Peripheral Nerve Blocks Overview and complications. Diane P. Welsh RN BSN MPA CCRN CAPA
|
|
|
- Gwendolyn Payne
- 5 years ago
- Views:
Transcription
1 Peripheral Nerve Blocks Overview and complications Diane P. Welsh RN BSN MPA CCRN CAPA
2 Objectives Discuss the advantages and disadvantages of peripheral nerve blocks Discuss the physiology and pharmacology of peripheral nerve blocks Identify the types of upper and lower extremity peripheral nerve blocks, their effects and uses. Discuss common complications of peripheral nerve blocks Describe nursing management of the patient undergoing peripheral nerve blockade to include patient education
3
4 Peripheral Nerve Blocks Part of a pre-emptive multimodal analgesic technique providing safe and effective post-operative pain management with minimal side effects. Appropriate for both the in-patient and out-patient setting, PNB s afford both anesthesia and extended analgesia for a variety of surgical procedures. Afferent nociceptive (pain) stimulus from the injured tissue is prevented from reaching the central nervous system by preinjury neural blockade. Pain may be eliminated or minimized.
5 Advantages of PNB Reduced postoperative pain resulting in greater patient satisfaction with their pain management Early ambulation and discharge Decreased side effects of nausea and vomiting, drowsiness secondary to less opioid use for pain control. Less sedation during surgery allows patients to remain conscious (MAC) thus protecting their airway and avoiding airway manipulation and intubation
6 Disadvantages of PNB Requires technical expertise from a variety of medical clinicians Time required preoperatively for block placement. This may be offset by decreased anesthesia time in the OR and shorter length of stay in the PACU Contraindicated in patients with a history of coagulopathies, preexisting neuropathies, anatomical aberrancy/pathology at injection site, or systemic disease or infection
7 Neurophysiology Local Anesthesia (LA) blocks transmission in ascending and descending nerve pathways. The order of the nerve fibers affected by LA is sensory, motor, and sympathetic. Of note, resolution or regression of the block occurs first in motor fibers, then sensory and lastly sympathetic. This pattern is important when instructing patients about preemptive pain management and postoperative use of the extremity.
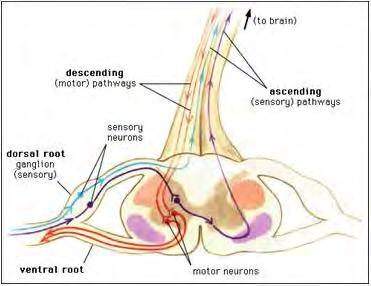
8 Neurophysiology
 changes the permeability of the cell membrane to sodium interfering with the ability of sodium to enter the cell.")
9 Neurophysiology On a cellular level, it is the influx of sodium into the cell that is responsible for generating an action potential causing depolarization and conduction of the nerve fibers. Local Anesthetic (LA) changes the permeability of the cell membrane to sodium interfering with the ability of sodium to enter the cell. This interference with nerve fiber conduction prevents the sensory or motor information from being transmitted to and from the brain. This also applies to cardiac conduction.
10 Pharmacology Peripheral nerve blocks (PNB) involve injecting a local anesthetic near or around the nerve or nerve plexus that supplies the surgical area. The duration of action for each anesthetic medication depends on several factors; injection volume, concentration of the medication, and absorption. Single injection commonly 30-40cc Percutaneous insertion of a catheter directly near the peripheral nerve supplies the surgical site with a continuous infusion
11 Local Anesthetics for Peripheral Nerve Blocks Drug Concentration (%) Onset Duration (min) Maximum Single Dose Lidocaine Fast mg Mepivacaine Fast 3-5min Peak min 400mg Bupivicaine Slow 4-10min Peak 30-45min 175mg Ropivacaine Slow min mg
12 Injection techniques Aspiration: occurs before the initial injection of LA to avoid intravascular infusion and after each 5ml of injected Local Anesthetic Injection pressure: Using one hand and a 20cc syringe, apply slow and deliberate force. If force is too high, nerve damage may occur Resistance: Discontinue the injection and notify anesthesia if there is high resistance to the injection. Needle needs repositioning.
13 Ultrasound Guidance Ultrasound guidance enhances visualization of the neural target and its surrounding structures. Able to differentiate between vascular and non-vascular structures with the use of Doppler flow, as well as other structures i.e. lung. Unintentional intraneural injection is reduced Assessment of the proper needle-tip position occurs in real time Visualization of LA spread around the neural target ensures a successful block procedure Allows for use of a smaller volume of LA due to the ability to visualize the administration during injection. Identification of anomalous anatomy or pathology,

14
15 Upper extremity Interscalene Supraclavicular Infraclavicular Axillary

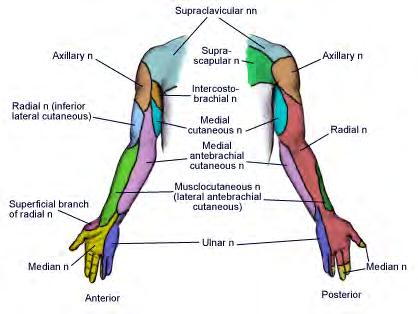
16 Brachial plexus anatomy The brachial plexus extends from C5 to T1; (C5, C6, C7, C8 and T1). It innervates the shoulder and arm. The brachial plexus begins as spinal nerve roots and continues to the terminal branches that supply the upper extremity. Specifically, the anatomy progresses from roots to trunks, trunks to divisions, divisions to cords (lateral, medial and posterior cords) and finally to terminal nerve branches

17 Brachial Plexus Nerves
18
19 Interscalene Block (ISB) Suitable for shoulder and upper arm procedures involving the lateral 2/3 of the clavicle, proximal humerus, and the shoulder joint i.e. total or hemiarthroplasty, arthroscopy, subacromial decompression, and procedures for the instability of the shoulder joint, rotator cuff repair and frozen shoulder. The block is performed at the level of the distal trunk and the origin of its divisions blocking nerves at C4-C6. It is the most proximal to the brachial plexus so not recommended for hand surgery Not recommended for patients with impaired pulmonary function. ISB obstructs the phrenic nerve, resulting in ipsilateral diaphragmatic paralysis
20 Interscalene Block The approach to the brachial plexus lies in the neck between the interscalene muscle and the clavicle. The patient lies supine with the head facing away from the side to be blocked. Landmarks include the sternocleidomastoid muscle, external jugular vein, and the cricoid cartilage. The level of the cricoid cartilage corresponds to the C6 vertebral body where the interscalene block is administered. The needle is inserted into the interscalene groove in a slightly medial, caudal, and posterior direction to avoid the vertebral column and vascular structures. Provides spread to the nonbrachial plexus Supraclavicular nerve which supplies sensory innervation to the cape of the shoulder. May not anesthetize the entire posterior aspect of the shoulder.
21 Interscalene landmarks
22 Ultrasound of Interscalene Anatomy
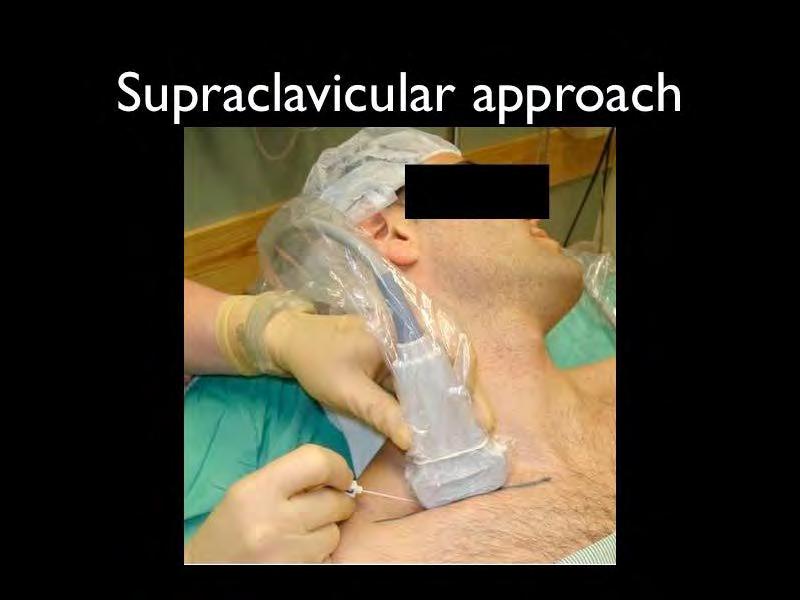
23 Supraclavicular Block (SCB) The indication for a Supraclavicular block is surgery of the upper arm, elbow, forearm, wrist, and hand excluding the shoulder area. The block is performed at the level of the trunks and divisions of the brachial plexus located lateral to the subclavian artery between the first rib and clavicle. The patient lies supine with the head turned away from the side to be blocked. Landmarks on the body include the first rib, subclavian artery and the apex of the lung. Pneumothorax is a potential complication due to the proximity to the apex of the lung.
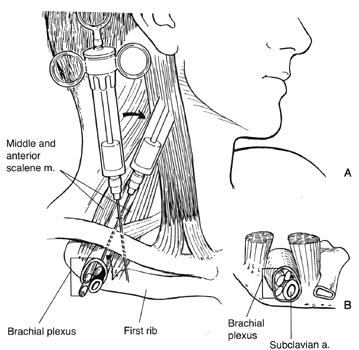
24 Supraclavicular Block

25 Infraclavicular Block The indication for the Infraclavicular block is surgery of the upper arm, elbow, forearm, wrist, and hand excluding the shoulder area. The block is performed at the level of the brachial plexus cords, at the clavicle pectoral triangle lateral to the axillary artery and vein. The patient lies supine with the head turned away from the side to be blocked. Landmarks on the body to consider are the subclavian artery, the apex of the lung and the pectoralis minor and major muscles. Used as a substitute for a Supraclavicular when there is difficult anatomy.

