PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD
|
|
|
- Irene Gilmore
- 6 years ago
- Views:
Transcription


1 PEDIATRICS WK 3 HEAD AND NECK ALISON WALLACE MD, PHD
2 Topics 1. Cervical lymphadenopathy 2. Lymphatic malformation 3. Thyroglossal duct cysts 4. Branchial cleft cysts 5. Thyroid masses
3 CASE 1
4 Case 1 A 2 yo boy is seen in your office with a midline neck mass that has been present for 2 months.
5 Differential diagnosis for a midline neck mass?
6 Differential diagnosis for a midline neck mass? Lymphadenopathy Ectopic thyroid Thyroglossal duct cyst Thymic cyst Dermoid cyst Ranula


7 Case 1 History? Physical? Work up?

8 Case 1 On examination, the mass is 2 cm in size, is not tender or pulsatile, and moves with protrusion of his tongue.
9 Case 1 Ultrasound of the neck demonstrates a midline cystic lesion sitting deep to the strap muscles with no surrounding lymphadenopathy or other pathology. The thyroid gland is noted in the normal location. Findings on thyroid function studies are normal.


10 U/S - Painless, fluctuant mass, spreads the strap muscles


11 CT - Thin walled, smooth, well defined homogeneously attenuating lesions
12 Case 1 - Summary A 2 yo boy is seen in your office with a midline neck mass that has been present for 2 months. On examination, the mass is 2 cm in size, is not tender or pulsatile, and moves with protrusion of his tongue. Ultrasound of the neck demonstrates a midline cystic lesion sitting deep to the strap muscles with no surrounding lymphadenopathy or other pathology. The thyroid gland is noted in the normal location. Findings on thyroid function studies are normal.
13 Case 1 Thyroglssal duct cyst
14 Which of the following statements is true regarding a thyroglossal duct cyst? 1. Simple excision of the mass is sufficient?
15 Which of the following statements is true regarding a thyroglossal duct cyst? 1. Simple excision of the mass is sufficient? 2. This mass most likely represents ectopic thyroid tissue?
16 Which of the following statements is true regarding a thyroglossal duct cyst? 1. Simple excision of the mass is sufficient? 2. This mass most likely represents ectopic thyroid tissue? 3. The rate of recurrence is very high after appropriate therapy?
17 Which of the following statements is true regarding a thyroglossal duct cyst? 1. Simple excision of the mass is sufficient? 2. This mass most likely represents ectopic thyroid tissue? 3. The rate of recurrence is very high after appropriate therapy? 4. These lesions can be found along the base of the tongue and hyoid bone?
18 Which of the following statements is true regarding a thyroglossal duct cyst? 1. Simple excision of the mass is sufficient? 2. This mass most likely represents ectopic thyroid tissue? 3. The rate of recurrence is very high after appropriate therapy? 4. These lesions can be found along the base of the tongue and hyoid bone? 5. Most lesions are associated with a draining cutaneous fistula?
19 TYROGLOSSAL DUCT CYSTS

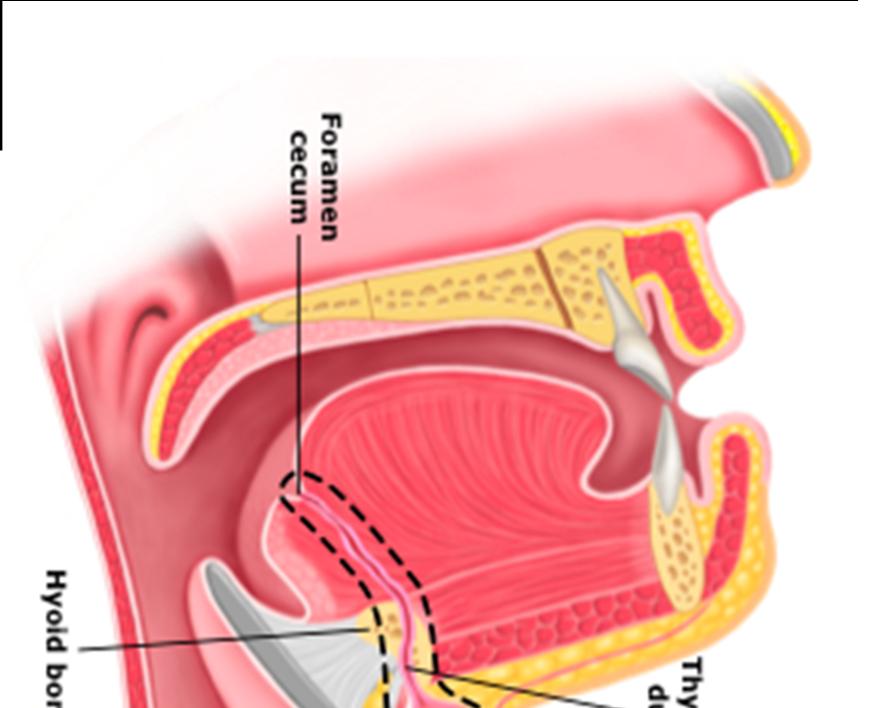
20 Thyroglossal duct The thyroglossal duct is an epitheliumlined connection between the foramen caecum and the thyroid that develops during the descent of the thyroid. It usually involutes in the 8th-10th week of gestation.
21 Gross Anatomy The thyroglossal duct arises from foramen caecum located at the junction of anterior two thirds and posterior third of the tongue. From there it passes in front of the body of the hyoid bone, curving backwards and superiorly to reach behind the bone before once more turning inferiorly and continuing to the isthmus of the thyroid. The pyramidal lobe, if present, marks this point.

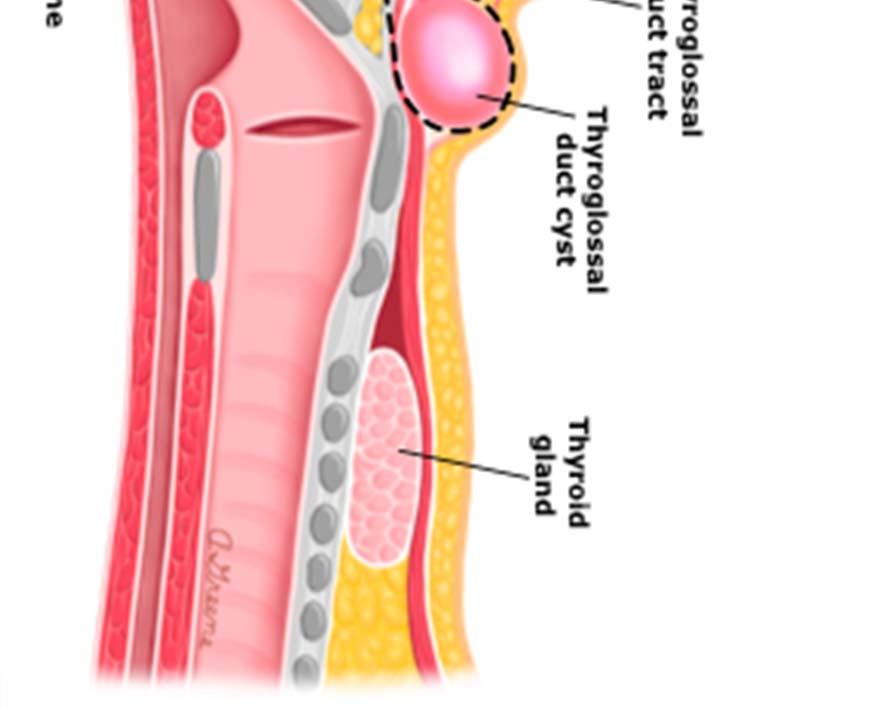
22 Thyroglossal duct cyst Failure of obliteration of the duct may lead to the formation of a thyroglossal duct cyst.
23 Epidemiology Typically present during childhood 90% present before the age of 10 If infected, they can present at any time Account for 70% of all congenital neck anomalies Second most common benign neck mass, after lymphadenopathy Most common midline neck mass in young patients
24 Clinical presentation Presentation is typically either as a painless rounded midline anterior neck swelling If infected, as a red warm painful lump It may move with swallowing and classically elevates on tongue protrusion
25 Location The cysts can occur anywhere along the course of the thyroglossal duct: Infrahyoid location is most common: ~45% (range 25-65%) At the level of hyoid bone: ~30% (range 15-50% Suprahyoid: 20-25% (less common in adults ~5%) Typically located in the midline (~70%) with those offmidline characteristically tucked next to the thyroid cartilage. Almost all are located within 2 cm of the midline, with more inferior lesions tending to be off midline.

