Juliana Barr, MD, FCCM
|
|
|
- Mitchell Cobb
- 5 years ago
- Views:
Transcription

1 Juliana Barr, MD, FCCM Staff Anesthesiologist and Intensivist, VA Palo Alto Health Care System Associate Professor, Anesthesiology, Perioperative, and Pain Medicine Stanford University School of Medicine

2 Faculty Disclosures: Lead Author, SCCM s ICU Pain, Agitation, and Delirium Guidelines 1 Member, SCCM ICU Liberation Committee Faculty, SCCM ABCDEF Bundle Collaborative Advisory Board Member, Medasense Biometrics, Ltd. 1 Barr J, et al. Crit Care Med (1):

3 Learning Objectives: To be able to: Describe risk factors, outcomes associated with ICU delirium. Diagnose delirium in ICU patients. Know the elements of the ABCDEF Bundle. Implement the ABCDEF Bundle in your ICU.

4 Acute onset of cerebral dysfunction, characterized by 3 features*: A change or fluctuation in baseline mental status. Inattention. and either disorganized thinking, or an altered level of consciousness. *In: DSM-V, American Psychiatric Association, 2013
 Emotional disturbances (e.g., fear, anger, depression, apathy)")
5 Symptoms of ICU Delirium Hallucinations, delusions Sleep disturbances Abnormal psychometric activity (e.g., agitation, lethargy) Emotional disturbances (e.g., fear, anger, depression, apathy)
 Hypoactive (44%-90%) (Easy to identify!")
 Pandharipande, IntCareMed (2007) 33:1726 1731")
6 Subtypes of ICU Delirium Mixed (9%-54%) Hyperactive (1-2%) Hypoactive (44%-90%) (Easy to identify!) (Worse outcomes!) Pandharipande, IntCareMed (2007) 33: Peterson, J Am Geriatr Soc (2006) 54:
7 Epidemiology of ICU delirium Incidence: Risk factors: 60-80% of Mech. Ventilated ICU patients 20-50% of non-mv ICU patients Baseline: dementia, HTN, ETOH, acuity ICU acquired: deep sedation, coma, benzodiazepines Outcomes: ICU/Hospital: duration of MV, LOS, mortality Post-D/C: PTSD, cognitive dysfunction, physical disability, SNF placement, mortality Costs: 39% ICU costs, 31% hospital costs* $6.5 - $20.4 billion annually** *Milbrandt EB, et al. Crit. Care Med. 32 (4): , 2004 **Chang B, et al. Anesthesiology Clin 33: , 2015
8 ICU Delirium Duration & 1 yr. Mortality ICU delirium duration P<0.001 Fig. 2 K-M curve, 1-yr mortality post ICU admission vs. ICU delirium duration Pisani MA, Am J Respir Crit Care Med Dec 1;180(11):

9 ICU Delirium - What ICU Survivors Say I saw outlines of skeletons on the wall, heard strange sounds, etc. I believed I had been moved into various parts of the hospital, including the basement. I misinterpreted environmental cues and attempts to help me were interpreted as meanness. I actually saw body bags with my children's names on them! I tried to help them and I tried to communicate this to others, but with the tracheostomy tube I was unable to do this. After I was extubated and sedation was discontinued, I continued to have paranoid delusions about the nurses wanting to harm me. I repeatedly told my family that when I was dead, the nurses were going to put my body in a large trash can at the foot of my bed.


10 Causes of ICU Delirium Cholinergic activity Genetic predisposition Dopaminergic activity Primed microglial cells / Serotonergic activity Cavallazzi R, Annals of Intensive Care 2012, 2:49 GABA/NMDA receptor imbalance

11 Delirium goes undetected in most ICU patients. Validated delirium assessment tools ICU delirium dx. CAM-ICU, ICDSC are the most valid, reliable tools.* Delirium assessments should be performed >Q shift in all pts.* Routine delirium assessments are feasible in clinical practice.** *Barr J, Crit Care Med 2013; 41: **Vasilevskis EE, J Am Geriatr Soc 2011; 59 (Suppl 2):S249 S255
. Use of a validated ICU delirium assessment tool RN delirium detection rates (27% 92%).")
12 ICU Delirium Detection Rates Delirium goes undetected in 72% of ICU patients. Hypoactive delirium is harder to diagnose without using a validated assessment tool. Only 25-59% of ICU MDs screen ICU pts. for delirium (2/3 use clinical judgement). Use of a validated ICU delirium assessment tool RN delirium detection rates (27% 92%).* *Mistarz R, Aust Crit Care May;24(2):126-32

