Traumatic Injuries to the Foot and Ankle
|
|
|
- Kelly Damon Griffith
- 6 years ago
- Views:
Transcription
1 Traumatic Injuries to the Foot and Ankle Dr. Joseph N. Daniel Clinical Associate Professor of Orthopaedic Surgery Foot and Ankle Service, The Rothman Institute Thomas Jefferson University Hospital Philadelphia, PA
2 Smith-Nephew Wright Medical Disclosure
3 Calcaneus Fractures Talus Fractures Lisfranc Complex Injuries


4 CALCANEUS FRACTURES
5 Objectives Anatomy Mechanisms of Injury Imaging Fracture Patterns Treatment Options / Timing of Surgery

6 Anatomy Lateral Superior
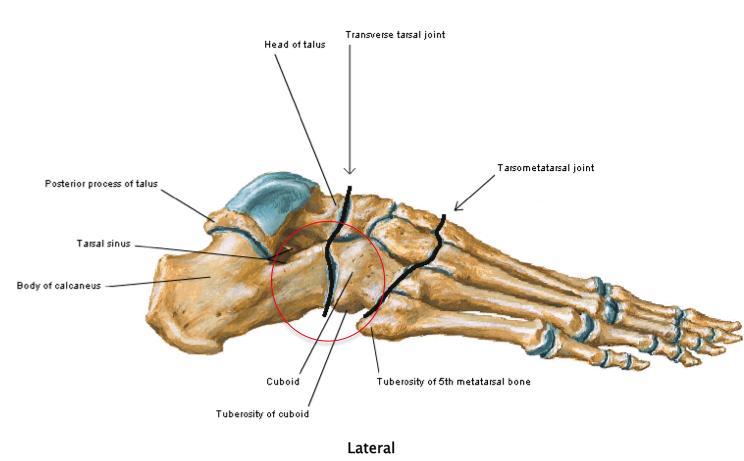
7 Anatomy
8 Mechanisms of Injury Axial load fall from height MVA Inversion / eversion injuries Forceful muscular contractions
9 Imaging Assumed WB AP, lateral and Mortise views ankle Assumed WB AP, lateral and oblique views foot Harris heel view




10 Imaging

11 Bohler s angle Gissane s angle Neutral triangle
12 Imaging CT scan 2 mm transaxial, coronal, sagittal and 3-D reconstruction views Semi-coronal CT = most important view

13 Fracture Patterns Direction of force Quality of bone Position of foot Extra- Articular 25% Intra- Articular 75%
14 Extra-Articular Fractures



15 Anterior Process Fracture comminuted frx


16 Calcaneal Body Fracture




17 Sustentaculum Tali Fracture FHL






18


19



20 Calcaneal Tuberosity Fracture


21 Peroneal Tubercle Fracture, Lateral Process Fracture, Medial Calcaneal Process Fracture


22 Intra-Articular Fractures
23 Intra-Articular Fractures Associated injuries: spine frx thoracolumbar lower extremity injuries bilateral frx
24


25 Primary Fracture Line
26 secondary frx line secondary frx line


27 lateral wall blow-out CCJ extension medial wall shortening varus mal-alignment


28 joint depression type tongue type Bohler s angle Gissane s angle


29 Sanders Classification

30 Intra-Articular Fracture Management Fracture pattern: displacement (2 mm) classification Open fracture Relative contraindications: edema / blisters DM severe PVD smoking elderly with minimal demands non-compliance surgeon experience
31 Non-op CRUA Perc. Stabilization ORIF Primary Arthrodesis +/- ORIF
 relative")
32 Sanders Classification Non-operative: Type I (non-displaced / minimally displaced frx) relative contraindications
33 Non-op CRUA Perc. Stabilization ORIF Primary Arthrodesis +/- ORIF
34 Open Calcaneus Fracture I & D traumatic wounds until clean medial / plantar < 4cm epithelium re-approximated stable 7 days ORIF Yes Yes Yes wound location No No No lateral perc. stabilization Thornton; Foot Ankle Int; 27: , 2006


35 Open Calcaneus Fracture


36 Open Calcaneus Fracture
37 Non-op CRUA Perc. Stabilization ORIF Primary Arthrodesis +/- ORIF


38 Sanders Classification Operative: ORIF Type II, III, IV primary arthrodesis +/- ORIF Type IV


39 Formal ORIF Primary subtalar arthrodesis +/- ORIF

40 plantar foot Achilles tendon



41 Formal ORIF


42 ORIF with primary subtalar arthrodesis
43 Calcaneus Fractures Treatment Summary Non-operative: non-displaced / minimally displaced frx relative contraindications Operative: displaced extra-articular frx with skin tenting; impending skin compromise anterior process frx with > 25% CCJ involvement calcaneal body frx with width; height; arch disruption displaced intra-articular frx certain open frx
44 Fracture Non-op CRUA Perc. ORIF Primary Arthrodesis anterior process calcaneal body < 25% CCJ X > 25% CCJ width; height susten. tali X PF + I displacement calcaneal tuberosity X skin tenting; impending compromise skin tenting; impending compromise peron. tub. / med. calc. process X joint depression type Sanders I Sanders II, III, IV Sanders IV tongue type Sanders I open X X Sanders II, III, IV Sanders IV
45 Calcaneus Fractures Treatment Summary Emergent: compartment syndrome* open fracture* skin tenting; impending skin compromise cannot reduce frx-dislocation Urgent (within 3 wks): displaced intra-articular frx displaced extra-articular frx anterior process frx with > 25% CCJ involvement Elective: massive edema; medical comorbidities non-reconstructable intraarticular frx symptomatic frx nonunion / malunion
46 Talus Fractures
47 Objectives Incidence Anatomy Mechanisms of Injury Imaging Fracture Patterns Treatment Options / Timing of Surgery
48 Incidence 3% of all foot fractures < 1% of all fractures Types: Neck: 50% Body: 7-38% Head: 10%
49 Anatomy Talus Vital part of ankle + subtalar complex of joints Vertical WB forces transferred to horizontal support structures of foot Small; irregular shape No muscular attachments 70% surface covered with articular cartilage Vascular supply tenuous
50 Anatomy Articulations btwn: Tibial plafond and dome of talus Posterior facet of talus with calcaneus Medial and anterior facets of talus and calcaneus and btwn head of talus and posterior surface of navicular
51 Anatomy Articulations: Posterior facet Inferior surface talus = concave Superior surface calcaneus = convex Anterior + middle facets Inferior surface talus = convex Superior surface calcaneus = concave
52 Anatomy Subtalar joint motion Screw mechanism Talonavicular joint motion Ball and socket mechanism
53 Mechanisms of Injury Fracture Location Mechanism Event Talar neck axial compression + DF high energy trauma Talar Head DF + I MVA; fall from ht Talar Body axial compression high energy trauma Lateral Process DF + I snowboarding Posteromedial pronation + DF sports; MVA; fall from ht
54 Imaging Assumed WB AP, lateral and Mortise views ankle Assumed WB AP, lateral and oblique views foot
55 Imaging CT scan 1.5 mm transaxial, coronal, sagittal and 3-D reconstruction views
56 Fracture Patterns Talar neck fracture: MOI: axial compression and DF Hawkins classification Type I: non-displaced; no sublux or disloc of STJ Type II: displaced; ankle nl; STJ sublux or disloc Type III: complete disloc of ankle + STJ Type IV: complete disloc of ankle + STJ + TNJ
57 Fracture Patterns Talar head fracture: MOI: DF + I Involves: middle facet + TNJ


58 Fracture Patterns Talar body fracture: MOI: axial load
59 Fracture Patterns Lateral process fracture: AKA snowboarder s frx MOI: DF + I