26 Associations Ectopic thyroid: ~40%

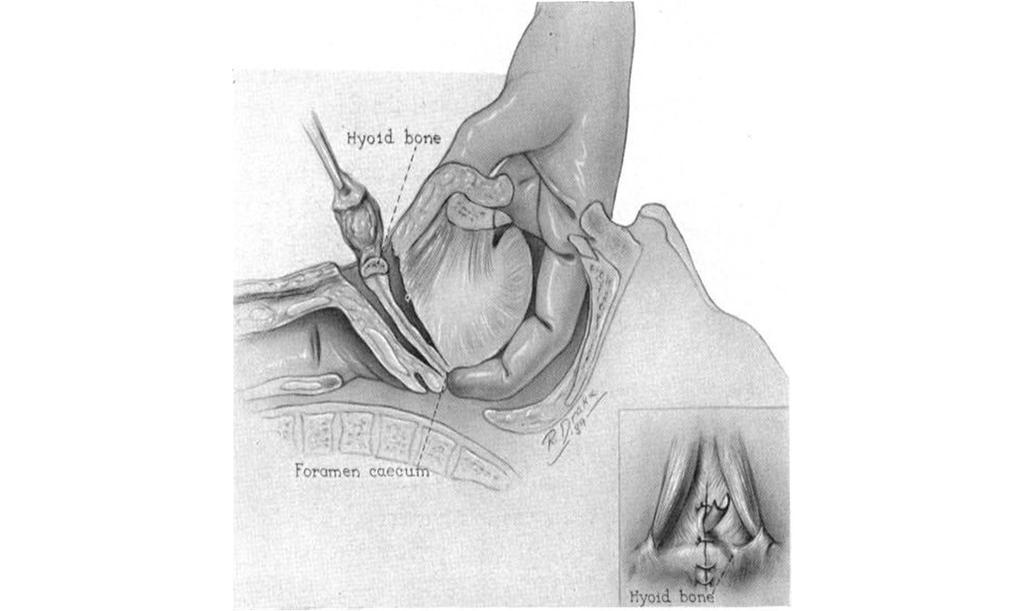
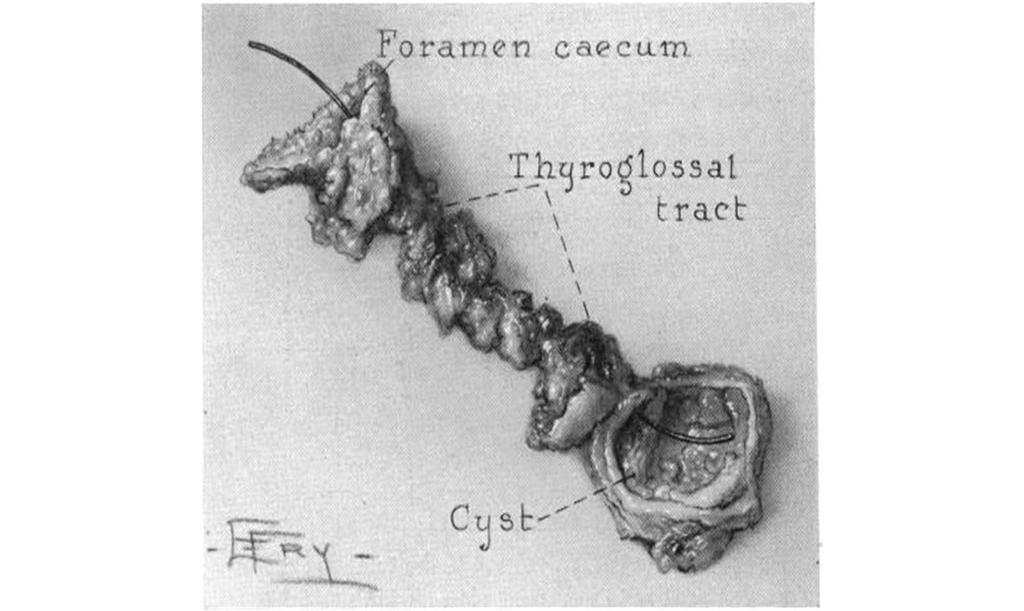
27 Treatment and prognosis Complete resection of the cyst and duct up to the foramen caecum is curative. The Sistrunk procedure includes resection of the middle third of the hyoid bone. There is small risk of recurrence (~2.5%).
28

29
30
31

32 Complications Infection Malignancy Rare Seen in <1% of cysts Most frequently papillary thyroid carcinoma
33 Which of the following statements is true regarding a thyroglossal duct cyst? 1. Simple excision of the mass is sufficient? 2. This mass most likely represents ectopic thyroid tissue? 3. The rate of recurrence is very high after appropriate therapy? 4. These lesions can be found along the base of the tongue and hyoid bone? 5. Most lesions are associated with a draining cutaneous fistula?
34 Comments Most do not have a draining fistula tact, as with branchial cleft remnants. Ultrasound and thyroid function tests should be performed to be certain that there is thyroid tissue in the normal anatomic location so that the patient is not rendered hypothyroid in the postoperative period. Surgical treatment involves removal of the cyst tract along with the central hyoid bone the Sistrunk procedure. Simple cyst excision alone results in high rates of recurrence, where as a Sistrunk procedure has reported recurrence rates of less than 5%.
35
36 CASE 2
37 Case 2 A 2 yo girl is seen in your office with a lateral neck mass that has been present for 2 months.
38 Differential diagnosis for a lateral neck mass?
39 Differential diagnosis for a lateral neck mass? Paramedian thyroglossal duct cyst Cystic lymph nodes Necrotic nodal metastases, especially SCC and papillary thyroid cancer Tuberculous adenitis Vascular lesions jugular vein thrombosis mycotic aneurysm of the neck Neurogenic tumours Neuroblastoma Schwannoma Neurofibroma Ganglioneuroma Cervical dermoid cyst Atypical mycobacterial infection
40 Case 2 History? Physical? Work up?

41 Case 2 On examination, there is a rounded swelling just below angle of mandible. It is non-tender and fluctuant.

42 U/s - sharply demarcated, anechoic

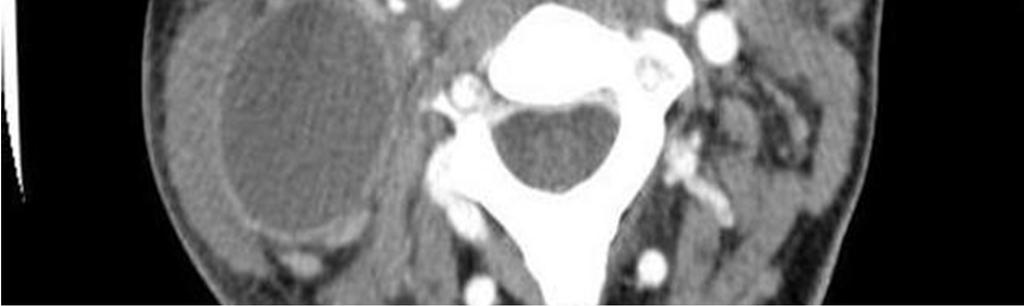
43 CT - rounded, sharply circumscribed fluid density