13 CAM-ICU Delirium Assessment Tool Sensitivity and Specificity >90%, = 0.91 Ely EW,

14 The Confusion Assessment Method for the ICU (CAM-ICU) training manual [
15 Within past 24 hr S A V E A H A A R T (>2 Errors) Inappropriate responses to questions or commands (>1 Error) CAM Positive RASS other than zero The Confusion Assessment Method for the ICU (CAM-ICU) training manual [
 Bergeron N. Intensive Care Med 2001, 27:859-864 Neziraj M, Acta Anaesthesiol Scand.")
16 Intensive Care Delirium Screening Checklist (ICDSC) Delirium Assessment Tool Delirious if ICDSC > 4 (sensitivity = 99%, specificity = 64%, κ = 0.92) Bergeron N. Intensive Care Med 2001, 27: Neziraj M, Acta Anaesthesiol Scand Aug;55(7):819-26




17 HALDOL


18 ICU Delirium Management Strategies Non- Pharmacologic Delirium Rx

19 What are Non-Pharmacologic ICU Delirium Management Strategies?


20 Non-Pharmacologic ICU Delirium Management Strategies 1. Optimize pain management 2. Avoid deep sedation 3. Eliminate deliriogenic medications 4. Facilitate ventilator weaning 5. Remove lines and tubes 6. Avoid restraints 7. Reorient patients 8. Promote normal sleep-wake cycles 9. Mobilize patients early 10. Engage ICU patients and families
21 Optimize ICU Pain Management Assess pain Q2hr, prn: NRS = 0 10 (self-report) CPOT (0 8) or BPS (3 12) (non-self report) Treat significant pain first before sedating pts (analgosedation): NRS 4 CPOT 3, BPS 6 Pain management: Non-neuropathic pain: IV opioids Neuropathic pain: PO gabapentin, carbamazepine Adjunctive: IV acetaminophen, NSAIDs, ketamine Thoracic epidurals: rib fractures, s/p AAA repair Barr J, et al. Crit Care Med (1):

22 Postoperative Pain Management Multimodal Pain Management Chou R, et al. The Journal of Pain 2016; 17(2):

23 Avoid Deep Sedation Deep Sedation: risk of ICU delirium (3x), MV, mortality! Tanaka LMS, et al. Critical Care 2014; 18:R156 Ouimet S, et al. Intensive Care Med 2007; 33:66 73 Hager DN, et al. Crit Care Med 2013 Jun; 41(6):
24 Avoid Deep Sedation Assess sedation Q2hr, prn: RASS (-5 to +4) SAS (1 to 7) Target light sedation: Definition: Patients are able to perform a variety of simple commands (i.e., RASS = 0 to -2, SAS = 3 to 4) Exceptions: ICP, status epilepticus, severe resp. failure, NMB Use sedation protocols sedative exposure: IV gtt: Targeted sedation strategy (TSS) constant light sedation Daily sedative interruption (DSI) deep to light sedation IV bolus dosing prn Barr J, et al. Crit Care Med 2013; 41(1): Shehabi Y, et al. AJRCCM 2012;186(8): Hager DN, et al. Crit Care Med 2013;41(6):
25 Deep Sedation In-Hospital Mortality (P = 0.004) Depth of Sedation On Day #2 Tanaka LMS, et al. Critical Care 2014; 18:R156
26 Deep Sedation Long-term Mortality Survival (%) Day #2 of sedation Shehabi Y, et al. AJRCCM 2012; 186:
 Antibiotics (e.g., quinalones, cefepime) Hayhurst CJ, et al. Anesthesiology 2016; 125(6):1299-41. Devlin JW, et al.")
27 Eliminate Deliriogenic Medications Sedatives (e.g, benzodiazepines >> propofol, DEX) Opioids (e.g, MSO4, meperidine) Anticholinergics (e.g., H2 blockers, atropine, diphenhydramine, amiodarone, ophthalmic medications) Corticosteroids (e.g., dexamethasone, methylprednisolone, hydrocortisone) Antibiotics (e.g., quinalones, cefepime) Hayhurst CJ, et al. Anesthesiology 2016; 125(6): Devlin JW, et al. (2012) In Papadopoulos J, et al. (Eds) Drug-Induced Coma and Delirium. In Drug-induced complications in the critically ill patient (pp ). Mount Prospect, IL: SCCM.
28 Sedation and Mechanical Ventilation DEX VERSED
29 Facilitate Ventilator Weaning: SAT + SBT Trials MV duration ICU LOS Control Intervention Difference P Control Intervention Difference P SAT 1 7.3d 4.9d 2.4d d 6.4d 3.5d 0.02 SBT 2 6d 4.5d 1.5d d 8d 1.0d NS SAT + SBT d* 14.7d* 3.1d d 9.1d 3.8d 0.01 *Vent free days 1 Kress JP, et al. NEJM 2000; 342: Ely EW, et al. NEJM 1996; 335: Girard T, et al. Lancet 2008; 371:

