What Fluid? Tim Harris Prof emergency Medicine
|
|
|
- Roger McDowell
- 5 years ago
- Views:
Transcription
1 What Fluid? Tim Harris Prof emergency Medicine
2 Why We prescribe fluids to prevent dehydra>on Oral or IV Post op care what do you use? fluids for resuscita>on Which and how much? 39 year old pyelonephri>s BP 90/64 aker 1500 ml Hartmanns
3 You are called to see 68 year old man Phx BPH and IHD with stent in situ but no CCF medn aspirin, ramipril, metoprolol, tamsulosin Now in ED with BP of 88/46, temp 40, P=118, GCS 15 with urosepsis Which fluid? How much No change aker 2000 ml crystalloid What would you do now? Which fluid? How much? His is now Hb 8.9 Which fluid how much? Blood transfusion?
4 Background - why we give fluids Maintenance preserve normovolaemia prevent intravascular dehydra>on Prevent unpleasant sensa>on of dehydra>on Therapeu>c intravascular & cellular dehydra>on Replace losses & restore circula>ng volume Resuscita>on cellular hypoxia and organ failure Restore oxygen delivery to match needs
5 Fluids available The pros and cons of fluid chooses
6 Dextrose Dextrose - expands all spaces, useful for longer term hydra>on aimed at ICS Is diure>c 60ml per 1000lm delivered remain IVS (poor resus fluid) Distribu>on to ICS causes cellular hydra>on (avoid any cerebral pathology) Not a resus fluid
7 Fluids for resuscita>on Predominantly distributed in IVS Crystalloids and colloids and blood products
8 NaCl 0.9% Crystalloid Balanced solu>ons refers to composi>on being similar to plasma Hartmann's (278, Na 131 mmoll, K 5 mmoll, Ca 2 mmoll, lactate 29 mmoll, Cl 111 mmoll) Ringer s (312, Na 147mmolL, K mmoll, Ca 2.2 mmoll, Cl 156 mmoll) Plasmolyte A & B Advantages Cheap, no anaphylaxis, replace lost fluids, target to ECF, IVS Disadvantages Oedema & fluid overload

9

10
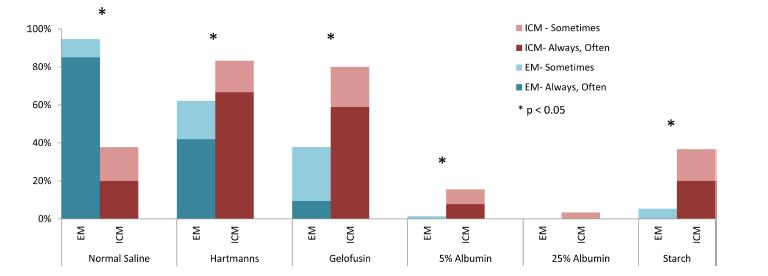
11 Why do we have Synthe>c colloids? Australia has free access to albumen, elsewhere expensive Colloids are manufactured to use in place of albumen Expensive Use driven by shareholders as expensive compared to crystalloid No evidence of benefit for colloids Huge varia>on between volume and type of fluids between clinicans, special>es and countries Most are delivered in saline
12 Albumen Remains circn 8-12 hrs, 50% IVS (5L) 50% ECS (12L), freely exchanged, half life 21 days Advantages: An>oxidant, Natural, Sugges>on of improved outcome in sepsis Buffer (half the anion gap) Transport pn - drugs, hormones, ions Disadvantages Blood product, expensive, may increase ICP(vs HES) Increased mortality in TBI -? as hypotonic Congenital absence confers no harm Nephro>cs do not go into APO - need change in hydrosta>c pressure too
 Expensive - ( 12.50-16.")

13 Starches 3 genera>ons, very different effects (elo- Haes, Haes- steril, hemohes, voluven - in 0.9% NaCl) Expensive - ( per 500ml) Large group, remain circ 2-12 hrs, KD Most widely used colloid in world, usu anaesthesia Accumulates in re>cular system renal impairment and pruri5s Coagulopathy - reduce vwf, 3rd genera>on do not effect
14 Gela>ns Anaphylaxis 0.03% In NS No evidence to support use, very few trials, emerging evidence of renal toxicity Gelofusion ml IVS 2-4 hours, 30 KD but - ve charge gives greater osmo>c effect Minimal metabolism, renal excre>on, cleared 3/7 plasma Minimal coagula>on effects un>l high mix (305 dilu>on), vwf/plt Haemaccel IVS 2 hours Renal excre>on, minimal metabolism Very high Ca++ load at 6.25 & cl at 145 (30ml Ca gluconate per 500ml)
15 Dextrans Developed WWII Remain circ 4-6 hrs Dextran 40 Improves rheology High allergy rate Marked an>coagulant - binds vwf and pnc Interferes with X match Dextran 70 Drama>c coagula>on effects equivalent heparin Prevents thromboembolism Improves microcircula>on
16 The great Fluid Debate: Colloid vs. crystalloid

17

18 RCT ICU Australia 6997 pts albumen in NS vs. NS End points death ICU, organ failure, ven>lated days, RRT no difference between two agents Important addi>onal findings: Colloid : crystalloid ra>o 1:1.4 not 1:3 s previously taught TBI mortality trend increased if used albumen as opposed to saline, fist study to show fluids alter mortality highly significant mortality 33 vs 20% P=0.003 Sep>c shock, non significant trend to increase survival with albumen resus as opposed to saline; need trial
19

20

21 FEAST NEJM 2011;354: RCT, Children sepsis & impaired perfusion, central Africa Excluded non- sep>c shock, gastroenteri>s, severe malnutri>on Interven>on groups: Albumen in saline 20-40ml/Kg vs 0.9% saline 20-40ml/Kg vs no bolus Fluids over one hour Primary end point Death at 48 hours, Mortality lower if no bolus fluid 10.6% vs. 10.5% vs. 7.3% RR 1.44 CI P=0.01 fro saline vs no bolus Startum B mortality 69% vs. 56% P=0.45 This study ques>ons the role of bolus therapy in fluids
22

23 7000 pts, ICU, 6% HES in NS (130/0.4 voluven) vs. NS powered to find 3.5% increase in mortality at 90 days Findings: HES vs. NS Mortality 18.0% vs. 17.0% P=0.26 RRT 7% vs. 5.8% RR 1.21 CI P=0.04 AKI 34.6% vs. 38.0% P=0.005 Adverse events 5.3 vs. 2.8% P<0.001
24

25
26
27 6S trial NEJM RCT 6% starch (HES 130/0.4) vs. Ringers acetate 26 Scandinavian ICU s, 798 pts, severe sepsis 1ry end point = death or RRT at day 90 primary end point, HES vs. Ringers 51% vs. 43% P=0.03 8% increase in mortality assoc starch use no difference at day 28 sugges>ng accumula>on of starch is the significant factor
28 Cochrane review 78 trials, 70 had mortality data Albumen 24 trials, 9220 pts, RR1.01 CI Starches, HES, 25 trials, 9147 pts, RR 1.10 CI Gela>ns, 11 trials, 506 pts, RR 0.91 CI (no change if Boldt s trials removed) Dextrans, 9 trials, 843 pts, RR Feb 2013

29


30 The great Fluid Debate: Which Crystalloid?
31 0.9% saline Not normal 200 million L annual consump>on! Osmolarity 308 (plasma , Na 154, Cl 154) Hyperchloraemic Commonest hospital cause acidosis is hyperchloraemia?significance of this Cause of acidosis rather than ph is what maters Chloride decreases renal blood flow, worsens renal func>on Pro- inflammatory Ques>on of worse outcomes in sepsis Useful where hypertonicity may be of benefit TBI, stroke, neurological illness
32 Hartmanns / Ringers Hyponatraemia 131, hypo osmolar 278, 281 Concern re cellular swelling, compartment syndrome, oedema, hyponatraemic encephalopathy Avoid post surgery, hyponatraemia May elevate lactate Advantages of low choride No adverse effects renal func>on, acid base
33 So why cant we just make fluid like plasma? The problem is bicarbonate is not stable in plas>c, needs to be stored glass So fluids need inorganic ions that body coverts to bicarbonate Hartmanns - lactate Plasmolyte - acetate & gluconate Answer is not simply to give HCO 3 as converts to CO 2 & this will require increased RR

34
35 Associa>on between chloride liberal vs chloride restrici>ve IV fluid administra>on and kidney injury in cri>cally ill adults. Bellomo et al JAMA ; Prospec>ve open label sequen>al period pilot trial 760 pts consequ>vely admited to ICU in control period vs. 773 pts admited during interven>on period Interven>on all chloride rich fluids (0.9% saline, 4% gela>ns, 4% albumen) restricted to specialist approval Std fluids were Hartmann solu>on, Plasmolyte 148 & salt poor albumen Results Mortality no difference AKI by RIFLE 14% vs. 8.4% (P<0.001) RRT 10% vs. 6.3% (P=0.005) Chloride restric-ve regieme assoc less AKI and RRT
36