44 Case 2 Branchial cleft cyst
45 Which of the following statements is false in regard to branchial cleft remnants? 1. Branchial fistulas are more common than external sinuses, which are more common than branchial cysts.
46 Which of the following statements is false in regard to branchial cleft remnants? 1. Branchial fistulas are more common than external sinuses, which are more common than branchial cysts. 2. First branchial cleft remnants are typically located along the anterior border of the SCM muscle.
47 Which of the following statements is false in regard to branchial cleft remnants? 1. Branchial fistulas are more common than external sinuses, which are more common than branchial cysts. 2. First branchial cleft remnants are typically located along the anterior border of the SCM muscle. 3. Second branchial cleft remnants are the most common branchial cleft remnants.
48 Which of the following statements is false in regard to branchial cleft remnants? 1. Branchial fistulas are more common than external sinuses, which are more common than branchial cysts. 2. First branchial cleft remnants are typically located along the anterior border of the SCM muscle. 3. Second branchial cleft remnants are the most common branchial cleft remnants. 4. Third branchial cleft remnants are typically located in the suprasternal notch or clavicular region.
49 Which of the following statements is false in regard to branchial cleft remnants? 1. Branchial fistulas are more common than external sinuses, which are more common than branchial cysts. 2. First branchial cleft remnants are typically located along the anterior border of the SCM muscle. 3. Second branchial cleft remnants are the most common branchial cleft remnants. 4. Third branchial cleft remnants are typically located in the suprasternal notch or clavicular region. 5. Second branchial cleft remnants are typicaly located along the anterior border of the sternocleidomastoid muscle.
50 BRANCHIAL CLEFT REMNANTS
51 Branchial Cleft Remnants Structures of the head and neck are derived from six pairs of branchial arches with intervening external clefts and internal pouches. Failure of these structures to regress leads to congenital branchial fistulas, sinuses and cysts. Fistula > sinus > cyst
52 Branchial Cleft Remnants
53 ANOMALIES The range of anomalies can include: Cyst: no internal or external communication Fistula: communicates both internally and externally Sinus: incomplete tract
54 First branchial remnants Typically located: In the front or back of the ear In the region of the mandible Fistulas typically course through the parotid gland deep or through branches of the facial nerve and end in the external auditory canal
55 Second branchial remnants Most common Typically located: Along the anterior border of the SCM muscle
56 Third branchial remnants Typically located: At the sternal notch or the clavicular region
57 Second branchial remnants Most common. Second branchial cleft cysts are a cystic dilatation of the remnant of the 2nd branchial apparatus, and along with 2nd branchial fistulae and sinuses accounts for 95% of all branchial cleft anomalies. Typically located along the anterior border of the sternocleidomastoid muscle.
58 Clinical Presentation Although a congenital abnormality, cysts tend to present in early adulthood (10-40 years of age) often after minor trauma or infection. Cysts present as a rounded swelling in the lateral neck Sinus or fistulas present earlier as continuous mucoid drainage.

59 Treatment Surgical excision

60 COMPLICATIONS Superimposed infection
61 Which of the following statements is false in regard to branchial cleft remnants? 1. Branchial fistulas are more common than external sinuses, which are more common than branchial cysts. 2. First branchial cleft remnants are typically located along the anterior border of the SCM muscle. 3. Second branchial cleft remnants are the most common branchial cleft remnants. 4. Third branchial cleft remnants are typically located in the suprasternal notch or clavicular region. 5. Second branchial cleft remnants are typicaly located along the anterior border of the sternocleidomastoid muscle.
62
63 CASE 3
64 Case 3 A 6 yo girl from Belarus is seen in your office with a neck mass that has been increasing in size for 2 months.

65 Case 3 History? Physical? Work up?

66 Case 3

67 Case 3

68 Case 3 Thyroid cancer
69 Thyroid nodules Uncommon in children Nodules diagnosed in children carry a greater risk of malignancy compared to those in adults (22%-26% vs 5%- 10%) Among 15- to 19-year- old adolescents, thyroid cancer is the eighth most frequently diagnosed cancer and the second most common cancer among girls.
70 Risk factors Radiation exposure Iodine deficiency A history of antecedent thyroid disease Several genetic syndromes High risk group - cancer survivors who were treated for their primary malignancy with radiation
71
72 Initial evaluation, treatment, and follow-up of the pediatric thyroid nodule Surgery implies lobectomy plus isthmusectomy in most cases
73 Initial postoperative staging
74
75 CERVICAL LYMPHADENOPATHY
76 Cervical lymphadenopathy Enlarged lymph nodes is one of the most common pediatric conditions. They occur usually along the sternocleidomastoid muscle border, often presenting in clusters.

77 Work up History Physical Imaging
78 Presentation Typical A small, mobile, rubbery, palpable mass in the anterior cervical triangle. Worrisome Fixed, nontender, progressively enlarging nodes in the supraclavicular region. Night sweats and a history of weight loss.

79 Workup Biopsy indications Worrisome features >2 cm Present for > 6 wks, not responsive to antibiotics Negative serology TB, EBV, Bartonella
80 Cervical lymphadenopathy
81
82 LYMPHATIC MALFORMATION
83 Lymphatic malformations Rare non-malignant masses consisting of fluid-filled channels or spaces thought to be caused by the abnormal development of the lymphatic system. Usually apparent at birth or by two years of age. Can affect any area of the body (except the brain), but most commonly affect the head and neck. Lymphatic malformations are not cancerous and there is no known risk of malignant transformation.

