGNOSIS Vincenzo Canzonieri, M.D. CRO - Aviano National Cancer Institute Dept of Pathology EUS European Cyto-Pathologist
Guidelines for Pancreaticobiliary Cytology from the Papanicolaou Society of Cytopathology: A Review
 Guidelines for Pancreaticobiliary Cytology from the Papanicolaou Society of Cytopathology: A Review Martha B. Pitman, MD 1 and Lester J. Layfield, MD 2 The newest installment on state-of-the-art standards
Guidelines for Pancreaticobiliary Cytology from the Papanicolaou Society of Cytopathology: A Review Martha B. Pitman, MD 1 and Lester J. Layfield, MD 2 The newest installment on state-of-the-art standards
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Overview. Disclosure. PRE INVASIVE NEOPLASIA OF BILIARY TREE New Perspectives on Old Themes. N. Volkan Adsay, MD
 PRE INVASIVE NEOPLASIA OF BILIARY TREE New Perspectives on Old Themes N. Volkan Adsay, MD Professor and Vice-Chair Director of Anatomic Pathology Emory University and Emory Winship Cancer Institute Atlanta,
PRE INVASIVE NEOPLASIA OF BILIARY TREE New Perspectives on Old Themes N. Volkan Adsay, MD Professor and Vice-Chair Director of Anatomic Pathology Emory University and Emory Winship Cancer Institute Atlanta,
PANCREATIC CYTOPATHOLOGY: PRACTICAL POINTS TO AVOID COMMON PITFALLS
 PANCREATIC CYTOPATHOLOGY: PRACTICAL POINTS TO AVOID COMMON PITFALLS Barbara A. Centeno, M.D. Senior Member and Director of Cytopathology/H. Lee Moffitt Cancer Center and Research Institute Professor/ Departments
PANCREATIC CYTOPATHOLOGY: PRACTICAL POINTS TO AVOID COMMON PITFALLS Barbara A. Centeno, M.D. Senior Member and Director of Cytopathology/H. Lee Moffitt Cancer Center and Research Institute Professor/ Departments
We herein describe new concepts in the diagnosis of the
 The Evolving Role of Pathology in New Developments, Classification, Terminology, and Diagnosis of Pancreatobiliary Neoplasms Michelle D. Reid, MD; Melinda M. Lewis, MD; Field F. Willingham, MD, MPH; N.
The Evolving Role of Pathology in New Developments, Classification, Terminology, and Diagnosis of Pancreatobiliary Neoplasms Michelle D. Reid, MD; Melinda M. Lewis, MD; Field F. Willingham, MD, MPH; N.
Management A Guideline Based Approach to the Incidental Pancreatic Cysts. Common Cystic Pancreatic Neoplasms.
 Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
Management 2016 A Guideline Based Approach to the Incidental Pancreatic Cysts ISMRM 2016 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
EUS-guided FNAB. Differential Diagnosis 3/14/2018. EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses
 EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
EUS-FNA of Solid and Cystic Lesions: Part 1: Solid Masses Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA EUS-guided
Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA. Leena Krogerus Helsinki, FINLAND
 Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology PSC- is a pre-neoplastc condition in youg individulas, the cure of which is
Biliary cytolgy and pancreatic endoscopic ultrasound-guided FNA Leena Krogerus Helsinki, FINLAND Reasons for biliary cytology PSC- is a pre-neoplastc condition in youg individulas, the cure of which is
SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H)
 - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H)") SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H) ASC refers to cytologic changes suggestive of SIL, which are qualitativley or quantitatively
SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H) ASC refers to cytologic changes suggestive of SIL, which are qualitativley or quantitatively
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
The Role of Molecular Analysis in the Diagnosis and Surveillance of Pancreatic Cystic Neoplasms
 JOP. J Pancreas (Online) 20 Mar 20; (2):-9. RESEARCH ARTICLE The Role of Molecular Analysis in the Diagnosis and Surveillance of Pancreatic Cystic Neoplasms Megan Winner, Amrita Sethi 2, John M Poneros
JOP. J Pancreas (Online) 20 Mar 20; (2):-9. RESEARCH ARTICLE The Role of Molecular Analysis in the Diagnosis and Surveillance of Pancreatic Cystic Neoplasms Megan Winner, Amrita Sethi 2, John M Poneros
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Workshop 9. Cytopathology of Solid and Cystic Neoplasms of the Pancreas: Everything You Need To Know For Daily Practice.