60 Fracture Patterns Posteromedial fracture MOI: direct impact; pronation + DF



61 Treatment Talar neck fracture: ORIF
62 Treatment Talar head fracture:


63 Treatment Talar body fracture: ORIF +/- medial malleolar osteotomy
64 Treatment Posteromedial fracture MOI: direct impact; pronation + DF
65 Lisfranc Complex Injuries
66 Objectives Incidence Anatomy Mechanisms of Injury Clinical Examination Imaging Treatment Options / Timing of Surgery Complications
67 Incidence Uncommon 0.2% of all frx 55,000 Lisfranc injuries annually Does not include ligamentous injuries
68 Incidence M > F Avg age: mid 30 s Up to 40% missed Most commonly on multi-trauma patients
69 Anatomy and Biomechanics Tarsometatarsal Joints (TMTJ s) Articulation btwn 1 st 3 MT and their respective cuneiforms Articulations btwn 4 th and 5 th MT and cuboid Stability osseous ligamentous tendinous
70 Anatomy and Biomechanics osseous configuration Greatest stability Coronal plane and transverse plane
71 Anatomy and Biomechanics osseous configuration Coronal plane stability TMTJ s form symmetric Roman arch Wider dorsal wedge shape 2d and 3d MT bases middle and lateral cuneiforms 2d MT base
72 Anatomy and Biomechanics osseous configuration Transverse plane stability 2d MT Longest Keystone Surrounded by 5 bones limits medial lateral translation
73 Anatomy and Biomechanics ligamentous configuration Stronger plantarly MT s attached to more proximal articulations Lesser MT s attached via interosseous ligaments No IM ligament bwtn 1 st and 2d MT s

74 Anatomy and Biomechanics ligamentous configuration 1 st MT attached only to medial cuneiform 2d MT attached to medial cuneiform via Lisfranc ligament 2 separate bands in 22% of population Dorsal weaker Plantar stronger
75 Anatomy and Biomechanics tendinous configuration Tibialis Anterior Insertion: medial aspect proximal 1 st MT Peroneus Longus Insertion: plantar lateral aspect 1 st MT
76 Anatomy and Biomechanics primary stabilizers 2d MT Keystone Surrounded by 5 adjacent bones 1 st and 3d MT Recessed between medial, middle and lateral cuneiforms Lisfranc ligament Plantar 2d MT base to medial cuneiform
77 Anatomy and Biomechanics secondary stabilizers Plantar fascia Intrinsic muscles Insertions of Tibialis Posterior, Tibialis Anterior and Peroneus Longus
78 Mechanisms of Injury MVA 65% Fall Crushing Injury Twisting Injury
79 Mechanisms of Injury Forces Direct Indirect
80 Mechanisms of Injury Direct Forces Less common Crushing injury Outcome: Fracture communition Soft tissue damage Compartment syndrome
81 Mechanisms of Injury F distal to Lisfranc complex plantar displacement of MT bases F proximal to Lisfranc complex dorsal displacement of MT bases
82 Mechanisms of Injury Indirect Forces More common Rotational Injury Foot: sl. equinus MT: firmly planted body projected over forefoot twisting + rotation + abduction
83 Mechanisms of Injury Indirect Forces Rotational injury Failure under tension dorsally Continued abduction leads to: 2d metatarsal base dislocation Lateral displacement of lesser metatarsals Compression fracture of cuboid

84 Mechanisms of Injury Dorsal displacement of MT bases
85 Mechanisms of Injury Direct or indirect forces: Perforating branch of dorsalis pedis aa may disrupt Hemmorhage with d interstitial fluid P compartment syndrome
86 Clinical Examination Routine foot and ankle examination NV Sensation Motor power Capillary refill PROM ankle, subtalar, Chopart complexes Forefoot examination
87 Clinical Examination Specific Foot and Ankle Examination Tenderness, crepitus and deformity at Lisfranc complex Compartments soft TTP compressible
88 Clinical Examination Specific Foot and Ankle Examination Skin integrity Tenting Frx blisters Ecchymosis Plantar mid foot» Classic finding Pronation abduction maneuver
89 Imaging Assumed WB AP, lateral and 30 IO images If unable to perform WB images and?? midfoot injury, repeat films in 2 wks in WB posture
90 Imaging AP: Frx pathology

91 Imaging AP: Frx pathology Fleck sign Avulsion frx off medial base of 2d MT or lateral border of medial cuneiform
92 Imaging AP: Frx pathology Fleck sign Avulsion frx off medial base of 2d MT Alignment
93 Imaging Alignment: Medial border 2d MT with medial border middle cuneiform
94 Imaging Alignment: 1 st intermetatarsal space continuous with space btwn medial and middle cuneiforms Nl: 1.3 mm
95 Imaging Lateral: Frx pathology
96 Imaging Lateral: Frx pathology Evaluate for dorsal displacement of MTs relative to cuneiforms
97 Imaging Lateral: Frx pathology Evaluate for dorsal displacement of MTs relative to cuneiforms Change in distance btwn plantar aspect medial cuneiform and 5 th MT
98 Imaging 30 IO: Frx pathology
99 Imaging Alignment: Lateral border 3d MT with lateral border of lateral cuneiform
100 Imaging Alignment: Medial border 4 th MT with medial border cuboid

101 Imaging Alignment: 2d IM space continuous with space btwn lateral cuneiform and cuboid
102 Imaging Stress Radiographs: Ligamentous injury with equivocal examination Ankle block anesthesia or O.R. setting

103 Imaging Malreduction: > 15 abduction of 1 st MT > 2 mm lateral shift of at least 1 MT > 2 mm

104 Imaging Magnetic Resonance Imaging: Clear diastasis on WB AP image do not MRI Equivocal or nl radiographs with pronounced mechanism and/or clinical examination Consider MRI dorsal plantar

105 Imaging CT Scan: Image all Lisfranc complex injuries 1.5 mm transaxial, sagittal and coronal cuts in assumed WB position
106 Treatment Optimal Treatment: Anatomic stable reduction of TMTJ s
107
108 Treatment Midfoot Sprain Stable: SLNWBC until asymptomatic then SLWC or boot with WBAT X 6-8 wks Activity level to tolerance
109 Treatment Midfoot Sprain Unstable: >15 1 st MT abduction >2 mm lateral shift of any MT ORIF vs. arthrodesis
110 Treatment Midfoot Sprain Equivocal: MRI No tear or partial tear of Lisfranc ligament (< 50%)» treat as sprain > 50% tear of Lisfranc ligament» ORIF» arthrodesis
111 Treatment Operative: Indications: Any degree of displacement of frx of TMTJ s (unstable) Pure ligamentous injury with instability
112 Treatment Operative: Timing of surgery based upon: Presence of compartment syndrome Degree of soft tissue swelling Can be performed up to 6 wks after injury
113 Treatment Fracture Fixation Options: K-wire ORIF arthrodesis
114 Treatment K-wire: Easy to insert Easy to back out Rarely used as sole means of fixation Useful with: Severe frx comminution Compartment syndrome with poor soft tissue envelope Can be performed up to 6 wks after injury

115 Treatment Fracture Fixation Options: ORIF 3.5 or 4.0 screws Cannulated Non-cannulated

116 Treatment Fracture Fixation Options: ORIF Mini-fragment plates




117 Treatment Fracture Fixation Options: Arthrodesis Joint preparation and mode of fixation different
118 Treatment Lee et al. Foot and Ankle International May 2004

119 Treatment Pure Ligamentous Injury Options: K-wire K-wire + screw fixation Screw fixation
120 Treatment Operative: In absence of compartment syndrome, ORIF Algorithm of stabilization based on column involvement
121 Treatment Operative: Isolated medial column or medial + middle column injury, reconstruct medial to lateral

122
123


124

125 3 2 1

126


127


128
129 Treatment Operative: Lateral column injury Ex fix lateral column Stabilize lateral column Stabilize medial column Stabilize middle column



130

131


132

133


134


135



136
137 Rehabilitation NWB 6-12 wks HWR s/p ORIF at wks Retention of HW? WBAT Custom B/L MLA support x 6 mo Avoid high impact L.E. athletic activity x 3 mo


138 Complications Acute: Compartment syndrome Long term: Post-traumatic arthritis 30% Pes planus + forefoot abduction

139 Thank you BE ASHAMED TO DIE UNTIL YOU HAVE DONE SOMETHING GOOD FOR MANKIND Dr. Vernon Johnson, American Pastor during the Revolutionary War
Peggers Super Summaries: Foot Injuries
 Lisfranc Injury ANATOMY Roman arch with recessed 2 nd MT base AP medial side of intermediate cuneiform to 2 nd MT base Oblique medial side of lateral cuneiform with 3 rd MT base and 4 th with medial boarder
Lisfranc Injury ANATOMY Roman arch with recessed 2 nd MT base AP medial side of intermediate cuneiform to 2 nd MT base Oblique medial side of lateral cuneiform with 3 rd MT base and 4 th with medial boarder
MIDFOOT INJURIES-ARE WE UNDERTREATING IT? Mr Rajiv Limaye Mr Prasad Karpe University Hospital of North Tees 3 rd Foot and Ankle Symposium
 MIDFOOT INJURIES-ARE WE UNDERTREATING IT? Mr Rajiv Limaye Mr Prasad Karpe University Hospital of North Tees 3 rd Foot and Ankle Symposium Introduction Increasing sports injuries RTA and traumatic injuries
MIDFOOT INJURIES-ARE WE UNDERTREATING IT? Mr Rajiv Limaye Mr Prasad Karpe University Hospital of North Tees 3 rd Foot and Ankle Symposium Introduction Increasing sports injuries RTA and traumatic injuries
Foot Injuries. Dr R B Kalia
 Foot Injuries Dr R B Kalia Overview Dramatic impact on the overall health, activity, and emotional status More attention and aggressive management Difficult appendage to study and diagnose. Aim- a stable
Foot Injuries Dr R B Kalia Overview Dramatic impact on the overall health, activity, and emotional status More attention and aggressive management Difficult appendage to study and diagnose. Aim- a stable
Radiographic Evaluation of Calcaneal Fractures. Kali Luker, PGY-1
 Radiographic Evaluation of Calcaneal Fractures Kali Luker, PGY-1 Anatomy Extraarticular Fractures Involve body, anterior process or tuberosity Treated with immobilization and NWB x 6 wks UNLESS Displaced
Radiographic Evaluation of Calcaneal Fractures Kali Luker, PGY-1 Anatomy Extraarticular Fractures Involve body, anterior process or tuberosity Treated with immobilization and NWB x 6 wks UNLESS Displaced
Anatomy of Foot and Ankle
 Anatomy of Foot and Ankle Surface anatomy of the ankle & foot Surface anatomy of the ankle & foot Medial orientation point medial malleous sustentaculum tali tuberosity of navicular TA muscle TP muscle
Anatomy of Foot and Ankle Surface anatomy of the ankle & foot Surface anatomy of the ankle & foot Medial orientation point medial malleous sustentaculum tali tuberosity of navicular TA muscle TP muscle
5 COMMON INJURIES IN THE FOOT & ANKLE
 5 COMMON INJURIES IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MECHANISM OF INJURY HOW DID IT HAPPEN? HIGH ENERGY VS LOW ENERGY DIRECTION OF FORCES INVOLVED LIVING
5 COMMON INJURIES IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MECHANISM OF INJURY HOW DID IT HAPPEN? HIGH ENERGY VS LOW ENERGY DIRECTION OF FORCES INVOLVED LIVING
Talus Fractures: When and Why on Screws and Plates
 Talus Fractures: When and Why on Screws and Plates Frank A. Liporace, MD Associate Professor Director of Orthopaedic Research New York University / Hospital for Joint Diseases, NY, NY Director Orthopaedic
Talus Fractures: When and Why on Screws and Plates Frank A. Liporace, MD Associate Professor Director of Orthopaedic Research New York University / Hospital for Joint Diseases, NY, NY Director Orthopaedic
Fractures of the Calcaneus
 Fractures of the Calcaneus Anthony T. Sorkin, M.D. Rockford Orthopedic Trauma Service Rajeev Garapati, MD Illinois Bone and Joint Institute Assistant Clinical Professor University of Illinois at Chicago
Fractures of the Calcaneus Anthony T. Sorkin, M.D. Rockford Orthopedic Trauma Service Rajeev Garapati, MD Illinois Bone and Joint Institute Assistant Clinical Professor University of Illinois at Chicago
Complexities surrounding Lisfranc injuries
 Complexities surrounding Lisfranc injuries Lisfranc injuries are commonly associated with sporting injuries and are easily diagnosed with severe midfoot pain, swelling, deformity and inability to bear
Complexities surrounding Lisfranc injuries Lisfranc injuries are commonly associated with sporting injuries and are easily diagnosed with severe midfoot pain, swelling, deformity and inability to bear
radiologymasterclass.co.uk
 http://radiologymasterclass.co.uk Hip X-ray anatomy - Normal AP (anterior-posterior) Shenton's line is formed by the medial edge of the femoral neck and the inferior edge of the superior pubic ramus Loss
http://radiologymasterclass.co.uk Hip X-ray anatomy - Normal AP (anterior-posterior) Shenton's line is formed by the medial edge of the femoral neck and the inferior edge of the superior pubic ramus Loss
Introduction. The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking.
 The ankle 1 Introduction The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking. OSTEOLOGRY The term ankle refers primarily to the talocrural joint,
The ankle 1 Introduction The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking. OSTEOLOGRY The term ankle refers primarily to the talocrural joint,
Surgery-Ortho. Fractures of the tibia and fibula. Management. Treatment of low energy fractures. Fifth stage. Lec-6 د.
 Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Selected Fractures of the Foot: Diagnosis and Treatment.
 Selected Fractures of the Foot: Diagnosis and Treatment www.fisiokinesiterapia.biz Overview Forefoot Fractures Lisfranc MT 5 th MT Hindfoot Fractures Calcaneus Talus Tarsometatarsal (Lisfranc s) Fracture
Selected Fractures of the Foot: Diagnosis and Treatment www.fisiokinesiterapia.biz Overview Forefoot Fractures Lisfranc MT 5 th MT Hindfoot Fractures Calcaneus Talus Tarsometatarsal (Lisfranc s) Fracture
Midfoot - Reduction & Fixation - ORIF - screw fixation - AO Surgery Reference. ORIF - screw fixation
 Midfoot - TMT (Lisfranc) injury 1. Diagnosis ORIF - screw fixation Authors Mechanism of the injury Tarso-metatarsal (Lisfranc) injuries may be caused by direct or indirect forces. Direct forces include
Midfoot - TMT (Lisfranc) injury 1. Diagnosis ORIF - screw fixation Authors Mechanism of the injury Tarso-metatarsal (Lisfranc) injuries may be caused by direct or indirect forces. Direct forces include
X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle.
 Radiographic Evaluation of the Ankle.") X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle www.fisiokinesiterapia.biz Anatomy Complex hinge joint Articulations among: Fibula Tibia Talus Tibial plafond Distal tibial articular surface
X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle www.fisiokinesiterapia.biz Anatomy Complex hinge joint Articulations among: Fibula Tibia Talus Tibial plafond Distal tibial articular surface
EASILY MISSED FOOT AND ANKLE FRACTURES NORDIC TRAUMA COURSE 2016, AARHUS
 EASILY MISSED FOOT AND ANKLE FRACTURES NORDIC TRAUMA COURSE 2016, AARHUS Ken F. Linnau, MD, MS Emergency Radiology Harborview Medical Center University of Washington Seattle, WA Thanks to Claire K Sandstrom
EASILY MISSED FOOT AND ANKLE FRACTURES NORDIC TRAUMA COURSE 2016, AARHUS Ken F. Linnau, MD, MS Emergency Radiology Harborview Medical Center University of Washington Seattle, WA Thanks to Claire K Sandstrom
Computed Tomographic Imaging of Foot and Ankle trauma