84 Presentation Soft cystic masses that distort the surrounding anatomy, including the airway Posterior neck region

85 Complications Airway compromise Infection Hemorrhage
86 Classification 1. Macrocystic 2. Microcystic 3. Mixed (a combination of the other two)
87 Macrocystic Characterized by a single or multiple fluid-filled pockets or cysts Generally form soft, large translucent masses Overlying skin may have a bluish tinge Macrocystic lymphatic malformations can potentially be extremely large, even large enough to obstruct the airway at delivery
88 Microcystic Appear as several small, raised sacs (vesicles) on the skin that contain clear or bloody (hemorrhagic) fluid. They generally grow slowly usually in proportion with a growing child. Microcystic lymphatic malformations can thicken or swell causing enlargement of surrounding soft tissue and bones.
89 Diagnosis?
90 Treatment options 1. Percutaneous drainage 2. Surgery 3. Sclerotherapy 4. Laser therapy 5. Radiofrequency ablation These different treatment options may be used in various combinations.
91 Treatment Complete surgical excision Difficult because of the intimate involvement with surrounding vital structures Radical resection with sacrifice of vital structures is not advocated Sclerosing agents include bleomycin or OK-432, derived from Streptococcus pyogenes
92
Congenital Neck Masses C. Stefan Kénel-Pierre, MD
 Congenital Neck Masses C. Stefan Kénel-Pierre, MD SUNY-LICH Medical Center Department of Surgery Case Presentation xx year old male presents with sudden onset left lower neck swelling x 1 week Denies pain,
Congenital Neck Masses C. Stefan Kénel-Pierre, MD SUNY-LICH Medical Center Department of Surgery Case Presentation xx year old male presents with sudden onset left lower neck swelling x 1 week Denies pain,
Neck lumps in children
 Neck lumps in children Midline Lateral Midline neck lumps Thyroglossal cyst - 80% Dermoid cyst Submental lymph node Ectopic thyroid Some rare lesions Thyroglossal cyst Diagnosis: midline, usually overlying
Neck lumps in children Midline Lateral Midline neck lumps Thyroglossal cyst - 80% Dermoid cyst Submental lymph node Ectopic thyroid Some rare lesions Thyroglossal cyst Diagnosis: midline, usually overlying
Chapter 13: Mass in the Neck. Raymond P. Wood II:
 Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Thyroglossal cyst our experience
 Volume 3 Issue 1 2013 ISSN: 2250-0359 Thyroglossal cyst our experience Balasubramanian Thiagarajan 1 Ulaganathan Venkatesan 2 Geetha Ramamoorthy 1 1 Stanley Medical College 2 Meenakshi Medical College
Volume 3 Issue 1 2013 ISSN: 2250-0359 Thyroglossal cyst our experience Balasubramanian Thiagarajan 1 Ulaganathan Venkatesan 2 Geetha Ramamoorthy 1 1 Stanley Medical College 2 Meenakshi Medical College
THYROID & PARATHYROID. By Prof. Saeed Abuel Makarem & Dr. Sanaa Al-Sharawy
 THYROID & PARATHYROID By Prof. Saeed Abuel Makarem & Dr. Sanaa Al-Sharawy 1 OBJECTIVES By the end of the lecture, the student should be able to: Describe the shape, position, relations and structure of
THYROID & PARATHYROID By Prof. Saeed Abuel Makarem & Dr. Sanaa Al-Sharawy 1 OBJECTIVES By the end of the lecture, the student should be able to: Describe the shape, position, relations and structure of
Neckmasses in infancy and childhood: Clinical and radiological classification and imaging approaches M. Mearadji
 Neckmasses in infancy and childhood: Clinical and radiological classification and imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Neck masses are a frequent
Neckmasses in infancy and childhood: Clinical and radiological classification and imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Neck masses are a frequent
LUMPS AND BUMPS: EVALUATION AND MANAGEMENT OF SOFT TISSUE MASSES IN PEDIATRICS. By Elizabeth A. Paton, MSN, RN-BC, PPCNP-BC, FAEN
 LUMPS AND BUMPS: EVALUATION AND MANAGEMENT OF SOFT TISSUE MASSES IN PEDIATRICS By Elizabeth A. Paton, MSN, RN-BC, PPCNP-BC, FAEN I. Objectives II. By the end of this presentation, the learner will be able
LUMPS AND BUMPS: EVALUATION AND MANAGEMENT OF SOFT TISSUE MASSES IN PEDIATRICS By Elizabeth A. Paton, MSN, RN-BC, PPCNP-BC, FAEN I. Objectives II. By the end of this presentation, the learner will be able
Cystic Head and Neck Lesions
 Cystic Head and Neck Lesions Disclosures None Brad Wright, MD 19 March 2018 Key points Huge variety of cystic lesions in H&N May be cystic, necrotic, or solid but cystic-appearing Patient age, clinical
Cystic Head and Neck Lesions Disclosures None Brad Wright, MD 19 March 2018 Key points Huge variety of cystic lesions in H&N May be cystic, necrotic, or solid but cystic-appearing Patient age, clinical
Thyroid gland. importance. relations and connections. external laryngeal nerves. malformations.
 Thyroid gland 1. Recognize and understand the coverings of the thyroid gland and their clinical importance. 2. Recognize and understand the main parts of the thyroid gland and their locations, relations
Thyroid gland 1. Recognize and understand the coverings of the thyroid gland and their clinical importance. 2. Recognize and understand the main parts of the thyroid gland and their locations, relations
HEAD & NECK SWELLINGS
 HEAD & NECK SWELLINGS EXCLUDING GOITRE FAISAL GHANI SIDDIQUI MBBS; FCPS; MCPS-HPE; PGDIP-BIOETHICS PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y MIDLINE SWELLINGS NECK SWELLINGS
HEAD & NECK SWELLINGS EXCLUDING GOITRE FAISAL GHANI SIDDIQUI MBBS; FCPS; MCPS-HPE; PGDIP-BIOETHICS PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y MIDLINE SWELLINGS NECK SWELLINGS
Evaluation of Neck Mass. Disclosure. Learning Objectives 3/24/2014. Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ. Nothing to disclose
 Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Dr Nick McIvor. Dr John Chaplin. Head & Neck Surgeon Auckland City Hospital Auckland. Auckland Head & Neck Surgeon Gillies Hospital Auckland
 Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
Thyroid and Parathyroid Glands
 Thyroid and Parathyroid Glands Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/ explanation Objectives: By the end of the lecture,
Thyroid and Parathyroid Glands Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/ explanation Objectives: By the end of the lecture,
Lecture 01. The Thyroid & Parathyroid Glands. By: Dr Farooq Khan PMC Date: 12 th March. 2018
 Lecture 01 The Thyroid & Parathyroid Glands By: Dr Farooq Khan PMC Date: 12 th March. 2018 INTRODUCTION LAYERS OF THE NECK The neck has four major compartments or layer which are enclosed by an outer musculofascial
Lecture 01 The Thyroid & Parathyroid Glands By: Dr Farooq Khan PMC Date: 12 th March. 2018 INTRODUCTION LAYERS OF THE NECK The neck has four major compartments or layer which are enclosed by an outer musculofascial
REVIEW OF CLINICAL EMBRYOLOGY OF HEAD AND NECK
 REVIEW OF CLINICAL EMBRYOLOGY OF HEAD AND NECK OUTLINE - EMBRYOLOGY UNDERLYING CLINICAL CONDITIONS I. EARLY DEVELOPMENT OF FACE: CLEFT LIP, CLEFT PALATE, OBSTRUCTED NASOLACRIMAL DUCT II. BRANCHIAL ARCHES
REVIEW OF CLINICAL EMBRYOLOGY OF HEAD AND NECK OUTLINE - EMBRYOLOGY UNDERLYING CLINICAL CONDITIONS I. EARLY DEVELOPMENT OF FACE: CLEFT LIP, CLEFT PALATE, OBSTRUCTED NASOLACRIMAL DUCT II. BRANCHIAL ARCHES
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS. Dr. Pamela Hanson DO PGY3
 PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
PAPILLARY THYROID CARCINOMA PRESENTING AS A LATERAL NECK MASS MASS Dr. Pamela Hanson DO PGY3 MK CASE PRESENTATION 28 yo Female presented to the ENT Clinic in October 2016, with the complaint of chronic
Anatomy of the Thyroid Gland
 Anatomy of the Thyroid Gland Introduction Nomenclature G, thyreos= shield, eidos= like Location Root of the neck ventrally (C5-T1) Function endocrine gland that secretes: Thyroxine (T4) T3 Calcitonin LWW,
Anatomy of the Thyroid Gland Introduction Nomenclature G, thyreos= shield, eidos= like Location Root of the neck ventrally (C5-T1) Function endocrine gland that secretes: Thyroxine (T4) T3 Calcitonin LWW,
PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY
 PATIENT CENTERED MEDICINE - 1 GOALS & OUTCOMES: PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY 1. To introduce the applied anatomy relevant for the examination of the head
PATIENT CENTERED MEDICINE - 1 GOALS & OUTCOMES: PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY 1. To introduce the applied anatomy relevant for the examination of the head
Head and Neck Case Studies
 Head and Neck Case Studies John Chaplin & Nick McIvor www.headneck.co.nz Head and Neck lumps every lump must have a diagnosis Working diagnosis» +/- investigations Review» +/- investigations auckland head
Head and Neck Case Studies John Chaplin & Nick McIvor www.headneck.co.nz Head and Neck lumps every lump must have a diagnosis Working diagnosis» +/- investigations Review» +/- investigations auckland head
Branchial Cleft and Pouch Anomalies
 Branchial Cleft and Pouch Anomalies Prof.Mohamed Hesham Alexandria Faculty of Medicine Alexandria, Egypt Emberyological Basis Branchial Clefts 1st 2nd Pinna EAC 3rd 4th 4th 6th Cervical sinus Branchial
Branchial Cleft and Pouch Anomalies Prof.Mohamed Hesham Alexandria Faculty of Medicine Alexandria, Egypt Emberyological Basis Branchial Clefts 1st 2nd Pinna EAC 3rd 4th 4th 6th Cervical sinus Branchial
Shadow because the air
 Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
"Mummy what's this on my neck? - A pictorial review of paediatric neck masses"
 "Mummy what's this on my neck? - A pictorial review of paediatric neck masses" Poster No.: C-0405 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Farrugia, A. S. Gatt; Msida/MT Keywords: Education,
"Mummy what's this on my neck? - A pictorial review of paediatric neck masses" Poster No.: C-0405 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Farrugia, A. S. Gatt; Msida/MT Keywords: Education,
Ultrasound Interpretation of Non-Thyroid Neck Pathology
 Ultrasound Interpretation of Non-Thyroid Neck Pathology Kevin T. Brumund, M.D., F.A.C.S. Associate Professor of Surgery Head and Neck Surgery University of California, San Diego Health Sciences VA Medical
Ultrasound Interpretation of Non-Thyroid Neck Pathology Kevin T. Brumund, M.D., F.A.C.S. Associate Professor of Surgery Head and Neck Surgery University of California, San Diego Health Sciences VA Medical
Clinical Anatomy of the Thyroid and Adrenal Glands
 Clinical Anatomy of the Thyroid and Adrenal Glands Handout download: http://www.oucom.ohiou.edu/dbms-witmer/gs-rpac.htm 28 October 2003 Lawrence M. Witmer, PhD Department of Biomedical Sciences College
Clinical Anatomy of the Thyroid and Adrenal Glands Handout download: http://www.oucom.ohiou.edu/dbms-witmer/gs-rpac.htm 28 October 2003 Lawrence M. Witmer, PhD Department of Biomedical Sciences College
A CASE OF A Huge Submandibular Pleomorphic Adenoma
 ISPUB.COM The Internet Journal of Head and Neck Surgery Volume 4 Number 2 S VERMA Citation S VERMA.. The Internet Journal of Head and Neck Surgery. 2009 Volume 4 Number 2. Abstract Pleomorphic adenoma
ISPUB.COM The Internet Journal of Head and Neck Surgery Volume 4 Number 2 S VERMA Citation S VERMA.. The Internet Journal of Head and Neck Surgery. 2009 Volume 4 Number 2. Abstract Pleomorphic adenoma
The Neck the lower margin of the mandible above the suprasternal notch and the upper border of the clavicle
 The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
Cervical Lymph Nodes
 Cervical Lymph Nodes Diana Gaitini, MD Unit of Ultrasound, Department of Medical Imaging Rambam Medical Center and Faculty of Medicine Technion, Israel Institute of Technology Haifa, Israel Learning Targets
Cervical Lymph Nodes Diana Gaitini, MD Unit of Ultrasound, Department of Medical Imaging Rambam Medical Center and Faculty of Medicine Technion, Israel Institute of Technology Haifa, Israel Learning Targets
Evaluation of Head and Neck Masses in Adults
 Evaluation of Head and Neck Masses in Adults Kristi Chang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery University of Iowa Hospitals and Clinics Annual Refresher Course for
Evaluation of Head and Neck Masses in Adults Kristi Chang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery University of Iowa Hospitals and Clinics Annual Refresher Course for
 Drawings illustrating the human pharyngeal apparatus. Drawings illustrating the human pharyngeal apparatus. Drawings illustrating the human pharyngeal apparatus. Drawings illustrating the human pharyngeal
Drawings illustrating the human pharyngeal apparatus. Drawings illustrating the human pharyngeal apparatus. Drawings illustrating the human pharyngeal apparatus. Drawings illustrating the human pharyngeal
Anatomy: head and Neck (6 questions) 1. Prevertebral Flexor Musculature (lying in front of the vertebrae) include all, EXCEPT: Longus Colli.
 1. Prevertebral Flexor Musculature (lying in front of the vertebrae) include all, EXCEPT: Longus Colli.") Anatomy: head and Neck (6 questions) 1. Prevertebral Flexor Musculature (lying in front of the vertebrae) include all, EXCEPT: Longus Colli. Rectus Capitis Anterior. Rectus Capitis Lateralis. Rectus Capitis
Anatomy: head and Neck (6 questions) 1. Prevertebral Flexor Musculature (lying in front of the vertebrae) include all, EXCEPT: Longus Colli. Rectus Capitis Anterior. Rectus Capitis Lateralis. Rectus Capitis
INFECTION. HIV Infection DWI
 HIV Infection INFECTION DWI Fig Axial CT and MRI images show multiple enlarged lymph nodes in the neck as well as in the parotid gland bilaterally. These nodes were suppurative with positive diffusion.
HIV Infection INFECTION DWI Fig Axial CT and MRI images show multiple enlarged lymph nodes in the neck as well as in the parotid gland bilaterally. These nodes were suppurative with positive diffusion.
A clinical study on branchial arch anomalies
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 18, Issue 1 Ver. 5 (January. 2019), PP 05-10 www.iosrjournals.org Ashim Sarkar 1, Ritam Ray 2 1 (Clinical
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 18, Issue 1 Ver. 5 (January. 2019), PP 05-10 www.iosrjournals.org Ashim Sarkar 1, Ritam Ray 2 1 (Clinical
Imaging Work-Up of a Neck Mass - Adults & Children
 Disclosures Imaging Work-Up of a Neck Mass - Adults & Children I have nothing to disclose Christine M Glastonbury MBBS Professor of Radiology & Biomedical Imaging Otolaryngology-Head & Neck Surgery and
Disclosures Imaging Work-Up of a Neck Mass - Adults & Children I have nothing to disclose Christine M Glastonbury MBBS Professor of Radiology & Biomedical Imaging Otolaryngology-Head & Neck Surgery and
DEVELOPMENT & STRUCTURE OF THYROID GLAND DR TATHEER ZAHRA ASSISTANT PROFESSOR ANATOMY
 DEVELOPMENT & STRUCTURE OF THYROID GLAND DR TATHEER ZAHRA ASSISTANT PROFESSOR ANATOMY DEVELOPMENT OF THYROID Concept of pharyngeal arch 3 rd week 4 th week Adults 7 th week HISTOGENESIS OF THYROID GLAND
DEVELOPMENT & STRUCTURE OF THYROID GLAND DR TATHEER ZAHRA ASSISTANT PROFESSOR ANATOMY DEVELOPMENT OF THYROID Concept of pharyngeal arch 3 rd week 4 th week Adults 7 th week HISTOGENESIS OF THYROID GLAND
CERVICAL LYMPH NODES
 CERVICAL LYMPH NODES (ANATOMY & EXAMINATION) Hemant (DTCD 1 st YEAR) 1. Lymphatic Tissues: A Type of connective tissue that contains large numbers of lymphocytes. 2. Lymphatic Vessels: Are Tubes that assist
CERVICAL LYMPH NODES (ANATOMY & EXAMINATION) Hemant (DTCD 1 st YEAR) 1. Lymphatic Tissues: A Type of connective tissue that contains large numbers of lymphocytes. 2. Lymphatic Vessels: Are Tubes that assist
AACE/ACE Principles of Endocrine Neck Sonography Course
 AACE/ACE Principles of Endocrine Neck Sonography Course Primary objective of thyroid ultrasound: assess for malignant disease Nodular Disease Benign Malignant Goiter Iodine deficient Thyroiditis Organification
AACE/ACE Principles of Endocrine Neck Sonography Course Primary objective of thyroid ultrasound: assess for malignant disease Nodular Disease Benign Malignant Goiter Iodine deficient Thyroiditis Organification
Conflict of Interest: none. Neonatal Airway Masses. Neonatal Respiratory Papillomatosis. Paul J. Samuels, MD
 Paul J. Samuels, MD Professor of Anesthesiology and Pediatrics Director of Education Cincinnati Children s Hospital Cincinnati, Ohio Conflict of Interest: none Neonatal Respiratory Papillomatosis Caused