 Workshop 9 Cytopathology of Solid and Cystic Neoplasms of the Pancreas: Everything You Need To Know For Daily Practice Michelle Reid, MD Momin Siddiqui, MD,FIAC There are no disclosures necessary. Cytopathology
Workshop 9 Cytopathology of Solid and Cystic Neoplasms of the Pancreas: Everything You Need To Know For Daily Practice Michelle Reid, MD Momin Siddiqui, MD,FIAC There are no disclosures necessary. Cytopathology
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
ROSE (Rapid on site evaluation) in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits
 in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits") ROSE (Rapid on site evaluation) in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits Charitini Salla, MD Head of Cytopathology Department, Hygeia Hospital, Athens, Greece There is
ROSE (Rapid on site evaluation) in EUS-FNA in solid and cystic pancreatic lesions: possibilities and limits Charitini Salla, MD Head of Cytopathology Department, Hygeia Hospital, Athens, Greece There is
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
O Farrell Legacy UPDATE ON WHO NOMENCLATURE. World Health Organization, 2010 DISCLOSURES WITH EMPHASIS ON PROBLEM HEPATOCELLULAR TUMORS
 O Farrell Legacy UPDATE ON WHO NOMENCLATURE WITH EMPHASIS ON PROBLEM HEPATOCELLULAR TUMORS Linda Ferrell, MD University of California San Francisco Vice Chair, Director of Surgical Pathology World Health
O Farrell Legacy UPDATE ON WHO NOMENCLATURE WITH EMPHASIS ON PROBLEM HEPATOCELLULAR TUMORS Linda Ferrell, MD University of California San Francisco Vice Chair, Director of Surgical Pathology World Health
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD
 CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
CHRONIC PANCREATITIS OR DUCTAL ADENOCARCINOMA? N. Volkan Adsay, \ MD Case for discussion 67 y/o male Back pain and weight loss CT: 4.5 cm ill-defined, solid lesion in the head FNA/Core bx: Inconclusive
Cytopathology Study Day 16 April RCPath - BAC. Digital cytology: EUS FNA pancreas and head and neck
 Cytopathology Study Day 16 April 2017 Guy s Hospital London RCPath - BAC Digital cytology: EUS FNA pancreas and head and neck R. Dina MD, FIAC, FRCPath Consultant Cyto/Histopathologist Hon Sen Lecturer
Cytopathology Study Day 16 April 2017 Guy s Hospital London RCPath - BAC Digital cytology: EUS FNA pancreas and head and neck R. Dina MD, FIAC, FRCPath Consultant Cyto/Histopathologist Hon Sen Lecturer
Pancreatic Cystic Neoplasms: Guidelines and beyond
 Pancreatic Cystic Neoplasms: Guidelines and beyond Kenneth J. Chang, MD, FACG, FASGE Executive Director, Comprehensive Digestive Disease Center Professor and Chief, Gastroenterology Vincent & Anna Kong
Pancreatic Cystic Neoplasms: Guidelines and beyond Kenneth J. Chang, MD, FACG, FASGE Executive Director, Comprehensive Digestive Disease Center Professor and Chief, Gastroenterology Vincent & Anna Kong
Pancreatic intraepithelial
 Pancreatic intraepithelial neoplasia (PanIN) Markéta Hermanová St. Anne s University Hospital Brno Faculty of Medicine, Masaryk University Precursor lesions of invasive pancreatic cancer Pancreatic intraepithelial
Pancreatic intraepithelial neoplasia (PanIN) Markéta Hermanová St. Anne s University Hospital Brno Faculty of Medicine, Masaryk University Precursor lesions of invasive pancreatic cancer Pancreatic intraepithelial
Enterprise Interest None
 Enterprise Interest None Risk stratification of salivary gland lesions on cytology based on the proposed Milan System for reporting salivary gland cytopathology: A pilot study Kartik Viswanathan, M.D.,