26 Axillary Block The indication for an Axillary block is surgery involving the elbow, forearm and hand. The block targets three of the four major terminal nerves of the brachial plexus: ulnar, radial, and median nerves. The axillary nerve itself is not blocked. Multiple injections are used to target these nerves. The patient lies in the supine position with abduction of the arm to be blocked. Excessive abduction is avoided since it stretches the brachial plexus increasing vulnerability to injury. Landmarks are the axillary artery, the biceps, coracobrachialis, and triceps muscle.
27 Lower extremity Femoral Adductor Canal Popliteal Ankle Sciatic
28

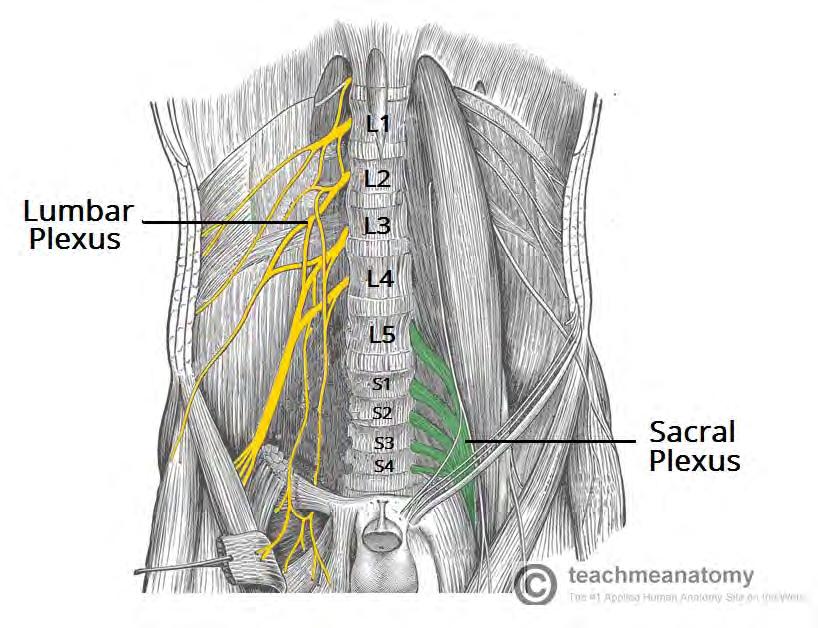
29 Lumbar plexus The lumbar plexus comprises the bundle of nerves which control movement and sensation in the lower extremities. The nerve roots exit the spine at L1-5 and S1-2. They further branch to form several nerves that descend from the plexus down the thigh and leg into the foot. Only nerves roots and branches, no trunks or cords like the brachial plexus The major branches are the lateral femoral cutaneous, femoral, obturator, and sciatic nerves providing sensation to the medial, lateral and anterior aspects of the thigh.
30 Femoral Block The femoral nerve is the largest branch of the lumbar plexus with origins in L2, L3, and L4 Provides motor and sensory innervation to the anterior aspect of the thigh, to the knee and to the medial aspects of the calf, ankle, and foot. Used for hip fracture repair and mid to distal femur fracture repair. Analgesia is only partial (usually paired with a spinal) Indications for single injections are knee arthroscopy, total knee arthroplasty; sometimes paired with a proximal sciatic block, BKA; sometimes paired with a popliteal sciatic block, AKA; paired with a sciatic block, ACL repair; paired with a single shot sciatic block, other hip or knee surgeries.

31 Patient is positioned in a supine position with the arm on the procedural side stationed out of the sterile field. The injection point is at the intersection of a line drawn from the anterior superior iliac spine to the pubic symphysis and a vertical line just lateral to the femoral artery. The femoral crease and the femoral artery pulse serve as guides. If groin accessibility is limited, secondary to obesity, special positioning or taping may be necessary for pannus retraction Femoral Block

32 Adductor Canal Serves as a passageway for the saphenous nerve, the vastus medialis, medial femoral cutaneous, articular branches from the obturator nerve and the medial retinacular nerve as well as the femoral artery and femoral vein Sensory changes of the Adductor Canal block involve the saphenous nerve including the medial and anterior aspect of the knee from the superior pole of the patella to the proximal tibia. Adductor canal block generally spares the quadriceps muscles so pt. able to flex hip with comparable pain control. Placement is mid-thigh around the femoral nerve before it exits the adductor canal Effective alternative to the FNB for patients undergoing TKA or surgery involving the distal thigh and femur, knee and lower leg on the medial side.

33 Femoral/Adductor Anatomy
34 Sciatic Block The sacral plexus provides motor and sensory innervation to the entire lower extremity including hip, ankle and knee. Important components are the sciatic and posterior cutaneous nerves Landmarks are the greater trochanter, the posterior superior iliac spine, and the sacral hiatus. Twitch monitors may be used with the goal of visible or palpable twitches of the hamstrings, calf muscles, foot or toes. The patient needs adequate sedation; commonly painful. Onset of block usually occurs in minutes. It provides for complete anesthesia of the leg except for the medial strip of skin innervated by the saphenous nerve. Combined with a femoral block, complete anesthesia of the leg may be achieved. More discreet posterior blocks are generally used

35 Sciatic Nerve Block
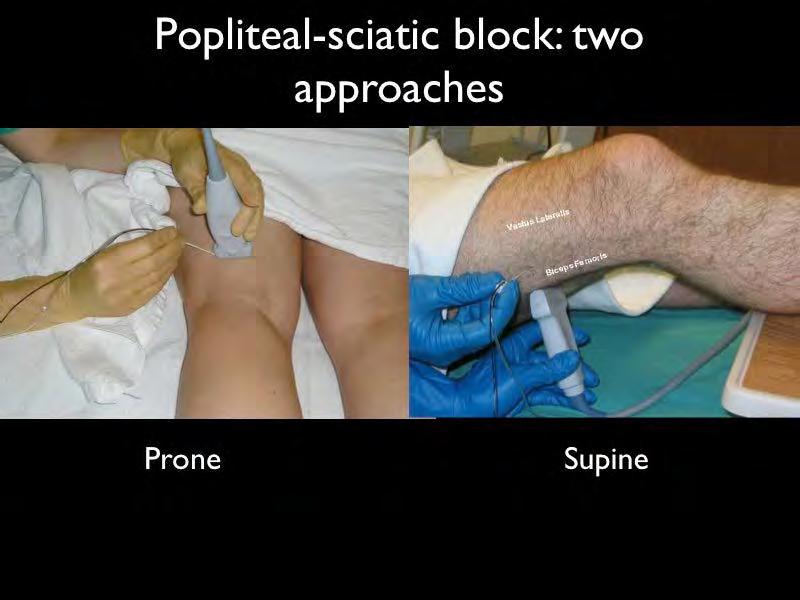
36 Popliteal Sciatic Block Anesthetizes the entire leg below the tibial plateau except the skin of the medial aspect of the calf and foot (saphenous nerve distribution) The popliteal block is performed on the sciatic nerve proximal to this bifurcation; about 10 cm from the popliteal crease. Landmarks include the popliteal crease, tendons of the biceps femoris and the semitendonisimus muscles Used for minor surgeries of the distal lower leg, foot or ankle
37 Popliteal fossa
38 Popliteal Sciatic Block Pt. is positioned in the prone position or in a modified exaggerated lateral position with the leg to be blocked uppermost and flexed at the knee touching the bed and the underlying leg straight. Advantages are improved calf tourniquet tolerance and an immobile foot. Complications may be persistent foot drop with potential pressure necrosis
39