Paul J. Samuels, MD Professor of Anesthesiology and Pediatrics Director of Education Cincinnati Children s Hospital Cincinnati, Ohio Conflict of Interest: none Neonatal Respiratory Papillomatosis Caused
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV
 DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
Management of thyroglossal duct cysts in children
 Pediatrics International (2004) 46, 77 80 Original Article Management of thyroglossal duct cysts in children ZAFER TÜRKYILMAZ, 1 KAAN SÖNMEZ, 1 RAMAZAN KARABULUT, 1 BILLUR DEMIR}OULLARI, 1 CEM SEZER, 2
Pediatrics International (2004) 46, 77 80 Original Article Management of thyroglossal duct cysts in children ZAFER TÜRKYILMAZ, 1 KAAN SÖNMEZ, 1 RAMAZAN KARABULUT, 1 BILLUR DEMIR}OULLARI, 1 CEM SEZER, 2
Chief complaint. A mass at right chest
 Chief complaint A mass at right chest Present illness This 1-year-5-month-old girl had a mass at right side chest since one month ago. flat and not tender at first In the recent 2 days, the mass enlarged
Chief complaint A mass at right chest Present illness This 1-year-5-month-old girl had a mass at right side chest since one month ago. flat and not tender at first In the recent 2 days, the mass enlarged
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Radiology- Pathology Conference 4/29/2012. Lymph Nodes. John McGrath
 Radiology- Pathology Conference 4/29/2012 Lymph Nodes John McGrath 1 Presentation material is for education purposes only. All rights reserved. 2012 URMC Radiology Page 1 of 24 Case 1: 51 year-old male
Radiology- Pathology Conference 4/29/2012 Lymph Nodes John McGrath 1 Presentation material is for education purposes only. All rights reserved. 2012 URMC Radiology Page 1 of 24 Case 1: 51 year-old male
Case Presentation. x year old African American male seen in Pediatric Surgery Clinic. History: NKDA
 Case Presentation ALIREZA SADEGHI MD Kings County Hospital Center University Hospital of Brooklyn Downstate Medical Center Division of Pediatric Surgery July 7 th 2006 Case Presentation x year old African
Case Presentation ALIREZA SADEGHI MD Kings County Hospital Center University Hospital of Brooklyn Downstate Medical Center Division of Pediatric Surgery July 7 th 2006 Case Presentation x year old African
Neck-2. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
Lies in front and sides of the neck. Consists of two lobe connected anterior to the trachea by an isthmus.
 THYROID GLAND 1 Lies in front and sides of the neck. Consists of two lobe connected anterior to the trachea by an isthmus. A small pyramidal lobe projects upwards from the left lobe in 40% of cases. The
THYROID GLAND 1 Lies in front and sides of the neck. Consists of two lobe connected anterior to the trachea by an isthmus. A small pyramidal lobe projects upwards from the left lobe in 40% of cases. The
Clinical Presentations and Management of Thyroglossal Duct Cyst and Sinuses
 THYROGLOSSAL THE IRAQI POSTGRADUATE CYST MEDICAL AND SINUSES JOURNAL Clinical Presentations and Management of Thyroglossal Duct Cyst and Sinuses Ayad Ahmed Shihab Al-Azzawi*, Azzam M. A. Al-Salami **,
THYROGLOSSAL THE IRAQI POSTGRADUATE CYST MEDICAL AND SINUSES JOURNAL Clinical Presentations and Management of Thyroglossal Duct Cyst and Sinuses Ayad Ahmed Shihab Al-Azzawi*, Azzam M. A. Al-Salami **,
ORIGINAL ARTICLE. and histological data. An additional confounding factor is infection, which oftendivertsthephysician sattention.
 ORIGINAL ARTICLE First Branchial Cleft Anomalies A Study of 39 Cases and a Review of the Literature Jean-Michel Triglia, MD; Richard Nicollas, MD; Vincent Ducroz, MD; Peter J. Koltai, MD; Erea-Noël Garabedian,
ORIGINAL ARTICLE First Branchial Cleft Anomalies A Study of 39 Cases and a Review of the Literature Jean-Michel Triglia, MD; Richard Nicollas, MD; Vincent Ducroz, MD; Peter J. Koltai, MD; Erea-Noël Garabedian,
Asian Journal of Pharmacy and Life Science ISSN Vol.3 (2), April-June, 2013
, April-June, 2013") RECURRENT NECK INFECTION ASSOCIATED WITH FOURTH BRANCHIAL POUCH SINUS: A RARE CLINICAL ENTITY WITH DELAYED DIAGNOSIS Bhawana Pant* 1, Sanjay Gaur 2, Shahzad Ahmad 1 1. Department of E.N.T, Government Medical
RECURRENT NECK INFECTION ASSOCIATED WITH FOURTH BRANCHIAL POUCH SINUS: A RARE CLINICAL ENTITY WITH DELAYED DIAGNOSIS Bhawana Pant* 1, Sanjay Gaur 2, Shahzad Ahmad 1 1. Department of E.N.T, Government Medical
Neck Ultrasound. Faculty Info: Amy Kule, MD
 Neck Ultrasound Date: Friday, October 19, 2018 Time: 11:00 AM Location: SMALL GROUP LABORATORY SSOM L71 Watch: Ø Neck Ultrasound Scanning Protocol (4:00): https://www.youtube.com/watch?v=zozd2x2ll4q Faculty
Neck Ultrasound Date: Friday, October 19, 2018 Time: 11:00 AM Location: SMALL GROUP LABORATORY SSOM L71 Watch: Ø Neck Ultrasound Scanning Protocol (4:00): https://www.youtube.com/watch?v=zozd2x2ll4q Faculty
Management of unknown primary with neck node metastasis: Current evidence
 Management of unknown primary with neck node metastasis: Current evidence Dr. Pooja Nandwani Patel Associate Professor Dept. of Radiation Oncology GCRI, Ahmedabad Introduction- Approach to Topic What is
Management of unknown primary with neck node metastasis: Current evidence Dr. Pooja Nandwani Patel Associate Professor Dept. of Radiation Oncology GCRI, Ahmedabad Introduction- Approach to Topic What is
For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER
 GROSS ANATOMY EXAMINATION May 15, 2000 For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER 1. Pain associated with an infection limited to the middle
GROSS ANATOMY EXAMINATION May 15, 2000 For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER 1. Pain associated with an infection limited to the middle
MDCT and Ultrasound Evaluation of Primary Masses of Neck with Pathological Correlation
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 9 Ver. IX (September). 2016), PP 63-71 www.iosrjournals.org MDCT and Ultrasound Evaluation
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 9 Ver. IX (September). 2016), PP 63-71 www.iosrjournals.org MDCT and Ultrasound Evaluation
REVIEW/PREVIEW OF HEAD AND NECK ANATOMY FOR ENT EXAM
 REVIEW/PREVIEW OF HEAD AND NECK ANATOMY FOR ENT EXAM - 2017 PALPATE CAROTID ARTERY: AT LEVEL OF CAROTID BIFURCATION VERTEBRAL LEVEL C4 Sternocleidomastoid Muscle INTERNAL CAROTID EXTERNAL CAROTID COMMON
REVIEW/PREVIEW OF HEAD AND NECK ANATOMY FOR ENT EXAM - 2017 PALPATE CAROTID ARTERY: AT LEVEL OF CAROTID BIFURCATION VERTEBRAL LEVEL C4 Sternocleidomastoid Muscle INTERNAL CAROTID EXTERNAL CAROTID COMMON
Neck mass Evaluation & Management OTOLARYNGOLOGY, HEAD & NECK SURGICAL ONCOLOGY
 Neck mass Evaluation & Management MOHAMMED ALESSA MBBS,FRCSC ASSISTANT PROFESSOR CONSULTANT OTOLARYNGOLOGY, HEAD & NECK SURGICAL ONCOLOGY KSU, MEDICAL CITY & KKUH Objectives Obtain map overview in neck
Neck mass Evaluation & Management MOHAMMED ALESSA MBBS,FRCSC ASSISTANT PROFESSOR CONSULTANT OTOLARYNGOLOGY, HEAD & NECK SURGICAL ONCOLOGY KSU, MEDICAL CITY & KKUH Objectives Obtain map overview in neck
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Evaluation of congenital masses of the neck in children: embryological, clinical and radiological review
 Evaluation of congenital masses of the neck in children: embryological, clinical and radiological review Poster No.: C-1731 Congress: ECR 2014 Type: Educational Exhibit Authors: N. C. S. D. Ferreira, A.
Evaluation of congenital masses of the neck in children: embryological, clinical and radiological review Poster No.: C-1731 Congress: ECR 2014 Type: Educational Exhibit Authors: N. C. S. D. Ferreira, A.
Deepak M. Sampathu MD, PhD Assistant Professor of Clinical Radiology University of Pennsylvania
 Deepak M. Sampathu MD, PhD Assistant Professor of Clinical Radiology University of Pennsylvania Objectives Recognize benign masses and masslike lesions of the neck and skull base Understand the imaging
Deepak M. Sampathu MD, PhD Assistant Professor of Clinical Radiology University of Pennsylvania Objectives Recognize benign masses and masslike lesions of the neck and skull base Understand the imaging