 Vs.")
37 60734 pa>ents, 360 ICU USA NS mortality 20.2% vs. NS & balanced soln 17.7% (P<0.001) Vs. NS + colloid 24.2% (P<0.001) Vs. NS + bal + colloid 19.2% (P=0.401)


38
39
40

41
42

43


44 NICE 2013
45 Fluids and Cloxng Need ica > 0.5 for coagula>on, Mg also impt for coagula>on an>coagulants are in lower concentra>on than procoagulants in blood so at lower levels dilu>on alone is procoagulant Arterial clot is mainly plt dependent (plt <1% HCT) Venous clot/capillary ooze thrombin dependent and more effected by fluids Many colloids are an5coagulant and as such may increase bleeding
46 Transfusion in haemorrhage


47 Hypotensive resuscitation Fluid increases BP, dilutional anaemia/coag proteins, acidosis and crystalloid load assoc impaired tissue perfusion Pop the clot Clot reaches 80% ultimate tensile strength in first hour
48 Trauma - haemosta>c resuscita>on For the very few who are dying of blood loss Resus strategy targe>ng early coagulopathy to improve outcome via haemorrhage control Coagulopathy accompanies trauma TIC occurs minutes of injury and assoc 4 fold mortality increase
49 Haemosta>c resuscita>on Resus strategy targe>ng early coagulopathy to improve outcome via haemorrhage control Blood and blood product based fluid resus Whole blood or RBCs/FFP then +platelets/cryoppt Avoid crystalloids and catecholamines No RCT, retrospec>ve data Is bennefit from blood products or avoiding crystalloid?
 3% (US) require massive transfusion (50% blood use) Massive")
50 Trauma Transfusion 9% require transfusion 0.5% (UK) 3% (US) require massive transfusion (50% blood use) Massive transfusion carries mortality 30-60%
 (Borgman J Trauma 2007) Further military & civilian data Rajasekhar Crit care med 2011;39:1507-13 PRBCs > 14 days doubled mortality")
51 TIC and blood products MT data - FFP:RBC 1:1 vs. 1:8 reduced mortality by 60% 1:8 = 65%; 1:4 = 34%; 1:2.5 = 19% (p=o.oo1) (Borgman J Trauma 2007) Further military & civilian data Rajasekhar Crit care med 2011;39: PRBCs > 14 days doubled mortality Weinberg J trauma 2008
? Effect of TBI?? Underpowered as power cal to 10% mortality difference Significant difference in exanguina>on at 24 hours in 1:1:1 group, mortality 9.2 vs. 14.6%, (CI - 5.4/- 10.")
52 Mul>center RCT, major trauma, median ISS 26 Plasma:platelets:PRBC 1:1:1 (338 pa>ents) vs. 1:1:2 (342 pa>ents) 24 hour mortality 12.7% vs. 17.0%, P=0.12 (CI / 1.1); 30/7 mortality 22.4 vs 26.1% (CI - 10/2.7)? Effect of TBI?? Underpowered as power cal to 10% mortality difference Significant difference in exanguina>on at 24 hours in 1:1:1 group, mortality 9.2 vs. 14.6%, (CI - 5.4/- 10.4) Beter haemostsis in 1:1:1 group, 86% vs. 78%, p<0.001 JAMA Feb 2015

53
54 Liberal vs. restric>ve transfusion strategy GI bleed Non blinded single centre RCT, Acute upper GI bleed, target Hb 7 vs 10, 900 pts Exclude lower/ac>ve cardiovasular syndromes/extanguishing Did include liver diseases Endoscopy within 6 hours key to risk stra>fica>on Results: Restric>ve group had less blood, more pts had no transfusion Mortality at 6 weeks 9% 10 Hb vs 5% 7 Hb (less re- bleeding, lower adverse events) Why? Lower portal pressure, beter coagula>on similar trauma
55 Summary Oral fluids unless C/I Fluids are toxic drugs and colloids are more toxic than crystalloids and have no place outside clinical trials No ideal crytsalloid Blood product based resuscita>on paradyne in severe trauma
56 Summary Haemosta>c resuscita>on hypotension & 1:1:1 severe blood loss in severe trauma Tolerate anaemia in most illness (Hb >7, > 10 IHD,? Neurological disease) including GI bleed Top up transfusion very rarely needed


57

58
59 Anemia and blood transfusion in cri>cally ill pa>ents JAMA 2002;288: pts, ICU, 146 ICU s in W Europe, prospec>ve observa>onal study ICU (18.5 vs. 10.1% P<0.001) & overall (19 vs. 14.9% P<0.001) mortality higher in pts who had vs. had not had blood transfusion Matched pts 28/7 mortality 22.7 vs % P=0.02 Associa>on but may not be cause and effect
60
61 The Evidence around Blood Transfusion Neutral SOAP pts - ICU, europe - showed no harm from transfusion?leucoreduc>on accounts for difference fro other trials Favours not transfusing ACS pts, post hoc analysis from GUSTO Iib, PURSUIT, PARAGON; transfusion assoc increased mortality, esp if hct > 25% (retrospec>ve analysis, (JAMA 2004;292: ) Post op: 8787 pts post NOF, observa>onal trial, 42% transfused, data avilable only for hb > 80 g/l, transfusion did not alter 30/7 or 90/7 mortality (JAMA 1998;279: ) CRIT study USA, 4892 pts, 213 hospitals, ICU study, 44% ICU pts received >= 1 unit PRBC s, number transfusions independently assoc mortality but does not necessarily imply cause & effect (crit care 2004;32:39-52)
62 The Evidence around blood Transfusion Favor's higher Hb TRICC inves>gators crit care pts, anaemia (Hb<100) assoc increased risk death in pts with heart disease (Am J Resp crit Care Med 1997;155: ) ACS - Retrospec>ve study 78974pts > 65yrs with AMI, lower Hct assoc increased mortality, tranfusion trigger of 110gL (HCT<33%) assoc lower 30/7 mortality (NEJM 2001;345: ) CCF NY 3/4, increase Hb 103 to 129 assoc improved LF EF and lower mortality (J Am Coll Card 2001;29: ) Common factor is IHD/cardiac disease

63
64 Top up transfusion
65 Blood Transfusion Severe anaemia kills, blood harms Anaemia effects - DO2, pulse, infec>on, APO Hb 40-50gL well tolerated in normovolaemic young fit pts if reached slowly as adequate DO2 In young fit adult at rest adequate DO2 can be met with Hb 3 (increases in CO and extrac>on) (JAMA 1998; 279:217-21) Jehovas witness do badly Hb 6 mort 16x Don't confuse minimal tolerated Hb with clinically acceptable Hb in elderly diseased ac>vely bleeding pt - they can not increase CO and selec>vely dilate organ perfusion to compensate
66 Dangers of Blood Transfusion Mechanical Air embolism, microembolism, fluid overload Anaphylac>c/oid reac>ons Infec>on HIV HABCV prion malaria (s>ll 1: HIV, 1: HCV) Incompa>bility and haemolysis ABO resus duffy kell TRIM (transfusion related immunomodula>on) Increased renal allograk survival, enhanced metasts>c spread cancer, increased post op infec>on TRALI (transfusion related lung injury)
67 838 pts, euvolaemic, ini>al Hb<9 within 72 hours admission Randomised to Restric>ve group transfused if Hb < 7 & maintained 7-9 Liberal group transfused if Hb < 10 and Hb maintained g/ dl 1ry end point 30/7 mortality 18.7% vs. 23.3% P=0.11 If less sick, APACHE <=20 then 8.7 vs. 16.1% P=0.03, in favour of restric>ve group If < 55 yrs old 5.7% vs. 13.0%, P=0.02 But not if cardiac disease, 20.5% vs. 22.2%, P=0.69 Mortality rate during hospitaliza>on lower in restric>ve group, 22.2% vs. 28.1% P=0.05
68
69 So when to Transfuse Target Hb 70 in young, 100 in elderly/cvs disease Weigh up risks and benefits using Phase of illness (acute, high VO2, ongoing losses) Co morbidity - IHD, CVD Age Predicted cause Probably wise to use leuco- reduced RBCs
Fluids in ICU. JMO teaching 5th July 2016
 Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
What is the Role of Albumin in Sepsis? An Evidenced Based Affair. Justin Belsky MD PGY3 2/6/14
 What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What works in sepsis. Topics. EGDT: Severe Sepsis/ Shock. Sepsis
 What works in sepsis Eric Schmidt, MD Denver Health Medical Center University of Colorado School of Medicine Topics Understanding and implemen@ng early goal directed therapy (EGDT) Ac@vated Protein C should
What works in sepsis Eric Schmidt, MD Denver Health Medical Center University of Colorado School of Medicine Topics Understanding and implemen@ng early goal directed therapy (EGDT) Ac@vated Protein C should
JOURNAL CLUB: THE FLUIDS DEBATE. Veronica Ueckermann
 JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
Intravenous Fluid Therapy in Critical Illness
 Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
Kristan Staudenmayer, MD Stanford University, Stanford, CA
 Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
INTRAVENOUS FLUID THERAPY. Tom Heaps Consultant Acute Physician
 INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
J v /A = L p { (P c - P i ) σ (π p - π i ) } 7/13/14. Current Concepts and Controversies in Small Animal Critical Care. Goals and Objec.
 σ (π p - π i ) } 7/13/14. Current Concepts and Controversies in Small Animal Critical Care. Goals and Objec.") The Crystalloid vs. Colloid Controversy Continues Karl E. Jandrey, DVM, MAS, DAVCECC Associate Professor of Clinical Small Animal Emergency & Critical Care 2 nd Annual Conti Symposium, UC Irvine August
The Crystalloid vs. Colloid Controversy Continues Karl E. Jandrey, DVM, MAS, DAVCECC Associate Professor of Clinical Small Animal Emergency & Critical Care 2 nd Annual Conti Symposium, UC Irvine August
Blood transfusions in sepsis, the elderly and patients with TBI
 Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
What is the right fluid to use?
 What is the right fluid to use? L McIntyre Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute Centre for Transfusion Research CCCF, November 2, 2016 Disclosures
What is the right fluid to use? L McIntyre Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute Centre for Transfusion Research CCCF, November 2, 2016 Disclosures
Red Cell Transfusion triggers: A moving target When, who, and how much?
 Red Cell Transfusion triggers: A moving target When, who, and how much? Tim Walsh Professor of Critical Care, Edinburgh University A transfusion threshold of 70 g/l or below, with a target Hb range of
Red Cell Transfusion triggers: A moving target When, who, and how much? Tim Walsh Professor of Critical Care, Edinburgh University A transfusion threshold of 70 g/l or below, with a target Hb range of
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Fluid Treatments in Sepsis: Meta-Analyses
 Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Getting smart with fluids in the critically ill. NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia
 Getting smart with fluids in the critically ill NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia Isotonic Solutions and Major Adverse Renal Events Trial
Getting smart with fluids in the critically ill NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia Isotonic Solutions and Major Adverse Renal Events Trial
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR
 Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Fluids in Sepsis Less is more. Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth,
 Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
I Suggest Abnormal Saline
 I Suggest Abnormal Saline Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta CCCF Oct 27, 2015 2015 Disclosures Salary support: Canada/Alberta government Grant support: Canada/Alberta
I Suggest Abnormal Saline Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta CCCF Oct 27, 2015 2015 Disclosures Salary support: Canada/Alberta government Grant support: Canada/Alberta
EVIDENCE BASED RED CELL TRANSFUSION. Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System
 EVIDENCE BASED RED CELL TRANSFUSION Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System HISTORY Blood transfusion works (ie: red cell transfusion saves lives). based on
EVIDENCE BASED RED CELL TRANSFUSION Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System HISTORY Blood transfusion works (ie: red cell transfusion saves lives). based on
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Modern fluid therapy. Anders Perner. Dept of Intensive Care, Rigshospitalet, University of Copenhagen
 Modern fluid therapy Anders Perner Dept of Intensive Care, Rigshospitalet, University of Copenhagen Scandinavian Critical Care Trials Group www.ssai.info/research/scctg Intensive Care Medicine www.icmjournal.esicm.org
Modern fluid therapy Anders Perner Dept of Intensive Care, Rigshospitalet, University of Copenhagen Scandinavian Critical Care Trials Group www.ssai.info/research/scctg Intensive Care Medicine www.icmjournal.esicm.org
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Early Management of the Patient with Acute GI Bleeding
 Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
INTRAVENOUS FLUIDS. Ahmad AL-zu bi
 INTRAVENOUS FLUIDS Ahmad AL-zu bi Types of IV fluids Crystalloids colloids Crystalloids Crystalloids are aqueous solutions of low molecular weight ions,with or without glucose. Isotonic, Hypotonic, & Hypertonic
INTRAVENOUS FLUIDS Ahmad AL-zu bi Types of IV fluids Crystalloids colloids Crystalloids Crystalloids are aqueous solutions of low molecular weight ions,with or without glucose. Isotonic, Hypotonic, & Hypertonic
12/29/2014. IV/IO Therapy & Fluid Administration. Objectives. Cleansing of the soul
 IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
FLUID RESUSCITATION SUMMARY
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Fluid resuscitation in specific patient populations: sepsis and traumatic brain injury
 Fluid resuscitation in specific patient populations: sepsis and traumatic brain injury John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University
Fluid resuscitation in specific patient populations: sepsis and traumatic brain injury John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University
Dr Tushar Mahambrey. Consu ltant Critical Care Med icine & Anaesthetics St Helens and Knowsley N H S teaching hospitals Liverpool
 Dr Tushar Mahambrey Consu ltant Critical Care Med icine & Anaesthetics St Helens and Knowsley N H S teaching hospitals Liverpool History Why do we give blood Why does anaemia occur in critical care patients
Dr Tushar Mahambrey Consu ltant Critical Care Med icine & Anaesthetics St Helens and Knowsley N H S teaching hospitals Liverpool History Why do we give blood Why does anaemia occur in critical care patients
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
Patient Blood Management: Enough is Enough
 Patient Blood Management: Enough is Enough Richard Benjamin, MBChB, PhD, FRCPath Professor of Pathology Georgetown University Medical Center Washington, D.C. Chief Medical Officer Cerus Corporation Concord,
Patient Blood Management: Enough is Enough Richard Benjamin, MBChB, PhD, FRCPath Professor of Pathology Georgetown University Medical Center Washington, D.C. Chief Medical Officer Cerus Corporation Concord,
Resuscitation fluids in critical care
 Resuscitation fluids in critical care John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University of New South Wales St George Hospitals, Sydney
Resuscitation fluids in critical care John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University of New South Wales St George Hospitals, Sydney
Transfusions in Acute Care Too Little?
 Transfusions in Acute Care Too Little? Keyvan Karkouti MD FRCPC MSc Associate Professor Department of Anesthesia; Department of Health Policy, Management, and Evaluation; University of Toronto Scientist
Transfusions in Acute Care Too Little? Keyvan Karkouti MD FRCPC MSc Associate Professor Department of Anesthesia; Department of Health Policy, Management, and Evaluation; University of Toronto Scientist
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
Fluid assessment, monitoring and therapy for the acute nurse
 Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid Resuscitation in Sepsis. A Literature Review
 Fluid Resuscitation in Sepsis A Literature Review "On the floor lay a girl of slender make and juvenile height, but with the face of a superannuated hag... The colour of her countenance was that of lead
Fluid Resuscitation in Sepsis A Literature Review "On the floor lay a girl of slender make and juvenile height, but with the face of a superannuated hag... The colour of her countenance was that of lead
IV Fluids Do you know what you are doing?
 IV Fluids Do you know what you are doing? Probably not Dr Mike Stroud Gastroenterologist and Senior Lecturer in Medicine & Nutrition Southampton University Hospitals Foundation Trust CG 174 December 2013
IV Fluids Do you know what you are doing? Probably not Dr Mike Stroud Gastroenterologist and Senior Lecturer in Medicine & Nutrition Southampton University Hospitals Foundation Trust CG 174 December 2013
Approach to Severe Sepsis. Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore
 Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Fluid management of Neurosurgical patient, Recent update
 Fluid management of Neurosurgical patient, Recent update Catholic University of Daegu Department of anesthesiology and pain medicine Taeha. Ryu. Fluid management of Neurosurgical patient The major aims.
Fluid management of Neurosurgical patient, Recent update Catholic University of Daegu Department of anesthesiology and pain medicine Taeha. Ryu. Fluid management of Neurosurgical patient The major aims.
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes. Richard Beale
 Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Blood transfusion. General surgery department of SGMU Lecturer ass. Khilgiyaev R.H.
 Blood transfusion General surgery department of SGMU Sources of blood Donors Own blood of patient (autoreinfusion): autoreinfusion of blood from cavities (haemotorax, haemoperitoneum) in case of acute
Blood transfusion General surgery department of SGMU Sources of blood Donors Own blood of patient (autoreinfusion): autoreinfusion of blood from cavities (haemotorax, haemoperitoneum) in case of acute
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Transfusion Triggers. Richard Soutar January 2012
 Transfusion Triggers Richard Soutar January 2012 1 Educational objectives: To understand the risks of transfusion - the known, the uncertain and unknown To understand the fear of the unknown in Transfusion
Transfusion Triggers Richard Soutar January 2012 1 Educational objectives: To understand the risks of transfusion - the known, the uncertain and unknown To understand the fear of the unknown in Transfusion
My Bloody Talk. Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne
 My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
Fluids and Lactate. A/Prof Peter Morley
 Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
CPR What Works, What Doesn t
 Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Fluid balance in Critical Care
 Fluid balance in Critical Care By Dr HP Shum Nephrologist and Critical Care Physician Department of Intensive Care, PYNEH Fluid therapy is a critical aspect of initial acute resuscitation in critically
Fluid balance in Critical Care By Dr HP Shum Nephrologist and Critical Care Physician Department of Intensive Care, PYNEH Fluid therapy is a critical aspect of initial acute resuscitation in critically
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Transfusion for the sickest ICU patients: Are there unanswered questions?
 Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Supplementary Online Content
 Supplementary Online Content Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney
Supplementary Online Content Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Bicarbonate in the NICU
 OMG Bicarbonate in the NICU A Useless Therapy? At first I thought I was going to have to refute the paper Then I got into it and thought: I m so confused Then I learned a lot HOPEFULLY I CAN LEARN YOU
OMG Bicarbonate in the NICU A Useless Therapy? At first I thought I was going to have to refute the paper Then I got into it and thought: I m so confused Then I learned a lot HOPEFULLY I CAN LEARN YOU
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
3/16/15. Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation. Obligatory Traumatologist Slide
 Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
Management of the Bleeding Trauma Patient: Concepts in Damage Control Resuscitation Courtney Sommer, MD MPH Duke Trauma Symposium March 12, 2015 Obligatory Traumatologist Slide In 2010 trauma was leading
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
Hydroxyethyl starch and bleeding
 Hydroxyethyl starch and bleeding Anders Perner Dept. of Intensive Care, Rigshospitalet University of Copenhagen Scandinavian Critical Care Trials Group Intensive Care Medicine COIs Ferring, LFB - Honoraria
Hydroxyethyl starch and bleeding Anders Perner Dept. of Intensive Care, Rigshospitalet University of Copenhagen Scandinavian Critical Care Trials Group Intensive Care Medicine COIs Ferring, LFB - Honoraria
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Anaemia in the ICU: Is there an alternative to using blood transfusion?
 Anaemia in the ICU: Is there an alternative to using blood transfusion? Tim Walsh Professor of Critical Care, Edinburgh University World Health Organisation grading of the severity of anaemia Grade of
Anaemia in the ICU: Is there an alternative to using blood transfusion? Tim Walsh Professor of Critical Care, Edinburgh University World Health Organisation grading of the severity of anaemia Grade of
Citrate Anticoagulation
 Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
HHS. Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours. Page 1 of 2 AFFIX PATIENT LABEL ! INFORM DIABETES TEAM OF ADMISSION!
 Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours Page 1 of 2 Time of Arrival Loca8on Date / / Diagnosis the characteris8c features of a person with HHS are a) Hypovolaemia b) Marked
Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours Page 1 of 2 Time of Arrival Loca8on Date / / Diagnosis the characteris8c features of a person with HHS are a) Hypovolaemia b) Marked
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED. Surgical Grand Rounds
 Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
Salty Solutions or Salty Problems? Outline. Outline 29/04/2013
 Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
بسم اهلل الرحمن الرحيم
 بسم اهلل الرحمن الرحيم o Always we try to maintain a Homeostasis mechanism. Homeostasis : maintenance of internal environment. How?! The environment,that cells live in it,must be in a constant natural
بسم اهلل الرحمن الرحيم o Always we try to maintain a Homeostasis mechanism. Homeostasis : maintenance of internal environment. How?! The environment,that cells live in it,must be in a constant natural
Transfusion triggers in acute coronary syndromes: The MINT trial
 Transfusion triggers in acute coronary syndromes: The MINT trial Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Objectives Review evidence on transfusion triggers
Transfusion triggers in acute coronary syndromes: The MINT trial Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Objectives Review evidence on transfusion triggers