Enterprise Interest None Risk stratification of salivary gland lesions on cytology based on the proposed Milan System for reporting salivary gland cytopathology: A pilot study Kartik Viswanathan, M.D.,
"Atypical": Criteria and
 "Atypical": Criteria and Controversies Esther Rossi MD PhD MIAC Division of Anatomic Pathology and Cytology Catholic University of Sacred Heart Rome, Italy CASE HISTORY In 2015, 45 y/o woman underwent
"Atypical": Criteria and Controversies Esther Rossi MD PhD MIAC Division of Anatomic Pathology and Cytology Catholic University of Sacred Heart Rome, Italy CASE HISTORY In 2015, 45 y/o woman underwent
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches
 Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Index 179. Genital tract contaminants, 17, 20, 22, 150 papilloma virus-infected cells, 47 squamous cells, sources of, 7
 Index Accuracy of urinary cytology, 166 Acute inflammatory cells, 38 catheter sample, 39 herpes simplex infections, 44 carcinomas, 104, 105 non-viral inclusions, 52, 53 voided urine, 17 Adenocarcinoma
Index Accuracy of urinary cytology, 166 Acute inflammatory cells, 38 catheter sample, 39 herpes simplex infections, 44 carcinomas, 104, 105 non-viral inclusions, 52, 53 voided urine, 17 Adenocarcinoma
Cytology for the Endocrinologist. Nicole Massoll M.D
 Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
State of the Art Symposium
 State of the Art Symposium Syed Z. Ali, MD There is no disclosure necessary Martha B. Pitman, MD There is no disclosure necessary Lester Layfield, MD There is no disclosure necessary Joseph Herman, MD
State of the Art Symposium Syed Z. Ali, MD There is no disclosure necessary Martha B. Pitman, MD There is no disclosure necessary Lester Layfield, MD There is no disclosure necessary Joseph Herman, MD
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
TBSRTC 1- Probabilistic approach and Relationship to Clinical Algorithms
 The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
ASSESSMENT QUESTIONS: THE BASICS
 ASSESSMENT QUESTIONS: THE BASICS Diane Davis Davey, MD Univ. of Central Florida Chair, Continuing Education Oversight Committee Disclosures I am President of the American Board of Pathology for 2012. None
ASSESSMENT QUESTIONS: THE BASICS Diane Davis Davey, MD Univ. of Central Florida Chair, Continuing Education Oversight Committee Disclosures I am President of the American Board of Pathology for 2012. None
Pancreatic Cysts. Pancreatic Cysts. Multidisciplinary and Multimodal Approach To the Pre-Operative Diagnosis of Pancreatic Cysts
 Multidisciplinary and Multimodal Approach To the Pre-Operative Diagnosis of Pancreatic Cysts Martha Bishop Pitman, M.D. Director of Cytopathology Massachusetts General Hospital Professor of Pathology Harvard
Multidisciplinary and Multimodal Approach To the Pre-Operative Diagnosis of Pancreatic Cysts Martha Bishop Pitman, M.D. Director of Cytopathology Massachusetts General Hospital Professor of Pathology Harvard
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts
 Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts Authors Alexander Lee 1, Vivek Kadiyala 2,LindaS.Lee 3 Institutions 1 Texas Digestive Disease Consultants,
Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts Authors Alexander Lee 1, Vivek Kadiyala 2,LindaS.Lee 3 Institutions 1 Texas Digestive Disease Consultants,
HANDOUT. Bile Duct Brushing Cytology: A Morphologic and Molecular Approach
 HANDOUT Bile Duct Brushing Cytology: A Morphologic and Molecular Approach Lester J. Layfield, M.D. Professor and Chair Department of Pathology & Anatomical Sciences University of Missouri Introduction