 Computed Tomographic Imaging of Foot and Ankle trauma Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of Medicine San Diego, California CT of Foot and Ankle Trauma
Computed Tomographic Imaging of Foot and Ankle trauma Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of Medicine San Diego, California CT of Foot and Ankle Trauma
Hany El-Rashidy and Anand Vora
 Chapter 194 Lisfranc Injuries Chapter 194 Lisfranc Injuries Hany El-Rashidy and Anand Vora 8 ICD-9 CODE 838.03 Lisfranc (Tarsometatarsal) Fracture-Dislocation Key Concepts The Lisfranc joint represents
Chapter 194 Lisfranc Injuries Chapter 194 Lisfranc Injuries Hany El-Rashidy and Anand Vora 8 ICD-9 CODE 838.03 Lisfranc (Tarsometatarsal) Fracture-Dislocation Key Concepts The Lisfranc joint represents
Clarification of Terms
 Clarification of Terms The plantar aspect of the foot refers to the role or its bottom The dorsal aspect refers to the top or its superior portion The ankle and foot perform three main functions: 1. shock
Clarification of Terms The plantar aspect of the foot refers to the role or its bottom The dorsal aspect refers to the top or its superior portion The ankle and foot perform three main functions: 1. shock
LISFRANC FRACTURE-DISLOCATION
 LISFRANC FRACTURE-DISLOCATION Napoleon at Mont St. Bernard, Jacques-Louis David, 1800, Oil on Canvas, Musee du Louvre, Paris. This is Jacques-Louis David s immortal depiction of a young Napoleon Bonaparte,
LISFRANC FRACTURE-DISLOCATION Napoleon at Mont St. Bernard, Jacques-Louis David, 1800, Oil on Canvas, Musee du Louvre, Paris. This is Jacques-Louis David s immortal depiction of a young Napoleon Bonaparte,
Ankle Tendons in Athletes. Laura W. Bancroft, M.D.
 Ankle Tendons in Athletes Laura W. Bancroft, M.D. Outline Protocols Normal Anatomy Tendinopathy, partial and complete tears Posterior tibial, Flexor Hallucis Longus, Achilles, Peroneal and Anterior Tibial
Ankle Tendons in Athletes Laura W. Bancroft, M.D. Outline Protocols Normal Anatomy Tendinopathy, partial and complete tears Posterior tibial, Flexor Hallucis Longus, Achilles, Peroneal and Anterior Tibial
Managing Tibialis Posterior Tendon Injuries
 Managing Tibialis Posterior Tendon Injuries by Thomas C. Michaud, DC Published April 1, 2015 by Dynamic Chiropractic Magazine Tibialis posterior is the deepest, strongest, and most central muscle of the
Managing Tibialis Posterior Tendon Injuries by Thomas C. Michaud, DC Published April 1, 2015 by Dynamic Chiropractic Magazine Tibialis posterior is the deepest, strongest, and most central muscle of the
Section 3: Foot Subluxations and Dislocations
 Section 3: Foot Subluxations and Dislocations Case Study F: Lisfranc s Midfoot Dislocation Clinical History: J.K. a 28 year old female presents complaining of a painful right foot. She sustained an acute
Section 3: Foot Subluxations and Dislocations Case Study F: Lisfranc s Midfoot Dislocation Clinical History: J.K. a 28 year old female presents complaining of a painful right foot. She sustained an acute
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program
 Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Copyright 2012 by The McGraw-Hill Companies, Inc. All rights reserved. McGraw-Hill/Irwin
 CHAPTER 8: THE LOWER EXTREMITY: KNEE, ANKLE, AND FOOT KINESIOLOGY Scientific Basis of Human Motion, 12 th edition Hamilton, Weimar & Luttgens Presentation Created by TK Koesterer, Ph.D., ATC Humboldt State
CHAPTER 8: THE LOWER EXTREMITY: KNEE, ANKLE, AND FOOT KINESIOLOGY Scientific Basis of Human Motion, 12 th edition Hamilton, Weimar & Luttgens Presentation Created by TK Koesterer, Ph.D., ATC Humboldt State
Injuries of the Foot and Ankle. Introduction. Introduction 10/2/2009. Bryan Lapinski, MD
 Injuries of the Foot and Ankle Bryan Lapinski, MD Introduction The average person takes 1 million steps per year Approximately 30 bones in the foot and ankle are subjected to forces of 3 7 times body weight
Injuries of the Foot and Ankle Bryan Lapinski, MD Introduction The average person takes 1 million steps per year Approximately 30 bones in the foot and ankle are subjected to forces of 3 7 times body weight
SURGICAL AND APPLIED ANATOMY
 Página 1 de 9 Copyright 2001 Lippincott Williams & Wilkins Bucholz, Robert W., Heckman, James D. Rockwood & Green's Fractures in Adults, 5th Edition SURGICAL AND APPLIED ANATOMY Part of "47 - ANKLE FRACTURES"
Página 1 de 9 Copyright 2001 Lippincott Williams & Wilkins Bucholz, Robert W., Heckman, James D. Rockwood & Green's Fractures in Adults, 5th Edition SURGICAL AND APPLIED ANATOMY Part of "47 - ANKLE FRACTURES"
DEPARTMENT OF TRAUMATOLOGY AND HAND SURGERY INSTITUTE OF MUSCULOSKELETAL SURGERY ANKLE AND FOOT INJURIES
 DEPARTMENT OF TRAUMATOLOGY AND HAND SURGERY INSTITUTE OF MUSCULOSKELETAL SURGERY ANKLE AND FOOT INJURIES Presenter: Dr George Ayerh ENGLISH PROGRAM LECTURES EN_11/A - 2018 TOPICS I. Part: Ankle & Foot
DEPARTMENT OF TRAUMATOLOGY AND HAND SURGERY INSTITUTE OF MUSCULOSKELETAL SURGERY ANKLE AND FOOT INJURIES Presenter: Dr George Ayerh ENGLISH PROGRAM LECTURES EN_11/A - 2018 TOPICS I. Part: Ankle & Foot
Copyright 2004, Yoshiyuki Shiratori. All right reserved.
 Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
No disclosures relevant to this topic Acknowledgement: some clinical pictures were obtained from the OTA fracture lecture series and AO fracture
 CALCANEUS FRACTURES No disclosures relevant to this topic Acknowledgement: some clinical pictures were obtained from the OTA fracture lecture series and AO fracture lecture series INCIDENCE 2% of all fractures
CALCANEUS FRACTURES No disclosures relevant to this topic Acknowledgement: some clinical pictures were obtained from the OTA fracture lecture series and AO fracture lecture series INCIDENCE 2% of all fractures
17/10/2017. Foot and Ankle
 17/10/2017 Alicia M. Yochum RN, DC, DACBR, RMSK Foot and Ankle Plantar Fasciitis Hallux Valgus Deformity Achilles Tendinosis Posterior Tibialis Tendon tendinopathy Stress Fracture Ligamentous tearing Turf
17/10/2017 Alicia M. Yochum RN, DC, DACBR, RMSK Foot and Ankle Plantar Fasciitis Hallux Valgus Deformity Achilles Tendinosis Posterior Tibialis Tendon tendinopathy Stress Fracture Ligamentous tearing Turf
Outline. Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t
 Ankle Injuries Outline Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t Anatomy: Ankle Mortise Bony Anatomy Lateral Ligament Complex Medial Ligament Complex Ankle Sprains
Ankle Injuries Outline Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t Anatomy: Ankle Mortise Bony Anatomy Lateral Ligament Complex Medial Ligament Complex Ankle Sprains
2017 SAFSA CONGRESS PROGRAMME
 2017 SAFSA CONGRESS PROGRAMME THURSDAY, MAY 25 07h45 07h55: WELCOME & INTRODUCTIONS Forefoot I: Hallux Valgus and Lesser Toes (08h00-10h00 Lectures) 08h00 08h30: Surgical Management of Hallux Valgus Rippstein,
2017 SAFSA CONGRESS PROGRAMME THURSDAY, MAY 25 07h45 07h55: WELCOME & INTRODUCTIONS Forefoot I: Hallux Valgus and Lesser Toes (08h00-10h00 Lectures) 08h00 08h30: Surgical Management of Hallux Valgus Rippstein,
Extraarticular Lateral Ankle Impingement
 Extraarticular Lateral Ankle Impingement Poster No.: C-1282 Congress: ECR 2016 Type: Educational Exhibit Authors: C. Cevikol; Keywords: Trauma, Diagnostic procedure, MR, CT, Musculoskeletal system, Musculoskeletal