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
Fluid Therapy and Outcome: Balance Is Best
 The Journal of ExtraCorporeal Technology Fluid Therapy and Outcome: Balance Is Best Sara J. Allen, FANZCA, FCICM Department of Anaesthesia and the Cardiothoracic and Vascular Intensive Care Unit, Auckland
The Journal of ExtraCorporeal Technology Fluid Therapy and Outcome: Balance Is Best Sara J. Allen, FANZCA, FCICM Department of Anaesthesia and the Cardiothoracic and Vascular Intensive Care Unit, Auckland
Welcome! While we wait, please open PollEv.com/jhhicu012
 Welcome! While we wait, please open PollEv.com/jhhicu012 Login username jhhicu012 Password jhhicupoll OR Text JHHICU012 to 0427541357 once to join the poll response and be able to answer polls by SMS Same
Welcome! While we wait, please open PollEv.com/jhhicu012 Login username jhhicu012 Password jhhicupoll OR Text JHHICU012 to 0427541357 once to join the poll response and be able to answer polls by SMS Same
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
"Small Volume" Resuscitation for Trauma Cases : PRO Aspects
 "Small Volume" Resuscitation for Trauma Cases : PRO Aspects Jim Holliman, M.D., F.A.C.E.P. Program Manager, Afghanistan Health Care Sector Reconstruction Project Center for Disaster and Humanitarian Assistance
"Small Volume" Resuscitation for Trauma Cases : PRO Aspects Jim Holliman, M.D., F.A.C.E.P. Program Manager, Afghanistan Health Care Sector Reconstruction Project Center for Disaster and Humanitarian Assistance
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Fine-tuning Management in Dengue Fever
 Fine-tuning Management in Dengue Fever Annual Scientific Meeting On Intensive Care 16 August 2014 Eg Kah Peng University of Malaya Medical Centre Rise In Dengue Infection New Straits Times 8 July 2014
Fine-tuning Management in Dengue Fever Annual Scientific Meeting On Intensive Care 16 August 2014 Eg Kah Peng University of Malaya Medical Centre Rise In Dengue Infection New Straits Times 8 July 2014
MASSIVE HAEMORRHAGE POLICY. ABMU HB Transfusion Team
 MASSIVE HAEMORRHAGE POLICY ABMU HB Transfusion Team Objec@ves To define the responsibili@es and roles of the Clinical team and the Haematology Department in the management of MASSIVE HAEMORRHAGE To describe
MASSIVE HAEMORRHAGE POLICY ABMU HB Transfusion Team Objec@ves To define the responsibili@es and roles of the Clinical team and the Haematology Department in the management of MASSIVE HAEMORRHAGE To describe
SEPSIS: Seeing Through the. W. Graham Carlos MD, MSCR, ATSF, FACP
 SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
Goal Directed Therapy : Liberal vs Restrictive Transfusion.. Syafri Kamsul Arif
 Goal Directed Therapy : Liberal vs Restrictive Transfusion. Syafri Kamsul Arif Sepsis Perioperative EGDT PGDT PGDT Protocol Stroke volume optimization with fluid protocol SVV or PPV based GDT Protocol
Goal Directed Therapy : Liberal vs Restrictive Transfusion. Syafri Kamsul Arif Sepsis Perioperative EGDT PGDT PGDT Protocol Stroke volume optimization with fluid protocol SVV or PPV based GDT Protocol
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY. Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center
 UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center DISCLOSURE STATEMENT OF FINANCIAL INTEREST I, Vera Wilson,
UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center DISCLOSURE STATEMENT OF FINANCIAL INTEREST I, Vera Wilson,
VI.2 ELEMENTS FOR A PUBLIC SUMMARY (VOLUVEN 10%)
") VI.2 ELEMENTS FOR A PUBLIC SUMMARY (VOLUVEN 10%) VI.2.1 OVERVIEW OF DISEASE EPIDEMIOLOGY Hypovolaemia is a state of decreased or reduced circulating blood volume which can be caused by a number of medical
VI.2 ELEMENTS FOR A PUBLIC SUMMARY (VOLUVEN 10%) VI.2.1 OVERVIEW OF DISEASE EPIDEMIOLOGY Hypovolaemia is a state of decreased or reduced circulating blood volume which can be caused by a number of medical
L : Line and Tube อ นตรายป องก นได จากการให สารน า
 L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
TXA. Things Change. Tranexamic Acid TXA. Resuscitation 2017 TXA In The ED March 31, MAST Trousers. High Flow IV Fluids.
 Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
2 Liters. Goal: Basic Algorithm Volume Resuscitation in Trauma. Initial Fluids. Blood. Where do Blood Products Come From?
 Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Goal: Basic Algorithm Volume Resuscitation in Trauma Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 Initial
Albumin: rationale, use and evidence
 Albumin: rationale, use and evidence Michaël Chassé, MD, MSc, FRCPC Intensivist, CHU de Québec PhD Candidate, Epidemiology, uottawa Research Fellow, Clinical Epidemiology Program Ottawa Hospital Research
Albumin: rationale, use and evidence Michaël Chassé, MD, MSc, FRCPC Intensivist, CHU de Québec PhD Candidate, Epidemiology, uottawa Research Fellow, Clinical Epidemiology Program Ottawa Hospital Research
Administration of blood components. Tina Parker - Transfusion Practitioner
 . Administration of blood components Tina Parker - Transfusion Practitioner Red Cells Each unit contains 250-350mls Preserved with glucose and Mannitol to keep the correct tension Lasts 35 days from midnight
. Administration of blood components Tina Parker - Transfusion Practitioner Red Cells Each unit contains 250-350mls Preserved with glucose and Mannitol to keep the correct tension Lasts 35 days from midnight
Kay Barrera MD. Surgery Grand Rounds June 19, 2014 SUNY Downstate
 Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use
Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Kay Barrera MD Surgery Grand Rounds June 19, 2014 SUNY Downstate Outline Why are we talking about this SCORE expectations When do we use