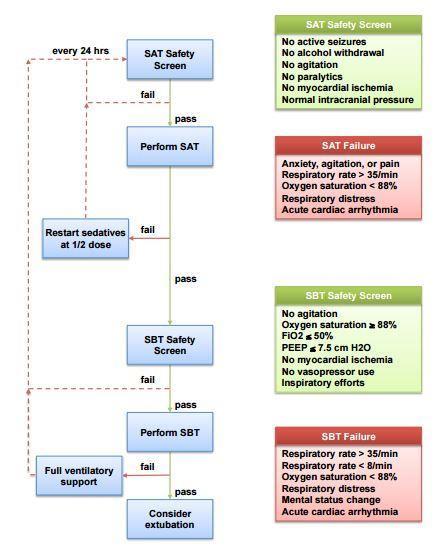
30 SAT-SBT Protocol SAT + SBT Trials

31 Remove Lines and Tubes
:105-114 Halm MA.")
32 Remove Lines and Tubes Chen Y, et al. Am J Crit Care 2013;22(2): Halm MA. Am J Crit Care 2008; 17(6):



33 Avoid Restraints Micek ST, et al. Crit Care Med 2005; 33:
. Van Rompaey B.")
34 Avoid Restraints The use of physical restraints before the onset of delirium showed a very high risk (OR 33.84). Van Rompaey B. Intensive and Critical Care Nursing 2008; 24:98 107


35 Avoid Restraints
 DSI CAM-ICU assessments BID (when RASS = -3 to +3) Intervention group: daily reorientation (5Ws +")
 Colombo R, et al.")
36 Reorient ICU Patients N = 314 med-surg ICU patients (excluded neuro, psych pts.) DSI CAM-ICU assessments BID (when RASS = -3 to +3) Intervention group: daily reorientation (5Ws + H), stimulation (wall clock, reading, favorite music), hearing aids/eyeglasses prn during DSI minimal light, noise at night Results: delirium incidence (35% 22%, P=0.02) Colombo R, et al. Minerva Anestesiol 2012; 78:

37 Promote Normal Sleep-Wake Cycles
:809-18.")
38 ICU Patient Sleep-Wake Cycles Cooper AB, et al. CHEST 2000; 117(3):
 Pain Medications (e.g., sedatives, opioids, etc.")
39 Sleep Deprivation in ICU Patients Causes: Round-the-clock environmental stimuli (e.g., noise, light, interactions) Pain Medications (e.g., sedatives, opioids, etc.) Mechanical ventilation Underlying acute illness Delirium Kaplow R. CCCNA 2016; 28(2):

40 ICU Nighttime Care Interactions N = 50 ICU pts., 147 nights Average of 42.6 interactions/night; only 6% of nights with no interactions x 2-3 hr! Tamburri LM, et al. AJCC 2004; 13:

41 Sleep Deprivation and ICU Delirium??
42 ICU Sleep Hygiene Programs Create a protected nighttime sleeping period (i.e., 2200 hr 0600 hr): Minimize, cluster patient care activities. Decrease light and noise in the patient s room. Have patients wear earplugs, eye masks. Use relaxation techniques (e.g., soothing music, massage, aromatherapy) Avoid sedatives, caffeinated beverages (i.e., nighttime sedation sleep promotion) Increase daytime activity: Increase mobility Open window shades Avoid daytime naps Oral melatonin Qhs? (Huang H, et al. Trials 2014;15:327, Burry L, et al. BMJ Open 2017; 7(3), Martinez FE, et al. Trials 2017;18(1):4) ICU sleep hygiene programs* incidence, duration of ICU delirium >50% *Alway A, et al. AACN 2013;22(4): *Van Rompaey B, et al. Critical Care 2012;16(3):R73 *Kamdar BB, et al. Anaesthesia 2014;69(6): *Patel J, et al. Anaesthesia 2014;69(6): Shaw R. AJCC 2016; 25(2):181-4.
43 Mobilize ICU Patients Early ICU Acquired Weakness*: Multifactorial syndrome myopathy &/or polyneuropathy Risk factors: sepsis, inflammation, MOSF, MV, BG, steroids, NMB agents >48h, F>M, immobility Incidence: 25% 100% Outcomes**: risk of MV wean failure (30%), ICU mortality (30%), hospital mortality (31%); hospital $$, 1 yr mortality, 50% of pts. fail to return to previous level of function! *Kress JP, et al. NEJM 2014; 370(17): **Hermans G, et al. AJRCCM 2014; 190(4): **Needham DM, et al. BMJ (Clinical research ed) 2013; 346:f1532 **Herridge MS, et al. NEJM 2003; 348(8):

:1874-1882 Morris PE, et al.")
44 Mobilize ICU Patients Early Mobility is Medicine. - Heidi Engel, PT, UCSF ICU/hospital LOS, sedative use, deep sedation, delirium Functional status at d/c Schweickert WD, et al. Lancet 2009; 373(9678): Morris PE, et al. Crit Care Med 2008; 36(8): Needham DM, et al. Topics in Stroke Rehab 2010; 17(4):



45 Mobilize ICU Patients Early Deep Sedation No Sedation
46 Engage ICU Patients and Families Davidson JF, et al. Crit Care Med 2017; 45:

47 Engage ICU Patients and Families ICU family presence 24h visitation, ICU rounds, resuscitations. ICU family support education, how to assist in pt. care, ICU diaries. Communication with ICU family members routine family conferences, using VALUE tool, provider education. Palliative Care involvement ICU patients with poor prognosis. Family /Staff Goals-of-Care conflicts Ethics consults, Social Work, Spiritual support Create ICU Policies EOL sedation/analgesia, create sleep promoting environment for ICU patients, families. Davidson JF, et al. Crit Care Med 2017; 45:
48 Engage ICU Patients and Families Family Members ICU Team
49 Medications Used to Treat Refractory ICU Delirium Sedatives Benzodiazepines: Midazolam Lorazepam Propofol Dexmedetomidine* Antipsychotics Haloperidol Atypical antipsychotics: Risperidone Ziprasidone Quetiapine Olanzapine No clear evidence for safety and efficacy in the treating delirium in ICU patients! *Reade, et al. JAMA 2016 Apr 12;315(14):1460-8
50 Provider Survey of Medications Used to Treat ICU Delirium Mo Y, et al. J Pharm Pract Apr;30(2):


51 Design: RCT Enrollment: 600+ Med-Surg ICU pts. dx. with delirium Rx: Haldol vs. Ziprasidone vs. Placebo 14d Outcomes: DCFD; side effects; ICU LOS; LTCD; 30d, 90d, 1yr survival





52 Treating ICU Delirium in the Substance Abuse Patient
53 Treatment of Withdrawal Symptoms Withdrawal From Alcohol Nicotine Opioids Benzodiazepines Dex, clonidine, gabapentin Illicit drugs (e.g., meth, PCP) Treatment* 1 st line: benzodiazepines; 2 nd line: phenobarbital, haldol, [chlomethiazole], clonidine? 3 rd line: propofol, Dex gtt (adj.) transdermal nicotine patch??? replacement rx, slow wean replacement rx, slow wean slow wean symptom management *Treatment should be symptom triggered, prn dosing, titrated to effect. (Few studies in ICU patients demonstrating safety, efficacy!) Awissi D, et al. Crit Care Med. 2013; 41:S57-S68.

54
55 ABCDEF Bundle* A Assess, Prevent and Manage Pain B Both SATs and SBTs C Choice of Sedation D Delirium: Assess, Prevent and Manage E Early Mobility and Exercise F Family Engagement and Empowerment *
56 ABCDEF Bundle Objectives Optimize pain management. Break the cycle of deep sedation and prolonged mechanical ventilation. Reduce the incidence, duration of ICU delirium. Improve short, long-term ICU patient outcomes. Reduce health care costs! *


:243-248 http://www.ihi.")
57 Why a Bundle? Standardize Care Processes Reduce Practice Variation Better Outcomes! Improve ICU Team Communication Every Patient, Every Time Resar R, Pronovost P, et al. JQPC 2005;31(5):


 ACT ABCDEF Bundle DO Tweak interventions")

58 ABCDEF Bundle Implementation Create multidisciplinary team Identify clinical champion Perform Gap Analysis Develop ABCDEF Bundle implementation plan PLAN Educate stakeholders Trial interventions Collect process, outcome data (EMR) ACT ABCDEF Bundle DO Tweak interventions Prepare to retest STUDY Analyze data Share results Get staff feedback *Pun BT, et al. Semin Resp Crit Care Med 2013;34:



59 How to implement the ABCDEF Bundle in Your ICU HELP! VS. Where to begin????

60 Implementing ABCDEF Bundle Elements Seven Steps to Success! STEP 1: Implement Pain, Sedation, Delirium assessment tools. STEP 2: Incorporate PAD assessments into daily ICU care plan. STEP 3: Create ICU specific PAD management protocols. STEP 4: Integrate PAD protocols w/ SATs, SBTs, EM protocols. STEP 5: Engage ICU patients and families. STEP 6: Measure Bundle Compliance, Performance. STEP 7: Measure Bundle impact on ICU patient outcomes. *Pun BT, et al. Semin Resp Crit Care Med 2013;34:



61 Step 1: Implement ICU Pain, Sedation, and Delirium Assessment Tools Pain, coma, & delirium = barriers! You don t know what you don t measure! SAT-SBT, Mobility, Family Engagement HOUSE OF PAD ICU PAD Protocols PAD Assessment Tools Assessments without protocols won t change practice!
62 Step 2: Incorporate PAD Assessments Into the Daily ICU Care Plan What is the patient s current pain score and their analgesia regimen? What is the patient s current and target sedation scores, and their current sedation regimen? What is the patient s current delirium score and what are their delirium risk factors? How do these PAD assessment influence our ICU care plan for today?
63 Step 3: Create ICU Specific Pain, Agitation, and Delirium Management Protocols Make protocols specific to your ICU culture, formulary. Use opt out rather than opt in protocol designs. Protocol benefits: Help transfer EBM best practices to the bedside. Limit practice variation. Reduce treatment delays. Improve ICU patient outcomes. Link to quality assurance efforts.






64 Step 4: Integrate PAD Management Early Mobility Pain Management SATs Sedation/ Agitation Management Delirium Management SBTs



65 Step 5: Engage ICU Patients and Families
66 Step 6: Measure ABCDEF Bundle Compliance and Performance* How do you know if your Bundle elements are working???
67 Bundle Element A Step 6: Measuring ABCDEF Bundle Compliance and Performance* Process Measure Chart NRS or CPOT Q2h Compliance Target Outcome Measure Performance Target >90% NRS 4 or CPOT 3 <30% B Daily SAT-SBT 1 >90% Extubated <60 min >80% C Chart RASS Q2hr >90% RASS > 0 or < -2 <30% D E F Chart CAM-ICU Q12h Chart mobility level Q24h Chart ICU Family Engagement QD >90% CAM-ICU positive <30% >90% >90% Standing or walking by ICU d/c >80% Family Satisfaction Survey 2 >80% 1 Mechanically ventilated ICU patients only, who passed SAT, SBT safety screens. 2 Satisfied or very satisfied responses *VA Palo Alto Medical Surgical ICU

68 Step 6: Measuring ABCDEF Bundle Compliance and Performance* VA Palo Alto Medical Surgical ICU
69 STEP 7: Measure ABCDEF Bundle Impact on ICU Patient Outcomes How do you know if your Bundle implementation is making a difference???
70 STEP 7: Measuring Impacts on ICU Patient Outcomes Outcome HRET Performance Target ICU Outcomes: Duration of MV N/A LOS N/A Mortality N/A Hospital Outcomes: LOS N/A Mortality Mobility status at D/C N/A N/A HAI Rate (CLABSI, CAUTI, VAE) <20% SSI Rate <20% VTE Rate <20% HAPU Rate <20% Fall Rate <20% Discharge Outcomes: D/C to home N/A 30d Readmission Rate <12% Post D/C Mortality (6 mo, 1 yr) N/A


71 STEP 7: Measuring Bundle Impact on ICU Outcomes CMS Medicare Reimbursement SGR Fee for Service Volume-based reimbursement MACRA MIPS Value-based reimbursement

72 ABCDEF Bundle: Improving ICU Patient Outcomes How do we know this works???? Barnes-Daly, et al. Crit Care Med 2017; 45:
73 ABCDEF Bundle: Improving ICU Patient Outcomes Hospital Survival Delirium, Coma Free Days Total Bundle Compliance N = 5,471 OR = 1.12 (95% CI, ; P <0.001) N = 5,581 IRR N = 1.02 (95% CI, ; IRR =, P P = 0.004) Partial Bundle Compliance N = 5,471 OR = 1.23 (95% CI, ; P <0.001) N = 5,581 IRR = 1.15 (95% CI, ; P = 0.001) Bundle Dose-Response Effect! Barnes-Daly, et al. Crit Care Med 2017; 45:
74
, 3 Regions (SE, MW, West) Tools: meetings, webinars, list serve, REDCAP database. QI strategies: Bundle adoption, compliance, and improve outcomes.")
75 ICU Liberation Collaborative Andrea Saito, ACNP (Team Leader) ABCDEF Bundle Team VA Palo Alto Health Care System Palo Alto, CA Goal: Implement the ABCDEF Bundle over 20 months ( ). ICUs: 77 U.S. ICUs (69 adult, 8 pediatric), 3 Regions (SE, MW, West) Tools: meetings, webinars, list serve, REDCAP database. QI strategies: Bundle adoption, compliance, and improve outcomes. Enrollment: Total N = 17,069 ICU pts. Pre-Bundle: 1,982 pts. (6 mo.) Post-Bundle: 15,087 pts. (14 mo.)
76 VAPAHCS* ABCDEF Bundle Compliance and Performance Bundle Element A B C D E F Process Measure Assess NRS or CPOT <Q2h Assess SAT/SBT Daily Assess RASS Q2hr Assess CAM-ICU Q12h Assess Mobility QD Chart ICU Family Engagement QD Compliance Outcome Performance Pre Post Measure Pre Post 100% 100% NRS 4 or CPOT 3 38% 47% 13%/ 14% 54%/ 100% Perform Daily SAT/SBT 16%/ 54% 31%/ 100% 96% 98% RASS -4 or -5 >1d 42% 30% 71% 97% CAM-ICU + >1d 21% 19% 0% 12% 65% 60% Active transfer, standing, or walking 44% 59% Family Satisfaction Survey N/A N/A *VAPAHCS Pre: (Retrospective = 6 mo.) N=33; Post: (Prospective = 14 mo.) N = 238

77 VAPAHCS Overall ABCDEF Bundle Performance VAPAHCS Post Bundle = 86% Pre Bundle = 68% 27% increase!
78 VAPAHCS* ABCDEF Bundle Collaborative Patient Outcomes Outcome Pre Bundle 1 Post Bundle 1 Duration of MV 2 21 hours 22 hours ICU LOS 7.3 days 5.0 days Hospital LOS 21 days 19 days ICU Mortality Rate 6% 5% Hospital Mortality Rate 3 0% 5% *VAPAHCS Total N = 271 Pre N = 33 (Retrospec. = 6 mo.), Post N = 238 (Prospec. = 14 mo.) 1 Results reported as Medians, P Values TBD 2 MV pts: Total = 116 (19 pre, 97 post) 3 Died during hospitalization after ICU discharge.

79 ICU Liberation Collaborative

80 ICU Liberation Collaborative

81 ICU Liberation Collaborative

82 ICU Liberation Collaborative

83 ICU Liberation Collaborative

84 ICU Liberation Collaborative NEVER Delirious! Increased 41% to 56%

85 ICU Liberation Collaborative

86 ICU Liberation Collaborative Active Mobility Mean Increase: 20% to 24%

87 ICU Liberation Collaborative

88 ICU Liberation Collaborative
89 ICU Liberation Collaborative Patient Outcomes Outcome Pre-Bundle 1 Post-Bundle 1 Duration of MV 2 65 hours 55 hours ICU LOS 3.5 days 3.0 days Hospital LOS 8.5 days 8.0 days ICU Mortality Rate 13% 11% Hospital Mortality Rate 3 4% 3% Total N = 17,069, Pre Bundle N = 1,982, Post Bundle N = 15,087 1 Results Reported as Medians, P Values TBD 2 MV pts: Total = 16,735 (Pre N = 1,905, Post N = 14,830) 3 Died during hospitalization after ICU discharge.