The Neck. BY: Lina Abdullah & Rahaf Jreisat
 The Neck BY: Lina Abdullah & Rahaf Jreisat Boundaries of the Neck: generally from base of the skull to root of the neck Superior margin :From superior nuchal line of occipital bone up to mastoid process
The Neck BY: Lina Abdullah & Rahaf Jreisat Boundaries of the Neck: generally from base of the skull to root of the neck Superior margin :From superior nuchal line of occipital bone up to mastoid process
Ectopic cervical thymic cyst in a seven year old: A diagnostic challenge.
 ecommons@aku Section of Otolaryngology, Head & Neck Surgery Department of Surgery May 2018 Ectopic cervical thymic cyst in a seven year old: A diagnostic challenge. Haissan Iftikhar Aga Khan University,
ecommons@aku Section of Otolaryngology, Head & Neck Surgery Department of Surgery May 2018 Ectopic cervical thymic cyst in a seven year old: A diagnostic challenge. Haissan Iftikhar Aga Khan University,
Large veins of the thorax Brachiocephalic veins
 Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Osman Ilkay Ozdamar, 1 Gul Ozbilen Acar, 1 Cigdem Kafkasli, 1 M. Tayyar Kalcioglu, 1 Tulay Zenginkinet, 2 and H. Gonca Tamer 3. 1.
 Case Reports in Otolaryngology Volume 2015, Article ID 79658, 4 pages http://dx.doi.org/10.1155/2015/79658 Case Report Papillary Thyroid Microcarcinoma with a Large Cystic Dilated Lymph Node Metastasis
Case Reports in Otolaryngology Volume 2015, Article ID 79658, 4 pages http://dx.doi.org/10.1155/2015/79658 Case Report Papillary Thyroid Microcarcinoma with a Large Cystic Dilated Lymph Node Metastasis
Swelling. Size: measure exact size in cm using a tape measure (measure longitudinal and transverse axis and if possible the depth)
") Swelling Inspection Site: exact anatomic position Number: single or multiple Shape: spherical, oval, kidney-shaped or irregular Size: measure exact size in cm using a tape measure (measure longitudinal
Swelling Inspection Site: exact anatomic position Number: single or multiple Shape: spherical, oval, kidney-shaped or irregular Size: measure exact size in cm using a tape measure (measure longitudinal
Case Report Cervical Thymic Cyst: A Rare Differential Diagnosis in Lateral Neck Swelling
 Case Reports in Otolaryngology Volume 2013, Article ID 350502, 4 pages http://dx.doi.org/10.1155/2013/350502 Case Report Cervical Thymic Cyst: A Rare Differential Diagnosis in Lateral Neck Swelling Vijendra
Case Reports in Otolaryngology Volume 2013, Article ID 350502, 4 pages http://dx.doi.org/10.1155/2013/350502 Case Report Cervical Thymic Cyst: A Rare Differential Diagnosis in Lateral Neck Swelling Vijendra
Advanced Anatomy of the Neck
 AACE 2018 Advanced Anatomy of the Neck Alex Tessnow, MD, MBA, FACE, ECNU University of Texas Southwestern Dallas, TX Content contributed by: H. Jack Baskin, Daniel Duick, Diana Dean, Robert A. Levine,
AACE 2018 Advanced Anatomy of the Neck Alex Tessnow, MD, MBA, FACE, ECNU University of Texas Southwestern Dallas, TX Content contributed by: H. Jack Baskin, Daniel Duick, Diana Dean, Robert A. Levine,
Uncommon ultrasound findings in the cervical region
 Uncommon ultrasound findings in the cervical region Poster No.: C-1132 Congress: ECR 2014 Type: Educational Exhibit Authors: V. Donciu, S. M. Petrescu, E. NEGUT, C. ZAHARIA ; 1 1 1 2 1 2 Bucharest/RO,
Uncommon ultrasound findings in the cervical region Poster No.: C-1132 Congress: ECR 2014 Type: Educational Exhibit Authors: V. Donciu, S. M. Petrescu, E. NEGUT, C. ZAHARIA ; 1 1 1 2 1 2 Bucharest/RO,
Preface... Contributors... 1 Embryology... 3
 Contents Preface... Contributors... vii xvii I. Pediatrics 1 Embryology... 3 Pearls... 3 Branchial Arch Derivatives... 3 Branchial Arch Anomalies: Cysts, Sinus, Fistulae... 4 Otologic Development... 4
Contents Preface... Contributors... vii xvii I. Pediatrics 1 Embryology... 3 Pearls... 3 Branchial Arch Derivatives... 3 Branchial Arch Anomalies: Cysts, Sinus, Fistulae... 4 Otologic Development... 4
Contents. Basic Ultrasound Principles and Terminology. Ultrasound Nodule Characteristics
 Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Alexander C Vlantis. Selective Neck Dissection 33
 05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
Neoplasms that present as a swelling in the neck may be either
 Problems in otolaryngology Inflammatory swellings Viral and bacterial infection are frequent causes of swellings in the neck. Enlargement of the cervical lymph nodes is most likely but a dormant branchial
Problems in otolaryngology Inflammatory swellings Viral and bacterial infection are frequent causes of swellings in the neck. Enlargement of the cervical lymph nodes is most likely but a dormant branchial
Hemangioma of Tongue with Phlebolith: A Rare presentation
 Journal of Government Dental College and Hospital, October 2017, Vol.-04, Issue- 01, P. 20-25 Original article: Hemangioma of Tongue with Phlebolith: A Rare presentation 1 Dr. Jigna S Shah (MDS) 1, 2 Dr.
Journal of Government Dental College and Hospital, October 2017, Vol.-04, Issue- 01, P. 20-25 Original article: Hemangioma of Tongue with Phlebolith: A Rare presentation 1 Dr. Jigna S Shah (MDS) 1, 2 Dr.
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AACE 2018 Advanced Endocrine Neck Ultrasound and UGFNA Course
 AACE 2018 Advanced Endocrine Neck Ultrasound and UGFNA Course Describe the sonographic appearance of diffuse thyroid diseases: autoimmune thyroid disease Review non thyroidal findings that can be encountered
AACE 2018 Advanced Endocrine Neck Ultrasound and UGFNA Course Describe the sonographic appearance of diffuse thyroid diseases: autoimmune thyroid disease Review non thyroidal findings that can be encountered
Chapter 20: Branchial cleft anomalies, thyroglossal cysts and fistulae. P. D. M. Ellis. Branchial cleft anomalies. Embryology
 Chapter 20: Branchial cleft anomalies, thyroglossal cysts and fistulae P. D. M. Ellis Branchial cleft anomalies and thyroglossal cysts and fistulae are the end result of defects in development in the neck
Chapter 20: Branchial cleft anomalies, thyroglossal cysts and fistulae P. D. M. Ellis Branchial cleft anomalies and thyroglossal cysts and fistulae are the end result of defects in development in the neck
Evaluation and Management of Pediatric Neck masses
 Evaluation and Management of Pediatric Neck masses Steven T. Wright, M.D. Faculty Advisor: Ronald Deskin, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation
Evaluation and Management of Pediatric Neck masses Steven T. Wright, M.D. Faculty Advisor: Ronald Deskin, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation
Peripheral mycobacterial lymphadenitis (TB, NTM and BCG)
") Peripheral mycobacterial lymphadenitis (TB, NTM and BCG) H Simon Schaaf Desmond Tutu TB Centre, Department of Paediatrics and Child Health, Stellenbosch University, Cape Town, South Africa Questions Peripheral
Peripheral mycobacterial lymphadenitis (TB, NTM and BCG) H Simon Schaaf Desmond Tutu TB Centre, Department of Paediatrics and Child Health, Stellenbosch University, Cape Town, South Africa Questions Peripheral
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Lecture 07. Lymphatic's of Head & Neck. By: Dr Farooq Amanullah Khan PMC
 Lecture 07 Lymphatic's of Head & Neck By: Dr Farooq Amanullah Khan PMC Dated: 28.11.2017 Lymphatic Vessels Of the 800 lymph nodes in the human body, 300 are in the Head & neck region. The lymphatic vessels
Lecture 07 Lymphatic's of Head & Neck By: Dr Farooq Amanullah Khan PMC Dated: 28.11.2017 Lymphatic Vessels Of the 800 lymph nodes in the human body, 300 are in the Head & neck region. The lymphatic vessels
Veins of the Face and the Neck
 Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
04 Development of the Face and Neck. Development of the Face Development of the neck
 04 Development of the Face and Neck Development of the Face Development of the neck Development of the face Overview of facial development The fourth week ~ the twelfth week of prenatal development Between
04 Development of the Face and Neck Development of the Face Development of the neck Development of the face Overview of facial development The fourth week ~ the twelfth week of prenatal development Between