Extraarticular Lateral Ankle Impingement Poster No.: C-1282 Congress: ECR 2016 Type: Educational Exhibit Authors: C. Cevikol; Keywords: Trauma, Diagnostic procedure, MR, CT, Musculoskeletal system, Musculoskeletal
Foot & Ankle Disorders
 Foot & Ankle Disorders Hillingdon PGMC 6-7-2013 Htwe Zaw FRCS (Tr&Orth) Consultant Foot & Ankle and Trauma Surgeon Hillingdon Hospitals NHS Foundation Trust Overview Anatomy: hindfoot-midfoot coupling
Foot & Ankle Disorders Hillingdon PGMC 6-7-2013 Htwe Zaw FRCS (Tr&Orth) Consultant Foot & Ankle and Trauma Surgeon Hillingdon Hospitals NHS Foundation Trust Overview Anatomy: hindfoot-midfoot coupling
Calcaneal Fractures: Lateral Extensile Incision
 Calcaneal Fractures: Lateral Extensile Incision AS Flemister JR, MD University of Rochester Disclosures I have no financial disclosures 1/27/2016 2 Mechanism Axial Loading Fall From Height MVA BAD SOFT
Calcaneal Fractures: Lateral Extensile Incision AS Flemister JR, MD University of Rochester Disclosures I have no financial disclosures 1/27/2016 2 Mechanism Axial Loading Fall From Height MVA BAD SOFT
High Ankle Sprains: Diagnosis & Treatment
 High Ankle Sprains: Diagnosis & Treatment Mark J. Mendeszoon, DPM, FACFAS, FACFAOM Precision Orthopaedic Specialties University Regional Hospitals Advanced Foot & Ankle Fellowship- Director It Is Only
High Ankle Sprains: Diagnosis & Treatment Mark J. Mendeszoon, DPM, FACFAS, FACFAOM Precision Orthopaedic Specialties University Regional Hospitals Advanced Foot & Ankle Fellowship- Director It Is Only
The University Of Jordan Faculty Of Medicine FOOT. Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan
 The University Of Jordan Faculty Of Medicine FOOT Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan Tarsal Tunnel Syndrome Due to compression of Tibial nerve as it travels through the
The University Of Jordan Faculty Of Medicine FOOT Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan Tarsal Tunnel Syndrome Due to compression of Tibial nerve as it travels through the
Dr Nabil khouri MD. MSc. Ph.D
 Dr Nabil khouri MD. MSc. Ph.D Foot Anatomy The foot consists of 26 bones: 14 phalangeal, 5 metatarsal, and 7 tarsal. Toes are used to balance the body. Metatarsal Bones gives elasticity to the foot in
Dr Nabil khouri MD. MSc. Ph.D Foot Anatomy The foot consists of 26 bones: 14 phalangeal, 5 metatarsal, and 7 tarsal. Toes are used to balance the body. Metatarsal Bones gives elasticity to the foot in
BIOMECHANICS OF ANKLE FRACTURES
 BIOMECHANICS OF ANKLE FRACTURES William R Reinus, MD MBA FACR Significance of Ankle Fractures Most common weight-bearing Fx 70% of all Fxs Incidence is increasing Bimodal distribution Men 15-24 Women over
BIOMECHANICS OF ANKLE FRACTURES William R Reinus, MD MBA FACR Significance of Ankle Fractures Most common weight-bearing Fx 70% of all Fxs Incidence is increasing Bimodal distribution Men 15-24 Women over
ABC of Emergency Radiology
 l ja ) $% _2) < j> ~~~~~~~~~~~~~~~~~foot ABC of Emergency Radiology THE FOOT D A Nicholson, D O'Keeffe, P A Driscoll Accurate clinical assessment of injuries to the foot will avoid unnecessary exposure
l ja ) $% _2) < j> ~~~~~~~~~~~~~~~~~foot ABC of Emergency Radiology THE FOOT D A Nicholson, D O'Keeffe, P A Driscoll Accurate clinical assessment of injuries to the foot will avoid unnecessary exposure
The plantar aponeurosis
 Anatomy of the foot The plantar aponeurosis Is a triangular thickening of the deep fascia Its apex is attached to the medial and lateral tubercles of the calcaneum. The base of the aponeurosis divides
Anatomy of the foot The plantar aponeurosis Is a triangular thickening of the deep fascia Its apex is attached to the medial and lateral tubercles of the calcaneum. The base of the aponeurosis divides
Temporary bridge plating of the medial column in Chopart and Lisfranc injuries
 Temporary bridge plating of the medial column in Chopart and Lisfranc injuries by Alaa Mansour DPM 1*, Lawrence Fallat DPM, FACFAS 2 The Foot and Ankle Online Journal 10 (1): 5 Severe traumatic injuries
Temporary bridge plating of the medial column in Chopart and Lisfranc injuries by Alaa Mansour DPM 1*, Lawrence Fallat DPM, FACFAS 2 The Foot and Ankle Online Journal 10 (1): 5 Severe traumatic injuries
Review relevant anatomy of the foot and ankle. Learn the approach to examining the foot and ankle
 Objectives Review relevant anatomy of the foot and ankle Learn the approach to examining the foot and ankle Learn the basics of diagnosis and treatment of ankle sprains Overview of other common causes
Objectives Review relevant anatomy of the foot and ankle Learn the approach to examining the foot and ankle Learn the basics of diagnosis and treatment of ankle sprains Overview of other common causes
Recurrent Fifth Metatarsal Fractures. Carol Frey MD Fellowship Co - Director West Coast Sports Medicine Foundation UCLA Manhattan Beach, California
 Recurrent Fifth Metatarsal Fractures Carol Frey MD Fellowship Co - Director West Coast Sports Medicine Foundation UCLA Manhattan Beach, California General 5th MT fracture fairly common Mechanism: Hindfoot
Recurrent Fifth Metatarsal Fractures Carol Frey MD Fellowship Co - Director West Coast Sports Medicine Foundation UCLA Manhattan Beach, California General 5th MT fracture fairly common Mechanism: Hindfoot
Disclosures. Syndesmosis Injury. Syndesmosis Ligaments. Objectives. Mark M. Casillas, M.D.
 Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
Paul Alley MD,DPM,MS,FACS,FAAOS,BFD Eby Orthopaedics,Jasper,Indiana
 Paul Alley MD,DPM,MS,FACS,FAAOS,BFD Eby Orthopaedics,Jasper,Indiana Very common Bone=fractures Description (cracked,broke,busted,or smashed) A=anatomic area of bone eg: head,neck,shaft B=bone involved
Paul Alley MD,DPM,MS,FACS,FAAOS,BFD Eby Orthopaedics,Jasper,Indiana Very common Bone=fractures Description (cracked,broke,busted,or smashed) A=anatomic area of bone eg: head,neck,shaft B=bone involved
Annual Surgical Conference LisFranc Fractures. Zeeshan S. Husain, DPM, FACFAS, FASPS. Great Lakes Foot and Ankle Institute September 21, 2018
 Annual Surgical Conference 2018 LisFranc Fractures Zeeshan S. Husain, DPM, FACFAS, FASPS Great Lakes Foot and Ankle Institute September 21, 2018 None Disclosures Jacques LisFranc 1790 1847 History LisFranc
Annual Surgical Conference 2018 LisFranc Fractures Zeeshan S. Husain, DPM, FACFAS, FASPS Great Lakes Foot and Ankle Institute September 21, 2018 None Disclosures Jacques LisFranc 1790 1847 History LisFranc
Commonly Missed Foot and Ankle Conditions. David Miller, DPM AMG Podiatry
 Commonly Missed Foot and Ankle Conditions David Miller, DPM AMG Podiatry Lisfranc Injuries Wide spectrum of injuries High energy Subtle subluxation which could be easily missed injuries Men are 2-4x s
Commonly Missed Foot and Ankle Conditions David Miller, DPM AMG Podiatry Lisfranc Injuries Wide spectrum of injuries High energy Subtle subluxation which could be easily missed injuries Men are 2-4x s
Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity
 Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity Mr Amit Chauhan Mr Prasad Karpe Ms Maire-claire Killen Mr Rajiv Limaye University Hospital of North
Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity Mr Amit Chauhan Mr Prasad Karpe Ms Maire-claire Killen Mr Rajiv Limaye University Hospital of North
EDL EHL. Extensor Hallucis Longus L5 Extensor Digitorum longus L5,1 Peroneus Tertius L5 1 Extensor Digitorum Brevis S1,2 [like intrinsic muscle]
![EDL EHL. Extensor Hallucis Longus L5 Extensor Digitorum longus L5,1 Peroneus Tertius L5 1 Extensor Digitorum Brevis S1,2 [like intrinsic muscle]](/thumbs/78/77875930.jpg "EDL EHL. Extensor Hallucis Longus L5 Extensor Digitorum longus L5,1 Peroneus Tertius L5 1 Extensor Digitorum Brevis S1,2 [like intrinsic muscle]") ANATOMY OF ANKLE AND FOOT Lateral aspect: [Dorsal medial to lateral= dorsal under extensor retinaculum] Tibialis Anterior EHL Artery [Dorsal pedal A] and Anterior tibial N EDL Peroneus Tertius Behind the
ANATOMY OF ANKLE AND FOOT Lateral aspect: [Dorsal medial to lateral= dorsal under extensor retinaculum] Tibialis Anterior EHL Artery [Dorsal pedal A] and Anterior tibial N EDL Peroneus Tertius Behind the
SUBTLE CAVUS IN SPORTS INJURIES
 SUBTLE CAVUS IN SPORTS INJURIES MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA NON-NEUROMUSCULAR NORMAL VARIANT: 20-25% INCIDENCE LEDOUX, ET AL. FAI 24, 2003 FOREFOOT-DRIVEN / MORE SUBTLE
SUBTLE CAVUS IN SPORTS INJURIES MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA NON-NEUROMUSCULAR NORMAL VARIANT: 20-25% INCIDENCE LEDOUX, ET AL. FAI 24, 2003 FOREFOOT-DRIVEN / MORE SUBTLE
FIBULAR & SYNDESMOSIS MALUNIONS
 FIBULAR & SYNDESMOSIS MALUNIONS MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MORTISE INHERENTLY UNSTABLE LATERAL MALLEOLUS ACTS AS BUTTRESS / POST RESIST LATERAL TRANSLATION OF TALUS
FIBULAR & SYNDESMOSIS MALUNIONS MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MORTISE INHERENTLY UNSTABLE LATERAL MALLEOLUS ACTS AS BUTTRESS / POST RESIST LATERAL TRANSLATION OF TALUS
Case. 15 Y old boy presented with pain in the foot. No history of injury or any constitutional symptoms. Your diagnosis?
 Case 15 Y old boy presented with pain in the foot. No history of injury or any constitutional symptoms Your diagnosis? Diagnosis: Calcaneo-navicular tarsal coalition. C sign Talar beaking Ant eaters nose
Case 15 Y old boy presented with pain in the foot. No history of injury or any constitutional symptoms Your diagnosis? Diagnosis: Calcaneo-navicular tarsal coalition. C sign Talar beaking Ant eaters nose
The Leg. Prof. Oluwadiya KS
 The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
Foot. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Foot Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Dorsum of the Foot Sole of the Foot Plantar aponeurosis It is a triangular thickening of deep fascia in the sole of the foot Attachments:
Foot Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Dorsum of the Foot Sole of the Foot Plantar aponeurosis It is a triangular thickening of deep fascia in the sole of the foot Attachments:
Index. Clin Sports Med 23 (2004) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Clin Sports Med 23 (2004) 169 173 Index Note: Page numbers of article titles are in boldface type. A Achilles enthesopathy, calcaneal spur with, 133 clinical presentation of, 135 136 definition of, 131
Clin Sports Med 23 (2004) 169 173 Index Note: Page numbers of article titles are in boldface type. A Achilles enthesopathy, calcaneal spur with, 133 clinical presentation of, 135 136 definition of, 131
Closed Reduction and Internal Fixation of Lisfranc Fracture Dislocations
 Closed Reduction and Internal Fixation of Lisfranc Fracture Dislocations Anish R. Kadakia, Mark S. Myerson, and Milap Patel Contents Mechanism of Injury... 2 Radiographic Evaluation... 3 Classification...
Closed Reduction and Internal Fixation of Lisfranc Fracture Dislocations Anish R. Kadakia, Mark S. Myerson, and Milap Patel Contents Mechanism of Injury... 2 Radiographic Evaluation... 3 Classification...
Imaging of Ankle and Foot pain
 Imaging of Ankle and Foot pain Pramot Tanutit, M.D. Department of Radiology Faculty of Medicine, Prince of Songkla University 1 Outlines Plain film: anatomy Common causes of ankle and foot pain Exclude:
Imaging of Ankle and Foot pain Pramot Tanutit, M.D. Department of Radiology Faculty of Medicine, Prince of Songkla University 1 Outlines Plain film: anatomy Common causes of ankle and foot pain Exclude:
Merete PlantarMAX Lapidus Plate Surgical Technique. Description of Plate
 Merete PlantarMAX Lapidus Plate Surgical Technique Description of Plate Merete Medical has designed the PlantarMax; a special Plantar/Medial Locking Lapidus plate which places the plate in the most biomechanically
Merete PlantarMAX Lapidus Plate Surgical Technique Description of Plate Merete Medical has designed the PlantarMax; a special Plantar/Medial Locking Lapidus plate which places the plate in the most biomechanically
Injuries to the lower extremity II Aree Tanavalee MD Associate Professor Department of Orthopaedics Faculty of Medicine Chulalongkorn University
 Injuries to the lower extremity II Aree Tanavalee MD Associate Professor Department of Orthopaedics Faculty of Medicine Chulalongkorn University Topics Fracture of the shaft of the femur Fractures around
Injuries to the lower extremity II Aree Tanavalee MD Associate Professor Department of Orthopaedics Faculty of Medicine Chulalongkorn University Topics Fracture of the shaft of the femur Fractures around
Physical Examination of the Foot & Ankle
 Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Cavus Foot: Subtle and Not-So-Subtle AOFAS Resident Review Course September 28, 2013
 Cavus Foot: Subtle and Not-So-Subtle Course September 28, 2013 Matthew M. Roberts, MD Associate Professor of Clinical Orthopaedic Surgery Co-Chief, Foot and Ankle Service Hospital for Special Surgery Disclosure
Cavus Foot: Subtle and Not-So-Subtle Course September 28, 2013 Matthew M. Roberts, MD Associate Professor of Clinical Orthopaedic Surgery Co-Chief, Foot and Ankle Service Hospital for Special Surgery Disclosure
ANKLE JOINT ANATOMY 3. TALRSALS = (FOOT BONES) Fibula. Frances Daly MSc 1 CALCANEUS 2. TALUS 3. NAVICULAR 4. CUBOID 5.
 Fibula. Frances Daly MSc 1 CALCANEUS 2. TALUS 3. NAVICULAR 4. CUBOID 5.") ANKLE JOINT ANATOMY The ankle joint is a synovial joint of the hinge type. The joint is formed by the distal end of the tibia and medial malleolus, the fibula and lateral malleolus and talus bone. It is
ANKLE JOINT ANATOMY The ankle joint is a synovial joint of the hinge type. The joint is formed by the distal end of the tibia and medial malleolus, the fibula and lateral malleolus and talus bone. It is
THE JOURNAL OF NUCLEAR MEDICINE Vol. 56 No. 3 March 2015 Rauscher et al.
 Supplemental Figure 1 Correlation analysis of tracer between and subsequent as assessed by SUV max in focal lesions (A). x-axis displays quantitative values as obtained by, and y-axis displays corresponding
Supplemental Figure 1 Correlation analysis of tracer between and subsequent as assessed by SUV max in focal lesions (A). x-axis displays quantitative values as obtained by, and y-axis displays corresponding
Columbia/NYOH FOOT and ANKLE ROTATION-SPECIFIC OBJECTIVES
 Updated 2/8/10 Columbia/NYOH FOOT and ANKLE ROTATION-SPECIFIC OBJECTIVES INTERPERSONAL AND COMMUNICATION SKILLS Resident will at all times demonstrate behavior that is beyond reproach. Residents must be
Updated 2/8/10 Columbia/NYOH FOOT and ANKLE ROTATION-SPECIFIC OBJECTIVES INTERPERSONAL AND COMMUNICATION SKILLS Resident will at all times demonstrate behavior that is beyond reproach. Residents must be
What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne
 What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne We don t know!! Population Studies 2300 children aged 4-13 years Shoe wearers Flat foot 8.6% Non-shoe wearers
What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne We don t know!! Population Studies 2300 children aged 4-13 years Shoe wearers Flat foot 8.6% Non-shoe wearers
Posterior Tibialis Tendon Dysfunction & Repair
 1 Posterior Tibialis Tendon Dysfunction & Repair Surgical Indications and Considerations Anatomical Considerations: The posterior tibialis muscle arises from the interosseous membrane and the adjacent
1 Posterior Tibialis Tendon Dysfunction & Repair Surgical Indications and Considerations Anatomical Considerations: The posterior tibialis muscle arises from the interosseous membrane and the adjacent
Arthroscopy Of the Ankle.
 Arthroscopy Of the Ankle www.fisiokinesiterapia.biz Ankle Arthroscopy Anatomy Patient setup Portal placement Procedures Complications Anatomy Portals Anterior Anteromedial Anterolateral Anterocentral Posterior
Arthroscopy Of the Ankle www.fisiokinesiterapia.biz Ankle Arthroscopy Anatomy Patient setup Portal placement Procedures Complications Anatomy Portals Anterior Anteromedial Anterolateral Anterocentral Posterior
EVOS MINI with IM Nailing
 Case Series Dr. John A. Scolaro EVOS MINI with IM Nailing A series of studies Introduction Intramedullary nailing has become the standard for many long bone fractures. Fracture reduction prior to nail
Case Series Dr. John A. Scolaro EVOS MINI with IM Nailing A series of studies Introduction Intramedullary nailing has become the standard for many long bone fractures. Fracture reduction prior to nail
5 COMMON CONDITIONS IN THE FOOT & ANKLE
 5 COMMON CONDITIONS IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA IN A NUTSHELL ~ ALL ANATOMY & BIOMECHANICS >90% OF CONDITIONS IN FOOT & ANKLE DIAGNISED FROM GOOD
5 COMMON CONDITIONS IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA IN A NUTSHELL ~ ALL ANATOMY & BIOMECHANICS >90% OF CONDITIONS IN FOOT & ANKLE DIAGNISED FROM GOOD
Fractures and dislocations around elbow in adult
 Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
The Lower Limb VII: The Ankle & Foot. Anatomy RHS 241 Lecture 7 Dr. Einas Al-Eisa
 The Lower Limb VII: The Ankle & Foot Anatomy RHS 241 Lecture 7 Dr. Einas Al-Eisa Ankle joint Synovial, hinge joint Allow movement of the foot in the sagittal plane only (1 degree of freedom): dorsiflexion:
The Lower Limb VII: The Ankle & Foot Anatomy RHS 241 Lecture 7 Dr. Einas Al-Eisa Ankle joint Synovial, hinge joint Allow movement of the foot in the sagittal plane only (1 degree of freedom): dorsiflexion:
Foot and Ankle Update
 Foot and Ankle Update 2019 Instructional Course Hiro Tanaka It s your on-call weekend Objectives We are going to apply evidence based treatment for 2 patients who are admitted under your care 1. Dislocated
Foot and Ankle Update 2019 Instructional Course Hiro Tanaka It s your on-call weekend Objectives We are going to apply evidence based treatment for 2 patients who are admitted under your care 1. Dislocated
Index. B Backslap technique depth assessment, 82, 83 diaphysis distal trocar, 82 83
 Index A Acromial impingement, 75, 76 Aequalis intramedullary locking avascular necrosis, 95 central humeral head, 78, 80 clinical and functional outcomes, 95, 96 design, 77, 79 perioperative complications,
Index A Acromial impingement, 75, 76 Aequalis intramedullary locking avascular necrosis, 95 central humeral head, 78, 80 clinical and functional outcomes, 95, 96 design, 77, 79 perioperative complications,
pedcat Clinical Case Studies
 pedcat Clinical Case Studies C u r v e B e a m 1 7 5 T i t u s A v e, S u i t e 3 0 0 W a r r i n g t o n, P A 1 8 9 7 6 267-4 8 3-8081 w w w. c u r v e b e a m. c o m PedCAT: Clinical Evidence of diagnostic
pedcat Clinical Case Studies C u r v e B e a m 1 7 5 T i t u s A v e, S u i t e 3 0 0 W a r r i n g t o n, P A 1 8 9 7 6 267-4 8 3-8081 w w w. c u r v e b e a m. c o m PedCAT: Clinical Evidence of diagnostic
*Rippstein, Trnka, Saragas, Hoffman
 THURS 25th MAY 07:00 07:10 Welcome and Introductions Paulo Ferrao Lecture 1: 07:10 09:45 Forefoot I: Hallux Valgus and Lesser Toes Mark Easley 40 mins 07:10 07:50 Surgical Management of Hallux Valgus 30
THURS 25th MAY 07:00 07:10 Welcome and Introductions Paulo Ferrao Lecture 1: 07:10 09:45 Forefoot I: Hallux Valgus and Lesser Toes Mark Easley 40 mins 07:10 07:50 Surgical Management of Hallux Valgus 30
SUBTALAR ARTHROEREISIS IN THE OLDER PATIENT
 C H A P T E R 1 7 SUBTALAR ARTHROEREISIS IN THE OLDER PATIENT William D. Fishco, DPM, MS INTRODUCTION Arthroereisis is a surgical procedure designed to limit the motion of a joint. Subtalar joint arthroereisis
C H A P T E R 1 7 SUBTALAR ARTHROEREISIS IN THE OLDER PATIENT William D. Fishco, DPM, MS INTRODUCTION Arthroereisis is a surgical procedure designed to limit the motion of a joint. Subtalar joint arthroereisis
CURRENT TREATMENT OPTIONS
 CURRENT TREATMENT OPTIONS Fix single column or both: Always fix both. A study by Svend-Hansen corroborated the poor results associated with isolated medial malleolar fixation in bimalleolar ankle fractures.
CURRENT TREATMENT OPTIONS Fix single column or both: Always fix both. A study by Svend-Hansen corroborated the poor results associated with isolated medial malleolar fixation in bimalleolar ankle fractures.
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT
 SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
PAINFUL SESAMOID OF THE GREAT TOE Dr Vasu Pai ANATOMICAL CONSIDERATION. At the big toe MTP joint: Tibial sesamoid (medial) & fibular (lateral)
 & fibular (lateral)") PAINFUL SESAMOID OF THE GREAT TOE Dr Vasu Pai ANATOMICAL CONSIDERATION At the big toe MTP joint: Tibial sesamoid (medial) & fibular (lateral) They are contained within the tendons of Flexor Hallucis Brevis
PAINFUL SESAMOID OF THE GREAT TOE Dr Vasu Pai ANATOMICAL CONSIDERATION At the big toe MTP joint: Tibial sesamoid (medial) & fibular (lateral) They are contained within the tendons of Flexor Hallucis Brevis
Calcaneus (Heel Bone) Fractures
 Fractures") Page 1 of 8 Calcaneus (Heel Bone) Fractures A fracture of the calcaneus, or heel bone, can be a painful and disabling injury. This type of fracture commonly occurs during a high-energy event such as a
Page 1 of 8 Calcaneus (Heel Bone) Fractures A fracture of the calcaneus, or heel bone, can be a painful and disabling injury. This type of fracture commonly occurs during a high-energy event such as a
Rippstein, Trnka, Saragas, Narramore
 THURS 25th MAY 07:45 07:55 Welcome and Introductions Paulo Ferrao Lecture 1: 08:00 10:20 Forefoot I: Hallux Valgus and Lesser Toes Mark Easley 30 mins 08:00 08:30 Surgical Management of Hallux Valgus Saragas,
THURS 25th MAY 07:45 07:55 Welcome and Introductions Paulo Ferrao Lecture 1: 08:00 10:20 Forefoot I: Hallux Valgus and Lesser Toes Mark Easley 30 mins 08:00 08:30 Surgical Management of Hallux Valgus Saragas,
9/22/2017. I am a local. Born at Desert Samaritan
 I am a local Born at Desert Samaritan 1 MOUNTAIN VIEW HIGH SCHOOL ASU U OF IOWA MED SCHOOL PHOENIX FOR RESIDENCY 2 Discuss the 5 most controversial topics in foot and ankle Injuries that are routinely
I am a local Born at Desert Samaritan 1 MOUNTAIN VIEW HIGH SCHOOL ASU U OF IOWA MED SCHOOL PHOENIX FOR RESIDENCY 2 Discuss the 5 most controversial topics in foot and ankle Injuries that are routinely
American Family Physician
 Page 1 of 12 American Family Physician Return to Previous Page Jul 1, 1998 Table of Contents Lisfranc Injury of the Foot: A Commonly Missed Diagnosis KEVIN E. BURROUGHS, M.D, Moses Cone Family Practice
Page 1 of 12 American Family Physician Return to Previous Page Jul 1, 1998 Table of Contents Lisfranc Injury of the Foot: A Commonly Missed Diagnosis KEVIN E. BURROUGHS, M.D, Moses Cone Family Practice
Retrospective Study of Surgical Outcomes for Combined Ankle and Subtalar Joint Arthrodesis, Cavovarus Deformity Correction and Ankle Fractures
 FOOT/ ANKLE RETROSPECTIVE STUDYIC S Retrospective Study of Surgical Outcomes for Combined Ankle and Subtalar Joint Arthrodesis, Cavovarus Deformity Correction and Ankle Fractures Adult & Pediatric Deformity
FOOT/ ANKLE RETROSPECTIVE STUDYIC S Retrospective Study of Surgical Outcomes for Combined Ankle and Subtalar Joint Arthrodesis, Cavovarus Deformity Correction and Ankle Fractures Adult & Pediatric Deformity
Sports Injuries of the Foot and Ankle. Mark McEleney, MD University of Iowa College of Medicine Refresher Course for the Family Physician 4/4/2018
 Sports Injuries of the Foot and Ankle Mark McEleney, MD University of Iowa College of Medicine Refresher Course for the Family Physician 4/4/2018 I. Objectives A. By the end of the lecture attendees will
Sports Injuries of the Foot and Ankle Mark McEleney, MD University of Iowa College of Medicine Refresher Course for the Family Physician 4/4/2018 I. Objectives A. By the end of the lecture attendees will
Feet First. Michael K. Cooper, DO FACOFP Family Practice/OMM St John Clinic - Claremore OOA 2018 Annual Convention
 Feet First Michael K. Cooper, DO FACOFP Family Practice/OMM St John Clinic - Claremore OOA 2018 Annual Convention Disclaimer I have no conflict of interest. I am not on any pharmaceutical company payroll
Feet First Michael K. Cooper, DO FACOFP Family Practice/OMM St John Clinic - Claremore OOA 2018 Annual Convention Disclaimer I have no conflict of interest. I am not on any pharmaceutical company payroll
Ankle Ligament Injury: Don t Worry- It s Only a Sprain Wes Jackson MD Orthopaedic Foot & Ankle
 Ankle Ligament Injury: Don t Worry- It s Only a Sprain Wes Jackson MD Orthopaedic Foot & Ankle Outline I. Epidemiology II. Classification and Types of Sprains III. Anatomy IV. Clinical Assessment and Imaging
Ankle Ligament Injury: Don t Worry- It s Only a Sprain Wes Jackson MD Orthopaedic Foot & Ankle Outline I. Epidemiology II. Classification and Types of Sprains III. Anatomy IV. Clinical Assessment and Imaging
Ultrasound of Mid and Hindfoot Pathology
 Ultrasound of Mid and Hindfoot Pathology Levon N. Nazarian, M.D. Professor of Radiology Thomas Jefferson University Hospital Disclosures None relevant to this presentation Educational Objective Following
Ultrasound of Mid and Hindfoot Pathology Levon N. Nazarian, M.D. Professor of Radiology Thomas Jefferson University Hospital Disclosures None relevant to this presentation Educational Objective Following
Anatomy of the lower limb
 Anatomy of the lower limb Arches & sole of the foot Dr. Hayder ARCHES OF THE FOOT The foot as a mechanical unit performs two major functions: - It acts as a pliable platform to support the body weigh during
Anatomy of the lower limb Arches & sole of the foot Dr. Hayder ARCHES OF THE FOOT The foot as a mechanical unit performs two major functions: - It acts as a pliable platform to support the body weigh during
Biokinesiology of the Ankle Complex
 Rehabilitation Considerations Following Ankle Fracture: Impact on Gait & Closed Kinetic Chain Function Disclosures David Nolan, PT, DPT, MS, OCS, SCS, CSCS I have no actual or potential conflict of interest
Rehabilitation Considerations Following Ankle Fracture: Impact on Gait & Closed Kinetic Chain Function Disclosures David Nolan, PT, DPT, MS, OCS, SCS, CSCS I have no actual or potential conflict of interest
7/23/2018 DESCRIBING THE FRACTURE. Pattern Open vs closed Location BASIC PRINCIPLES OF FRACTURE MANAGEMENT. Anjan R. Shah MD July 21, 2018.
 BASIC PRINCIPLES OF FRACTURE MANAGEMENT Anjan R. Shah MD July 21, 2018 DESCRIBING THE FRACTURE Pattern Open vs closed Location POLL OPEN HOW WOULD YOU DESCRIBE THIS FRACTURE PATTERN? 1 Spiral 2 Transverse
BASIC PRINCIPLES OF FRACTURE MANAGEMENT Anjan R. Shah MD July 21, 2018 DESCRIBING THE FRACTURE Pattern Open vs closed Location POLL OPEN HOW WOULD YOU DESCRIBE THIS FRACTURE PATTERN? 1 Spiral 2 Transverse
Case Report Bipartite Medial Cuneiform: Case Report and Retrospective Review of 1000 Magnetic Resonance (MR) Imaging Studies
 Imaging Studies") Case Reports in Medicine, Article ID 130979, 4 pages http://dx.doi.org/10.1155/2014/130979 Case Report Bipartite Medial Cuneiform: Case Report and Retrospective Review of 1000 Magnetic Resonance (MR) Imaging
Case Reports in Medicine, Article ID 130979, 4 pages http://dx.doi.org/10.1155/2014/130979 Case Report Bipartite Medial Cuneiform: Case Report and Retrospective Review of 1000 Magnetic Resonance (MR) Imaging
FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]
![FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]](/thumbs/83/88335212.jpg "FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]") FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
Ankle Sprains and Their Imitators
 Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
The Foot. Dr. Wegdan Moh.Mustafa Medicine Faculty Assistant Professor Mob:
 The Foot Dr. Wegdan Moh.Mustafa Medicine Faculty Assistant Professor Mob: 0127155717 The skeleton of the foot Cutaneous innervations Sole of foot layers of muscles First layer -Abductor hallucis -Flexor
The Foot Dr. Wegdan Moh.Mustafa Medicine Faculty Assistant Professor Mob: 0127155717 The skeleton of the foot Cutaneous innervations Sole of foot layers of muscles First layer -Abductor hallucis -Flexor
Clinical evaluation where no obvious fracture a. Squeeze test
 7:43 am The Syndesmotic Injury: From Subtle to Severe Robert B. Anderson, MD Chief, Foot and Ankle Carolinas Medical Center OrthoCarolina (Charlotte, North Carolina) 7:30-8:25 am Symposium 1: Management
7:43 am The Syndesmotic Injury: From Subtle to Severe Robert B. Anderson, MD Chief, Foot and Ankle Carolinas Medical Center OrthoCarolina (Charlotte, North Carolina) 7:30-8:25 am Symposium 1: Management
Pelvic cavity. Gross anatomy of the lower limb. Walking. Sándor Katz M.D.,Ph.D.
 Pelvic cavity. Gross anatomy of the lower limb. Walking. Sándor Katz M.D.,Ph.D. Lower limb Pelvic girdle Free lower extremity Hip bone Definitive fusion of the Y- shaped growth plate occurs 16th -18th
Pelvic cavity. Gross anatomy of the lower limb. Walking. Sándor Katz M.D.,Ph.D. Lower limb Pelvic girdle Free lower extremity Hip bone Definitive fusion of the Y- shaped growth plate occurs 16th -18th
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Laboratory RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Department of Physical Therapy King Saud University Talocrural and Subtalar Joint
بسم هللا الرحمن الرحيم Laboratory RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Department of Physical Therapy King Saud University Talocrural and Subtalar Joint