90 ABCDEF Bundle

91 The ABCDEF Bundle Redefining ICU Outcomes Immobility Deep Sedation Mechanical Ventilation






92 The ABCDEF Bundle Redefining ICU Outcomes Not just surviving, but thriving!


93 Thank You!

94 Questions?
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018
 ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
KEY REFERENCES Laying the foundation for D of ABCDEF bundle
 KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS
 ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation
 Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
Executive Sponsorship of Delirium Initiatives Lessons from ICU Liberation J. Matthew Aldrich, MD Co-Chair, SCCM ICU Liberation Committee Associate Professor Medical Director, Critical Care Medicine UCSF
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network
 Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium
 ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium Diane Byrum MSN RN CCRN-K CCNS FCCM Quality Implementation Consultant Innovative Solutions For Healthcare Education, LLC Oak Island, NC ICU
ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium Diane Byrum MSN RN CCRN-K CCNS FCCM Quality Implementation Consultant Innovative Solutions For Healthcare Education, LLC Oak Island, NC ICU
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Delirium Screening and Prevention Faculty Disclosures
 Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention. Faculty Disclosures. Objectives 5/13/2014. I have nothing to disclose
 Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Critical Care Strategic Clinical Network Provincial ICU Delirium Framework
 Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry
 Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients
 Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice
 in the Intensive Care Unit: Translating Evidence Into Practice") Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
ICU Delirium and sedation: understanding their role in long-term patient outcomes. Yoanna Skrobik MD FRCP(c)
") ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients
 Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Conflict of Interest. Patient Case. Objectives. The Balancing Act. Why We Need Sedation
 Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Putting the Pieces of the Puzzle Together: A Journey through ABCDEF
 Putting the Pieces of the Puzzle Together: A Journey through ABCDEF Kristy Colford RN,BSN, CCRN Clinical Nurse Educator Avera McKennan Intensive Care Kristy Colford- Have No Disclosures ZOOM in & ZOOM
Putting the Pieces of the Puzzle Together: A Journey through ABCDEF Kristy Colford RN,BSN, CCRN Clinical Nurse Educator Avera McKennan Intensive Care Kristy Colford- Have No Disclosures ZOOM in & ZOOM
Implementing the 2013 PAD Guidelines
 1 of 20 8/11/2013 10:25 PM www.medscape.com Implementing the 2013 PAD Guidelines Top Ten Points to Consider Brenda T. Pun, MSN, RN, ACNP, Michele C. Balas, PhD, RN, APRN-NP, CCRN, Judy Davidson, DNP, RN,
1 of 20 8/11/2013 10:25 PM www.medscape.com Implementing the 2013 PAD Guidelines Top Ten Points to Consider Brenda T. Pun, MSN, RN, ACNP, Michele C. Balas, PhD, RN, APRN-NP, CCRN, Judy Davidson, DNP, RN,
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR
 Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION
 ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
Delirium: Prevention with Melatonin
 Delirium: Prevention with Melatonin Lisa Burry, PharmD Department of Pharmacy, Mount Sinai Hospital Leslie Dan Faculty of Pharmacy, University of Toronto Disclosures Centre for Collaborative Drug Research,
Delirium: Prevention with Melatonin Lisa Burry, PharmD Department of Pharmacy, Mount Sinai Hospital Leslie Dan Faculty of Pharmacy, University of Toronto Disclosures Centre for Collaborative Drug Research,
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
KEY REFERENCES laying the foundation for A of ABCDEF bundle
 KEY REFERENCES laying the foundation for A of ABCDEF bundle Puntillo K. Am J Crit Care (Response Procedural Pain) 2001;10:238-251 Payen J. Crit Care Med (Behavioral Pain Scale) 2001;29:2258-2263 Gelinas
KEY REFERENCES laying the foundation for A of ABCDEF bundle Puntillo K. Am J Crit Care (Response Procedural Pain) 2001;10:238-251 Payen J. Crit Care Med (Behavioral Pain Scale) 2001;29:2258-2263 Gelinas
Strategies for Enhancing Sepsis Survivorship
 Strategies for Enhancing Sepsis Survivorship Hallie Prescott, MD, MSc Ohio Hospital Association August 16, 2016 Disclosures I have no relevant financial conflicts of interest Key Funding NIH/NIGMS American
Strategies for Enhancing Sepsis Survivorship Hallie Prescott, MD, MSc Ohio Hospital Association August 16, 2016 Disclosures I have no relevant financial conflicts of interest Key Funding NIH/NIGMS American
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Delirium and ICU Liberation: Impact on Survival and Survivorship
 Delirium and ICU Liberation: Impact on Survival and Survivorship E. Wesley Ely, MD, MPH Professor of Medicine and Critical Care Vanderbilt University, Nashville, TN VA TN Valley Health Care System GRECC
Delirium and ICU Liberation: Impact on Survival and Survivorship E. Wesley Ely, MD, MPH Professor of Medicine and Critical Care Vanderbilt University, Nashville, TN VA TN Valley Health Care System GRECC
Management of delirium in mechanically ventilated patients. Advances in Critical Care Medicine King Hussein Cancer Center
 Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know
 Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, MS, CPNP-AC/PC, CNS, CCRN Pediatric Intensive Care Nurse Practitioner Lucile Packard
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, MS, CPNP-AC/PC, CNS, CCRN Pediatric Intensive Care Nurse Practitioner Lucile Packard
What you need to know about Delirium in ICU. Dr Valerie Page Watford General Hospital
 What you need to know about Delirium in ICU Dr Valerie Page Watford General Hospital Delirium and outcome 40 year old ARDS ICU survivor college graduate I have been out of hospital and trying to get on
What you need to know about Delirium in ICU Dr Valerie Page Watford General Hospital Delirium and outcome 40 year old ARDS ICU survivor college graduate I have been out of hospital and trying to get on