1. Thyroxine (inactive form) also called T4 (90% of the secretion). 2. Triiodothyronine (active form) also called T3 (10% of the secretion).
 also called T4 (90% of the secretion). 2. Triiodothyronine (active form) also called T3 (10% of the secretion).") A Introduction The nomenclature of the thyroid gland comes from its close relation to the thyroid cartilage (the thyroid cartilage was named like this because thyroid means shield and it is shielding the
A Introduction The nomenclature of the thyroid gland comes from its close relation to the thyroid cartilage (the thyroid cartilage was named like this because thyroid means shield and it is shielding the
Management of Thyroglossal Duct Remnants: Our Experience
 ISSN 2231-4261 ORIGINAL ARTICLE Management of Thyroglossal Duct Remnants: Our Experience 1* 1 1 1 Arunkumar J. S., Shibani Anchan, Santhosh S. G., Muhammed Ahsan 1 Department of ENT, Sri Dharmastala Manjuntheswara
ISSN 2231-4261 ORIGINAL ARTICLE Management of Thyroglossal Duct Remnants: Our Experience 1* 1 1 1 Arunkumar J. S., Shibani Anchan, Santhosh S. G., Muhammed Ahsan 1 Department of ENT, Sri Dharmastala Manjuntheswara
ENT in Primary Care. Learning Objectives. Eustachian Tube (ET) Dysfunction. Eustachian Tube (ET) Dysfunction. Middle Ear Effusion
 Dysfunction. Eustachian Tube (ET) Dysfunction. Middle Ear Effusion") Learning Objectives ENT in Primary Care Paul A. Kedeshian, MD Associate Clinical Professor David Geffen School of Medicine at UCLA Department of Head and Neck Surgery Identifying common ENT problems and
Learning Objectives ENT in Primary Care Paul A. Kedeshian, MD Associate Clinical Professor David Geffen School of Medicine at UCLA Department of Head and Neck Surgery Identifying common ENT problems and
Chapter 10: Salivary Gland Disorders. Raymond P. Wood. History
 Chapter 10: Salivary Gland Disorders Raymond P. Wood Dysfunction of the salivary glands is usually manifested in one of two ways: swelling of the gland, either diffuse or discrete, or by dry mouth (xerostomia).
Chapter 10: Salivary Gland Disorders Raymond P. Wood Dysfunction of the salivary glands is usually manifested in one of two ways: swelling of the gland, either diffuse or discrete, or by dry mouth (xerostomia).
OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function
 The root of the neck Jeff Dupree, Ph.D. e mail: jldupree@vcu.edu OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function READING ASSIGNMENT: Moore and
The root of the neck Jeff Dupree, Ph.D. e mail: jldupree@vcu.edu OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function READING ASSIGNMENT: Moore and
Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi
 Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi For the purpose of anatomical description the neck is sub divided into two major triangles, the Anterior and the Posterior by muscle bellies
Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi For the purpose of anatomical description the neck is sub divided into two major triangles, the Anterior and the Posterior by muscle bellies
Sonography of soft-tissue vascular lesions
 Sonography of soft-tissue vascular lesions Oscar M. Navarro Associate Professor, University of Toronto Dept. of Diagnostic Imaging, The Hospital for Sick Children Toronto, Canada Declaration of Disclosure
Sonography of soft-tissue vascular lesions Oscar M. Navarro Associate Professor, University of Toronto Dept. of Diagnostic Imaging, The Hospital for Sick Children Toronto, Canada Declaration of Disclosure
F. B. Sobri, M. Ramli, U. N. Sari, M. Umar, and D. K. Mudrick
 Case Reports in Surgery Volume 2015, Article ID 872054, 5 pages http://dx.doi.org/10.1155/2015/872054 Case Report Papillary Carcinoma Occurrence in a Thyroglossal Duct Cyst with Synchronous Papillary Thyroid
Case Reports in Surgery Volume 2015, Article ID 872054, 5 pages http://dx.doi.org/10.1155/2015/872054 Case Report Papillary Carcinoma Occurrence in a Thyroglossal Duct Cyst with Synchronous Papillary Thyroid
A rare case of solitary toxic nodule in a 3yr old female child a case report
 Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Case Presentation and Discussion on Posterior Neck Mass. Martin Joseph S. Cabahug
 Case Presentation and Discussion on Posterior Neck Mass Martin Joseph S. Cabahug General Data: C.A, 60 y/o male Sta. Ana, Mla Chief Complaint: Posterior Neck Mass History and Physical Exam 2 wks PTA mass,
Case Presentation and Discussion on Posterior Neck Mass Martin Joseph S. Cabahug General Data: C.A, 60 y/o male Sta. Ana, Mla Chief Complaint: Posterior Neck Mass History and Physical Exam 2 wks PTA mass,
Refresher Course EAR TUMOR. Sasikarn Chamchod, MD Chulabhorn Hospital
 Refresher Course EAR TUMOR Sasikarn Chamchod, MD Chulabhorn Hospital Reference: Perez and Brady s Principles and Practice of radiation oncology sixth edition Outlines Anatomy Epidemiology Clinical presentations
Refresher Course EAR TUMOR Sasikarn Chamchod, MD Chulabhorn Hospital Reference: Perez and Brady s Principles and Practice of radiation oncology sixth edition Outlines Anatomy Epidemiology Clinical presentations
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Scrofula Joseph Junewick, MD FACR
 Scrofula Joseph Junewick, MD FACR 06/20/2012 History 4 year old male with refractory cervical adenopathy Diagnosis Scrofula Additional Clinical Positive PPD skin test. Discussion Scrofula refers to tuberculous
Scrofula Joseph Junewick, MD FACR 06/20/2012 History 4 year old male with refractory cervical adenopathy Diagnosis Scrofula Additional Clinical Positive PPD skin test. Discussion Scrofula refers to tuberculous
Anterior triangle of neck
 Anterior triangle of neck Dept. of Anatomy Zhou Hong Ying Outline boundary and subdivisions of ant. triangle contents of the triangle Muscles: suprahyoid muscles, infrahyoid muscles Nerves: CNⅩ, CNⅪ, CNⅫ,
Anterior triangle of neck Dept. of Anatomy Zhou Hong Ying Outline boundary and subdivisions of ant. triangle contents of the triangle Muscles: suprahyoid muscles, infrahyoid muscles Nerves: CNⅩ, CNⅪ, CNⅫ,
Part Ten: Thyroid / Parathyroid. Chapter 133: Anatomy. Daniel O. Graney, Ronald C. Hamaker. Development of the Thyroid Gland
 Part Ten: Thyroid / Parathyroid Chapter 133: Anatomy Daniel O. Graney, Ronald C. Hamaker Development of the Thyroid Gland The thyroid gland begins as an endodermal bud from the floor of the pharynx between
Part Ten: Thyroid / Parathyroid Chapter 133: Anatomy Daniel O. Graney, Ronald C. Hamaker Development of the Thyroid Gland The thyroid gland begins as an endodermal bud from the floor of the pharynx between
Case Presentation 主治醫師 : 宋文鑫日期 :
 Case Presentation 主治醫師 : 宋文鑫日期 : 2015-2-28 General Data Name:OOO Chart Number:OOOOOOO Date of Admission:2014 年 08 月 04 日 Age: 33 y/o Sex:female Occupation : 會計 Chief Complaint Palpable soft tissue mass
Case Presentation 主治醫師 : 宋文鑫日期 : 2015-2-28 General Data Name:OOO Chart Number:OOOOOOO Date of Admission:2014 年 08 月 04 日 Age: 33 y/o Sex:female Occupation : 會計 Chief Complaint Palpable soft tissue mass
Term: FIMS Week: CBL SESSION
 Term: FIMS Week: CBL SESSION CBL Title: Neck Lumps CBL Session Coordinators: Coordinators email/phone: Key issues that may be addressed in CBL sessions: SUGGESTED LIKELY CASES FOR DISCUSSION Patient with
Term: FIMS Week: CBL SESSION CBL Title: Neck Lumps CBL Session Coordinators: Coordinators email/phone: Key issues that may be addressed in CBL sessions: SUGGESTED LIKELY CASES FOR DISCUSSION Patient with
Title. CitationInternational Cancer Conference Journal, 4(1): Issue Date Doc URL. Rights. Type. File Information
: Issue Date Doc URL. Rights. Type. File Information") Title Lymph node metastasis in the suprasternal space from Homma, Akihiro; Hatakeyama, Hiromitsu; Mizumachi, Ta Author(s) Tomohiro; Fukuda, Satoshi CitationInternational Cancer Conference Journal, 4(1):
Title Lymph node metastasis in the suprasternal space from Homma, Akihiro; Hatakeyama, Hiromitsu; Mizumachi, Ta Author(s) Tomohiro; Fukuda, Satoshi CitationInternational Cancer Conference Journal, 4(1):