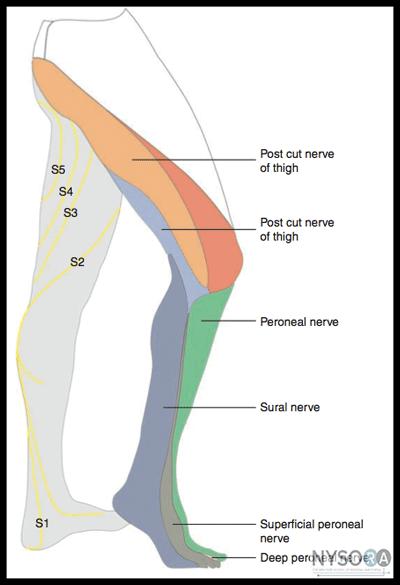
40 Sensory distribution of block except blue area
41 Ankle block The ankle block is performed at the tibial nerve and the deep and superficial aspects of the peroneal nerve. The peripheral nerves at the ankle and metatarsal level are the terminal branches of the sciatic (posterior tibial, superficial peroneal, deep peroneal, sural) and femoral saphenous nerves. Indicated for surgery of the foot. The pertinent landmarks are the posterior tibial and dorsalis pedis arteries, tendon of the hallucis longus and medial malleolus
42 Ankle Block Patient is positioned in a supine position. Elevation of the patients calf permits the various insertion sites (ring-like) to be more easily accessed. An uncomfortable block requiring 5 different injections Epinephrine is contraindicated. Potential arterial vasoconstriction may lead to foot and/or toe ischemia secondary to the lack of collateral circulation at that location.

43 Lower extremity nerve anatomy


44 Ankle Block
45 Transversus Abdominis Plane (TAP) Block Provides analgesia to the skin and muscles of the antero-lateral abdominal wall and parietal peritoneum. Does not block visceral pain. Goal of the block is to place LA between the internal oblique and transversus abdominis muscle layers resulting in the interruption to the innervation of the abdominal skin, muscles and parietal peritoneum. Administered by landmark, ultrasound guided by anesthesia or direct visualization by the surgeon Single injection vs. catheter bolus. Bupivicaine, Ropivicaine, and Levobupivicaine commonly used. Used for patients undergoing lower abdominal surgery; appendectomy, c-sect, hernia repair, abdominal hysterectomy and prostatectomy.

46 Transversus Abdominis Plane (TAP) Block Triangle of Petit: bounded by the latissimus dorsi posteriorly, the external oblique anteriorly and the iliac crest inferiorly. Needle is inserted perpendicular to all planes looking for the tactile sensation of 2 pops. First indicates penetration of the external oblique fascia into the plane between external and oblique muscles. Second pop signifies entry into the plane between internal oblique and transversus abdominis muscles.

47
48 Complications
49 Peripheral Nerve Injury May be associated with needle trauma, inadvertent injection of the nerve, or high injection pressures Intraneural injection may be identified during block administration by the patient complaining of a sharp pain. The injection is stopped immediately. Surgical trauma may also cause nerve damage May not manifest until 7-14 days post-op. Symptoms: persistent c/o paresthesia, aching or sensory or motor deficits Treatment is prevention
50 Pneumothorax Associated with Supraclavicular blocks Causes pts to present with anxiety, tachycardia, tachypnea, chest pain, sub-q emphysema, and diminished breath sounds. Pts. may not develop symptoms for 6-12 hours Pneumothorax requires a chest tube. Ultrasound guidance reduces the incidence since the pleura and first rib is easily visualized.
51 Horner s syndrome Ipsilateral sympathetic blockade which includes nasal congestion, ptosis of one eyelid, miosis, and conjunctive hyperemia. Hoarseness occurs in approximately 10% of patients and is the result of laryngeal nerve block. More prevalent with right sided blocks
52 Hemidiaphragmatic paralysis The proximity of the phrenic nerve and its originating cervical roots to the brachial plexus often lends to unintended local anesthetic blockade and diaphragmatic dysfunction. The incidence is 100% after interscalene block Some patients will report mild shortness of breath or altered respiratory sensations and may experience 25-32% reduction in spirometric measures of pulmonary function Supraclavicular blocks have a lower incidence.
53 Local Anesthetic Systemic Toxicity or LAST A complication caused by the inadvertent injection of LA into the vascular system or the rapid absorption from the tissue into the vascular system. Studies suggest a more forceful, rapid injection carries a much higher risk than a slow, gentle injection. Prevention must include prudent selection of LA concentration and volume, slow, gentle injection, frequent aspiration, and vigilant monitoring of vital signs Injection into the vein is more serious than into an artery. Arterial allows for dilution and redistribution of the anesthetic into the tissue before it reaches the systemic circulation. Injection into the vein carries the LA directly to the heart and brain.
54 LAST A RARE EVENT BUT LETHAL Early studies ( ) in France of the incidence of LAST had a range of / 10,000 cases of Peripheral Nerve Blocks. Study by Sites of an 8 years period the incidence was 1/12,668. Decrease attributed to Ultrasound guidance. Study by DeGregorio ( ) of 93 cases of LAST Epidural 33%, Axillary Block 17%, Interscalene Block 13% (77) Single injection, (14) Continuous infusion (52) or 55% Bupivicaine, (28) or 30% Ropivicaine, (4) or 4% Levobupivicaine, (9) or 11% Other Certain characteristics may increase incidence: Age: children or elderly, high output cardiac states which increases vascular absorption, Co-morbidities: cardiac disease, pregnancy, hepatic dysfunction, metabolic syndromes.
55 LAST Symptoms: ringing in the ears, metallic taste in the mouth, numbness of the lips, twitching of the eyes and lips leading to seizures. Most serious; cardiovascular arrest, respiratory, and central nervous system depression (LOC)
56 LAST Immediate treatment: provide adequate ventilation, oxygenation, and circulation (CPR) Infusion of Intralipid Adult Bolus ml/kg over 1-2 minutes. Pediatric Bolus 1ml/kg. Repeat dosing every 3-5 minutes up to max dose of 3ml/kg. Provide maintenance infusion ml/kg/min
57 Nursing Responsibilities
58 Preoperative Assess the patient for physical (neuropathy, coagulopathies, infection) and psychosocial conditions that may influence PNB, baseline VS Assess respiratory status for pathophysiology to rule out COPD and other lung diseases, liver disorders Inability to tolerate the position required for administration of the nerve block Allergies Present identified risk factors to the Anesthesia team

59
60 Block Procedure Educate the patient and family about the block procedure and advantages Attach monitors; BP, EKG. SO2, nasal O2, 5 minute interval assessment Participate in Time Out procedure Assist with procedure as needed, PNS adjustment, Ultrasound picture Monitor patient post-procedure VS and progression of block Monitor for side effects and/or complications Protect anesthetized limb in anatomical alignment.
61 Postoperative Assess neurovascular status of limb for color, temperature and capillary refill. Protect the limb from injury by appropriate positioning Repeatedly assess the patient s level of sensory and motor function and analgesia. Assess the dressing or cast Place limb in neutral alignment and provide support. For upper extremity nerve blocks, place pillow under the patients elbow to prevent stretching of the brachial plexus and pressure on the ulnar nerve. For lower limb, use pillows to support the entire leg and prevent heel pressure. Movement or sensation especially pain suggests the need for supplemental analgesia Continuous infusion requires checking the catheter placement and the insertion site as well as the delivery device, correct medication and dose.
62 Pain management Review the pain management prescription Need to take pain medication before the block wears off emphasizing the time frame for taking the medications Resolution of block is unpredictable so start on a specific schedule When a block begins to wear off, anesthetic effects may be gone within 60 minutes. Generally begins with ability to move limb, followed by numbness, tingling and heaviness. May vary. If experiencing continued side effects that are block related; longer than 48 hours, call doctor.
63 Instructions for Upper Extremity Blocks Wear the arm brace or sling at all times until the block has worn off and as prescribed by the physician. Helpful to sleep in a recliner chair with pillow under the arm or in bed with head elevated and arm supported by pillows in anatomically appropriate position.
64 Instructions for Lower extremity blocks Do not bear weight on the affected leg until the block wears off. Exception is with the use of a long leg brace and crutches if prescribed by physician Use caution and assistance when standing or trying to move or walk to reduce the risk of falling Crutch walking instructions and demonstration
65 Patient Education Discuss prevention of injury to the anesthetized limb. Absence of protective pain reflexes and reduced proprioperception The ability of the patient to move the limb before the ability to sense can lead to injury. Protection of the affected limb, immobilization Correct positioning of the limb to avoid prolonged pressure Check the color of fingers or toes with tight dressing or cast. Call MD if dusky or darkened, excessive swelling Discuss common side effects: Horner s syndrome, pneumothorax
66 Bibliography Beaussier M, Atchabahian A, Dufeu N, Regional anesthesia and the perioperative period: basis and principles, Techniques in Regional Anesthesia and Pain Management, 2008; 12: Burch M, McAllister R, Meyer T, Treatment of local-anesthetic toxicity with lipid emulsion therapy, Am J Health Syst Pharm, 2011; 88: Dickerson D,Apfelbaum J, Local anesthetic systemic toxicity, Anethetic Surgery Journal, 2014;34(7) Drasner K, Local anesthetic systemic toxicity a historical perspective, Regional Anesthesia and Pain Medicine, 2010;35(2) Eng H, Ghosh S and Chin K, Practical use of local anesthetics in regional anesthesia, Current Opinion Anesthesiology, 2014;27(4): Enneking F, Chan V, Greger J, Hadzic A, Lang S, Horlocker T, Lower extremity peripheral nerve blocks, Regional Anesthesia and Pain Medicine, 2005; 30(1):5-34. Finnerty,O, McDonnell,J. Transversus abdominis plane block, Current Opinion Anesthesiology; 2012; 25(5) Ladak S, Jiang J, Ojba, M. Transversus abdominis plane block: an overview of indication and nursing care, Pain Management Nursing, 2014;15(3) McCamant k, Peripheral nerve blocks;understanding the nurses role, Journal of Perianesthesia Nursing, 2006;21(1): Micromedex, Bupivicaine, Accessed 11/10/2014. Micromedex, Lidocaine, Accessed 11/10/2014. Micromedex, Mepivicaine, Accessed 11/10/2014. Micromedix, Ropivicaine, Accessed 11/10/2014. Mishra,M, Mishra S, Transversus abdominis plane block: The new horizon for postoperative analgesia following abdominal surgery, Egyptian Journal of Anaesthesia, 2016;32: Mukhtark K, Tansverse abdominal plane block, The Journal of New York School of Regional Anesthesia, 2009; 12: Neal J,Gerancher J, Hebl, B, Ilfield B, McCartney C, Franco C, Hogan,Q, Upper extremity regional anesthesia: essential of our current understanding, 2008, Regional Anesthesia and Pain Medicine, 2009; 34(2): Sandling-Lemming, Resuscitaion of local anesthesia-induced cardiac arrest: lipids to the rescue, Journal of Perianesthesia Nursing,2010;25(6) Stein E, Sridumaran U, Tan E, Freehill M, Wilckens J, Lower-extremity peripheral nerve blocks in the perioperative pain management of orthopaedic patients, The Journal of Bone and Joint Surgery, 2012, Accessed 10/8/2014 Transversus Abdominis Plane (TAP) Block, USRA, accessed10/09/2017. Urigel S, Molter J, Transversus Abdominis Plane (TAP) Blocks, AANA Journal, 2014;82 (1): Wright I, Peripheral nerve blocks in the outpatient surgery setting, AORN, 2011; 94(1):

67

68

69
70
Dr Kelly Jones Anesthesiologist at Northwest Orthopedics
 Dr Kelly Jones Anesthesiologist at Northwest Orthopedics Decrease narcotic use in the immediate post operative period. Better Pain Control Less side effects then General Anesthesia Sedation Post operative
Dr Kelly Jones Anesthesiologist at Northwest Orthopedics Decrease narcotic use in the immediate post operative period. Better Pain Control Less side effects then General Anesthesia Sedation Post operative
Surgery Under Regional Anesthesia
 Surgery Under Regional Anesthesia Jean Daniel Eloy, MD Assistant Professor Residency Program Director Rutgers-New Jersey Medical School Rutgers The State University of New Jersey Peripheral Nerve Block
Surgery Under Regional Anesthesia Jean Daniel Eloy, MD Assistant Professor Residency Program Director Rutgers-New Jersey Medical School Rutgers The State University of New Jersey Peripheral Nerve Block
Brachial plexus blockade within the interscalene groove involves local anesthetic
 Interscalene Brachial Plexus Block- How I do it. Part 1 of a 2 part discussion on technique. Stuart Grant Professor of Anesthesiology Duke University Medical Center Durham NC Brachial plexus blockade within
Interscalene Brachial Plexus Block- How I do it. Part 1 of a 2 part discussion on technique. Stuart Grant Professor of Anesthesiology Duke University Medical Center Durham NC Brachial plexus blockade within
inerve Guide to Nerves 2009
 inerve Guide to Nerves 2009 A guide to self learning and self assessment Context: The following guide is intended to help interpret the sono-anatomy and follow a systematic stepwise approach to the practice
inerve Guide to Nerves 2009 A guide to self learning and self assessment Context: The following guide is intended to help interpret the sono-anatomy and follow a systematic stepwise approach to the practice
Peripheral Nerve Blocks
 Peripheral Nerve Blocks N U R S I N G E D U C A T I O N JPS Acute Pain Service Peripheral nerve blocks are used as part of a multimodal analgesic program which provides the patient with safe and effective
Peripheral Nerve Blocks N U R S I N G E D U C A T I O N JPS Acute Pain Service Peripheral nerve blocks are used as part of a multimodal analgesic program which provides the patient with safe and effective
USRA OF THE LOWER EXTREMITY
 USRA OF THE LOWER EXTREMITY Christian R. Falyar, CRNA, DNAP Department of Nurse Anesthesia Virginia Commonwealth University Disclosure Statement of Financial Interest I, Christian Falyar, DO NOT have a
USRA OF THE LOWER EXTREMITY Christian R. Falyar, CRNA, DNAP Department of Nurse Anesthesia Virginia Commonwealth University Disclosure Statement of Financial Interest I, Christian Falyar, DO NOT have a
Ultrasound Guided Lower Extremity Blocks
 Ultrasound Guided Lower Extremity Blocks CONTENTS: 1. Femoral Nerve Block 2. Popliteal Nerve Block Updated December 2017 1 1. Femoral Nerve Block Indications Surgery involving the knee, anterior thigh,
Ultrasound Guided Lower Extremity Blocks CONTENTS: 1. Femoral Nerve Block 2. Popliteal Nerve Block Updated December 2017 1 1. Femoral Nerve Block Indications Surgery involving the knee, anterior thigh,
The Upper Limb III. The Brachial Plexus. Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa
 The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
Lower Extremity Ultrasound-Guided Regional Anesthesia. Stephanie Duffy, CRNA Regional Anesthesia Faculty Acute Pain Service NMCSD
 Lower Extremity Ultrasound-Guided Regional Anesthesia Stephanie Duffy, CRNA Regional Anesthesia Faculty Acute Pain Service NMCSD Objectives Review anatomy of lumbosacral plexus Lumbar plexus blocks Psoas
Lower Extremity Ultrasound-Guided Regional Anesthesia Stephanie Duffy, CRNA Regional Anesthesia Faculty Acute Pain Service NMCSD Objectives Review anatomy of lumbosacral plexus Lumbar plexus blocks Psoas
USRA OF THE UPPER EXTREMITY
 USRA OF THE UPPER EXTREMITY Christian R. Falyar, DNAP, CRNA Department of Nurse Anesthesia Virginia Commonwealth University Disclosure Statement of Financial Interest I, Christian Falyar, DO NOT have a
USRA OF THE UPPER EXTREMITY Christian R. Falyar, DNAP, CRNA Department of Nurse Anesthesia Virginia Commonwealth University Disclosure Statement of Financial Interest I, Christian Falyar, DO NOT have a
Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions.
 Section 1 Anatomy Chapter 1. Trachea 1 Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions. Pretracheal fascia 1 2 5 3 4 Questions 1. Label the
Section 1 Anatomy Chapter 1. Trachea 1 Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions. Pretracheal fascia 1 2 5 3 4 Questions 1. Label the
Ultrasound Guided Regional Nerve Blocks
 Ultrasound Guided Regional Nerve Blocks In the country of the blind the one eyed man is King -Deciderius Erasmus (1466-1536) Objectives Benefits of Regional Anesthesia Benefits of US guidance Role of ultrasound
Ultrasound Guided Regional Nerve Blocks In the country of the blind the one eyed man is King -Deciderius Erasmus (1466-1536) Objectives Benefits of Regional Anesthesia Benefits of US guidance Role of ultrasound
Lower Limb Nerves. Clinical Anatomy
 Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
The Lower Limb II. Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa
 The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
The thigh. Prof. Oluwadiya KS
 The thigh Prof. Oluwadiya KS www.oluwadiya.com The Thigh: Boundaries The thigh is the region of the lower limb that is approximately between the hip and knee joints Anteriorly, it is separated from the
The thigh Prof. Oluwadiya KS www.oluwadiya.com The Thigh: Boundaries The thigh is the region of the lower limb that is approximately between the hip and knee joints Anteriorly, it is separated from the
Where should you palpate the pulse of different arteries in the lower limb?
 Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
FASCIAL PLANE BLOCKS TOM BARIBEAULT MSN, CRNA
 FASCIAL PLANE BLOCKS TOM BARIBEAULT MSN, CRNA TECHNIQUES Abdominal Wall TAP Rectus Sheath Quadratus Lumborum Erector Spinae Chest PECS I & II Erector Spinae TECHNIQUES Knee Ipack/LIA Hip Fascia Iliaca
FASCIAL PLANE BLOCKS TOM BARIBEAULT MSN, CRNA TECHNIQUES Abdominal Wall TAP Rectus Sheath Quadratus Lumborum Erector Spinae Chest PECS I & II Erector Spinae TECHNIQUES Knee Ipack/LIA Hip Fascia Iliaca
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
Surface Anatomy and Sonoanatomy for the Occasional Regional Anesthesiologist
 Surface Anatomy and Sonoanatomy for the Occasional Regional Anesthesiologist Edward R. Mariano, M.D., M.A.S. Professor of Anesthesiology, Perioperative & Pain Medicine Stanford University School of Medicine
Surface Anatomy and Sonoanatomy for the Occasional Regional Anesthesiologist Edward R. Mariano, M.D., M.A.S. Professor of Anesthesiology, Perioperative & Pain Medicine Stanford University School of Medicine
MUSCULOSKELETAL LOWER LIMB
 MUSCULOSKELETAL LOWER LIMB Spinal Cord Lumbar and Sacral Regions Spinal cord Dorsal root ganglion Conus medullaris Cauda equina Dorsal root ganglion of the fifth lumbar nerve End of subarachnoid space
MUSCULOSKELETAL LOWER LIMB Spinal Cord Lumbar and Sacral Regions Spinal cord Dorsal root ganglion Conus medullaris Cauda equina Dorsal root ganglion of the fifth lumbar nerve End of subarachnoid space
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
Sign up to receive ATOTW weekly -
 1 SUBCLAVIAN PERIVASCULAR BRACHIAL PLEXUS BLOCK ANAESTHESIA TUTORIAL OF THE WEEK 156 19 th OCTOBER 2009 Dr. Martin Herrick Department of Anaesthesia, Addenbrooke s Hospital, Cambridge, U.K. Correspondence
1 SUBCLAVIAN PERIVASCULAR BRACHIAL PLEXUS BLOCK ANAESTHESIA TUTORIAL OF THE WEEK 156 19 th OCTOBER 2009 Dr. Martin Herrick Department of Anaesthesia, Addenbrooke s Hospital, Cambridge, U.K. Correspondence
Part 1: Communication between CNS & PNS
 Ch. 6: Peripheral Nervous System Objectives: 1. Communication between CNS & PNS: afferent (sensory) pathway versus efferent (motor) pathway of information. 2. Regulation of somatic (voluntary) motor system
Ch. 6: Peripheral Nervous System Objectives: 1. Communication between CNS & PNS: afferent (sensory) pathway versus efferent (motor) pathway of information. 2. Regulation of somatic (voluntary) motor system
Lumbar Plexus. Ventral rami L1 L4 Supplies: Major nerves.. Abdominal wall External genitalia Anteromedial thigh
 Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer What is the importance of plexuses? plexuses provides us the advantage of a phenomenon called convergence
musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer What is the importance of plexuses? plexuses provides us the advantage of a phenomenon called convergence
*the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone
, to the elbow joint (distal) - it has one bone ; the humerus which is a long bone") *the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone - muscles in the arm : *brachialis muscle *Biceps brachii
*the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone - muscles in the arm : *brachialis muscle *Biceps brachii
Regional Anaesthesia of the Thoracic Limb
 Regional Anaesthesia of the Thoracic Limb Trauma and inflammation cause sensitization of the peripheral nervous system and the subsequent barrage of nociceptive input (usually by surgery) produces sensitization
Regional Anaesthesia of the Thoracic Limb Trauma and inflammation cause sensitization of the peripheral nervous system and the subsequent barrage of nociceptive input (usually by surgery) produces sensitization
Australian and New Zealand Registry of Regional Anaesthesia (AURORA)
") Australian and New Zealand Registry of Regional Anaesthesia (AURORA) Overview of Results First 4000 procedures recorded to - www.anaesthesiaregistry.org June 1st 2011 to February 2012 Background Australian
Australian and New Zealand Registry of Regional Anaesthesia (AURORA) Overview of Results First 4000 procedures recorded to - www.anaesthesiaregistry.org June 1st 2011 to February 2012 Background Australian
213: HUMAN FUNCTIONAL ANATOMY: PRACTICAL CLASS 1: Proximal bones, plexuses and patterns
 213: HUMAN FUNCTIONAL ANATOMY: PRACTICAL CLASS 1: Proximal bones, plexuses and patterns CLAVICLE Examine an isolated clavicle and compare it with a clavicle on an articulated skeleton. Viewed from above,
213: HUMAN FUNCTIONAL ANATOMY: PRACTICAL CLASS 1: Proximal bones, plexuses and patterns CLAVICLE Examine an isolated clavicle and compare it with a clavicle on an articulated skeleton. Viewed from above,
Sign up to receive ATOTW weekly -
 ULTRASOUND GUIDED ADDUCTOR CANAL BLOCK (SAPHENOUS NERVE BLOCK) ANAESTHESIA TUTORIAL OF THE WEEK 301 13 TH JANUARY 2014 Dr Daniel Quemby, Specialist Trainee Anaesthesia Dr Andrew McEwen, Consultant Anaesthetist
ULTRASOUND GUIDED ADDUCTOR CANAL BLOCK (SAPHENOUS NERVE BLOCK) ANAESTHESIA TUTORIAL OF THE WEEK 301 13 TH JANUARY 2014 Dr Daniel Quemby, Specialist Trainee Anaesthesia Dr Andrew McEwen, Consultant Anaesthetist
Practical 1 Worksheet
 Practical 1 Worksheet ANATOMICAL TERMS 1. Use the word bank to fill in the missing words. reference side stand body arms palms anatomical forward All anatomical terms have a(n) point which is called the
Practical 1 Worksheet ANATOMICAL TERMS 1. Use the word bank to fill in the missing words. reference side stand body arms palms anatomical forward All anatomical terms have a(n) point which is called the
The arm: *For images refer back to the slides
 The arm: *For images refer back to the slides Muscles of the arm: deltoid, triceps (which is located at the back of the arm), biceps and brachialis (it lies under the biceps), brachioradialis (it lies
The arm: *For images refer back to the slides Muscles of the arm: deltoid, triceps (which is located at the back of the arm), biceps and brachialis (it lies under the biceps), brachioradialis (it lies
3 Mohammad Al-Mohtasib Areej Mosleh
 3 Mohammad Al-Mohtasib Areej Mosleh ***Muscles Connecting the Upper Limb to the Vertebral Column 1.Trapezius Muscle ***The first muscle on the back is trapezius muscle, it s called so according
3 Mohammad Al-Mohtasib Areej Mosleh ***Muscles Connecting the Upper Limb to the Vertebral Column 1.Trapezius Muscle ***The first muscle on the back is trapezius muscle, it s called so according
PERIPHERAL REGIONAL BLOCKS. by Mike DeBroeck, DNP, CRNA
 PERIPHERAL REGIONAL BLOCKS by Mike DeBroeck, DNP, CRNA Why am I bothering with this topic at all? Do CRNAs REALLY even do peripheral regional anesthetics? YES!!!!!!! TOPICS GENERAL INFO SUCCESS RATES
PERIPHERAL REGIONAL BLOCKS by Mike DeBroeck, DNP, CRNA Why am I bothering with this topic at all? Do CRNAs REALLY even do peripheral regional anesthetics? YES!!!!!!! TOPICS GENERAL INFO SUCCESS RATES
The posterior abdominal wall. Prof. Oluwadiya KS
 The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
Regional Anesthesia. procedure if required. However, many patients prefer to receive sedation either during the
 1 Regional Anesthesia Regional anaesthesia (or regional anesthesia) is anesthesia affecting only a large part of the body, such as a limb or the lower half of the body. Regional anaesthetic techniques
1 Regional Anesthesia Regional anaesthesia (or regional anesthesia) is anesthesia affecting only a large part of the body, such as a limb or the lower half of the body. Regional anaesthetic techniques
Acute Peri-Operative Pain Management Strategies
 Slide 1 Acute Peri-Operative Pain Management Strategies Phillip Gallegos, MD USAP Pinnacle Anesthesiologist Director of Anesthesia and Peri-Operative Medicine BOSHA Slide 2 ERAS Enhanced Recovery After
Slide 1 Acute Peri-Operative Pain Management Strategies Phillip Gallegos, MD USAP Pinnacle Anesthesiologist Director of Anesthesia and Peri-Operative Medicine BOSHA Slide 2 ERAS Enhanced Recovery After
Regional Anesthesia. Fatiş Altındaş Dept. of Anesthesiology
 Regional Anesthesia Fatiş Altındaş Dept. of Anesthesiology Regional anesthesia - Definition Renders a specific area of the body, e.g. foot, arm, lower extremities insensating to stimulus of surgery or
Regional Anesthesia Fatiş Altındaş Dept. of Anesthesiology Regional anesthesia - Definition Renders a specific area of the body, e.g. foot, arm, lower extremities insensating to stimulus of surgery or
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
ASA Closed Claims Project: Regional Anesthesia Claims 1990 or later Lorri A. Lee MD Department of Anesthesiology University of Washington, Seattle, WA
 ASA Closed Claims Project: Regional Anesthesia Claims 1990 or later Lorri A. Lee MD Department of Anesthesiology, Seattle, WA OVERVIEW 1. Closed Claims Project 2. Peripheral Nerve Blocks 3. Neuraxial Claims
ASA Closed Claims Project: Regional Anesthesia Claims 1990 or later Lorri A. Lee MD Department of Anesthesiology, Seattle, WA OVERVIEW 1. Closed Claims Project 2. Peripheral Nerve Blocks 3. Neuraxial Claims
region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla.
 1 region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla. Inferiorly, a number of important structures pass between arm & forearm through cubital fossa. 2 medial
1 region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla. Inferiorly, a number of important structures pass between arm & forearm through cubital fossa. 2 medial
Femoral Artery. Its entrance to the thigh Position Midway between ASIS and pubic symphysis
 Lower Limb Vessels Lecture Objectives Describe the major arteries of the lower limb. Describe the deep and superficial veins of the lower limb. Describe the topographical relationships of the arteries
Lower Limb Vessels Lecture Objectives Describe the major arteries of the lower limb. Describe the deep and superficial veins of the lower limb. Describe the topographical relationships of the arteries
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
Ali Yaghi. Omar Eyad. Ahmad Salman. 1 P a g e
 5 Ali Yaghi Omar Eyad Ahmad Salman 1 P a g e **There are two types of groin hernia; the femoral hernia and the inguinal hernia. But how can we differentiate between the inguinal hernia and the femoral
5 Ali Yaghi Omar Eyad Ahmad Salman 1 P a g e **There are two types of groin hernia; the femoral hernia and the inguinal hernia. But how can we differentiate between the inguinal hernia and the femoral
The Lower Limb VI: The Leg. Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa
 The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
Artery 1 Head and Thoracic Arteries. Arrange the parts in the order blood flows through them.
 Artery 1 Head and Thoracic Arteries 1. Given the following parts of the aorta: 1. abdominal aorta 2. aortic arch 3. ascending aorta 4. thoracic aorta Arrange the parts in the order blood flows through
Artery 1 Head and Thoracic Arteries 1. Given the following parts of the aorta: 1. abdominal aorta 2. aortic arch 3. ascending aorta 4. thoracic aorta Arrange the parts in the order blood flows through
Anatomy of the Musculoskeletal System
 Anatomy of the Musculoskeletal System Kyle E. Rarey, Ph.D. Department of Anatomy & Cell Biology and Otolaryngology University of Florida College of Medicine Outline of Presentation Vertebral Column Upper
Anatomy of the Musculoskeletal System Kyle E. Rarey, Ph.D. Department of Anatomy & Cell Biology and Otolaryngology University of Florida College of Medicine Outline of Presentation Vertebral Column Upper
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes
 Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Disclaimer. Why Regional anesthesia? Peripheral Nerve Blocks: Upper/Lower Extremity & TAP BLOCKS
 Peripheral Nerve Blocks: Upper/Lower Extremity & TAP BLOCKS Presented by: Nathan Merritt, MD Director of Regional Anesthesia and Acute Pain Parkhill Medical Center Fort Worth Co authored by: Mark Zimmerman,
Peripheral Nerve Blocks: Upper/Lower Extremity & TAP BLOCKS Presented by: Nathan Merritt, MD Director of Regional Anesthesia and Acute Pain Parkhill Medical Center Fort Worth Co authored by: Mark Zimmerman,
VENOUS DRAINAGE OF THE LOWER LIMB
 Anatomy of the lower limb Superficial veins & nerve injuries Dr. Hayder VENOUS DRAINAGE OF THE LOWER LIMB The venous drainage of the lower limb is of huge clinical & surgical importance. Since the venous
Anatomy of the lower limb Superficial veins & nerve injuries Dr. Hayder VENOUS DRAINAGE OF THE LOWER LIMB The venous drainage of the lower limb is of huge clinical & surgical importance. Since the venous
Cadaver Muscular System Practice Practical
 Cadaver Muscular System Practice Practical Station 1 Station 1 1. Specific structure 1. Rectus sheath 2. Red line 2. Linea alba Station 2 Station 2 3. Red muscle 1. Rectus abdominis 4. Red muscle actions
Cadaver Muscular System Practice Practical Station 1 Station 1 1. Specific structure 1. Rectus sheath 2. Red line 2. Linea alba Station 2 Station 2 3. Red muscle 1. Rectus abdominis 4. Red muscle actions
rotation of the hip Flexion of the knee Iliac fossa of iliac Lesser trochanter Femoral nerve Flexion of the thigh at the hip shaft of tibia
 Anatomy of the lower limb Anterior & medial compartments of the thigh Dr. Hayder The fascia lata encloses the entire thigh like a sleeve/stocking. Three intramuscular fascial septa (lateral, medial, and
Anatomy of the lower limb Anterior & medial compartments of the thigh Dr. Hayder The fascia lata encloses the entire thigh like a sleeve/stocking. Three intramuscular fascial septa (lateral, medial, and
Human Anatomy. Spinal Cord and Spinal Nerves
 Human Anatomy Spinal Cord and Spinal Nerves 1 The Spinal Cord Link between the brain and the body. Exhibits some functional independence from the brain. The spinal cord and spinal nerves serve two functions:
Human Anatomy Spinal Cord and Spinal Nerves 1 The Spinal Cord Link between the brain and the body. Exhibits some functional independence from the brain. The spinal cord and spinal nerves serve two functions:
Compartment Syndrome
 Compartment Syndrome Chapter 34 Compartment Syndrome Introduction Compartment syndrome may occur with an injury to any fascial compartment. The fascial defect caused by the injury may not be adequate to
Compartment Syndrome Chapter 34 Compartment Syndrome Introduction Compartment syndrome may occur with an injury to any fascial compartment. The fascial defect caused by the injury may not be adequate to
Lecture 09. Popliteal Fossa. BY Dr Farooq Khan Aurakzai
 Lecture 09 Popliteal Fossa BY Dr Farooq Khan Aurakzai Dated: 14.02.2018 What is popliteus? Introduction Anything relating to, or near the part of the leg behind the knee. From New Latin popliteus the muscle
Lecture 09 Popliteal Fossa BY Dr Farooq Khan Aurakzai Dated: 14.02.2018 What is popliteus? Introduction Anything relating to, or near the part of the leg behind the knee. From New Latin popliteus the muscle
Ultrasound-guided supraclavicular block
 THE JOURNAL OF NEW YORK SCHOOL J u l y 2009 V o l u m e OF REGIONAL ANESTHESIA 1 3 Ultrasound-guided supraclavicular block Arthur Atchabahian, MD Department of Anesthesiology, St. Vincent Medical Center,
THE JOURNAL OF NEW YORK SCHOOL J u l y 2009 V o l u m e OF REGIONAL ANESTHESIA 1 3 Ultrasound-guided supraclavicular block Arthur Atchabahian, MD Department of Anesthesiology, St. Vincent Medical Center,
Regional Anaesthesia
 Regional Anaesthesia Basic Sciences Anaesthetic Course Dr Vassilis ATHANASSOGLOU FRCA Consultant Anaesthetist and Lecturer in Medicine Oxford University Hospitals NHS Trust, UK Geneva, 5th June 2017 Faculty
Regional Anaesthesia Basic Sciences Anaesthetic Course Dr Vassilis ATHANASSOGLOU FRCA Consultant Anaesthetist and Lecturer in Medicine Oxford University Hospitals NHS Trust, UK Geneva, 5th June 2017 Faculty
lower limb Anterior Compartment: lecture 3 The deep fascia ( fascia lata) divides the thigh into 3 compartments:
 divides the thigh into 3 compartments:") lower limb lecture 3 The deep fascia ( fascia lata) divides the thigh into 3 compartments: 1. Anterior Extensor compartment 2. Medial Adductor compartment 3. Posterior Flexor compartment Anterior Compartment:
lower limb lecture 3 The deep fascia ( fascia lata) divides the thigh into 3 compartments: 1. Anterior Extensor compartment 2. Medial Adductor compartment 3. Posterior Flexor compartment Anterior Compartment:
Anatomy MCQs Week 13
 Anatomy MCQs Week 13 1. Posterior to the medial malleolus of the ankle: The neurovascular bundle lies between Tibialis Posterior and Flexor Digitorum Longus The tendon of Tibialis Posterior inserts into
Anatomy MCQs Week 13 1. Posterior to the medial malleolus of the ankle: The neurovascular bundle lies between Tibialis Posterior and Flexor Digitorum Longus The tendon of Tibialis Posterior inserts into
The Muscular System PART C. PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College
 PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College The Muscular System 6 PART C Five Golden Rules of Skeletal Muscle Activity Table 6.2 Muscles and Body
PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College The Muscular System 6 PART C Five Golden Rules of Skeletal Muscle Activity Table 6.2 Muscles and Body
OBJECTIVES. Unit 7:5 PROPERTIES OR CHARACTERISTICS OF MUSCLES. Introduction. 3 Kinds of Muscles. 3 Kinds of Muscles 4/17/2018 MUSCULAR SYSTEM
 OBJECTIVES Unit 7:5 MUSCULAR SYSTEM Compare the three main kinds of muscles by describing the action of each Differentiate between voluntary and involuntary muscles List at least three functions of muscles
OBJECTIVES Unit 7:5 MUSCULAR SYSTEM Compare the three main kinds of muscles by describing the action of each Differentiate between voluntary and involuntary muscles List at least three functions of muscles
Prime movers provide the major force for producing a specific movement Antagonists oppose or reverse a particular movement Synergists
 Dr. Gary Mumaugh Prime movers provide the major force for producing a specific movement Antagonists oppose or reverse a particular movement Synergists Add force to a movement Reduce undesirable or unnecessary
Dr. Gary Mumaugh Prime movers provide the major force for producing a specific movement Antagonists oppose or reverse a particular movement Synergists Add force to a movement Reduce undesirable or unnecessary
The posterolateral thoracotomy is still probably the
 Posterolateral Thoracotomy Jean Deslauriers and Reza John Mehran The posterolateral thoracotomy is still probably the most commonly used incision in general thoracic surgery. It provides not only excellent
Posterolateral Thoracotomy Jean Deslauriers and Reza John Mehran The posterolateral thoracotomy is still probably the most commonly used incision in general thoracic surgery. It provides not only excellent
Quillen College of Medicine
 Ea s t T e n n e s s e e St a t e Un i v e r s i t y Quillen College of Medicine Failing to prepare is preparing to fail. John Wooden, UCL A Dr. Tom Kwasigroch Associate Dean Director, Medical Human Gross
Ea s t T e n n e s s e e St a t e Un i v e r s i t y Quillen College of Medicine Failing to prepare is preparing to fail. John Wooden, UCL A Dr. Tom Kwasigroch Associate Dean Director, Medical Human Gross
Anterior and Medial compartments of the thigh. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Anterior and Medial compartments of the thigh Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Terms Related to Movements Movement Flexion Extension Abduction Adduction Medial (internal)
Anterior and Medial compartments of the thigh Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Terms Related to Movements Movement Flexion Extension Abduction Adduction Medial (internal)
Gateway to the upper limb. An area of transition between the neck and the arm.
 Gateway to the upper limb An area of transition between the neck and the arm. Pyramidal space inferior to shoulder @ junction of arm & thorax Distribution center for the neurovascular structures that serve
Gateway to the upper limb An area of transition between the neck and the arm. Pyramidal space inferior to shoulder @ junction of arm & thorax Distribution center for the neurovascular structures that serve
Peripheral Vascular Examination. Dr. Gary Mumaugh Western Physical Assessment
 Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Functional anatomy and variability of the blood vessels of the upper and lower limbs. Anastasia Bendelic Human Anatomy Departament
 Functional anatomy and variability of the blood vessels of the upper and lower limbs Anastasia Bendelic Human Anatomy Departament Plan: 1. Variations of the branching pattern of the aortic arch 2. Arterial
Functional anatomy and variability of the blood vessels of the upper and lower limbs Anastasia Bendelic Human Anatomy Departament Plan: 1. Variations of the branching pattern of the aortic arch 2. Arterial
CENTRAL IOWA HEALTHCARE Marshalltown, Iowa
 CENTRAL IOWA HEALTHCARE Marshalltown, Iowa CARE OF PATIENT POLICY & PROCEDURES Policy Number: 4.84 Subject: Policy: Purpose: Continuous Epidural Analgesia Acute or chronic pain relief provided to a patient
CENTRAL IOWA HEALTHCARE Marshalltown, Iowa CARE OF PATIENT POLICY & PROCEDURES Policy Number: 4.84 Subject: Policy: Purpose: Continuous Epidural Analgesia Acute or chronic pain relief provided to a patient
Mohammad Ashraf. Abdulrahman Al-Hanbali. Ahmad Salman. 1 P a g e
 - 7 Mohammad Ashraf Abdulrahman Al-Hanbali Ahmad Salman 1 P a g e Structures under the cover of Gluteus Maximus: 1-Bones: Ileum, Femur (Head, greater trochanter and gluteal tuberosity), Ischium (ischial
- 7 Mohammad Ashraf Abdulrahman Al-Hanbali Ahmad Salman 1 P a g e Structures under the cover of Gluteus Maximus: 1-Bones: Ileum, Femur (Head, greater trochanter and gluteal tuberosity), Ischium (ischial
Upper limb Arm & Cubital region 黃敏銓
 Upper limb Arm & Cubital region 黃敏銓 1 Arm Lateral intermuscular septum Anterior (flexor) compartment: stronger Medial intermuscular septum Posterior (extensor) compartment 2 Coracobrachialis Origin: coracoid
Upper limb Arm & Cubital region 黃敏銓 1 Arm Lateral intermuscular septum Anterior (flexor) compartment: stronger Medial intermuscular septum Posterior (extensor) compartment 2 Coracobrachialis Origin: coracoid
Misc Anatomy. Upper Limb! 2. Lower Limb! 5. Venous Drainage! Head & neck! 8
 Misc Anatomy Upper Limb! 2 Arteries!... 2 Veins!... 2 Spaces!... 4 Lower Limb! 5 Arteries!... 5 Venous Drainage!... 6 Spaces!... 7 Head & neck! 8 Artery!... 8 Ultrasound View for IJ CVL!... 8 Arteries
Misc Anatomy Upper Limb! 2 Arteries!... 2 Veins!... 2 Spaces!... 4 Lower Limb! 5 Arteries!... 5 Venous Drainage!... 6 Spaces!... 7 Head & neck! 8 Artery!... 8 Ultrasound View for IJ CVL!... 8 Arteries
topographical anatomy
 Kaan Yücel M.D., Ph.D. 30. September 2014 Tuesday topographical anatomy organization of the human body as major parts or segments Head Neck Trunk thorax, abdomen, back, & pelvis/perineum Upper limbs &
Kaan Yücel M.D., Ph.D. 30. September 2014 Tuesday topographical anatomy organization of the human body as major parts or segments Head Neck Trunk thorax, abdomen, back, & pelvis/perineum Upper limbs &
Regional Blocks a practical guide:
 Regional Blocks a practical guide: Author Fleur Roberts email: fleur_roberts@hotmail.com Please use this guide in conjunction with the previous tutorial (16/01/06) which describes the rules for performing
Regional Blocks a practical guide: Author Fleur Roberts email: fleur_roberts@hotmail.com Please use this guide in conjunction with the previous tutorial (16/01/06) which describes the rules for performing
Contents of the Posterior Fascial Compartment of the Thigh
 Contents of the Posterior Fascial Compartment of the Thigh 1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t
Contents of the Posterior Fascial Compartment of the Thigh 1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t
Dexamethasone Improves Outcome Of Infraclavicular Brachial Plexus Block
 Tanta Medical Journal Vol. (6), April 2008 Original Article ABSTRACT Dexamethasone Improves Outcome Of Infraclavicular Brachial Plexus Block Mohamed Samy Seddik Department of Anesthesia & Intensive Care,
Tanta Medical Journal Vol. (6), April 2008 Original Article ABSTRACT Dexamethasone Improves Outcome Of Infraclavicular Brachial Plexus Block Mohamed Samy Seddik Department of Anesthesia & Intensive Care,
COMPLETION PROJECT POSITIONING THE PATIENT IN THE OR Source- Alexander s Care of the Patient in Surgery
 COMPLETION PROJECT POSITIONING THE PATIENT IN THE OR Source- Alexander s Care of the Patient in Surgery Name Date 1. The systems involved with anesthesia, positioning and operative procedures are: a. b.
COMPLETION PROJECT POSITIONING THE PATIENT IN THE OR Source- Alexander s Care of the Patient in Surgery Name Date 1. The systems involved with anesthesia, positioning and operative procedures are: a. b.
TRAINING TOOLS THE MOST ADVANCED. ULTRASOUND
 THE MOST ADVANCED ULTRASOUND TRAINING TOOLS Introducing NYSORA ULTRASOUND SIMULATORS Developed by opinion leaders and educators, NYSORA ULTRASOUND SIMULATORS are the most anatomically accurate, tissue-like
THE MOST ADVANCED ULTRASOUND TRAINING TOOLS Introducing NYSORA ULTRASOUND SIMULATORS Developed by opinion leaders and educators, NYSORA ULTRASOUND SIMULATORS are the most anatomically accurate, tissue-like
Chapter 1: Introduction to the Human Body Test Bank
 Chapter 1: Introduction to the Human Body Test Bank MULTIPLE CHOICE 1. What is the branch of science that studies how the body functions? a. Anatomy b. Histology c. Pathology d. Physiology 2. Which word
Chapter 1: Introduction to the Human Body Test Bank MULTIPLE CHOICE 1. What is the branch of science that studies how the body functions? a. Anatomy b. Histology c. Pathology d. Physiology 2. Which word
How to Triage Orthopaedic Care. David W. Gray, M.D.
 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
The Human Body. Lesson Goal. Lesson Objectives 9/10/2012. Provide a brief overview of body systems, anatomy, physiology, and topographic anatomy
 The Human Body Lesson Goal Provide a brief overview of body systems, anatomy, physiology, and topographic anatomy Medial Lateral Proximal Distal Superior Inferior Anterior Lesson Objectives Explain the
The Human Body Lesson Goal Provide a brief overview of body systems, anatomy, physiology, and topographic anatomy Medial Lateral Proximal Distal Superior Inferior Anterior Lesson Objectives Explain the
Nerves of the upper limb Prof. Abdulameer Al-Nuaimi. E. mail:
 Nerves of the upper limb Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Brachial plexus Median nerve After originating from the brachial plexus in the axilla,
Nerves of the upper limb Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Brachial plexus Median nerve After originating from the brachial plexus in the axilla,
BRACHIAL PLEXUS. DORSAL SCAPULAR NERVE (C5) supraclavicular branch innervates rhomboids (major and minor) and levator scapulae
 supraclavicular branch innervates rhomboids (major and minor) and levator scapulae") THE BRACHIAL PLEXUS DORSAL SCAPULAR NERVE (C5) supraclavicular branch innervates rhomboids (major and minor) and levator scapulae SCHEMA OF THE BRACHIAL PLEXUS THE BRACHIAL PLEXUS PHRENIC NERVE supraclavicular
THE BRACHIAL PLEXUS DORSAL SCAPULAR NERVE (C5) supraclavicular branch innervates rhomboids (major and minor) and levator scapulae SCHEMA OF THE BRACHIAL PLEXUS THE BRACHIAL PLEXUS PHRENIC NERVE supraclavicular
perivascular, sensory and motor effects, 62, side effects, 64 and subfascial hematoma, 221 axillary plexus, 6 7 axonotmesis, 221, 222
 249 Index A abscess, and continuous peripheral nerve block, 244 Achilles tendon rupture, 173 and saphenous nerve block, 208 and sural nerve block, 209 and tibial nerve block, 203, 204, 210, 211 acromion,
249 Index A abscess, and continuous peripheral nerve block, 244 Achilles tendon rupture, 173 and saphenous nerve block, 208 and sural nerve block, 209 and tibial nerve block, 203, 204, 210, 211 acromion,
Nerve Injury. 1) Upper Lesions of the Brachial Plexus called Erb- Duchene Palsy or syndrome.
 Upper Lesions of the Brachial Plexus called Erb- Duchene Palsy or syndrome.") Nerve Injury - Every nerve goes to muscle or skin so if the nerve is injured this will cause paralysis in the muscle supplied from that nerve (paralysis means loss of function) then other muscles and other
Nerve Injury - Every nerve goes to muscle or skin so if the nerve is injured this will cause paralysis in the muscle supplied from that nerve (paralysis means loss of function) then other muscles and other
1-Muscles: 2-Blood supply: Branches of the profunda femoris artery. 3-Nerve supply: Sciatic nerve
 1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t r i n g p a r t o r i s c h i a l p a r t ) 2-Blood supply:
1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t r i n g p a r t o r i s c h i a l p a r t ) 2-Blood supply:
PNS and ANS Flashcards
 1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
Brachial plexuses and axillary lymph nodes
 Brachial plexuses and axillary lymph nodes Introduction about nervous system nervous system central nervous system periphral nervous system brain spinal cord 31 pairs of spinal nerves 12 paris of cranial
Brachial plexuses and axillary lymph nodes Introduction about nervous system nervous system central nervous system periphral nervous system brain spinal cord 31 pairs of spinal nerves 12 paris of cranial
Muscles of the lower extremities. Dr. Nabil khouri MD, MSc, Ph.D
 Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
SARASOTA MEMORIAL HOSPITAL. NURSING PROCEDURE INTRAOSSEOUS NEEDLE: INSERTION, CARE, AND REMOVAL (inv08) 12/18 12/18 1 of 7 RESPONSIBILITY:
 12/18 12/18 1 of 7 RESPONSIBILITY:") SARASOTA MEMORIAL HOSPITAL TITLE: ISSUED FOR: NURSING PROCEDURE INTRAOSSEOUS NEEDLE: INSERTION, CARE, AND REMOVAL (inv08) Nursing DATE: REVIEWED: PAGES: 12/18 12/18 1 of 7 RESPONSIBILITY: PS1094 Insertion-
SARASOTA MEMORIAL HOSPITAL TITLE: ISSUED FOR: NURSING PROCEDURE INTRAOSSEOUS NEEDLE: INSERTION, CARE, AND REMOVAL (inv08) Nursing DATE: REVIEWED: PAGES: 12/18 12/18 1 of 7 RESPONSIBILITY: PS1094 Insertion-
Lab no 1 Structural organization of the human body
 Physiology Lab Manual Page 1 of 6 Lab no 1 Structural organization of the human body Physiology is the science which deals with functions of the body parts, and how they work. Since function cannot be
Physiology Lab Manual Page 1 of 6 Lab no 1 Structural organization of the human body Physiology is the science which deals with functions of the body parts, and how they work. Since function cannot be
Synapse Homework. Back page last question not counted. 4 pts total, each question worth 0.18pts. 26/34 students answered correctly!
 Synapse Homework Back page last question not counted 26/34 students answered correctly! 4 pts total, each question worth 0.18pts Business TASS hours extended! MWF 1-2pm, Willamette 204 T and Th 9:30-10:30am,
Synapse Homework Back page last question not counted 26/34 students answered correctly! 4 pts total, each question worth 0.18pts Business TASS hours extended! MWF 1-2pm, Willamette 204 T and Th 9:30-10:30am,
ARROW EZ-IO Intraosseous Vascular Access System Procedure Template
 ARROW EZ-IO Intraosseous Vascular Access System Procedure Template PURPOSE To provide procedural guidance for establishment of intraosseous vascular access using the ARROW EZ-IO Intraosseous Vascular Access
ARROW EZ-IO Intraosseous Vascular Access System Procedure Template PURPOSE To provide procedural guidance for establishment of intraosseous vascular access using the ARROW EZ-IO Intraosseous Vascular Access
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 October 6, 2006
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 October 6, 2006 PART l. Answer in the space provided. (8 pts) 1. Identify the structures. (2 pts) B C A. _pisiform B. _ulnar artery A C. _flexor carpi
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 October 6, 2006 PART l. Answer in the space provided. (8 pts) 1. Identify the structures. (2 pts) B C A. _pisiform B. _ulnar artery A C. _flexor carpi
Gross Anatomy Coloring Book Series. Lower Extremity Arteries
 Gross Anatomy Coloring Book Series Lower Extremity Arteries 1 Femoral Artery and Associated Branches For the life of the flesh is in the blood. Leviticus 17:11 Femoral Artery and Associated Branches After
Gross Anatomy Coloring Book Series Lower Extremity Arteries 1 Femoral Artery and Associated Branches For the life of the flesh is in the blood. Leviticus 17:11 Femoral Artery and Associated Branches After
Key Relationships in the Upper Limb
 Key Relationships in the Upper Limb This list contains some of the key relationships that will help you identify structures in the lab. They are organized by dissection assignment as defined in the syllabus.
Key Relationships in the Upper Limb This list contains some of the key relationships that will help you identify structures in the lab. They are organized by dissection assignment as defined in the syllabus.
Profession experiences
 WACHARIN SRISUK Bangkok Hospital Udon,HOD Education :2000 Bachelor of Nursing science, Thai Red Cross College of Nursing Profession experiences :2000-2014 @Professional Orthopaedic OR Nurse at King Chulalongkorn
WACHARIN SRISUK Bangkok Hospital Udon,HOD Education :2000 Bachelor of Nursing science, Thai Red Cross College of Nursing Profession experiences :2000-2014 @Professional Orthopaedic OR Nurse at King Chulalongkorn
Understanding Leg Anatomy and Function THE UPPER LEG
 Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.