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know
 Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, PhD, CPNP-AC/PC, CNS; Cincinnati Children s Hospital Medical Center Mary Rummell,
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, PhD, CPNP-AC/PC, CNS; Cincinnati Children s Hospital Medical Center Mary Rummell,
MARIA KOBYLECKY RN, MScN, CNCC JEANENE LUCKHART BSc, Grad Dip PT CELINA ROGERS RRT SUZANNE WATTS BHSc PT
 MARIA KOBYLECKY RN, MScN, CNCC JEANENE LUCKHART BSc, Grad Dip PT CELINA ROGERS RRT SUZANNE WATTS BHSc PT Objectives Understand some of the detrimental effects of critical illness, prolonged bed rest and
MARIA KOBYLECKY RN, MScN, CNCC JEANENE LUCKHART BSc, Grad Dip PT CELINA ROGERS RRT SUZANNE WATTS BHSc PT Objectives Understand some of the detrimental effects of critical illness, prolonged bed rest and
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Early Goal Directed Sedation In Critically Ill Patients
 Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018
 Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Charles Bernick, MD, MPH Cleveland Clinic Lou Ruvo Center for Brain Health June 2, 2018 Delirium common Prolongs hospitalization Worsens dementia ( if you survive) Increased risk of institutionalization
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc.
 MSc.") Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment
 Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment Julie Miller, RN, BSN, CCRN How many of you routinely assess for delirium in your patients? 2013 SCCM Guidelines Pain Recommend
Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment Julie Miller, RN, BSN, CCRN How many of you routinely assess for delirium in your patients? 2013 SCCM Guidelines Pain Recommend
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Management of pain, agitation, and delirium in critically ill patients
 REVIEW ARTICLE Management of pain, agitation, and delirium in critically ill patients Pratik P. Pandharipande 1,2, Mayur B. Patel 2,3, Juliana Barr 4 1 Division of Critical Care, Department of Anesthesiology,
REVIEW ARTICLE Management of pain, agitation, and delirium in critically ill patients Pratik P. Pandharipande 1,2, Mayur B. Patel 2,3, Juliana Barr 4 1 Division of Critical Care, Department of Anesthesiology,
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
7/6/ ANNUAL MEETING BRINGING THE ABC(DEF) S TO THE ICU ICU TRIAD DISCLOSURE ICU TRIAD SEDATION AND ANALGESIA OBJECTIVES
 S TO THE ICU ICU TRIAD DISCLOSURE ICU TRIAD SEDATION AND ANALGESIA OBJECTIVES") ICU TRIAD BRINGING THE ABC(DEF) S TO THE ICU GINA RIGGI, PHARMD, BCPS, BCCCP CLINICAL HOSPITAL PHARMACIST- TRAUMA INTENSIVE CARE UNIT JACKSON MEMORIAL HOSPITAL MIAMI, FLORIDA Figure 1. Reade M and Finfer
ICU TRIAD BRINGING THE ABC(DEF) S TO THE ICU GINA RIGGI, PHARMD, BCPS, BCCCP CLINICAL HOSPITAL PHARMACIST- TRAUMA INTENSIVE CARE UNIT JACKSON MEMORIAL HOSPITAL MIAMI, FLORIDA Figure 1. Reade M and Finfer
Sedation in The ICU: The Biological Cost of the Depression of Consciousness
 Sedation in The ICU: The Biological Cost of the Depression of Consciousness Michael Ramsay MD FRCA Chairman Department of Anesthesia Baylor University Medical Center Professor Texas A&M University Clinical
Sedation in The ICU: The Biological Cost of the Depression of Consciousness Michael Ramsay MD FRCA Chairman Department of Anesthesia Baylor University Medical Center Professor Texas A&M University Clinical
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit
 Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit BY: ABBY WACHHOLTZ, BSN, RN, PEDIATRIC ACUTE CARE DNP STUDENT Disclosures I have no disclosures. 1 Objectives 1. Recognize
Implementation of a Delirium Screening Tool in a Pediatric Intensive Care Unit BY: ABBY WACHHOLTZ, BSN, RN, PEDIATRIC ACUTE CARE DNP STUDENT Disclosures I have no disclosures. 1 Objectives 1. Recognize
Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine
 Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine Define AMS and delirium Describe how to recognize and diagnose delirium Identify the predisposing or precipitating
Renee Flores, MD Division of Geriatrics & Palliative Medicine Department of Internal Medicine Define AMS and delirium Describe how to recognize and diagnose delirium Identify the predisposing or precipitating
Integrated Care of Patients on Constant Observation in a General Hospital Setting Aaron Pinkhasov, MD
 Integrated Care of Patients on Constant Observation in a General Hospital Setting Aaron Pinkhasov, MD Chairman, Department of Behavioral Health NYU Winthrop Hospital Associate Professor of Psychiatry and
Integrated Care of Patients on Constant Observation in a General Hospital Setting Aaron Pinkhasov, MD Chairman, Department of Behavioral Health NYU Winthrop Hospital Associate Professor of Psychiatry and
Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes
 The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium Monograph - Update, Spring 2014
 Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
Symptom Management Pocket Guides: DELIRIUM
 Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
ICU Delirium A Real Epidemic (or are we delirious)?
?") ICU Delirium A Real Epidemic (or are we delirious)? CCCF: Toronto October 2014 Jesse Hall MD University of Chicago Section of Pulmonary and Critical Care Medicine Faculty Disclosures Dr. Hall receives
ICU Delirium A Real Epidemic (or are we delirious)? CCCF: Toronto October 2014 Jesse Hall MD University of Chicago Section of Pulmonary and Critical Care Medicine Faculty Disclosures Dr. Hall receives
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients
 Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Naeem Ali, MD Medical Director. The Ohio State University Wexner Medical Center
 Update in Critical Care, 2012: Teamwork in the ICU Naeem Ali, MD Medical Director Medical Intensive Care Unit The Ohio State University Wexner Medical Center 1 Many developments in Critical Care Emergence
Update in Critical Care, 2012: Teamwork in the ICU Naeem Ali, MD Medical Director Medical Intensive Care Unit The Ohio State University Wexner Medical Center 1 Many developments in Critical Care Emergence
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State
 Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health