Disclosures. Grant funding, salary/employment, consulting fee, honorarium or equity
|
|
|
- Gordon Thomas
- 5 years ago
- Views:
Transcription
1 Grant funding, salary/employment, consulting fee, honorarium or equity Disclosures IP related to concussion and brain injury assessment IP related to assessment of dementia after brain injury IP related to treatment of intracranial hemorrhage Abbott Diagnostic Laboratories Continuing Legal Education in MN, NY Hennepin County Medical Center Hennepin Health Foundation Integra Corporation Islamic Medical Association of North America Medtronic Corporation Minnesota Brain Injury Alliance National Football League National Neurotrauma Society North American Brain Injury Society Oculogica Inc. Steven and Alexandra Cohen Foundation for Veteran Post Traumatic Stress and Traumatic Brain Injury Texas, Minnesota, and Wisconsin High School Coaches Association United States Veterans Administration and Office of Research and Development USA Football


2 Prospective Treatment of Traumatic Brain Injuries by Vagus Nerve Stimulation Presenters: Hannah Casey and Tessneem Abdallah Molly Hubbard, MD, Thomas Bergman, MD, Rebekah Kroll, BA, Uzma Samadani, MD, PhD

3

4
5 Our Mission "The goal of the Hennepin County Medical Center Brain Injury Research Lab is to classify, treat, and prevent brain injury, and improve brain health in the greater Minneapolis/St Paul community by creating innovative, sustainable solutions that can then be scaled to serve larger communities throughout the world."
6
7 I. CLASSIFY A. CLASSIFY-I: Biomarkers in CT + patients B. CLASSIFY-II: Serum biomarkers in Pediatric vs Adult population C. CLASSIFY-III: Serum vs CSF biomarkers D. CLASSIFY-IV: BDNF and TAU in Acute vs. Long Term patients E. CLASSIFY-V: Biomarkers in Blunt Force vs Non-trauma patients F. CLASSIFY-VI: Intracranial Hemorrhage size and GFAP G. CLASSIFY-VII: Biomarkers in Anoxia vs DAI H. CLASSIFY-VIII: Biomarkers in Brain Death I. CLASSIFY-IX: Early biomarkers in TBI J. CLASSIFY-X: Biomarkers in Crush Injury 1. MRI 2. Kinetic 3. i-stat II. Chronic Effects of Neurotrauma (CENTS) III. Eye Tracking and Neurovision Rehabilitation of Oculomotor Dysfunction in Mild Traumatic Brain Injuries IV. Transforming Research and Clinical Knowledge in TBI (TRACK-TBI) V. Traumatic brain injury Reduction in Athletes by Neck strengthening (TRAiN) VI. Epidural STimulation After Neurologic Damage (E-STAND) Clinical Trial VII. VERTEX VIII.VANISH Clinical Trial (Vagal Activation of NeuroImmune Systems to Heal traumatic brain injury)
8 Vagus Nerve Stimulation (VNS)
9 History of VNS In 1937, Percival Bailey- neurosurgeon and psychiatrist- found that stimulation of the severed end of a vagus nerve would induce cortical changes on an EEG. In 1988, Jacob Zabara developed a vagus nerve stimulator which reduced seizure activity in dogs. In 1997: FDA approved VNS for seizure activity In 2005: It was approved as treatment for depression
10 Vagus Nerve (Cranial Nerve X)
11

12
13
14

15


16


17


18 Forebrain Cerebrum, thalamus, hypothalamus Complex sensory and neural functions

19 Thalamus Relay Center of the brain Regulates consciousness, sleep/alertness

20 Reticular Formation Nerve pathways that mediate level of consciousness
21

22
23

24
25
26 VANISH Clinical Trial Vagal Activation of NeuroImmune Systems to Heal traumatic brain injury
27 Molly Hubbard, MD Rebekah Kroll, BA Thomas Bergman, MD Tessneem Abdallah, BA Hannah Casey Uzma Samadani, MD, PhD
28 Study Type Single-center Randomized (1:1) Group 1: 30 subjects with concussion TBI Group 2: 30 subjects with moderate TBI 15 active/15 sham in each group Double-blind Sham-controlled Parallel-arm study
29 Objective The primary objective of this study is to provide initial evidence of use of the noninvasive vagus nerve stimulator (gammacore device) for treatment of patients recovering from concussion and moderate traumatic brain injury to improve clinical recovery. This study generally aims to collect randomized comparative data on the safety and efficacy of the device.
30 Hypotheses Stimulation of the vagus nerve results in increased cerebral blood flow and metabolism in the forebrain, thalamus and reticular formation (1), which promotes arousal and improved consciousness (2), thereby improving outcome after traumatic brain injury resulting in impaired consciousness.
31 Interventional Treatment Dosing 2 stimulation doses each day Each dose consists of two 120 second stimulation treatments Left side of the neck 12 week period Patient-administered


32

33
34 Effectiveness Endpoints Primary Effectiveness Endpoint The primary effectiveness endpoints are to evaluate whether vagus nerve stimulation impacts clinical recovery from moderate traumatic brain injury as assessed by the cognitive assessments, functional assessments, and depression index at all study time-points between treatment groups. Secondary Endpoint The secondary endpoints for concussion and moderate traumatic brain injury patients are: heart rate variability (HRV), commercially available cognitive assessments, functional recovery assessments, depression inventory, blood-based biomarkers, non-invasive physical exam, and eye tracking metrics relative to norms. The final secondary endpoint is determination of whether a large-scale prospective randomized trial evaluating the efficacy and parameters of vagus nerve stimulation for recovery from concussion and moderate traumatic brain injury is justifiable.
35 Time of Injury 2 weeks 6 weeks 12 weeks 18 weeks
36 Time of Injury 2 weeks 6 weeks 12 weeks 18 weeks Visit 0 Visit 1 Visit 2
37 T 0 : Visit 0 (Screening Visit) General Medical Questions EKG Urine Pregnancy tests (females) EEG
38 Inclusion Criteria Written Informed Consent years Meets the criteria of the Head Injury Interdisciplinary Special Interest Group of the American Congress of Rehabilitation Medicine, which defines a head injury as a traumatically induced physiologic disruption of brain function, as manifested by one of the following: Any period of loss of consciousness (LOC), Any loss of memory for events immediately before or after the accident, Any alteration in mental state at the time of the accident, Focal neurologic deficits, which may or may not be transient.
39 Inclusion Criteria (continued) Meets the criteria for moderate TBI as defined by the Head Injury Interdisciplinary Special Interest Group of the American Congress of Rehabilitation Medicine, which are as follows: Length of stay at least 48 hours, Glasgow Coma Scale (GCS score of 9-12 or higher) Operative intracranial lesion, Abnormal CT scan findings. May have had a craniotomy, but those with hydrocephalus or active intracranial pressure elevation will be excluded. Able to accurately communicate the sensation of amplitude of intensity by the stimulation treatment with the GammaCore device. Has a stable orthopedic or other traumatic body injury. Is capable of completing all study assessments.
40 Inclusion Criteria (continued) Agrees to use the GammaCore device as intended and follow all of the requirements of the study, including follow-up visits. Agrees to record usage of the GammaCore device, all required study data, and report any adverse effects to the sponsor/investigator within 24 hours of any such adverse event. No evidence of focal or generalized interictal discharges on EEG. Willing and able to complete the study
41 Exclusion Criteria Has an active DNR/DNI (do not resuscitate/do not intubate) request. Has dissent among family members/next of kin regarding level of care. Has a penetrating injury. Has concurrent active severe medical problems (psychiatric or otherwise) or conditions, which could prevent survival during the course of the study. Has pre-existing central nervous system disease or associated comorbidities that may not allow for an 18-week follow-up visit. Has an abscess, infection or lesion (including lymphadenopathy) at the gammacore treatment site. Has known or suspected moderate to severe atherosclerotic cardiovascular disease, carotid artery disease (e.g. bruits or history of TIA or CVA). Has a clinically significant irregular heart rate or rhythm.
42 Exclusion Criteria (continued) Has uncontrolled hypertension (systolic bp > 200 or diastolic bp >100), recent (within the last 3 months) heart attack, recent (within the last 3 months) stroke, known aortic aneurysm, or congestive heart failure (CHF). Is currently implanted with an electrical and/or neurostimulator device, including but not limited to cardiac pacemaker, defibrillator, vagal neurostimulator, deep brain stimulator, spinal stimulator, bone growth stimulator, or cochlear implant. Has a history of significant carotid endarterectomy, vagotomy, dysaesthesia or vascular neck surgery on either side of the neck. Has been implanted with metal cervical spine hardware. Has a recent or repeated history of syncope. Has a recent or repeated history of seizures.
43 Exclusion Criteria (continued) Has known clotting disorder or hemophilia. Has anemia (hb<12). Is pregnant or nursing, or of childbearing potential and is unwilling to use an accepted form of birth control (hormonal, barrier method, surgical, or abstention or is at least two years post-menopause). Is participating in any other therapeutic clinical investigation or has participated in a clinical trial in the preceding 30 days. Is an employee of the clinical study site or a relative of the Investigator. Has an abnormal baseline electrocardiogram (ECG), including second and third degree heart block, atrial fibrillation, atrial flutter, recent history of ventricular tachycardia or ventricular fibrillation or clinically significant premature ventricular contraction. Has a known history or suspicion of substance abuse or addiction.
44 If eligible... Assigned study materials Training on administration of treatment with the device Training on all aspects and requirements of the study including completion of the Subject Diary, post-treatment and adverse event reporting and follow-up visit requirements, Vital signs (temperature, heart rate, respiratory rate, and blood pressure) Neurologic and cognitive evaluations Functional measure of independence Depression questionnaire Eye tracking algorithm Non-invasive physical examination Heart rate variability 10 cc baseline serum sample will be obtained by phlebotomy Schedule Visit 1 Follow Up within 72 hours +/- 1 day from screening visit
45 T 1 : Visit 1 (Baseline) Review subject s general well-being First interventional treatment with the gammacore device and review of any adverse events, discuss any unresolved or new adverse events identified T 2 : Visit 2 (Phone Call) Review subject s general well-being Discuss interventional treatment with the gammacore device and for any adverse events, discuss any unresolved or new adverse events identified since the previous visit, document and record according to the parameters of the Adverse Event CRF
46 Time of Injury 2 weeks 6 weeks 12 weeks 18 weeks Visit 3
47 T 3 : Visit 3 Return of completed diary and is provided with new diary if needed Review subject s diary for adverse events, discuss any unresolved or new adverse events identified since the previous visit. Review medications (specifically for change in medication usage), and that all diary questionnaires have been completed. Perform gammacore treatment during office visit (to assure treatment procedure is being performed accurately). Vital signs (temperature, heart rate, respiratory rate, and blood pressure). Neurologic and Cognitive evaluations Non-invasive physical exam Eye tracking algorithm EKG Heart rate variability Discuss requirements of the next 4-weeks with the subject and subjects caregiver, including completion of the Subject Diary, adverse event reporting and follow-up visit requirements
48 Time of Injury 2 weeks 12 weeks 18 weeks 6 weeks Visit 4
49 T 4 : Visit 4 Return of completed diary and is provided with new diary if needed Review subject s diary for adverse events, discuss any unresolved or new adverse events identified since the previous visit. Review medications (specifically for change in medication usage), and that all diary questionnaires have been completed. Perform gammacore treatment during office visit (to assure treatment procedure is being performed accurately). Vital signs (temperature, heart rate, respiratory rate, and blood pressure). Neurologic and Cognitive evaluations Non-invasive physical exam Eye tracking algorithm EKG Heart rate variability Discuss requirements of the next 6-weeks with the subject and subjects caregiver, including completion of the Subject Diary, adverse event reporting and follow-up visit requirements
50 Time of Injury 2 weeks 6 weeks 18 weeks 12 weeks Visit 5
51 T 5 : Visit 5 Return used device. Return of completed diary and is provided with new diary. Review subject s diary for adverse events, discuss any unresolved or new adverse events identified since the previous visit. Review medications (specifically for change in medication usage), and that all diary questionnaires have been completed. Perform gammacore treatment during office visit (to assure treatment procedure is being performed accurately) Vital signs (temperature, heart rate, respiratory rate, and blood pressure) Neurologic and cognitive evaluations Non-invasive physical exam Eye tracking algorithm EKG Heart rate variability Serum sample will be obtained by phlebotomy Discuss requirements of the next 6-weeks with the subject, including completion of the Subject Diary, adverse event reporting and follow-up visit requirements.
52 Time of Injury 2 weeks 6 weeks 12 weeks 18 weeks Visit 6
53 T 6 : Time 6 Return of completed diary. Review subject s diary for adverse events, discuss any unresolved or new adverse events identified since the previous visit. Review medications (specifically for change in medication usage), and that all diary questionnaires have been completed. Vital signs (temperature, heart rate, respiratory rate, and blood pressure) Neurologic and cognitive evaluations Non-invasive physical exam Eye tracking algorithm EKG Serum sample will be obtained by phlebotomy, EEG will be done on all patients to evaluate for changes from baseline using quantitative EEG.
54 Eye-Tracking

55

56 Control


57 Week 2 Week 18
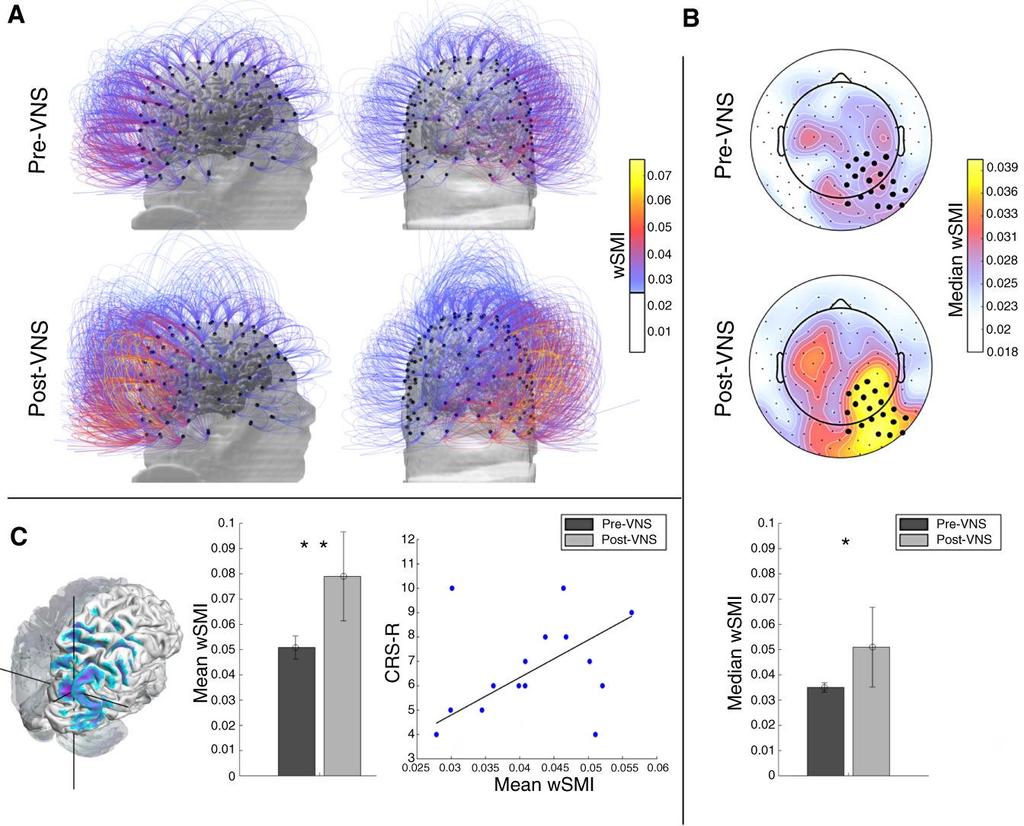
58 Preliminary Data

59
60 Side Effects Redness at the treatment site Irritation at the treatment site Related to previous case of shingle and existing burning from injury Tingling at the treatment site Headaches

61
62 Website: Facebook: Brain Injury Research Lab YouTube: Brain Injury Research Lab
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
(U) USSOCOM. (U) Magnetic qeeg guided Resonance Therapy (MeRT)
 USSOCOM. (U) Magnetic qeeg guided Resonance Therapy (MeRT)") United States Special Operations Command (U) USSOCOM MeRT Clinical Trial for Treatment of TBI COL Mark Baggett, Ph.D., US Army USSOCOM Command Psychologist Date: 14 Feb 2018 1 (U) Magnetic qeeg guided
United States Special Operations Command (U) USSOCOM MeRT Clinical Trial for Treatment of TBI COL Mark Baggett, Ph.D., US Army USSOCOM Command Psychologist Date: 14 Feb 2018 1 (U) Magnetic qeeg guided
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Neurology: The pilot, the AME, the FAA. John Hastings CAMA, Greensboro NC September 2017
 Neurology: The pilot, the AME, the FAA John Hastings CAMA, Greensboro NC September 2017 Aviation Safety As AME s and regulators, we have a primary obligation to aviation safety Arguably, we also have an
Neurology: The pilot, the AME, the FAA John Hastings CAMA, Greensboro NC September 2017 Aviation Safety As AME s and regulators, we have a primary obligation to aviation safety Arguably, we also have an
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
The Brain Injury Research Lab Spring 2018 Newsletter
 The Brain Injury Research Lab Spring 2018 Newsletter Did you miss our patient presentations at the Minnesota State Spinal Cord Injury and Traumatic Brain Injury Research Symposium? No problem! Catch them
The Brain Injury Research Lab Spring 2018 Newsletter Did you miss our patient presentations at the Minnesota State Spinal Cord Injury and Traumatic Brain Injury Research Symposium? No problem! Catch them
Alliance A Symptomatic brain radionecrosis after receiving radiosurgery for
 RANDOMIZED PHASE II STUDY: CORTICOSTEROIDS + BEVACIZUMAB VS. CORTICOSTEROIDS + PLACEBO (BEST) FOR RADIONECROSIS AFTER RADIOSURGERY FOR BRAIN METASTASES Pre-registration Eligibility Criteria Required Initial
RANDOMIZED PHASE II STUDY: CORTICOSTEROIDS + BEVACIZUMAB VS. CORTICOSTEROIDS + PLACEBO (BEST) FOR RADIONECROSIS AFTER RADIOSURGERY FOR BRAIN METASTASES Pre-registration Eligibility Criteria Required Initial
Disclosure Statement. Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk.
 Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Disclosure Statement Dr. Kadish has no relevant financial relationships with any commercial interests mentioned in this talk. Head Trauma Evaluation Primary and secondary injury Disposition Sports related
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
THE FRAMINGHAM STUDY Protocol for data set vr_soe_2009_m_0522 CRITERIA FOR EVENTS. 1. Cardiovascular Disease
 THE FRAMINGHAM STUDY Protocol for data set vr_soe_2009_m_0522 CRITERIA FOR EVENTS 1. Cardiovascular Disease Cardiovascular disease is considered to have developed if there was a definite manifestation
THE FRAMINGHAM STUDY Protocol for data set vr_soe_2009_m_0522 CRITERIA FOR EVENTS 1. Cardiovascular Disease Cardiovascular disease is considered to have developed if there was a definite manifestation
Single Seizure of Unknown Cause
 S1: Medical Standards for Safety Critical Workers with Seizures of Unknown Cause 1. Seizure or Epilepsy of Unknown Cause are the classifications used in these medical standards for a probable seizure(s),
S1: Medical Standards for Safety Critical Workers with Seizures of Unknown Cause 1. Seizure or Epilepsy of Unknown Cause are the classifications used in these medical standards for a probable seizure(s),
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Patient Manual Brainsway Deep Transcranial Magnetic Stimulation (Deep TMS) System for Treatment of Major Depressive Disorder
 System for Treatment of Major Depressive Disorder") Dr. Zahida Tayyib www.mvptms.com Patient Manual Brainsway Deep Transcranial Magnetic Stimulation (Deep TMS) System for Treatment of Major Depressive Disorder If you are considering Brainsway Deep treatment
Dr. Zahida Tayyib www.mvptms.com Patient Manual Brainsway Deep Transcranial Magnetic Stimulation (Deep TMS) System for Treatment of Major Depressive Disorder If you are considering Brainsway Deep treatment
Cardiovascular Diseases and Diabetes
 Cardiovascular Diseases and Diabetes LEARNING OBJECTIVES Ø Identify the components of the cardiovascular system and the various types of cardiovascular disease Ø Discuss ways of promoting cardiovascular
Cardiovascular Diseases and Diabetes LEARNING OBJECTIVES Ø Identify the components of the cardiovascular system and the various types of cardiovascular disease Ø Discuss ways of promoting cardiovascular
DISORDERS OF THE NERVOUS SYSTEM
 DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
Procedures commonly seen at Vanderbilt Medical Center PACU s: Cervical, thoracic, lumbar, and sacral spine surgeries. Goes to 6N
 Procedures commonly seen at Vanderbilt Medical Center PACU s: Cervical, thoracic, lumbar, and sacral spine surgeries Goes to 6N Burr holes and Craniotomies for hemorrhage, tumors, trauma, debulking Goes
Procedures commonly seen at Vanderbilt Medical Center PACU s: Cervical, thoracic, lumbar, and sacral spine surgeries Goes to 6N Burr holes and Craniotomies for hemorrhage, tumors, trauma, debulking Goes
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Recommendations. for Care of Adults with Epilepsy. Seeking the best treatment from the right doctor at the right time!
 Recommendations for Care of Adults with Epilepsy Seeking the best treatment from the right doctor at the right time! Contents This booklet is to help adults and their caregivers know when it is appropriate
Recommendations for Care of Adults with Epilepsy Seeking the best treatment from the right doctor at the right time! Contents This booklet is to help adults and their caregivers know when it is appropriate
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Epilepsy Pictures Slideshow: Symptoms, Causes and Treatment.
 Epilepsy Pictures Slideshow: Symptoms, Causes and Treatment. Reviewed by Louise Chang, MD on Friday, August 12, 2011 What Is Epilepsy? Epilepsy is a disorder of the brain's electrical system. Abnormal
Epilepsy Pictures Slideshow: Symptoms, Causes and Treatment. Reviewed by Louise Chang, MD on Friday, August 12, 2011 What Is Epilepsy? Epilepsy is a disorder of the brain's electrical system. Abnormal
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders
 C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
MAPS Study MP-10 1 Study Synopsis UK April 18, 2011
 MAPS Study MP-10 1 Study Synopsis A Randomized, Triple-Blind, Phase 2 Pilot Study with an Open-Label Lead-in Comparing 3 Different Doses of MDMA in Conjunction with Manualized Psychotherapy in 20 Subjects
MAPS Study MP-10 1 Study Synopsis A Randomized, Triple-Blind, Phase 2 Pilot Study with an Open-Label Lead-in Comparing 3 Different Doses of MDMA in Conjunction with Manualized Psychotherapy in 20 Subjects
Product Catalog. Pediatric Learning Solutions. Listing of all current products (as of May, 2013) offered by Children's Hospital Association.
 offered by Children's Hospital Association.") Product Catalog Pediatric Learning Solutions Listing of all current products (as of May, 2013) offered by Children's Hospital Association. Acquired Heart Disease in Children WBT Acute Respiratory Distress
Product Catalog Pediatric Learning Solutions Listing of all current products (as of May, 2013) offered by Children's Hospital Association. Acquired Heart Disease in Children WBT Acute Respiratory Distress
Lecture 8 Cardiovascular Health Lecture 8 1. Introduction 2. Cardiovascular Health 3. Stroke 4. Contributing Factors
 Lecture 8 Cardiovascular Health 1 Lecture 8 1. Introduction 2. Cardiovascular Health 3. Stroke 4. Contributing Factors 1 Human Health: What s Killing Us? Health in America Health is the U.S Average life
Lecture 8 Cardiovascular Health 1 Lecture 8 1. Introduction 2. Cardiovascular Health 3. Stroke 4. Contributing Factors 1 Human Health: What s Killing Us? Health in America Health is the U.S Average life
Alpha-Stim 6/19/2018. Objectives. Cranial Electrotherapy Stimulation 3, 6 History
 Alpha-Stim Tamra Standage, DPT, COMT Objectives Participants should be able to state underlining principles behind the usage of microcurrent therapy, both with probe application and with cranial electrotherapy
Alpha-Stim Tamra Standage, DPT, COMT Objectives Participants should be able to state underlining principles behind the usage of microcurrent therapy, both with probe application and with cranial electrotherapy
Appendix e-1. University HealthSystem Consortium (UHC) database description
 database description") Appendix e-1. University HealthSystem Consortium (UHC) database description UHC is an alliance of academic medical centers and their affiliated hospitals. Member institutions have the goal of sharing clinical,
Appendix e-1. University HealthSystem Consortium (UHC) database description UHC is an alliance of academic medical centers and their affiliated hospitals. Member institutions have the goal of sharing clinical,
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
TMS: Full Board or Expedited?
 TMS: Full Board or Expedited? Transcranial Magnetic Stimulation: - Neurostimulation or neuromodulation technique based on the principle of electro-magnetic induction of an electric field in the brain.
TMS: Full Board or Expedited? Transcranial Magnetic Stimulation: - Neurostimulation or neuromodulation technique based on the principle of electro-magnetic induction of an electric field in the brain.
ATTENDING PHYSICIAN'S STATEMENT STROKE / BRAIN ANEURYSM SURGERY OR CEREBRAL SHUNT INSERTION / CAROTID ARTERY SURGERY
 ATTENDING PHYSICIAN'S STATEMENT STROKE / BRAIN ANEURYSM SURGERY OR CEREBRAL SHUNT INSERTION / CAROTID ARTERY SURGERY A) Patient s Particulars Name of Patient Gender NRIC/FIN or Passport No. Date of Birth
ATTENDING PHYSICIAN'S STATEMENT STROKE / BRAIN ANEURYSM SURGERY OR CEREBRAL SHUNT INSERTION / CAROTID ARTERY SURGERY A) Patient s Particulars Name of Patient Gender NRIC/FIN or Passport No. Date of Birth
Unit #3: Dry Lab A. David A. Morton, Ph.D.
 Unit #3: Dry Lab A David A. Morton, Ph.D. Skull Intracranial Hemorrhage Pg. 26 Epidural Hematoma Pg. 26 Skull Pg. 26 Subdural Hematoma Pg. 26 Subdural Hematoma Pg. 26 Subarachnoid Hemorrhage Pg. 26 Subarachnoid
Unit #3: Dry Lab A David A. Morton, Ph.D. Skull Intracranial Hemorrhage Pg. 26 Epidural Hematoma Pg. 26 Skull Pg. 26 Subdural Hematoma Pg. 26 Subdural Hematoma Pg. 26 Subarachnoid Hemorrhage Pg. 26 Subarachnoid
FORM ID. Patient's Personal Details. SECTION A : Medical Record of the Patient. Name. Policy Number. NRIC/Old IC/Passport/Birth Cert/Others
 CRITICAL ILLNESS CLAIM - DOCTOR'S STATEMENT Brain and Nerve Related Conditions Note: This form is to be completed at the Patient s expense by the Attending Physician/ Surgeon who treated the patient. Patient's
CRITICAL ILLNESS CLAIM - DOCTOR'S STATEMENT Brain and Nerve Related Conditions Note: This form is to be completed at the Patient s expense by the Attending Physician/ Surgeon who treated the patient. Patient's
InterQual Level of Care 2018 Index
 InterQual Level of Care 2018 Index Rehabilitation Criteria Index Words by Subset The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where
InterQual Level of Care 2018 Index Rehabilitation Criteria Index Words by Subset The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
History of Present Condition
 Name: Date: Address: City: Province: Postal Code: Home Phone: Cell Phone: Work Phone: Email: Marital Status: Name Of Family Physician (MD): Age: Occupation: Employer: Extended Health Care Company: Policy
Name: Date: Address: City: Province: Postal Code: Home Phone: Cell Phone: Work Phone: Email: Marital Status: Name Of Family Physician (MD): Age: Occupation: Employer: Extended Health Care Company: Policy
Spring Semester OST 571 Neuromusculoskeletal Lecture-Lab Schedule Revised
 Revised 1-07-16 Week 1: Monday, January 11, 2016 9:00-9:50 a.m. 001 - Principles of Neurobiology/Orientation Lovell Online 10:00-10:50 a.m. 002 - Cells, synapses & neurotransmitter systems Nazaroff Online
Revised 1-07-16 Week 1: Monday, January 11, 2016 9:00-9:50 a.m. 001 - Principles of Neurobiology/Orientation Lovell Online 10:00-10:50 a.m. 002 - Cells, synapses & neurotransmitter systems Nazaroff Online
ARRHYTHMIAS AND DEVICE THERAPY
 Topic List A BASICS 1 History of Cardiology 2 Clinical Skills 2.1 History Taking 2.2 Physical Examination 2.3 Electrocardiography 2.99 Clinical Skills - Other B IMAGING 3 Imaging 3.1 Echocardiography 3.2
Topic List A BASICS 1 History of Cardiology 2 Clinical Skills 2.1 History Taking 2.2 Physical Examination 2.3 Electrocardiography 2.99 Clinical Skills - Other B IMAGING 3 Imaging 3.1 Echocardiography 3.2
FORENSIC SCIENCE NEWSLETTER Forensic Pathology and Neuropathology. William A. Cox, M.D., FCAP.
 NEUROPATHOLOGY FORENSIC SCIENCE NEWSLETTER Forensic Pathology and Neuropathology William A. Cox, M.D., FCAP www.forensicjournals.cm May 15, 2016 This issue of the Forensic Science Newsletter will address
NEUROPATHOLOGY FORENSIC SCIENCE NEWSLETTER Forensic Pathology and Neuropathology William A. Cox, M.D., FCAP www.forensicjournals.cm May 15, 2016 This issue of the Forensic Science Newsletter will address
Patient Name: Date of Birth:
 Patient Name: Date of Birth: Marital Status: Single Married Divorced Widowed Height: Referring Doctor: Weight: Primary Care Dr.: Preferred Pharmacy:(name/address) ALLERGIES: Do you have any drug allergies?
Patient Name: Date of Birth: Marital Status: Single Married Divorced Widowed Height: Referring Doctor: Weight: Primary Care Dr.: Preferred Pharmacy:(name/address) ALLERGIES: Do you have any drug allergies?
Enrolled Copy H.B. 204
 1 PROTECTION OF ATHLETES WITH HEAD INJURIES 2 2011 GENERAL SESSION 3 STATE OF UTAH 4 Chief Sponsor: Paul Ray 5 Senate Sponsor: John L. Valentine 6 7 LONG TITLE 8 General Description: 9 This bill enacts
1 PROTECTION OF ATHLETES WITH HEAD INJURIES 2 2011 GENERAL SESSION 3 STATE OF UTAH 4 Chief Sponsor: Paul Ray 5 Senate Sponsor: John L. Valentine 6 7 LONG TITLE 8 General Description: 9 This bill enacts
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
MRI Patient Screening and History
 Griffin Imaging, LLC Fax:: (770) 229-4632 Specializing In Open MRI, CT & Ultrasound MRI Patient Screening and History Patient Information Sheet PATIENT NAME: AGE: WEIGHT: SEX: MALE FEMALE REFERRED BY DOCTOR:
Griffin Imaging, LLC Fax:: (770) 229-4632 Specializing In Open MRI, CT & Ultrasound MRI Patient Screening and History Patient Information Sheet PATIENT NAME: AGE: WEIGHT: SEX: MALE FEMALE REFERRED BY DOCTOR:
PA SYLLABUS. Syllabus for students of the FACULTY OF MEDICINE No.2
 Approved At the meeting of the Faculty Council Medicine No. of Approved At the meeting of the chair of Neurosurgery No. of Dean of the Faculty Medicine No.2 PhD, associate professor M. Betiu Head of the
Approved At the meeting of the Faculty Council Medicine No. of Approved At the meeting of the chair of Neurosurgery No. of Dean of the Faculty Medicine No.2 PhD, associate professor M. Betiu Head of the
Spring Semester OST 571 Neuromusculoskeletal Lecture-Lab Schedule
 Week 1: Monday, January 5, 2015 9:00-9:50 a.m. 001 - Principles of Neurobiology Lovell Online 10:00-10:50 a.m. 002 - Cells, synapses & neurotransmitters Nazaroff Online 11:00-11:50 a.m. 003 - Development
Week 1: Monday, January 5, 2015 9:00-9:50 a.m. 001 - Principles of Neurobiology Lovell Online 10:00-10:50 a.m. 002 - Cells, synapses & neurotransmitters Nazaroff Online 11:00-11:50 a.m. 003 - Development
Central nervous system
 Central nervous system By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 7 th Lecture Lecture outline Review of structure & function. Symptoms, signs & tests. Specific diseases. Review of structure
Central nervous system By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 7 th Lecture Lecture outline Review of structure & function. Symptoms, signs & tests. Specific diseases. Review of structure
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACTIVASE (t-pa) INFUSION PROTOCOL FOR ACUTE MYOCARDIAL INFARCTION
 INFUSION PROTOCOL FOR ACUTE MYOCARDIAL INFARCTION") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACTIVASE (t-pa) FOR ACUTE MYOCARDIAL INFARCTION I. PURPOSE: A. To reduce the extent of myocardial infarction by lysing the clot in
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACTIVASE (t-pa) FOR ACUTE MYOCARDIAL INFARCTION I. PURPOSE: A. To reduce the extent of myocardial infarction by lysing the clot in
Faculty Disclosure. Sanjay P. Singh, MD, FAAN. Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion
 Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
: STROKE. other pertinent information such as recent trauma, illicit drug use, pertinent medical history or use of oral contraceptives.
 INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
Understanding. Epilepsy. Berit, diagnosed in 2005, with her mother, Jenine.
 Understanding Epilepsy Berit, diagnosed in 2005, with her mother, Jenine. What Are Seizures and Epilepsy? Epilepsy is a medical condition where a person has recurring unprovoked seizures. Having a single
Understanding Epilepsy Berit, diagnosed in 2005, with her mother, Jenine. What Are Seizures and Epilepsy? Epilepsy is a medical condition where a person has recurring unprovoked seizures. Having a single
SYNCOPE. Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope
 SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
See Policy CPT/HCPCS CODE section below for any prior authorization requirements
 Effective Date: 1/1/2019 Section: SUR Policy No: 395 1/1/19 Medical Policy Committee Approved Date: 8/17; 2/18; 12/18 Medical Officer Date APPLIES TO: Medicare Only See Policy CPT/HCPCS CODE section below
Effective Date: 1/1/2019 Section: SUR Policy No: 395 1/1/19 Medical Policy Committee Approved Date: 8/17; 2/18; 12/18 Medical Officer Date APPLIES TO: Medicare Only See Policy CPT/HCPCS CODE section below
Mini Research Paper: Traumatic Brain Injury. Allison M McGee. Salt Lake Community College
 Running Head: Mini Research Paper: Traumatic Brain Injury Mini Research Paper: Traumatic Brain Injury Allison M McGee Salt Lake Community College Abstract A Traumatic Brain Injury (also known as a TBI)
Running Head: Mini Research Paper: Traumatic Brain Injury Mini Research Paper: Traumatic Brain Injury Allison M McGee Salt Lake Community College Abstract A Traumatic Brain Injury (also known as a TBI)
ADVANCED SPINE HEALTH AND WELLNESS CENTER DR. PAUL BACON
 ADVANCED SPINE HEALTH AND WELLNESS CENTER DR. PAUL BACON Patient Name: Address: City: State: Zip Code: H. Phone: W. Phone: Cell Phone: Email Address: Sex M F Marital Status M S D W Date of Birth Age Social
ADVANCED SPINE HEALTH AND WELLNESS CENTER DR. PAUL BACON Patient Name: Address: City: State: Zip Code: H. Phone: W. Phone: Cell Phone: Email Address: Sex M F Marital Status M S D W Date of Birth Age Social
HYPERBARIC OXYGEN BRAIN INJURY TREATMENT TRIAL: A MULTICENTER PHASE II ADAPTIVE CLINICAL TRIAL
 HYPERBARIC OXYGEN BRAIN INJURY TREATMENT TRIAL: A MULTICENTER PHASE II ADAPTIVE CLINICAL TRIAL Gaylan Rockswold, MD, PhD, Principal Investigator William Barsan, MD, Principal Investigator, CCC, SIREN Byron
HYPERBARIC OXYGEN BRAIN INJURY TREATMENT TRIAL: A MULTICENTER PHASE II ADAPTIVE CLINICAL TRIAL Gaylan Rockswold, MD, PhD, Principal Investigator William Barsan, MD, Principal Investigator, CCC, SIREN Byron
EKG Abnormalities. Adapted from:
 EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
Centers for Disease Control and Prevention Guideline on the Diagnosis and Management of Mild Traumatic Brain Injury Among Children September 2018
 Centers for Disease Control and Prevention Guideline on the Diagnosis and Management of Mild Traumatic Brain Injury Among Children September 2018 Nothing to Disclose CDC Guidelines- Objective Question-
Centers for Disease Control and Prevention Guideline on the Diagnosis and Management of Mild Traumatic Brain Injury Among Children September 2018 Nothing to Disclose CDC Guidelines- Objective Question-
UWSP Medical History Form
 UWSP Medical History Form 2017-2018 Student: Please complete the first 6 pages prior to your appointment with your medical provider. The medical provider must sign off on the medical history form. Student
UWSP Medical History Form 2017-2018 Student: Please complete the first 6 pages prior to your appointment with your medical provider. The medical provider must sign off on the medical history form. Student
Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS
 STROKE Name: PID: DOB: Consultant: Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS November 2010 TIME IS BRAIN SUSPECTED STROKE Onset Within 6 Hours? (FAST TEST
STROKE Name: PID: DOB: Consultant: Heart of England Foundation Trust ACUTE STROKE PATHWAY EMERGENCY DEPARTMENT ATTACHMENTS November 2010 TIME IS BRAIN SUSPECTED STROKE Onset Within 6 Hours? (FAST TEST
Syncope. Charles DeBerardinis, DO Iredell Health Systems
 Syncope Charles DeBerardinis, DO Iredell Health Systems Syncope Syncope loss of consciousness Vertigo sensation of motion Drop attacks fall without loss of consciousness seizure Syncope Constatino n=670
Syncope Charles DeBerardinis, DO Iredell Health Systems Syncope Syncope loss of consciousness Vertigo sensation of motion Drop attacks fall without loss of consciousness seizure Syncope Constatino n=670
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
2015 Preliminary Agenda
 2015 Preliminary Agenda Revised 10/08/15 THURSDAY, NOVEMBER 12, 2015 PRE-COURSE WORKSHOP LEARNING OBJECTIVES: At the conclusion of this activity, participants will be better able to: 1. Identify subtle
2015 Preliminary Agenda Revised 10/08/15 THURSDAY, NOVEMBER 12, 2015 PRE-COURSE WORKSHOP LEARNING OBJECTIVES: At the conclusion of this activity, participants will be better able to: 1. Identify subtle
DVLA Medical Questionnaire
 DVLA Medical Questionnaire Your Name: DOB: Today s Date: 2016 - www.countryhealth.co.uk Contents Introduction Key Client Information Important notes Vision assessment Health questionnaire Nervous system
DVLA Medical Questionnaire Your Name: DOB: Today s Date: 2016 - www.countryhealth.co.uk Contents Introduction Key Client Information Important notes Vision assessment Health questionnaire Nervous system
A DAYS CARDIOVASCULAR UNIT GUIDE DUE WEDNESDAY 4/12
 A DAYS CARDIOVASCULAR UNIT GUIDE DUE WEDNESDAY 4/12 MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY 3/20 - B 3/21 - A 3/22 - B 3/23 - A 3/24 - B 3/27 - A Dissection Ethics Debate 3/28 - B 3/29 - A Intro to Cardiovascular
A DAYS CARDIOVASCULAR UNIT GUIDE DUE WEDNESDAY 4/12 MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY 3/20 - B 3/21 - A 3/22 - B 3/23 - A 3/24 - B 3/27 - A Dissection Ethics Debate 3/28 - B 3/29 - A Intro to Cardiovascular
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES
 PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES INTRODUCTION: Traumatic Brain Injury (TBI) is an important clinical entity in acute care surgery without well-defined guidelines
PROPOSAL FOR MULTI-INSTITUTIONAL IMPLEMENTATION OF THE BRAIN INJURY GUIDELINES INTRODUCTION: Traumatic Brain Injury (TBI) is an important clinical entity in acute care surgery without well-defined guidelines
Cerebrovascular accident icd 10
 Cerebrovascular accident icd 10 I69.21 is a billable ICD code used to specify a diagnosis of cognitive deficits following other nontraumatic intracranial hemorrhage. A 'billable code' is detailed. Conventions.
Cerebrovascular accident icd 10 I69.21 is a billable ICD code used to specify a diagnosis of cognitive deficits following other nontraumatic intracranial hemorrhage. A 'billable code' is detailed. Conventions.
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Review Evaluation of Residuals of Traumatic Brain Injury (R-TBI) Disability Benefits Questionnaire * Internal VA or DoD Use Only*
 Disability Benefits Questionnaire * Internal VA or DoD Use Only*") Review Evaluation of Residuals of Traumatic Brain Injury (R-TBI) Disability Benefits Questionnaire * Internal VA or DoD Use Only* Name of patient/veteran: SSN: Your patient is applying to the U. S. Department
Review Evaluation of Residuals of Traumatic Brain Injury (R-TBI) Disability Benefits Questionnaire * Internal VA or DoD Use Only* Name of patient/veteran: SSN: Your patient is applying to the U. S. Department
The determination of eligible population for this measure requires administrative claims data.
 Overuse of Imaging Measure 6: Ratio of Magnetic Resonance Imaging Scans to Computed Tomography Scans for the Evaluation of Children with Atraumatic Headache Description This measure assesses the ratio
Overuse of Imaging Measure 6: Ratio of Magnetic Resonance Imaging Scans to Computed Tomography Scans for the Evaluation of Children with Atraumatic Headache Description This measure assesses the ratio
MEDICAL POLICY No R9 DETOXIFICATION I. POLICY/CRITERIA
 DETOXIFICATION MEDICAL POLICY Effective Date: January 1, 2018 Review Dates: 1/93, 2/97, 4/99, 2/01, 12/01, 2/02, 2/03, 1/04, 1/05, 12/05, 12/06, 12/07, 12/08, 12/09, 12/10, 12/11, 12/12, 12/13, 11/14,
DETOXIFICATION MEDICAL POLICY Effective Date: January 1, 2018 Review Dates: 1/93, 2/97, 4/99, 2/01, 12/01, 2/02, 2/03, 1/04, 1/05, 12/05, 12/06, 12/07, 12/08, 12/09, 12/10, 12/11, 12/12, 12/13, 11/14,
Quality Measures MIPS CV Specific
 Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Neuromodulation in Dravet Syndrome. Eric BJ Segal, MD Director of Pediatric Epilepsy Northeast Regional Epilepsy Group Hackensack, New Jersey
 Neuromodulation in Dravet Syndrome Eric BJ Segal, MD Director of Pediatric Epilepsy Northeast Regional Epilepsy Group Hackensack, New Jersey What is neuromodulation? Seizures are caused by synchronized
Neuromodulation in Dravet Syndrome Eric BJ Segal, MD Director of Pediatric Epilepsy Northeast Regional Epilepsy Group Hackensack, New Jersey What is neuromodulation? Seizures are caused by synchronized
10/8/2018. Lecture 9. Cardiovascular Health. Lecture Heart 2. Cardiovascular Health 3. Stroke 4. Contributing Factor
 Lecture 9 Cardiovascular Health 1 Lecture 9 1. Heart 2. Cardiovascular Health 3. Stroke 4. Contributing Factor 1 The Heart Muscular Pump The Heart Receives blood low pressure then increases the pressure
Lecture 9 Cardiovascular Health 1 Lecture 9 1. Heart 2. Cardiovascular Health 3. Stroke 4. Contributing Factor 1 The Heart Muscular Pump The Heart Receives blood low pressure then increases the pressure
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Patient Resources: Arrhythmias and Congenital Heart Disease
 Patient Resources: Arrhythmias and Congenital Heart Disease Overview Arrhythmias (abnormal heart rhythms) can develop in patients with congenital heart disease (CHD) due to thickening/weakening of their
Patient Resources: Arrhythmias and Congenital Heart Disease Overview Arrhythmias (abnormal heart rhythms) can develop in patients with congenital heart disease (CHD) due to thickening/weakening of their
New Patient Questionnaire
 New Patient Questionnaire Name: Primary Care Physician: Date of Birth: / / Home Phone: ( ) Cell Phone: ( ) Why are you seeing a cardiologist? (please answer in detail) Have you ever seen a cardiologist
New Patient Questionnaire Name: Primary Care Physician: Date of Birth: / / Home Phone: ( ) Cell Phone: ( ) Why are you seeing a cardiologist? (please answer in detail) Have you ever seen a cardiologist
Spine Center. at Stamford Hospital s Orthopedic Institute
 Spine Center at Stamford Hospital s Orthopedic Institute Back pain related to spinal deformity and injury or congenital conditions is a common health complaint, which can be very debilitating. At Stamford
Spine Center at Stamford Hospital s Orthopedic Institute Back pain related to spinal deformity and injury or congenital conditions is a common health complaint, which can be very debilitating. At Stamford
Syncope Guidelines: What s New?
 Syncope Guidelines: What s New? Dr. Samuel Asirvatham Professor of Medicine and Pediatrics Mayo Clinic College of Medicine Medical Director, Electrophysiology Laboratory Program Director, EP Fellowship
Syncope Guidelines: What s New? Dr. Samuel Asirvatham Professor of Medicine and Pediatrics Mayo Clinic College of Medicine Medical Director, Electrophysiology Laboratory Program Director, EP Fellowship
Initial Pain Management Patient Questionnaire
 Appt. Date: Appt. Time: Boston Out-Patient Surgical Suites North Tel Fax: 781-407-5892 Initial Pain Management Patient Questionnaire Dear New Pain Management Patient, Welcome to the New England Pain Management
Appt. Date: Appt. Time: Boston Out-Patient Surgical Suites North Tel Fax: 781-407-5892 Initial Pain Management Patient Questionnaire Dear New Pain Management Patient, Welcome to the New England Pain Management
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Brain Injury and Epilepsy
 Slide 1 Brain Injury and Epilepsy Presented by: Paula St. John, MA Education and Community Outreach Manager Minnesota Brain injury Alliance www.braininjurymn.org l 612-378-2742 800-669-6442 Slide 2 Objectives:
Slide 1 Brain Injury and Epilepsy Presented by: Paula St. John, MA Education and Community Outreach Manager Minnesota Brain injury Alliance www.braininjurymn.org l 612-378-2742 800-669-6442 Slide 2 Objectives:
Appendix Criteria used for the automated chart review
 Appendix Criteria used for the automated chart review A. Heart attack i. 410.01 (Acute myocardial infarction of anterolateral wall initial episode of ii. 410.11 (Acute myocardial infarction of other anterior
Appendix Criteria used for the automated chart review A. Heart attack i. 410.01 (Acute myocardial infarction of anterolateral wall initial episode of ii. 410.11 (Acute myocardial infarction of other anterior
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function
 Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function") 1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
PEDIATRIC MILD TRAUMATIC HEAD INJURY
 PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
PEDIATRIC MILD TRAUMATIC HEAD INJURY October 2011 Quality Improvement Resources Illinois Emergency Medical Services for Children is a collaborative program between the Illinois Department of Public Health
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
THN. Sleep Therapy Study. ImThera. Information for Participants. Caution: Investigational device. Limited by United States law to investigational use.
 THN Sleep Therapy Study Information for Participants Caution: Investigational device. Limited by United States law to investigational use. ImThera Obstructive sleep apnea (OSA) is a very serious condition.
THN Sleep Therapy Study Information for Participants Caution: Investigational device. Limited by United States law to investigational use. ImThera Obstructive sleep apnea (OSA) is a very serious condition.
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS)
 Stroke (2 of 2) Seizures Altered Mental Status (AMS)") 1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Assessment and Scoring Tools
 Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System EMS System Policy Change Coversheet EMS SYSTEM POLICY CHANGE COVERSHEET Policy Number and Name: 605: Prehospital Trauma Triage Date: May 27, 2014
County of Santa Clara Emergency Medical Services System EMS System Policy Change Coversheet EMS SYSTEM POLICY CHANGE COVERSHEET Policy Number and Name: 605: Prehospital Trauma Triage Date: May 27, 2014