A Review of Differentiated Thyroid Cancer
|
|
|
- Isabella Hoover
- 6 years ago
- Views:
Transcription


1 A Review of Differentiated Thyroid Cancer April 21 st, 2016 FPON Webcast Jonn Wu BMSc MD FRCPC Radiation Oncologist, Vancouver Centre Chair, Provincial H&N Tumour Group, BCCA Clinical Associate Professor, UBC

2 Disclosure(s) Genzyme/Sanofi Advisory Board, Research Grant
3 Objectives By the end of this session, participants will be able to describe: 1. the excellent prognosis for most patients diagnosed with well differentiated thyroid carcinomas; 2. the general management of well differentiated thyroid carcinomas; and 3. management of thyroxine (Synthroid) for replacement and TSH suppressive purposes.
4 Outline Introduction, Epidemiology Diagnosis, Surgical Management Staging and Risk Assessment Radioiodine Remnant Ablation and Therapy Thyrotropin Suppression Therapy Surveillance Future Directions, Clinical Trials
5 Outline Introduction, Epidemiology Diagnosis, Surgical Management Staging and Risk Assessment Radioiodine Remnant Ablation and Therapy Thyrotropin Suppression Therapy Surveillance Future Directions, Clinical Trials

6 Scope of the Problem Relatively uncommon (1%) 50,000 cases in US 230,000 breast 230,000 lung 75% are Females Incidence tripled: 1975: 4.9 / 100, : 14.3 / 100,000 Increasing 10% per year More micro-carcinomas (< 1.0 cm) 1988: 25% 2008: 39%


7 Scope of the Problem Canada: Incidence: Approximately 6,300 in 2015 Deaths: 185 deaths in 2010 BC (2007): New cases: 68 men, 211 women Deaths: 5 men and 9 women Most deaths in patients over 60 yrs

8 Scope of the Problem

9 Scope of the Problem


 4% Medullary")
10 Carcinoma of the Thyroid 90% differentiated tumours arising from follicular epithelial cells 80% papillary +/- follicular elements 10% pure follicular (incl Hurthle cell) 4% Medullary 5% Anaplastic

11 Carcinoma of the Thyroid Papillary ca 98% Follicular ca 94% Medullary ca 80% Anaplastic ca 10% Relative rarity and high survival mean that there are very few prospective randomised trials so most management is based on retrospective data

12 Risk Factors Majority are sporadic Iodine deficiency Radiation exposure Family history Rare familial disorders: Gardner s syndrome, Cowden s disease, familial polyposis, MEN2, Werner Syndrome
13 Outline Introduction, Epidemiology Diagnosis, Surgical Management Staging and Risk Assessment Radioiodine Remnant Ablation and Therapy Thyrotropin Suppression Therapy Surveillance Future Directions, Clinical Trials


14 Clinical Presentation Palpable thyroid mass Palpable cervical lymphadenopathy Incidental finding on cross sectional imaging or ultrasound
 ** Iodine")


 found > 50% of individuals")
15 Thyroid Nodule ** Ultrasound + Fine Needle Aspiration (FNA) ** Iodine Scan: only if thyrotoxic 15% inadequate repeat Adequate specimen false +ve & -ve rates of 5% Ultrasound more sensitive than CT but operator dependent Incidental nodules (<1cm) found > 50% of individuals These are rarely malignant
:109-42.")
16 Surgical Management Surgery Primary Treatment Adjuvant Radiation Radioiodine (131-Iodine) External Beam Radiation Thyroxine ** No Prospective Randomized Trials ** Cooper et al, Thyroid Feb;16(2):
 Total thyroidectomy, Central Neck Dissection 2. Lobectomy + isthmusectomy 3.")
17 Surgical Management Primary therapy for thyroid cancer 1. (near) Total thyroidectomy, Central Neck Dissection 2. Lobectomy + isthmusectomy 3. And/Or Neck dissection Cooper et al, Thyroid Feb;16(2):
18 Surgical Management Near total thyroidectomy, because >60% have foci in contralateral lobe 5-10% of recurrences are in contralateral lobe 131 Iodine is more effective if less residual thyroid Serum thyroglobulin is a more specific marker Recurrence rate is lower than after lobectomy

19 Surgical Management Near total thyroidectomy! BUT: No substantial survival benefit Higher risk of hypoparathyroidism Higher risk to recurrent laryngeal nerves Lobectomy is reasonable in low risk patients Completion thyroidectomy if high risk features are found from pathological assessment




20 Surgical Management Neck Dissection Lateral and Central Nodal recurrence lower if central neck dissection done at time of thyroidectomy 35% gross involvement, 80% microscopic +LN doesn t reduce survival rates +LN increases risk of recurrence

21 Surgical Management Post-operative Thyroxine T4 (levothyroxine) Begin with mcg Average therapeutic dose is mcg 4-6 weeks to clear
22 Outline Introduction, Epidemiology Diagnosis, Surgical Management Staging and Risk Assessment Radioiodine Remnant Ablation and Therapy Thyrotropin Suppression Therapy Surveillance Future Directions, Clinical Trials
23 Staging, Risk Assessment Risk of Recurrence ATA Risk Stratification Risk of Death TNM, AJCC AMES, AGES MACIS

24 Staging, Risk Assessment Risk of Recurrence ATA Risk Stratification
25 Staging, Risk Assessment Risk of Recurrence ATA Risk Stratification Recurrence Vs Survival?



26 Staging, Risk Assessment AJCC/TNM Papillary carcinoma Follicular carcinoma SEER
27 Staging, Risk Assessment AGES Age: >45 years of age Grade: problematic Extrathyroidal (soft tissue) extension Size: 2cm (6%) vs 7cm (50%) mortality AMES Age Metastasis Extrathyroidal extension Size Hay et al, Surgery 1987 Dec;102(6): < 40 yrs Metastases <1cm < 40 yrs Metastases >1cm > 40 yrs Metastases <1cm > 40 yrs Metastases >1cm Baudin and Schlumberger, Lancet Oncology, 2007 Brierley et al Clin Endocrinology 2005
28 Staging, Risk Assessment MACIS 3.1 (<40yo) or 0.08 x age (if 40 or more years old) 0.3 x tumor size (in cm) +1 if incompletely resected +1 if locally invasive +3 if distant metastases MACIS 20yr Disease Specific Mortality <6.0 = 1% = 11% = 44% >8 = 76% Hay et al, Surgery 1993 Dec;114(6):1050-7; discussion
29 Outline Introduction, Epidemiology Diagnosis, Surgical Management Staging and Risk Assessment Radioiodine Remnant Ablation and Therapy Thyrotropin Suppression Therapy Surveillance Future Directions, Clinical Trials
30 Adjuvant Therapy Radioiodine (131-I) Ablation of remnant Therapy of disease External beam radiotherapy Thyroxine Chemotherapy, targeted agents
31 Adjuvant Therapy Radioiodine (131-I) microscopic disease Ablation of remnant Therapy of disease External beam RT macroscopic disease Thyroxine Chemotherapy, targeted agents
32 Adjuvant Therapy Radioiodine (131-I) microscopic disease Ablation of remnant Therapy of disease External beam RT macroscopic disease Thyroxine Chemotherapy, targeted agents
, some gamma Concentrated by thyroid follicular cells Cancer cells less iodine-avid than normal cells")
33 Adjuvant Therapy Radioiodine (131-I) what is it? Primarily short-range beta (1-2mm), some gamma Concentrated by thyroid follicular cells Cancer cells less iodine-avid than normal cells Remove as much normal thyroid as possible (total thyroidectomy) Improve uptake stimulate with TSH
34 Adjuvant Therapy Radioiodine (131-I) why ablation? Improve value of serum thyroglobulin measurements. Increase specificity of US and 131-I scanning. Treat microscopic disease. Low dose: 30 mci Radioiodine (131-I) why therapy? Destroy residual malignant cells Adjuvant treatment of high risk patients Treatment of established metastases Higher dose: 150 to 200 mci
:741-60.")
35 Adjuvant Therapy Radioiodine (131-I) who should be treated? No randomized data 131-I reduces risk of recurrence Evidence of survival benefit Wong et al, Endocrinol Metab Clin North Am 1990 Sep;19(3): DeGroot et al, J Clin Endocrinol Metab 1990 Aug;71(2): Mazzaferri et al, Am J Med 1994 Nov;97(5): Hay et al, World J Surg 2002 Aug;26(8): Epub 2002 May 21.
36 Adjuvant Therapy Radioiodine (131-I) who should be treated? No randomized data 131-I reduces risk of recurrence?? Evidence of survival benefit?? Hay 2002 (Mayo Clinic) no difference! vs (131-I) Wong et al, Endocrinol Metab Clin North Am 1990 Sep;19(3): DeGroot et al, J Clin Endocrinol Metab 1990 Aug;71(2): Mazzaferri et al, Am J Med 1994 Nov;97(5): Hay et al, World J Surg 2002 Aug;26(8): Epub 2002 May 21.

 Treat less! (Hay et al) BCCA: MACIS score > 6.")

37 Adjuvant Therapy Radioiodine (131-I) who should be treated? No randomized data 131-I reduces risk of recurrence?? Evidence of survival benefit?? Two schools of thought Treat more! (Mazzaferri et al) Treat less! (Hay et al) BCCA: MACIS score > 6.0 = Treat MACIS score 5.0 to 6.0 = Review at Provincial Thyroid Conference Treating fewer patients Using lower doses for Ablation: 30 mci vs 60 or 100 mci More outpatient therapy
 Two methods: Endogenous TSH ie.")
 rhtsh (thyrotropin alpha) Two retrospective studies:")
: fatigue, insomnia, vomiting, diarrhea, weakness Low")
:1371-7.")
38 Radioiodine (131-I) how do we do it? TSH stimulation (> 30) Two methods: Endogenous TSH ie. Thyroxine withdrawal Exogenous TSH ie. Thyrotropin alpha (rhtsh) rhtsh (thyrotropin alpha) Two retrospective studies: rhtsh = withdrawal Improved quality of life Expensive Side effects Common: Nausea 10%, Headache: 7% Rare (<3%): fatigue, insomnia, vomiting, diarrhea, weakness Low Iodine Diet Adjuvant Therapy Luster, Eur J Nucl Med Mol Imaging 2003 Oct;30(10): Epub 2003 Jul 15 Barbaro, J Clin Endocrinol Metab 2003 Sep;88(9): Robbins, J Nucl Med 2002 Nov;43(11): Schroeder, J Clin Endocrinol Metab Mar;91(3): Epub 2006 Jan 4

 Wednesday: 123-I scan")

39 Adjuvant Therapy Radioiodine (131-I) Protocol Protocol Monday: 0.9mg IM (thyrotropin alpha) Tuesday: 0.9mg IM (thyrotropin alpha) Wednesday: 123-I scan I therapy radioactive Wednesday, Thursday, Friday Inpatient versus Outpatient Monday: Whole body scan Blood tests: TSH, Tg 131-I Rx + Dx
40 Adjuvant Therapy Radioiodine (131-I) Side Effects Discomfort, Fatigue Xerostomia Dysgeusia Sialodenitis Transient hypogonadism (spermatopenia) Myelosuppression (transient versus permanent) Hypothetical risk of aplastic anaemia and leukaemia Doses >1000mCi (usual dose mCi)
41 Adjuvant Therapy Radioiodine (131-I) microscopic disease Ablation of remnant Therapy of disease External beam RT macroscopic disease Thyroxine Chemotherapy, targeted agents
 disease")

42 Adjuvant Therapy External Beam Radiotherapy Gross (macroscopic) disease Unresectable gross disease Gross disease not responding to 131-I 5 to 7 weeks, daily treatment




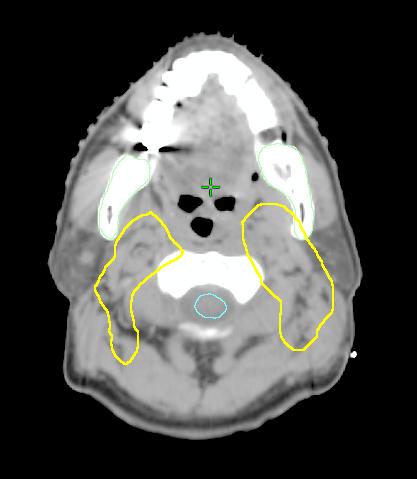
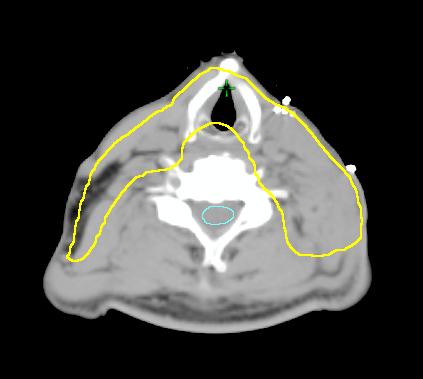

43 Adjuvant Therapy Immobilization Shell CT Planning


44 Adjuvant Therapy External Beam Radiation Sequelae: Xerostomia, altered taste, esophagitis, pharyngitis, laryngitis, fatigue, dry/moist desquamation
45 Adjuvant Therapy Radioiodine (131-I) microscopic disease Ablation of remnant Therapy of disease External beam RT macroscopic disease Thyroxine Chemotherapy, targeted agents

46 Adjuvant Therapy Thyroxine - Rationale: 1. Replacement Therapy FT4 2. Suppressive Therapy TSH Issues: 4-6 weeks to equilibrate Need both: FT4 and TSH FT4: Upper limits of normal TSH: <0.1 to 2.0 mu/l TSH Suppression: How low do you go?

47 Adjuvant Therapy TSH Suppression: How low do you go? Low Risk: 0.5 to 2.0 mu/l Intermediate Risk: 0.1 to 0.5 mu/l High Risk: < 0.1 mu/l BCCA: Generally < 1.0 mu/l, depending on risk category Evidence strongest for High Risk Why not < 0.1 mu/l for everyone? Low TSH = High FT4 Prolonged hyperthyroidism atrial fibrillation cardiac hypertrophy and dysfunction accelerated osteoporosis Balance risk of recurrence vs hyperthyroidism
48 (Adjuvant) Palliative Therapy Radioiodine (131-I) microscopic disease Ablation of remnant Therapy of disease External beam RT macroscopic disease Thyroxine Chemotherapy, targeted agents
49 Outline Introduction, Epidemiology Diagnosis, Surgical Management Staging and Risk Assessment Radioiodine Remnant Ablation and Therapy Thyrotropin Suppression Therapy Surveillance Future Directions, Clinical Trials

50 Surveillance Frequency depends on response: BCCA: TSH-Stimulated Tg < 1 ng/ml Post-131-I scan: Clear
51 Surveillance Blood tests Serum Thyroglobulin (Tg) Excellent tumour marker Produced by thyroid follicular cells (and well differentiated tumours) Most sensitive with TSH stimulation Anti thyroglobulin antibodies Interferes with Tg Iodine avid tumours produce Tg Not all tumours with elevated Tg take up iodine

 4.")


52 Surveillance Clinical exam: q6-12 months Blood tests: q3-12 months - I do all FOUR: 1. FT4 2. TSH 3. Tg (> 98% sensitivity) 4. Anti-Tg-Ab Imaging US Neck: Yes or No? How frequent? 5 mci 131-I Scan NO! (unless the scan is after treatment) Others: CXR, CT Neck, TSH stimulated PET/CT



53 Gross disease: If resectable: Surgery Not resectable: 131-I +/- EBRT If non-iodine-avid: EBRT Rising Tg No gross disease? Empiric dose ( mci) 131-I ** NOT a 5 mci SCAN ** TSH-stimulated PET scan Sx/RT-resistant disease: Chemotherapy: doxorubicin Recurrence Tyrosine Kinase Inhibitors: vandetanib, sorafenib, lenvatinib Sequelae: diarrhea, fatigue, HPT, hepatotoxicity, skin changes, nausea, dysgeusia, anorexia, thrombosis, heart failure,
54 Outline Introduction, Epidemiology Diagnosis, Surgical Management Staging and Risk Assessment Radioiodine Remnant Ablation and Therapy Thyrotropin Suppression Therapy Surveillance Future Directions, Clinical Trials
55 Clinical Trials Future Directions Tyrosine Kinase Inhibitors: OS, QOL Molecular Markers Diagnosis, prognosis, therapeutic targets Improved Risk Stratification Who truly needs 131-I? US? Which LNs to biopsy? Minimally invasive follicular variant of papillary carcinoma in the absence of angio-invasion Improve Surveillance Regimens Tg in the face of Anti-Tg-Antibodies
56 Summary Well Differentiated Thyroid Cancer Relatively uncommon cancer Excellent prognosis Treatment: Surgery +/- Radioactive Iodine Life Long Thyroxine Blood Tests: 1. FreeT4: upper limits of normal 2. TSH: generally < Tg: excellent tumour marker 4. Anti-Tg-antibodies: surrogate marker, interferes with Tg
57
58 Medullary Thyroid Cancer Para-follicular c-cells Calcitonin Does not produce Tg Does not respond to TSH or 131-I Work-Up Serum calcitonin, CEA CT neck/chest MEN Types 2A/2B
59 Medullary Thyroid Cancer Management Surgery Thyroidectomy + central neck dissection Adjuvant External Beam RT Serum calcitonin (?when) Thyroxine (replacement) Metastatic disease TKI: sunitinib, sorafenib (20-50%) Chemo: doxorubicin, etc (10-20%) Survival: < 40 yrs 75% ten year disease specific survival > 40 yrs 50% ten year disease specific survival
60 Anaplastic Thyroid Carcinoma 2-5% of thyroid cancers Disease specific mortality = 100% Most = locally advanced >50% distant diagnosis Management Maximal surgery + external beam RT EBRT + chemotherapy
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer
 Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Thyroid Cancer & rhtsh: When and How?
 Thyroid Cancer & rhtsh: When and How? 8 th Postgraduate Course in Endocrine Surgery Capsis Beach, Crete, September 21, 2006 Quan-Yang Duh, Professor of Surgery, UCSF Increasing Incidence of Thyroid Cancer
Thyroid Cancer & rhtsh: When and How? 8 th Postgraduate Course in Endocrine Surgery Capsis Beach, Crete, September 21, 2006 Quan-Yang Duh, Professor of Surgery, UCSF Increasing Incidence of Thyroid Cancer
I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
3/29/2012. Thyroid cancer- what s new. Thyroid Cancer. Thyroid cancer is now the most rapidly increasing cancer in women
 Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
Reference No: Author(s) Approval date: October committee. September Operational Date: Review:
 Approval date: October committee. September Operational Date: Review:") Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) guidelines for Thyroid cancer Dr Fionnuala Houghton Consultant Clinical Oncologist & Dr Lois Mulholland Consultant Clinical Oncologist
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) guidelines for Thyroid cancer Dr Fionnuala Houghton Consultant Clinical Oncologist & Dr Lois Mulholland Consultant Clinical Oncologist
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Risk Adapted Follow-Up
 Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update
 thyroid carcinoma-an update") Bangladesh J Otorhinolaryngol 2010; 16(2): 126-130 Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update Md. Abdul Mobin Choudhury 1, Md. Abdul Alim Shaikh
Bangladesh J Otorhinolaryngol 2010; 16(2): 126-130 Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update Md. Abdul Mobin Choudhury 1, Md. Abdul Alim Shaikh
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD
 Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Case-Based Discussion of Thyroid Cancer Therapy
 Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans
 131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Radiation Therapy for Thyroid Cancer. When is Radiation Therapy indicated in Thyroid Cancer of Follicular or Parafollicular Cell Origin?
 When is Radiation Therapy indicated in Thyroid Cancer of Follicular or Parafollicular Cell Origin? Jeanne Marie Quivey MD FACR October 200 Radiation Therapy for Thyroid Cancer Radioactive 3- I (RAI) External
When is Radiation Therapy indicated in Thyroid Cancer of Follicular or Parafollicular Cell Origin? Jeanne Marie Quivey MD FACR October 200 Radiation Therapy for Thyroid Cancer Radioactive 3- I (RAI) External
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Anca M. Avram, M.D. Professor of Radiology
 Thyroid Cancer Theranostics: the case for pre-treatment diagnostic staging 131-I scans for 131-I therapy planning Anca M. Avram, M.D. Professor of Radiology Department of Nuclear Medicine University of
Thyroid Cancer Theranostics: the case for pre-treatment diagnostic staging 131-I scans for 131-I therapy planning Anca M. Avram, M.D. Professor of Radiology Department of Nuclear Medicine University of
American College of Radiology ACR Appropriateness Criteria
 American College of Radiology ACR Criteria Thyroid Carcinoma Variant 1: T1a N0 M0 papillary thyroid cancer: 40-year-old woman. 30 mci with thyrotropin 100 mci with thyrotropin 30 mci with thyroid hormone
American College of Radiology ACR Criteria Thyroid Carcinoma Variant 1: T1a N0 M0 papillary thyroid cancer: 40-year-old woman. 30 mci with thyrotropin 100 mci with thyrotropin 30 mci with thyroid hormone
What you need to know about Thyroid Cancer
 What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
A Risk-Adapted Approach to the Use of Radioactive Iodine and External Beam Radiation in the Treatment of Well-Differentiated Thyroid Cancer
 Both radioactive iodine and external beam radiation can play roles in well-differentiated thyroid cancer. Rebecca Kinkead. Hula No. 3 (detail), 2010. Oil on canvas, 45 37. A Risk-Adapted Approach to the
Both radioactive iodine and external beam radiation can play roles in well-differentiated thyroid cancer. Rebecca Kinkead. Hula No. 3 (detail), 2010. Oil on canvas, 45 37. A Risk-Adapted Approach to the
CLINICAL CONSIDERATIONS FOR I-131 THERAPY
 CLINICAL CONSIDERATIONS FOR I-131 THERAPY Oneil Lee, MD, PhD Kaiser Permanente Orange County Department of Radiology/Nuclear Medicine GOAL Understand thyroid cancer: Biology, epidemiology, treatment strategies,
CLINICAL CONSIDERATIONS FOR I-131 THERAPY Oneil Lee, MD, PhD Kaiser Permanente Orange County Department of Radiology/Nuclear Medicine GOAL Understand thyroid cancer: Biology, epidemiology, treatment strategies,
COME HOME Innovative Oncology Business Solutions, Inc.
 COME HOME Thyroid Cancer pathway development worksheet, v9 April 13, 2015 Required Structured Data: Stage Staging Components Staging Date Histology Quality Measure(s): Staging (clinical or pathologic)
COME HOME Thyroid Cancer pathway development worksheet, v9 April 13, 2015 Required Structured Data: Stage Staging Components Staging Date Histology Quality Measure(s): Staging (clinical or pathologic)
The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer
 for Differentiated Thyroid Cancer") The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer Wendy Sacks, M.D. Cedars Sinai Medical Center California Chapter Annual Meeting, AACE Nov 5, 2016 Increasing Incidence of Thyroid Cancer
The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer Wendy Sacks, M.D. Cedars Sinai Medical Center California Chapter Annual Meeting, AACE Nov 5, 2016 Increasing Incidence of Thyroid Cancer
Correspondence should be addressed to Stan H. M. Van Uum;
 Oncology Volume 2016, Article ID 6496750, 6 pages http://dx.doi.org/10.1155/2016/6496750 Research Article Recombinant Human Thyroid Stimulating Hormone versus Thyroid Hormone Withdrawal for Radioactive
Oncology Volume 2016, Article ID 6496750, 6 pages http://dx.doi.org/10.1155/2016/6496750 Research Article Recombinant Human Thyroid Stimulating Hormone versus Thyroid Hormone Withdrawal for Radioactive
Success rate of thyroid remnant ablation for differentiated thyroid cancer based on 5550 MBq post-therapy scan
 ORIGINAL ARTICLE Success rate of thyroid remnant ablation for differentiated thyroid cancer based on 5550 MBq post-therapy scan I. Hommel 1 *, G.F. Pieters 1, A.J.M. Rijnders 2, M.M. van Borren 3, H. de
ORIGINAL ARTICLE Success rate of thyroid remnant ablation for differentiated thyroid cancer based on 5550 MBq post-therapy scan I. Hommel 1 *, G.F. Pieters 1, A.J.M. Rijnders 2, M.M. van Borren 3, H. de
Pediatric Thyroid Cancer Lung Metastases. Liora Lazar MD
 Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
THYROID CANCER IN CHILDREN
 THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
Calcitonin. 1
 Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Thyroid carcinoma. Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec.
 Thyroid carcinoma Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec. Thyroid tumors PRIMARY TUMORS Tumors of the follicular epithelium : - Tumors of the follicular
Thyroid carcinoma Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec. Thyroid tumors PRIMARY TUMORS Tumors of the follicular epithelium : - Tumors of the follicular
Management of Recurrent Thyroid Cancer
 Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Differentiated Thyroid Cancer: Reclassification of the Risk of Recurrence Based on the Response to Initial Treatment
 ORIGINAL ARTICLE Differentiated Thyroid Cancer: Reclassification of the Risk of Recurrence Based on the Response to Initial Treatment Martínez MP, Lozano Bullrich MP, Rey M, Ridruejo MC, Bomarito MJ, Claus
ORIGINAL ARTICLE Differentiated Thyroid Cancer: Reclassification of the Risk of Recurrence Based on the Response to Initial Treatment Martínez MP, Lozano Bullrich MP, Rey M, Ridruejo MC, Bomarito MJ, Claus
Mandana Moosavi 1 and Stuart Kreisman Background
 Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Thyroid and Adrenal Gland
 Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
1. Protocol Summary Summary of Trial Design. IoN
 1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting?
 Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
Thyroid Surgery: Lobectomy, total thyroidectomy, LN biopsies or only watchful waiting? Jacob Moalem, MD, FACS Associate Professor Endocrine Surgery and Endocrinology URMC Agenda 1. When is lobectomy alone
RESEARCH ARTICLE. Importance of Postoperative Stimulated Thyroglobulin Level at the Time of 131 I Ablation Therapy for Differentiated Thyroid Cancer
 RESEARCH ARTICLE Importance of Postoperative Stimulated Thyroglobulin Level at the Time of 131 I Ablation Therapy for Differentiated Thyroid Cancer Zekiye Hasbek 1 *, Bulent Turgut 1, Fatih Kilicli 2,
RESEARCH ARTICLE Importance of Postoperative Stimulated Thyroglobulin Level at the Time of 131 I Ablation Therapy for Differentiated Thyroid Cancer Zekiye Hasbek 1 *, Bulent Turgut 1, Fatih Kilicli 2,
Radioiodine-refractory DTC
 Oncology: Radioiodine-refractory DTC New Developments in Giuseppe COSTANTE, MD, Head, Endocrinology Clinic Institut Jules Bordet Université Libre de Bruxelles (U.L.B.) Targeted Therapies Targeted Treatments
Oncology: Radioiodine-refractory DTC New Developments in Giuseppe COSTANTE, MD, Head, Endocrinology Clinic Institut Jules Bordet Université Libre de Bruxelles (U.L.B.) Targeted Therapies Targeted Treatments
Disclosures Nodal Management in Differentiated Thyroid Carcinoma
 Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
9 year-old Female with Papillary Thyroid Cancer. Katie O Sullivan, M.D. Fellow Medicine/Pediatric Endocrinology Thursday, January 16 th, 2014
 9 year-old Female with Papillary Thyroid Cancer Katie O Sullivan, M.D. Fellow Medicine/Pediatric Endocrinology Thursday, January 16 th, 2014 Chief Complaint Mass on the right side of the neck x 2-3 weeks
9 year-old Female with Papillary Thyroid Cancer Katie O Sullivan, M.D. Fellow Medicine/Pediatric Endocrinology Thursday, January 16 th, 2014 Chief Complaint Mass on the right side of the neck x 2-3 weeks
Current Issues in Thyroid Cancer Surgery in 2017
 Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
10/24/2008. Surgery for Well-differentiated Thyroid Carcinoma- The Primary
 Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience
 Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
(Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE
 New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE") (Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some
(Not so) New Guidelines for Management of Thyroid Nodules and Differentiated Thyroid Cancer Minnesota/Midwest Chapter of AACE Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some
Dr J K Jekel Dept. Surgery University of Pretoria
 Dr J K Jekel Dept. Surgery University of Pretoria No Maybe ( T`s and C`s apply ) 1. Total thyroidectomy 2. Neck dissection only if nodes are involved 3. Ablative dose or doses of Radioactive Iodine 4.
Dr J K Jekel Dept. Surgery University of Pretoria No Maybe ( T`s and C`s apply ) 1. Total thyroidectomy 2. Neck dissection only if nodes are involved 3. Ablative dose or doses of Radioactive Iodine 4.
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Imaging in Thyroid Cancer
 Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
14 Clinical Review Volume 2 No. 1, 2004
 14 Clinical Review Volume 2 No. 1, 2004 CLINICAL REVIEW Well-Differentiated Thyroid Carcinoma: A Review of the Available Follow-Up Modalities Taryn Davids, MD Ally P.H. Prebtani, MD ABSTRACT Well-differentiated
14 Clinical Review Volume 2 No. 1, 2004 CLINICAL REVIEW Well-Differentiated Thyroid Carcinoma: A Review of the Available Follow-Up Modalities Taryn Davids, MD Ally P.H. Prebtani, MD ABSTRACT Well-differentiated
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017
 the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017") How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
How Will (Should) the Latest Guidelines Affect the Endocrinologist s Management of Thyroid Cancer? AACE 2017 Bryan R. Haugen, MD University of Colorado, School of Medicine Outline Some statistics New guidelines
Objectives. 1)To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy
To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy") Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY
 THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
SCIENTIFIC DISCUSSION
 London, 20 January 2005 Product Name: THYROGEN Procedure No.: EMEA/H/C/220/II/18 SCIENTIFIC DISCUSSION 7 Westferry Circus, Canary Wharf, London E14 4HB, UK Tel. (44-20) 74 18 84 00 Fax (44-20) 74 18 86
London, 20 January 2005 Product Name: THYROGEN Procedure No.: EMEA/H/C/220/II/18 SCIENTIFIC DISCUSSION 7 Westferry Circus, Canary Wharf, London E14 4HB, UK Tel. (44-20) 74 18 84 00 Fax (44-20) 74 18 86
RESEARCH ARTICLE. Comparison of Presentation and Clinical Outcome between Children and Young Adults with Differentiated Thyroid Cancer
 RESEARCH ARTICLE Comparison of Presentation and Clinical Outcome between Children and Young Adults with Jian-Tao Wang 1,2&, Rui Huang 1&, An-Ren Kuang 1 * Abstract Background: The aim of the present study
RESEARCH ARTICLE Comparison of Presentation and Clinical Outcome between Children and Young Adults with Jian-Tao Wang 1,2&, Rui Huang 1&, An-Ren Kuang 1 * Abstract Background: The aim of the present study
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
New York, the nation s thyroid gland. Christopher Morley ( ), "Shore Leave"
, Shore Leave") New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination
 Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Diagnostic 131 I whole body scanning after thyroidectomy and ablation for differentiated thyroid cancer
 European Journal of Endocrinology (2004) 150 649 653 ISSN 0804-4643 CLINICAL STUDY Diagnostic 131 I whole body scanning after thyroidectomy and ablation for differentiated thyroid cancer Henry Taylor,
European Journal of Endocrinology (2004) 150 649 653 ISSN 0804-4643 CLINICAL STUDY Diagnostic 131 I whole body scanning after thyroidectomy and ablation for differentiated thyroid cancer Henry Taylor,
Objectives. How to Investigate Thyroid Nodules like A Pro
 How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
Evaluation and Management of Thyroid Nodules. Overview of Thyroid Nodules and Their Management. Thyroid Nodule detection: U/S versus Exam
 Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Thyroid Cancer: Imaging Techniques (Nuclear Medicine)
") Thyroid Cancer: Imaging Techniques (Nuclear Medicine) Andrei Iagaru, MD MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology Introduction Ø There are
Thyroid Cancer: Imaging Techniques (Nuclear Medicine) Andrei Iagaru, MD MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology Introduction Ø There are
Management of Thyroid Nodules
 Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
 To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer
 DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
Medical Sciences, 4301 W Markham Street, Little Rock, AR 72205, USA. Correspondence should be addressed to Syed A. Abid;
 Case Reports in Endocrinology, Article ID 584513, 6 pages http://dx.doi.org/10.1155/2014/584513 Case Report Metastatic Follicular Thyroid Carcinoma Secreting Thyroid Hormone and Radioiodine Avid without
Case Reports in Endocrinology, Article ID 584513, 6 pages http://dx.doi.org/10.1155/2014/584513 Case Report Metastatic Follicular Thyroid Carcinoma Secreting Thyroid Hormone and Radioiodine Avid without
5/18/2013. Most thyroid nodules are benign. Thyroid nodules: new techniques in evaluation
 Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
저작권법에따른이용자의권리는위의내용에의하여영향을받지않습니다.
 저작자표시 - 비영리 - 변경금지 2.0 대한민국 이용자는아래의조건을따르는경우에한하여자유롭게 이저작물을복제, 배포, 전송, 전시, 공연및방송할수있습니다. 다음과같은조건을따라야합니다 : 저작자표시. 귀하는원저작자를표시하여야합니다. 비영리. 귀하는이저작물을영리목적으로이용할수없습니다. 변경금지. 귀하는이저작물을개작, 변형또는가공할수없습니다. 귀하는, 이저작물의재이용이나배포의경우,
저작자표시 - 비영리 - 변경금지 2.0 대한민국 이용자는아래의조건을따르는경우에한하여자유롭게 이저작물을복제, 배포, 전송, 전시, 공연및방송할수있습니다. 다음과같은조건을따라야합니다 : 저작자표시. 귀하는원저작자를표시하여야합니다. 비영리. 귀하는이저작물을영리목적으로이용할수없습니다. 변경금지. 귀하는이저작물을개작, 변형또는가공할수없습니다. 귀하는, 이저작물의재이용이나배포의경우,
Thyroid Cancer. With 51 Figures and 30 Tables. Springer
 H.-J. Biersack F. Griinwald (Eds.) Thyroid Cancer With 51 Figures and 30 Tables Springer PART 1 Basics 1 The Changing Epidemiology of Thyroid Cancer 3 R. GORGES 1.1 Basic Epidemiological Problems in Thyroid
H.-J. Biersack F. Griinwald (Eds.) Thyroid Cancer With 51 Figures and 30 Tables Springer PART 1 Basics 1 The Changing Epidemiology of Thyroid Cancer 3 R. GORGES 1.1 Basic Epidemiological Problems in Thyroid
Thyroid Cancer (Carcinoma)
") Information for Patients Thyroid Cancer (Carcinoma) Prepared by the American Association of Clinical Endocrinologists (AACE), a not-for-profit national organization of highly qualified specialists in hormonal
Information for Patients Thyroid Cancer (Carcinoma) Prepared by the American Association of Clinical Endocrinologists (AACE), a not-for-profit national organization of highly qualified specialists in hormonal
CANCERS OF THE ENDOCRINE ORGANS RARE THYROID CANCERS PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES
 CANCERS OF THE ENDOCRINE ORGANS RARE THYROID CANCERS PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES Coordinator: Giuseppe COSTANTE (Endocrinology, Institut Jules Bordet), Ahmad AWADA (Medical
CANCERS OF THE ENDOCRINE ORGANS RARE THYROID CANCERS PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES Coordinator: Giuseppe COSTANTE (Endocrinology, Institut Jules Bordet), Ahmad AWADA (Medical
34 year-old Female with Thyroid Cancer
 34 year-old Female with Thyroid Cancer KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY UNIVERSITY OF CHICAGO ENDORAMA THURSDAY, SEPTEMBER 15 TH, 2016 Disclosures: I do not have any relevant
34 year-old Female with Thyroid Cancer KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY UNIVERSITY OF CHICAGO ENDORAMA THURSDAY, SEPTEMBER 15 TH, 2016 Disclosures: I do not have any relevant
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study
 ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer
 THYROID Volume 16, Number 2, 2006 American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer The American Thyroid Association Guidelines Taskforce*
THYROID Volume 16, Number 2, 2006 American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer The American Thyroid Association Guidelines Taskforce*
Thyroid remnant volume and Radioiodine ablation in Differentiated thyroid carcinoma.
 ORIGINAL ARTICLE Thyroid remnant volume and Radioiodine ablation in Differentiated thyroid carcinoma. Md. Sayedur Rahman Miah, Md. Reajul Islam, Tanjim Siddika Institute of Nuclear Medicine & Allied Sciences,
ORIGINAL ARTICLE Thyroid remnant volume and Radioiodine ablation in Differentiated thyroid carcinoma. Md. Sayedur Rahman Miah, Md. Reajul Islam, Tanjim Siddika Institute of Nuclear Medicine & Allied Sciences,
Thyroid Cancer: Overview And Peculiar Aspects In Philippines Nemencio A. Nicodemus Jr., MD
 16 April 2016, Manila, Philippines Thyroid Cancer: Overview And Peculiar Aspects In Philippines Nemencio A. Nicodemus Jr., MD IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Learning
16 April 2016, Manila, Philippines Thyroid Cancer: Overview And Peculiar Aspects In Philippines Nemencio A. Nicodemus Jr., MD IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Learning
Tania Gallant MD, FRCPC Internal Medicine Update April
 Tania Gallant MD, FRCPC Internal Medicine Update April 28 2017 Disclosures Honoraria/Ad board: Sanofi-Aventis, Janssen, Merck Frosst, Eli-Lilly, Astra Zeneca, Boehringer-Ingelheim Objectives By the end
Tania Gallant MD, FRCPC Internal Medicine Update April 28 2017 Disclosures Honoraria/Ad board: Sanofi-Aventis, Janssen, Merck Frosst, Eli-Lilly, Astra Zeneca, Boehringer-Ingelheim Objectives By the end
Review Article Management of thyroid carcinoma Alauddin M, Joarder AH
 Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together