HANDOUT Bile Duct Brushing Cytology: A Morphologic and Molecular Approach Lester J. Layfield, M.D. Professor and Chair Department of Pathology & Anatomical Sciences University of Missouri Introduction
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology
 New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Pancreatic malignant tumors are the fifth leading cause of cancerrelated
 44 CANCER CYTOPATHOLOGY Cytologic Criteria for Well Differentiated Adenocarcinoma of the Pancreas in Fine-Needle Aspiration Biopsy Specimens Fan Lin, M.D., Ph.D. 1 Gregg Staerkel, M.D. 2 1 Department of
44 CANCER CYTOPATHOLOGY Cytologic Criteria for Well Differentiated Adenocarcinoma of the Pancreas in Fine-Needle Aspiration Biopsy Specimens Fan Lin, M.D., Ph.D. 1 Gregg Staerkel, M.D. 2 1 Department of
Atypical Pancreatic Endoscopic Ultrasound-Guided Fine Needle Aspiration Cytology: A Study of Interobserver Agreement
 ORIGINAL ARTICLE Atypical Pancreatic Endoscopic Ultrasound-Guided Fine Needle Aspiration Cytology: A Study of Interobserver Agreement Li Yan Khor, Simin Zeng, Lee Hong Song, Issam Al Jajeh, Kiat Hon Lim,
ORIGINAL ARTICLE Atypical Pancreatic Endoscopic Ultrasound-Guided Fine Needle Aspiration Cytology: A Study of Interobserver Agreement Li Yan Khor, Simin Zeng, Lee Hong Song, Issam Al Jajeh, Kiat Hon Lim,
Pancreatic Cancer: The ABCs of the AJCC and WHO
 Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Pancreatic Cancer: The ABCs of the AJCC and WHO Aatur D. Singhi, MD PhD Assistant Professor University of Pittsburgh Medical Center Department of Pathology singhiad@upmc.edu Case presentation Objectives
Intro to Gallbladder & Pancreas Pathology
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
DOWNLOAD ENTIRE DOCUMENT FROM
 PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
PREVIEW ONLY 1 Atlas on Bethesda system for reporting Thyroid Cytology PREVIEW ONLY 2 OVERVIEW 1. Indications and goal of thyroid FNA 2. Contraindications 3. Procurement of cell sample 4. Staining methods
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Prepared By Jocelyn Palao and Layla Faqih
 Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Kenneth D. Chi, MD Medical Director GI Lab Advocate Lutheran General Hospital
 Kenneth D. Chi, MD Medical Director GI Lab Advocate Lutheran General Hospital Advances in Digestive Health for the Primary Care Physician Symposium May 2, 2015 None Case Presentation Types of Pancreatic
Kenneth D. Chi, MD Medical Director GI Lab Advocate Lutheran General Hospital Advances in Digestive Health for the Primary Care Physician Symposium May 2, 2015 None Case Presentation Types of Pancreatic
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo. Case Discussions. 60 year old woman Routine gynecologic control LBC
 BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS
 Shamlal Mangray, MB, BS") Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
p53 expression in invasive pancreatic adenocarcinoma and precursor lesions
 Malaysian J Pathol 2011; 33(2) : 89 94 ORIGINAL ARTICLE p53 expression in invasive pancreatic adenocarcinoma and precursor lesions NORFADZILAH MY MBBCH,* Jayalakshmi PAILOOR MPath, FRCPath,* RETNESWARI
Malaysian J Pathol 2011; 33(2) : 89 94 ORIGINAL ARTICLE p53 expression in invasive pancreatic adenocarcinoma and precursor lesions NORFADZILAH MY MBBCH,* Jayalakshmi PAILOOR MPath, FRCPath,* RETNESWARI
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
3/28/2017. Disclosure of Relevant Financial Relationships. GU Evening Subspecialty Case Conference. Differential Diagnosis:
 GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
Background to the Thyroid Nodule
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological